

Abstract
A prospective randomized phase III study was performed to evaluate whether intensified cytarabine would induce a higher response rate and longer event-free interval as compared to low-dose cytarabine in chronic myeloid leukemia (CML). One hundred and eighteen patients with CML in early chronic phase entered the study. Twenty-eight out of 32 patients assigned to group A received two cycles of a combination of intensified cytarabine and idarubicin followed by interferon alfa (IFN-α) maintenance, 28 patients in group B received standard treatment by a combination of low-dose cytarabine and IFN-α. Forty-nine patients with a human leukocyte antigen-identical sibling donor proceeded to allogeneic stem cell transplantation (allo-SCT) and nine patients were excluded from the analysis. Hematological response was observed in 97% of the patients in group A vs 86% of the patients in group B during the first year of treatment. In group A, 16 patients (50%) achieved a major cytogenetic response, which compared to seven patients (25%) with a major cytogenetic response in group B. With a median follow-up of 58 months (range 34–76), event-free survival was not significantly different between arms A and B. The estimated 5-year survival rate was 56% in the intensified arm and 77% in the low-dose arm (P = 0.05). Recipients of allo-SCT showed a 5-year estimated survival rate of 55%. Although intensified cytarabine induced a higher initial percentage of major and complete cytogenetic responses, responses were not sustained by IFN-α maintenance therapy.
Keywords: Chronic myeloid leukemia, Cytarabine, Interferon alfa, Allogeneic stem cell transplantation, Cytogenetic response
Introduction
Chronic myeloid leukemia is a malignant hematopoietic stem cell disorder, characterized by a unique reciprocal translocation between the long arms of chromosomes 9 and 22 resulting in an aberrant chromosome 22, also known as the Philadelphia chromosome [1]. The result of the translocation is the generation of a BCR-ABL fusion gene which encodes for a chimeric protein (p210) with dysregulated tyrosine-kinase activity sufficient for leukemogenesis in mice [2].
Before the introduction of imatinib, which is currently considered standard first line treatment, patients with CML in first chronic phase were preferably treated with a combination of interferon alfa (IFN-α) and low-dose cytarabine, as the addition of cytarabine had been shown to result in a higher response rate and enhanced survival in a randomized study [3]. We performed a pilot study in 19 patients exploring the feasibility of intensified cytarabine in patients with CML [4], as cytarabine may exert a dose–response effect in myeloid leukemias [5, 6]. This schedule of intensified cytarabine combined with idarubicin proved feasible in these patients, while an encouraging major cytogenetic response rate of 60% was observed. In contrast to acute myeloid leukemia (AML), intensive chemotherapy has received relatively little attention in CML so far, as the potential morbidity and mortality was considered a major hurdle.
In studies exploring the efficacy of intensive chemotherapy, a major cytogenetic response was observed in 30–60% of patients [7–10], but these responses proved transient without maintenance therapy. Given the dose–response effect of cytarabine in other myeloid leukemias, e.g., AML, we wished to address the question whether intensified cytarabine based chemotherapy followed by IFN-α maintenance would be superior to low-dose cytarabine combined with IFN-α.
Materials and methods
Patients with CML were eligible for randomization if they were between 16 and 65 years of age, in first chronic phase (≤ 6 months after diagnosis), WHO performance scale ≤ 2, if cytogenetic evaluation showed the Philadelphia chromosome, or the BCR-ABL oncogene was shown by polymerase chain reaction (PCR). Patients with features of accelerated phase or blastic phase were not eligible, nor were those with severe concomitant illness as severe hepatic or renal dysfunction, severe cardiac, pulmonary or neurological disease, human immunodeficiency virus infection, prior malignancies except stage I cervix carcinoma and basocellular carcinoma, and pregnant or lactating women. Patients ≤ 55 years of age with a human leukocyte antigen (HLA)-matched sibling donor were not randomized and proceeded directly to allogeneic stem cell transplantation (allo-SCT). Written informed consent was obtained from all patients.
