

Abstract
Background
After a 1999 National Cancer Institute (NCI) clinical alert was issued, chemoradiotherapy has become widely used in treating women with cervical cancer. Two subsequent systematic reviews found that interpretation of the benefits was complicated and some important clinical questions were unanswered.
Objectives
We initiated a meta‐analysis seeking updated individual patient data (IPD) from all randomised controlled trials (RCTs) to assess the effect of chemoradiotherapy on all outcomes. We pre‐specified analyses to investigate whether the effect of chemoradiotherapy differed by trial or patient characteristics.
Search methods
We supplemented MEDLINE, LILACS and CANCERLIT searches with information from trial registers, by handsearching relevant meeting proceedings and by discussion with relevant trialists and organisations. Searches were updated until October 2009.
Selection criteria
Both published and unpublished trials were eligible for inclusion provided the patients had been randomised between radiotherapy (with or without surgery) versus concomitant chemoradiotherapy (with or without surgery); that the method of randomisation precluded prior knowledge of the treatment to be assigned; and that the trial had completed patient recruitment before the date of the final analyses.
Data collection and analysis
We carried out a quantitative meta‐analysis using updated information from individual patients from all available RCTs. We sought data from all patients randomised in all eligible trials. We obtained updated information on survival, recurrence and date of last follow up. To avoid potential bias, we requested information for all randomised patients, including those who had been excluded from the investigators' original analyses.
Main results
Eighteen trials were identified and 15 of these were eligible for inclusion in the main analysis. On the basis of 13 trials that compared chemoradiotherapy versus the same radiotherapy, there was a 6% improvement in 5‐year survival with chemoradiotherapy (hazard ratio (HR) = 0.81, P < 0.001). A larger survival benefit was seen for the two further trials in which chemotherapy was administered after chemoradiotherapy. There was a significant survival benefit for both the group of trials that used platinum‐based (HR = 0.83, P = 0.017) and non‐platinum based (HR = 0.77, P = 0.009) chemoradiotherapy, but no evidence of a difference in the size of the benefit by radiotherapy or chemotherapy dose or scheduling was seen. Chemoradiotherapy also reduced local and distant recurrence and progression and improved disease‐free survival (DFS). There was a suggestion of a difference in the size of the survival benefit with tumour stage, but not across other patient subgroups. Acute haematological and gastro‐intestinal toxicity were increased with chemoradiotherapy, but data were too sparse for an analysis of late toxicity.
Authors' conclusions
These results endorse the recommendations of the NCI alert, but also demonstrate their applicability to all women and a benefit of non‐platinum based chemoradiotherapy. Furthermore, although these results suggest an additional benefit from adjuvant chemotherapy this requires testing in RCTs.
Keywords: Female, Humans, Antineoplastic Combined Chemotherapy Protocols, Antineoplastic Combined Chemotherapy Protocols/adverse effects, Antineoplastic Combined Chemotherapy Protocols/therapeutic use, Cisplatin, Cisplatin/administration & dosage, Combined Modality Therapy, Combined Modality Therapy/methods, Fluorouracil, Fluorouracil/administration & dosage, Mitomycin, Mitomycin/administration & dosage, Randomized Controlled Trials as Topic, Uterine Cervical Neoplasms, Uterine Cervical Neoplasms/drug therapy, Uterine Cervical Neoplasms/radiotherapy
Plain language summary
Chemoradiotherapy for cervical cancer: results of a meta‐analysis
Women with cervical cancer that is too big to be removed by surgery, or has spread to the tissues around the cervix (often called locally advanced cervical cancer) may be treated with radiotherapy (treatment with x‐rays). They might also get chemotherapy (drug treatment) alongside radiotherapy. This is called chemoradiotherapy (or chemoradiation). This review brought together 18 randomised controlled trials (RCTs) that were carried out in many countries. The results of the review showed that women who had chemoradiotherapy for cervical cancer were likely to live for longer than women who had just radiotherapy. Five years after being treated, 66 out of every 100 women who received chemoradiotherapy were still alive compared with 60 out of every 100 who just had radiotherapy. Women who received chemoradiotherapy were also less likely to have the cancer come back or spread to other parts of the body. Chemoradiotherapy helped all women, even those with bigger tumours, or tumours that had spread more. Also, the different drugs that had been used in the trials (cisplatin, 5‐fluourouracil or mitomycin‐C) all helped women to live longer or stop the cancer from coming back or spreading. Some of the short term side effects were worse for women who received chemoradiotherapy. Doctors can usually help women to cope with the short term side effects of their treatment. Unfortunately, there was not enough information to be certain whether the long‐term side effects are worse with chemoradiotherapy or not.
The review also seemed to show that women who have extra chemotherapy (after they have had chemoradiotherapy) live longer than those who just have chemoradiotherapy. However, the researchers are less certain about these results and suggest that new RCTs are needed to find out whether giving extra chemotherapy is better for women with cervical cancer, or not.
Background
Cervical cancer is the second most common cancer among women worldwide and the main cancer affecting women in sub‐Saharan Africa, Central America and south‐central Asia (Parkin 2002). A significant decline in incidence and mortality have been seen in North America, parts of Europe, Australia and New Zealand, where screening programmes have been implemented for some time (Arbyn 2007; Australian Institute of Health and Welfare 2007; Canadian Cancer Society 2007; Ries 2006).
In 1999, after publication of five trials (Keys 1999; Morris 1999; Peters 2000; Rose 1999a; Rose 1999b; Whitney 1999) the NCI issued an alert (National Cancer Institute 1999) recommending that 'concomitant chemoradiotherapy should be considered instead of radiotherapy alone in women with cervical cancer'. This has lead to a change in the treatment for many women with cervical cancer (Pearcey 2007; Trimble 2007). Two subsequent reviews (Green 2001: Green 2005; Lukka 2002) reported improvements in survival, progression‐free survival (PFS) and recurrence rates with chemoradiotherapy. However, interpretation of the benefits were complicated by the use of different treatments on the control arms of the included studies (Lukka 2002) heterogeneity in trial results and inconsistency in the definition of outcomes between trials (Green 2005). The authors concluded that an individual patient data (IPD) meta‐analysis would be required to obtain time‐to‐event analyses of local and distant recurrence, more reliable estimates of effect in patient subgroups, and a better attribution of relative toxicities.
Objectives
We therefore initiated a systematic review and meta‐analysis that aimed to collect, validate and re‐analyse IPD from all relevant RCTs (Stewart 1995). This permits time‐to‐event analyses and investigation of differences in the effect of chemoradiotherapy by trial or patient characteristics and, by seeking updated follow‐up, provides a unique opportunity to look at these outcomes in the long‐term. This IPD meta‐analysis was initiated and coordinated by the Medical Research Council (UK) Clinical Trials Unit and carried out by the Concomitant chemoradiotherapy in Cervical Cancer Meta‐analysis Collaboration (CCCMAC).
Methods
Criteria for considering studies for this review
Types of studies
The methods for this systematic review and meta‐analysis followed a detailed, pre‐specified protocol (September 2004, a copy of which is available on request). Trials had to be properly randomised and should have completed patient accrual by the time of the final analyses (May 2007).
Types of participants
Women with locally advanced cancer of the uterine cervix who had not received any previous treatments likely to interfere with protocol treatments or comparisons.
Types of interventions
Our inclusion criteria limited the main analysis to trials that compared concomitant chemotherapy and radical radiotherapy (with or without surgery) with the same radical radiotherapy (with or without surgery). However, given the importance of two trials using hydroxyurea on the control arm (Rose 1999a; Rose 1999b; Whitney 1999) and one trial giving extended field radiotherapy on the control arm (Morris 1999) to the NCI alert (National Cancer Institute 1999) and for completeness, we analysed these trials alongside the main comparison to establish how sensitive the effect of chemoradiotherapy is to different trial designs. Chemotherapy should have been given on the experimental arm only. Trials were excluded if they used additional non‐cytotoxic treatments or only non‐cytotoxic radiosensitisers/radioprotectors on the experimental arm. Trials that used hydroxyurea as the sole chemotherapy agent have been considered in a prior systematic review (Symonds 2004a; Symonds 2004b) and have not been included here.
Types of outcome measures
The primary outcome, overall survival (OS), was defined as the time from randomisation until death by any cause. Living patients were censored on the date of last follow‐up. Locoregional progression/recurrence and metastases were supplied as classified in the individual trials. Locoregional disease free survival (DFS) was defined as the time from randomisation until locoregional recurrence or progression or death by any cause. Patients alive with no locoregional disease were censored on the date of last follow‐up. Metastases‐free survival was defined as the time from randomisation until first metastasis or death by any cause. Patients alive without metastases were censored on the date of last follow‐up. In trials where only the first recurrence (either locoregional or distant) was recorded, patients with metastatic disease were censored in the analysis of locoregional recurrence and those with locoregional disease were censored in the analysis of metastases. Overall DFS was defined as the time from randomisation until locoregional recurrence, metastasis or death by any cause. For the exploratory analyses of time to locoregional recurrence and time to metastases, time to locoregional recurrence was defined as the time from randomisation until the first local recurrence or progression. Patients without local recurrence or progression were censored on the date of last follow up or death. Time to metastases was defined as the time from randomisation until first metastases. Patients without metastases were censored on the date of last follow up or death. For trials that only recorded the first recurrence event, the methods of censoring described above were used.
Investigators were asked to supply acute and late toxicity data according to the criteria used in their own trials. Although different scales were used to measure both, each was based on a 5‐grade system where 0 signifies no toxicity and 5 signifies death, making it reasonable to combine the results.
Search methods for identification of studies
To avoid publication bias, published and unpublished trials were included in the meta‐analysis. We searched Medline and CancerLit using an optimal search strategy (Dickersin 1995)(Appendix 1) and also LILACS (Appendix 2), the Physician Data Query (Open and Closed Protocols), and other trial registers. These were supplemented from reference lists of identified trial reports and review articles and meeting proceedings of the International Gynecologic Cancer Society and the Society for Gynecologic Oncology (1994 to )2009). Furthermore, all participating investigators were asked to supplement our provisional list of trials. Searches were regularly updated until October 2009.
The search strategies used have been developed and executed by the author team.
Data collection and analysis
We sought to collect up‐to‐date information for all patients randomised, including those excluded from the investigators’ own analyses, on date of randomisation, treatment allocation, tumour response, locoregional and distant progression/recurrence status, survival, cause of death, and acute and late toxicity. Baseline data on age, histology, FIGO stage, tumour grade, performance status and lymph node involvement were also sought. All data were thoroughly checked for validity, consistency and integrity of randomisation and follow‐up (Stewart 1995). Inconsistencies were resolved and final database entries validated by the responsible trial investigator, data manager or statistician.
