

Abstract
The virology, immunology, diagnosis, clinical symptoms, treatment, epidemiology and prevention measures relating to the most common viral causes of acute gastroenteritis (rotaviruses, human caliciviruses, astroviruses and enteric adenoviruses) are briefly reviewed. Uncommon viral causes of acute gastroenteritis and viruses causing gastroenteritis in immunodeficient patients are mentioned. The main change over the past three years has been the development, licensing and wide application of new live attenuated rotavirus vaccines.
Keywords: acute gastroenteritis, astrovirus, enteric adenovirus, human calicivirus, norovirus, rotavirus, rotavirus vaccine, sapovirus
Acute gastroenteritis and vomiting are easily recognized as a clinical entity, but may be caused by very different agents (viruses, bacteria, parasites), or may have a non-infectious cause.
Table 1 lists viruses found in the human gut that have been recognized as:
-
•
common causes of diarrhoea and vomiting in humans
-
•
uncommon causes or not a cause of diarrhoea and vomiting in humans
-
•
causes of diarrhoea in immunodeficient individuals.
Table 1.
Viruses infecting the human gut
| Common causes of diarrhoea and vomitinga |
|
| Uncommon causes of diarrhoea and vomiting or asymptomatic infection |
|
| Causes of diarrhoea in immunodeficient individualsc |
|
Viruses other than those that commonly cause diarrhoea are seen sporadically; on average, viruses represent about one-third of all microbial causes of childhood diarrhoea.
Figures in parentheses are detection ranges in various surveys.
Most common cause of outbreaks.
In addition to common causes of diarrhoea and vomiting.
This contribution discusses the major groups of viruses that commonly cause gastroenteritis in humans.
The viruses
Rotaviruses,1 caliciviruses,2 astroviruses3 and enteric adenoviruses4 are the principal virus groups involved. Their size, particle and genome structure, classification and epidemiological significance are summarized in Table 2 . Their appearance by electron microscopy is shown in Figure 1 .
Table 2.
Characteristics of viruses that commonly cause gastroenteritis in humans
| Virus (family) | Size and structure | Genome composition | Classification | Epidemiology |
|---|---|---|---|---|
| Rotaviruses (Reoviridae) |
75 nm, triple-layered, wheel-shaped |
11 segments of dsRNA totalling 18.5 kb |
Groups A–G Within group A subgroups, G and P types |
Endemic in children, winter outbreaks in temperate climates, small epidemics in the elderly |
| Caliciviruses (Caliciviridae) |
About 30 nm, surface cup-shaped |
ssRNA, 7.7 kb | Two genera Noroviruses Sapoviruses |
Epidemics in all age groups |
| Enteric adenoviruses (Adenoviridae) |
About 70 nm, icosahedral |
dsDNA, 36 kb | Group F serotypes 40, 41 | Endemic in children |
| Astroviruses (Astroviridae) |
About 30 nm, star-like appearance | ssRNA, 6.8 kb | Eight serotypes/genotypes | Epidemics in children and adults |
Figure 1.
