

Abstract
Aim
Increasing numbers of older gravidas compel research into best practices for their labour‐related outcomes. Responding to this need, this study sought to develop and evaluate a programme for older primigravidas.
Design
The authors developed a simulated practice programme for older primigravidas and tested its effects.
Methods
A non‐equivalent control group pre‐ and post‐test design was used with 49 community‐dwelling primigravidas. The programme taught the stages of labour using a realistic scenario‐based practice and a debriefing session. Data were collected between June and September 2015. Participants were divided into intervention (N = 25) and control (N = 24) groups. Postintervention group effects were analysed with independent t tests.
Results
The intervention group's levels of anxiety and stress decreased and their knowledge and self‐confidence increased. The intervention group's labour duration was also shorter than that of the control group.
Keywords: advanced maternal age, anxiety, emotional stress, obstetric labour, patient simulation, pregnancy outcomes
1. INTRODUCTION
Improvements in education, social advancement, female life expectancy and infertility treatments have caused a worldwide increase in the number of older gravidas, that is, women who give birth at 35 years of age or older (Laopaiboon et al., 2014; Ojule, Ibe, & Fiebai, 2011). The proportion of older gravidas in Korea has increased fivefold in the past 10 years from 4.7% in 2005–23.8% in 2015 (Statistics Korea, 2016). This increase in the average age of pregnancy affects delivery outcomes (Hwang, Kim, Yoon, & Lee, 2011; Jahan et al., 2009): older primigravidas have a higher likelihood than older multigravida of developing obstetric problems such as hypertensive illnesses, diabetes, pre‐mature birth, stillbirth, abruptio placentae and placenta previa. (Moses, & Dalal, 2016; Eleje, Okonkwo, Udigwe, & Eke, 2014; Ojule et al., 2011). These obstetric problems ultimately increase the frequency of induced labours or caesarean births (Fitzpatrick, Tuffnell, Kurinczuk, & Knight, 2016; Sauer, 2015). Accordingly, it is not surprising that fear of childbirth is a common emotion among pregnant women. Studies report that primigravidas experience more anxiety than multigravidas, that some pregnant women experience severe anxiety, that women experience increased anxiety during labour and that maternal anxiety and stress are related to health problems in newborns (Molgora et al., 2018; Zijlmans, Beijers, Riksen‐Walraven, & de Weerth, 2017). Pre‐natal training, especially that which provides emotional support for anxiety, leads to positive pregnancy outcomes; pre‐natal health experts would thus do well to implement programmes that reduce unnecessary anxiety in gravidas and increase their capacities for self‐care by providing accurate information (Isbir & Serçekus, 2017; Karabulut, Coşkuner Potur, Doğan Merih, Cebeci Mutlu, & Demirci, 2016). Although, as noted above, the proportion of older gravidas in Korea has significantly increased over the last decade, the Korean government does not yet emphasize the importance of preventative care for older gravidas or primigravidas—although it does encourage pre‐natal training and provides financial support to relieve costs related to pregnancy and delivery (Kim, 2012).
Notably, pre‐natal training for primigravidas often provides knowledge about key topics such as Doula Touch, Lamaze techniques, ball exercises and coaching consultation programmes. Primigravidas who participate in these training sessions experience increased labour confidence and perceive positive labour experiences, while also demonstrating shorter labour durations and decreased anxiety and pregnancy‐related stress (Yeo, 2010; Ip, Tang, & Goggins, 2009; Kim, 2013). Although few studies provide and test the results of pre‐natal care for older gravidas who experience social isolation compared with young gravidas, Wang’s (2014) paper on a web‐based pre‐natal care programme is helpful to note: the study reveals that the programme affected participants' knowledge, self‐efficacy and practice behaviour (Wang, 2014). However, in step with the Korean government's lack of focus on older primigravidas, few studies, including Wang's, examine the nuances of providing pre‐natal care to older primigravidas or examine their outcomes for labour and delivery.