All analyses (unless otherwise stated) were pre‐specified in the meta‐analysis protocol (available on request) and were performed on an intention‐to‐treat (ITT) basis. For all survival and recurrence outcomes, individual times to event were used to obtain hazard ratio (HR) estimates of treatment effect for individual trials, which were pooled across trials, using a stratified‐by‐trial, fixed‐effect model (Yusuf 1985). For binary outcomes such as response and toxicity, the number of events and numbers of patients were used to calculate Peto odds ratio (OR) estimates of treatment effect (Yusuf 1985) for individual trials which were pooled across trials, using the stratified‐by‐trial fixed‐effect model (Yusuf 1985). Trial results were also combined using the random effects approach (DerSimonian 1986).
Three 4‐arm trials in the meta‐analysis (Chen 1997a; Chen 1997b; Lorvidhaya 2003a; Lorvidhaya 2003b;Thomas 1998a; Thomas 1998b) used a factorial design to assess the impact of two treatments at once, one of which was chemoradiotherapy. Each was split into two unconfounded comparisons of chemoradiotherapy versus radiotherapy and analysed as though they were separate trials (a) and (b) (Characteristics of included studies). Two three‐arm trials (Lanciano 2005a; Lanciano 2005b; Rose 1999a, Rose 1999b) in the meta‐analysis compared two different forms of chemoradiotherapy with a single control arm. The treatment arms were combined and compared with the control group for analysis for both trials.
To explore the impact of trial characteristics on the effect of chemoradiotherapy, we pre‐specified analyses that grouped trials according to chemotherapy scheduling (chemotherapy entirely during radiotherapy, chemotherapy during and after radiotherapy), chemotherapy type (platinum‐based chemotherapy, non‐platinum based chemotherapy), planned radiotherapy dose (‘optimal’ radiotherapy of greater than or equal to 45Gy external beam plus brachytherapy (any dose), ‘sub‐optimal’ radiotherapy of greater than 45Gy external beam without brachytherapy or less than 45Gy external beam with or without brachytherapy), planned radiotherapy duration (less than or equal to 8 weeks, greater than 8 weeks). For the subset of trials that used cisplatin‐based chemotherapy only, we also planned analyses of chemotherapy cycle length (less than or equal to one week, greater than one week) and chemotherapy dose intensity (less than or equal to 25mg/m2/week cisplatin, greater than 25mg/m2/week cisplatin). Hazard ratios (HRs) were calculated for each trial group and for all trials together. These analyses focused on the primary outcome of OS and were also carried out on the other outcomes to support or refute any patterns found. For 'serious' acute toxicity, defined as grades 3 to 5, trials were grouped according to their use of platinum‐based chemoradiotherapy, non platinum‐based chemoradiotherapy, chemoradiotherapy plus additional chemotherapy, extended field radiotherapy on the control arm and additional hydroxyurea on the control arm, with HRs calculated for each group.
The effects of chemoradiotherapy within subgroups of patients were investigated using similar stratified analyses. HRs were obtained for each pre‐defined subgroup within each trial, for example, a HR for patients with good performance status and a HR for patients with poor performance status. These HRs were then combined to give overall HRs, e.g. for good and poor performance patients. Chi‐square tests for interaction or trend were used to investigate whether there were any substantial differences in the effect of concomitant chemoradiotherapy between different groups of trials or subgroups of patients.
Results are also presented as absolute differences, calculated from the overall HR and the control arm event rate (Parmar 1995). Chi square heterogeneity tests (ABOC 1995) and the I2 statistic (Higgins 2003) were used to assess statistical heterogeneity across trials. Kaplan‐Meier curves are non‐stratified (Kaplan 1958). All P‐values are two‐sided.
Where IPD were not available, wherever possible we calculated HRs and associated statistics from reported time to event analyses (Parmar 1998; Tierney 2007) and considered the impact on the analyses of IPD.
Selection of studies
All titles and abstracts, identified by both electronic searching and by hand searching of conference proceedings, were checked and full publications were obtained for those thought to be potentially relevant. These were assessed independently by two review authors (CV, JT) to reach consensus on their eligibility for inclusion in the review. Individual patient data was sought from trial authors including updated follow‐up, where available.
Assessment of risk of bias in included studies
The methodological quality of included studies was assessed using the risk of bias tool (Table 1) and checked with a second review author. Trials were individually assessed for risk of bias on the basis of adequate sequence generation, allocation concealment, blinding, whether incomplete outcome data was presented or if there was evidence of selective outcome reporting (Characteristics of included studies). Trials considered to be free of substantial biases that might affect the results were included in the meta‐analysis, with any potential sources of bias are clearly highlighted (Risk of bias in included studies).
1. Patient characteristics.
| Subgroup | chemoradiotherapy(1745 Patients) | Control (1707 patients) | Total (3452 Patients) |
| Age <35 35‐50 >50‐65 >65 Unknown Median age Range | 233 (13%) 873 (50%) 538 (31%) 98 (6%) 3(<1%) 47.00 20‐87 | 249 (15%) 775 (45%) 555 (33%) 125 (7%) 3 (<1%) 47.00 20‐91 | 482 1648 1093 223 6 47.00 20‐91 |
|
Histology Squamous cell Adenocarcinoma Adenosquamous Other Unknown |
1541(88%) 87 (5%) 51 (3%) 32 (2%) 34 (2%) | 1531 (89%) 90 (5%) 32 (2%) 17 (1%) 37 (2%) | 3072 177 83 49 71 |
|
Stage 1a‐2a 2b 3‐4a Unknown |
413(24%) 625 (36%) 667 (38%) 40 (2%) | 417 (24%) 601 (35%) 658 (39%) 31 (2%) |
830 1226 1325 71 |
|
Grade
Well differentiated Moderately well differentiated Poorly / undifferentiated Unknown |
157 (9%) 600 (34%) 223 (13%) 765 (44%) | 155 (9%) 594 (35%) 195 (11%) 763 (45%) | 312 1194 418 1528 |
|
Performance status 0 1 2 3‐4 Unknown |
692 (40%) 498 (29%) 29 (2%) 1(0%) 525 (30%) | 655 (38%) 508 (30%) 23 (1%) 0 (0%) 521 (31%) | 1347 1006 52 1 1046 |
|
Pelvic node involvement Involved Not involved Unknown |
191(11%) 535 (31%) 1019 (58%) | 173 (10%) 549 (32%) 985 (58%) | 364 1084 2004 |
|
Para‐aortic node involvement Involved Not involved Unknown |
32 (2%) 823 (47%) 890 (51%) | 21 (1%) 801 (47%) 885 (52%) | 53 1624 1775 |
|
Iliac node involvement Involved Not involved Unknown |
50(3%) 591 (34%) 1104 (63%) | 55 (3%) 591 (35%) 1061 (62%) | 105 1182 2165 |
Results
Description of studies
Main analysis
Trials comparing radiotherapy with concomitant chemotherapy plus the same radiotherapy
We identified 25 randomised trials that were eligible for the main analysis. We were unable to include data from 10 trials (1113 patients), either because data could not be located (6 trials, 814 patients) (Fernandez 1995; Lira‐Puerto 1989; Singh 1985; Tseng 1997; Wong 1989; Wong 1999) or because we were unable to make contact with the relevant investigators (4 trials, 299 patients) (Bulnes 1986; Dawel 1997; Hernandez 1991; Singh 2003). Data were therefore available for 3452 women from 15 trials (Chen 1997a; Chen 1997b; Cikaric 2005; Garipağaoğlu 2004; Kantardzic 2004: Keys 1999; Lal 2004; Lanciano 2005a; Lanciano 2005b; Leborgne 1995: Lorvidhaya 2003a; Lorvidhaya 2003b; Onishi 2000; Pearcey 2002; Peters 2000; Pras 1995; Roberts 2000; Thomas 1998a; Thomas 1998b. This includes 85% of women from trials that used cisplatin‐based chemoradiotherapy and almost 80% of women from trials that used 5FU and / or mitomycin‐C based (66% of all women who took part in trials of non‐platinum based) chemoradiotherapy. Data were obtained for 118 women (100%) who were excluded from the investigators’ original analyses and reinstated in the meta‐analysis. Characteristics of the included trials are shown in Characteristics of included studies.
The 15 available trials accrued 44 to 926 patients between May 1987 and June 2006. Eleven trials used platinum‐based chemoradiotherapy in the experimental arm, either as a single agent (6 trials Cikaric 2005; Garipağaoğlu 2004; Keys 1999; Lal 2004; Onishi 2000, Pearcey 2002) or in combination regimens (5 trials Chen 1997a; Chen 1997b; Kantardzic 2004; Leborgne 1995; Peters 2000; Pras 1995). Three trials (Lorvidhaya 2003a; Lorvidhaya 2003b; Roberts 2000; Thomas 1998a; Thomas 1998b) used non‐platinum regimens comprising either 5FU, mitomycin‐C or a combination of the two. One three‐arm trial randomised patients to receive chemoradiotherapy either with cisplatin or 5FU (Lanciano 2005a; Lanciano 2005b). Each of the trials aimed to prescribe external beam radiation at a dose to the tumour of between 40 ‐ 61.2Gy and all except one trial (Peters 2000) (which used primary hysterectomy) also used brachytherapy. The planned total duration of all radiotherapy (external beam plus brachytherapy) was from 40 to 70 days across all trials. The median follow up for living patients across all 15 trials was 5.2 years. Data on OS, DFS, locoregional DFS and metastases‐free survival were available for all trials, but tumour response was only available in full for two trials (Kantardzic 2004; Pras 1995, preventing an analysis of this outcome.
Patient characteristics for the 15 trials are given in Table 1. Data on age were provided for all trials, data on histology and stage were provided for 14 trials, data on performance status were provided for 12 trials, and data on grade were available for 9 trials. Data on pelvic node involvement and iliac node involvement were available for six trials, with para‐aortic node involvement available for nine trials. On the basis of the available data, women were mostly aged between 35 and 64 years of age, with good performance status. They had tumours that were largely of squamous cell histology (89%), stage 2b (36%) or stage 3 (36%), and moderately differentiated (35%). However, as there was generally no central pathology review, the precise definition of tumour grade may vary from trial to trial. Three trials excluded women with involved para‐aortic nodes (Keys 1999; Lanciano 2005a; Lanciano 2005b; Pras 1995) and para‐aortic nodal status was either uninvolved (48%) or unknown (51%) for the vast majority of the women from the remaining trials.
