

Abstract
Spontaneous coronary artery dissection (SCAD) is a relatively infrequent cause of acute coronary syndrome that usually affects young to middle-aged women. Mainly because of its low prevalence, until recently, most of the evidence on this condition was derived from case reports and small series. Over the last 5 years, more robust evidence has become available from larger retrospective and prospective cohorts of patients with SCAD. The increase in knowledge and recognition of this entity has led to the publication of expert consensus on both sides of the Atlantic. However, new data are continuously accumulating from larger cohorts of patients with SCAD, bringing new light to this little-understood condition. The aim of this article is to update the knowledge on SCAD, including new information from recent studies published since the consensus documents from the European Society of Cardiology and the American Heart Association.
Keywords: Spontaneous coronary artery dissection, fibromuscular dysplasia, optical coherence tomography, intravascular ultrasound, percutaneous coronary intervention
Spontaneous coronary artery dissection (SCAD) can be defined as the acute development of a false lumen within the coronary artery wall that may lead to flow limitation by compression of the true coronary lumen. This definition of SCAD excludes coronary dissections that are secondary to atherosclerotic disease, produced by the extension of an aortic dissection, iatrogenic or related to a trauma.[1,2]
Physiopathology
Two mechanisms have been proposed to explain the development of the false lumen in SCAD. Under the “inside-out” hypothesis, the cause is a disruption of the endothelial-intimal layer, which allows blood from the lumen to enter the vessel wall, leading to the formation of an intramural haematoma (IMH). Under the “outside-in” hypothesis the primary event is a bleeding episode within the coronary artery wall (at the level of the vasa vasorum), which generates an IMH without intimal disruption. Both mechanisms can lead to haematoma extension and compression of the true lumen, resulting in myocardial ischaemia in the territory of the affected coronary artery.[3]
Some authors suggest that the outside-in hypothesis might be the primary event in the majority of SCAD cases. In some patients, rising pressure in this primarily produced IMH would lead to the development of an intimal disruption, which explains cases with double lumen on angiography and/or evidence of intimo-medial dissections with intracoronary imaging (ICI). In keeping with this, Waterbury et al. analysed predictors of SCAD progression in patients who had initially been treated in a conservative manner.[4] Interestingly, they found that 20% of lesions initially defined as IMH on repeated coronary angiogram progressed to a double lumen on angiography.
Epidemiology
The true incidence of SCAD is unknown. Since the first case reported by Pretty in 1931, and for the next eight decades, most of the evidence came from isolated case reports and small series of patients.[5] A classic study series described a prevalence of between 0.07 and 1.1% among patients referred for coronary angiography.[6–8] With the standardisation of an early invasive approach in the context of acute coronary syndrome (ACS), coupled with the development of techniques, such as high-sensitivity troponin and the increased use of ICI, more cases have been diagnosed.[3] In a 2016 study, the prevalence of SCAD as the underlying substrate of ACS was approximately 4%.[9] This prevalence is higher in young- to middle-aged women (aged ≤50 years), where SCAD is the substrate for acute MI in approximately 24–35% of the cases.[10,11]
SCAD mainly affects women. In three of the largest series on SCAD, the percentage of women is around 81–96%, with a mean age at diagnosis of the index event between 45 and 52 years.[12–15]
Conditions Related to Spontaneous Coronary Artery Dissection
A long list of conditions has been related to SCAD, either as predisposing factors that make a coronary artery wall structure more prone to dissection, or as factors that precipitate acute episodes of SCAD.
