

ABSTRACT |
Background:
The prevalence of low back pain is high among the economically active population. Low back pain reduces productivity and causes absenteeism, impaired quality of life and leaves of absence. Several measures were suggested to reduce the occurrence of this occupational condition, among which physical exercise at the workplace stands out.
Aim:
To analyze studies which assessed physical exercise at the workplace for treatment of low back pain.
Methods:
The present study consisted of a systematic review with meta-analysis. An electronic search was conducted on database MEDLINE using keywords “workplace,” “low back pain” and “exercise,” synonyms and headings located on Health Sciences Descriptors and Medical Subject Headings. We considered all the studies that included physical exercise at the workplace and defined low back pain as outcome.
Results:
We located 499 potential studies and finally included 15 for review. The duration of treatment varied from 3 weeks to 18 months, and the main interventions were strength and stretching exercises and muscle relaxation.
Conclusions:
The meta-analysis showed that physical exercise at the workplace did not reduce the occurrence of low back pain (difference of means=0.62, 95%CI -0.8-2.04, p<0.4). The present systematic review was registered in database PROSPERO, registration number CRD42017071563.
Keywords |: workplace, low back pain, exercise
RESUMO |
Contexto:
A dor lombar apresenta alta prevalência na população economicamente ativa, promovendo a diminuição da capacidade produtiva, absenteísmo, prejuízos à qualidade de vida e afastamento previdenciário. Medidas diversas têm sido adotadas no intuito de diminuir esse infortúnio laboral, destacando-se a prática de exercício físico no ambiente de trabalho.
Objetivo:
O objetivo desta revisão foi identificar estudos que utilizaram o exercício físico realizado no ambiente laboral para tratamento da dor lombar.
Métodos:
Trata-se de uma revisão sistemática com metanálise. Foi realizada busca eletrônica na base de dados MEDLINE utilizando os descritores “workplace”; “low back pain” e “exercise” e os respectivos sinônimos e palavras-chaves identificados nos Descritores em Ciências da Saúde e no Medical Subject Headings.
Resultados:
Foram considerados todos os estudos que adotaram exercício físico no ambiente de trabalho e possuíam desfechos relacionados à dor lombar. Foram encontrados 499 estudos em potencial, resultando na inclusão final de 15 artigos. O tempo de tratamento variou de 3 semanas a 18 meses, e as principais intervenções foram exercícios de força, alongamentos e relaxamento muscular.
Conclusão:
A metanálise demonstrou que não há efeito do exercício físico no ambiente de trabalho na redução da percepção da dor lombar (diferença entre médias=0.62, CI95%, -0.8,2.04; p<0.4). Esta revisão sistemática foi registrada no PROSPERO, sob protocolo CRD42017071563.
INTRODUCTION
The prevalence of low back pain, which might be defined as pain between the lower rib margin and the gluteal fold1, is high: about 84% of adults will complain of low back pain at some point in life2. A systematic review3 analyzed the literature on low back pain among the Brazilian population. The results showed a larger number of chronic episodes (14.7%) in a town with higher proportion of non-whites, individuals from lower social classes, lower educational level, obese and with sedentary lifestyle compared to another town with a predominantly white population and better socioeconomic and health indices (4.2 to 9.6%).
The prevalence of low back pain varies considerably among groups of Brazilian workers as a function of time frame and job. In a study4 conducted with 410 Brazilian male truck drivers, the prevalence of low back pain was 59%. In another study5 that assessed 61 workers involved in patient transport, prevalence was 11.9% (along a 7-day period) and 59% (along one year). Relative to office workers, a study6 with 505 employees of a Brazilian public university found that 19.4% complained of low back pain.
Low back pain has multifactorial etiology, including social and mental factors, as well as risk factors such as excess weight7, low physical activity levels and type of job8-involving lifting weights and repeated movements3. Treatment of patients with low back pain is essentially based on rehabilitation, which comprises physical exercise, manual procedures and pharmacological treatment9. The available evidence indicates that physical exercise plays an outstanding role in both prevention and treatment of low back pain, as in addition to contributing to reduce signs and symptoms, it improves the functional status of patients10.
Performance of physical activity at the workplace is a strategy suggested to prevent occupational musculoskeletal injury. Programs usually include muscle strengthening and stretching exercises, in addition to other tasks involving motor coordination and muscle relaxation11,12. Nevertheless, the actual effectiveness of interventions for prevention of this type of occupational injury to reduce the occurrence of low back pain might be put into question. Exercise at the workplace might afford several benefits to workers with musculoskeletal complaints, as well as to the ones who perform repeated tasks, such as increased productivity, feeling of professional recognition and, at least theoretically, prevention of musculoskeletal injury. Several authors did describe such effects13,14, but their assertions have been contested15.
