

Abstract
Background
The epidemic of hand, foot, and mouth disease (HFMD) has become a severe public health problem in the world and has also brought a high economic and health burden. Furthermore, the prevalence of HFMD varies significantly among different locations. However, there have been few investigations of the effects of socioeconomic factors and air pollution factors on the incidence of HFMD.
Methods
This study collected data on HFMD in Shenzhen, China, from 2012 to 2015. We selected eleven factors as potential risk factors for HFMD. A Bayesian spatiotemporal model was used to quantify the influence of the factors on HFMD and to identify the relative risks in different districts.
Results
The risk factors of HFMD were the population, population density, concentration of SO2, and concentration of NO2. The relative risks (RRs) were 1.00473 (95% CI: 1.00059–1.00761), 1.00010 (95% CI: 1.00002–1.00016), 1.00215 (95% CI: 1.00170–1.00232) and 1.00058 (95% CI: 1.00028–1.00078), respectively. The protective factors against HFMD were the per capita GDP, the number of public kindergartens, the concentration of PM10, and the concentration of O3. The RRs were 0.98840 (95% CI: 0.98660–0.99026), 0.97686 (95% CI: 0.96946–0.98403), 0.99108 (95% CI: 0.98551–0.99840) and 0.99587 (95% CI: 0.99534–0.99610), respectively. The risk of incidence in Longgang district and Pingshan district decreased, while the risk of incidence in Baoan district increased.
Conclusions
Studies have confirmed that socioeconomic factors and air pollution factors have an impact on the incidence of HFMD in Shenzhen, China. The results will be of great practical significance to local authorities, which is conducive to accurate prevention and can be used to formulate HFMD early warning systems.
Author summary
This study used Bayesian spatiotemporal modelling to analyze the factors that influence the incidence of hand, foot, and mouth disease (HFMD)in Shenzhen, including socioeconomic factors and air pollution factors. A total of 171,210 HFMD cases and socioeconomic and air pollution data from 2012–2015 were included in the analysis. Studies have confirmed that socioeconomic factors and air pollution factors affect the risk of HFMD in Shenzhen, China. By testing the optimal model, the relative risk map of each area was drawn to identify the high-risk areas of HFMD and the future trends of the disease. The results will be of great practical significance to local authorities, which is conducive to accurate prevention and can be used to formulate targeted disease intervention measures.
Introduction
Hand, foot and mouth disease (HFMD) is a common viral disease in infants and children under 5 years of age. This infection is caused by polio-enterovirus infection. Coxsackievirus A16 (Cox A16) and Enterovirus 71 (EV 71) are the most common etiologic agents [1,2]. The specific clinical manifestations of HFMD include oral pain, anorexia, and fever, and the hands, feet, mouth or other areas of the body will appear to have small sores or ulcers [3]. Usually, HFMD can heal itself, and some patients can heal without medication within about a week. Therefore, its clinical burden and health hazards are often neglected.
There have been millions of cases of HFMD around the world, and it formed a large-scale epidemic on a global scale [4–10]. The study also showed that the average cost (USD) of outpatients with mild infections, inpatients with mild infections, severe cases and fatal cases of HFMD were $201 (95% CI $187, $215), $1072 (95% CI $999, $1144), $3051 (95% CI $2905, $3197) and $2819 (95% CI $2068, $3571), respectively [11]. Therefore, HFMD epidemics has become a serious public health problem and has also brought a high economic and health burden.
The incidence of HFMD in all age groups in mainland China from 2009 to 2014 were 86.59/100000, 132.35/100000, 120.21/100000, 160.17/100000, 134.37/100000, and 203.16/100000, respectively [12]. According to the communicable disease surveillance system of Guangdong Province, China, the numbers of reported cases of HFMD from 2008 to 2013 were 48917, 93067, 226622, 274006, 330621 and 358068, respectively [13].
Although the first EV-A71 vaccine was already on the market in China, this vaccine could not protect against other novel emerging etiologies of HFMD. Hence, there is no general vaccine available for HFMD [14,15]. Therefore, identifying its influencing factors and working toward early warning and timely prevention are still the keys to reducing the severity of the incidence of HFMD [16].
Research over the past decade has repeatedly verified the association between HFMD epidemics and climatic factors [17]. However, due to rapid urbanization and climate change in recent years, severe and sustained air pollution has also led to an increase in morbidity and mortality [18–20]. In the past, research on the adverse health effects of air pollution has focused on the relationship between air pollution and chronic noncommunicable diseases [21,22]. However, recent studies have shown that air pollution may affect the incidence of infectious diseases [23–26]. The adhesion of the virus to gaseous particulate matter and the dissolution of substances such as NO2 in the respiratory tract may promote the occurrence of infectious diseases [22]. Enteroviruses attached to environmental particles can be transported longer distances under favorable weather conditions [27]. However, there have been few studies of the relationship between air pollution and HFMD thus far. Understanding the influence of air pollution factors, social factors and their combined effects on HFMD will help the relevant departments formulate more accurate and practical preventive measures.
In the past, most studies have used time-series models (SIR, ARIMA) to estimate the impacts of variables [28–30]. In recent years, since the discovery that logistic regression cannot explain spatial heterogeneity and spatial correlation well, it is recommended that the Bayesian spatiotemporal model be used to identify spatiotemporal variations and the effects of potential predictors [31–33]. The method uses Markov chain Monte Carlo simulation to estimate the posterior distribution of random variables and to identify the relative risks in different districts. As a result, the relevant departments can adequately implement preventive measures in high-risk areas, reduce the harm of HFMD and protect public health.
We aimed to quantify the influence of factors on HFMD and to discuss the possibility of improving the early predicted warning system in Shenzhen by using the Bayesian spatiotemporal model in this study.
Methods
Ethics statement
Not applicable. The Ethics Committee of Shantou University Medical College declared that this study did not require ethics approval.
Data collection
Study area
Shenzhen (Fig 1) is located in the southern part of Guangdong Province and includes 10 administrative districts (Yantian, Luohu, Futian, Nanshan, Dapeng, Longhua, Longgang, Pingshan, Baoan, and Guangming). It is the central city in China’s economy, and its total economy ranks third in mainland China. Moreover, Shenzhen city, as an immigrant metropolis connecting China and Hong Kong, has a high population density and strong liquidity. These characteristics have also led to a high incidence of HFMD in Shenzhen over the years that is four times the national average [34].
Fig 1. Shenzhen city and its location in Guangdong province.

This figure was generated using ArcGIS Geographic Information Systems software version 10.2 (ESRI, USA).
Yantian, Luohu, Futian, and Nanshan are the economic core areas of Shenzhen and are the former Shenzhen special economic zones. Yantian, Luohu and Futian are also on the border with Hong Kong, which is a transport hub for Shenzhen and Hong Kong. The remaining six districts (Dapeng, Longhua, Longgang, Pingshan, Baoan, and Guangming) have been developed in the past 20 years and have large populations, but the economic level is lower than those of the other 4 districts (Yantian, Luohu, Futian, and Nanshan).