Fibromuscular Dysplasia
During the last decade, the association of this condition with SCAD has received major attention. Fibromuscular dysplasia (FMD) is a non-atherosclerotic and non-inflammatory idiopathic arteriopathy. A relationship (even when not confirmed as causative) has been found between these two entities (Figure 1). Among the different series, the prevalence of FMD in patients with SCAD has ranged between 25% and 86%. This variability is explained by the differences in the type of technique used for screening and/or the number of territories screened.[13,16–18] In the first large prospective cohort published, Saw et al. reported signs of FMD in 31% of the total cohort, with this percentage rising to 57% in patients with a complete screening.[15] Some authors have described the presence of ‘stigmas’ of FMD on the coronary arteries of patients with SCAD on both angiography and ICI.[19,20] While this theory is plausible, more data are needed to corroborate these preliminary findings. The question of whether SCAD and FMD are independent, overlapping entities or manifestations of the same disorder remains unclear, although there is now evidence of a common genetic variant linking these conditions.
Figure 1: Fibromuscular Dysplasia in Spontaneous Coronary Artery Dissection.
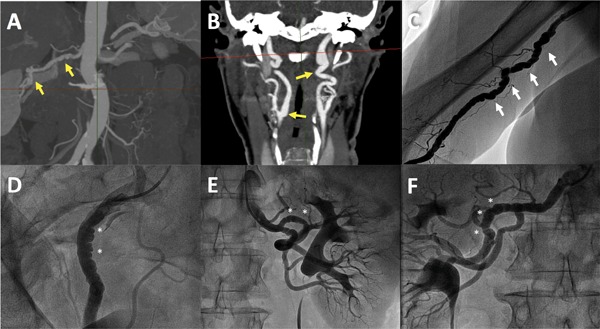
A and B: Angio-CT showing signs of multifocal fibromuscular dysplasia (FMD) with zones of stenosis alternating with dilatation in right renal artery (A) and both bilateral carotid arteries (B) in a 67-year-old woman with spontaneous coronary artery dissection (SCAD). C: Angiogram of the brachial artery confirming the typical string-of-beads appearance of multifocal FMD in a 70-year-old patient with SCAD. D-F: Selective angiograms with signs of multifocal FMD in right external iliac artery (D) and both left (E) and right (F) renal arteries in a 60-year-old woman with previous SCAD.
Collagen Vascular Disorders
Based on the first description of isolated cases of SCAD associated with some of these entities, a relationship of SCAD with some collagen vascular disorders has been proposed. Among the conditions cited in these reports are Marfan syndrome, Ehlers-Danlos syndrome, Alport syndrome and Nail-patella syndrome.[21–24] Mayo Clinic investigators tested 59 patients with diagnosis of SCAD for these genetic mutations related to collagen disorders. They found only 5% of pathogenic mutations related to collagen disorders.[25] Similarly, contemporary SCAD series systematically showed a low prevalence (1–2%) of these disorders.[13,18]
Chronic Inflammatory Systemic Diseases
SCAD has been associated with some chronic inflammatory systemic diseases. Previous case reports suggested a potential relationship between SCAD and systemic lupus erythematosus, inflammatory bowel disease and sarcoidosis.[26–33] In the Canadian registry, the prevalence of these disorders was 11.9%.[34] Furthermore, a vasculitic inflammatory mechanism, mainly mediated by eosinophils from the adventitial and peri-adventitial layers, has been suggested as the potential primary event leading to subsequent SCAD. Data from anatomopathological studies showed the presence of this peri-arterial eosinophilic infiltrate in patients with SCAD and confirmed its absence in patients with iatrogenic or traumatic dissections.[35]
Hypothyroidism
A potential association between SCAD and thyroid dysfunction (mainly hypothyroidism) has recently been suggested.[36] Theoretically, a thyroid hormone deficit might lead to a modification in the structure of the coronary artery wall, making it more prone to SCAD. In a study by Camacho et al., which included 73 patients with SCAD, the prevalence of hypothyroidism was 26%, significantly higher than that found in a matched control group of patients with ACS. Furthermore, patients with SCAD and hypothyroidism had more distal lesions and more tortuous coronary arteries. However, this association has not been yet confirmed in other studies on SCAD.