Study design and treatment
Initially, treatment with hydroxyurea was allowed to control the white blood cell count (WBC). In this period, HLA-typing of the patients and available siblings were performed. Patients without an HLA-matched sibling donor were randomized between two groups. Randomization was stratified by center, by age (≤60 vs >60 years) and Sokal risk score (< 0.8 vs 0.8–1.2 vs >1.2). The high-dose arm A consisted of two courses of intensified cytarabine based chemotherapy. The first cycle consisted of cytarabine 200 mg/m2 (days 1–7) combined with idarubicin 12 mg/m2 (days 1 and 2). The second course consisted of high-dose cytarabine 3 g/m2 × 2 (days 1, 3, 5, and 7). The dose of cytarabine was reduced to 1 g/m2 in patients above 60 years of age. The low-dose cytarabine was given to patients assigned to arm B of the study. They received IFN-α 3–9 × 106 Units (U) daily in combination with cytarabine 20 mg/m2 s.c., days 1–10, administered every 4 weeks. If the WBC reached a nadir of 1 × 109/l or the platelet count was below 50 × 109/l, the dose of cytarabine was reduced to 15 mg/m2 for 10 days in the subsequent cycles. A similar dose adaptation was performed if the WBC and platelet count had not recovered to, respectively, 3 and 100 × 109/l, within 5 weeks after start of cytarabine. Combination therapy was given for 1 year, but could be prolonged for a maximum of 2 years in patients achieving cytogenetic response. Cytarabine was discontinued in case of a complete cytogenetic response documented twice at least 3 months apart. Both therapies were followed by IFN-α maintenance therapy until disease progression or intolerance. Maintenance treatment with IFN-α was started at a dose of 3 × 106 U daily. After 1 week, the dose was increased to 4.5–6 × 106 U daily. Thereafter, the highest tolerable dosage was given, aiming at a dose of 4.5–9 × 106 U daily. In case of common toxicity criteria (CTC), grade 3 (severe), or grade 4 (life threatening) toxicity, therapy was interrupted and resumed at a lower dose after recovery of toxicity. In case of hematological toxicity, therapy was temporarily withheld if the WBC was below 2 × 109/l or the platelet count dropped below 25 × 109/l. When the platelet count measured between 25 and 50 × 109/l, the dose was reduced with 50%. The concurrent administration of hydroxyurea was allowed only when the WBC exceeded 10 × 109/l despite adequate IFN-α treatment or above 5 × 109/l in the presence of CTC grade 3–4 toxicity, in patients not receiving low-dose cytarabine.
Endpoints
Event-free survival (EFS) was defined as the time from randomization until either no cytogenetic response achieved at 12 months, or complete loss of any cytogenetic response thereafter (documented twice), accelerated phase, blastic phase, or death, whichever came first. Overall survival (OS) was calculated from the date of registration until death from any cause. Patients still alive were censored at the time of last contact. The criteria for a complete hematological response were normalization of the WBC (< 10 × 109/l) with no immature forms, a platelet count (< 450 × 109/l) and disappearance of clinical signs and symptoms (including splenomegaly) and for failure a WBC > 20 × 109/l. A partial hematological response was defined by a WBC between 10 and 20 × 109/l or a WBC < 10 × 109/l but with > 5% immature cells or platelets > 450 × 109/l or a palpable spleen. Any hematological response is the sum of complete and partial hematological response. Cytogenetic analysis was performed every 6 months and classified as absent (100% Ph chromosome positive metaphases), minor (between 35–99% Ph chromosome positive metaphases), partial (<35% Ph chromosome positive metaphases), and complete (elimination of Ph chromosome positive metaphases).
Statistics
The primary objective of the study was to evaluate the effect of intensified cytarabine preceding IFN-α maintenance compared to low-dose cytarabine combined with and followed by IFN-α on EFS. To detect with an 80% power an increase in 5-year EFS from 32 to 50% (2-sided significance level α = 0.05) and assuming an accrual of 4 years and an additional follow-up of 2 years, 230 patients had to be randomized. Secondary endpoints were OS, hematological, and cytogenetic response between the two treatment arms, as well as side effects and infections of the different treatment regimens. Patient characteristics were compared between patient groups with the Pearson’s χ 2 test in case of discrete variables, or the Kruskal–Wallis test in case of continuous variables. Hematological and cytogenetic response rates were compared using Pearson’s χ 2 test or Fisher’s exact test, whichever appropriate. Event-free survival and OS were estimated by the actuarial Kaplan–Meier method, and 95% confidence intervals (CI) were calculated. Kaplan–Meier curves were constructed to illustrate survival, and compared between patient groups using the log-rank test. Side effects and infections were scored according to the National Cancer Institute (NCI) Common Toxicity Criteria (CTC) and summarized using descriptive statistics. All reported P-values are two-sided, and a significance level α = 0.05 was used.
Results
From February 1998 to February 2001, 118 patients entered the study. The study was closed prematurely after patient accrual ceased due to the introduction of imatinib mesylate. Sixty-three patients were randomized, 34 to arm A and 29 to arm B. However, two patients in arm A refused intensive treatment, were lost to follow-up since and have therefore been excluded from the analysis. One patient in arm B had an allogeneic donor and was therefore excluded from arm B and included in the allo-SCT group. A total of 49 patients received an allo-SCT in first chronic phase. The seven remaining patients were excluded: one patient refused randomization and was lost to follow-up, while in six patients the planned allo-SCT was cancelled or performed in accelerated phase or blastic crisis. Results are therefore presented for 32 patients in arm A, 28 in arm B, and for 49 patients who received an allo-SCT in first chronic phase. The analysis reported in this study was performed with a median follow-up of patients still alive of 58 months. Patient baseline characteristics were in general not different between the three groups (Table 1), except that patients in the allo-SCT group were somewhat younger, which is a direct consequence of the lower age limit for allo-SCT in this trial. Twenty-eight patients in group A received the two scheduled courses of intensified chemotherapy and two patients received only one course of chemotherapy. Two patients received IFN-α in combination with low-dose cytarabine instead of high-dose chemotherapy. Twenty-six patients in group B received a median of 12 courses of low-dose cytarabine (range 2–31). Two patients received IFN-α only, without addition of low-dose cytarabine as a result of early toxicity. The median IFN-α dose was 3.3 × 106 U (range 0.7–8.4) daily during 11.6 months (range 0.5–47.6) in group A and 4.9 × 106 U (range 1.6–9.1) daily (P = 0.03) during 15.2 months (range 2.3–60.9) in group B.