Surveillance data of HFMD
Case-based HFMD surveillance data from 2012 to 2015 were obtained from the Shenzhen Center for Disease Control and Prevention (Shenzhen CDC). The clinical criteria for the diagnosis of HFMD were provided by a guidebook published by the Ministry of Health of China in 2009 [35]. Since May 2, 2008, HFMD has been included in the class C infectious diseases. When patients are diagnosed with HFMD, all kinds of medical institutions are required to register the cases on the Notifiable Infectious Diseases Reporting Information System (NIDRIS) within 24 hours of diagnosis. The reports include the patient information, including name, age, gender, address, symptoms, and date of onset.
HFMD is a kind of infectious disease that legally must be reported. The Shenzhen Center for Disease Control and Prevention organize an investigation into underreporting by medical institutions every year [36]. In addition, the outpatient log and the hospital records of the medical institutions in Shenzhen basically implement electronic data collection [37]. It is also beneficial to the self-investigation of medical institutions and the integrity of the collection of HFMD information. Therefore, the data source of this study is accurate and reliable.
Potential predictor data
Previous studies have confirmed the relationship between demographic factors, socioeconomic factors, air pollution factors and the risk of HFMD [19,24,26,29,38]. Some studies have also established models to predict the incidence of HFMD through these factors [19,29,38,39]. However, at present, no model uses the above factors to predict the incidence of HFMD. The more comprehensive the influencing factors considered in the model, the more accurate the prediction effect will be.
The average concentration of SO2, the average concentration of NO2, the average concentration of PM10, and the average concentration of O3 were obtained from the Shenzhen environmental protection station, and no data were missing for the study period.
The “Shenzhen Yearbook” collects substantial social and economic information, including the population, geographical area, GDP (gross domestic product), and number of kindergartens. The population density is calculated by the population and area. The per capita GDP is calculated by the population and GDP.
The ESRI ArcGIS software (U.S. Environmental Systems Institute) was used to plot the spatial distribution of the data.
Incidence rate standardization
Because the populations of each district in Shenzhen were different from 2012 to 2015, it was necessary to standardize the annual incidence of each district. Finally, the average value was used as an index to evaluate the incidence of disease in each district for 4 years. The average incidence rate (p) in Shenzhen city from 2012 to 2015 was used as the standard;
The expected number of cases were calculated as follows: p *ni,k (ni,k represents the corresponding population, where index i represents the different districts, and index k represents the different years);
The standardized rate was calculated as follows: (Pi,k / p *ni,k)* (ni,k /Nk), where Pi,k represents the actual number of cases and Nk represents the population of Shenzhen.
The average value of each district was calculated over the 4 years.
Identification of risk variables
To assess the multicollinearity between the independent variables and select the variables that were included in the model, we used R software version 3.4.4 to calculate the variance inflation factor (VIF) between the variables.
Statistical analysis
The HFMD cases (Oi,k) for the i-th district were assumed to have a Poisson distribution with mean μi,k · (i = 1,2,…,10; k = 1,2,…,4). Index i represents the different district (space), and index k represents the different years (time):
| (1) |
and
| (2) |
where Ei,k is the expected cases in the i-th district and θi,k is the mean log relative risk (RR), which is as follows:
| (3) |
which is modeled as follows:
| (4) |
| (5) |
Formula (4) is the spatiotemporal effect estimation model, where α is the intercept, Ui represents the spatially unstructured random effect, and Si represents the spatially structured random effect. The prior distribution of the spatial structure effects was a conditional autoregressive process, considering the adjacent relationship (i.e., the incidence risk of HFMD in the adjacent area was more closely related, and the adjacency matrix W is an N × N-order matrix (N is the number of districts)). The value wij on the diagonal is 0. If district i and district j have a common boundary, wij is 1 and is 0 if they do not have a common boundary. Gk represents the temporal random effect, and . Tk represents the time-structured random effect, which was assumed to follow a 1-order random walk. δi,k represents the spatiotemporal interaction term.
Formula (5) is the model to which the explanatory variable was added, where Xi,k,j is the value of the variable j in the k-th year of the i-th district; βj is the regression coefficient corresponding to the variable j; ψi,k represents the random effect; and .
The explanatory variables selected in this study were mainly selected by reading the relevant literature [18–20,29,38] and combining that knowledge with the actual available data, including 11 variables such as the population, population density, GDP, per capita GDP, number of kindergartens, number of public kindergartens, number of private kindergartens, concentration of SO2, concentration of NO2, concentration of PM10, and concentration of O3.
We used the OpenBUGS software version 3.2.3 (MRC, UK, 2015) to develop a Poisson regression model under the region-level Bayesian framework to assess the spatial sociological effects of HFMD in Shenzhen city. The basic principle was to use Gibbs sampling to sample from the complete conditional probability distribution to generate the Markov chain. Then, through iteration, the model parameters were finally estimated. After running 1000 iterations of this experiment as the burn-in, a total of 15,000 iterations were run. To obtain a steady distribution, the convergence was evaluated by examining the trace plot of the samples for each chain. The deviance information criterion (DIC) values were used to compare the pros and cons of the different models and select the optimal model. The smaller the DIC value was, the better the goodness of fit of the model.
Finally, based on the determined optimal model, we used GeoBUGS software 1.2 to map the relative risk of HFMD for different districts in Shenzhen city. GeoBUGS is an add-on to OpenBUGS that fits spatial models and produces a range of maps as outputs.
Results
Descriptive statistics
A total of 171210 laboratory or clinically confirmed cases of HFMD in Shenzhen were reported from 2012 to 2015. There were 103802 male patients (60.63%) and 67408 female patients (39.37%). The main incidence group was the 1-year-old group (59096 cases; 34.52%), followed by the 2-year-old group (31042 cases; 18.13%). The median age was 2 years old, and the interquartile range was 1–3 years old. The specific age groups and sex distribution characteristics are shown in Table 1 and Fig 2A. The annual average incidences from 2012 to 2015 were 334.07/100000, 333.97/100000, 446.77/100000, 439.33/100000, respectively. A descriptive summary of the socioeconomic and air pollution variables is shown in Table 2. Fig 3 shows the variation in the pollutants over the 4-year period. In addition to the peak concentration of ozone in October, the peak concentrations of SO2, NO2 and PM10 were mainly during the winter from December to January. In the high incidence period of HFMD (May to July), they maintained a low concentration or showed a downward trend.
Table 1. Descriptive statistics of the basic characteristics of the HFMD cases [n (%)].
| <1-year-old | 1-year-old | 2-year-old | 3-year-old | 4-year-old | 5-year-old | >5-year-old | Total | |
|---|---|---|---|---|---|---|---|---|
| Male | 15267(8.9) | 35225(20.6) | 18660(10.9) | 15471(9.0) | 9182(5.4) | 4485(2.6) | 5512(3.2) | 103802(60.6) |
| Female | 9948(5.8) | 23817(13.9) | 12382(7.2) | 9735(5.7) | 5378(3.1) | 2625(1.5) | 3469(2.0) | 67408(39.4) |
| Total | 25215(14.7) | 59096(34.5) | 31042(18.1) | 25206(14.7) | 14560(8.5) | 7110(4.2) | 8981(5.3) | 171210(100) |
*<1: A child who is less than 1 year of age; >5: A child who is greater than 5 years of age
Fig 2. The statistical graph of the reported HFMD cases in Shenzhen, from 2012 to 2015.
