

Abstract
This study identified social network profiles among children, determined whether profiles vary across sociodemographic characteristics, and investigated links between childhood profiles and depressive symptomology using three waves of data spanning 23 years (Wave 1, 1992 Metro-Detroit representative sample: n=193, ages 8–12). Latent profile analysis revealed three profiles: Close Family (22%), Varied Family (57%), Friend and Family (21%). White children were more likely than Black children to be in the Friend and Family profile. Children in the Close Family profile reported the lowest levels of depressive symptomology in childhood, but exhibited the steepest increase over time. Findings suggest that close, family-centric networks are protective in childhood, but less so as children develop into adulthood, highlighting the importance of considering developmental perspectives.
Children form and maintain social ties with multiple individuals during childhood and into adolescence, including family and friends, adults and peers (Furman & Buhrmester, 1985; Levitt, 2005; Levitt & Cici-Gokaltun, 2011). Previous research has focused on investigations of specific relationships in childhood (Chu, Saucier, & Hafner, 2010), such as the parent-child tie or peer friendships. There is limited research about the structure of social relations and social networks at earlier periods in the lifespan, particularly during middle childhood (i.e., ages 8 to 12). Similarly, little is known about their short- and long-term influences on health and well-being. The present study addresses this gap in the literature by examining the social networks of children in middle childhood and their association with depressive symptomology in childhood and over time into early adulthood.
Theoretical Framework
The present study is guided primarily by the convoy model of social relations, which describes social relations as dynamic and multidimensional (Antonucci, Fiori, Birditt, & Jackey, 2010; Kahn & Antonucci, 1980). Using this framework, the complexity of children’s social worlds is captured through multiple dimensions of social relations, including social network structure, function, and quality. Social network structure refers to the objective characteristics of personal networks, including size, composition (e.g., age, gender of, and relationship to network members), proximity to, and contact with network members. These aspects together represent the availability of interpersonal resources and social support. It is important to distinguish between social networks, social support, and relationship quality, because they each may differentially influence developmental outcomes (Antonucci & Akiyama, 1994). To gain a more holistic understanding of social network structure among children, this study examined multiple aspects of social network structure simultaneously using a pattern-centered approach.
There has been a concerted effort by researchers to look beyond the nuclear family and study social networks at large. Much of what we know about early life social relations comes from studies of early childhood or adolescence. This research informs the present study of older children’s social networks. Size and composition of children’s networks are most often studied, whereas research on other aspects of network structure, such as proximity and contact frequency, is less common (e.g., Franco & Levitt, 1997). Children’s social networks are small, relative to adults’, and dominated by family (Levitt, Guacci-Franco, Levitt, 1993). Close family members are typically the most important members of children’s social networks, but other family and non-kin are often included and take part in support exchanges. Even preschool-aged children frequently nominate peers (e.g., siblings, friends) and extended family as network members (Franco & Levitt, 1997). When children transition into adolescence, changes in their social networks reflect developmental shifts in social relations. Total number of friends, for example, increases with age as friends take on more significant social support functions (del Valle, Bravo, & Lopez, 2010; Levitt, Guacci-Franco, Levitt, 1993; Lewis, 2005). Older children also include more extended family (e.g., grandparents) and school-related figures (e.g., teachers, coaches) in their networks, reflecting their expanding social worlds and increased reliance on other significant adults for support (Furman & Buhrmester, 1992; Levitt, Guacci-Franco, et al., 1993). Network size, particularly of global and friendship networks, increases into early adulthood with the addition of co-workers, neighbors, and romantic partners as significant social figures, reflecting developmental milestones of this transition period, such as entry into the workplace, independent living, and family formation (Wrzus, Hänel, Wagner, & Neyer, 2013). These age-related changes in social network structure and social support are consistent with normative developmental trends, but highlight the need to attend to the unique role of family ties in childhood.
Research in developmental psychology has long demonstrated the importance of social relations for developmental outcomes. Classic developmental perspectives, including attachment theory (Bowlby, 1969) and the bioecological model (Bronfenbrenner & Morris, 2006), recognize that children are embedded within larger social networks that contribute to their development. The convoy model also has life course and lifespan foundations, proposing the long lasting effects effects of social relationships on health and well-being across the entire lifespan (Antonucci et al., 2010; Kahn & Antonucci, 1980). Several studies using the convoy model have documented independent associations of different dimensions of social relations on health and well-being (see Antonucci et al., 2010). Childhood social relations are thought to be particularly influential because these early relationships provide a foundation (i.e., secure base) for later life relationships. Further, the protective aspects of childhood social relations may serve as a buffer against the stresses and challenges that accompany development.
Empirical Evidence for Profiles of Social Relations
Although research on individual network characteristics is valuable for understanding the nature and implications of children’s social networks, variable-centered approaches do not capture systematic linkages between different components of social network structure. There is evidence that social network characteristics are systematically linked, and that these patterns of social relations influence outcomes beyond the implications of individual measures. Techniques like cluster analysis and latent class/profile analysis capture variations in patterns based on multiple indicators of social relations, including network structure (e.g., network size) and function (e.g., support exchanges). Although most studies have examined adult populations, particularly older adults (Fiori, Antonucci, & Cortina, 2006; Fiori, Smith, & Antonucci, 2007; Suanet, Antonucci, & Carr, 2016), the present study is relatively unique in that it focuses on children and follows them into early adulthood.
Pattern-centered approaches often yield common network typologies including: diverse, restricted, family-focused, and friend-focused. Diverse networks are usually relatively large and are composed of a number of different relationships, including family and friends. In contrast, restricted networks are small and only include very close individuals, usually close and immediate family. Other network types are primarily characterized by network composition (e.g., family or friend) and vary in size and support exchanges. Friend-focused networks include a majority of friends or other non-kin, whereas family-focused networks are predominantly made up of various combinations of immediate and extended family.
Studies that utilize pattern-centered techniques of children are less common. Alternative approaches, including social-cognitive maps and social network analysis, have been used to examine specific types of childhood networks, such as friendship networks (Cairns, Leung, Buchanan, & Cairns, 1995). The Affective Relationships Scale captures the multiplicity of relationships by characterizing patterns of social relations based on support exchanges among children and adolescents (Takahashi, 2005; Takahashi & Sakamoto, 2000). Common typologies among adolescents include mother-type, friend-type, and romantic partner-type, based on the person who fulfills the most support functions. These studies also recognize that there may not be one focal person in social networks, but multiple persons or none at all (e.g., lone wolf-type).
In one of the few studies with young people, Levitt and colleagues (2005) examined the social networks of 4th and 6th grade children undergoing the transition to adolescence to identify patterns of support using cluster analysis. Three patterns of social relations were identified initially and at the 2-year follow-up: close family/friends, close family, and close/extended family. There was variation among these patterns in the primary source of support. For instance, those in the close family/friends typology reported receiving support from a combination of family and friends. Similar patterns were identified upon closer examination of gender, ethnicity, and cohort, highlighting the robustness of these patterns in a diverse sample of children.