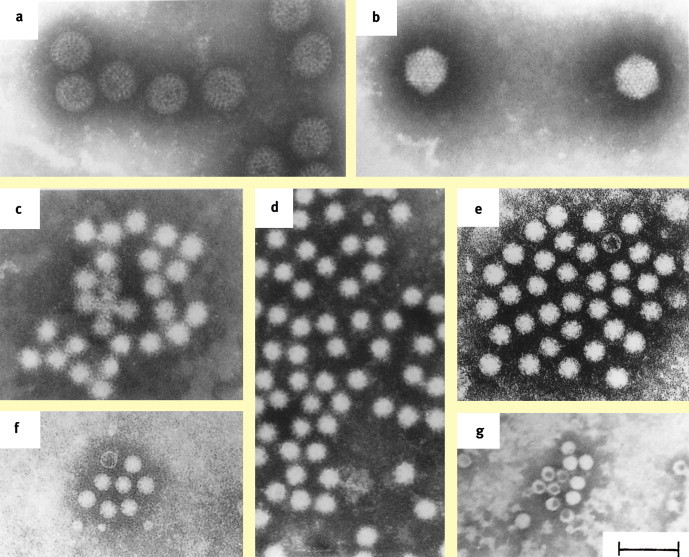
Electron micrographs showing. a rotavirus. b enteric adenovirus. c Norwalk-like virus. d calicivirus. e astrovirus. f enterovirus. g parvovirus. (Negative staining with 3% phosphotungstate, pH 6.3; bar 100 nm). (By courtesy Dr J Gray (a–d, f, g) and Dr J Kurtz (e)).Source: Zuckerman A, Banatvala J, Pattison J, eds. Principles and practice of clinical virology. 4th edn. Chichester: Wiley, 2000 © John Wiley & Sons Limited. Reproduced with permission.)
Rotaviruses
These are the major cause of infantile gastroenteritis worldwide.
Structure – rotaviruses comprise an inner core containing a genome of eleven segments of double-stranded RNA and the transcription/replication complex, a middle layer (inner capsid) consisting of viral protein 6 (VP6), and an outer layer made of VP7 and VP4, the latter protruding as spikes.1
Classification – rotaviruses are a genus of the Reoviridae family and are routinely classified according to the immunological reactivities and genomic sequences of three of their structural components. Cross-reactivities of VP6 distinguish at least seven groups (A–G). Most human infections are caused by group A rotaviruses, which have been divided into several subgroups. The surface proteins VP4 and VP7 elicit type-specific neutralizing antibodies. Accordingly, for group A rotaviruses, a dual-type classification system has been established, differentiating G types (VP7-specific, G derived from glycoprotein) and P types (VP4-specific, P derived from protease-sensitive protein); 16 G types and 27 P types have been described, of which at least 11 G types and 11 P types have so far been found in humans. Because G and P proteins are encoded by different RNA segments, and rotaviruses of group A are found to reassort readily in doubly infected cells, various combinations of G and P types have been observed in natural human rotavirus isolates.5 Recently, a comprehensive classification system involving genotyping of all 11 RNA segments has been proposed.6
Replication and pathogenesis – rotaviruses replicate in mature epithelial cells at the tips of the villi of the small intestine. After virus replication, mature particles are released from cells by lysis. Rotavirus replication is rapid and reaches high titres (up to 1011 virus particles/ml faeces at the peak of acute diarrhoea) within a short period of time. The diarrhoea arises from epithelial necrosis and atrophy, leading to reduced absorption of carbohydrates and increased osmotic pressure in the gut lumen. Cells emerging from the crypts of the gut epithelium, which exhibit reactive hyperplasia, repair the damage to villous cells. This is accompanied by increased secretion of fluid, which also contributes to the diarrhoea. A viral non-structural protein (NSP4, encoded by RNA segment 10) was shown to be an enterotoxin (the first viral protein) identified to exert this function.7 Furthermore, a toxic effect of rotavirus infection on the autonomous nervous system of the gut has been described.8
Immune response – primary rotavirus infection leads to a serotype-specific humoral immune response with initially monotypic protection. During the first two years of life, children are repeatedly infected with rotaviruses of various types, resulting in a more complex immune response that seems to provide partial heterotypic protection.9 Rotavirus-specific secretory copro-antibodies of the IgA subclass have been identified as the best correlate of protection.10
Caliciviruses
Noroviruses (previously termed ‘Norwalk-like viruses’) and sapoviruses (previously termed ‘Sapporo-like viruses’) are two genera of the Caliciviridae family. They are classified into two or possibly three genogroups containing 16 genotypes. Noroviruses of different genotypes co-circulate but genotype II-4 predominates worldwide. Recombination among norovirus strains has been observed and may be more common than initially anticipated. Genetic and antigenic diversity arise through the accumulation of point mutations and the selection of variants through evolutionary pressure likely to be exerted by short-term herd immunity.