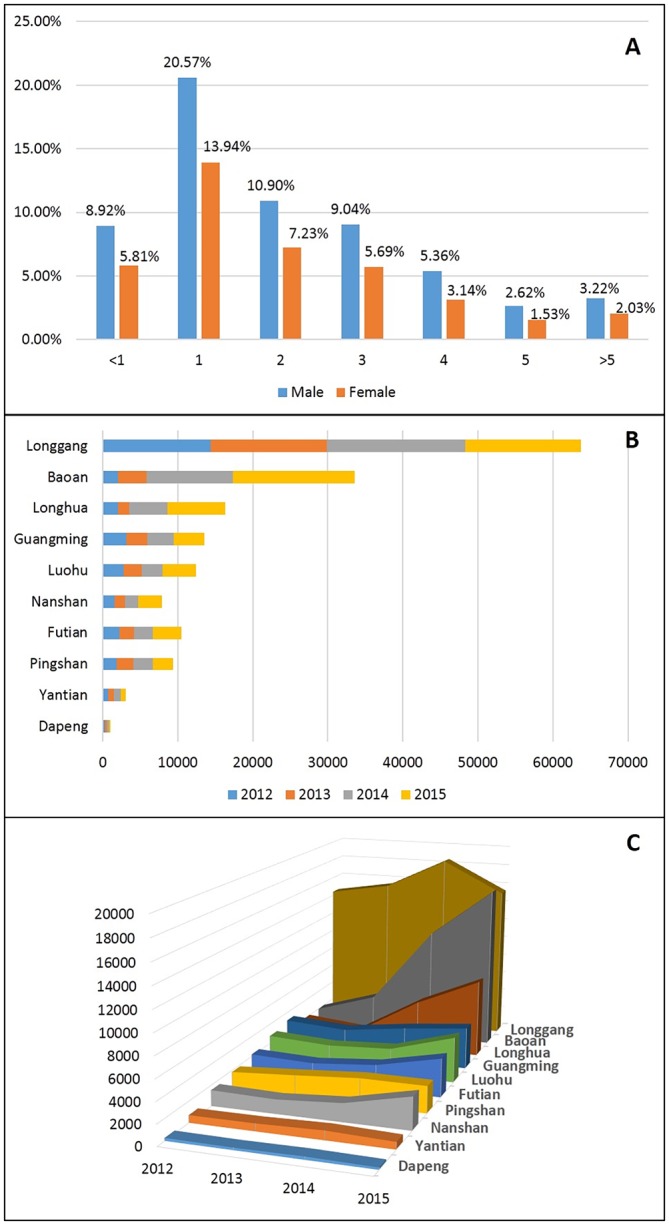
The characteristics distribution of age groups and sex, from 2012 to 2015(Fig.2.A). The distribution of the number of cases of each district from 2012 to 2015(Fig.2.B). The trends in the number of cases of each district from 2012 to 2015(Fig.2.C).
Table 2. Descriptive statistics of the socioeconomic and air pollution variables.
| Variables | Minimum | 2.5% Percentile | Median | 97.5% Percentile | Maximum |
|---|---|---|---|---|---|
| Population (100,000)(P) | 1.31 | 3.23 | 10.42 | 14.39 | 28.63 |
| Population Density (1000 person/ km2)(D) | 0.44 | 2.87 | 5.63 | 8.15 | 18.31 |
| GDP (¥10 billion)(G) | 2.45 | 4.56 | 15.62 | 26.38 | 37.16 |
| Per Capita GDP (¥10,000)(PCG) | 7.52 | 11.13 | 15.16 | 20.39 | 30.50 |
| Number of Kindergartens (per 10 kindergartens)(C) | 1.10 | 4.00 | 14.45 | 18.33 | 35.80 |
| Number of Public Kindergartens (C1) | 1.00 | 2.00 | 4.00 | 9.00 | 18.00 |
| Number of Private Kindergartens (per 10 kindergartens)(C2) | 0.8 | 3.32 | 12.65 | 17.73 | 35.10 |
| SO2 (mg/m3) | 5.94 | 8.44 | 8.91 | 12.15 | 17.92 |
| NO2 (mg/m3) | 30.62 | 33.35 | 41.78 | 46.37 | 60.61 |
| PM10 (mg/m3) | 45.89 | 47.32 | 55.50 | 59.62 | 76.51 |
| O3 (mg/m3) | 40.48 | 54.69 | 61.37 | 78.91 | 79.58 |
Fig 3. The variation of the pollutant over the 4 years, from 2012 to 2015.

Spatiotemporal statistical analysis
This study selected data on the incidence of HFMD in 10 districts of Shenzhen from 2012 to 2015. The districts were Baoan, Nanshan, Longhua, Guangming, Longgang, Futian, Luohu, Yantian, Pingshan and Dapeng.
Through statistical analysis, a statistical graph of the annual number of cases was created (Fig 2). The overall number of cases of HFMD in Shenzhen showed a significant upward trend. As shown in Fig 2B, Longgang district had the largest number of cases, followed by Baoan district, and Dapeng district had the fewest cases. In addition, as shown in Fig 2C, the number of cases in Baoan district and Longhua district increased sharply from 2013–2015, while the number of cases in Longgang district peaked in 2014 but declined in 2015.
Due to the significant differences in the numbers of cases of HFMD and the populations in different areas, to spatially describe the areas with a higher risk of HFMD, we made a gradient diagram of the average incidence of HFMD in the various districts of Shenzhen (the number of cases of HFMD per 100000 people). Fig 4 shows the spatial distribution of the standardized incidence rates of HFMD in Shenzhen. The spatial distribution of the disease was mainly concentrated in northeastern Shenzhen city. According to the comparison of the standardized incidence rate of each region, the incidence rate of Longgang district was the highest, followed by Pingshan district and Guangming district.
Fig 4. The Spatial distribution of standardized incidence rates of HFMD in each region in Shenzhen, from 2012 to 2015.

This figure was generated using ArcGIS Geographic Information Systems software version 10.2 (ESRI, USA).
Spatiotemporal trend analysis
We use the spatiotemporal effect estimation model (without explanatory variables) to estimate the risk of HFMD in various districts in Shenzhen and map the relative risk (RR), as shown in Fig 5. Compared with the direct use of the incidence of HFMD in each district, the Bayesian spatiotemporal model considered the proximity information, and its estimation results were more representative. It can be seen from Fig 5 that the relative risk (RR) value of Yantian district was the highest when only considering the spatiotemporal effects, and the areas with higher relative risk were mainly concentrated in the eastern part, while the risk in the western region was relatively low.
Fig 5. The spatial distribution of relative risk (only spatio-temporal effect) of HFMD in each region in Shenzhen.