Distinguishing Factors in Childhood Social Networks
Social relations convoys evolve and are influenced by personal and situational characteristics that remain stable as well as those that change over time (Antonucci & Akiyama, 1987; Antonucci, Birditt, & Ajrouch, 2011). According to the convoy model, personal characteristics (e.g., age, sex, race, socioeconomic status) shape how individuals’ social networks are structured and the types of support they are likely to provide and receive (Antonucci et al., 2011). Older children are more likely to have friends in their networks, so it is hypothesized that age will be a distinguishing factor between networks that are characterized by the inclusion of same aged peers (Levitt, Weber, & Guacci, 1993). Women tend to report larger networks (Ajrouch, Blandon, & Antonucci, 2005), and girls have been found to include more friends in their networks compared to boys (Feiring & Lewis, 1991).
For children, the personal and situational characteristics of their parents may also play a strong role in shaping their own social relations. For example, in one of the only studies addressing this issue, Cochran and Riley (1990) identified race and household structure (i.e., one- or two-parent family) as two of the most influential characteristics for children’s social relations. Race, in particular, has been shown to shape social relations, especially in a multigenerational context in the United States. Black families have historically been more likely than White families to be extended and to live in multigenerational households (Wilson, 1989), and racial/ethnic minorities continue to exhibit this pattern today (Cohn & Passel, 2018). Levitt and colleagues (1993) found that White children were less likely to include and receive less support from extended family in their social networks than Black or Hispanic children, patterns that also reflect the family ecologies of adults (Ajrouch, Antonucci, & Janevic, 2001). Thus, we predict that the social networks of Black children will be characterized by a higher proportion of extended family than those of White children.
Children’s networks could also be considered to be a reflection of their parents’ networks and circumstances, specifically parental educational and economic resources (Cochran & Riley, 1990). Thus, it is useful to examine parental characteristics, including mother’s marital status and educational attainment, that contribute to building social capital for children (Parcel & Bixby, 2016). Higher educational attainment was associated with larger, more diverse, networks in a U.S. based sample of middle-aged and older adults (Ajrouch et al., 2005). This converging evidence suggests that mothers who are partnered and have attained higher levels of education shape their children’s social networks in ways that increases the availability of social resources.
Implications of Childhood Social Networks for Depressive Symptomology
The link between social relations and health has been well established, and numerous studies have identified social network structure and function as independent mechanisms of this association (Umberson & Montez, 2010). Prior research that identified social network typologies based on network structure and support have also indicated that these typologies are differentially linked to health and well-being. Generally, diverse, supportive networks are associated with the most adaptive outcomes, whereas restricted or unsupportive networks are associated with the worst outcomes. Findings for depressive symptomology as an indicator of well-being are particularly robust, especially for adult samples. Fiori and colleagues (2006) found that individuals in the diverse network profile exhibited the lowest levels of depression. In contrast, across multiple studies that used pattern-centered approaches, depressive symptomology was highest for respondents in restricted network profiles, characterized by the absence of or lack of support from both family and friends (Fiori, Antonucci, & Akiyama, 2008; Fiori et al., 2006; Fiori & Jager, 2011). More recently, Fuller-Iglesias and colleagues (2015) found that a lower proportion of family and larger family size, were associated with lower depressive symptomology among younger adults, but this association was only observed among older adults who reported low family negativity. This finding illuminates the nuanced link between social network structure and depressive symptomology across development.
Research on the social networks of children similarly suggests that diverse, supportive networks are the most adaptive. Using a pattern-centered analysis, Levitt and colleagues (2005) found that children in the close family/friends and close/extended family typologies reported more positive self-concept and decreased loneliness when compared to children in the close family typology. Most studies of childhood social relations, however, have been conducted in the context of specific relationships. For example, Ueno (2005) examined friendship networks of a nationally representative sample of adolescents and found that number of friends was negatively associated with depressive symptoms. Parental support is particularly influential for predicting depressive symptomology over time (Stice, Ragan, & Randall, 2004). Other studies provide evidence for unique interactions between family and peer relations on well-being (Erdley, Nangle, Newman, & Carpenter, 2001), pointing to systematic linkages among different social ties. These studies suggest that diverse networks containing multiple sources of support, particularly from family, promote well-being and protect against depressive symptomology.
Longitudinal studies across adulthood suggest that social relations are predictive of depression (Teo, Choi, & Valenstein, 2013). Studies that follow children into adulthood are limited, so it is unclear whether social networks in childhood are linked to trajectories of depressive symptomology over time. Prospective studies of early life predictors of depression during the transition to adulthood provide evidence for the influence of family network characteristics, including large family size and low parental support (Auerbach, Bigda-Peyton, Eberhart, Webb, & Ho, 2011; Meadows, Brown, & Elder, 2006; Reinherz, Paradis, Giaconia, Stashwick, & Fitzmaurice, 2003). Reciprocal friendships and lower levels of peer rejection in childhood have been linked to positive adjustment in adulthood (Bagwell, Newcomb, & Bukowski, 1998), whereas having no friends in childhood was associated with higher likelihood of exhibiting internalizing and externalizing problems in early adulthood (Sakyi, Surkan, Fombonne, Chollet, & Melchior, 2015). Given that most studies on the long-term influence of social networks and depression have been conducted on adult samples, the present study aims to fill this literature gap by investigating whether childhood social networks are predictive of trajectories of depressive symptomology over time.
Present Study
In the present study, we identify network typologies in children and investigate the association between children’s social network patterns and depressive symptomology both contemporaneously and longitudinally. Despite the well-established importance of children’s social ties on development, relatively little research has examined patterns of social relations including broader social networks, as well as implications for health and well-being in childhood and beyond. To obtain a better understanding of the social networks in childhood that are associated with depressive symptomology, we investigated components of social network structure and their mutual interplay by using latent profile analysis to identify profiles of social networks. This study addresses three research questions:
What are the patterns of social relations that can be identified among children using network structure? It is expected that patterns of social relations in childhood and early adulthood will be consistent with those previously identified in child samples (e.g., Levitt et al., 2005), with size and composition serving as defining characteristics. Specifically, it is hypothesized that observed patterns will include family-focused, friend-focused, and diverse networks of family and friends.
Is children’s membership in the identified profiles distinguishable by sociodemographic characteristics? We hypothesize that Black children’s networks will be characterized by the inclusion of more extended family. Older age is expected to be predictive of more friend-focused networks. We also hypothesize that children whose mothers report higher levels of education will have more diverse networks. No specific hypotheses are made with regard to gender and mother’s marital status.
Are social network profiles associated with depressive symptomology in childhood and trajectories of depressive symptomology over time into early adulthood? We expect that social network patterns that are characterized by limited availability of family ties or close others will be associated with higher depressive symptomology in childhood. Given the lack of research on long-term implications of childhood network structure, we make no specific predictions for how childhood social network patterns are associated with trajectories of depressive symptomology.
By leveraging self-report child social network data from a longitudinal study of social relations, this study contributes to the literature in several ways. With three data points over 23 years, following children from childhood into early adulthood, we can assess the short- and long-term impacts of childhood social relations. The present study includes children’s self reports of whom they consider close and important, rather than reporting on role prescribed relations or relying on parent or teacher reports. Finally, new and evolving methodological approaches such as latent profile analysis (LPA) are uniquely appropriate to address the complex, multidimensional nature of social relations. By uncovering patterns of social relations among children, and investigating how these patterns are linked to health and well-being, we hope to identify children who are most vulnerable, and those with the most adaptive social networks.
