

Abstract
Background
Ninety confirmed cases of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) have been reported to the World Health Organization. We report the details of a second family cluster of MERS-CoV infections from Riyadh, Saudi Arabia.
Methods
We present the clinical, laboratory and epidemiological details of 3 patients from a family cluster of MERS-CoV infections.
Results
The first patient developed respiratory symptoms and fever 14 days after admission to hospital for an unrelated reason. He died 11 days later with multi-organ failure. Two of his brothers presented later to another hospital with respiratory symptoms and fever. MERS-CoV infection in the latter 2 patients was confirmed by reverse transcriptase polymerase chain reaction testing. All 3 patients had fever, cough, shortness of breath, bilateral infiltrates on chest x-ray, thrombocytopenia, lymphopenia and rises in serum creatinine kinase and alanine transaminase. No hospital or other social contacts are known to have acquired the infection. It appears that the index patient in this cluster acquired MERS-CoV infection whilst in hospital from an unrecognized mild or asymptomatic case.
Conclusion
MERS-CoV acquisition from unrecognized mild or asymptomatic cases may be a more important contributor to ongoing transmission than previously appreciated.
Keywords: Middle East Respiratory Syndrome Coronavirus, MERS-CoV, Viral pneumonia, Cluster, Saudi Arabia
1. Introduction
A novel coronavirus causing severe respiratory infection was first described in September 2012.1 The virus, which later became known as Middle East Respiratory Syndrome Coronavirus (MERS-CoV), belongs to lineage C of the genus Betacoronavirus and is closely related to bat coronaviruses HKU4 and HKU5.2, 3 Though an animal reservoir is considered likely, none has been identified yet.4 The exact mechanism through which MERS-CoV infection is acquired remains uncertain. Up to 24 July 2013, a total of 90 confirmed cases of MERS-CoV infection have been reported to the World Health Organization (WHO), including 45 deaths. The majority of infections are sporadic. Human to human transmission has been documented in at least 3 hospital settings6, 7, 8 and 4 community clusters.9, 10, 11, 12 We report the clinical and epidemiological details of a second family cluster of two confirmed and one probable MERS-CoV infections in Riyadh, Saudi Arabia, occurred in February and March 2013. We hypothesize that the index case in the cluster is likely to have acquired the infection whilst in hospital from a contact with unrecognized MERS-CoV infection.
2. Case histories
Patient 1 was a 51-year old male with history of obesity and uncomplicated type II diabetes mellitus. He was admitted on 30 January 2013 thru the Emergency Department in Hospital A in Riyadh, Saudi Arabia, with a 2-month history of progressive back pain, lower limb weakness and urinary incontinence. There was no history of travel or recent contact with sick animals. Magnetic resonance imaging showed evidence of a paraspinal mass at the 4th lumbar vertebral level. Further investigations confirmed a diagnosis of multiple myeloma. He was transferred to a medical ward on 8 February 2013 for further management. On 13 February 2013, 14 days after hospital admission, he developed high fever, cough, shortness of breath and hypoxia requiring high flow oxygen via face mask. He commenced meropenem, vancomycin, voriconazole and oseltamivir. By the morning of 15 February 2013, his condition deteriorated with respiratory failure and progressive pulmonary infiltrates on chest x-ray. He was transferred to the intensive care unit (ICU) where he was intubated and put on mechanical ventilation. Renal failure ensued and continuous renal replacement therapy was started on 18 February 2013. Colistin and tigecycline were added on 20 February 2013. The patient's condition remained poor and he passed away on 24 February 2013, 11 days after the onset of his respiratory symptoms. Bacterial cultures of blood, urine and sputum were all negative.