Despite the acknowledged effects of exercise to improve physical fitness aspects, such as muscle strength and flexibility, performance of any modality of physical activity at the workplace is not legally compulsory in Brazil. Given the aforementioned considerations, we performed a systematic review with meta-analysis of studies that assessed physical exercise at the workplace for treatment of low back pain.
METHODS
The present study consisted of a systematic review with meta-analysis, following PRISMA recommendations, of studies located on the electronic database MEDLINE via PubMed. The search was conducted from May through September 2017 using keywords related to workplace, physical exercise and low back pain and Boolean operators “OR” and “AND.” “Workplace” and “exercise” were the keywords selected from Descritores em Ciências da Saúde (Health Sciences Descriptors, DeCS) and Medical Subject Headings (MeSH). The search had no limits for year of publication, language or follow-up length. Low back pain was defined as pain between the lower rib margin and the gluteal fold. Outcome low back pain ought to be described in the included studies. The protocol describing the steps followed in the present systematic review was registered in International Prospective Register of Systematic Reviews (PROSPERO) registration number CRD42017071563.
SEARCH STRATEGY
In the present systematic review we employed a broad-scoped combination of keywords relevant to the research question. The search strategy considered recommendations to achieve high sensitivity (about 99%) and moderate specificity (about 70%) in the retrieval of clinical trials16: “Search ((((((clinical[Title/Abstract] AND trial[Title/Abstract]) OR clinical trials as topic[MeSH Terms] OR clinical trial[Publication Type] OR random*[Title/Abstract] OR random allocation[MeSH Terms] OR therapeutic use[MeSH Subheading])))) AND ((((((workplace) OR working environment) OR work location) OR work place) OR work-site) OR worksite)) AND ((((((exercise) OR exercise therapy) OR therapy, exercise) OR gymnastics) AND (exercise movement and techniques)) OR muscle stretching exercises)”.
RESEARCH QUESTION
The aim of the present review was to investigate the effect of physical exercise at the workplace for treatment of low back pain.
INCLUSION CRITERIA
The following types of studies were included in the present review:
Clinical trials that assessed physical exercise at the workplace;
Studies which sought to analyze improvement of low back pain or changes in the occurrence of cases;
Studies which included other procedures in combination with physical exercise, such as ergonomic orientation and/or bodily practices.
EXCLUSION CRITERIA
The exclusion criteria concerned methodological aspects:
Studies which did not specify eligibility criteria;
Studies in which subjects were not randomly allocated to groups;
Studies in which groups were not similar in regard to the most relevant prognostic indicators;
Studies that did not describe the results of intergroup statistical comparison of at least one key-outcome.
DATA COLLECTION
Relevant articles were first selected based on their titles and abstracts; next we performed full-text analysis of the articles located in the database.
The selected articles were first subjected to exploratory full-text analysis, which was followed by in-depth selective analysis of relevant parts. The data extracted from articles (authors, title, journal, summary and conclusions) were recorded to order and summarize the material in a way it could yield information relevant to the study aims.
Methodological assessment and data extraction were independently performed by two reviewers. In case of disagreement, the full text of articles was reanalyzed, and when discrepancies persisted, a third reviewer was called in to solve them. Finally, meta-analysis was performed with software Review Manager Analysis (RevMan 5.3), Cochrane Collaboration. Effects were summarized as difference of means with 95% confidence interval (95%CI) by means of a random effects model. The I2 statistic was used to investigate heterogeneity.
RESULTS
The initial search retrieved 499 articles, from which 443 were excluded based on title and/or abstract analysis; as a result 56 articles were subjected to full-text analysis. Following application of the inclusion criteria, 15 studies were selected for review (Figure 1). Only 5 articles (33.3%) scored 7 or higher on the PEDro scale (Chart 1).
Figure 1. Selection of randomized controlled studies located on electronic search, Salvador, 2017.