Method
Sample & Procedure
The Social Relations and Health over the Life Course Study is a three-wave, longitudinal study that began in 1992 (Antonucci & Akiyama, 1994). The first wave of this regionally representative sample (W1) was drawn from a stratified probability sample of 1,702 people aged 8–93 in the greater Detroit metropolitan area. The present study used the child sub-sample, which included 193 children aged 8 to 12 at W1. Recruitment efforts for child respondents targeted mothers who were participating in the study. In Wave 2 (W2; 2005), 143 (74.1%) of the original child sample in W1 was re-interviewed by telephone. In Wave 3 (W3; 2015), 109 (56.5%) of the original child sample were interviewed again. Of the sample, 90 respondents (47%) participated in all three waves, 53 respondents (28%) participated only in W1 and W2, 19 respondents (10%) participated only in W1 and W3, and 31 respondents (16%) participated only in W1. Table 1 provides demographic characteristics of the samples at each wave. An attrition analysis comparing child respondents who participated in subsequent waves with those who did not showed that respondents who participated in W2 were more likely to be female (χ (1) = 4.11, p < .05) and White (χ (1) = 8.13, p < .01), and those who participated in W3 were more likely to be White (χ (1) = 5.06, p < .05). They did not differ in terms of age, mother’s educational attainment, or mother’s marital status (at W1).
Table 1.
Social Relations and Health Study Child Sample, Descriptive Statistics
| M (SD)/% | |||
|---|---|---|---|
| Wave 1 (N = 193) | Wave 2 (N = 143) | Wave 3 (N = 109) | |
| Female | 52% | 57% | 56% |
| Race | 59% White | 65% White | 66% White |
| 32% Black | 30% Black | 26% Black | |
| Mother married/cohabiting | 72% | ||
| Child married/cohabiting | 25% | 60% | |
| Child age (years) | 10.08 (1.38) | 23.36 (1.47) | 33.37 (1.46) |
| [8–12] | [21–26] | [31–36] | |
| Child education (years) | 4.96 (1.42) | 13.54 (1.94) | 14.70 (1.92) |
| [2–8] | [9–17] | [8–17] | |
| Mother’s education (years) | 12.95 (1.94) | ||
| [7–17] | |||
| Child’s depressive symptoms | 4.20 (3.29) | 10.83 (11.05) | 8.69 (8.92) |
| [0–20] | [0–53] | [0–47] | |
Notes. Depressive symptoms were measured in W1 using the Childhood Depression Inventory (max score = 38), and in W2 and W3 using the the CES-D (max score = 60). Ranges presented in brackets.
To obtain social network data, child respondents enumerated those whom they considered close and important. Children were then asked to place those individuals in three circles representing varying levels of closeness (Antonucci, 1986). The inner circle included those whom the child considers “so close and important it is hard to imagine life without them”, and the middle and outer circles included those who were less close but still important enough to be part of the child’s social network. Children then answered a series of questions about the first 10 network members, including age, sex, and relationship.
Measures
Social network variables.
Childhood social network characteristics were assessed at W1. Descriptive statistics are provided in Table 2. Total network size represents the number of people the child included on his/her diagram (i.e., inner, middle, and outer circles combined). Less than 4% of the children included more than 20 network members, so the total network size was capped at 20, resulting in possible values of 0 to 20. Network composition includes the relative numbers of immediate and extended family, as well as gender and age composition of the child’s network. Percentages of the network that were immediate family, extended family, female, and age-mates were calculated by dividing the number of the network members in each category by the total number of network members (up to 10). Immediate family consisted of parents and siblings in childhood, including step-family. Extended family included grandparents and great-grandparents, cousins, and aunts/uncles. Age-mates included network members who were aged within one year (older or younger) of the child. Contact frequency with each network member was assessed with a single item, “How often are you in touch with [network member]?”, and averaged to represent the average frequency with which the child had contact with his or her network from irregularly (1) to lived with/everyday (5). Proximity indicates the percentage of network members that live within an hour’s drive of the respondent. Close others in the network represents the percentage of the network that is in the inner circle (out of a maximum of 10).
Table 2.
Correlations, Means, and Standard Deviations of Social Network Characteristics (Wave 1; n = 193)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | M (SD) | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Network Size | 1 | 8.66 (4.99) | |||||||
| 2. Contact Frequency | −0.21** | 1 | 4.34 (0.58) | ||||||
| 3. Close Others | −0.06 | 0.21** | 1 | 58.18 (27.76) | |||||
| 4. Proximate | −0.12 | 0.49*** | 0.17* | 1 | 87.93 (20.31) | ||||
| 5. Immediate Family | −0.38*** | 0.47*** | 0.42*** | 0.27*** | 1 | 47.65 (26.64) | |||
| 6. Extended Family | 0.38*** | −0.41*** | −0.17* | −0.37*** | −0.52*** | 1 | 31.52 (26.58) | ||
| 7. Female | −0.01 | 0.10 | 0.10 | 0.03 | 0.21** | 0.06 | 1 | 53.09 (20.70) | |
| 8. Age-mates | −0.01 | −0.02 | −0.29*** | 0.08 | −0.43*** | −0.38*** | −0.38*** | 1 | 21.68 (24.40) |
Notes.
p < .05
p < .01
p < .001
Depressive Symptoms.
Children’s depressive symptoms were assessed in W1 using the Children’s Depression Inventory (CDI). On each of 19 items, children were asked to indicate which of three statements best applied to them (e.g., I am sad once in a while [0]/ I am sad a lot [1]/ I am sad all the time [2]). In W2 and W3, depressive symptoms were assessed using the Center for Epidemiological Studies Depression Scale, which consists of 20 statements (e.g., I felt lonely). Respondents indicated, from 0 (rare/none of the time) to 3 (most/all of the time), how often they had felt that way over the past week. Total depressive symptomology was computed by summing the individual items to yield a maximum score of 38 in W1 and 60 in W2/W3.
Sociodemographics.
Sociodemographic characteristics were collected from child and mother reports. Sex (1 = female, −1 = male), race (1 = White, −1 = Black), and mother’s marital status at W1 (1 = married/living with partner, −1 = not married/living with partner) were dichotomous variables. Childhood socioeconomic status was measured using mother’s educational attainment in years at W1. Child age and years of education were also measured in years at each wave.
Analysis Strategy
Identification of patterns of social networks.
Latent profile analysis (LPA) was used to identify profiles among children who share similar social network characteristics at W1. Two-, three-, and four-class models were tested in MPlus Version 7.4. With LPA, the approximate number of relevant profiles can be empirically determined using a number of model fit statistics, including Bayesian information criteria (BIC), Lo-Mendell-Rubin (LMR) test, and entropy (Tein, Coxe, & Cham, 2013). A lower BIC indicates better model fit. A significant result on the LMR test indicates that the model tested, k –profile, is a significant improvement over the (k-1)–profile model. Higher entropy indicates better separation between profiles. Posterior profile membership probabilities were used to assign respondents to a profile in the best fitting model.
Distinguishing social network profiles.
Multinomial logistic regression was conducted to assess if childhood (i.e., W1) sociodemographic characteristics are associated with the probability of membership in childhood network profiles. The sociodemographics examined in the model included the child’s sex, race, and age, and the mother’s education and marital status. Continuous variables were mean centered and dichotomous variables were effect coded.