This figure was generated using ArcGIS Geographic Information Systems software version 10.2 (ESRI, USA).
Analysis of influencing factors
Due to the multicollinearity between the variables, multicollinearity analysis was used to calculate the variance inflation factor (VIF) between the 11 initial variables, and the variables with serious collinearity were excluded. It can be seen from Table 3 that the number of kindergartens (C) showed serious collinearity and were excluded from the model, so we cannot calculate its VIF value. Since the multicollinearity analysis only examined the integral correlation between the explanatory variables, the results were only used as a preliminary reference for the screening variables. The Bayesian model univariate regression results (Table 4) should be further selected as the criterion for selecting explanatory variables.
Table 3. Multicollinearity evaluation results (VIF: Variance inflation factor).
| Variables | VIF | Variables | VIF |
|---|---|---|---|
| Population (100,000)(P) | 11.45 | Number of public kindergartens (C1) | 5.87 |
| Population Density (1000 Person/ km2)(D) | 5.42 | SO2 (mg/m3) | 1.91 |
| GDP (¥10 billion)(G) | 1.58 | NO2 (mg/m3) | 4.89 |
| Per capita GDP (¥10,000)(PCG) | 2.04 | PM10 (mg/m3) | 7.57 |
| Number of private kindergartens (per 10 kindergartens)(C2) | 9.67 | O3 (mg/m3) | 2.35 |
*The number of kindergartens (C) showed serious collinearity and was excluded by the model.
Table 4. The regression coefficients of the univariate Bayesian models with respect to the different factor variables.
| Variables | RR | 95% CI |
|---|---|---|
| Population (100,000)(P) | 0.98969 | (0.98408,0.99835) |
| Population Density (1000 person/ km2)(D) | 0.96027 | (0.94960,0.97204) |
| GDP (¥10 billion)(G) | 0.98040 | (0.97638,0.98639) |
| Per capita GDP (¥10,000)(PCG) | 0.97290 | (0.96381,0.98340) |
| Number of Private Kindergartens (per 10 kindergartens)(C2) | 1.01265 | (1.00966,1.01922) |
| Number of Public Kindergartens (C1) | 0.94763 | (0.93995,0.96956) |
| SO2 (mg/m3) | 0.95988 | (0.94598,0.98719) |
| NO2 (mg/m3) | 0.99264 | (0.98764,0.99569) |
| PM10 (mg/m3) | 0.99308 | (0.98980,0.99644) |
| O3 (mg/m3) | 0.99779 | (0.99684,0.99956) |
As seen from Table 4, during the period from 2012–2015, the factors related to the risk of HFMD included the population, population density, GDP, per capita GDP, number of private kindergartens, number of public kindergartens, concentration of SO2, concentration of NO2, concentration of PM10, and concentration of O3. We input the 10 variables that were meaningful according to the univariate Bayesian model analysis into the model for the next multivariate analysis. The DIC value of the model was 234.2. The smaller the value of DIC is, the better the goodness of fit of the model. The results of the multivariate analysis are shown in Table 5.
Table 5. Results of the regression coefficients for the multivariate Bayesian models with respect to the seven factor variables.
| Variables | RR | 95% CI |
|---|---|---|
| Population (100,000)(P) | 1.00473 | (1.00059,1.00761) |
| Population Density (1000 person/ km2)(D) | 1.00010 | (1.00002,1.00016) |
| GDP (¥10 billion)(G) | 0.99897 | (0.99662,1.00084) |
| Per Capita GDP (¥10,000)(PCG) | 0.98840 | (0.98660,0.99026) |
| Number of Private Kindergartens (per 10 kindergartens)(C2) | 0.99998 | (0.99995,1.00003) |
| Number of Public Kindergartens (C1) | 0.97686 | (0.96946,0.98403) |
| SO2 (mg/m3) | 1.00215 | (1.00170,1.00232) |
| NO2 (mg/m3) | 1.00058 | (1.00028,1.00078) |
| PM10 (mg/m3) | 0.99108 | (0.98551,0.99840) |
| O3 (mg/m3) | 0.99587 | (0.99534,0.99619) |
From 2012–2015, the relative risk factors of HFMD were as follows: population, population density, per capita GDP, number of public kindergartens, concentration of SO2, concentration of NO2, concentration of PM10, and concentration of O3. GDP and the number of private kindergartens had no significant effect on the risk of HFMD. The population, population density, concentration of SO2 and concentration of NO2 were positively correlated with the risk of HFMD. The relative risks were 1.00473 (95% CI: 1.00059–1.00761), 1.00010 (95% CI: 1.00002–1.00016), 1.00215 (95% CI: 1.00170–1.00232) and 1.00058 (95% CI: 1.00028–1.00078), respectively. The per capita GDP, number of public kindergartens, concentration of PM10 and concentration of O3 were negatively correlated with the risk of HFMD. The relative risks were 0.98840 (95% CI: 0.98660–0.99026), 0.97686 (95% CI: 0.96946–0.98403), 0.99108 (95% CI: 0.98551–0.99840) and 0.99587 (95% CI: 0.99534–0.99610), respectively.
Finally, we calculated the relative risk of HFMD in the various regions of Shenzhen and plotted the relative risk map, which is shown in Fig 6. Yantian district had the highest relative risk, which meant that the risk of incidence in Yantian district was the highest, followed by Baoan district.
Fig 6. The Spatial distribution of relative risk (added explanatory variables) of HFMD in each region in Shenzhen.

This figure was generated using ArcGIS Geographic Information Systems software version 10.2 (ESRI, USA).
The variation between Figs 4 and 6 shows that the model was gradually optimized or the prediction accuracy was improved. In Fig 4, we hope to judge the future incidence trends by comparing the average incidences of each district of Shenzhen from 2012–2015. However, such a prediction was not sufficiently accurate. Therefore, we considered the effects of the spatiotemporal interactions of the disease (Fig 5). Fig 5 showed slight changes in the tendency of the disease and high-risk areas compared to Fig 4. In Fig 6, we not only retained the spatiotemporal interaction effect but also added the effects of the influencing factors.
To demonstrate the validity of the model, we obtained the RR values (RRik) for each area of each year through the model. Then, we made the point diagram of the RR values (RRik) of each region over the four years (2012–2015) to reflect the change during the time scale. On this basis, the fitting trend line of each region was increased (the goodness of fit R2 was more than 0.8), and the RR values of each region in 2016 were estimated. Finally, the ranking of the RR values were compared with the ranking of the incidence of each region in 2016.
In 2016, the top five high-incidence areas in Shenzhen were Guangming, Baoan, Longhua, Pingshan and Longgang, which had incidence rates of 492.70/100000, 426.12/100000, 415.88/100000, 367.31/100000, 323.28/1000000, respectively. The top five high-RR values areas were Yantian, Baoan, Guangming, Pingshan and Longgang, which had values of 5.28, 4.62, 3.59, 3.76 and 3.27, respectively. Although there were minor differences in the individual values, the basic order of the first five was consistent.