Table 1.
Baseline characteristics of the patients
| Characteristic | High-dose cytarabine (N = 32) | Low-dose cytarabine (N = 28) | Allogeneic transplantation (N = 49) |
|---|---|---|---|
| Age at diagnosis (year) | |||
| Median | 45 | 52 | 43 |
| Range | 22–64 | 24–65 | 17–55 |
| Sex | |||
| Male | 20 | 18 | 33 |
| Female | 12 | 10 | 16 |
| Spleen size (cm below mid left costal margin) | |||
| Median | 4 | 1 | 5 |
| Range | 0–16 | 0–20 | 0–20 |
| Platelets (×109/l) | |||
| Median | 460 | 384 | 496 |
| Range | 90–1,113 | 116–3,400 | 30–1,358 |
| White cell count (×109/l) | |||
| Median | 148 | 77 | 175 |
| Range | 5–446 | 4–323 | 12–402 |
| Blasts in peripheral blood (%) | |||
| Median | 2 | 1 | 2 |
| Range | 0–17 | 0–9 | 0–15 |
| Sokal risk group | |||
| Low <0.8 | 10 | 9 | 18 |
| Intermediate 0.8–1.2 | 12 | 10 | 14 |
| High >1.2 | 8 | 8 | 12 |
| Unknown | 2 | 1 | 5 |
| Initial hydroxyurea treatment (weeks) | |||
| Median | 10 | 8 | |
| Range | 2–60 | 2–20 | |
Hematological and cytogenetic responses, duration, and survival
The cumulative incidence of a complete hematological response was 75% in group A and 75% in group B and of a partial hematological response 22 and 11%, respectively, in the first year of treatment (Table 2). Best cytogenetic response in the first year included a major cytogenetic response in 16 patients (50%) in group A, including six patients with a complete cytogenetic response vs seven patients (25%) in group B (P = 0.06) including one patient with a complete cytogenetic response (P = 0.11). Overall, any cytogenetic response was observed in group A in 84% compared with 57% in group B (P = 0.02).
Table 2.
Cumulative incidence of hematological and cytogenetic responses in the first year of treatment
| Type of response | High-dose cytarabine (N = 32) | Low-dose cytarabine (N = 28) | P value |
|---|---|---|---|
| Hematological response | ns | ||
| Complete | 24 (75%) | 21 (75%) | |
| Partial | 7 (22%) | 3 (11%) | |
| Failure | 1 (3%) | 4 (14%) | |
| Cytogenetic response | 0.02 | ||
| Complete | 6 (19%) | 1 (4%) | 0.11 |
| Partial | 10 (31%) | 6 (21%) | |
| Minor | 11 (34%) | 9 (32%) | |
| Absent | 5 (16%) | 12 (43%) | |
Event-free survival measured 61% at 12 months and 23% at 36 months in patients receiving intensified cytarabine followed by IFN-α maintenance. By comparison, patients treated with standard low-dose cytarabine and IFN-α showed EFS of 54 and 37% at 12 and 36 months, respectively, (P = 0.83). Results are shown in Fig. 1. Although an initial higher response rate was observed in patients treated with intensified cytarabine, the response was not maintained in the majority of patients developing such a response. Fifteen of 27 responding patients lost their response including two patients with blast crisis, six patients with accelerated disease, and seven patients showed complete loss of previously established cytogenetic response. Focusing on complete cytogenetic responses: six patients in the intensified cytarabine arm obtained a complete cytogenetic response (Table 2), which lasted for a median of 5 months (range 1–10). In the standard arm, only one patient achieved a complete cytogenetic response, which has persisted for 5 years.
Fig. 1.
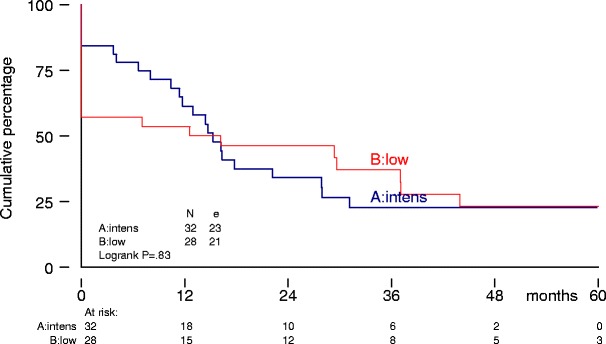
Event-free survival from randomization
The median follow-up of the 42 randomized patients who are still alive, is 58 months (range 34–76). Eighteen randomized patients have died, 13 in arm A and five in arm B (Table 3). Causes of death in group A included one patient with accelerated disease, six patients with blast crisis, three patients due to treatment related mortality (TRM), and three patients due to TRM secondary to a matched unrelated donor (MUD) allo-SCT. In contrast, five patients died in arm B, including two patients after accelerated disease, two patients after blast crisis, and one patient as a result of an unrelated illness. Consequently, at 5 years, the estimated survival rates were 56% (95% CI, 35–73%) in group A and 77% (95% CI, 52–90%) in group B (P = 0.05). Results are shown in Fig. 2.