Risk of bias in included studies
IPD for all included trials was checked for integrity of randomisation. There were no unusual patterns of randomisation noted and patient characteristics were well balanced across the treatment arms for all included trials. All trials reported adequate concealment of allocation, except for one trial (Pras 1995) for which no details were available. The nature of the treatment interventions is such that blinding was not appropriate for any of the trials. IPD were supplied for all outcomes except for acute and late toxicity, largely because these data were not collected or recorded for the individual trials. However, some of the trials that were able to supply late toxicity outcomes had substantial missing data (Chen 1997a; Chen 1997b; Lorvidhaya 2003a; Lorvidhaya 2003b; Onishi 2000; Thomas 1998a; Thomas 1998b) which may lead to bias in any analyses of these outcomes.
Effects of interventions
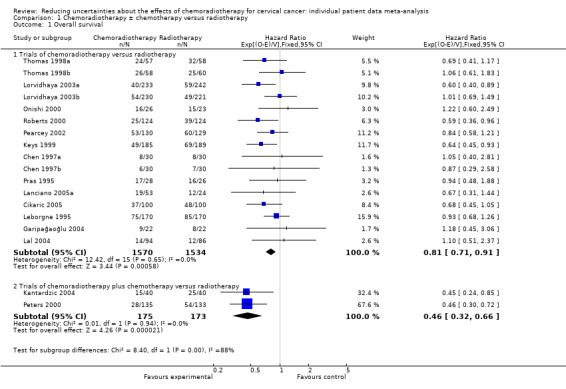
OS data were supplied for 15 trials including 3452 women and 1138 deaths have been recorded (Chen 1997a; Chen 1997b; Cikaric 2005; Garipağaoğlu 2004; Kantardzic 2004; Keys 1999; Lal 2004; Lanciano 2005a; Lanciano 2005b; Leborgne 1995; Lorvidhaya 2003a; Lorvidhaya 2003b; Onishi 2000; Pearcey 2002; Peters 2000; Pras 1995; Roberts 2000; Thomas 1998a; Thomas 1998b). The results for these trials are grouped according to whether chemoradiotherapy only was used or whether additional chemotherapy after chemoradiotherapy was administered (Analysis 1.1). Although there was no evidence of statistical heterogeneity within each trial group (chemoradiotherapy only P = 0.65, I2 = 0.00; chemoradiotherapy plus adjuvant chemotherapy P = 0.95, I2 = 0.00), there was a large and significant difference between groups in the benefit of chemoradiotherapy (interaction P = 0.004). The HR for the two trials that gave chemoradiotherapy plus adjuvant chemotherapy of 0.46 (95% CI 0.32 to 0.66, P < 0.001), represents a 54% reduction in the risk of death with this treatment and translates into an absolute survival benefit of 19% at 5 years (from 60% to 79%) (Kantardzic 2004; Peters 2000 ). However, the most reliable and unconfounded estimate of the effect of chemoradiotherapy alone is obtained from the 13 trials whose design did not include the use of additional chemotherapy (Analysis 2.1). The HR for this group of 0.81 (95% CI 0.71 to 0.91) represents a highly significant (P < 0.001), 19% relative reduction in the risk of death with chemoradiotherapy compared with radiotherapy and translates to an absolute survival benefit of 6% at five years (from 60% to 66%). The survival curves for these 13 trials and for the two trials that used adjuvant chemotherapy follow a similar pattern, although separation of the curves is greater with adjuvant chemotherapy (Figure 1), albeit that follow‐up for one of the trials (Kantardzic 2004) in this group is somewhat less mature (median follow‐up 2.35 years) than for the main group of 13 trials (overall median follow‐up 4.77 years). The results are similar when a random effects model was applied (DerSimonian 1986).
1.1. Analysis.
Comparison 1 Chemoradiotherapy ± chemotherapy versus radiotherapy, Outcome 1 Overall survival.
2.1. Analysis.
Comparison 2 Chemoradiotherapy versus Radiotherapy, Outcome 1 Overall survival.
1.
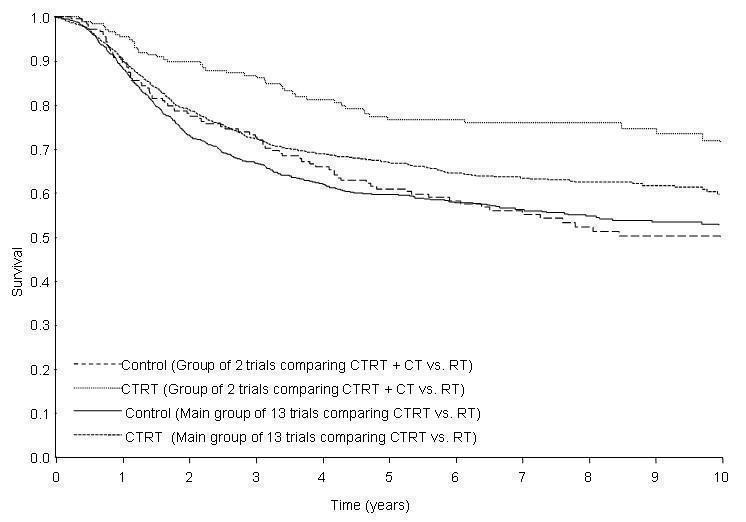
Simple (unstratified ) Kaplan Meier Curves for Overall Survival: chemoradiotherapy versus radiotherapy and chemoradiotherapy plus chemotherapy versus radiotherapy
CTRT ‐ chemoradiotherapy
CT ‐ chemotherapy
RT ‐ radiotherapy
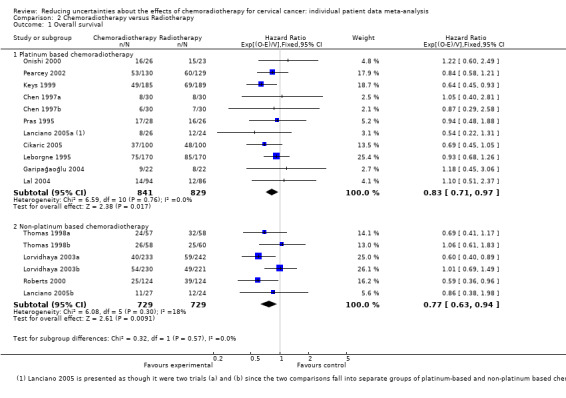
Subsequent pre‐specified analyses by trial group were therefore restricted to the 13 trials that had an unconfounded comparison of chemoradiotherapy versus radiation (Chen 1997a; Chen 1997b; Cikaric 2005; Garipağaoğlu 2004; Keys 1999; Lal 2004; Lanciano 2005a; Lanciano 2005b; Leborgne 1995; Lorvidhaya 2003a; Lorvidhaya 2003b; Onishi 2000; Pearcey 2002; Pras 1995; Roberts 2000; Thomas 1998a; Thomas 1998b). We found no evidence of a difference in the size of the effect of chemoradiotherapy when trials were grouped according to the type of chemotherapy they had used (platinum‐based or non‐platinum‐based) (Analysis 2.1) the planned radiotherapy dose or the total planned duration of radiation (Table 2). Similarly, for the ten trials that used cisplatin‐based chemoradiotherapy (Chen 1997a; Chen 1997b; Cikaric 2005; Garipağaoğlu 2004; Keys 1999; Lal 2004; Lanciano 2005a; Leborgne 1995; Onishi 2000; Pearcey 2002; Pras 1995), we found no evidence that the effect of chemoradiotherapy differed according to the cycle length or the dose intensity of cisplatin used (Table 2). However, the power of these analyses, particularly those involving just the cisplatin‐based chemoradiotherapy trials, is limited.
2. Results of trial group analyses for overall survival (Main group of 13 trials only).
| HR(95%CI) | Interaction p‐value | |
|
Planned Chemotherapy type Platinum based Non‐platinum based |
0.84 (0.72‐0.98) 0.76 (0.62‐0.94) | 0.48 |
|
Planned Radiotherapy dose > 45 Gy + BRT < 45 Gy + BRT |
0.78 (0.68‐0.89) 0.93 (0.70‐1.24) |
0.26 |
|
Planned Radiotherapy duration < 8 weeks > 8 weeks |
0.83 (0.72‐0.96) 0.73 (0.57‐0.93) | 0.35 |
|
Planned chemotherapy cycle length < 1 week > 1 week |
0.74 (0.60‐0.92) 0.95 (0.72‐1.25) |
0.16 |
|
Planned Cisplatin dose intensity < 25mg/m2/week > 25mg/m2/week |
0.93 (0.70‐1.24) 0.76 (0.62‐0.96) | 0.25 |
| Cisplatin regimen Single‐agent Combination | 0.76 (0.62‐0.93) 0.93 (0.70‐1.24) | 0.25 |
|
Chemotherapy regimen Single agent Combination |
0.75 (0.63‐0.88) 0.86 (0.71‐1.04) | 0.29 |
Data on overall DFS, locoregional DFS and metastases free survival were available from all of the 13 trials in the unconfounded comparison of chemoradiotherapy versus radiation. For DFS, there were 1376 events in total, of which 1087 were recurrences or metastases and 289 were deaths (Figure 2). The HR of 0.78 (95% CI 0.70 to 0.87, P < 0.001) translates to an absolute DFS benefit of 8% at 5 years (from 50% to 58%). There were similar and significant absolute benefits of chemoradiotherapy on 5‐year locoregional DFS (9%, P < 0.001), time to locoregional recurrence/progression (6%, P = 0.00009) and metastases‐free survival (7%, P < 0.001). However, there was a smaller and less convincing improvement in time to metastases at 5 years (4%, P = 0.04). Insufficient data were available to assess the impact of chemoradiotherapy on response (Table 3).
2.