Patient 2, a 39-year old brother of Patient 1 and Patient 2, became unwell on 24 February 2013 with fever, generalized fatigue, cough productive of bloody sputum and progressive shortness of breath. He had had no significant past medical history prior to this acute illness. He visited a private clinic on 27 February 2013 and was prescribed a course of oral cefuroxime without any improvement. He was admitted on 28 February to Hospital B in Riyadh, Saudi Arabia with hypoxia and extensive bilateral pulmonary infiltrates (Figure 1 ). He received vancomycin, piperacillin-tazobactam, azithromycin and oseltamivir, in addition to intravenous hydrocortisone and high flow oxygen by a face mask. Twenty-four hours later, he required endotracheal intubation and mechanical ventilation. The next day, vancomycin and piperacillin-tazobactam were substituted with linezolid and imipenem and his ventilation was switched to high frequency oscillatory mode. On 2 March 2013, continuing respiratory failure prompted a shift to extra-corporal membrane oxygenation. The patient's clinical condition failed to improve and he passed away 2 hours later, 7 days after the onset of symptoms. Cultures of blood, urine and sputum taken at the time of admission to hospital were all negative. Candida albicans was isolated from culture of sputum taken on 2 March 2013. Sputum smear microscopy for acid-fast bacilli and mycobacterial cultures were negative.
Figure 1.
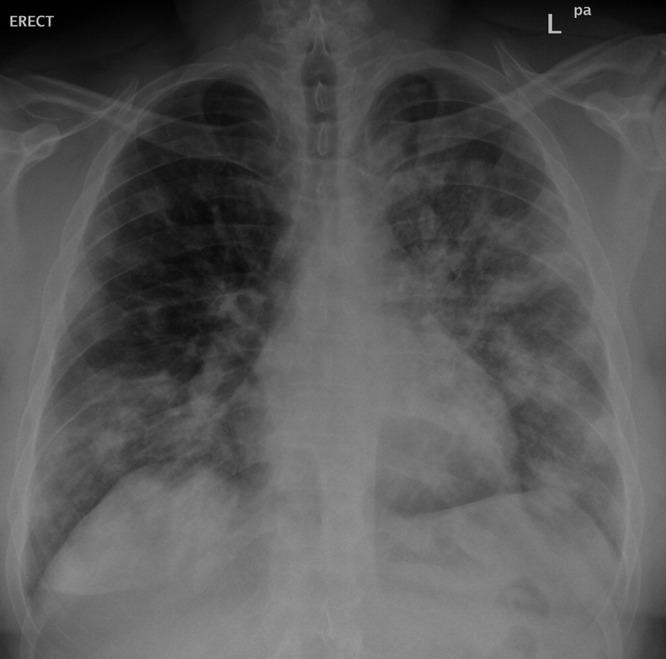
Chest radiograph from patient 2 with severe MERS-CoV pneumonia showing bilateral pulmonary infiltrates.
Patient 3, a 40-year old brother to patient 1 and 2, became ill on 2 March 2013. He was overweight but had no pre-existing chronic medical illness. He was admitted to Hospital B on 4 March 2013 with fever and cough productive of clear sputum. His initial chest x-ray was unremarkable. He received ceftriaxone, azithromycin and oseltamivir. A chest x-ray, taken 3 days later, showed focal areas of consolidation in the right middle and upper lobes. A computerized axial tomographic scan of the chest showed bilateral, peripheral air space consolidation with some degree of ground glass changes (Figure 2 ). His clinical course remained largely uncomplicated. He did not receive any corticosteroids, immune modulatory therapy or antivirals other than oseltamivir. Patient 3 was discharged from hospital alive and well on 11 March 2013. Cultures of respiratory tract samples, blood and urine were all negative. Sputum smear microscopy for acid-fast bacilli and mycobacterial cultures were also negative.
Figure 2.