Table 3.
Causes of death according to treatment arm
| Cause | High-dose cytarabine (N = 13) | Low-dose cytarabine (N = 5) | Allogeneic transplantation (N = 21) |
|---|---|---|---|
| Accelerated disease | 1 | 2 | 3 |
| Blast crisis | 6 | 2 | 1 |
| Treatment related mortality (TRM) | 3 | 15 | |
| TRM after matched unrelated donor transplantation | 3 | ||
| Unrelated illness | 1 | 2 | |
Fig. 2.
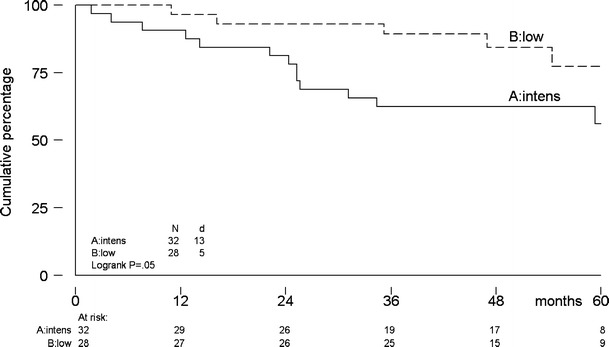
Overall survival from randomization
Discontinuation of treatment
Protocol treatment was received for a median time of 15 months in group A vs a median time of 19 months in group B. In both arms, one patient was still on protocol treatment. Reasons for going off-protocol in group A included loss of hematological or cytogenetic response in six patients and accelerated disease or blast crisis in seven patients. In addition, 18 patients changed to off-protocol treatment due to side effects of IFN-α or preference for imatinib. Reasons for going off-protocol treatment in group B included loss of hematological or cytogenetic response in four patients and accelerated disease or blast crisis in five patients. Side effects of IFN-α or a preference for imatinib were causes for off-protocol treatment in another 18 patients. Ultimately, 22 patients in group A and 22 patients in group B switched to imatinib therapy. Matched unrelated donor allo-SCT was performed in eight patients in group A and in six patients in group B. These transplants were performed because of absence of hematological response in one patient, loss of cytogenetic response in four patients, and accelerated disease or blast crisis in nine patients.
Toxicity and side effects
In group A, 49 episodes of grade II, 11 episodes of grade III, and nine episodes of grade IV toxicities were reported in 58 cycles. Grade IV toxicities included: liver function abnormalities in two patients, diarrhea in one, drug-related fever in one, cutaneous lesions in one, cardiac arrhythmia in one, dyspnoe in two, and ARDS in one. Two toxic deaths were reported in this group. In group B, 35 episodes of grade II, nine episodes of grade III, and no grade IV toxicities were reported in 74 periods of 6 months treatment. More grade II–IV infections were observed in group A: 42 vs 7 episodes in group B.
Allogeneic stem cell transplantation
Conditioning therapy for allo-SCT was myeloablative in all patients and consisted of total-body irradiation (TBI) in combination with cyclophosphamide in 43 patients and chemotherapy only (busulfan and cyclophosphamide) in six patients. Table 4 shows details with respect to conditioning therapy, graft characteristics, and immunosuppressive regimen applied. Sixteen patients developed acute grade II–IV graft vs host disease (GVHD), chronic GVHD was observed in 25 patients, in 10 limited, and extended in 15. After a median follow-up of 58 months (range 19–77), 21 patients had died. Causes of death included TRM in 15 patients, progression of CML in four patients (accelerated disease in three and blastic crisis in one), and intercurrent illness in two patients. Donor lymphocyte infusions (DLI) were given to 25 of the 49 who received an allo-SCT. In four patients it was given prophylactically, in five patients for molecular residual disease, in 14 patients as a treatment for cytogenetic relapse, and in two patients after accelerated disease or blast crisis. Thirteen patients became PCR negative again after DLI. Recipients of allo-SCT showed a 5-year estimated survival of 55% (95% CI, 39–68%). Results are shown in Fig. 3.
Table 4.
Patient and donor and graft characteristics of allo-SCT recipients
| Parameter | Number |
|---|---|
| Patient | |
| CMV+ | 20 |
| CMV− | 27 |
| Unknown | 2 |
| Conditioning regimen | |
| Cyclophosphamide/TBI | 43 |
| Busulphan/cyclophosphamide | 6 |
| Donor | |
| Age (year) median, range | 42 (13–64) |
| Sex | |
| Female | 25 |
| Male | 24 |
| CMV+ | 21 |
| CMV− | 22 |
| Unknown | 6 |
| Donor relation to patient | |
| HLA-identical sib | 47 |
| Identical twin | 2 |
| Source of stem cells | |
| Bone marrow | 33 |
| Peripheral blood | 16 |
| Nucleated cells infused | |
| CD34+ 109/l (median, range) | 2.4 (0.6–8.5) |
| T-cell depletion | |
| No | 12 |
| Yes | 37 |
| Immunosuppression | |
| Ciclosporine | 33 |
| Ciclosporine and MTX | 6 |
| Other | 3 |
| No medication | 7 |
Fig. 3.