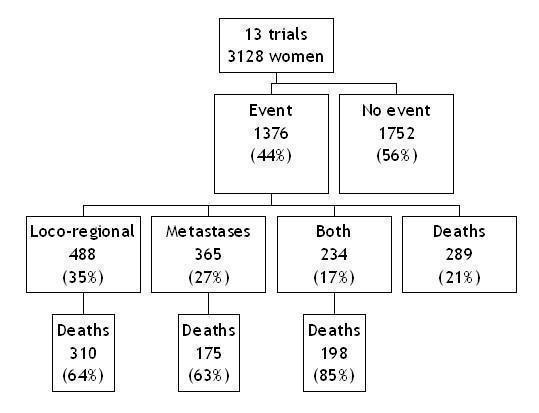
Flow diagram showing deaths and recurrences (Chemoradiotherapy versus radiotherapy trials only)
3. Results of all outcomes (Main group of 13 trials only).
| HR(95%CI) | P‐value |
Absolute benefit (5 years) |
|
| Overall disease‐free survival | 0.78 (0.70‐0.87) | 0.000005 | 8% |
| Locoregional disease‐free survival | 0.76 (0.68‐0.86) | 0.000003 | 9% |
| Metastases‐free survival | 0.81 (0.72‐0.91) | 0.0004 | 7% |
| Locoregional disease‐free interval | 0.74 (0.64‐0.86) | 0.00009 | 6% |
| Metastases‐free interval | 0.83 (0.71‐0.99) | 0.037 | 4% |
Patient subgroup analyses were similarly restricted to those 13 trials in the unconfounded group that were able to supply data. A planned analysis based on iliac node involvement was not completed as there were insufficient data (Table 1). Also, most patients for whom data were supplied had good performance status and either unknown or negative para‐aortic nodal status, so there was little to gain from analyses of these subgroups. We found no evidence to suggest that the effect of chemoradiotherapy differed in groups of women defined by age, histology, tumour grade or whether they had pelvic lymph node involvement , although the analyses by grade and pelvic node involvement were limited to eight and five trials respectively (Table 4). There was a suggestion of trend in the relative effect of chemoradiotherapy by tumour stage (P = 0.017), with the benefit of chemoradiotherapy decreasing with increasing stage. The HRs obtained for each stage translate to 5‐year survival benefits of 10% for women with stages 1b to 2a cervical cancer, 7% for women with stage 2b cervical cancer, and 3% for women with stage 3 to 4a cancer. However, there was no significant trend for the analysis of DFS by stage (test for trend, P = 0.073) (Figure 3).
4. Patient subgroup analyses.
| Patient Subgroup | χ2 | P‐value |
| Age (<35, 35 to 49, 50 to 64, ?65) | 0.61* | 0.436 |
| Stage (1a to 2a, 2b, 3 to 4a) | 5.65* | 0.017 |
| Histology (Squamous, Adenosquamous or adenocarcinoma) | 0.00 | 0.992 |
| Grade (Well / moderately well differentiated, poorly differentiated) | 0.00 | 0.961 |
| Pelvic node involvement (Not involved, Involved) | 0.49 | 0.483 |
*Test for trend (otherwise Test for Interaction)
3.
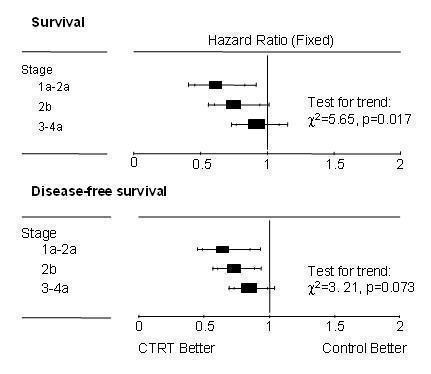
Subgroup analysis for FIGO stage for chemoradiotherapy versus radiotherapy trials only (Overall survival and Disease‐free survival)
For trials for which IPD were not available, it was only possible to estimate HRs for survival (Parmar 1998; Tierney 2007) for three of the 10 trials, two of which contribute to the main group of 13 trials (Hernandez 1991; Tseng 1997) and one to the group of trials that used additional chemotherapy after chemoradiotherapy (Wong 1999). However, incorporating them into the meta‐analysis did not materially change the results for either group (data not shown).
Sensitivity analyses
Trials of different design
Three trials were included in the sensitivity analysis of trials of different designs (Morris 1999; Rose 1999a: Rose 1999b: Whitney 1999). Data were supplied for 1366 women (100%), including 84 women who had been excluded from the investigator’s original analyses and were reinstated in the meta‐analysis. The three trials recruited 388 to 575 women between August 1986 and October 1997. All used platinum‐based chemoradiotherapy; however in one trial, extended field radiotherapy was administered in the control arm (Morris 1999) and in two trials, additional hydroxyurea (HU) was administered in the control arm (Rose 1999a; Rose 1999b; Whitney 1999). The three trials planned to give between 40.8 to 61.2Gy external beam radiation plus brachytherapy. The planned total duration for all radiotherapy (external beam and brachytherapy) was less than 56 days (Morris 1999) and fewer than 70 days (Rose 1999a; Rose 1999b; Whitney 1999). The median follow‐up for living patients across these trials was 8.4 years (see Characteristics of included studies). Patient characteristics in the three trials included in the sensitivity analyses were broadly similar to those in the main analyses, however women with para‐aortic nodal involvement were actively excluded from each trial.
Inclusion of the three trials alongside the 13 trials of the main analysis substantially increased overall heterogeneity (P = 0.12, I2 = 28.28). Moreover, Analysis 3.1 illustrates that the treatment effect observed in trials using HU on control (HR 0.63 95% CI 0.52 to 0.76, P < 0.001) differed to that in the main analysis (test for interaction, P = 0.03), with an absolute survival benefit of 15% (from 45% to 60%) at 5 years. The effect of the trial using extended field radiotherapy on the control arm (HR 0.50 95% CI 0.37 to 0.67, P < 0.001) also differed from that in the main analysis (test for interaction, P = 0.004), with an absolute survival benefit of 21% (from 50% to 71%) at 5 years. Whilst these benefits seem greater, the control group survival for both groups is lower than that for the main group of 13 trials (Figure 4). Because these trials differ from the trials in the main analysis in terms of both trial design and the size of the treatment effect, the best estimate of the effect of chemoradiotherapy over radiotherapy remains that from the unconfounded analysis of 6% at 5 years.
3.1. Analysis.
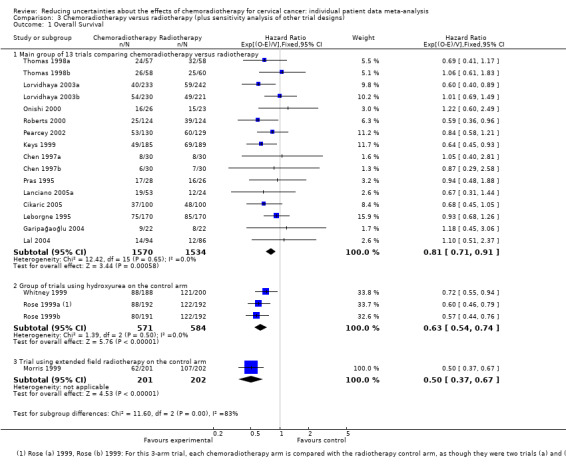
Comparison 3 Chemoradiotherapy versus radiotherapy (plus sensitivity analysis of other trial designs), Outcome 1 Overall Survival.
4.
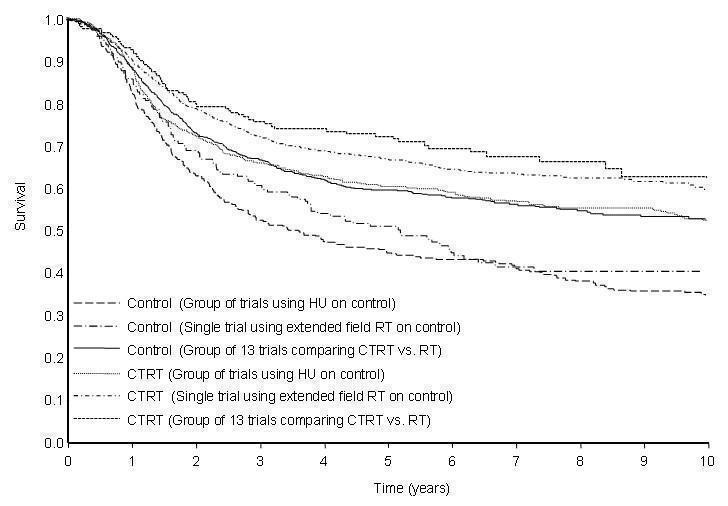
Simple (unstratified) Kaplan Meier Curves for Overall Survival: Chemoradiotherapy versus radiotherapy plus sensitivity analysis of other trial designs
CTRT ‐ chemoradiotherapy; RT ‐ radiotherapy; HU ‐ hydroxyurea
Analyses of toxicity
Data on overall acute haematological toxicity and GI toxicity were supplied for 16 trials. Data were available on white blood cell and genitourinary toxicity for 14 trials, haemoglobin toxicity from 13 trials, platelet toxicity from 12 trials and skin toxicity from 10 trials.
Serious haematological toxicity increased by approximately two‐fold to ten‐fold in individual trials. However, for the group of trials that used HU on the control arm, a high level of serious haematological toxicity was evident on both arms (slightly greater on the control arm, OR 0.74, 95% CI 0.53 to 1.03, P = 0.08). A similar pattern of results was observed for white blood cell toxicity, which accounted for most (92%, 517 events) of the overall haematological toxicity. There was a significant increase in serious GI toxicity for the groups of trials using platinum‐based chemoradiotherapy (P = 0.000002), chemoradiotherapy plus additional chemotherapy (P = 0.001) and additional radiotherapy on the control arm (P = 0.000002). This increase was not observed for the group of trials using non‐platinum based chemoradiotherapy (P = 0.465), where the event rate was low ( approximately 2%) on both arms, or for the trials that gave HU on the control arm (P = 0.591), where the event rate was high (approximately 10%) on both arms. For acute haemoglobin toxicity, acute platelet toxicity, genitourinary toxicity and skin toxicity, very few serious events were recorded and so formal analyses were inappropriate.
Data on late toxicity were not recorded for the majority of trials in the meta‐analysis. Data on late rectal toxicity were available for seven trials, late bladder toxicity for five trials and late intestinal and late vaginal toxicity available for only four trials. Furthermore, within these trials there was substantial missing data for the trials that were able to supply data. Therefore, there was insufficient data available to assess whether serious late toxicity is affected by the type of treatment. The available data suggests that only a small number of women across all trials (1 to 3%) experienced serious late toxicities, including nine deaths, but these data may not represent the true levels of late toxicity across all trials.
Discussion
Our findings are based on the results of 18 trials from 11 countries worldwide, including the 5 studies that formed the basis of the NCI alert in 1999 (National Cancer Institute 1999). Based on the main analysis , there was clear evidence that adding chemotherapy to radiotherapy improves both OS and DFS. For the group of 13 trials in which chemoradiotherapy alone was used, there was a 6% absolute survival benefit and an 8% DFS benefit at 5 years, with no evidence of heterogeneity. These analyses endorse the recommendations made in the 1999 NCI alert (National Cancer Institute 1999) but with far greater reliability and precision regarding the gains of chemoradiotherapy.
The benefit of chemoradiotherapy on OS and DFS was supported by similar benefits on the other outcomes analysed, although the evidence for time to metastases was less compelling. Chemoradiotherapy is thought to exert its major beneficial effects by improving local disease control. However, the benefit of chemoradiotherapy on metastases, suggested previously (Green 2005) and confirmed in this meta‐analysis may indicate that it has a modest systemic effect.