2. BACKGROUND
The most effective learning outcome for a particular population might be determined by applying various theories of learning to the situation at hand; moreover, educating medical personnel using simulation training reveals the particular ways such simulated practices may improve knowledge, skills, learning satisfaction, critical thinking and self‐confidence (Jeffries, 2005; Park, 2012). Simulation‐based experiential education fits well with adult education focused on standard clinical care. Designing effective simulations generally requires a sense of the intended results of the pedagogy's structure, processes and goals as well as the nuances of the situation to be simulated (The International Nursing Association for Clinical Simulation & Learning, 2016; Lavoie et al., 2018). Notably, a simulation‐based training programme is advantageous because it enables learners to receive immediate feedback, learn by practice and enjoy the opportunity for individualized learning and, moreover, because it can be easily adapted to fit a particular student's education level (Issenberg, Mcgaghie, Petrusa, Gordon, & Scalese, 2005).
Taking these strengths of simulation‐based education to task to address the lack of research around preventative pre‐natal training for older primigravidas, the authors created a labour and delivery simulated practice programme for older primigravidas (LDSPP_EP) that sought to prevent health problems that can occur during pregnancy for older primigravidas. The programme included distinct labour phrases, peer support and a debriefing session. The authors also tested the effects of the programme, including its impact on the participants' levels of anxiety, stress, labour knowledge and confidence and labour‐related outcomes. Ultimately, this study sought to answer: does this simulation‐based based educational programme improve the rate at and quality with which older primigravidas practice self‐care related to labour and delivery and, relatedly, increase positive labour outcomes?
2.1. Design
This study used a non‐equivalent control group pre‐ and post‐test design to develop, apply and analyse the effects of LDSPP_EP. The intervention group comprised pregnant women living in D Area who were selected through the “Mom Mom Mom” café on a social network service. The control group comprised pregnant women who also lived in D Area and who were receiving pre‐natal care from the same maternity hospital as the women in the intervention group. The study was conducted from 10 June 10 – 30 September 2015. The eligible population was 60 people during the study.
The inclusion criteria for participants were as follows: (a) primigravidas aged ≥35 years; (b) between 3–35 weeks of gestation; (c) no complications for a high‐risk pregnancy other than age; (d) consented to participate after hearing a study description from a research participant; and (e) had not participated in other programmes related to labour training. Women with plural pregnancies or who had pre‐planned caesarean sections were excluded.
The required sample size was 26 per group, which was calculated with G*Power 3.1.9.2 using an effect size (f) of 0.8, a significance level (α) of 0.05 and power (1‐β) of 0.80. To allow for a 15% dropout rate, the authors decided on 30 participants per group. In the intervention group, two participants refused to participate and three did not finish the 5‐week programme. In the control group, six participants refused to participate. Therefore, data from the remaining 49 participants were analysed (intervention, n = 25; control, n = 24). Further, 31 individuals participated in the postdelivery survey (Figure 1).
Figure 1.
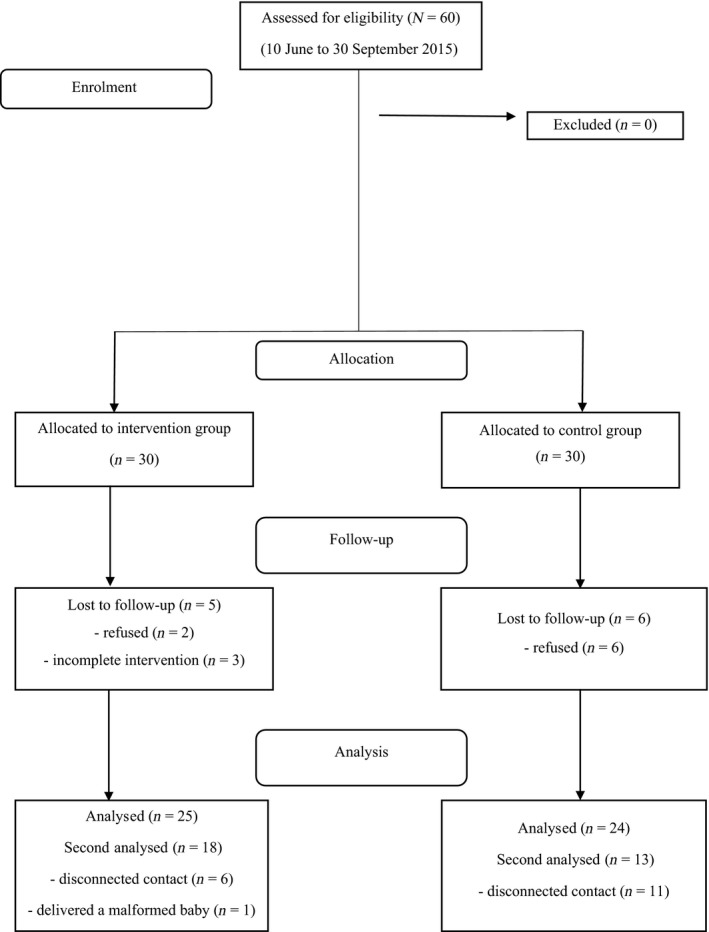
Participant flowchart
2.2. Methods
The methods are detailed below under headings that reference the items they sought to measure.