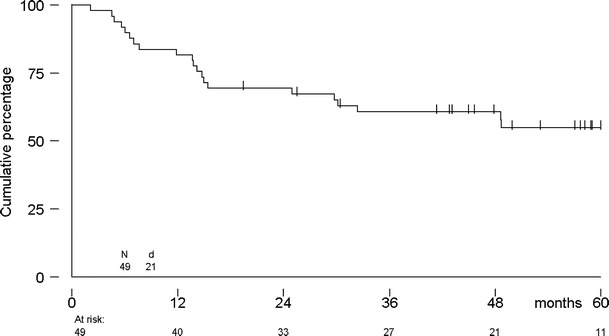
Overall survival from allogeneic stem cell transplantation
Discussion
In this prospective randomized study, started before the introduction of imatinib, we compared intensified cytarabine followed by IFN-α maintenance with low-dose cytarabine combined with IFN-α. The design of the study was based on earlier experience by us and others [4, 7–9] and on the assumption that cytarabine may exert a dose-dependent effect as can be observed in AML [5, 6]. In addition, as previous studies evaluating more intensive chemotherapy showed relatively high rates of cytogenetic relapse, we added IFN-α maintenance after two courses of chemotherapy to prevent relapse. While the cytogenetic response rate proved superior in the intensified arm (P = 0.02), the majority of patients lost their initial cytogenetic response emphasizing that IFN-α maintenance proved to be insufficient to preserve the initial cytogenetic response. As a result, EFS was comparable among the two treatment arms.
The lack of a sustained beneficial effect of intensified cytarabine followed by IFN-α maintenance may be explained in several ways. Cytarabine acts almost exclusively on proliferating cells. Apart from a large pool of proliferating malignant mature and more immature myeloid cells, CML is also characterized by the presence of quiescent noncycling Ph+ progenitors [11–14], which may not have been affected sufficiently by cytarabine. As earlier shown by Holyoake et al. [12], these progenitors may have a proliferative advantage over their quiescent normal counterparts and may, hereby, be responsible for gradually resuming malignant hematopoiesis after recovery from cytarabine induced cytopenia. Interferon-alfa maintenance did not prevent the regrowth of malignant hematopoiesis in most patients with an initial cytogenetic response. In view of the relatively low rates of complete cytogenetic responses to IFN-α [3, 15], also IFN-α may have been unable to eliminate malignant progenitor cells that were responsible for the recapitulation of malignant hematopoiesis in our patients. The relatively low dose of IFN-α administered after intensified cytarabine may have contributed to that effect. However, reports in literature do not support a dose response effect for IFN-α. A metaanalysis of three prospective controlled trials comparing low-dose and high-dose IFN-α showed no benefit for high-dose therapy [16].
What has been accomplished with intensive therapy so far? Kantarjian et al. [9] treated 32 patients with intensive chemotherapy consisting of daunorubicin, cytarabine, vincristine, and prednisone followed by IFN-α maintenance. Overall, 60% of patients showed a major cytogenetic response, but only eight patients (25%) had a sustained cytogenetic response. No survival benefit was observed compared with a matched historical control group. Improved survival by intensive chemotherapy was suggested by Giles et al. [10] in patients who did not benefit from IFN-α. The projected 10-year survival was 50% for the study group vs 35% for patients who received an IFN-α based regimen at the MD Anderson. Alternatively, chemotherapy may be further intensified and supported by autologous transplantation. McGlave et al. [17] summarized results of eight transplant centers. One hundred and forty-two patients in first chronic phase received an autologous transplantation. The 3-year survival was approximately 60% with some indication of a plateau after 3.6 years in the survival curve. Simonsson et al. [18] reported the Swedish results with autologous transplantation. Initial treatment included hydroxyurea and IFN-α and one to three courses of intensive chemotherapy. The actuarial 6-year survival from diagnosis of all 160 registered patients was 68%, including 30 patients having received an autograft and 59 patients who were allografted. The survival of 581 patients retrieved from the EBMT registry who received an autologous transplantation between 1983 and 1998 were reported by Olavarria et al. [19]. The median survival was 8 years from SCT without indication of a plateau in survival curve. Patients with a major cytogenetic response 1–2 years post SCT and also patients who received IFN-α post SCT did significantly better. Although none of these studies show definite proof of a survival advantage with intensive therapy, a subgroup of yet to be defined patients could potentially benefit from more intensive chemotherapy.