These viruses were first recognized as a cause of human gastroenteritis outbreaks in the 1960s and are now considered the most important cause of non-bacterial gastroenteritis outbreaks and epidemics worldwide. In the UK, calicivirus outbreaks are common in hospital settings, old people's homes, etc. Human infection with caliciviruses elicits virus-specific immune responses, though these do not seem to provide full protection from subsequent infections.2
Astroviruses
Astroviruses are members of the Astroviridae family and have a characteristic appearance by electron microscopy (Figure 1). Eight different serotypes/genotypes have been distinguished; serotype 1 is most common. Little is known about immunity conveyed after astrovirus infection or the relative cross-protective effect of the immune response on re-infection with heterotypic strains.3
Adenoviruses
Enteric adenoviruses of subgroup F (serotypes 40 and 41) of the Adenoviridae are a less common cause of diarrhoea in infants and small children. They replicate in the cell nucleus and cytoplasm. Some adenovirus proteins inhibit apoptosis and others decrease host cell metabolism, including expression of MHC class I antigens on the surface of infected cells, thereby reducing susceptibility to adenovirus-specific cytotoxic T cells. A serotype-specific humoral immune response provides homotypic protection.4
Epidemiology
Rotaviruses
Infections occur endemically worldwide, causing over 600,000 deaths each year in children under five years, mainly in low-income countries of sub-Saharan Africa and South East Asia.11 The epidemiology of these infections is complex. There is a strict winter peak in temperate climates, but in tropical and subtropical regions infections occur throughout the year. Transmission is mainly by the faeco-oral route. Nosocomial infections on infant and paediatric wards are difficult to eliminate.
Group A rotaviruses of different G and P types co-circulate in different populations within a geographical location, varying over time. Types G1, G2, G3, G4 and G9 represent more than 90% of co-circulating strains in temperate climates, but other G types (e.g. G5, G8, G10) are increasing and may even become most prevalent, particularly in tropical and subtropical areas.12, 13
The young of many mammalian species harbour diverse rotaviruses and may act as reservoirs for human infections. Most human infections are caused by group A rotaviruses; however, group B rotaviruses were established as the cause of acute gastroenteritis outbreaks in children and adults in China in the 1980s, and recently in Calcutta, India and in other South East Asian countries. Group C rotavirus infections are associated with isolated cases and small outbreaks of diarrhoea in humans.1
Noroviruses
Norovirus infections exhibit a winter peak, and the associated clinical picture has become known as ‘winter vomiting disease’. Age-related seroprevalence surveys have shown that many infections with noroviruses occur in the young and are often inapparent. About 50% of children have been infected by the age of two years. It is now accepted that the incidence of infection with noroviruses and sapoviruses is largely underestimated. Noroviruses cause outbreaks of acute gastroenteritis, some resulting from the ingestion of contaminated food (oysters, green salad) or water, although person-to-person spread is the predominant mode of transmission. Such outbreaks occur in both children and adults in recreational camps, hospitals, nursing homes, schools and on cruise ships.14
Astroviruses
These cause both endemic infections and food-borne outbreaks. Seroprevalence surveys have shown that individuals can become infected by more than one serotype.
Clinical features
Onset of acute viral gastroenteritis is after an incubation period of 1–2 days, with watery diarrhoea lasting 4–7 days, vomiting and varying dehydration. Fever is not common. As a rule, the duration of diarrhoea after infection with norovirus is shorter than after infection with rotaviruses or enteric adenoviruses. Infection may be accompanied by abdominal cramps, headache, myalgia and projectile vomiting, which are regarded as typical of norovirus infection. After rotavirus infection, all degrees of severity of clinical symptoms are seen. The outcome depends on viral pathogenicity factors and host immune status. Inapparent infections can occur, particularly in neonates. Although rotavirus infection is often accompanied by respiratory symptoms, there is no strong evidence that rotaviruses replicate in the respiratory tract. Extra-intestinal spread of rotaviruses has been reported and may result in viraemia or, rarely, encephalopathy.