Larger benefits were seen for the trials in which additional chemotherapy was administered following chemoradiotherapy, with an absolute improvement of 19% at 5 years. However this result is based on two relatively small trials of differing design and with less mature follow up and is therefore not conclusive. Inlcusion of published summary data from one unavailable trial does not materially alter the estimate of effect for this group. Furthermore, we cannot be certain that the larger benefit is not due to factors other than the additional chemotherapy following chemoradiotherapy. Nevertheless, the results are promising and may warrant a direct comparison with chemoradiotherapy alone.
Inclusion of trials that used additional treatments on the control arm in previous meta‐analyses led to difficulties in interpretation (Lukka 2002) and significant statistical heterogeneity (Green 2001). Analysing these trials separately facilitates interpretation and minimises heterogeneity. There were larger absolute survival benefits for the group of trials in which HU was administered on the control arm and for the single in which extended field radiotherapy was administered on the control arm. However, these trials all excluded women with surgically identified positive para‐aortic nodes (compared with only two out of 13 trials in the main analysis) and so included women who may have been more likely to benefit from chemoradiotherapy. Furthermore, this highly selected group of women is unlikely to be representative of the general population of women with cervical cancer. Patient selection may also explain why the benefits observed in this meta‐analysis are smaller than had been previously reported (Green 2001; Green 2005; Lukka 2002). These benefits are, however, more likely to be generalisable to more women with cervical cancer.
Importantly, this meta‐analysis shows that the benefit associated with chemoradiotherapy may not depend on the use of platinum. Previous recommendations have been limited to platinum‐based chemoradiotherapy (National Cancer Institute 1999) but this meta‐analysis shows a significant benefit also associated with non‐platinum regimens, specifically those containing 5‐FU and/or mitomycin‐C. However, as our results are not based on a direct comparison, we cannot be clear about the relative merits of platinum versus non‐platinum. The only randomised trial that has directly compared platinum (cisplatin) and non‐platinum‐based (5FU) chemoradiotherapy closed early because interim analyses suggested that 5FU‐based chemoradiotherapy was unlikely to significantly improve PFS compared with cisplatin, even if full accrual had been completed. Furthermore, because it closed early, it was underpowered to detect a difference between the two chemoradiotherapy regimens (Lanciano 2005a; Lanciano 2005b). For women who are unable to tolerate cisplatin, or more easily tolerated chemotherapy is required, non‐cisplatin based chemoradiotherapy perhaps offers an additional option.
Other planned analyses by trial characteristics were hampered, because most trials had planned to give radiotherapy over eight weeks or less in addition to weekly, high dose‐intensity cisplatin‐based chemotherapy, and so should be interpreted cautiously. Nevertheless, we found no evidence to suggest that the effect of chemoradiotherapy differs by any of the trial characteristics investigated. Currently therefore, there is insufficient evidence to suggest that any one treatment type, dose or schedule is better than any other.
The effect of chemoradiotherapy appears consistent across patient subgroups defined by age, histology, grade or pelvic node involvement. There was however the suggestion of a decreasing relative effect of chemoradiotherapy on survival with increasing tumour stage, with estimated absolute survival benefit of 10% (stage 1a to 2a), 7% (stage 2b) and 3% (stage 3 to 4a) at 5 years. Even if this trend had occurred by chance, applying the overall HR (0.81) to each of the stage subgroups gives an improvement in OS at 5 years for all stages, thus confirming chemoradiotherapy benefits women with all stages of cervical cancer, although the size of the benefit may vary.
Although chemoradiotherapy increases some serious acute toxicity, particularly haematological and GI toxicities, few of the trials in this meta‐analysis measured late toxicity and only one of the 25 trials eligible for inclusion in this main analysis reported quality of life (QoL) outcomes (Lira‐Puerto 1989). This highlights the need for prospective evaluations of treatment tolerability and QoL in future trials that investigate the use of new or targeted therapies.
Although this meta‐analysis provides the most comprehensive and up to date summary of the effects of chemoradiotherapy and is based on a large number of women from the large majority of the international trials, IPD from 10 trials were unavailable and might impact on these results. Nine of these trials including 891 randomised patients would contribute to the main analysis. Although HR estimates based on the publications of three unavailable trials suggest that their inclusion would not change the results, and all of the unavailable data would only contribute 20% more data to the main analysis, it is possible that inclusion of IPD from these trials could modify our estimate of treatment effect to some degree. Since the final analyses were completed, we have also become aware of one completed trial that compared weekly cisplatin based chemoradiotherapy with radiotherapy alone in 160 patients (Mitra 2006) and one large ongoing trial of chemoradiotherapy versus radiotherapy (NCT00193791), both from India. Once completed, we will seek inclusion of these recent trials in an updated analysis.
Authors' conclusions
Implications for practice.
This meta‐analysis provides an unconfounded estimate of the effect of chemoradiotherapy compared with radiotherapy. Adding chemotherapy to radiotherapy offers a modest, but significant, additional benefit on all outcomes and for all stages of disease. There is also the potential to use both platinum and non‐platinum regimens. With wider implementation of national screening and vaccination programs it is likely that the incidence of cervical cancer will continue to decrease. However, financial and organisational difficulties, particularly in the developing world, mean that in countries unable to implement such programmes, substantial numbers of women will continue to be affected by cervical cancer. Even access to radiotherapy continues to be a barrier to effective treatment in large parts of the world.
Implications for research.
Effective and affordable treatments, such as those used in this meta‐analysis, provide a standard against which promising new drug regimens or novel treatment approaches should be compared. There is also the potential to investigate whether additional chemotherapy offers additional benefits. Prospective evaluations of the late effects of chemoradiotherapy must be included in future trials that aim to improve treatment tolerability and quality of life with existing regimens, or that investigate the use of new or targeted therapies.
What's new
| Date | Event | Description |
|---|---|---|
| 11 February 2015 | Amended | Contact details updated. |
| 22 April 2013 | Review declared as stable | IPD data review |
Acknowledgements
We are grateful to the UK Medical Research Council for funding this work and to the UK National Coordinating Centre for Research Capacity Development for funding Claire Vale through a post‐doctoral award. We would like to thank all those patients who took part in these trials and contributed to this research. The meta‐analysis would not have been possible without the collaborating institutions that kindly supplied their trial data or without the help of those responsible for maintaining, updating and preparing trial data (David S Alberts, Mark Brady, Slobodan Cikaric, Hongwei Chen, Ketayun Dinshaw, Patricia J Eifel, Melahat Garipagaoglu, Anders Jakobsen, Nermina Kantardzic, Henry Keys, Punita Lal, Rachelle Lanciano, Felix Leborgne, Vicharn Lorvidhaya, Hiroshi Onishi, Mahesh KB Parmar, Robert G Pearcey, Elizabeth Pras, Kenneth Roberts, Peter G Rose, Lesley A Stewart, Jayne F Tierney, Gillian Thomas, Ted Trimble, Claire Vale, Charles W. Whitney). We would also like to thank the Patient Research Partners (Alison Nightingale, Andrea Whelan, Nicolette Spera and Sue Davidson) for their comments and contributions throughout the project. We are also grateful to the Director of Licensing, American Society of Clinical Oncology for granting permission to re‐publish this review, originally published in the Journal of Clinical Oncology (CCCMAC 2008).
Appendices
Appendix 1. Medline search strategy
PT=RANDOMIZED‐CONTROLLED‐TRIAL
RANDOMIZED‐CONTROLLED‐TRIALS.DE.
RANDOM‐ALLOCATION.DE.
DOUBLE‐BLIND‐METHOD.DE.
SINGLE‐BLIND‐METHOD.DE.
1 OR 2 OR 3 OR 4 OR 5
PT=CLINICAL‐TRIAL
CLINICAL‐TRIALS#.DE.
(CLIN$ WITH TRIAL$).AB,TI.
((SINGL$ OR DOUBL$ OR TREBL$ OR TRIPL$) WITH (BLIND$ OR MASK$)).AB,TI.
PLACEBO$.DE.
PLACEBO$.AB,TI.
RANDOM$.AB,TI.
RESEARCH‐DESIGN.DE.
7 OR 8 OR 9 OR 10 OR 11 OR 12 OR 13 OR 14
6 OR 15
CERVICAL ADJ CARCINOMA$.AB,TI.
CERVICAL ADJ CANCER$.AB,TI.
CERVIX ADJ CARCINOMA$.AB,TI.
CERVIX ADJ CANCER$.AB,TI.
(CANCER WITH CERVIX).AB,TI.
(CARCINOMA WITH CERVIX).AB,TI.
CHEMOTHERAPY.AB,TI.
RADIOTHERAPY.AB,TI.