Is there still a role for chemotherapy in the current imatinib era? In the IRIS trial, the estimated rate of major cytogenetic response and complete cytogenetic response rates were 87 and 76% in the imatinib group, respectively, compared with 35 and 15% in the group given IFN-α plus cytarabine at 18 months [20]. Less then 5% of patients achieved a complete molecular response. In patients with a major molecular response within 12 months, estimated progression-free survival at 24 months was 100% compared with 95% for patients in complete cytogenetic response without a 3 log reduction of BCR-ABL and 85% for patients who did not have a complete cytogenetic remission [21]. As a result, the current goal of treatment in first chronic phase CML patients is to aim for a major molecular response [21, 22]. Resistance, however, is a major concern. Different mechanisms of resistance against imatinib have been reported, including, mutations of the BCR-ABL kinase domain, gene amplification or overexpression of BCR-ABL, clonal evolution, overexpression of the multidrug resistance P-glycoprotein, and inactivation by α-1 acid glycoprotein [23–27]. Currently, combination therapies are being developed to prevent resistance or to treat patients that have acquired resistance [28]. Apart from the combination of imatinib with alternative signal transduction inhibitors, also the combination with conventional chemotherapy is being explored. With respect to the combination of imatinib and cytarabine, two groups have reported initial results. The French CML group performed a phase II trial in 30 patients [29]. A complete cytogenetic response was obtained in 70% of the patients at 12 months. We performed a phase I/II study exploring the feasibility and efficacy of escalating doses of imatinib and two different dosages of cytarabine [30]. The probability of reaching a complete cytogenetic response was 67%, a major molecular response was 51%, and a complete molecular response was 28% at 18 months of treatment. While these initial molecular results seem promising, longer follow-up is needed to evaluate whether cytarabine significantly adds to the efficacy of imatinib and may prevent resistance.
In conclusion, high-dose cytarabine based chemotherapy followed by IFN-α maintenance was not better as compared to low-dose cytarabine in combination with IFN-α in early diagnosed CML patients. As imatinib may reverse the relative insensitivity to chemotherapeutic agents [31, 32], the role of chemotherapy now deserves to be defined in particular in combinations with imatinib, with the purpose of preventing and treating tyrosine kinase inhibitor resistant CML.
References
- 1.Rowley JD. A new consistent chromosomal abnormality in chronic myelogenous leukaemia identified by quinacrine fluorescence and Giemsa staining. Nature. 1973;243:290–293. doi: 10.1038/243290a0. [DOI] [PubMed] [Google Scholar]
- 2.Daley GQ, Van Etten RA, Baltimore D. Induction of chronic myelogenous leukemia in mice by the P210bcr/abl gene of the Philadelphia chromosome. Science. 1990;344:251–253. doi: 10.1126/science.2406902. [DOI] [PubMed] [Google Scholar]
- 3.Guilhot F, Chastang C, Michallet M, Guerci A, Harousseau JL, Maloisel F, Bouabdalla R, Guyotat D, Cheron N, Nicolini F, Abgrall JF, Tanzer J. Interferon alpha-2b combined with cytarabine versus interferon alone in chronic myelogenous leukemia. N Engl J Med. 1997;337:223–229. doi: 10.1056/NEJM199707243370402. [DOI] [PubMed] [Google Scholar]
- 4.Janssen JJ, van Rijn RS, van der Holt B, Schuurhuis GJ, Vellenga E, Verhoef GE, Ossenkoppele GJ, van den Berg E, Hagemeijer A, Slater R, Nieuwint AW, Cornelissen JJ. Mobilisation of haemopoietic progenitors in CML: a second course of intensive chemotherapy does not improve Ph-negativity in stem cell harvests. Bone Marrow Transplant. 2000;25:1147–1155. doi: 10.1038/sj.bmt.1702420. [DOI] [PubMed] [Google Scholar]
- 5.Mayer RJ, Davis RB, Schiffer CA, Berg DT, Powell BL, Schulman P, Omura GA, Moore JO, McIntyre OR, Frei E. Intensive post-remission chemotherapy in adults with acute myeloid leukemia. N Engl J Med. 1994;331:896–903. doi: 10.1056/NEJM199410063311402. [DOI] [PubMed] [Google Scholar]
- 6.Bishop JF, Matthews JP, Young GA, Szer J, Gillett A, Joshua D, Bradstock K, Enno A, Wolf MM, Fox R. A randomized study of high-dose cytarabine in induction in acute myeloid leukemia. Blood. 1996;87:1710–1717. [PubMed] [Google Scholar]