Discussion
As a highly developed first-tier city in China, Shenzhen is also a hub linking mainland China and Hong Kong. The city belongs to the subtropical climate region, and it is highly populated, highly mobile, and crowded from housing and traffic and has a shrinking living space. These characteristics cause Shenzhen to have a high frequency of infectious diseases, such as HFMD [40–43]. This study included 171,210 cases of HFMD in Shenzhen from 2012 to 2015. The Bayesian spatiotemporal model was used to analyze the factors that influenced the incidence of HFMD in Shenzhen, including the population factors (population and population density), economic factors (GDP and GDP per capita), educational resource factors (public, private and total numbers of kindergartens), and environmental pollution factors (the concentrations of SO2, NO2, PM10, and O3). By testing the optimal model, the relative risk map of each district was drawn to predict the high-risk areas of HFMD and the future trend of the disease in Shenzhen.
The results of the study indicated that the population and the population density were positively correlated with the risk of HFMD. HFMD is an infectious disease, and an increase in population size or population density may increase the risk of disease transmission, which is consistent with national research results [29]. The per capita GDP was negatively correlated with the risk of HFMD. This may be because Shenzhen’s overall economic level is good. In general, the children living in areas with social and economic benefits were less likely to be infected with HFMD due to the availability of local health care and better sanitation [29,38].
In China, children in kindergarten are usually aged 3–6, and this age group is most vulnerable to HFMD. Although the number of private kindergartens was not related to the incidence of HFMD, the number of public kindergartens was negatively correlated with the incidence of HFMD. At present, as far as Guangdong Province is concerned, public kindergartens generally have stronger financial support and more standardized management systems. Therefore, in general, the sanitary environment of public kindergartens is better, leading to a decreased risk of disease transmission [44,45].
The study found that SO2 increased the risk of HFMD, with an RR of 1.00215 (95% CI: 1.00170–1.00232). However, we still do not know the exact mechanism by which exposure to SO2 increases the risk of HFMD in children. However, from a biological point of view, HFMD can be transmitted through the respiratory tract, and SO2 also has a strong stimulating effect on the respiratory mucosa, which can induce oxidative stress and systemic inflammation or increase the permeability of the solute [18,46]. This increases the susceptibility of children to HFMD. The study also found that NO2 increased the risk of HFMD, which was consistent with the results of another Shenzhen air pollution study [47]. Although no laboratory studies were found on the direct effect of NO2 on enterovirus, it has been confirmed that the NO2 concentration was positively correlated with the incidence of rotavirus [48]. Another study also confirmed that NO2 may have direct effects on epithelial cells, cause systemic inflammation and immune activation and modulate the intestinal microbiota [49].
The study also found that high concentrations of ozone play a protective role. At present, research on the relationship between ozone concentration and infectious diseases is still limited. Although some of the basic mechanisms of action of ozone in pulmonary toxicology and in medicine have been clarified, and the absolute view of ozone toxicity (that ozone is toxic and harmful to humans) is incorrect [50–53]. To judge its toxicity, it is necessary to consider the exposure dose, molecular structure and the susceptibility of individuals to exposure at the same time. At present, some studies have been based either on lungs or on studies performed in artificial environments that do not correspond to the real antioxidant capacity of the body compartments [50]. Ozone doses that are well calibrated against the potent antioxidant capacity of blood can trigger several useful biochemical mechanisms and reactivate the antioxidant system [51]. Ozone may inhibit the ability of viruses to survive or replicate in the external environment, affecting the spread of HFMD [54]. Studies have also confirmed that appropriate ozone concentrations limit the production of viruses, prolong the survival time of cells, and inhibit the production of the cytokines related to EV 71 infection [55].
In addition, the study found that the concentration of PM10 was inversely related to the risk of HFMD, and this result was consistent with the research results of the relationship between PM10 and HFMD in Yuexiu district from 2010 to 2011 [56]. At present, the exact mechanism of the relationship between exposure to PM10 and the risk of HFMD in children is still unknown. However, studies in Nanjing, Beijing, and Guangzhou have shown that public perception and acceptable risk levels of air pollution can prompt individual behavioral changes (risk reduction behaviors) [57–61]. When the haze weather is severe or the AQI (air quality index) is large, the public might reduce the number of outings, wear masks when going out, use air purifiers, reduce the number of open windows, and increase the frequency of cleaning mouths and noses. These behaviors reduce exposure to environmental pollution, thus reducing the risk of HFMD [57,62]. More studies have confirmed that families with children, in particular, are more likely to engage in these risk reduction behaviors [57,60]. In addition, the negative correlation with PM10 may also be related to the special geographical environment of Shenzhen. Shenzhen is located between 113°46’-114°37’ east longitude and 22°27’-22° north latitude. It is close to the sea, has a warm climate, and is humid and rainy. Warm and humid sea breezes are very beneficial to the diffusion and deposition of pollutants [63].
This study is the first a Bayesian spatiotemporal model has been used to analyze the impact of socioeconomic factors and air pollution factors on the risk of HFMD from urban spatial dimensions. Second, this study established a more mature Bayesian spatiotemporal prediction model for HFMD that can calculate the risk of HFMD in each area, to identify high-risk areas. However, these high-risk areas are not fixed, and as long as the original data are updated, the relative risk of each district will be updated, resulting in changes in the high-risk areas. However, for the predicted high-risk areas, we can implement preventive measures in a timely manner to reduce the harm of the disease. Therefore, early discovery, early prevention and effective protection of children’s health are needed.
The risk of disease in Yantian district was the largest when only the spatiotemporal effects were analyzed. In Fig 4, from the spatial scale, we can see that the high-risk areas from 2012 to 2015 were mainly concentrated in northern Shenzhen (Longgang district, Pingshan district). The risks of disease in Longgang district and Pingshan district decreased, while the risk of disease in Baoan district increased.
There were some limitations to our research. First, some patients have mild symptoms and do not go to the hospital for treatment. Our reporting system does not record such self-treating individuals, so the incidence may be underestimated. The use of clinical diagnosis rather than laboratory diagnosis in most cases is another source of reporting bias. Second, only 4 years of data were analyzed in this study, and there was a certain degree of collinearity between the variables, both of which may reduce the stability of the model. Third, the purpose of this study was to explore the relationship among the socioeconomic factors, the air pollution factors and the incidence of HFMD, which cannot be used as evidence to judge a causal relationship. Further studies are needed to explore the physiological mechanisms of the effects of air pollution on HFMD and whether other air pollutants may affect the incidence of HFMD in children.
Conclusion
Studies have confirmed that socioeconomic factors and air pollution factors have an impact on the incidence of HFMD in Shenzhen, China. Among these factors, the population, the population density, the concentration of SO2 and the concentration of NO2 were positively correlated with the risk of HFMD, and the per capita GDP, the number of public kindergartens, the concentration of PM10 and the concentration of O3 were negatively correlated with the risk of HFMD. According to the map of relative risk obtained from the Bayesian spatiotemporal multifactor model, the risk of Longgang district and Pingshan district decreased, while the risk of Baoan district increased. The results will have important practical implications for local authorities, which is conducive to accurate prevention and can be used to formulate targeted disease intervention measures.