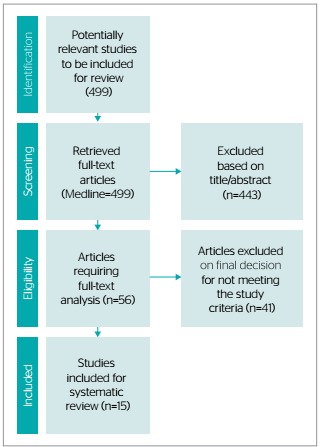
Chart 1. Studies included for review, effects, assessment measurements and methodological quality according to the PEDro scale, Salvador, 2017.
| Author, year | Population | Intervention | Follow-up | Outcome | Assessment | Results | PEDro score |
|---|---|---|---|---|---|---|---|
| Telles et al., 200917 | 291 professional computer users | Intervention (n=146): yoga program Control (n=145): usual recreational activities | 2 months | Musculoskeletal discomfort and low back flexibility | Musculoskeletal disorders were assessed with the Nordic Musculoskeletal Questionnaire; flexibility testing | Group intervention exhibited significant reduction of musculoskeletal discomfort (p<0.01) and improved low back flexibility (p<0.001) | 5/10 |
| Kamioka et al., 201118 | 88 female caregivers in nursing homes | Intervention (n=44): stretching exercises based on the MacKenzie method and orientation on posture Control (n=44): orientation on exercise | 12 weeks | Low back pain | Low back pain was assessed on Visual Analogue Scale (VAN) | Improvement in intervention group was not significant; no changes on VAS. However, the control group exhibited higher scores (p=0.068) | 5/10 |
| Del Pozo-Cruz et al., 201219 | 100 office workers | Intervention (n=50): physical training program combined with orientation on posture by means of online videos Control (n=50): orientation per e-mail | 9 months | Low back pain | Low back pain episodes; functional disability by means of the Roland-Morris Disability Questionnaire | The scores on the Roland-Morris Disability Questionnaire improved for the intervention group (95%CI -8.41--6.31) and became poorer for the control group (95%CI 0.71-2.65) | 7/10 |
| Alexandre et al., 200120 | 56 nursing professionals | Intervention (n=27): strength and flexibility exercising program combined with educational program for posture Control (n=29): lecture on spine anatomy and patient transfer techniques | 4 months | Backache | Low back pain was assessed with a pain intensity VAS. Use of medications and frequency of backache were assessed through a questionnaire | Reduced use of medications (p=0.0002), frequency of pain in home activities (p=0.000) and pain intensity (p=0.008) in group intervention | 4/10 |
| Pillastrini et al., 200921 | 71 nursery school teachers | Intervention (n=35): program to reinforce lumbar extension and strengthen the primary stabilizers of the spine + orientation on low back pain Control (n=36): ergonomic brochure | 3 weeks | Neck and low back pain | Physical ability was measured by means of the Roland-Morris Disability Questionnaire and the Oswestry Disability Index. Pain intensity was assessed with VAS | Significant improvement of neck pain (p=0.0246), perceived pain on VAS (62.9%) and physical capacity (37.2%) in group intervention | 8/10 |
| Horneij et al., 200122 | 282 nursing aides and assistant nurses | Intervention 1 (n=90): individual physical training program Intervention 2 (n=93): group stress management program Control (n=99): orientation on environment changes and health | 18 months | Backache and interference with work | Musculoskeletal disorders were assessed with the Nordic Musculoskeletal Questionnaire | Group intervention 1 reported less interference of spine discomfort (especially on the low back area) with work compared to the control group (p=0.02). Group intervention 2 did not exhibit any difference compared to the control group (p=0.057) | 4/10 |
| Anema et al., 200723 | 196 workers | Intervention 1 (n=96): workplace assessment and changes and case management Intervention 2 (n=100): orientation on usual care | 8 weeks | Return to work and functional status | Workplace assessment and length of sick leaves. Functional status was assessed through a questionnaire | Intervention 1 was associated with better return-to-work outcomes and improved functional status compared to intervention 2 (HR=1,7; 95%CI 1.2-2.3; p=0.002). | 7/10 |
| Ewert et al., 200924 | 169 nurses | Intervention 1 (n=86): warming up, strengthening, stretching and aerobic exercises Intervention 2 (n=83): segmental stabilization exercises, psychological and ergonomic orientation | 13 weeks | Backache and interference with work | Pain interference and intensity were measured by means of the West Haven-Yale Multidimensional Pain Inventory and Short Form-36 | There was not any statistically significant difference between the groups. Both programs had small to moderate effects. For pain interference, the effect size of intervention 1 was 0.58 and 0.47 for intervention 2 | 6/10 |