Social network profiles and depressive symptomology.
The link between childhood network profile and depressive symptomology was assessed both cross-sectionally and longitudinally using SAS version 9.4. To investigate whether the identified social network profiles were differentially linked to depressive symptoms in childhood, multiple linear regression analysis was conducted on the full W1 sample (n = 193). We also considered childhood (i.e., W1) sociodemographic characteristics that contribute to depressive symptomology and include them as covariates (Twenge & Nolen-Hoeksema, 2002). The final model controlled for child sex, race, age and mother’s education and marital status at W1.
Next, to assess whether childhood network profiles were associated with depressive symptomology over time, multilevel growth curve models were fit using data from respondents with complete W3 data (n = 109) to ensure that the growth curves captured the span of 23 years represented in the longitudinal data. Due to the different instruments for measuring depressive symptoms in childhood (i.e., CDI) and adulthood (i.e., CES-D), we first standardized the scores to make them comparable over time. Although the standardized scores are not absolute measures, they provide a general idea of change over time relative to the samples (Bayley, 1956). First, an empty model was fit with random intercepts to examine between person variance. Next, standardized scores for depressive symptomology were modeled as a function of time and all sociodemographic covariates from all three waves (base model). Sex, race, and childhood socioeconomic status (i.e., mother’s education) were time-invariant, whereas respondents’ age and educational attainment were time-varying. Next, we entered a main effect term for childhood network profile (Model 1) to test the association of childhood network profile, measured at W1, and average level of depressive symptomology across time. Finally, we added an interaction term for childhood network profile by time to determine whether childhood network profile was associated with the rate of change in depressive symptomology over time (Model 2).
Results
We begin by identifying the children’s social network profiles and then examine whether network profiles vary by sociodemographic characteristics. We turn next to the contemporaneous assessment of the association between the profiles and the CDI. Finally, we examine the longitudinal association between the childhood profiles and depressive sympotomology.
Profiles of Children’s Social Networks
Network size, composition, contact frequency, proximity, and close others were included in a latent class analysis to identify typologies of social networks among children. As the number of profiles tested increased, the BIC decreased and the entropy remained stable, around 0.90. However, results from the LMR test indicated that a 4-profile solution did not significantly improve the model fit compared to the three-profile solution (LMR = 116.03, p = .39). Based on these fit statistics (Supplemental Table 1), a three-profile model was adopted as the best fit to the data. The identified profiles, distinguished primarily by variations in network size and composition, included: Varied Family, Friend and Family, and Close Family (Table 3).
Table 3.
Social Network Structure Characteristics and Sociodemographics by Network Type (N = 193)
| M (SD)/ % | |||
|---|---|---|---|
| Varied Family | Friend and Family | Close Family | |
| n (%) | 110 (57%) | 41 (21%) | 42 (22%) |
| Social Network Characteristics | |||
| Network Size | 10.55 (4.86) | 7.98 (3.98) | 4.40 (3.17) |
| Contact Frequency | 4.17 (0.57) | 4.36 (0.55) | 4.78 (0.39) |
| % Close Others | 55.30 (27.11) | 46.36 (20.43) | 77.23 (26.69) |
| % Proximate | 83.00 (22.77) | 91.26 (18.44) | 97.60 (7.03) |
| % Immediate Family | 37.29 (13.63) | 33.24 (19.24) | 88.85 (15.33) |
| % Extended Family | 51.12 (16.61) | 5.97 (9.07) | 5.15 (9.99) |
| % Female | 55.14 (13.06) | 57.94 (21.83) | 58.96 (20.77) |
| % Age-mates | 13.15 (13.06) | 57.94 (21.84) | 8.62 (13.60) |
| Sociodemographics | |||
| Child Age (years) | 10.02 (1.37) | 10.17 (1.51) | 10.17 (1.29) |
| Child Grade (years) | 4.87 (1.43) | 5.03 (1.56) | 5.14 (1.26) |
| Mother’s Education | 12.96 (1.82) | 13.15 (2.10) | 12.71 (2.10) |
| Mother Married/ Cohabiting | 69% | 85% | 64% |
| Female | 57% | 46% | 45% |
| Race | 56% White | 83% White | 45% White |
| 36% Black | 7% Black | 48% Black | |
Description of Profiles.
Most respondents were characterized by the Varied Family profile (57%), followed by the Close Family profile (22%), then the Friend and Family profile (21%). Members of the Varied Family profile were characterized by relatively large networks, on average 10 people, consisting of both immediate and extended family, but with a larger percentage of extended family. The Friend and Family profile was characterized by average-sized networks, approximately 8 people, consisting of mostly immediate family and non-kin, but a smaller percentage of extended family. These respondents included the greatest proportion of age-mates in their networks. Finally, the Close Family profile was characterized by relatively small-sized networks, on average 4 people, dominated by immediate family. In addition to being relationally close, respondents in the Close Family profile were also geographically and emotionally close, as indicated by the high percentages of proximate and close others.
Based on the distinguishing feature of network composition, we explored whether there were variations in the types of relationship partners that children included in their networks by network profile. We examined whether or not respondents included a mother, father, sibling, grandparent, aunt or uncle, cousin, and friend in their network (Supplemental Table 2). Most distinctively, all respondents in the Close Family profile included at least one parent and no friends in their networks. In contrast, all respondents in the Friend and Family profile included at least one friend in their network, whereas only 78% of them included a parent.
Sociodemographics Distinguishing Profiles
The Close Family profile served as the reference group for the multinomial logistic regression models (Table 4). Results indicated that race was the only significant predictor of profile membership, such that White children were significantly more likely than Black children to be in the Friend and Family profile (b = 0.79, p < .01). Child sex, age, mother’s marital status, and mother’s education level were not associated with childhood network profiles.
Table 4.
Results of Multinomial Logistic Regression Examining Sociodemographic Predictors of Network Type (N = 193)
| Close Family vs. Varied Family |
Close Family vs. Friend and Family |
|||
|---|---|---|---|---|
| b (SE) | OR | b (SE) | OR | |
| Intercept | 0.95 (0.20)*** | −0.40 (0.29) | ||
| Sex (1=Female) | 0.26 (0.19) | 1.30 | −0.004 (0.23) | 1.00 |
| Race (1=White) | 0.16 (0.20) | 1.17 | 0.79 (0.28)** | 2.20 |
| Age (years) | −0.09 (0.13) | 0.91 | 0.001 (0.17) | 1.00 |
| Mother’s education level (years) | 0.06 (0.10) | 1.07 | 0.05 (0.12) | 1.05 |
| Mother’s marital status (1=married) | 0.03 (0.22) | 1.03 | 0.24 (0.30) | 1.28 |
Notes. OR = Odds Ratio
p < .01
Links to Depressive Symptoms
To test whether children’s network typologies were linked to depressive symptoms in childhood, multiple linear regression was conducted. The Close Family profile served as the reference group. Membership in the Varied Family profile was not associated with depressive symptomology (b = 0.54, n.s.), whereas membership in the Friend and Family profile was associated with higher levels of depressive symptomology (b = 2.15, p < .01; Table 5).
Table 5.