Pregnancy
Pregnancy and the peripartum period have been classically linked to an increased risk of SCAD. Based on the first descriptions of case reports, SCAD was initially considered as a peripartum condition. However, a recent series showed that peripartum SCAD (P-SCAD) is infrequent, accounting for fewer than 5% of SCAD cases.[15] On the other hand, SCAD is the main cause of acute MI during pregnancy and peripartum period.[37] A hormone-mediated mechanism, related to both progesterone and oestrogens, has been suggested. Hormonal changes during pregnancy might lead to a weakening of the coronary artery wall and, under certain circumstances, favour the SCAD mechanism. Studies have showed that women with P-SCAD are a high-risk subgroup of patients with SCAD. P-SCAD more frequently affects proximal segments and present with multi-vessel involvement.[38,39] In a recently published prospective Canadian cohort study, P-SCAD was related to a higher risk of adverse events both in hospital and within 30 days of discharge.[15]
Genetics
Apart from cases related to connective tissue disorders or FMD, it seems that SCAD is not strongly familial. To date, few studies have focused on this. Goel et al. found five cases of familial SCAD in 412 patients included in the Mayo Clinic SCAD Registry, with both dominant and recessive patterns of inheritance.[40] Recently, Adlam et al. described the first genetic variant associated with SCAD.[41] The common variant rs9349379 in the locus PHACTR1/EDN1 has been associated with FMD, SCAD, coronary artery disease and MI. In this study, patients carrying the rs9349379-A allele had an increased risk of FMD and SCAD. Even though this study is a milestone in the field of SCAD, more studies are needed to unravel the relevance of genetics in the context of SCAD.
Precipitating Factors
Several factors have been linked to the acute onset of SCAD.[5] In the Canadian cohort study, a precipitant factor was found in 57% of patients, with emotional stressors (41%) being the most frequent, followed by physical stressors (24%).[13] Data from the same cohort showed different patterns of precipitating factors in men and women with SCAD. In men, isometric physical exercise was the most frequent factor (44%), while in women it was the presence of an emotional stress (54.8%).[42]
Clinical Presentation
The proportion of patients with SCAD presenting as ST-segment elevation MI versus non-ST-segment elevation MI varies widely between different series (26-49%).[13,14,43] Other clinical presentations, such as ventricular tachycardia or ventricular fibrillation are infrequent (4–10%).[13,43] Presentation as out-of-hospital sudden cardiac death was 3% in the Italian cohort.[14] Symptoms at the time of presentation described in the Canadian cohort are fairly typical of MI, with the vast majority of patients presenting with chest pain (96%), half of them with pain radiating to left upper limb. Other symptoms, such as nausea/vomiting (24%) and sweating (21%), were frequently seen.[44]
Diagnosis
Coronary Angiography
Invasive coronary angiography is still the main technique used in the diagnosis of SCAD.[1,2] The advent of ICI revealed that a large majority of SCAD cases do not show a double lumen pattern on angiography. This finding led to a specific classification of SCAD by angiographic patterns, different from those of iatrogenic dissections induced by balloon angioplasty.[45] This classification includes three main angiographic patterns (Figure 2). Type 1 lesions are defined by the presence of a double lumen image. Type 2 lesions are defined by the presence of a lumen narrowing, with a lesion length usually over 20 mm. Type 2 lesions are classified in two subtypes: type 2a, when the distal vessel recovers the normal size; and type 2b, when the IMH extends distally to the end of the coronary artery. Last, type 3 lesions are defined by an abrupt lumen narrowing with distal vessel size recovering that limits a focal lesion (length <20 mm), mimicking an atherosclerotic lesion.
Figure 2: Angiographic Patterns in Spontaneous Coronary Artery Dissection.