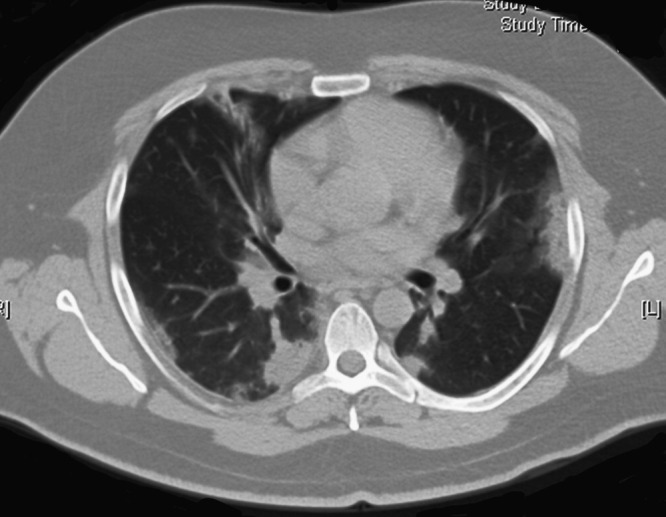
Computerized tomography scan from patient 3 with mild to moderate MERS-CoV infection showing bilateral peripheral air space consolidation.
Key clinical findings for the 3 patients are summarized in Table 1 . Figure 3 illustrates the clinical course and timelines for the 3 patients.
Table 1.
Clinical and investigational features of a family cluster of 3 patients with Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infections from Riyadh, Saudi Arabia and from previously reported cases.a
| Patient 1 | Patient 2 | Patient 3 | Data from previous MERS-CoV reportsb | |
|---|---|---|---|---|
| Fever | Yes | Yes | Yes | 30/33 (90.9%) |
| Cough | Yes | Yes | Yes | 30/33 (90.9%) |
| Dyspnea | Yes | Yes | Yes | 20/33 (60.6%) |
| Gastrointestinal symptoms | No | No | No | 12/33 (36.4%) |
| Chest x-ray infiltrates | Yes | Yes | Yes | 25/33 (75.8%) |
| Lymphopenia | Yes | Yes | Yes | 9/9 (100%) |
| Thrombocytopenia | Yes | Yes | Yes | 11/32 (34.4%) |
| Creatinine kinase rise | Yes | Yes | Yes | 2/2 (100%) |
| Alanine transaminase rise | Yes | Yes | Yes | 3/7 (42.9%) |
| Lactate dehydrogenase rise | Not available | Yes | Yes | 3/6 (50%) |
| Acute renal failure | Yes | Yes | No | 7/10 (70%) |
| ICUc admission | Yes | Yes | No | 26/33 (78.8%) |
| Mechanical ventilation | Yes | Yes | No | 26/33 (78.8%) |
Data collated from reports in which clinical details of patients with MERS-CoV infection were made available.1, 7, 8, 10, 19, 24, 27
Numerator indicates number of patients in whom a particular characteristic was present; denominator indicates the total number in which the presence or absence of the particular characteristic was reported.
ICU denotes intensive care unit.
Figure 3.

Clinical timelines for three patients with definite or probable Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infection.
3. Laboratory testing
Patient 1 had no samples tested for respiratory viruses or MERS-CoV. Nasopharyngeal swabs from Patient 2 and Patient 3 and a tracheal aspirate from Patient 2 were all negative by reverse transcriptase polymerase chain reaction (RT-PCR) for Influenza A virus RNA, Influenza B virus RNA, H1N1 Influenza virus RNA, Respiratory syncytial virus RNA, Adenovirus DNA, Rhinovirus RNA and seasonal Coronavirus RNA (HCoV 229, OC43, NL63). RT-PCR testing for MERS-CoV upE, ORF 1b and N genes was positive on upper and lower respiratory tract samples from Patient 2. Two upper respiratory tract samples from Patient 3 were negative; while a lower respiratory tract sample collected a day earlier was positive for MERS-CoV. All RT-PCR tests for MERS-CoV were performed at the Saudi Ministry of Health regional laboratory in Jeddah, and confirmed at the Public Health England, United Kingdom, Laboratories.13, 14
4. Contact investigation
All 3 patients lived in one large house in Urban Riyadh. There were 10 adults in the household; the mother, who had history of multiple medical problems including diabetes mellitus, hypertension, bronchial asthma and hypothyroidism, Patient 1 and his wife, 4 others sons (including Patient 2 and Patient 3), 2 daughters, and a female housemaid. Moreover, 4 married daughters and their spouses and children visited the family home frequently and often slept over too. The married couple shared one bedroom. Each of the other members of the household had his or her own bedroom. The men and women usually had their meals separately. Patients 2 and 3 are described as very close, spending most of their free time together. There were no domestic animals or birds in the family home, but bats had been noted in a small neglected park behind the house. Patient 1 had a farm outside Riyadh, in which he kept sheep, chicken, ducks and pigeons. He visited the farm once or twice a week. His last visit was 2 days prior to his admission to hospital. Patient 2 visited the farm occasionally. He also climbed palm trees in the house garden from time to time to pollinate the dates. None of the other family members frequented Patient 1's farm.