Childhood Depressive Symptomology as a Function of Child Network Profiles (N = 193)
| B | SE | β | |
|---|---|---|---|
| Intercept | 3.51 | 0.52 | |
| Childhood Network Profile | |||
| Varied Family | 0.54 | 0.61 | 0.08 |
| Friend & Family | 2.15 | 0.76 | 0.27** |
| Sex (1=female) | 0.10 | 0.25 | 0.03 |
| Race (1=White) | −0.34 | 0.26 | −0.10 |
| Age | −0.05 | 0.18 | −0.02 |
| Mother’s Education | −0.16 | 0.13 | −0.09 |
| Adjusted R2 | 0.028 | ||
Notes. Reference group is Close Family typology coded 0;
p < .01
Growth curve analysis was used to determine whether childhood network profile was associated with trajectories of depressive symptomology over time. The ICC obtained from the empty model indicated that 54% of the variance in depressive symptomology can be attributed to between person variation over time. The base model, which included time and all sociodemographic covariates, showed an average increase in depressive symptomology over time (b = 0.03, p < .01). The main effects model, which included the childhood network profiles, showed no main effect of social network in childhood on depressive symptomology (Table 6, Model 1). In other words, social network profile in childhood was not significantly associated with average levels of depressive symptomology over time. Finally, we tested interactions between childhood network profile and time. These results (Table 6, Model 2) showed that the rate of change of depressive symptomology was dependent on childhood social networks. Compared to respondents in the Close Family profile, who experienced the steepest increase in depressive symptoms, those in the Friend and Family profile showed increases at significantly slower rates (Figure 1). We also conducted follow-up analyses to test the independent effects of childhood network profile on adult depressive symptomology, but found no direct effects after accounting for childhood depressive symptoms and other sociodemographic covariates.
Table 6.
Fixed effects for multilevel models of change in depressive symptomology from childhood to adulthood (n = 109)
| Model 1 | Model 2 | |
|---|---|---|
| B (SE) | B (SE) | |
| Intercept | 0.60 (0.20)** | 0.33 (0.23) |
| Time (Rate of change) | 0.03 (0.01)** | 0.05 (0.01)*** |
| Childhood Network Profile | ||
| Varied Family | −0.23 (0.16) | 0.05 (0.22) |
| Friend and Family | −0.10 (0.20) | 0.34 (0.27) |
| Childhood Network Profile x Time | ||
| Varied Family | −0.02 (0.01)+ | |
| Friend and Family | −0.04 (0.01)* | |
| Sex (1=female) | 0.14 (0.07)* | 0.14 (0.07)* |
| Race (1=White) | −0.08 (0.08) | −0.08 (0.08) |
| Age | 0.08 (0.05) | 0.08 (0.05) |
| Education | −0.08 (0.02)*** | −0.07 (0.05)** |
| Mother’s Education (W1) | −0.02 (0.04) | −0.02 (0.04) |
| Variance Estimates | ||
| Intercept | 0.22 (0.06)*** | 0.23 (0.06)*** |
| Within Residual | 0.61 (0.06)*** | 0.59 (0.06)*** |
| −2LL | 774.0 | 768.0 |
| −2LL change | 2.1 | 6.0* |
Notes. Reference group Close Family profile coded 0. −2LL change for Model 1 represents change from the covariates only model (−2LL = 804.8).
p < .10
p < .05
p < .01
p < .001
Figure 1.
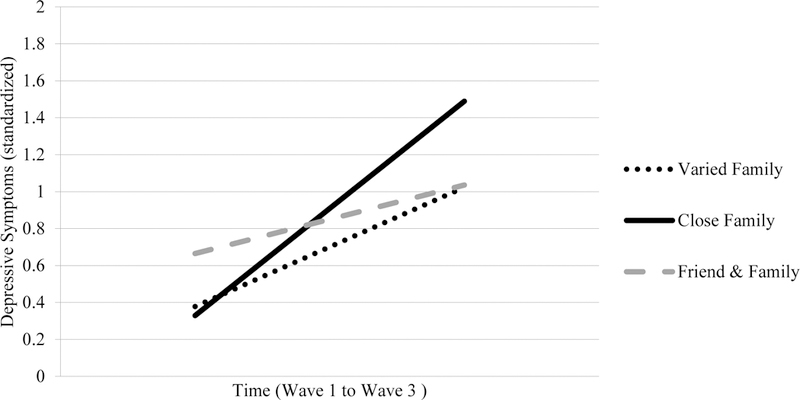
Trajectories of depressive symptomology over time from childhood to adulthood by childhood network profile. Simple slopes: Varied Family (b = 0.029, t = 2.40, p < .05); Close Family (b = 0.053, t = 3.60, p < .001); Friend & Family (b = 0.017, t = 1.15, n.s.).
Discussion
Children are embedded within larger social networks, and the constellation of these social ties contributes to development in childhood and beyond. The goals of this study were to (1) identify distinct profiles of social network structure among a sample of children, (2) determine whether these patterns varied by sociodemographic characteristics, and (3) evaluate the links between childhood social networks and concurrent and long-term depressive symptomology. The results indicated that three distinct profiles of social network structure could be identified, and that children’s membership in these profiles varied by race. Further, results suggested that childhood social networks are associated with childhood depressively symptomology, as well as change in depressive symptomology over time into young adulthood.
Patterns and Predictors of Children’s Networks
The current analysis identified three distinct network typologies among a regionally representative sample of children. The predominant pattern of children’s social networks was the Varied Family profile, which was characterized by a large-sized network with the inclusion of mostly immediate and extended family. The Friend and Family profile was characterized by average-sized networks consisting of mostly immediate family and friends, but relatively little extended family. A descriptive assessment of network composition revealed that all children who were categorized into this typology included a friend in their social networks. Finally, the Close Family profile consisted predominantly of immediate family and captured networks that were geographically proximate and emotionally close. These derived profiles are consistent with previous research on childhood social networks (Levitt et al., 2005), as well as the main network types that have been identified in studies of adult samples. For example, the Varied Family pattern in childhood best exemplifies “family-focused” networks of adulthood, whereas the Friend and Family pattern best exemplifies “diverse” networks. This consistency might indicate the robustness of certain social network patterns or typologies across the lifespan. Alternatively, there may be only a finite number of patterns that will emerge given the possible combinations of network size, composition, contact, and proximity.
Further, White children were more likely than Black children to exhibit the Friend and Family pattern than they were to exhibit the Close Family pattern. This might be a consequence of parents or other caregivers shaping children’s social networks. In adult samples, non-Hispanic White individuals interact and exchange support with friends more often than Black individuals (Taylor et al., 2013). Because the measures of network composition were proportions, rather than totals, social networks with a relatively high proportion of non-kin, including friends, also had a relatively low proportion of family. Contrary to prior research with adult samples, Black children did not fall disproportionately into the Varied Family profile. Furthermore, mother’s marital status and educational attainment were not associated with membership across the classes. These findings might be explained by lack of variability in mothers’ educational attainment. Nguyen (2017) identified social network typologies among an ethnically diverse sample of older adults, and found that while profile membership was not differentiated by race, there was a race by education interaction. It is also surprising that there were no age differences in terms of network profile membership, given that age differences in social network size and composition are so commonly observed. One possible explanation is that the age range of the current sample was not wide enough to capture the changes that occur during the transition to adolescence.