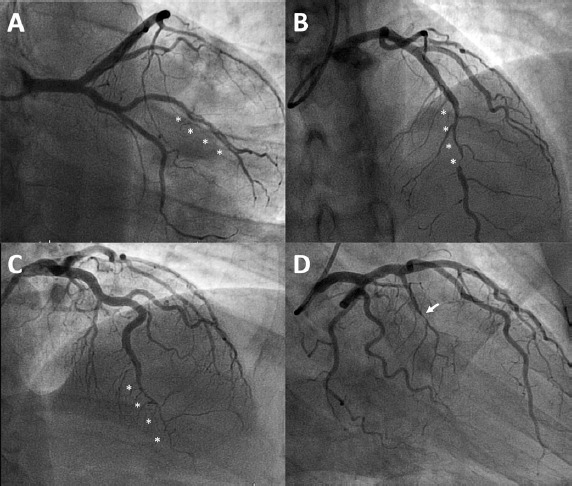
Coronary angiographic projections showing: A: an image of double lumen at first marginal branch of the left circumflex coronary artery in a 49-year-old woman compatible with type 1 spontaneous coronary artery dissection; B: a smooth stenosis at mid-left anterior descending (LAD) coronary artery with distal vessel calibre normalisation compatible with type 2a intramural haematoma; C: Smooth long stenosis from mid-to-distal LAD compatible with type 2b intramural haematoma; D: Focal stenosis at a septal branch of LAD that mimics atherosclerotic lesion compatible with type 3 spontaneous coronary artery dissection.
In the Canadian cohort (which included 168 patients with SCAD), Saw et al. observed that 67% of patients had type 2 lesions, 29% had type 1 lesions and 4% had type 3 lesions.[13] Following this, other authors have defined type 4 lesions as a total occlusion (TIMI grade flow 0) of the vessel segment on initial presentation. In this context, making a diagnosis of SCAD is complex, as it requires the presence of some signs of SCAD immediately after vessel flow restoration during percutaneous coronary intervention (PCI) or, on follow-up, after confirming the healing of the vessel with normal distal flow, having ruled out causes of coronary embolism.[46]
In addition to this angiographic classification, other angiographic characteristics have been associated with SCAD. It usually affects more distal segments than atherosclerotic disease. Furthermore, the left anterior descending coronary artery is the most frequently involved vessel. Patients with SCAD have more tortuous vessels than controls without coronary artery disease.[12] Motreff et al. described some morphological clues in SCAD.[47] First, atherosclerotic lesions are usually absent on the coronary arteries that are not affected by SCAD. Second, the start and/or end of the SCAD lesion often coincides with the presence of a sidebranch. Third, there are unique patterns described as looking like a stick insect or a radish, which are produced by external lumen compression by the IMH. Another angiographic characteristic linked to SCAD is a broken-line appearance, defined as the development of sharp angles in an otherwise tortuous but smooth coronary artery segment.[48,49] Anecdotally, the association between SCAD and segments of myocardial bridging has been described.[50]
Intracoronary Imaging
During the last few years, ICI has been found to help in the diagnosis of SCAD and in guiding PCI when this is needed. Where there is diagnostic uncertainty (e.g. where SCAD mimics atherosclerotic disease as in type 3 lesions), ICI has a unique role in confirming the diagnosis of SCAD (Figure 3). In this context, the benefits of ICI should be balanced against potential complications due to the necessity of instrumentation within an injured coronary vessel, which could make it more prone to further dissection. Compared to intravascular ultrasound (IVUS), optical coherence tomography (OCT) in this context may have some theoretical limitations due to: the necessity of contrast injection, which could potentially lead to expansion of the IMH by hydraulic pressure; and the difficulty of assessment in flow-limiting lesions.
Figure 3: Intracoronary Imaging.