2.2.1. Anxiety
The authors measured anxiety with the Korean version (Kim & Shin, 1978) of the Spielberger Trait Anxiety Inventory for Korea, which was developed by Spielberger (1975). It comprises 20 items measured with a four‐point scale. Higher scores signify higher levels of perceived anxiety. Cronbach's α was 0.90 at the time of development and 0.87 in this study.
2.2.2. Pregnancy‐related stress
The authors used the pregnancy‐related stress instrument developed by Ahn (1985), which comprises 26 items measured with a four‐point scale. Higher scores signify higher levels of pregnancy‐related stress. Cronbach's α was 0.82 at the time of development and 0.82 in this study.
2.2.3. Knowledge of labour and delivery
Kang (1980) developed a scale to measure knowledge of labour and delivery. It comprises items addressing the physiology of labour, process of labour, pre‐natal exercises, breathing methods and how to strain. The scores range from 0–20 points, with higher scores indicating deeper knowledge of labour and delivery.
2.2.4. Self‐confidence concerning labour and delivery
Lee (2005) developed a scale to measure labour confidence. It comprises 15 items measured with a four‐point scale and higher scores indicate higher confidence concerning labour. Cronbach's α was 0.89 at the time of development and 0.87 in this study.
2.2.5. Delivery‐related outcomes
Delivery‐related outcomes included duration of labour and perception of labour. For the duration of labour, the pregnant women were questioned about the duration of time between first feeling pain and delivering their babies. For perception of labour and delivery, the authors used an instrument developed by Marut and Mercer (1979) and translated by Cho (1990). This instrument comprised 20 items measured with a four‐point scale, with higher scores indicating more positive perceptions of labour and delivery. Cronbach's α was 0.83 at the time of development and 0.89 in this study.
Labour and delivery simulated practice programme for older primigravidas is an empirically based pre‐natal training programme that was developed by the researchers. In a previous study (blinded for review), older primigravidas stated they would prefer to learn by practice rather than by theory. Reflecting their opinions, the researchers restructured the programme to strengthen its teachings of relaxation, breathing and stretching. The programme also reflects the women's sense that the educational setting should mirror a hospital environment. The details of the five‐session programme are provided in Table 1, which was structured in conversation with Jeffries' (2005) theory of simulation education.
Table 1.
Labour and delivery simulated practice programme for elderly primigravidas
| Session | Phase | Activity | Activity type |
|---|---|---|---|
| 1st | Introductory period (30 min) |
|
Orientation Mini lecture |
| Simulated practice (40 min) | Demonstration and practice | ||
| Debriefing (30 min) | Debriefing | ||
| 2nd | Introductory period (30 min) |
|
Peer interactions Mini lecture |
| Simulated practice (40 min) | Demonstration and practice | ||
| Debriefing (30 min) | Debriefing | ||
| 3rd | Introductory period (30 min) |
|
Peer interactions Mini lecture |
| Simulated practice (40 min) | Demonstration and practice | ||
| Debriefing (30 min) | Debriefing | ||
| 4th | Introductory period (30 min) |
|
Peer interactions Mini lecture |
| Simulated practice (40 min) | Demonstration and practice | ||
| Debriefing (30 min) | Debriefing | ||
| 5th | Introductory period (30 min) |
|
Peer interactions Mini lecture |
| Simulated practice (40 min) | Demonstration and practice | ||
| Debriefing (30 min) | Debriefing |
The first session sought to give participants a basic understanding of labour and muscle relaxation. Participants practiced muscle relaxation by being alerted to the start and end of a uterine contraction with a cue, including a scenario with the following variables: cervix dilation of 3 cm, 60% effacement, medium pain intensity, women displaying stable vital signs, a foetal heart rate of approximately 149 beats per minute and women being able to move freely.