Patient 1 was initially admitted to a curtained-off bed in the Emergency Department where he stayed for 9 days. He was then transferred to a 2-bedded room in a medical ward where he stayed for 2 nights. A comatose patient, who had no visitors, occupied the second bed in the room. Patient 1 was moved once more to another 2-bedded room in the same ward. His roommate was discharged home 2 days later and the bed remained unoccupied for the remainder of the time that Patient 1 was in the room. Patient 2 and Patient 3 visited Patient 1 in the ward and in the ICU several time but usually did not stay for too long. Numerous friends, relatives and work colleagues visited Patient 1 while he was in the ward, before developing fever and respiratory symptoms. Patient 1's wife and 2 of his unaffected brothers spent especially long periods of time at his bedside throughout his hospital admission. All nursing and medical care for Patient 1 followed standard infection control precautions.
Influenza was suspected upon Patient 2's admission to Hospital B. He was transferred to a single room within 2 hours of his arrival and healthcare staff implemented contact and droplet infection control precautions throughout the patient's hospital stay.15 The patient's visitors were directed to do the same. On clinical deterioration, Patient 2 was transferred to the Resuscitation Bay in the main Emergency Department, where he was intubated in the presence of 5 healthcare workers (HCWs), all of whom wore surgical masks, gloves and full-length isolation gowns. Patient 2 was later transferred to a single room in the ICU, where droplet and contact precautions continued.
MERS-CoV infection was suspected upon Patient 3's presentation. He was thus admitted directly into a single room where all care was provided under strict contact and droplet infection control precautions.15
Nasopharyngeal swabs obtained from all household contacts of the patients were negative by RT-PCR for MERS-CoV infection. Moreover, all household contacts were followed daily for 14 days for presence of respiratory symptoms and none developed any. Serum samples were also obtained and stored pending the availability of validated serological assays. In the ensuing weeks, no HCWs in either hospital developed any symptoms to fulfill the surveillance requirement for MER-CoV testing.16 Patient 2 was overtly symptomatic during Patient 1's funeral. None of the dozens of mourners who attended the funeral is known to have developed a respiratory illness consistent with MERS-CoV infection.
5. Discussion
Patient 1's clinical course and subsequent microbiological confirmation of MERS-CoV infection in his brothers provide adequate basis for labeling his illness as probable MERS-CoV infection.17 The onset of his symptoms was 14 days after admission to hospital. He had spent 9 days in the Emergency Department before he was transferred to 2 different 2-bedded rooms. The upper end of MERS-CoV incubation period is thought to be around 14 days, with most patients having symptoms within the first week of contact.8, 18 It is therefore likely that Patient 1 acquired MERS-CoV infection during his hospitalization. This could have been from an asymptomatic HCW, one of the patients who were placed in close proximity to Patient 1 during his stay in the Emergency Department or from one of the numerous visitors he received whilst in the medical ward. In a previously described family cluster of MER-CoV infections, the index patient had a protracted clinical course including urinary tract infection and cardiac failure before respiratory infection became apparent.10 The authors suggest that in-hospital acquisition might be one explanation. Furthermore, in the largest human-to-human cluster of MERS-CoV infections described so far, one of the index cases was identified as a probable case based on his son's subsequent positive test.8 Unrecognized MERS-CoV infection in the community and in healthcare settings may be a more significant problem than previously appreciated.