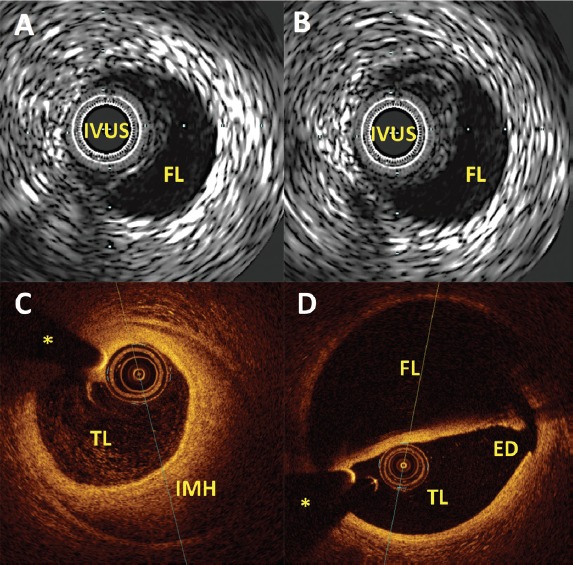
A and B: IVUS images in spontaneous coronary artery dissection, confirming the presence of the IVUS catheter within the true lumen and clearly depicting the presence of an anechoic FL; C and D: Optical coherence tomography images in spontaneous coronary artery dissection; C clearly depicts the presence of the catheter within the TL with and near 180° IMH. D: Optical coherence tomography high spatial resolution enables the clear definition of the ED of the dissection. ED = entry door; FL = false lumen; IMH = intramural haematoma; IVUS = intravascular ultrasound; TL = true lumen. *Wire artefact.
Previous studies have described the absence of complications related to the use of OCT to confirm SCAD where it was suspected from an angiographic pattern.[51] However, Jackson et al. found complications related to OCT in five out of 63 patients with SCAD, even though none of these complications led to an adverse outcome.[52] Although ICI, IVUS and OCT can be used to confirm a diagnosis of SCAD, most experts recommend OCT over IVUS, mainly because its better spatial resolution enables clinicians to determine the presence or absence and the extent of the intimo-medial flap.
Intravascular Ultrasound
The standard IVUS technology of 20-40 MHz (spatial resolution ~150 μm) allows SCAD confirmation. Because it has greater penetration than OCT, IVUS may enable a better visualisation of the entire IMH, although in-depth visualisation is not usually an issue for a condition that mostly affects distal coronary territories. However, this technique does not usually allow assessment of subtle anatomic features, such as localised fenestrations, an intimal flap or true luminal thrombus. The first description about the role of IVUS in the diagnosis and management of SCAD was published in 2008 by Arnold et al. in a small series of four SCAD patients.[53] Since then, some papers (mostly case reports and small series of patients) have described the usefulness of IVUS for: diagnostic confirmation of SCAD; as a guiding tool during PCI; and to confirm IMH has completely resolved on follow-up.[54–59] The experience with high-definition 60 MHz IVUS (with a spatial resolution closer to that of OCT) is anecdotal and limited to a case description.[60]
Optical Coherence Tomography
With its near-histological spatial resolution, OCT can detect the presence and extension of the IMH and can clearly characterise the existence of an intimo-medial flap or fenestration. Alfonso et al. first described the utility of this technique in the context of SCAD.[51] In this study, OCT was used to confirm the diagnosis in 11 out of 17 consecutive patients with clinical suspicion of SCAD. OCT proved to be able to identify the rupture site (the entry tear), visualise the intimo-medial membrane and comprehensively assess the characteristics, extent and distribution of the true and false lumen/IMH.