- 7.Cunningham I, Gee T, Dowling M, Chaganti R, Bailey R, Hopfan S, Bowden L, Turnbull A, Knapper W, Clarkson B. Results of treatment of Ph’+ chronic myelogenous leukemia with an intensive treatment regimen (L-5 protocol) Blood. 1979;53:375–395. [PubMed] [Google Scholar]
- 8.Kantarjian HM, Vellekoop L, McCredie KB, Keating MJ, Hester J, Smith T, Barlogie B, Trujillo J, Freireich EJ. Intensive combination chemotherapy (ROAP 10) and splenectomy in the management of chronic myelogenous leukemia. J Clin Oncol. 1985;3:192–200. doi: 10.1200/JCO.1985.3.2.192. [DOI] [PubMed] [Google Scholar]
- 9.Kantarjian HM, Talpaz M, Keating MJ, Estey EH, O’Brien S, Beran M, McCredie KB, Gutterman J, Freireich EJ. Intensive chemotherapy induction followed by Interferon-alpha maintenance in patients with Philadelphia chromosome-positive chronic myelogenous leukemia. Cancer. 1991;68:1201–1207. doi: 10.1002/1097-0142(19910915)68:6<1201::AID-CNCR2820680604>3.0.CO;2-1. [DOI] [PubMed] [Google Scholar]
- 10.Giles FJ, Kantarjian H, O’Brien S, Rios MB, Cortes J, Beran M, Koller C, Keating M, Talpaz M. Results of therapy with interferon alpha and cyclic combination chemotherapy in patients with Philadelphia chromosome positive chronic myelogenous leukemia in early chronic phase. Leuk Lymphoma. 2001;41:309–319. doi: 10.3109/10428190109057985. [DOI] [PubMed] [Google Scholar]
- 11.Holyoake TL, Jiang X, Eaves C, Eaves A. Isolation of a highly quiescent subpopulation of primitive leukemic cells in chronic myeloid leukaemia. Blood. 1999;94:2056–2064. [PubMed] [Google Scholar]
- 12.Holyoake TL, Jiang X, Jorgensen HG, Graham S, Alcorn MJ, Laird C, Eaves AC, Eaves CJ. Primitive quiescent leukemic cells from patients with chronic myeloid leukaemia spontaneously initiate factor-independent growth in vitro in association with up-regulation of expression of interleukin-3. Blood. 2001;97:720–728. doi: 10.1182/blood.V97.3.720. [DOI] [PubMed] [Google Scholar]
- 13.Bhatia R, Holtz M, Niu N, Gray R, Snyder DS, Sawyers CL, Arber DA, Slovak ML, Forman SJ. Persistence of malignant hematopoietic progenitors in chronic myelogenous leukemia patients in complete cytogenetic remission following imatinib mesylate treatment. Blood. 2003;101:4701–4707. doi: 10.1182/blood-2002-09-2780. [DOI] [PubMed] [Google Scholar]
- 14.Graham SM, Jorgensen HG, Allan E, Pearson C, Alcorn MJ, Richmond L, Holyoake TL. Primitive, quiescent, Philadelphia-positive stem cells from patients with chronic myeloid leukaemia are insensitive to STI571 in vitro. Blood. 2002;99:319–325. doi: 10.1182/blood.V99.1.319. [DOI] [PubMed] [Google Scholar]
- 15.Allan NC, Richards SM, Shepherd PCA. UK Medical Research Council randomised, multicentre trial of interferon-αn1 for chronic myeloid leukaemia: improved survival irrespective of cytogenetic response. Lancet. 1995;345:1392–1397. doi: 10.1016/S0140-6736(95)92596-1. [DOI] [PubMed] [Google Scholar]
- 16.Kluin-Nelemans HC, Buck G, le Cessie S, Richards S, Beverloo HB, Falkenburg JHF, Littlewood T, Muus P, Bareford D, van der Lelie H, Green AR, Roozendaal KJ, Milne AE, Chapman CS, Shepherd P, for the UK CML Working Group of NCRI and the HOVON trials group Randomized comparison of low-dose versus high-dose interferon-alfa in chronic myeloid leukemia: prospective collaboration of 3 joint trials by the MRC and HOVON groups. Blood. 2004;103:4408–4415. doi: 10.1182/blood-2003-10-3605. [DOI] [PubMed] [Google Scholar]
- 17.McGlave PB, De Fabritiis P, Deisseroth A, Goldman J, Barnett M, Reiffers J, Simonsson B, Carella A, Aeppli D. Autologous transplants for chronic myelogenous leukaemia: results from eight transplant groups. Lancet. 1994;343:1486–1488. doi: 10.1016/S0140-6736(94)92589-5. [DOI] [PubMed] [Google Scholar]
- 18.Simonsson B, Öberg G, Björeman M, Björkholm M, Carneskog J, Gahrton G, Hast R, Karl H, Lanng-Nielsen J, Lofvenberg E, Malm C, Turesson I, Uden AM, Vilen L, Weis-Bjerrum O. Intensive treatment in order to minimize the Ph-positive clone in CML. Bone Marrow Transplant. 1996;17:S63–S64. [PubMed] [Google Scholar]
- 19.Olavarria E, Reiffers J, Boque C, Sureda A, Meloni G, Michallet M, Clark RE, Blaise D, Carella AM, Cahn JY, Jouet JP, Rizzoli V, Van Biezen A, Gratwohl A, Goldman JM, Niederwieser D, Apperley JF. The post-transplant cytogenetic response to interferon is a major determinant of survival after autologous stem cell transplantation for chronic myeloid leukaemia in chronic phase. Br J Haematol. 2002;119:762–770. doi: 10.1046/j.1365-2141.2002.03600.x. [DOI] [PubMed] [Google Scholar]