Chronic gut infections with rotaviruses, adenoviruses, noroviruses, sapoviruses and astroviruses have been seen in immunocompromised children. Chronic gut infections with human cytomegalovirus, adenoviruses of new serotypes (types 42–47) and picobirnaviruses have been reported in HIV-infected patients with AIDS-defining illnesses.
Diagnosis
Diagnosis of rotavirus, astrovirus and enteric adenovirus infections is relatively easy because large numbers of particles are produced and shed during the acute phase of the illness. Noroviruses and sapoviruses are replicated to lower concentrations and for shorter periods. Diagnosis is by electron microscopy of negatively stained specimen suspensions (‘catch-all method’), by passive particle agglutination tests, by virus-specific enzyme-linked immunosorbent assay, and more recently by viral genome detection using polymerase chain reaction (PCR) analysis for adenoviruses and reverse transcription (RT)-PCR for rotaviruses, caliciviruses and astroviruses.
Management
Treatment is mainly by oral rehydration or, in more severe cases, intravenous rehydration. In tropical areas where rotavirus infections are associated with high mortality, standard formulas of oral rehydration fluid are recommended by the WHO and widely used. Otherwise, treatment is symptomatic. Use of antimotility drugs is not advised in children, although there have been recent promising developments in the use of drugs which have antisecretory activity. There are no specific antiviral chemotherapeutic agents in clinical use.15, 16
Outbreaks of nosocomial rotavirus infections are common in children on hospital wards and in day-care centres. Outbreaks of diarrhoea and vomiting caused by noroviruses occur in children and adults following banquets, on cruise ships, and in cafeterias, schools, hotels and fast-food restaurants. Outbreak control measures focus on interruption of person-to-person transmission and removal of sources of infection (food, water, food-handlers), with measures to improve environmental hygiene.
Vaccine development
Development of vaccines against viral gastroenteritis has been principally directed towards rotaviruses, which are the main cause of gastroenteritis and high mortality in developing countries.17, 18
A live attenuated, rhesus rotavirus-based human reassortant vaccine eliciting immunity to human rotavirus strains G1–G4 was found to protect significantly against severe disease, including dehydration. It received US Food and Drug Administration approval for universal use in the USA in August 1998, and 1.5 million doses were used between September 1998 and July 1999. However, a Vaccine Adverse Events Reporting System found gut intussusception to be a rare complication epidemiologically correlated with vaccination, particularly on days 3–7 after the first vaccination. The pathogenesis of this association is not clear. Although the vaccine-attributable risk of intussusception was considered very low in recent studies (<1/10,000), the recommendation for use of this vaccine in the USA was withdrawn in October 1999, and it was taken off the market by the manufacturer.
In the search for alternative vaccines, two further, live attenuated oral rotavirus vaccines have been developed. The underlying concepts of the vaccines are different. The pentavalent vaccine (RotaTeqRTM), containing the human antigens G1–G4 and P[8] in mono-reassortant viruses on a bovine rotavirus (WC3 strain) genetic backbone, is aimed at eliciting type-specific antibodies against all the rotavirus types that are recognized to circulate most frequently. The monovalent vaccine (RotarixRTM), an attenuated human G1P[8] strain, is based on two clinical observations. First, cross-protection is accumulated through successive natural infections, and rotavirus disease can be prevented by repeated natural infection.9 Second, vaccination with one rotavirus type can provide protection, even if subsequent infections are caused by rotaviruses of a different type. Both vaccines have been found to be effective and safe.19, 20 They have recently been licensed in numerous countries, and in some of them universal mass vaccination of children as part of childhood vaccination schemes has been started.21 In the USA initial results are very promising 22 with a distinct decline in clinic visits and hospital admissions for rotavirus disease. There will be intense post-marketing surveillance in order to determine the impact of the vaccine and also to monitor whether or not novel rotavirus strains may emerge. Clinical trials with the new vaccines are ongoing in developing countries where they are most needed in order to determine the impact on rotavirus disease-associated mortality.