Links to Depressive Symptoms
Findings from this study showed that compared to the Close Family profile, the Friend and Family profile was associated with the highest depressive symptomology. This pattern of results underscores the developmental significance of family ties in childhood. It should be noted that because network composition was a relative, rather than absolute, measure children in the Friend and Family profile may have been lacking close family ties, and substituting peer or other non-kin relations to compensate. Consequently, it may not be the availability of family support in the Close Family and Varied Family profiles that protects against depressive symptoms, but rather the lack of family support in the Friend and Family focused typology that makes those children more vulnerable. Studies of older adolescents suggest that parental support, in particular, is a robust protective factor against depression (Auerbach et al., 2011; Colarossi & Eccles, 2003). For children and younger adolescents who rely on parents and other caregivers, the absence of family support, even in the presence of peer support, may be especially harmful to psychological well-being. Indeed, results from a meta-analysis showed that friend support was not as strongly linked to well-being as family support among children and adolescents (Chu et al., 2010). In childhood, social networks that lack strong family ties, but are otherwise robust, still present vulnerability. It should be noted, however, that the observed levels of depressive symptomology are relatively low across the sample. These findings should be interpreted with caution, particularly in the context of clinical applications.
Interestingly, although the typologies were consistent with those identified by Levitt et al. (2005), they were not associated with well-being in the same way. Specifically, children in the Close Family typology reported poorer psychosocial adjustment (Levitt et al., 2005), but in the present study, children in the Close Family profile reported relatively low levels of depressive symptomology compared to the others. Although potentially supportive and beneficial, social ties often come with a cost (Antonucci, Akiyama, & Lansford, 1998). Larger social networks increase the likelihood of interpersonal stress or exposure to close others’ stress. Accordingly, close, supportive social networks in childhood would be more advantageous in terms of providing adequate support, but perhaps also in protecting against additional interpersonal stress.
An alternative explanation for these discrepant findings is that the Close Family typology identified by Levitt and colleagues (2005) is reminiscent of Takahashi’s (2001) “lone wolf” classification such that it is adversely related to well-being. Instead, the Close Family profile in the present study could reflect a tight-knit, supportive family network, which is a strength, particularly in childhood. It is developmentally normative in the U.S. for networks to be small and comprised of only very close individuals, like family, early in life. In adult samples, however, the Close Family profile that we identified would be considered “restricted” and characterized by small networks of only the closest individuals (Fiori et al., 2007; Park et al., 2013; Suanet et al., 2016). Restricted networks are typically the most socially isolated and, thus, most likely to be associated with poor well-being (e.g., depressive symptomology) in comparison to other network typologies. In childhood, however, the presence of close (i.e., nuclear) family is both culturally and developmentally appropriate, and even beneficial.
In contrast, the Friend and Family childhood profile would be considered “diverse” in most adult samples, and consequently, associated with better well-being. In the present study, respondents in the Friend and Family profile reported the greatest depressive symptomology. Despite the continuity of concepts of social relations, the observed links to depressive symptomology suggest that there is a developmental difference in manifestation and meaning.
Indeed, results from the longitudinal analysis provide further evidence of the differential impact of social network structure across development. Trajectories of depressive symptomology varied by childhood network profile such that respondents in the Close Family profile experienced the steepest increase in depressive symptomology over time into young adulthood, suggesting that a Close Family profile is not universally advantageous across development. It might be that close family networks are maximally beneficial in childhood but only if they later transition to more diverse Varied or Family and Friend networks. Supportive family relationships in childhood, particularly parent-child relationships, provide individuals with a secure base from which to diversify their social social networks and form similarly supportive relationships in adulthood. Indeed, conflictual parent-child relationships in adolescence have been shown to negatively affect partner relationships in young adulthood as well as psychological adjustment to the transition to adulthood (Overbeek, Stattin, Vermulst, Ha, & Engels, 2007). The current analysis does not consider stability or change in social networks over time, so it is unclear whether this association is a result of stability of a Close Family, or restricted, social network. There is evidence to suggest stability in the parent-child tie from adolescence to young adulthood (Aquilino, 1997). Future research should assess changes or transitions in social networks over time to more precisely identify what types of social networks are most adaptive at different developmental stages. This type of research is complicated by the difficulty of assessing similar concepts across different ages and developmental periods. Furthermore, Aquilino (1997) noted that observed changes in the parent-child tie were associated with changes in children’s role status, including marriage, parenthood, and employment. These role changes that define the transition to adulthood are accompanied by well-documented changes in social network structure (Wrzus et al., 2013). The W2 and W3 samples in the present study were not large enough to probe the effect of these role changes on social network structure and, subsequently, on health and well-being, but this is an important direction for future research.
Future Directions
The present study’s most notable strength is that the measures include self-reported survey data from children drawn from a regionally representative community based sample. Many other studies of children’s social relations rely on children from particular schools, clinics or laboratory studies or from parent reports of children’s social relations. Even though children’s social network data was self-reported, it is important to note that children can exert only so much control over their own social networks. Parents or other adults might serve as gatekeepers of their children’s interactions with other family members or friends which then, consequently, may influence whom they include in their social networks (Cochran & Riley, 1990). Future studies might examine this question empirically by exploring the similarity between parent and child networks. Although the regional representativeness of the study is a strength, that also limits generalizability to different populations. For example, this is a metropolitan sample and thus does not represent rural America. Further, it does not represent non-U.S. populations, limiting the cross-cultural application of these findings (Antonucci et al., 2010). The baseline data for this study were collected in 1992, and may be uniquely representative of that cohort. Given the role of technology and social media in the formation and maintenance of contemporary social ties for both children and adults (Antonucci, Ajrouch, & Manalel, 2017), the implications of these societal changes on children should also be addressed. In addition, the relatively small sample size may have limited our ability to detect more variation in children’s social networks or in the links between network profile and depressive symptomology. Despite limits in statistical power, the sample is relatively large for a descriptive analysis of children’s social networks.
Perceived relationship quality has been found to be a stronger predictor of health and well-being than network structure measures, including in childhood (Chu et al., 2010; Rueger, Malecki, Pyun, Aycock, & Coyle, 2016). Indeed, the convoy model argues that social network structure is associated with well-being through social support and relationship quality (Kahn & Antonucci, 1980). The present study used only social network structure to identify typologies, but social support may also have been incidentally captured in the identified network typologies. Compared to adults, children’s subjective evaluations of who is close and important enough to be included in their personal network may be more strongly influenced by their perceptions of support exchanges or relationship quality. Children in the present study may have confounded network structure with network function, nominating only those individuals with whom they exchange support. Future research should more precisely delineate the influences of social network structure and support in childhood.
The present study uniquely describes children’s social networks and the implications of different network typologies on well-being in childhood and over time, providing a basis for future inquiries into the continuity and consequences of children’s social networks. This study looks beyond the nuclear family to examine a larger constellation of social ties, providing a more holistic picture of children’s social worlds and the implications of these broader social connections. These findings contribute to our understanding children’s social networks, provide insight into ways to leverage social relations to improve health and well-being in childhood and beyond, and highlight the importance of incorporating developmental perspectives into the study of social relations across the lifespan.