| Nassif et al., 201125 | 75 workers | Intervention (n=37): muscle strength, flexibility and endurance training sessions Control (n=38): no direct intervention | 6 months | Low back pain and flexibility | Pain-related parameters were assessed by means of questionnaires and scales. Pain intensity was assessed on VAS. Physical assessment based on tests | Reduction of pain-related parameters (p<0.025) and pain intensity in group intervention compared to the control group (1.8 vs. 0.51) and improved flexibility (p<0.0001) | 4/10 |
| Elfering et al., 201326 | 54 office workers | Intervention (n=27): vibration training Control (n=27): same training starting 4 weeks later | 4 weeks | Musculoskeletal pain and body balance | Musculoskeletal pain was assessed with the Nordic Musculoskeletal Questionnaire. Body balance was assessed by means of the clinical test of sensory integration of balance (CTSIB) | Musculoskeletal pain significantly decreased among the participants who reported low back pain (p<0.05). Body balance was significantly increased (p<0.05) | 5/10 |
| Jakobsen et al., 201527 | 200 healthcare workers from 3 hospitals | Intervention (n=111): supervised high-intensity strength training with resistance bands and kettlebells at the workplace Control (n=89): exercise at home during leisure time | 10 weeks | Musculoskeletal pain, muscle strength and use of analgesics | Pain was assessed on VAS. Pain areas were defined based on the Nordic Musculoskeletal Questionnaire. Muscle strength testing. Use of analgesics was assessed through a questionnaire | Pain intensity, back muscle strength and use of analgesics improved in group intervention (p<0.05). Difference between groups was -0.7 for pain intensity (95%CI -0.1--0.3), 5.5 for back muscle strength (95%CI 2.0-9.0) and -0.4 days for use of analgesics (85%CI -0.7-0.2) | 7/10 |
| Mayer et al., 201528 | 96 firefighters | Intervention (n=54): supervised exercise targeting the back and core muscles while on duty in addition to usual physical activity Control (n=42): usual physical activity | 24 weeks | Low back pain, muscle strength and endurance | Muscle strength and resistance were assessed by means of the Biering-Sorensen and plank tests | Group intervention had 12% greater (p=0.021) back muscle endurance and 21% greater (p=0.0006) core muscle endurance compared to the control group | 7/10 |
| Kim et al., 201529 | 53 workers | Intervention (n=27): core muscle strengthening program (CORE) Control (n=26): hot-packs and transcutaneous electrical nerve stimulation | 2 months | Musculoskeletal pain, range of motion and proprioception | Resting and movement-induced pain were assessed on VAS. Pressure pain was assessed with pressure algometer. Active range of pain-free motion was assessed with inclinometer. Proprioception assessment | The intensity of resting (35.6±5.9 mm) and movement-induced (39.4-9.1 mm) pain significantly decreased in group intervention. Significant improvement of the pressure pain threshold (quadratus lumborum: 2.2±0.7 kg/cm2), active range of motion and proprioception (p<0.05) | 5/10 |
| Brandt et al., 201530 | 13 US Airforce helicopter crewmembers | Intervention (n=6): core strengthening exercises Control (n=7): usual exercising regimen | 12 weeks | In-flight low back pain and functional disability | Self-reported pain severity and disability were assessed with Numerical Pain Rating Scale - NPRS and the Modified Oswestry Low Back Pain Disability Index (MODI) | The average score on NPRS significantly decreased in group intervention and increased in the control group (-1.8 vs. +0.1 points). The mean score on MODI significantly decreased in group intervention and increased in the control group (-4.8 vs. +1.7 points) | 4/10 |
| Macedo, 201131 | 50 workers | Intervention (n=29): workplace fitness program with emphasis on stretching, relaxation and ludic activities Control (n=21): did not participate in the fitness program | 8 months | Musculoskeletal pain | Pain topography was assessed with the Nordic Musculoskeletal Questionnaire. Pain intensity was assessed with VAS | Group intervention exhibited significant low back pain improvement (p=0.001) | 5/10 |
The 15 selected articles were subjected to selective analysis, as shown in Chart 1. The following information was considered: first author; publication year; study population; activities performed by the intervention and control groups; total length of intervention; analyzed outcomes; methods for assessment; methods for analysis; results; and score on the PEDro scale. In addition, methodological aspects of articles were analyzed, including intention to treat, blinding, random allocation, group comparison and precision measurements (Chart 2).