QS Cervix‐Neoplasms# WITH (DT RT)
17 OR 18 OR 19 OR 20 OR 21 OR 22
23 OR 24
16 AND 26 AND 27
16 AND 25
28 OR 29
Appendix 2. LILACS search strategy
(Pt Randomized controlled trial Or Pt controlled clinical trial OR Mh Randomized controlled trials Or Mh random allocation Or Mh double‐blind method Or Mh single‐blind method OR Ex E05.318.760.535$ OR Mh PLACEBOS OR Mh RESEARCH DESIGN) AND NOT (Ct ANIMAL AND NOT (Ct HUMAN and Ct ANIMAL)) OR ((Tw clin$ AND (Tw trial$ OR Tw ensa$ OR Tw estud$ OR Tw experim$ OR Tw investiga$)) or ((Tw random$ OR Tw randon$ OR Tw casual$ OR Tw acaso$ OR Tw azar OR Tw aleator$) and (Tw singl$ OR Tw simple$ OR Tw doubl$ OR Tw doble$ OR Tw duplo$ OR Tw trebl$ OR Tw trip$) and (Tw blind$ OR Tw cego$ OR Tw ciego$ OR Tw mask$ OR Tw mascar$)) OR Tw placebo$ OR (Tw random$ OR Tw randon$ OR Tw casual$ OR Tw acaso$ OR Tw azar OR Tw aleator$)) AND NOT (Pt ENSAIO CONTROLADO ALEATORIO Or Pt ENSAIO CLINICO CONTROLADO OR Pt ENSAIO CLÍNICO OR Mh ENSAIOS CONTROLADOS ALEATORIOS Or Mh DISTRIBUICAO ALEATORIA Or Mh MÉTODO DUPLO‐CEGO Or Mh MÉTODO SIMPLES‐CEGO OR Ex E05.318.760.535$ OR Mh PLACEBOS OR Mh RESEARCH DESIGN) AND NOT (Ct ANIMAL AND NOT (Ct HUMAN and Ct ANIMAL)) OR ((Ct COMPARATIVE STUDY or Ex E05.337$ or Mh FOLLOW‐UP STUDIES or Mh PROSPECTIVE STUDIES or Tw control$ OR Tw prospectiv$ OR Tw volunt$ OR Tw vol‐unteer$) and not (Ct ANIMAL AND NOT (Ct HUMAN and Ct ANIMAL)) and not (Pt ENSAIO CONTROLADO ALEATORIO Or Pt ENSAIO CLINICO CONTROLADO Or Mh ENSAIOS CONTROLADOS ALEATORIOS Or Mh DISTRIBUICAO ALEATORIA Or Mh MÉTODO DUPLO‐CEGO Or Mh MÉTODO SIMPLES‐CEGO) OR ((Pt ENSAIO CLÍNICO or Ex E05.318.760.535$ or (Tw clin$ AND (Tw trial$ OR Tw ensa$ OR Tw estud$ OR Tw experim$ OR Tw investiga$)) OR ((Tw random$ OR Tw randon$ OR Tw casual$ OR Tw acaso$ OR Tw azar OR Tw aleator$) and (Tw singl$ OR Tw simple$ OR Tw doubl$ OR Tw doble$ OR Tw duplo$ OR Tw trebl$ OR Tw trip$) and (Tw blind$ OR Tw cego$ OR Tw ciego$ OR Tw mask$ OR Tw mascar$)) or Mh PLACEBOS or Tw placebo$ or (Tw random$ OR Tw randon$ OR Tw casual$ OR Tw acaso$ OR Tw azar OR Tw aleator$) or Mh RESEARCH DESIGN)) and not ((Pt ENSAIO CONTROLADO ALEATORIO Or Pt ENSAIO CLINICO CONTROLADO Or Mh ENSAIOS CONTROLADOS ALEATORIOS Or Mh DISTRIBUICAO ALEATORIA Or Mh MÉTODO DUPLO‐CEGO Or Mh MÉTODO SIMPLES‐CEGO)) and not (Ct ANIMAL AND NOT (Ct HUMAN and Ct ANIMAL)))
(Mh cervix neoplasms/) or (tw Cerv$ AND (Tw carcinoma$ or Tw cancer$))
(Mh Drug therapy/) or (Tw chemotherapy) or (Tw radiotherapy)
Data and analyses
Comparison 1. Chemoradiotherapy ± chemotherapy versus radiotherapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall survival | 18 | Hazard Ratio (95% CI) | Subtotals only | |
| 1.1 Trials of chemoradiotherapy versus radiotherapy | 16 | 3104 | Hazard Ratio (95% CI) | 0.81 [0.71, 0.91] |
| 1.2 Trials of chemoradiotherapy plus chemotherapy versus radiotherapy | 2 | 348 | Hazard Ratio (95% CI) | 0.46 [0.32, 0.66] |
Comparison 2. Chemoradiotherapy versus Radiotherapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall survival | 17 | Hazard Ratio (95% CI) | Subtotals only | |
| 1.1 Platinum based chemoradiotherapy | 11 | 1670 | Hazard Ratio (95% CI) | 0.83 [0.71, 0.97] |
| 1.2 Non‐platinum based chemoradiotherapy | 6 | 1458 | Hazard Ratio (95% CI) | 0.77 [0.63, 0.94] |
Comparison 3. Chemoradiotherapy versus radiotherapy (plus sensitivity analysis of other trial designs).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall Survival | 20 | Hazard Ratio (95% CI) | Subtotals only | |
| 1.1 Main group of 13 trials comparing chemoradiotherapy versus radiotherapy | 16 | 3104 | Hazard Ratio (95% CI) | 0.81 [0.71, 0.91] |
| 1.2 Group of trials using hydroxyurea on the control arm | 3 | 1155 | Hazard Ratio (95% CI) | 0.63 [0.54, 0.74] |
| 1.3 Trial using extended field radiotherapy on the control arm | 1 | 403 | Hazard Ratio (95% CI) | 0.50 [0.37, 0.67] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Chen 1997a.
| Methods | RCT 1993 to 1994 |
|
| Participants | 60 patients Stage IIB to IIIB |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (Cisplatin) | |
| Outcomes | Survival, disease free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | 4‐arm trial (with Chen B below) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Sealed envelope |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes. NB. Substantial proportion of data missing for late toxicity outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Chen 1997b.
| Methods | RCT 1993 to 1994 |
|
| Participants | 60 patients Stage IIB to IIIB |
|
| Interventions | Radiotherapy plus hypothermia versus concomitant chemoradiotherapy (Cisplatin) plus hypothermia | |
| Outcomes | Survival, disease free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Sealed envelope |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes. NB. Substantial proportion of data missing for late toxicity outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Cikaric 2005.
| Methods | RCT 2002‐2003 |
|
| Participants | 200 patients Stage IIB to IVA |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (Cisplatin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Sealed envelope |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Garipağaoğlu 2004.
| Methods | RCT 1996 to 1997 |
|
| Participants | 44 patients Stage IIB, IIIB |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (Cisplatin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Sealed envelope |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Kantardzic 2004.
| Methods | RCT 1996 to 1999 |
|
| Participants | 80 patients Stage IIB to III |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy plus additional chemotherapy (cisplatin + bleomycin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Central telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Keys 1999.
| Methods | RCT 1993‐1997 |
|
| Participants | 374 patients Stage IB (bulky) |
|
| Interventions | Radiotherapy plus hysterectomy versus concomitant chemoradiotherapy (Cisplatin) plus hysterectomy | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Central telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Lal 2004.
| Methods | RCT 2000‐2006 |
|
| Participants | 180 patients Stage II to IV |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (Cisplatin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | 'List ‐ blinded from the trial coordinator' |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Lanciano 2005a.
| Methods | RCT 1997 to 1998 |
|
| Participants | 50 patients Stage IIB, IIIB, IVA |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (Cisplatin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity | |
| Notes | 3‐arm trial with Lanciano (b) NB Control arm is the same for both trials | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Cental telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Lanciano 2005b.
| Methods | RCT 1997 to 1998 |
|
| Participants | 51 Patients Stage IIB, IIIB, IVA |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (5‐FU) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity | |
| Notes | 3‐arm trial with Lanciano (b) NB Control arm is the same for both trials | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Central telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Leborgne 1995.
| Methods | RCT 1995‐2004 |
|
| Participants | 340 patients Stage IB2 to IVB |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (Cisplatin, 5‐FU) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Sealed envelope |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except acute toxicity and late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except acute toxicity and late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Lorvidhaya 2003a.
| Methods | RCT 1987 to 1994 |
|
| Participants | 475 patients Stage IIB, IIIB, IVA |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (5‐FU, Mitomycin C) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | 4‐arm trial with Lorvidhaya (b) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Sealed envelope |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes. NB. Substantial proportion of data missing for late toxicity outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Lorvidhaya 2003b.
| Methods | RCT 1987 to 1994 |
|
| Participants | 451 patients Stage IIB, IIIB, IVA |
|
| Interventions | Radiotherapy plus adjuvant chemotherapy versus concomitant chemoradiotherapy (5‐FU, Mitomycin C) plus adjuvant chemotherapy | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | 4‐arm trial with Lorvidhaya (b) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Sealed envelope |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes. NB. Substantial proportion of data missing for late toxicity outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Morris 1999.
| Methods | RCT 1990 to 1997 |
|
| Participants | 403 patients Stage IB or IIA (>4cm or positive nodes only ); IIB to IVA |
|
| Interventions | Extended field radiotherapy versus concomitant chemoradiotherapy (Cisplatin, 5‐FU) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | Included in sensitivity analysis only as control arm RT differs to that on treatment arm | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Central telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Onishi 2000.
| Methods | RCT 1988 to 1998 |
|
| Participants | 49 patients Stage IIb to IV |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (cisplatin or carboplatin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Sealed envelope |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes. NB. Substantial proportion of data missing for late toxicity outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Pearcey 2002.
| Methods | RCT 1991 to 1996 |
|
| Participants | 259 patients Stage IB to IIB (> 4cm); III to IVA |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (cisplatin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Central telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Peters 2000.
| Methods | RCT 1991 to 1996 |
|
| Participants | 268 patients Stage IA2 to IIA |
|
| Interventions | Surgery plus radiotherapy versus surgery plus concomitant chemoradiotherapy plus additional chemotherapy | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | 'Assignment given by telephone upon study registration' |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Pras 1995.
| Methods | RCT 1995 to 1999 | |
| Participants | 54 patients Stage IB to IIA (> 4cm); IIB to IVA |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (carboplatin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except acute toxicity and late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except acute toxicity, late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Roberts 2000.
| Methods | RCT 1991 to 2001 | |
| Participants | 248 patients Stage IB2, II to IVa |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (Mitomycin C) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Central telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Rose 1999a.
| Methods | RCT 1992 to 1997 |
|
| Participants | 384 patients Stage IIB to IVA |
|
| Interventions | Radiotherapy plus hydroxyurea versus concomitant chemoradiotherapy (cisplatin) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity | |
| Notes | 3‐arm trial ‐ shares the same control arm as Rose (b) Only included in the sensitivity analysis due to use of additional hydroxyurea on the control arm only |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Central telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Rose 1999b.
| Methods | RCT 1992 to 1997 |
|
| Participants | 383 patients Stage IIB to IVA |
|
| Interventions | Radiotherapy plus hydroxyurea versus concomitant chemoradiotherapy (cisplatin, 5‐FU) plus hydroxyurea | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity | |
| Notes | 3‐arm trial ‐ shares the same control arm as Rose (b) Only included in the sensitivity analysis due to use of additional hydroxyurea on the control arm only |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Allocation concealment (selection bias) | Low risk | Central telephone |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Thomas 1998a.
| Methods | RCT 1987 to 1995 |
|
| Participants | 116 women Stage IB (>5cm) to IVA |
|
| Interventions | Radiotherapy versus concomitant chemoradiotherapy (5‐FU) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | 4‐arm trial with Thomas (b) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes. NB. Substantial proportion of data missing for late toxicity outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Thomas 1998b.
| Methods | RCT 1987 to 1995 |
|
| Participants | 118 women Stage IB (>5cm) to IVA |
|
| Interventions | Hyperfractionated radiotherapy versus concomitant chemotherapy (5‐FU )and hyperfractionated radiotherapy | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence, acute toxicity, late toxicity | |
| Notes | 4‐arm trial with Thomas (a) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes. NB. Substantial proportion of data missing for late toxicity outcomes |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Whitney 1999.