The second session sought to give women an understanding of the labour procedure that occurred in the hospital and breathing and relaxation methods for the first phase of labour. This session situated the labour as having progressed since the first session. Foetal heart monitoring was performed, cervix dilation was 5 cm, effacement was 60%, and uterine contractions lasting 50 s occurred every three minutes with a strong pain intensity. Latent breathing and relaxation methods were practiced.
The third session sought to teach participants methods for responding to hyperventilation during labour and straining during the second phase of labour. This session situated the labour as having further progressed since the second session. Cues such as feeling pain, a pounding heartbeat and dizziness were given during uterine contractions so that participants could practice responding to hyperventilation.
The fourth section sought to impart the nuances of prodromal labour and the straining method for the second stage of labour using the following scenario: cervix dilation of 10 cm, 100% effacement, strong pain intensity and a foetal heart rate of 150. Participants practiced second‐phase labour straining by being alerted to the start of uterine contractions with a cue.
In the fifth and final session, the first and second phases of labour were combined and practiced together. Training on postnatal care was also included in this session. Moreover, the participants were divided into groups of 6–7 to participate in debriefings and feedback. Peer debriefing occurred first, followed by an overall debriefing session using the “GAS (gather assessment summary).”
To increase the learning effect of the programme and to encourage participation, text messages were sent to participants twice a week. Furthermore, the authors produced a small 45‐page booklet with figures about the programme's content for distribution and posters were produced and attached to the walls of the room where the programme was conducted.
In sum, the LDSPP_EP was applied in four steps: pre‐test, application of the programme, post‐test and postlabour test. The location of the research was a conference room in the Community Demographic Welfare Association, which conducts health‐enhancement programmes related to multiculturalism, childrearing and pregnant women. The room was furnished with cushions, sound systems, mats, baby‐bathing products and baby models. The authors obtained approval from the director of the association. A research assistant, an experienced delivery‐room nurse, assisted with the pre‐test after being trained for the study. More specifically, these stages unfolded as follows:
2.2.6. Pre‐test
After obtaining consent (see below), participants completed surveys that measured their general characteristics, anxiety, pregnancy‐related stress and labour knowledge and confidence. The pre‐test took approximately 15–20 min to complete.
2.2.7. LDSPP_EP
As noted above, the programme comprised five sessions over 5 weeks. The researchers and the research assistant performed various interactions with participants, such as assessing their relaxation and playing the role of caregivers, to determine whether the women were following along in each situation. The light was dimmed to the lowest setting and quiet music was played in the background so that women could concentrate on relaxing. The authors posit that positive practice will foster positive experiences during labour and delivery. Self‐reflection was fostered through debriefing and the women's concerns were clarified after the programme to promote their confidence. Additional programme details are listed in Table 1.
2.2.8. Post‐test and postlabour test
After the 5‐week programme, a post‐test was conducted with the intervention group. A post‐test was also conducted with the control group, in an outpatient setting, 5 weeks after they completed the pre‐test. The postlabour tests included questions about the labour outcomes. Data from 20 items that addressed women's labour duration and perceptions were collected by the researchers and the research assistant, who directly visited the hospital at which the women gave birth.
2.3. Analysis
Collected data were processed using SPSS/WIN 21.0. Participants' general characteristics and their labour outcomes were analysed with frequencies and percentages. Measure reliability was computed using Cronbach's α. The effects of the programme were analysed using independent t tests.
3. ETHICS
Data were collected with approval from the institutional review of Keimyung University (no. 2015–05‐HR‐25–01). Participants provided voluntary, written consent after receiving information about the study purpose and procedure, risks and benefits of participation and a guarantee of privacy. Participants could cease participation at any time without penalty. To ensure privacy, surveys were retrieved immediately after completion and were stored in a locked location.
4. RESULTS
Participants' characteristics are displayed in Table 2. The mean age was 37 years. Nearly, all women were at 32–34 weeks' gestation. Weight gain ranged from 2–22 kg.