- 20.O’Brien SG, Guilhot F, Larson RA, Gathmann I, Baccarani M, Cervantes F, Cornelissen JJ, Fischer T, Hochhaus A, Hughes T, Lechner K, Nielsen JL, Rousselot P, Reiffers J, Saglio G, Shepherd J, Simonsson B, Gratwohl A, Goldman JM, Kantarjian H, Taylor K, Verhoef G, Bolton AE, Capdeville R, Druker BJ. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukaemia. N Engl J Med. 2003;348:994–1004. doi: 10.1056/NEJMoa022457. [DOI] [PubMed] [Google Scholar]
- 21.Hughes TP, Kaeda J, Branford S, Rudzki Z, Hochhaus A, Hensley ML, Gathmann I, Bolton AE, van Hoomissen IC, Goldman JM, Radich JP. Frequency of major molecular responses to imatinib or interferon alfa plus cytarabine in newly diagnosed chronic myeloid leukaemia. N Engl J Med. 2003;349:1423–1432. doi: 10.1056/NEJMoa030513. [DOI] [PubMed] [Google Scholar]
- 22.Goldman J. Monitoring minimal residual disease in BCR-ABL-positive chronic myeloid leukaemia in the imatinib era. Curr Opin Hematol. 2004;12:33–39. doi: 10.1097/01.moh.0000148551.93303.9e. [DOI] [PubMed] [Google Scholar]
- 23.Roche-Lestienne C, Soenen-Cornu V, Grardel-Duflos N, Lai JL, Philippe N, Facon T, Fenaux P, Preudhomme C. Several types of mutations of the Abl gene can pre-exist to the onset, of treatment. Blood. 2002;100:1014–1018. doi: 10.1182/blood.V100.3.1014. [DOI] [PubMed] [Google Scholar]
- 24.Gorre ME, Mohammed M, Ellwood K, Hsu N, Paquette R, Rao PN, Sawyers CL. Clinical resistance to STI-571 cancer therapy caused by BCR-ABL gene mutation or amplification. Science. 2001;292:876–880. doi: 10.1126/science.1062538. [DOI] [PubMed] [Google Scholar]
- 25.Marktel S, Marin D, Foot N, Szydlo R, Bua M, Karadimitris A, De Melo VA, Kotzampaltiris P, Dazzi F, Rahemtulla A, Olavarria E, Apperley JF, Goldman JM. Chronic myeloid leukaemia in chronic phase responding to imatinib: the occurrence of additional cytogenetic abnormalities predicts disease progression. Hematologica. 2003;88:260–267. [PubMed] [Google Scholar]
- 26.Mahon FX, Deininger MW, Shultheis B, Chabrol J, Reiffers J, Goldman JM, Melo JV. Selection and characterization of BCR-ABL positive cell lines with differential sensitivity to the tyrosine kinase inhibitor STI571: diverse mechanisms of resistance. Blood. 2000;96:1070–1079. [PubMed] [Google Scholar]
- 27.Gambacorti-Passerini C, Zucchetti M, Russo D, Frapolli R, Verga M, Bungaro S, Tornaghi L, Rossi F, Pioltelli P, Pogliani E, Alberti D, Corneo G, D’Incalci M. Alpha1 acid glycoprotein binds to imatinib (STI571) and substantially alters its pharmacokinetics in chronic myeloid leukemia patients. Clin Cancer Res. 2003;9:625–632. [PubMed] [Google Scholar]
- 28.Deininger M, Buchdunger E, Druker BJ. The development of imatinib as a therapeutic agent for chronic myeloid leukemia. Blood. 2005;105:2640–2653. doi: 10.1182/blood-2004-08-3097. [DOI] [PubMed] [Google Scholar]
- 29.Gardembas M, Rousselot P, Tulliez M, Vigier M, Buzyn A, Rigal-Huguet F, Legros L, Michallet M, Cheron N, Maloisel F, Mahon F-X, Facon T, Berthaud P, Guilhot J, Guilhot F, for the CML French Group Results of a prospective phase 2 study combining imatinib mesylate and cytarabine for the treatment of Philadelphia-positive patients with chronic myelogenous leukaemia in chronic phase. Blood. 2003;102:4298–4305. doi: 10.1182/blood-2003-04-1010. [DOI] [PubMed] [Google Scholar]
- 30.Cornelissen JJ, Valk P, Verhoef GEG, Smit WM, van Marwijk-Kooij M, Wittebol S, van Oers MHJ, Kluin-Nelemans HC, Lowenberg B, Willemze R, Schattenberg AVMB, Ossenkoppele G (2004) High rates of molecular response and low incidence of mutations in patients treated with newly diagnosed chronic myeloid leukaemia (CML) treated with a dose-escalated combination of imatinib and cytarabine. Blood 104(11) (Abstract 19)
- 31.Thiesing JT, Sayuri OJ, Kolibaba KS, Druker BJ. Efficacy of STI571, an Abl tyrosine kinase inhibitor, in conjunction with other antileukemic agents against Bcr-Abl-positive cells. Neoplasia. 2002;96:3195–3199. [PubMed] [Google Scholar]
- 32.La Rosee P, O’Dwyer ME, Druker BJ. Insights from pre-clinical studies for new combination treatment regimens with the Bcr-Abl kinase inhibitor imatinib mesylate (Gleevec/Glivec) in chronic myelogenous leukemia: a translational perspective. Leukemia. 2002;16:1213–1219. doi: 10.1038/sj.leu.2402555. [DOI] [PubMed] [Google Scholar]