The two family contacts of Patient 1 who went on to develop MERS-CoV infection had substantially less direct contact with him than other family members. It was suggested that higher viral shedding during the earlier phase of the clinical illness may result in higher infectiousness.19 In our report however, Patient 1's wife and two of his unaffected brothers were in regular close contact with him throughout his illness without ever taking any specific infection prevention precautions. They, as well as numerous other social and healthcare contacts, remained well. It continues to be unclear why some close contacts of individuals with MERS-CoV infection develop a clinical illness while others do not.
A large number of HCWs were in close contact with Patient 1 and Patient 2, some of which did not adhere strictly to appropriate infection control precautions. None of them was apparently infected. This is not dissimilar to the observations from four previous extensive public health investigations into cases of MERS-CoV infections. Out of over 400 HCWs who had been in contact with 31 patients in 4 different countries, only 2 had documented MERV-CoV infection.8, 9, 20, 21 Whether HCWs play a role in transmitting MERS-CoV through hand and surface contamination is an interesting but yet unproven hypothesis. Fourteen confirmed cases of asymptomatic MERS-CoV infection have so far been reported to the WHO, including 4 HCWs.22 Such asymptomatic carriage may explain some of the transmission that has taken place in hospital and in community settings. Furthermore, phylogenetic analyses of the available MERS-CoV genomes suggested a common ancestor halfway through the year 2011.8, 19 It appears that the virus circulated in the community for at least one year before the first clinical case was recognized.
The relatively low attack rate amongst social and HCW contacts in our report and in previous reports is reassuring but should not detract from continuing aggressive efforts to understand the pathogenesis of MERS-CoV. Two recent documented outbreaks illustrate the possible risks. Human to human transmission in 3 hospitals in eastern Saudi Arabia was responsible for 21 out of 23 MERS-CoV infections, of which at least 15 were fatal.8 Another outbreak in Jordan in April 2012 affected a total of 13 individuals, including 10 HCW.6, 23
The recommended contact and droplet precautions were implemented to a reasonable extent during the hospital care for all patients in our report.15 Reassuringly, this appears to have been effective in preventing nosocomial transmission of MERS-CoV. Previous studies showed that from the onset of illness, MERS-CoV was detectable by RT-PCR up to 14 days in lower airway samples, 13 days in urine and 16 days in stool.7, 19, 24 The importance of stringent infection control practice to interrupt any potential sustained MERS-CoV transmission can not be over stated.
MERS-CoV infection was fatal in 2 of the 3 patients described in our report. The high mortality rate associated with MERS-CoV infection increasingly appears to be due to the under-diagnosis of mild and asymptomatic cases as a result of the restrictive case definition put forward by WHO.16 All 3 patients in our report had fever, cough, shortness of breath, pulmonary infiltrates on chest x-rays, lymphopenia, thrombocytopenia and rises in serum creatinine kinase and alanine transaminase. All these are relatively common clinical features amongst patients with MERS-CoV infection (Table 1). Many of these were also seen in patients affected by Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) outbreak in 2003; however, the 2 diseases have distinctly different infectivity patterns.25 Although not necessarily diagnostic, the presence of these findings without an alternative explanation should prompt earlier consideration of MERS-CoV infection and initiation of appropriate investigations. It should be noted that collating data from small reports in order to understand the clinical features of an emergent infection has numerous self-evident limitations. A global, collaborative effort among clinicians and scientists studying this disease is needed to develop and identify more predictive diagnostic and prognostic markers.26
A number of knowledge gaps remain in relation to MERS-CoV infection. These include identification of its source and intermediate host and better understanding of the pathogenesis, infectivity and risk factors. Further work is also needed to optimize MERS-CoV diagnostic assays and to identify the most effective therapeutic interventions. The existing number of cases globally over the past 2 years is relatively small to address all these areas.
6. Conclusion
In-hospital transmission of MERS-CoV infection from undetected infection or asymptomatic carriage may be a larger contributor than previously appreciated. Early recognition of MERS-CoV infected patients and rigorous implementation of appropriate infection control measures are essential for effective control of the epidemic.