Table 2.
Participant characteristics (N = 49)
| Variable | Category | Intervention group (n = 25) | Control group (n = 24) | x2 | p |
|---|---|---|---|---|---|
| n (%) | n (%) | ||||
| Age (years) |
35 36–37 38–39 40–42 |
7 (14.3) 10 (20.4) 6 (12.2) 2 (4.1) |
4 (8.2) 11 (22.4) 5 (10.2) 6 (6.0) |
4.89 | .559 |
| Gestation (weeks) |
30 31 32 33 34 |
‐ 1 (2.0) 9 (18.4) 7 (14.3) 8 (16.3) |
1 (2.0) 1 (2.0) 8 (8.3) 6 (6.4) 8 (7.8) |
1.12 | .892 |
| Admission history |
Yes No |
‐ 25 (51) |
1 (2.0) 23 (46.9) |
1.12 | .490a |
| Weight gain postpregnancy (kg) |
<5 5–8 9–12 13–15 >15 |
4 (8.1) 10 (20.4) 5 (10.2) 5 (10.2) 1 (2.0) |
3 (6.1) 7 (14.3) 11 (22.4) 2 (4.1) 1 (2.0) |
11.02 | .609 |
Fisher's exact test.
After participating in the programme, the anxiety and pregnancy‐related stress scores of the intervention group were significantly lower than the scores displayed by the control group. In addition, the labour knowledge and confidence scores of the intervention group were significantly higher than those of the control group (Table 3).
Table 3.
Primary outcomes of the intervention and control groups before and after the programme (N = 49)
| Variable | Intervention group (n = 25) | Control group (n = 24) | t | p | ||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | |||
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Anxietya | 1.99 ± 0.39 | 2.02 ± 0.43 | 1.88 ± 0.27 | 2.40 ± 0.37 | 3.31 | .002 |
| Pregnancy‐related stress | 1.96 ± 0.28 | 1.80 ± 0.30 | 1.99 ± 0.38 | 2.24 ± 0.08 | 4.58 | <.001 |
| Knowledge | 15.68 ± 1.44 | 18.44 ± 1.92 | 15.71 ± 1.76 | 15.13 ± 2.01 | 5.92 | <.001 |
| Self‐confidence | 2.66 ± 0.40 | 3.07 ± 0.44 | 2.57 ± 0.37 | 2.11 ± 0.39 | 8.10 | <.001 |
Korean adaptations of Spielberger's State‐Trait Anxiety Inventory.
Concerning labour‐related outcomes after LDSEP_EP, the intervention group had a significantly shorter labour duration in case of vaginal delivery than the control group. The groups did not differ in their perception of labour (Table 4).
Table 4.
Delivery outcomes of the intervention and control groups (N = 31)
| Variable |
Intervention group (n = 18) |
Control group (n = 13) |
t/x2 | p | |
|---|---|---|---|---|---|
| M ± SD or n (%) | M ± SD or n (%) | ||||
| Duration of laboura | Hours | 7.50 ± 3.22 | 9.92 ± 2.99 | −2.13 | .042 |
| Perception of labour | 2.78 ± 0.46 | 2.57 ± 0.33 | 0.38 | .117 | |
| Experience of Labour analgesia | Yes | 7 (38.9) | 11 (84.6) | 0.01 | .013 |
| No | 11 (61.1) | 2 (12.4) |
Vaginal delivery.
The authors applied and tested the effects of LDSPP_EP. After the application of LDSPP_EP, the anxiety and stress related to pregnancy of the older primigravidas in the intervention group decreased and labour knowledge and labour‐related self‐confidence increased. In addition, women in the intervention group had shorter labour durations than those in the control group. However, the fact that the data collection and experiments of this study are outdated is a limitation of this study.
CONFLICT OF INTEREST
None.
ACKNOWLEDGEMENTS
None.
Seong CH, Park KM, Moon KJ. Effects of a labour and delivery simulated practice programme for elderly primigravidas. Nursing Open. 2020;7:776–782. 10.1002/nop2.450
Funding information
This research was supported by the Keimyung University Research Grant of 2016.