Chart 2. Characteristics of articles, Salvador, 2017.
| Author, year | Intention to treat | Blinding | Random allocation | Group comparison | Precision measurements |
|---|---|---|---|---|---|
| Telles et al., 200917 | ● | ● | ● | ||
| Kamioka et al., 201118 | ● | ● | ● | ● | ● |
| Del Pozo-Cruz et al., 201219 | ● | ● | ● | ● | ● |
| Alexandre et al., 200120 | ● | ● | ● | ||
| Pillastrini et al., 200921 | ● | ● | ● | ● | |
| Horneij et al., 200122 | ● | ● | ● | ● | |
| Anema et al., 200723 | ● | ● | ● | ● | ● |
| Ewert et al., 200924 | ● | ● | ● | ● | ● |
| Nassif et al., 201125 | ● | ● | ● | ● | |
| Elfering et al., 201326 | ● | ● | ● | ||
| Jakobsen et al., 201527 | ● | ● | ● | ● | ● |
| Mayer et al., 201528 | ● | ● | ● | ● | ● |
| Kim et al., 201529 | ● | ● | ● | ● | |
| Brandt et al., 201530 | ● | ● | ● | ||
| Macedo, 201131 | ● | ● | ● |
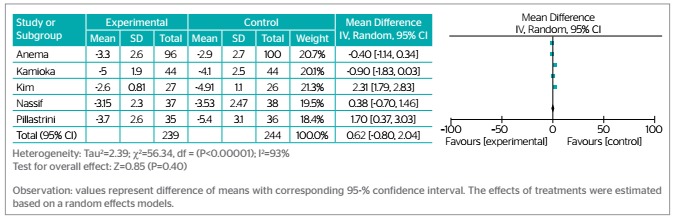
Meta-analysis of outcome measures: based on the characteristics of studies and outcome measures, the results of 5 studies were combined (n=483) in the meta-analysis. Effects were summarized as difference of means and corresponding 95%CI by means of a random effects model. The combined results indicated that the perceived pain intensity did not differ between the groups (difference of means=0.62, 95%CI -0.80-2.04, p<0.4) (Figure 2).
Figure 2. Workplace intervention involving physical exercise vs. controls, Salvador, 2017.
Although funding was not considered as a source of bias, only Kim et al. (2015)29 and Brandt et al. (2015)30 reported their studies had no external funding. Pillastrini et al. (2009)21 and Mayer et al. (2015)28 did not make any mention of funding or potential conflict of interest.
DISCUSSION
The main interventions for treatment of low back pain described in the analyzed studies were strength and flexibility exercises and relaxation techniques, while interventions consisting of physical exercises alone were not common.
Despite the acknowledged effect of physical exercise to improve physical fitness aspects, such as muscle strength and flexibility, physical exercise programs or other modalities of physical activity at the workplace are not legally compulsory in Brazil. The Brazilian legislation defines parameters to adjust the working conditions to the psychophysiological characteristics of workers. For this purpose, it establishes minimum comfort requirements at the workplace, in addition to paid breaks during working hours.
We should observe that the results of physical activity programs at the workplace go much beyond effects on the musculoskeletal system. A study that followed up Canadian workers enrolled in a physical activity program along 12 years detected discrete benefits for the participants physical condition, but substantial gains in terms of productivity and reduction of absenteeism, which thus represent an instance of the Hawthorne effect.
In their study with 162 professional computer users enrolled in a yoga program along eight weeks and a control group, Telles et al.17 found greater musculoskeletal discomfort among the latter. The authors attributed this finding mainly to the fact that the control group had been deprived of any physical activity. The results further evidenced that workers’ health care also involves professional recognition and inclusion of workers in social activities. In Kamioka et al.’s18 randomized controlled trial, the tested stretching exercises program was not able to reduce the incidence of low back pain nor to promote improvement of the grip strength. However, the small sample size might have caused a type II error.
Also other aspects, such as the cost-effectiveness of intervention, should be taken into consideration. Upon analyzing the cost-effectiveness of physical exercise combined with ergonomic orientation, Lindstrom-Hazel32 concluded that this type of intervention is attractive from the economic point of view. Del Pozo-Cruz et al.19 prescribed a web-based exercise program to office workers in Spain and found that intervention could reduce the social cost of low back pain by €500.00 per episode. In addition, they found that one and the same intervention might be more or less effective as a function of the methods of prescription of physical exercise and how orientation is given to workers.
In turn, different modalities of physical exercise combined with educational measures might be equally efficacious, as was found in the study by George et al.33, in which soldiers were subjected to specific exercises for low back pain prevention. This study was not included in the present review due to the specificity of the study population, namely, young soldiers, whereby the results might not be necessarily generalizable to the overall population. For the same reason, we neither included the study by Suni et al.34 with young conscripts, which evidenced the benefits of orientation on posture and strengthening exercises specifically targeting the low back muscles.