| Methods | RCT 1986 to 1990 |
|
| Participants | 388 patients Stage IIB to IVA |
|
| Interventions | Radiotherapy plus hydroxyurea versus concomitant chemoradiotherapy (cisplatin, 5FU) | |
| Outcomes | Survival, disease‐free survival, local and distant recurrence,acute toxicity | |
| Notes | Only included in the sensitivity analysis due to use of additional hydroxyurea on the control arm only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Data checks on IPD provided suggest adequate sequence generation |
| Blinding (performance bias and detection bias) All outcomes | High risk | Trial was not blinded due to nature of treatment interventions |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | IPD provided for all outcomes except late toxicity |
| Selective reporting (reporting bias) | Low risk | N/A (IPD supplied for all outcomes except late toxicity) |
| Other bias | Low risk | Data checks on IPD provided suggest study is free of follow‐up bias |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bulnes 1986 | Unable to make contact with the relevant investigators. |
| Dawel 1997 | Unable to make contact with the relevant investigators. |
| Fernandez 1995 | Data could not be located. |
| Hernandez 1991 | Unable to make contact with the relevant investigators. |
| Lira‐Puerto 1989 | Data could not be located. |
| Singh 1985 | Data could not be located. |
| Singh 2003 | Unable to make contact with the relevant investigators. |
| Tseng 1997 | Data could not be located. |
| Wong 1989 | Data could not be located. |
| Wong 1999 | Data could not be located. |
Contributions of authors
Concept and design: Claire Vale, Jayne F. Tierney, Lesley A. Stewart. Administrative support: Claire Vale. Provision of study materials or patients: David S. Alberts, Hongwei Chen, Slobodan Cikaric, Patricia J. Eifel, Melahat Garipagaoglu, Henry Keys, Nermina Kantardzic, Punita Lal, Rachelle Lanciano, Felix Leborgne, Vicharn Lorvidhaya, Hiroshi Onishi, Robert G. Pearcey, Elizabeth Pras, Kenneth Roberts, Peter G. Rose, Gillian Thomas, Charles W. Whitney. Collection and assembly of data: Claire Vale. Data analysis and interpretation; Claire Vale, Jayne F. Tierney, Lesley A. Stewart, Mark Brady, Ketayun Dinshaw, Anders Jakobsen, Mahesh KB Parmar, Gillian Thomas, Ted Trimble, David S. Alberts, Hongwei Chen, Slobodan Cikaric, Patricia J Eifel, Melahat Garipagaoglu, Henry Keys, Nermina Kantardzic, Punita Lal, Rachelle Lanciano, Felix Leborgne, Vicharn Lorvidhaya, Hiroshi Onishi, Robert G. Pearcey, Elizabeth Pras, Kenneth Roberts, Peter G. Rose, Charles W. Whitney. Manuscript writing: Claire Vale, Jayne F. Tierney, Lesley A. Stewart, Mark Brady, Ketayun Dinshaw, Anders Jakobsen, Mahesh K.B. Parmar, Gillian Thomas, Ted Trimble. Final approval of manuscript: Claire Vale, Jayne F. Tierney, Lesley A. Stewart, Mark Brady, Ketayun Dinshaw, Anders Jakobsen, Mahesh K.B. Parmar, Gillian Thomas, Ted Trimble, David S. Alberts, Hongwei Chen, Slobodan Cikaric, Patricia J. Eifel, Melahat Garipagaoglu, Henry Keys, Nermina Kantardzic, Punita Lal, Rachelle Lanciano, Felix Leborgne, Vicharn Lorvidhaya, Hiroshi Onishi, Robert G. Pearcey, Elizabeth Pras, Kenneth Roberts, Peter G. Rose, Charles W. Whitney.
Sources of support
Internal sources
UK Medical Research Council, UK.
External sources
No sources of support supplied
Declarations of interest
There were no conflicts of interest declared.
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Chen 1997a {published and unpublished data}
- Chen HW, Jei J, Wei L. A randomized trial of hyperthermo‐radiochemotherapy for uterine cancer. Chinese Journal of Oncology 1997;24:249‐51. [Google Scholar]
Chen 1997b {published and unpublished data}
- Chen HW, Jei J, Wei L. A randomized trial of hyperthermo‐radiochemotherapy for uterine cancer. Chinese Journal of Oncology 1997;24:249‐51. [Google Scholar]
Cikaric 2005 {published and unpublished data}
- Cikaric S, Petrovic‐Stupar S, Marjanov I, Rudan L, Colakovic S, Timasevic A, et al. Radiotherapy versus radiotherapy and chemotherapy of advanced cervical cancer: Regression of tumour, early and late sequalaes, relapses of disease and 3‐years survival (the third phase).. European Journal of Cancer 2005;3 (Suppl):266. [Google Scholar]
Garipağaoğlu 2004 {published and unpublished data}
- Garipağaoğlu M, Kayikcioglu F, Kose MF, Adli M, Gűlkesen KH, Koçak Z, et al. Adding concurrent low dose continuous infusion of cisplatin to radiotherapy in locally advanced cervical carcinoma: A prospective randomized pilot study. British Journal of Cancer 2004;77:581‐7. [DOI] [PubMed] [Google Scholar]
Kantardzic 2004 {published and unpublished data}
- Kantardzic N, Beslija S, Begic D. Comparison of parameters of myelotoxicity in patients treated with concomitant chemotherapy and radiotherapy versus radiotherapy alone. Medicinski Arhiv 2004;58:19‐22. [PubMed] [Google Scholar]
Keys 1999 {published and unpublished data}
- Keys HM, Bundy BN, Stehman FB, Muderspach LI, Chafe WE, Suggs CL, et al. Cisplatin, radiation and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. New England Journal of Medicine 1999;340:1154‐61. [DOI] [PubMed] [Google Scholar]
Lal 2004 {published and unpublished data}
- Saibish Kumar E, Lal P, Tiwari A, Kumar S, Dimri K, Rastogi N, et al. Chemo‐irradiation versus radiotherapy alone in locally advanced carcinoma of the uterine cervix: An onging phase III trial. Presented at the 23rd Annual Meeting of the European Society for Therapeutic Radiology and Oncology, Amsterdam, the Netherlands. October 24‐28. 2004; Vol. Abstract 673.
Lanciano 2005a {published and unpublished data}
- Lanciano RM, Calkins A, Bundy BN, Parham G, Lucci JA, Moore DH, et al. Randomized comparison of weekly cisplatin or protracted venous infusion of fluouracil in combination with pelvic radiation in advanced cervical cancer: A Gynecological Oncology Group study. Journal of Clinical Oncology 2005;23:8289‐95. [DOI] [PubMed] [Google Scholar]
Lanciano 2005b {published and unpublished data}
- Lanciano RM, Calkins A, Bundy BN, Parham G, Lucci JA, Moore DH, et al. Randomized comparison of weekly cisplatin or protracted venous infusion of fluouracil in combination with pelvic radiation in advanced cervical cancer: A Gynecological Oncology Group study. Journal of Clinical Oncology 2005;23:8289‐95. [DOI] [PubMed] [Google Scholar]
Leborgne 1995 {unpublished data only}
- Leborgne F. Unpublished.
Lorvidhaya 2003a {published and unpublished data}
- Lorvidhaya V, Chitapanaraux I, Sangruchi S, Lertsanguansinchai P, Kongthanarat Y, Tangkaratt S, et al. Concurrent mitomycin, 5‐fluourouracil and radiotherapy in the treatment of locally advanced carcinoma of the cervix: A randomized trial. International Journal of Radiation Oncology Biology and Physics 2003;55:1226‐32. [DOI] [PubMed] [Google Scholar]
Lorvidhaya 2003b {published and unpublished data}
- Lorvidhaya V, Chitapanaraux I, Sangruchi S, Lertsanguansinchai P, Kongthanarat Y, Tangkaratt S, et al. Concurrent mitomycin, 5‐fluourouracil and radiotherapy in the treatment of locally advanced carcinoma of the cervix: A randomized trial. International Journal of Radiation Oncology Biology and Physics 2003;55:1226‐32. [DOI] [PubMed] [Google Scholar]
Morris 1999 {published and unpublished data}
- Eifel PJ, Winter K, Morris M, Levenback C, Grigsby PW, Cooper J, et al. Pelvic irradiation with concurrent chemotherapy versus pelvic and para‐aortic irradiation for high‐risk cervical cancer: An update of Radiation Oncology Group Trial (RTOG) 90‐01. Journal of Clinical Oncology 2004;22:872‐80. [DOI] [PubMed] [Google Scholar]
- Morris M, Eifel PJ, Lu J, Grigsby PW, Levenbach C, Stevens RE, et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and para‐aortic radiation for high‐risk cervical cancer. New England Journal of Medicine 1999;340:1137‐43. [DOI] [PubMed] [Google Scholar]
Onishi 2000 {published and unpublished data}
- Onishi H, Yagamushi M, Kuriyama K, Tsukamoto T, Ishigame K, Ichikawa T, et al. Effet of concurrent intra‐arterial infusion of platinum drugs for patients with stage III of IV uterine cervical cacner treated with radiotherapy. Cancer Journal of Scientific American 2000;6:40‐5. [PubMed] [Google Scholar]
Pearcey 2002 {published and unpublished data}
- Pearcey R, Brundage M, Drouin P, Jeffrey J, Johnston D, Lukka H, et al. Phase III trial comparing radical radiotherapy with and without cisplatin chemotherapy in patients with advanced squamous cell cancer of the cervix. Journal of Clinical Oncology 2002;20:966‐72. [DOI] [PubMed] [Google Scholar]
Peters 2000 {published and unpublished data}
- Peters WA III, Lui PY, Barrett RJ, Stock RJ, Monk BJ, Berek JS, et al. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high risk early stage cancer of the cervix. Journal of clinical oncology 2000;18:1606‐13. [DOI] [PubMed] [Google Scholar]
Pras 1995 {unpublished data only}
- Pras E. Unpublished.