More attention is also focused on the use of virus-like particles obtained from baculovirus recombinant-expressed rotavirus proteins, enhancement of rotavirus immunogenicity by micro-encapsidation, DNA-based candidate vaccines, and possibly ‘edible vaccines’.
No vaccines against other viruses causing gastroenteritis in humans have been developed so far. For human caliciviruses, in particular noroviruses, vaccine development will be challenging, as long-term immunity does not usually seem to follow natural infection. A vaccine candidate specific for norovirus genotype II-4 seems to be most promising as its targeted use in healthcare settings would reduce hospital-acquired infection.
References
- 1.Estes M.K., Kapikian A.Z. Rotaviruses. In: Knipe D.M., Howley P.M., editors. Fields virology. 5th edn. Lippincott, Williams & Wilkins; Philadelphia: 2007. pp. 1917–1974. [Google Scholar]
- 2.Green K.Y. Caliciviridae: the noroviruses. In: Knipe D.M., Howley P.M., editors. Fields virology. 5th edn. Lippincott, Williams and Wilkins; Philadelphia: 2007. pp. 949–979. [Google Scholar]
- 3.Mendez E., Arias C.F. Astroviruses. In: Knipe D.M., Howley P.M., editors. Fields virology. 5th edn. Lippincott, Williams and Wilkins; Philadelphia: 2007. pp. 981–1000. [Google Scholar]
- 4.Berk A. Adenoviridae: the viruses and their replication. In: Knipe D.M., Howley P.M., editors. Fields virology. 5th edn. Lippincott, Williams & Wilkins; Philadelphia: 2007. pp. 2355–2394. [Google Scholar]
- 5.Iturriza-Gómara M., Isherwood B., Desselberger U., Gray J. Reassortment in vivo: driving force for diversity of human rotavirus strains isolated in the United Kingdom between 1995 and 1999. J Virol. 2001;75:3696–3705. doi: 10.1128/JVI.75.8.3696-3705.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Matthijnssens J., Ciarlet M., Rahman M. Recommendations for the classification of group A rotaviruses using all 11 genomic RNA segments. Arch Virol. 2008;153:1621–1629. doi: 10.1007/s00705-008-0155-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ball J.M., Tian P., Zeng C.Q.Y. Age dependent diarrhea induced by a rotaviral nonstructural glycoprotein. Science. 1996;272:101–104. doi: 10.1126/science.272.5258.101. [DOI] [PubMed] [Google Scholar]
- 8.Lundgren O., Peregrin A.T., Persson K., Kordasti S., Uhnoo I., Svensson L. Role of the enteric nervous system in the fluid and electrolyte secretion of rotavirus diarrhea. Science. 2000;287:409–411. doi: 10.1126/science.287.5452.491. [DOI] [PubMed] [Google Scholar]
- 9.Velazquez F.R., Matson D.O., Calva J.J. Rotavirus infection in infants as protection against subsequent infection. N Engl J Med. 1996;355:1022–1028. doi: 10.1056/NEJM199610033351404. [DOI] [PubMed] [Google Scholar]
- 10.Franco M.A., Angel J., Greenberg H.B. Immunity and correlates of protection for rotavirus vaccines. Vaccine. 2006;24:2718–2731. doi: 10.1016/j.vaccine.2005.12.048. [DOI] [PubMed] [Google Scholar]
- 11.Parashar U.D., Gibson C.J., Bresse J.S., Glass R.I. Rotavirus and severe childhood diarrhea. Emerg Infect Dis. 2006;12:304–306. doi: 10.3201/eid1202.050006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Desselberger U., Iturriza-Gómara M., Gray J. Rotavirus epidemiology and surveillance. Novartis Found Symp. 2001;238:125–147. doi: 10.1002/0470846534.ch9. [DOI] [PubMed] [Google Scholar]