In regard to the frequency of training, two weekly sessions seem efficacious to reduce the occurrence of low back pain episodes, as was found by Alexandre et al.20. In the study by Pillastrini et al.21, nursery school teachers were allocated to groups by means of cluster randomization, being blinded to the intervention received by the other group. The results showed that two weekly sessions at 2-day intervals along three weeks were effective to reduce low back pain and improve the participants’ physical capacity. These effects persisted along the full follow-up period, which shows that the modality, rather than the duration of intervention and number of sessions seems to be the main aspect to be considered in the implantation of physical exercise programs at the workplace. Muscle strengthening and stretching exercises at the workplace are feasible and efficacious. In addition, also orientation on posture and information on the etiology and pathogenesis of low back pain are recommended preventive measures.
The studies were assessed according to quality criteria: intention to treat, blinding, random allocation, group comparison and precision measurements. All the studies compared groups and the results before and after intervention between the intervention and control groups. Four (26.7%) out the 15 studies included in the present review scored 4/10 on the PEDro scale and five studies (33.3%) scored 5/10. The length of intervention varied from three weeks to 18 months. The low methodological quality of most studies and the wide variation of intervention might represent a considerable methodological limitation to the search for evidence.
In the studies that performed intention-to-treat analysis, subjects were followed up by the investigators independently from the fate of each one18,19,23,24,27,28. From the five studies selected for clustered measurement analysis, only two performed intention-to-treat analysis, which partially explains the high heterogeneity found (I2=93%). Blinding was reported in most studies18,19,21,22,23,24,25,26,27,28,29.
In regard to the limitations of the present systematic review, some derive from the fact that the literature search was performed on one single database, and that only electronic search was conducted, which might be a restricted approach to the treatment of low back pain. Then, we did not assess all the outcomes we originally intended. Our intention was to analyze outcome absenteeism, however, we did not include it in the assessment, which configures a protocol deviation. Finally, we did not perform sensitivity analysis. The high heterogeneity found (I2=93%) was attributed to intrinsic methodological differences among interventions and to the sociodemographic profile of the populations of workers who participated in the studies.
CONCLUSIONS
Functional incapacity related to low back pain at the workplace impairs productivity and is a cause of absenteeism. Physical exercise at the workplace stands out among the measures for prevention of this occupational condition. However, the results of the present systematic review with meta-analysis did not show that physical exercise at the workplace is efficacious to reduce the occurrence of low back pain. Additional systematic reviews with multiple comparisons of randomized controlled trials are needed to assess the various interventions performed at the workplace to reduce the occurrence of low back pain.
Footnotes
Funding: none
REFERENCES
- 1.Dionne CE, Dunn KM, Croft PR, Nachemson AL, Buchbinder R, Walker BF, et al. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine (Phila Pa 1976) 2008;33:95–103. doi: 10.1097/BRS.0b013e31815e7f94. [DOI] [PubMed] [Google Scholar]
- 2.Goubert L, Crombez G, De Bourdeaudhuij I. Low back pain, disability and back pain myths in a community sample: prevalence and interrelationships. Eur J Pain. 2004;8:385–394. doi: 10.1016/j.ejpain.2003.11.004. [DOI] [PubMed] [Google Scholar]
- 3.Nascimento PRC do, Costa LOP. Prevalência da dor lombar no Brasil: uma revisão sistemática. Cad Saúde Pública. 2015;31(6):1141–1156. doi: 10.1590/0102-311X00046114. [DOI] [PubMed] [Google Scholar]