Roberts 2000 {published and unpublished data}
- Roberts KB, Urdaneta N, Vera R, Vera A, Gutierrez E, Aguilar Y, et al. Interim results of a randomized trial of mitomycin C as an adjunct to radical radiotherapy in the treatment of locally advanced squamous cell carcinoma of the cervix. International Journal of Cancer 2000;90:206‐23. [DOI] [PubMed] [Google Scholar]
Rose 1999a {published and unpublished data}
- Rose PG, Bundy BN, Watkins EB, Thigpen T, Deppe G, Maiman MA, et al. Concurent cisplatin‐based radiotherapy and chemotherapy for locally advanced cervical cancer. New England Journal of Medicine 1999;340:1144‐53. [DOI] [PubMed] [Google Scholar]
Rose 1999b {published and unpublished data}
- Rose PG, Bundy BN, Watkins EB, Thigpen T, Deppe G, Maiman MA, et al. Concurent cisplatin‐based radiotherapy and chemotherapy for locally advanced cervical cancer. New England Journal of Medicine 1999;340:1144‐53. [DOI] [PubMed] [Google Scholar]
Thomas 1998a {published and unpublished data}
- Thomas G, Dembo A, Ackerman I, Franssen E, Balogh J, Fyles A, et al. A randomized trial of standard versus partially hyperfractionated radiation with or without concurrent 5‐fluourouracil in locally advanced cervical cancer. Gynecologic Oncology 1998;69:137‐45. [DOI] [PubMed] [Google Scholar]
Thomas 1998b {published and unpublished data}
- Thomas G, Dembo A, Ackerman I, Franssen E, Balogh J, Fyles A, et al. A randomized trial of standard versus partially hyperfractionated radiation with or without concurrent 5‐fluourouracil in locally advanced cervical cancer. Gynecologic Oncology 1998;69:137‐45. [DOI] [PubMed] [Google Scholar]
Whitney 1999 {published and unpublished data}
- Whitney CW, Sause W, Bundy BN, Malfetano JH, Hannigan EV, Fowler WC, et al. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea in stage IIB/IVA carcinoma of the cervix. Journal of Clinical Oncology 1999;17:1339‐48. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Bulnes 1986 {published data only}
- Bulnes R, Rivera R. Carcinoma of the uterine cervix: treatment with combined radiotherapy and chemotherapy [Carcinoma Epidermoide del cervix uterino: Tratamiento con radiotherapia y quimioterapia asociadas]. Prensa Medica Argentina 1986;73(3):100‐3. [Google Scholar]
Dawel 1997 {published data only}
- Dawel M, Brock A, Prager W, Pohlmann S, Schiller S. Simulatenous chemoradiotherapy with carboplatin in inoperable cervical cancer ‐ Results of a study [Simultane Radiochemotherapie mit Carboplatin beim inoperablen Zervixkarzinom ‐ Ergebinisse einer Studie]. Strahlentherapie Und Onkologie 1997;173(11):545. [Google Scholar]
Fernandez 1995 {published data only}
- Fernandez DJ, Vidyasagar MS, Rao KK, Shenoy A, Kasturi DP. Synchronous 5‐fluorouracil, mitomycin‐c and radiation therapy in the treatment of locally advanced carcimoma od the cervix. Proceedings of the 16th Annual Meeting of the Association of Radiation Oncologists of India 1995;Kerala:97‐103. [Google Scholar]
Hernandez 1991 {published data only}
- Hernandez JRA, Rafael de la Huerta S, Canfield FM, Orozco AF. Clinical stage III cervical cancer: treatment with combined chemotherapy and radiotherapy [Cáncer cervicouterino. Etapa clínica III. Tratamiento combinado de radioterapia quimioterapia.]. Ginecología y Obstetricia De Mexico 1991;59:238‐42. [PubMed] [Google Scholar]
Lira‐Puerto 1989 {published data only}
- Lira‐Puerto R, Huerta R, Cortes H, Fernandez A, Silva A, Martinez R, et al. Cisplatin (CDDP) plus radiotherapy (RT) versus radiotherapy alone in locally advanced cervical cancer. Proceedings of the American Society of Clinical Oncology 1990;9:A633. [Google Scholar]
Singh 1985 {published data only}
- Singh P, Dharmalingham SK, Tan MK, Tan CK. Chemotherapy ‐ radiotherapy combination in the treatment of carcinoma of the cervix. Southeast Asian Journal of Tropical Medicine and Public Health 1985;16(4):665‐8. [PubMed] [Google Scholar]
Singh 2003 {published data only}
- Singh TT, Singh IY, Sharma DT, Singh N. Role of chemoradiation in advanced cervical cancer. Indian Journal of Cancer 2003;40(3):101‐7. [PubMed] [Google Scholar]
Tseng 1997 {published data only}
- Tseng C‐J, Chang C‐T, Lai C‐H, Soong Y‐K, Hong J‐H, Tang SG, et al. A randomized trial of concurrent chemoradiotherapy versus radiotherapy in advanced carcinoma of the cervix. Gynecologic Oncology 1997;66:52‐8. [DOI] [PubMed] [Google Scholar]
Wong 1989 {published data only}
- Wong LC, Choo YS, Choy D, Sham JST, Ma HK. Long‐term follow‐up of potentiation of radiotherapy by cis‐platinum in advanced cervical cancer. Gynecologic Oncology 1989;35:159‐63. [DOI] [PubMed] [Google Scholar]
Wong 1999 {published data only}
- Wong LC, Ngan ANY, Cheung ANY, Cheng DKL, Ng TY, Choy DTK. Chemoradiation and adjuvant chemotherapy in cervical cancer. Journal of Clinical Oncology 1999;17(7):2055‐60. [DOI] [PubMed] [Google Scholar]
Additional references
ABOC 1995
- Advanced Bladder Cancer Overview Collaboration. Does neo‐adjuvant cisplatin‐based chemotherapy improve the survival of patients with locally advanced bladder cancer: a meta‐analysis of individual patient data from randomised clinical trials. British Journal of Urology 1995;75:206‐13. [DOI] [PubMed] [Google Scholar]
Arbyn 2007
- Arbyn M, Raifu AO, Autier P, Ferlay J. Burden of cervical cancer in Europe: estimates for 2004. Annals of Oncology 2007;doi:10:1093/annonc/mdm079. [DOI] [PubMed] [Google Scholar]
Australian Institute of Health and Welfare 2007
- Australian Institute of Health and Welfare. Cervical Screening in Australia 2004‐2005. Cancer Series No. 38. Cat no. CAN 33.(Canberra: AIHW).
Canadian Cancer Society 2007
- Canadian Cancer Society / National Cancer Institute of Canada. Canadian Cancer Statistics 2007; Vol. Toronto, Canada.
DerSimonian 1986
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7:177‐88. [DOI] [PubMed] [Google Scholar]
Dickersin 1995
- Dickersin K, Scherer R, Lefebvre C. Identifying relevant studies for systematic reviews. In: Chalmers I, Altman DG editor(s). Systematic Reviews. London: BMJ Publishing Group, 1995:17‐36. [DOI] [PMC free article] [PubMed] [Google Scholar]
Green 2001
- Green JA, Kirwan JM, Tierney JF, Symonds P, Fresco L, Collingwood M, et al. Survival and recurrence after concomitant chemotherapy and radiotherapy for cancer of the uterine cervix: a systematic review and meta‐analysis. Lancet 2001;358:781‐6. [DOI] [PubMed] [Google Scholar]
Green 2005
- Green J, Kirwan J, Tierney J, Vale CL, Symonds PR, Fresco LL, et al. Concomitant chemotherapy and radiation therapy for cancer of the uterine cervix. Cochrane Database of Systematic Reviews 2005, Issue (Issue 3):CD002225.pub2. [DOI: 10.1002/14651858.CD002225.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kaplan 1958
- Kaplan EL, Meier P. Nonparametric estimation from incomplete observation. Journal of the American Statistical Association 1958;53:457‐81. [Google Scholar]
Lukka 2002
- Lukka H, Hirte H, Fyles A, Thomas G, Elit L, Johnston M, et al. Concurrent cisplatin‐based chemotherapy plus radiotherapy for cervical cancer ‐ a meta‐analysis. Clinical Oncology 2002;14:203‐12. [DOI] [PubMed] [Google Scholar]
Mitra 2006
- Mitra D, Ghosh B, Kar A, Basu S, Deb AR, Sur PK. Role of chemoradiotherapy in advanced carcinoma cervix. Journal of the Indian Medical Association 2006;104(8):432,434,436. [PubMed] [Google Scholar]
National Cancer Institute 1999
- National Cancer Institute. NCI Issues Clinical Announcement on Cervical Cancer: Chemotherapy plus Radiation Improves Survival. [Web page] Available at http://www.nih.gov/news/pr/feb99/nci22.htm 1999.
Parkin 2002
- Parkin DM, Bray F, Ferlay J, Pisani Paola. Global cancer statistics, 2002. CA‐ Cancer J Clinicians 2005;55:74‐108. [DOI] [PubMed] [Google Scholar]
Parmar 1995
- Parmar MKB, Machin D. Survival Analysis: A Practical Approach. Chichester: John Wiley and Sons Ltd, 1995. [Google Scholar]
Parmar 1998
- Parmar MKB, Torri V, Stewart L. Extracting summary statistics to perform meta‐analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17:2815‐34. [DOI] [PubMed] [Google Scholar]
Pearcey 2007
- Pearcey R, Miao Q, Kong W, Zhang‐Salomens J, MacKillop WJ. Impact of adoption of Chemoradiotherapy on the outcome of cervical cancer in Ontario: Results of a population based cohort study. Journal of Clinical Oncology 2007;25(17):2383‐8. [DOI] [PubMed] [Google Scholar]
Ries 2006
- Ries LAG, Harkins D, Krapcho M, et al. SEER Cancer Statistics Review, 1975‐2003. National Cancer Institute, Bethseda, MD.Based on November 2005 SEER data submission,(posted to the SEER website, 2006).
Stewart 1995
- Stewart LA, Clarke MJ, on behalf of the Cochrane Working Party Group on Meta‐analysis using Individual Patient Data. Practical methodology of meta‐analyses (overviews) using updated individual patient data. Statistics in Medicine 1995;14:2057‐79. [DOI] [PubMed] [Google Scholar]
Symonds 2004a
- Symonds RP, Kirwan J, Williams CJ, Tierney JF, Green J, Collingwood M. Concomitant hydroxurea plus radiotherapy versus radiotherapy for carcinoma of the uterine cervix: a systematic review. Cochrane Database of Systematic Reviews 2004, Issue 1:CD003918. [DOI] [PMC free article] [PubMed] [Google Scholar]
Symonds 2004b
- Symonds RP, Collingwood M, Kirwan J, Humber CE, Tierney JF, Green JA, et al. Concomitant hydroxyurea plus radiotherapy versus radiotherapy for carcinoma of the uterine cervix: a systematic review. Cancer Treatment Reviews 2004;30:405‐14. [DOI] [PubMed] [Google Scholar]
Tierney 2007
- Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time‐to‐event data into meta‐analysis. Trials 2007;8(1):16. [DOI] [PMC free article] [PubMed] [Google Scholar]
Trimble 2007
- Trimble E, Gius D, Harlan LC. Impact of NCI announcement upon use of chemoradiation for women with cervical cancer. Journal of Clinical Oncology 2007;25(18S):5537. [Google Scholar]
Yusuf 1985
- Yusuf S, Peto R, Lewis JA, Collins R, Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Progress in Cardiovascular Diseases 1985;27:335‐71. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
CCCMAC 2008
- Chemoradiotherapy for cervical cancer meta‐analysis collaboration. Reducing Uncertainties about the effects of chemoradiotherapy for cervical cancer: a systematic review and meta‐analysis of individual patient data from 18 randomised trials. Journal of Clinical Oncology 2008;26:5802‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]