REFERENCES
- Ahn, H. L. (1985). An experimental study of the effects of husband's supportive behavior reinforcement education on stress relief of primigravidas. The Journal of Nurses Academic Society, 15(1), 5–16. 10.4040/jnas.1985.15.1.5 [DOI] [Google Scholar]
- Cho, M. Y. (1990). Primiparas' perceptions of their delivery experience and their maternal‐interaction: Compared according to delivery method. The Journal of Nurses Academic Society, 20(2), 153–173. 10.4040/jnas.1990.20.2.153 [DOI] [PubMed] [Google Scholar]
- Eleje, G. U. , Okonkwo, J. E. , Udigwe, G. O. , & Eke, A. C. (2014). Elderly primigravidae versus young primigravidae: A review of pregnancy outcome in a low resource setting. Nigerian Journal of Medicine: Journal of the National Association of Resident Doctors of Nigeria, 23(3), 220–229. [PubMed] [Google Scholar]
- Fitzpatrick, K. E. , Tuffnell, D. , Kurinczuk, J. J. , & Knight, M. (2016). Pregnancy at very advanced maternal age: A UK population‐based cohort study. An International Journal of Obstetrics and Gynaecology, 124(7), 1097–1106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hwang, R. I. , Kim, K. H. , Yoon, J. W. , & Lee, J. S. (2011). The trend of national health insurance service use among pregnant and postpartum women aged 35 years and older. Health Policy and Management, 21(4), 585–598. 10.4332/KJHPA.2011.21.4.585 [DOI] [Google Scholar]
- International Nursing Association for Clinical Simulation and Learning (2016). Standards of best practice: simulationSM simulation design. Clinical Simulation in Nursing, 12, S5–S12. 10.1016/j.ecns.2016.09.005 [DOI] [Google Scholar]
- Ip, W. Y. , Tang, C. S. , & Goggins, W. B. (2009). An educational intervention to improve women’s ability to cope with childbirth. Journal of Clinical Nursing, 18(15), 2125–2135. 10.1111/j.1365-2702.2008.02720.x [DOI] [PubMed] [Google Scholar]
- Isbir, G. G. , & Serçekus, P. (2017). The effects of intrapartum supportive care on fear of delivery and labor outcomes: A single‐blind randomized controlled trial. Journal of Nursing Research, 25(2), 112–119. 10.1097/JNR.0000000000000129 [DOI] [PubMed] [Google Scholar]
- Issenberg, S. B. , Mcgaghie, W. C. , Petrusa, E. R. , Gordon, D. L. , & Scalese, R. J. (2005). Features and uses of high‐fidelity medical simulations that lead to effective learning: A BEME systematic review. Medical Teacher, 27(1), 10–28. 10.1080/01421590500046924 [DOI] [PubMed] [Google Scholar]
- Jahan, M. K. , Shafiquzzaman, M. , Nahar, K. , Rahman, M. , Sultana, N. , Rahman, M. M. , & Begum, R. (2009). Outcome of pregnancy in women 35 years of age and above. Mymensingh Medical Journal, 18(1), 7–12. [PubMed] [Google Scholar]
- Jeffries, P. R. (2005). A framework for designing, implementing and evaluating: Simulations used as teaching strategies in nursing. Nursing Education Perspectives, 26(2), 96–103. [PubMed] [Google Scholar]
- Kang, J. H. (1980). A study on fear and anxiety of pregnant women. The Journal of Nurses Academic Society, 10(2), 1 10.4040/jnas.1980.10.2.1 [DOI] [Google Scholar]
- Karabulut, Ö. , Coşkuner Potur, D. , Doğan Merih, Y. , Cebeci Mutlu, S. , & Demirci, N. (2016). Does antenatal education reduce fear of childbirth? International Nursing Review, 63(1), 60–67. 10.1111/inr.12223 [DOI] [PubMed] [Google Scholar]
- Kim, D. S. (2012). Birth outcomes of late pregnant women and suggestions for policy support. Seoul, South Korea: Korean Women's Development Institute. [Google Scholar]