- 4.Andrusaitis SF, Oliveira RP, Barros TEP., Filho Study of the prevalence and risk factors for low back pain in truck drivers in the state of São Paulo, Brazil. Clinics. 2006;61:503–510. doi: 10.1590/S1807-59322006000600003. [DOI] [PubMed] [Google Scholar]
- 5.Célia RCRS, Alexandre NMC. Distúrbios osteomusculares e qualidade de vida em trabalhadores envolvidos com transporte de pacientes. Rev Bras Enferm. 2003;56:494–498. doi: 10.1590/S0034-71672003000500005. [DOI] [PubMed] [Google Scholar]
- 6.Kreling MC, da Cruz DA, Pimenta CA. Prevalência de dor crônica em adultos. Rev Bras Enferm. 2006;59:509–513. doi: 10.1590/S0034-71672006000400007. [DOI] [PubMed] [Google Scholar]
- 7.Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between obesity and low back pain: a meta-analysis. Am J Epidemiol. 2010;171:135–154. doi: 10.1093/aje/kwp356. [DOI] [PubMed] [Google Scholar]
- 8.Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64:2028–2037. doi: 10.1002/art.34347. [DOI] [PubMed] [Google Scholar]
- 9.Majchrzycki M, Kocur P, Kotwicki T. Deep tissue massage and nonsteroidal anti-inflammatory drugs for low back pain: a prospective randomized trial. Scientific World J. 2014 Feb 23;2014:287597–287597. doi: 10.1155/2014/287597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hayden JA, van Tulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non-specific low back pain. Cochrane Database Syst Rev. 2005;(3):CD000335–CD000335. doi: 10.1002/14651858.CD000335.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Serra MVGB, lC Pimenta, Quemelo PRV. Efeitos da ginástica laboral na saúde do trabalhador: uma revisão da literatura. Rev Pesq Fisioterapia. 2014;4 [Google Scholar]
- 12.Maciel RH, Albuquerque AMFC, Melzer AC, Leônidas SR. Quem se beneficia dos programas de ginástica laboral? Cad Psicol Soc Trab. 2005;8:71–86. doi: 10.11606/issn.1981-0490.v8i0p71-86. [DOI] [Google Scholar]
- 13.Brian A, Casazza MD. Diagnosis and Treatment of Acute Low Back Pain. Am Fam Physician. 2012 Feb 15;85(4):343–350. [PubMed] [Google Scholar]
- 14.Bottamedi X, Ramos JS, Arins MR, Murara N, Woellner SS, Soares AV. Programa de tratamento para dor lombar crônica baseado nos princípios da Estabilização Segmentar e na Escola de Coluna. Rev Bras Med Trab. 2016;14(3):206–213. doi: 10.5327/Z1679-443520164815. [DOI] [Google Scholar]
- 15.Dishman RK, Oldenburg B, O'Neal H, Shephard RJ. Worksite physical activity interventions. Am J Prev Med. 1998 Nov;15(4):344–361. doi: 10.1016/s0749-3797(98)00077-4. [DOI] [PubMed] [Google Scholar]
- 16.Haynes RB, McKibbon KA, Wilczynski NL, Walter SD, Werre SR. Optimal search strategies for retrieving scientifically strong studies of treatment from Medline: analytical survey. BMJ. 2005 May 13; doi: 10.1136/bmj.38446.498542.8F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Telles S, Dash M, Naveen KV. Effect of yoga on musculoskeletal discomfort and motor functions in professional computer users. Work. 2009;33(3):297–306. doi: 10.3233/WOR-2009-0877. [DOI] [PubMed] [Google Scholar]
- 18.Kamioka H, Okuizumi H, Okada S, Takahashi R, Handa S, Kitayuguchi J, et al. Effectiveness of intervention for low back pain in female caregivers in nursing homes: a pilot trial based on multicenter randomization. Environ Health Prev Med. 2011 Mar;16(2):97–105. doi: 10.1007/s12199-010-0170-1. https://dx.doi.org/10.1007%2Fs12199-010-0170-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Del Pozo-Cruz B, Adsuar JC, Parraca J, Del Pozo-Cruz J, Moreno A, Gusi N. A web-based intervention to improve and prevent low back pain among office workers: a randomized controlled trial. J Orthop Sports Phys Ther. 2012 Oct;42(10):831–841. doi: 10.2519/jospt.2012.3980. [DOI] [PubMed] [Google Scholar]
- 20.Alexandre NM, de Moraes MA, Corrêa HR, Filho, Jorge SA. Evaluation of a program to reduce back pain in nursing personnel. Rev Saúde Pública. 2001 Aug;35(4):356–361. doi: 10.1590/S0034-89102001000400004. [DOI] [PubMed] [Google Scholar]
- 21.Pillastrini P, Mugnai R, Bertozzi L, Costi S, Curti S, Mattioli S. Effectiveness of an at-work exercise program in the prevention and management of neck and low back complaints in nursery school teachers. Ind Health. 2009 Aug;47(4):349–354. doi: 10.2486/indhealth.47.349. [DOI] [PubMed] [Google Scholar]