Data Availability
All relevant data are within the manuscript and its Supporting Information files.
Funding Statement
This study is funded by Guangdong Science and Technology Department (No. 2016A020216026), and the Department of Guangdong the Top-tier University Development Scheme for Research and Control of Infectious Diseases (No. 2016040). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Frydenberg A, Starr M. Hand, foot and mouth disease. AUST FAM PHYSICIAN. [Journal Article; Review]. 2003 2003-August-01;32(8):594–5. [PubMed] [Google Scholar]
- 2.Flett K, Youngster I, Huang J, McAdam A, Sandora TJ, Rennick M, et al. Hand, foot, and mouth disease caused by coxsackievirus a6. EMERG INFECT DIS. [Letter; Research Support, N.I.H., Extramural]. 2012 2012-October-01;18(10):1702–4. 10.3201/eid1810.120813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Murase C, Akiyama M. Hand, Foot, and Mouth Disease in an Adult. N Engl J Med. [Case Reports; Journal Article]. 2018 2018-April-05;378(14):e20 10.1056/NEJMicm1713548 [DOI] [PubMed] [Google Scholar]
- 4.Mirand A, le Sage FV, Pereira B, Cohen R, Levy C, Archimbaud C, et al. Ambulatory Pediatric Surveillance of Hand, Foot and Mouth Disease as Signal of an Outbreak of Coxsackievirus A6 Infections, France, 2014–2015. EMERG INFECT DIS. [Historical Article; Journal Article]. 2016 2016-November-01;22(11):1884–93. 10.3201/eid2211.160590 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nanda C, Singh R, Rana SK. An outbreak of hand-foot-mouth disease: A report from the hills of northern India. NATL MED J INDIA. [Journal Article]. 2015 2015-May-01;28(3):126–8. [PubMed] [Google Scholar]
- 6.El HN, Cointat V, Mirand A, Fouilloux V, Bzdrenga J, Bakour S, et al. An Outbreak of Kingella Kingae Infections Complicating a Severe Hand, Foot, And Mouth Disease Outbreak in Nice, France, 2016. PEDIATR INFECT DIS J. [Case Reports; Journal Article]. 2017 2017-May-01;36(5):530–2. 10.1097/INF.0000000000001487 [DOI] [PubMed] [Google Scholar]
- 7.Sumi A, Toyoda S, Kanou K, Fujimoto T, Mise K, Kohei Y, et al. Association between meteorological factors and reported cases of hand, foot, and mouth disease from 2000 to 2015 in Japan. EPIDEMIOL INFECT. [Journal Article; Research Support, Non-U.S. Gov’t]. 2017 2017-October-01;145(14):2896–911. 10.1017/S0950268817001820 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.NikNadia N, Sam IC, Rampal S, WanNorAmalina W, NurAtifah G, Verasahib K, et al. Cyclical Patterns of Hand, Foot and Mouth Disease Caused by Enterovirus A71 in Malaysia. PLoS Negl Trop Dis. [Journal Article; Research Support, Non-U.S. Gov’t]. 2016 2016-March-01;10(3):e4562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chansaenroj J, Tuanthap S, Thanusuwannasak T, Duang-In A, Klinfueng S, Thaneskongtong N, et al. Human enteroviruses associated with and without diarrhea in Thailand between 2010 and 2016. PLOS ONE. [Journal Article]. 2017 2017-January-20;12(7):e182078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mauleekoonphairoj J, Puenpa J, Korkong S, Vongpunsawad S, Poovorawan Y. PREVALENCE OF HUMAN ENTEROVIRUS AMONG PATIENTS WITH HAND, FOOT, AND MOUTH DISEASE AND HERPANGINA IN THAILAND, 2013. Southeast Asian J Trop Med Public Health. [Journal Article; Research Support, Non-U.S. Gov’t]. 2015 2015-November-01;46(6):1013–20. [PubMed] [Google Scholar]
- 11.Zheng Y, Jit M, Wu JT, Yang J, Leung K, Liao Q, et al. Economic costs and health-related quality of life for hand, foot and mouth disease (HFMD) patients in China. PLOS ONE. [Journal Article]. 2017 2017-January-20;12(9):e184266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhuang ZC, Kou ZQ, Bai YJ, Cong X, Wang LH, Li C, et al. Epidemiological Research on Hand, Foot, and Mouth Disease in Mainland China. Viruses. [Journal Article; Research Support, Non-U.S. Gov’t; Review]. 2015 2015-December-07;7(12):6400–11. 10.3390/v7122947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zeng H, Lu J, Zheng H, Yi L, Guo X, Liu L, et al. The Epidemiological Study of Coxsackievirus A6 revealing Hand, Foot and Mouth Disease Epidemic patterns in Guangdong, China. Sci Rep. [Journal Article; Research Support, Non-U.S. Gov’t]. 2015 2015-May-21;5:10550 10.1038/srep10550 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Aswathyraj S, Arunkumar G, Alidjinou EK, Hober D. Hand, foot and mouth disease (HFMD): emerging epidemiology and the need for a vaccine strategy. Med Microbiol Immunol. [Journal Article; Review]. 2016 2016-October-01;205(5):397–407. 10.1007/s00430-016-0465-y [DOI] [PubMed] [Google Scholar]
- 15.Liu Q, Tong X, Huang Z. Towards broadly protective polyvalent vaccines against hand, foot and mouth disease. MICROBES INFECT. [Journal Article; Review]. 2015 2015-February-01;17(2):155–62. 10.1016/j.micinf.2014.11.004 [DOI] [PubMed] [Google Scholar]
- 16.A Guide to Clinical Management and Public Health Response for Hand, Foot and Mouth Disease (HFMD.