- 13.Santos N., Hoshino Y. Global distribution of rotavirus serotypes/genotypes and its implication for the development and implementation of an effective rotavirus vaccine. Rev Med Virol. 2005;15:29–56. doi: 10.1002/rmv.448. [DOI] [PubMed] [Google Scholar]
- 14.Koopmans M., van Strien E., Vennema H. Molecular epidemiology of human caliciviruses. In: Desselberger U., Gray J., editors. Viral gastroenteritis. Elsevier Science; Amsterdam: 2003. pp. 523–554. [Google Scholar]
- 15.Desselberger U. Rotavirus infections: guidelines for treatment and prevention. Drugs. 1999;58:447–452. doi: 10.2165/00003495-199958030-00005. [DOI] [PubMed] [Google Scholar]
- 16.Bass D. Treatment of viral gastroenteritis. In: Desselberger U., Gray J., editors. Viral gastroenteritis. Series perspectives in medical virology. Elsevier Science; Amsterdam: 2003. pp. 93–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Angel J., Franco M.A., Greenberg H.B. Rotavirus vaccines: recent developments and future considerations. Nat Rev. 2007;5:529–539. doi: 10.1038/nrmicro1692. [DOI] [PubMed] [Google Scholar]
- 18.Glass R.I., Parashar U.D., Bresee J.S. Rotavirus vaccines: current prospects and future challenges. Lancet. 2006;368:323–332. doi: 10.1016/S0140-6736(06)68815-6. [DOI] [PubMed] [Google Scholar]
- 19.Ruiz-Palacios G.M., Perez-Schael I., Velazquez F.R., Human Rotavirus Vaccine Study Group Safety and efficacy of an attenuated vaccine against severe rotavirus gastroenteritis. N Engl J Med. 2006;354:11–22. doi: 10.1056/NEJMoa052434. [DOI] [PubMed] [Google Scholar]
- 20.Vesikari T., Matson D.O., Dennehy P., Rotavirus Efficacy and Safety Trial (REST) Study Team Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N Engl J Med. 2006;354:23–33. doi: 10.1056/NEJMoa052664. [DOI] [PubMed] [Google Scholar]
- 21.Parashar U.D., Alexander J.P., Glass R.I., Advisory Committee on Immunization Practices (ACIP), Centers for Disease Control and Prevention (CDC) Prevention of rotavirus gastroenteritis among infants and children. Recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2006;55:1–13. [RR-12] [PubMed] [Google Scholar]
- 22.Centers for Disease Control and Prevention (CDC) Delayed onset and diminished magnitude of rotavirus activity–United States, November 2007–May 2008. MMWR Morb Mortal Wkly Rep. 2008;57:697–700. [PubMed] [Google Scholar]
Further reading
- 23.Amar C.F., East C.L., Gray J., Iturriza-Gómara M., Maclure E.A., McLauchlin J. Detection by PCR of eight groups of enteric pathogens in 4,627 faecal samples: re-examination of the English case-control Infectious Intestinal Disease Study (1993–1996) Eur J Clin Microbiol Infect Dis. 2007;26:311–323. doi: 10.1007/s10096-007-0290-8. [DOI] [PubMed] [Google Scholar]
- 24.Blutt S.E., Kirkwood C.D., Parreno V. Rotavirus antigenaemia and viraemia: a common event? Lancet. 2003;362:1445–1449. doi: 10.1016/S0140-6736(03)14687-9. [DOI] [PubMed] [Google Scholar]
- 25.Burke B., Desselberger U. Rotavirus pathogenicity. Virology. 1996;218:299–305. doi: 10.1006/viro.1996.0198. [DOI] [PubMed] [Google Scholar]