Conflict of interest statement: All authors have no financial or personal relationships with other people or organizations that could inappropriately influence this report. No funding was received from any source for this work.
Contributor Information
Ali S. Omrani, Email: asomrani@gmail.com.
Mohammad Abdul Matin, Email: mmatin64@yahoo.com.
Qais Haddad, Email: qaishaddad@yahoo.com.
Daifullah Al-Nakhli, Email: dralfardjh@gmail.com.
Ziad A. Memish, Email: zmemish@yahoo.com.
Ali M. Albarrak, Email: draalbarrak@yahoo.com.
References
- 1.Zaki A.M., van Boheemen S., Bestebroer T.M., Osterhaus A.D., Fouchier R.A. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367:1814–1820. doi: 10.1056/NEJMoa1211721. [DOI] [PubMed] [Google Scholar]
- 2.van Boheemen S., de Graaf M., Lauber C., Bestebroer T.M., Raj V.S., Zaki A.M. Genomic characterization of a newly discovered coronavirus associated with acute respiratory distress syndrome in humans. mBio. 2012;3 doi: 10.1128/mBio.00473-12. pii: e00473-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.de Groot R.J., Baker S.C., Baric R.S., Brown C.S., Drosten C., Enjuanes L. Middle East Respiratory Syndrome Coronavirus (MERS-CoV); Announcement of the Coronavirus Study Group. J Virol. 2013;87:7790–7792. doi: 10.1128/JVI.01244-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.World Health Organization. WHO guidelines for investigation of cases of human infection with Middle East Respiratory Syndrome Coronavirus (July 2013). (Accessed 12 July 2013, at http://www.who.int/csr/disease/coronavirus_infections/MERS_CoV_investigation_guideline_Jul13.pdf).
- 6.Hijawi B., Abdallat M., Sayaydeh A. Novel coronavirus infections in Jordan, April 2012: epidemiological findings from a retrospective investigation. East Mediterr Health J. 2013;19:S12–S18. [PubMed] [Google Scholar]
- 7.Guery B., Poissy J., El Mansouf L., Sejourne C., Ettahar N., Lemaire X. Clinical features and viral diagnosis of two cases of infection with Middle East Respiratory Syndrome Coronavirus: a report of nosocomial transmission. Lancet. 2013;381:2265–2272. doi: 10.1016/S0140-6736(13)60982-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Assiri A., McGeer A., Perl T.M., Price C.S., Al Rabeeah A.A., Cummings D.A.T. Hospital outbreak of Middle East Respiratory Syndrome Coronavirus. N Engl J Med. 2013 doi: 10.1056/NEJMoa1306742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Health Protection Agency UKNCIt Evidence of person-to-person transmission within a family cluster of novel coronavirus infections, United Kingdom, February 2013. Euro Surveill. 2013;18 doi: 10.2807/ese.18.11.20427-en. pii: 20427. [DOI] [PubMed] [Google Scholar]
- 10.Memish Z.A., Zumla A.I., Al-Hakeem R.F., Al-Rabeeah A.A., Stephens G.M. Family cluster of Middle East Respiratory Syndrome Coronavirus infections. N Engl J Med. 2013;368:2487–2494. doi: 10.1056/NEJMoa1303729. [DOI] [PubMed] [Google Scholar]
- 11.World Health Organization. MERS-CoV summary and literature update - 31 May 2013.(Accessed 12 July 2013, at http://www.who.int/csr/disease/coronavirus_infections/update_20130531/en/index.html.).
- 12.World Health Organization. Update: Middle East respiratory syndrome coronavirus (MERS-CoV) - 2 June 2013.(Accessed 12 July 2013, at http://www.who.int/csr/don/2013_06_02_ncov/en/index.html.).