- 17.Cheng Q, Bai L, Zhang Y, Zhang H, Wang S, Xie M, et al. Ambient temperature, humidity and hand, foot, and mouth disease: A systematic review and meta-analysis. SCI TOTAL ENVIRON. [Journal Article; Review]. 2018 2018-June-01;625:828–36. 10.1016/j.scitotenv.2018.01.006 [DOI] [PubMed] [Google Scholar]
- 18.Wei Q, Wu J, Zhang Y, Cheng Q, Bai L, Duan J, et al. Short-term exposure to sulfur dioxide and the risk of childhood hand, foot, and mouth disease during different seasons in Hefei, China. SCI TOTAL ENVIRON. 2019 2019-January-01;658:116–21. 10.1016/j.scitotenv.2018.11.481 [DOI] [PubMed] [Google Scholar]
- 19.Du Z, Lawrence WR, Zhang W, Zhang D, Yu S, Hao Y. Interactions between climate factors and air pollution on daily HFMD cases: A time series study in Guangdong, China. SCI TOTAL ENVIRON. 2019 2019-January-01;656:1358–64. 10.1016/j.scitotenv.2018.11.391 [DOI] [PubMed] [Google Scholar]
- 20.Yin F, Ma Y, Zhao X, Lv Q, Liu Y, Li X, et al. Analysis of the effect of PM10 on hand, foot and mouth disease in a basin terrain city. SCI REP-UK. 2019 2019-March-01;9(1):3233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zhou Y, Li L, Hu L. Correlation Analysis of PM10 and the Incidence of Lung Cancer in Nanchang, China. Int J Environ Res Public Health. [Journal Article; Research Support, Non-U.S. Gov’t]. 2017 2017-October-19;14(10). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Okada F. Inflammation-related carcinogenesis: Current findings in epidemiological trends, causes and mechanisms. YONAGO ACTA MED. 2014 2014-January-01;57(2):65–72. [PMC free article] [PubMed] [Google Scholar]
- 23.Chen G, Zhang W, Li S, Williams G, Liu C, Morgan GG, et al. Is short-term exposure to ambient fine particles associated with measles incidence in China? A multi-city study. ENVIRON RES. 2017;156:306–11. 10.1016/j.envres.2017.03.046 [DOI] [PubMed] [Google Scholar]
- 24.Yu G, Li Y, Cai J, Yu D, Tang J, Zhai W, et al. Short-term effects of meteorological factors and air pollution on childhood hand-foot-mouth disease in Guilin, China. SCI TOTAL ENVIRON. [Journal Article]. 2019 2019-January-01;646:460–70. 10.1016/j.scitotenv.2018.07.329 [DOI] [PubMed] [Google Scholar]
- 25.Huang R, Ning H, He T, Bian G, Hu J, Xu G. Impact of PM10 and meteorological factors on the incidence of hand, foot, and mouth disease in female children in Ningbo, China: a spatiotemporal and time-series study. Environ Sci Pollut Res Int. [Journal Article]. 2018 2018-July-01. [DOI] [PubMed] [Google Scholar]
- 26.Huang R, Bian G, He T, Chen L, Xu G. Effects of Meteorological Parameters and PM10 on the Incidence of Hand, Foot, and Mouth Disease in Children in China. Int J Environ Res Public Health. [Journal Article; Research Support, Non-U.S. Gov’t]. 2016 2016-May-10;13(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gralton J, Tovey E, McLaws M, Rawlinson WD. The role of particle size in aerosolised pathogen transmission: A review. J INFECTION. 2011;62(1):1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Du Z, Zhang W, Zhang D, Yu S, Hao Y. Estimating the basic reproduction rate of HFMD using the time series SIR model in Guangdong, China. PLOS ONE. [Journal Article]. 2017 2017-January-20;12(7):e179623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bo YC, Song C, Wang JF, Li XW. Using an autologistic regression model to identify spatial risk factors and spatial risk patterns of hand, foot and mouth disease (HFMD) in Mainland China. BMC PUBLIC HEALTH. [Journal Article; Research Support, Non-U.S. Gov’t]. 2014 2014-April-14;14:358 10.1186/1471-2458-14-358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wang P, Goggins WB, Chan EY. Hand, Foot and Mouth Disease in Hong Kong: A Time-Series Analysis on Its Relationship with Weather. PLOS ONE. [Journal Article]. 2016 2016-January-20;11(8):e161006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zhao J, Li X. Determinants of the Transmission Variation of Hand, Foot and Mouth Disease in China. PLOS ONE. 2016 2016-October-04;11(10):e163789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Li Shiyuan, Wang Xuemei. Research progress of Bayesian time-space model in space epidemiology. World Latest Medicine Information. 2017(34):55–7. [Google Scholar]
- 33.Wang Y, Lai Y, Du Z, Zhang W, Feng C, Li R, et al. Spatiotemporal Distribution of Hand, Foot, and Mouth Disease in Guangdong Province, China and Potential Predictors, 2009(-)2012. Int J Environ Res Public Health. [Journal Article; Research Support, Non-U.S. Gov’t]. 2019 2019-April-03;16(7). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Xiao K, Duan L, Peng Y, Wu M, Mai G, Yan Z, et al. Epidemiologic features of enterovirus associated with hand, foot and mouth disease in 2013 and 2014 in Shenzhen, China. Sci Rep. [Journal Article]. 2019 2019-March-07;9(1):3856 10.1038/s41598-019-40402-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Guidelines for the Prevention and Control of hand, foot and mouth Disease (version. 2009). Clinical education of general practice. 2010(02):125–7. [Google Scholar]
- 36.Li Yuan, Lv Qiuying, Cao Bin, Xie Xu, Mei Shujiang, Kong Dongfeng, et al. Analysis on the missing reports of infectious diseases in medical institutions in Shenzhen City. Practical Preventive Medicine. 2015;22(01):41–4. [Google Scholar]
- 37.Rang Qingxin. Taking Electronic Medical record as the Core, promoting the Construction of Hospital Information system. Information China(E-Healthcare). 2011(07):31. [Google Scholar]
- 38.Gou F, Liu X, Ren X, Liu D, Liu H, Wei K, et al. Socio-ecological factors and hand, foot and mouth disease in dry climate regions: a Bayesian spatial approach in Gansu, China. INT J BIOMETEOROL. [Journal Article]. 2017 2017-January-01;61(1):137–47. 10.1007/s00484-016-1197-9 [DOI] [PubMed] [Google Scholar]
- 39.Xu C. Spatio-Temporal Pattern and Risk Factor Analysis of Hand, Foot and Mouth Disease Associated with Under-Five Morbidity in the Beijing-Tianjin-Hebei Region of China. Int J Environ Res Public Health. [Journal Article; Research Support, Non-U.S. Gov’t]. 2017 2017-April-13;14(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mou J, Dawes M, Li Y, He Y, Ma H, Xie X, et al. Severe hand, foot and mouth disease in Shenzhen, South China: what matters most? EPIDEMIOL INFECT. [Journal Article; Research Support, Non-U.S. Gov’t]. 2014 2014-April-01;142(4):776–88. 10.1017/S0950268813001453 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Huang Y, Zhou Y, Lu H, Yang H, Feng Q, Dai Y, et al. Characterization of severe hand, foot, and mouth disease in Shenzhen, China, 2009–2013. J MED VIROL. [Journal Article; Research Support, Non-U.S. Gov’t]. 2015 2015-September-01;87(9):1471–9. 10.1002/jmv.24200 [DOI] [PubMed] [Google Scholar]