- 26.Desselberger U., Wolleswinkel-van den Bosch J., Mrukowicz J., Rodrigo C., Giaquinto C., Vesikari T. Rotavirus types in Europe and their significance for vaccination. Pediatr Infect Dis J. 2006;25:S30–S41. doi: 10.1097/01.inf.0000197707.70835.f3. [DOI] [PubMed] [Google Scholar]
- 27.Dormitzer P.R. Rotaviruses. In: Mandell G.L., Bennett J.E., Dolin R., editors. Principles and practice of infectious diseases. 6th edn. Elsevier; Philadelphia: 2005. pp. 1902–1913. [Google Scholar]
- 28.Gallimore C.I., Iturriza-Gómara M., Xerry J., Adigwe J., Gray J.J. Inter-seasonal diversity of norovirus genotypes: emergence and selection of virus variants. Arch Virol. 2007;152:1295–1303. doi: 10.1007/s00705-007-0954-9. [DOI] [PubMed] [Google Scholar]
- 29.Gray J.J., Jiang X., Morgan-Capner P. Prevalence of antibodies to Norwalk virus in England: detection by enzyme-linked immunosorbent assay using baculovirus-expressed Norwalk virus capsid antigen. J Clin Microbiol. 1993;31:1022–1025. doi: 10.1128/jcm.31.4.1022-1025.1993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Grohmann G.S., Glass R.I., Pereira H.G. Enteric viruses and diarrhea in HIV-infected patients. N Engl J Med. 1993;329:14–20. doi: 10.1056/NEJM199307013290103. [DOI] [PubMed] [Google Scholar]
- 32.Iturriza-Gómara M., Desselberger U., Gray J. Molecular epidemiology of rotaviruses: genetic mechanisms associated with diversity. In: Desselberger U., Gray J., editors. Viral gastroenteritis. Elsevier Science; Amsterdam: 2003. pp. 317–344. [Google Scholar]
- 33.Iturriza-Gómara M., Wong C., Blome C., Desselberger U., Gray J. Molecular characterisation of VP6 genes of human rotavirus isolates: correlation of genogroups with subgroups and evidence of independent segregation. J Virol. 2002;76:6596–6601. doi: 10.1128/JVI.76.13.6596-6601.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Iturriza-Gómara M., Simpson R., Perault A.M. Structured surveillance of infantile gastroenteritis in East Anglia, UK: incidence of infection with common viral gastroenteric pathogens. Epidemiol Infect. 2008;136:23–33. doi: 10.1017/S0950268807008059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Koopmans M., Vinjé J., Duizer E., de Wit M., van Duijnhoven Y. Molecular epidemiology of human enteric caliciviruses in The Netherlands. Novartis Found Symp. 2001;238:197–214. doi: 10.1002/0470846534.ch12. [discussion 214–18] [DOI] [PubMed] [Google Scholar]
- 37.Murphy T.V., Garguillo P.M., Massoudi M.S. Intussusception among infants given an oral rotavirus vaccine. N Engl J Med. 2001;344:564–572. doi: 10.1056/NEJM200102223440804. [DOI] [PubMed] [Google Scholar]
- 38.Nakata S., Honma S., Namata K.K. Members of the family Caliciviridae (NV and SV) are the most prevalent causes of gastroenteritis outbreaks among infants in Japan. J Infect Dis. 2000;181:2029–2032. doi: 10.1086/315500. [DOI] [PubMed] [Google Scholar]
- 40.Ramig R.F. Systemic rotavirus infection. Expert Rev Anti Infect Ther. 2007;5:591–612. doi: 10.1586/14787210.5.4.591. [DOI] [PubMed] [Google Scholar]
- 41.Van Damme P., Giaquinto C., Maxwell M., Todd P., van der Wielen M., REVEAL Study Group Distribution of rotavirus genotypes in Europe 2004–2005: the REVEAL Study. J Infect Dis. 2007;195:S17–S35. doi: 10.1086/516715. [DOI] [PubMed] [Google Scholar]