- 13.Corman V.M., Eckerle I., Bleicker T., Zaki A., Landt O., Eschbach-Bludau M. Detection of a novel human coronavirus by real-time reverse-transcription polymerase chain reaction. Euro Surveill. 2012;17 doi: 10.2807/ese.17.39.20285-en. pii: 20285. [DOI] [PubMed] [Google Scholar]
- 14.Corman V.M., Muller M.A., Costabel U., Timm J., Binger T., Meyer B. Assays for laboratory confirmation of novel human coronavirus (hCoV-EMC) infections. Euro Surveill. 2012;17 doi: 10.2807/ese.17.49.20334-en. pii: 20334. [DOI] [PubMed] [Google Scholar]
- 15.World Health Organization. Infection prevention and control of epidemic- and pandemic-prone acute respiratory diseases in health care - WHO Interim Guidelines June 2007.(Accessed 12 July 2013, at http://apps.who.int/iris/bitstream/10665/69707/1/WHO_CDS_EPR_2007.6_eng.pdf.).
- 16.World Health Organization. Interim surveillance recommendations for human infection with novel coronavirus - 3 December 2012.(Accessed 12 July 2013, at http://www.who.int/csr/disease/coronavirus_infections/InterimRevisedSurveillanceRecommendations_nCoVinfection_03Dec12.pdf.).
- 17.World Health Organization. Revised interim case definition for reporting to WHO – Middle East respiratory syndrome coronavirus (MERS-CoV) - Interim case definition as of 03 July 2013.(Accessed 12 July 2013, at http://www.who.int/csr/disease/coronavirus_infections/case_definition/en/index.html.).
- 18.Centers for Disease Control and Prevention Update: Severe respiratory illness associated with Middle East Respiratory Syndrome Coronavirus - worldwide, 2012–2013. MMWR Morb Mortal Wkly Rep. 2013;62:480–483. [PMC free article] [PubMed] [Google Scholar]
- 19.Drosten C., Seilmaier M., Corman V.M., Hartmann W., Scheible G., Sack S. Clinical features and virological analysis of a case of Middle East respiratory syndrome coronavirus infection. Lancet Infect Dis. 2013 doi: 10.1016/S1473-3099(13)70154-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Buchholz U., Muller M.A., Nitsche A., Sanewski A., Wevering N., Bauer-Balci T. Contact investigation of a case of human novel coronavirus infection treated in a German hospital, October-November 2012. Euro Surveill. 2013;18 pii: 20406. [PubMed] [Google Scholar]
- 21.Mailles A., Blanckaert K., Chaud P., van der Werf S., Lina B., Caro V. First cases of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infections in France, investigations and implications for the prevention of human-to-human transmission, France, May 2013. Euro Surveill. 2013;18 pii: 20502. [PubMed] [Google Scholar]
- 22.World Health Organization. MERS-CoV summary and literature update as of 09 July 2013.(Accessed 12 July 2013, at http://www.who.int/csr/disease/coronavirus_infections/update_20130709/en/index.html.).
- 23.World Health Organization. Novel coronavirus summary and literature update as of 25 April 2013.(Accessed 12 July 2013, at http://www.who.int/csr/disease/coronavirus_infections/update_20130425/en/index.html.).
- 24.Bermingham A., Chand M.A., Brown C.S., Aarons E., Tong C., Langrish C. Severe respiratory illness caused by a novel coronavirus, in a patient transferred to the United Kingdom from the Middle East, September 2012. Euro Surveill. 2012;17 pii: 20290. [PubMed] [Google Scholar]
- 25.Lee N., Hui D., Wu A., Chan P., Cameron P., Joynt G.M. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1986–1994. doi: 10.1056/NEJMoa030685. [DOI] [PubMed] [Google Scholar]
- 26.Cauchemez S., Van Kerkhove M., Riley S., Donnelly C., Fraser C., Ferguson N. Transmission scenarios for Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and how to tell them apart. Euro Surveill. 2013;18 pii: 20503. [PMC free article] [PubMed] [Google Scholar]
- 27.Albarrak A.M., Stephens G.M., Hewson R., Memish Z.A. Recovery from severe novel coronavirus infection. Saudi Med J. 2012;33:1265–1269. [PubMed] [Google Scholar]