- 42.He Y, Zou L, Chong M, Men R, Xu W, Yang H, et al. Genetic evolution of Human Enterovirus A71 subgenotype C4 in Shenzhen, China, 1998–2013. J Infect. [Journal Article; Research Support, Non-U.S. Gov’t]. 2016 2016-June-01;72(6):731–7. 10.1016/j.jinf.2016.03.014 [DOI] [PubMed] [Google Scholar]
- 43.Zheng S, Cao CX, Cheng JQ, Wu YS, Xie X, Xu M. Epidemiological features of hand-foot-and-mouth disease in Shenzhen, China from 2008 to 2010. EPIDEMIOL INFECT. [Journal Article; Research Support, Non-U.S. Gov’t]. 2014 2014-August-01;142(8):1751–62. 10.1017/S0950268813002586 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Chen Ruili, Wan Feng, Wang Song, Yao Bin, Luo Leilei, Guo Jiyao, Chunxiao Yang. Analysis of disinfection quality monitoring in private and public kindergartens in Zhuhai City. Practical Preventive Medicine 2012:1018–1020. [Google Scholar]
- 45.Liu X, Hou W, Zhao Z, Cheng J, van Beeck EF, Peng X, et al. A hand hygiene intervention to decrease hand, foot and mouth disease and absence due to sickness among kindergarteners in China: A cluster-randomized controlled trial. J Infect. [Journal Article]. 2019 2019-January-01;78(1):19–26. 10.1016/j.jinf.2018.08.009 [DOI] [PubMed] [Google Scholar]
- 46.Wigenstam E, Elfsmark L, Bucht A, Jonasson S. Inhaled sulfur dioxide causes pulmonary and systemic inflammation leading to fibrotic respiratory disease in a rat model of chemical-induced lung injury. TOXICOLOGY. 2016 2016-January-01;368–369:28–36. 10.1016/j.tox.2016.08.018 [DOI] [PubMed] [Google Scholar]
- 47.Yan Wei, Duan Li, Liao Lv, et al. Short-Term Effects of Meteorological Factors and Air Pollutants on Hand, Foot and Mouth Disease among Children in Shenzhen, China, 2009–2017. INT J ENV RES PUB HE. 2019 2019-January-01;16(19):3639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ye Q, Fu JF, Mao JH, Shen HQ, Chen XJ, Shao WX, et al. Haze is an important medium for the spread of rotavirus. ENVIRON POLLUT. [Journal Article;]. 2016 2016-January-20;216:324–31. 10.1016/j.envpol.2016.05.090 [DOI] [PubMed] [Google Scholar]
- 49.Beamish LA, Osornio-Vargas AR, Wine E. Air pollution: An environmental factor contributing to intestinal disease. J CROHNS COLITIS. [Journal Article;Research Support, Non-U.S. Gov’t;Review;]. 2011 2011-January-20;5(4):279–86. 10.1016/j.crohns.2011.02.017 [DOI] [PubMed] [Google Scholar]
- 50.Zanardi I, Borrelli E, Valacchi G, Travagli V, Bocci V. Ozone: A Multifaceted Molecule with Unexpected Therapeutic Activity. CURR MED CHEM. [Journal Article; Review]. 2016 2016-January-20;23(4):304–14. 10.2174/0929867323666151221150420 [DOI] [PubMed] [Google Scholar]
- 51.Bocci V, Borrelli E, Travagli V, Zanardi I. The ozone paradox: ozone is a strong oxidant as well as a medical drug. MED RES REV. [Journal Article; Review]. 2009 2009-July-01;29(4):646–82. 10.1002/med.20150 [DOI] [PubMed] [Google Scholar]
- 52.Bocci V, Borrelli E, Zanardi I, Travagli V. The usefulness of ozone treatment in spinal pain. Drug Des Devel Ther. [Journal Article; Review]. 2015 2015-January-20;9:2677–85. 10.2147/DDDT.S74518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Braidy N, Izadi M, Sureda A, Jonaidi-Jafari N, Banki A, Nabavi SF, et al. Therapeutic relevance of ozone therapy in degenerative diseases: Focus on diabetes and spinal pain. J CELL PHYSIOL. [Journal Article; Research Support, Non-U.S. Gov’t; Review]. 2018 2018-April-01;233(4):2705–14. 10.1002/jcp.26044 [DOI] [PubMed] [Google Scholar]
- 54.Lin Y, Wu S. Effects of ozone exposure on inactivation of intra- and extracellular enterovirus 71. ANTIVIR RES. 2006 2006-January-01;70(3):147–53. 10.1016/j.antiviral.2005.12.007 [DOI] [PubMed] [Google Scholar]
- 55.Lin Y, Juan H, Cheng Y. Ozone exposure in the culture medium inhibits enterovirus 71 virus replication and modulates cytokine production in rhabdomyosarcoma cells. ANTIVIR RES. 2007 2007-January-01;76(3):241–51. 10.1016/j.antiviral.2007.07.004 [DOI] [PubMed] [Google Scholar]
- 56.Luo Xiaofeng, Zhan Liuhua, Zhou Wen, Xiao Xiaoling. Correlation Analysis of 20102011 in Guangzhou City, Yuexiu District hand foot and Mouth Disease Incidence and Meteorological Factors and Air Pollution Index. China Journal of Pharmaceutical Economics. 2013(S3):182–4. [Google Scholar]
- 57.Xiong L, Li J, Xia T, Hu X, Wang Y, Sun M, et al. Risk Reduction Behaviors Regarding PM2.5 Exposure among Outdoor Exercisers in the Nanjing Metropolitan Area, China. Int J Environ Res Public Health. [Journal Article; Research Support, Non-U.S. Gov’t]. 2018 2018-August-12;15(8). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Sheeran P, Harris PR, Epton T. Does heightening risk appraisals change people’s intentions and behavior? A meta-analysis of experimental studies. PSYCHOL BULL. [Journal Article; Meta-Analysis; Research Support, Non-U.S. Gov’t; Review]. 2014 2014-March-01;140(2):511–43. 10.1037/a0033065 [DOI] [PubMed] [Google Scholar]
- 59.Patel D, Shibata T, Wilson J, Maidin A. Challenges in evaluating PM concentration levels, commuting exposure, and mask efficacy in reducing PM exposure in growing, urban communities in a developing country. SCI TOTAL ENVIRON. [Journal Article; Research Support, Non-U.S. Gov’t; Research Support, U.S. Gov’t, Non-P.H.S.]. 2016 2016-February-01;543(Pt A):416–24. 10.1016/j.scitotenv.2015.10.163 [DOI] [PubMed] [Google Scholar]
- 60.Huang L, Rao C, van der Kuijp TJ, Bi J, Liu Y. A comparison of individual exposure, perception, and acceptable levels of PM2.5 with air pollution policy objectives in China. ENVIRON RES. [Journal Article]. 2017 2017-August-01;157:78–86. 10.1016/j.envres.2017.05.012 [DOI] [PubMed] [Google Scholar]
- 61.Chakraborty J, Collins TW, Grineski SE, Maldonado A. Racial Differences in Perceptions of Air Pollution Health Risk: Does Environmental Exposure Matter? Int J Environ Res Public Health. [Comparative Study; Journal Article]. 2017 2017-01-;14(2). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.De Pretto L, Acreman S, Ashfold MJ, Mohankumar SK, Campos-Arceiz A. The Link between Knowledge, Attitudes and Practices in Relation to Atmospheric Haze Pollution in Peninsular Malaysia. PLOS ONE. [Journal Article; Research Support, Non-U.S. Gov’t]. 2015 2015-January-20;10(12):e143655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Zhan D, Kwan MP, Zhang W, Wang S, Yu J. Spatiotemporal Variations and Driving Factors of Air Pollution in China. Int J Environ Res Public Health. [Journal Article; Research Support, Non-U.S. Gov’t]. 2017 2017-December-08; 14(12). [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All relevant data are within the manuscript and its Supporting Information files.