Supplementary Material
Acknowledgements:
Presented are longitudinal data from the Social Relations and Health Over the Life Course Study (Toni Antonucci, Principal Investigator), which is supported by grants from the National Institute of Mental Health (MH46549 and MH066876) and the National Institute on Aging (AG13490, AG030569, AG045423). We gratefully acknowledge Angela Turkelson for her assistance with the analyses and Kira Birditt, Kai Cortina, Berit Ingersoll-Dayton, Jacqui Smith, and those in the Life Course Development Program at the University of Michigan, especially Emma Beyers-Carlson and Lauren Tighe in the LCD Jr. group, for their ideas and useful comments.
References
- Ajrouch KJ, Antonucci TC, & Janevic MR (2001). Social networks among blacks and whites: the interaction between race and age. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 56, S112–S118. 10.1093/geronb/56.2.S112 [DOI] [PubMed] [Google Scholar]
- Ajrouch KJ, Blandon AY, & Antonucci TC (2005). Social networks among men and women: The effects of age and socioeconomic status. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 60, S311–S317. 10.1093/geronb/60.6.S311 [DOI] [PubMed] [Google Scholar]
- Antonucci TC (1986). Hierarchical mapping technique. Generations, 10(4), 10–12. [Google Scholar]
- Antonucci TC, Ajrouch KJ, & Manalel JA (2017). Social relations and technology: Continuity, context, and change. Innovation in Aging, 1, 1–9. 10.1093/geroni/igx029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Antonucci TC, & Akiyama H. (1987). Social networks in adult life and a preliminary examination of the convoy model. Journal of Gerontology, 42, 519–527. 10.1093/geronj/42.5.519 [DOI] [PubMed] [Google Scholar]
- Antonucci TC, & Akiyama H. (1994). Convoys of attachment and social relations in children, adolescents, and adults In Social networks and Social Support in Childhood and Adolescence (pp. 37–52). Walter de Gruyter. [Google Scholar]
- Antonucci TC, Akiyama H, & Lansford JE (1998). Negative effects of close social relations. Family Relations, 47, 379–384. 10.2307/585268 [DOI] [Google Scholar]
- Antonucci TC, Birditt KS, & Ajrouch K. (2011). Convoys of social relations: Past, present, and future. In Fingerman KL, Berg C, Smith J, & Antonucci TC (Eds.), Handbook of Life Span Development; (pp. 161–182). [Google Scholar]
- Antonucci TC, Fiori KL, Birditt K, & Jackey LMH (2010). Convoys of social relations: Integrating life-span and life-course perspectives In Lamb ME & Freund AM (Eds.), The Handbook of Life-Span Development (Vol. 2, pp. 434–473). Hoboken, NJ: John Wiley & Sons, Incorporated; 10.1002/9780470880166 [DOI] [Google Scholar]
- Aquilino WS (1997). From adolescent to young adult: A prospective study of parent-child relations during the transition to adulthood. Journal of Marriage and the Family, 59, 670 10.2307/353953 [DOI] [Google Scholar]
- Auerbach RP, Bigda-Peyton JS, Eberhart NK, Webb CA, & Ho MHR (2011). Conceptualizing the prospective relationship between social support, stress, and depressive symptoms among adolescents. Journal of Abnormal Child Psychology, 39, 475–487. 10.1007/s10802-010-9479-x [DOI] [PubMed] [Google Scholar]
- Bagwell CL, Newcomb AF, & Bukowski WM (1998). Preadolescent friendship and peer rejection as predictors of adult adjustment. Child Development, 69, 140–153. 10.1111/j.1467-8624.1998.tb06139.x [DOI] [PubMed] [Google Scholar]
- Bayley N. (1956). Individual patterns of development. Child Development, 27, 45–74. 10.2307/1126330 [DOI] [PubMed] [Google Scholar]
- Bowlby J. (1969). Attachment and Loss: Attachment. New York: Basic Books. [Google Scholar]
- Bronfenbrenner U, & Morris PA (2006). The bioecologist model of human development. In Damon W & Lerner RM (Eds.), Handbook of Child Psychology; (6th ed, pp. 793–828). Hoboken, NJ: John Wiley& Sons, Incorporated. [Google Scholar]
- Cairns RB, Leung M-C, Buchanan L, & Cairns BD (1995). Friendships and social networks in childhood and adolescence: Fluidity, reliability, and interrelations. Child Development, 66, 1330–1345. 10.1111/j.1467-8624.1995.tb00938.x [DOI] [PubMed] [Google Scholar]
- Chu P. Sen, Saucier DA, & Hafner E. (2010). Meta-analysis of the relationships between social support and well-being in children and adolescents. Journal of Social and Clinical Psychology, 29, 624–645. 10.1521/jscp.2010.29.6.624 [DOI] [Google Scholar]
- Cochran MM, & Riley D. (1990). The social networks of six-year-olds: Context, content, and consequence In Cochran MM, Larner M, Riley D, Gunnarsson L, & Henderson CR (Eds.), Extending Families: The Social Networks of Parents and Their Children (pp. 154–179). New York, NY: Cambridge University Press. [Google Scholar]
- Cohn D, & Passel JS (2018). A record 64 million Americans live in multigenerational households. Retrieved from http://www.pewresearch.org/fact-tank/2018/04/05/a-record-64-million-americans-live-in-multigenerational-households/
- Colarossi LG, & Eccles JS (2003). Differential effects of support providers on adolescents’ mental health. Social Work Research, 27, 19–30. 10.1093/swr/27.1.19 [DOI] [Google Scholar]
- del Valle JF, Bravo A, & Lopez M. (2010). Parents and peers as providers of support in adolescents’ social network: A developmental perspective. Journal of Community Psychology, 38, 16–27. 10.1002/jcop [DOI] [Google Scholar]
- Erdley CA, Nangle DW, Newman JE, & Carpenter EM (2001). Children’s friendship experiences and psychological adjustment: Theory and research. New Directions for Child and Adolescent Development, 91, 5–24. 10.1002/cd.3 [DOI] [PubMed] [Google Scholar]
- Feiring C, & Lewis M. (1991). The transition from middle childhood to early adolescence: Sex differences in the social network and perceived self-competence. Sex Roles, 24 10.1007/BF00289335 [DOI] [Google Scholar]
- Fiori KL, Antonucci TC, & Akiyama H. (2008). Profiles of social relations among older adults: a cross-cultural approach. Ageing and Society, 28, 203–231. 10.1017/S0144686X07006472 [DOI] [Google Scholar]
- Fiori KL, Antonucci TC, & Cortina KS (2006). Social network typologies and mental health among older adults. Journals of Gerontology, Series B: Psychological Science, 61, 25–32. 10.1093/geronb/61.1.P25 [DOI] [PubMed] [Google Scholar]
- Fiori KL, & Jager J. (2011). The impact of social support networks on mental and physical health in the transition to older adulthood: A longitudinal, pattern-centered approach. International Journal of Behavioral Development, 36, 117–129. 10.1177/0165025411424089 [DOI] [Google Scholar]
- Fiori KL, Smith J, & Antonucci TC (2007). Social network types among older adults: A multidimensional approach. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 62, P322–30. 10.1093/geronb/62.6.P322 [DOI] [PubMed] [Google Scholar]
- Franco N, & Levitt MJ (1997). The social ecology of early childhood: Preschool social support networks and social acceptance. Social Development, 6, 292–306. 10.1111/j.1467-9507.1997.tb00107.x [DOI] [Google Scholar]