- Kim, G. J. (2013). The effects of doula touch delivery education on self‐confidence delivery, knowledge of childbirth, couple satisfaction. Journal of the Korea Academia‐Industrial Cooperation Society, 14(6), 2880–2888. 10.5762/KAIS.2013.14.6.2880 [DOI] [Google Scholar]
- Kim, J. T. , & Shin, D. K. (1978). A study based on the standardization of the STAI for Korea. New Medical Journal, 21(11), 69–75. [Google Scholar]
- Laopaiboon, M. , Lumbiganon, P. , Intarut, N. , Mori, R. , Ganchimeg, T. , Vogel, J. P. … WHO Multicountry Survey on Maternal Newborn Health Research Network (2014). Advanced maternal age and pregnancy outcomes: A multicountry assessment. BJOG: an International Journal of Obstetrics & Gynaecology, 121, 49–56. 10.1111/1471-0528.12659 [DOI] [PubMed] [Google Scholar]
- Lavoie, P. , Michaud, C. , Bélisle, M. , Boyer, L. , Gosselin, É. , Grondin, M. , … Pepin, J. (2018). Learning theories and tools for the assessment of core nursing competencies in simulation: A theoretical review. Journal of Advanced Nursing, 74(2), 239–250. 10.1111/jan.13416 [DOI] [PubMed] [Google Scholar]
- Lee, M. K. (2005). Factors influencing self confidence during delivery in laboring women. Korean Journal of Women Health Nursing, 11(1), 20–26. 10.4069/kjwhn.2005.11.1.20 [DOI] [Google Scholar]
- Marut, J. S. , & Mercer, R. T. (1979). Comparison of primiparas' perceptions of vaginal and cesarean births. Nursing Research, 28(5), 260–265. 10.1097/00006199-197909000-00002 [DOI] [PubMed] [Google Scholar]
- Molgora, S. , Fenaroli, V. , Prino, L. E. , Rollè, L. , Sechi, C. , Trovato, A. , … Saita, E. (2018). Fear of childbirth in primiparous Italian pregnant women: The role of anxiety, depression and couple adjustment. Women and Birth, 31(2), 117–123. 10.1016/j.wombi.2017.06.022 [DOI] [PubMed] [Google Scholar]
- Moses, V. , & Dalal, N. (2016). Pregnancy outcome in elderly primi gravidas. International Journal of Reproduction, Contraception, Obstetrics and Gynecology, 5(11), 3731–3735. 10.18203/2320-1779.ijrcog20163519 [DOI] [Google Scholar]
- Ojule, J. D. , Ibe, V. C. , & Fiebai, P. O. (2011). Pregnancy outcome in elderly primigravidae. Annals of African Medicine, 10(3), 204 10.4103/1596-3519.84699 [DOI] [PubMed] [Google Scholar]
- Park, S. J. (2012). A formative research on a lecture for educational administration utilizing action learning. The Journal of Korean Teacher Education, 29(4), 389–416. 10.24211/tjkte.2012.29.4.389 [DOI] [Google Scholar]
- Sauer, M. V. (2015). Reproduction at an advanced maternal age and maternal health. Fertility and Sterility, 103(5), 1136–1143. 10.1016/j.fertnstert.2015.03.004 [DOI] [PubMed] [Google Scholar]
- Spielberger, C. D. (1975). Anxiety: State‐trait process In Spielberger C. D., & Sarason I. G. (Eds.), Stress and Anxiety (pp. 115–143). New York, NY: Wiley. [Google Scholar]
- Statistics Korea (2016). South Korea birth statistics 2015 [Online]. Retrieved from: http://kostat.go.kr/portal/korea/kor_nw/1/2/1/index.board?bmode=read%26aSeq=355736 [Google Scholar]
- Wang, H. J. (2014). Development and evaluation of the mobile web‐based pregnancy health care educational program for old pregnant women aged 35 years. Seoul, South Korea: The Graduate School of Ewha Woman’s University. [Google Scholar]
- Yeo, J. H. (2010). Childbirth experience of participants in lamaze childbirth education. Korean Journal of Women Health Nursing, 16(3), 215–223. [DOI] [PubMed] [Google Scholar]
- Zijlmans, M. A. , Beijers, R. , Riksen‐Walraven, M. J. , & de Weerth, C. (2017). Maternal late pregnancy anxiety and stress is associated with children’s health: A longitudinal study. Stress, 20(5), 495–504. 10.1080/10253890.2017.1348497 [DOI] [PubMed] [Google Scholar]