- 22.Horneij E, Hemborg B, Jensen I, Ekdahl C. No significant differences between intervention programmes on neck, shoulder and low back pain a prospective randomized study among home-care personnel. J Rehabil Med. 2001 Jul;33(4):170–176. [PubMed] [Google Scholar]
- 23.Anema JR, Steenstra IA, Bongers PM, de Vet HC, Knol DL, Loisel P, et al. Multidisciplinary rehabilitation for subacute low back pain: graded activity or workplace intervention or both? A randomized controlled trial. Spine (Phila Pa 1976) 2007 Feb 01;32(3):291–298. doi: 10.1097/01.brs.0000253604.90039.ad. discussion 299-300. [DOI] [PubMed] [Google Scholar]
- 24.Ewert T, Limm H, Wessels T, Rackwitz B, von Garnier K, Freumuth R, et al. The comparative effectiveness of a multimodal program versus exercise alone for the secondary prevention of chronic low back pain and disability. PM R. 2009 Sep;1(9):798–808. doi: 10.1016/j.pmrj.2009.07.006. [DOI] [PubMed] [Google Scholar]
- 25.Nassif H, Brosset N, Guillaume M, Delore-Milles E, Tafflet M, Buchholz F, et al. Evaluation of a randomized controlled trial in the management of chronic lower back pain in a French automotive industry: an observational study. Arch Phys Med Rehabil. 2011 Dec;92(12):1927–36.e4. doi: 10.1016/j.apmr.2011.06.029. [DOI] [PubMed] [Google Scholar]
- 26.Elfering A, Arnold S, Schade V, Burger C, Radlinger L. Stochastic resonance whole-body vibration, musculoskeletal symptoms, and body balance: a worksite training study. Saf Health Work. 2013 Sep;4(3):149–155. doi: 10.1016/j.shaw.2013.07.002. https://dx.doi.org/10.1016%2Fj.shaw.2013.07.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jakobsen MD, Sundstrup E, Brandt M, Jay K, Aagaard P, Andersen LL. Effect of workplace- versus home-based physical exercise on musculoskeletal pain among healthcare workers: a cluster randomized controlled trial. Scand J Work Environ Health. 2015 Mar;41(2):153–163. doi: 10.5271/sjweh.3479. [DOI] [PubMed] [Google Scholar]
- 28.Mayer JM, Quillen WS, Verna JL, Chen R, Lunseth P, Dagenais S. Impact of a supervised worksite exercise program on back and core muscular endurance in firefighters. Am J Health Promot. 2015 Jan-Feb;29(3):165–172. doi: 10.4278/ajhp.130228-QUAN-89. [DOI] [PubMed] [Google Scholar]
- 29.Kim TH, Kim EH, Cho HY. The effects of the CORE programme on pain at rest, movement-induced and secondary pain, active range of motion, and proprioception in female office workers with chronic low back pain: a randomized controlled trial. Clin Rehabil. 2015 Jul;29(7):653–662. doi: 10.1177/0269215514552075. [DOI] [PubMed] [Google Scholar]
- 30.Brandt Y, Currier L, Plante TW, Schubert Kabban CM, Tvaryanas AP. A Randomized Controlled Trial of Core Strengthening Exercises in Helicopter Crewmembers with Low Back Pain. Aerosp Med Hum Perform. 2015 Oct;86(10):889–894. doi: 10.3357/AMHP.4245.2015. [DOI] [PubMed] [Google Scholar]
- 31.Macedo AC, Trindade CS, Brito AP, Dantas MS. On the Effects of a Workplace Fitness Program upon Pain Perception: a Case Study Encompassing Office Workers in a Portuguese Context. J Occup Rehabil. 2011 Sep;21:228–233. doi: 10.1007/s10926-010-9264-2. [DOI] [PubMed] [Google Scholar]
- 32.Lindstrom-Hazel D. A single-subject design of ergonomic intervention effectiveness for university employees in a new facility. Work. 2008;31(1):83–93. [PubMed] [Google Scholar]
- 33.George SZ, Childs JD, Teyhen DS, Wu SS, Wright AC, Dugan JL, et al. Brief psychosocial education, not core stabilization, reduced incidence of low back pain: results from the Prevention of Low Back Pain in the Military (POLM) cluster randomized trial. BMC Med. 2011;9:128–128. doi: 10.1186/1741-7015-9-128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Suni JH, Taanila H, Mattila VM, Ohrankämmen O, Vuorinen P, Pihlajamäki H, et al. Neuromuscular exercise and counseling decrease absenteeism due to low back pain in young conscripts: a randomized, population-based primary prevention study. Spine (Phila Pa 1976) 2013 Mar 01;38(5):375–384. doi: 10.1097/BRS.0b013e318270a12d. [DOI] [PubMed] [Google Scholar]