- Fuller-Iglesias HR, Webster NJ, & Antonucci TC (2015). The complex nature of family support across the life span: Implications for psychological well-Being. Developmental Psychology, 51, 277–288. 10.1037/a0038665 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furman W, & Buhrmester D. (1985). Children’s perceptions of the personal relationships in their social networks. Developmental Psychology, 21, 1016–1024. 10.1037/0012-1649.21.6.1016 [DOI] [Google Scholar]
- Furman W, & Buhrmester D. (1992). Age and sex differences in perceptions of networks of personal relationships. Child Development, 63, 103–115. 10.1111/j.1467-8624.1992.tb03599.x [DOI] [PubMed] [Google Scholar]
- Kahn RL, & Antonucci TC (1980). Convoys over the life course: Attachment, roles, and social support In Baltes PB & Brim OG (Eds.), Life-span development and behavior (pp. 254–286). Academic Press. [Google Scholar]
- Levitt MJ (2005). Social relations in childhood and adolescence: The convoy model perspective. Human Development, 48, 28–47. 10.1159/000083214 [DOI] [Google Scholar]
- Levitt MJ, & Cici-Gokaltun A. (2011). Close relationships across the life span In Fingerman KL, Berg CA, Smith J, & Antonucci TC (Eds.), Handbook of Life-Span Development (pp. 457–486). New York, NY: Springer Publishing Company. [Google Scholar]
- Levitt MJ, Guacci-Franco N, & Levitt JL (1993). Convoys of social support in childhood and early adolescence: Structure and function. Developmental Psychology, 29, 811–818. 10.1037//0012-1649.29.5.811 [DOI] [Google Scholar]
- Levitt MJ, Levitt J, Bustos G, Crooks NA, Santos JD, Telan P, … Milevsky A. (2005). Patterns of social support in the middle childhood to early adolescent transition: Implications for adjustment. Social Development, 14, 398–420. 10.1111/j.1467-9507.2005.00308.x [DOI] [Google Scholar]
- Levitt MJ, Weber RA, & Guacci N. (1993). Convoys of social support: an intergenerational analysis. Psychology and Aging, 8, 323–326. 10.1037/0882-7974.8.3.323 [DOI] [PubMed] [Google Scholar]
- Lewis M. (2005). The child and its family: The social network model. Human Development, 48, 8–27. 10.1159/000083213 [DOI] [Google Scholar]
- Meadows SO, Brown JS, & Elder GH (2006). Depressive symptoms, stress, and support: Gendered trajectories from adolescence to young adulthood. Journal of Youth and Adolescence, 35, 99–103. 10.1007/s10964-005-9021-6 [DOI] [Google Scholar]
- Nguyen AW (2017). Variations in social network type membership among older African Americans, Caribbean Blacks, and Non-Hispanic Whites. Journals of Gerontology - Series B Psychological Sciences and Social Sciences, 72, 716–726. 10.1093/geronb/gbx016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Overbeek G, Stattin H, Vermulst A, Ha T, & Engels RCME (2007). Parent-child relationships, partner relationships, and emotional adjustment: A birth-to-maturity prospective study. Developmental Psychology, 43, 429–437. 10.1037/0012-1649.43.2.429 [DOI] [PubMed] [Google Scholar]
- Parcel TL, & Bixby MS (2016). The ties that bind: Social capital, families, and children’s well-being. Child Development Perspectives, 10, 87–92. 10.1111/cdep.12165 [DOI] [Google Scholar]
- Park NS, Jang Y, Lee BS, Ko JE, Haley WE, & Chiriboga DA (2013). An empirical typology of social networks and its association with physical and mental health: A study with older Korean immigrants. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 70, 67–76. 10.1093/geronb/gbt065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinherz HZ, Paradis AD, Giaconia RM, Stashwick CK, & Fitzmaurice G. (2003). Childhood and adolescent predictors of major depression in the transition to adulthood. American Journal of Psychiatry, 160, 2141–2147. 10.1176/appi.ajp.160.12.2141 [DOI] [PubMed] [Google Scholar]
- Rueger SY, Malecki CK, Pyun Y, Aycock C, & Coyle S. (2016). A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychological Bulletin, 142, 1017–1067. 10.1037/bul0000058 [DOI] [PubMed] [Google Scholar]
- Sakyi KS, Surkan PJ, Fombonne E, Chollet A, & Melchior M. (2015). Childhood friendships and psychological difficulties in young adulthood: An 18-year follow-up study. European Child and Adolescent Psychiatry, 24, 815–826. 10.1007/s00787-014-0626-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Ragan J, & Randall P. (2004). Prospective relations between social support and depression: Differential direction of effects for parent and peer support? Journal of Abnormal Psychology, 113, 155–159. 10.1037/0021-843X.113.1.155 [DOI] [PubMed] [Google Scholar]
- Suanet B, Antonucci TC, & Carr D. (2016). Cohort differences in received social support in laterlife: The role of network type. Journals of Gerontology: Social Sciences, 00, 1–10. 10.1093/geronb/gbw075 [DOI] [PubMed] [Google Scholar]
- Takahashi K. (2005). Toward a life span theory of close relationships: The affective relationships model. Human Development, 48, 48–66. 10.1159/000083215 [DOI] [Google Scholar]
- Takahashi K, & Sakamoto A. (2000). Assessing social relationships in adolescents and adults: Constructing and validating the Affective Relationships Scale. International Journal of Behavioral Development, 24, 451–463. 10.1080/016502500750038008 [DOI] [Google Scholar]
- Taylor RJ, Chatters LM, Woodward AT, & Brown E. (2013). Racial and ethnic differences in extended family, friendship, fictive kin, and congregational informal support networks. Family Relations, 62, 609–624. 10.1111/fare.12030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tein J-Y, Coxe S, & Cham H. (2013). Statistical power to detect the correct number of classes in latent profile analysis. Structural Equation Modeling, 20, 640–657. 10.1080/10705511.2013.824781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teo AR, Choi HJ, & Valenstein M. (2013). Social relationships and depression: Ten-year follow-up from a nationally representative study. PLoS ONE, 8, 1–8. 10.1371/journal.pone.0062396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Twenge JM, & Nolen-Hoeksema S. (2002). Age, gender, race, socioeconomic status, and birth cohort differences on the Children’s Depression Inventory: A meta-analysis. Journal of Abnormal Psychology, 111, 578–588. 10.1037//0021-843X.111.4.578 [DOI] [PubMed] [Google Scholar]
- Ueno K. (2005). The effects of friendship networks on adolescent depressive symptoms. Social Science Research, 34, 484–510. 10.1016/j.ssresearch.2004.03.002 [DOI] [Google Scholar]
- Umberson D, & Montez JK (2010). Social Relationships and health: A flashpoint for health policy. Journal of Health and Social Behavior, 51, S54–S66. 10.1177/0022146510383501 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson MN (1989). Child development in the context of the Black extended family. American Psychologist, 44, 380–385. 10.1037/0003-066X.44.2.380 [DOI] [Google Scholar]
- Wrzus C, Hänel M, Wagner J, & Neyer FJ (2013). Social network changes and life events across the life span: A meta-analysis. Psychological Bulletin, 139, 53–80. 10.1037/a0028601 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.