The technique could also be used to disclose the involvement of related side branches and the presence of thrombus in the false or the true lumen. Other studies have confirmed the utility of OCT as a diagnostic tool as well as for guiding PCI.[61–64] Jackson et al. described unique OCT findings in a larger series of 65 SCAD patients. Interestingly, OCT showed an intimo-medial dissection/fenestration in only 37% of the lesions.[52] During follow-up, OCT can be used to confirm vessel healing. Indeed, in some patients, a completely normal artery – intima, media and adventitia – can clearly be visualised, demonstrating the vessel wall has been restored to its original condition.[51]
Coronary CT Angiography
The attraction of non-invasive coronary CT angiography (CCTA) in the acute setting where SCAD is suspected is its potential for avoiding invasive procedures within a coronary artery wall prone to secondary iatrogenic dissection. However, the spatial resolution of CCTA may lead to problems in detecting SCAD lesions, which frequently affect distal segments, sometimes do not produce significant lumen stenosis and where contrast may not penetrate the false lumen. Eleid et al. reported three cases where acute CCTA failed to lead to a diagnosis of SCAD that was later on confirmed on coronary angiography.[65] The same group reported retrospective findings on CCTA of patients in the acute phase of SCAD. The most frequent findings were the presence of an abrupt luminal narrowing, followed by IMH identification (similar on CCTA analysis to non-calcified atherosclerotic plaque). However, prospective information on how CCTA compares with the gold-standard coronary angiogram in the acute setting is still lacking. Nonetheless, CCTA has emerged as a useful technique for non-invasive angiographic follow-up. Roura et al. reported results of CCTA in 24 patients with SCAD 3–6 months after the initial event. The study showed the dissection had healed in 83% of the patients.[66]
FMD Screening
Because of the association between SCAD and FMD described above, systematic screening of SCAD survivors has been recommended.[1] Nevertheless, there is still no consensus on the appropriate imaging modality or whether follow-up imaging should be contemplated. Furthermore, it remains to be confirmed whether this screening would significantly alter patient management or outcomes. Available data reflect the presence of a sensitivity gradient in the detection of FMD among different imaging techniques, including invasive angiography, computed tomography angiography (CTA) and MR angiography. The Canadian cohort initially included a high percentage of invasive angiographic screening of the renal and iliac arteries. Angiography was shown to be the most sensitive method for detecting FMD, with a prevalence in this cohort as high as 86% of patients with SCAD.[3] However, recently published data on the prospective cohort from the same group reported a lower FMD prevalence (31%), probably related to the lower percentage of patients having invasive screening (44%).[67] On the other hand, the Mayo group reported the presence of extra-coronary vascular abnormalities (EVA), including FMD, in 69% of 39 patients with SCAD, using a comprehensive CTA protocol consisting of a single study of the neck, chest, abdomen and pelvis.[68] Toggweiler et al. were the first to describe the utility of whole-body MR angiography to detect the presence of EVA in patients with SCAD, and found a 25% prevalence of renal EVA in 12 SCAD survivors.[69] The temporal evolution of FMD in patients with SCAD is still unknown; this process might be dynamic with changes over time. However, the role of long-term surveillance beyond a single FMD screening in SCAD is unknown.
Differential Diagnosis
Both atherosclerotic ACS and conditions involved in the physiopathology of MI with non-obstructive coronary arteries (MINOCA) should be included in the differential diagnosis of SCAD.[70–72] Similarities and disparities between SCAD and these conditions are summarised in Table 1.
Table 1: Differential Diagnoses of Spontaneous Coronary Artery Dissection.
| Similarities | Differences | |
|---|---|---|
| Atherosclerotic acute coronary syndrome |
|
|
| Takotsubo cardiomyopathy |
|
|
| Coronary embolism |
|
|
| Coronary spasm |
|
|
Acute Management
Medical Therapies
Until recently, the treatment frequently adopted in SCAD had been essentially the same as that recommended for ACS due to atherosclerotic disease. With the previously described underlying physiopathology (basically involving a weaker coronary artery wall and a primary bleeding event leading to an IMH), the rationale for potent antiplatelet therapy and lipid-lowering drugs seems unclear. On the other hand, some hypothesis-generating observational data has suggested that some medications may modify the risk of recurrences in SCAD survivors.
Thrombolysis, Antiplatelet and Anticoagulant Agents
Information about safety and efficacy of thrombolysis in the context of SCAD is lacking and mostly comes from isolated case reports, ranging from successful results to dissection extension and even coronary rupture.[73–76] It seems reasonable to avoid thrombolytic therapy where SCAD is suspected, as the European Society of Cardiology-Acute Cardiovascular Care Association position paper recommends.[1]
The use of antiplatelet therapies and the duration of therapy are still controversial. The rationale to add dual antiplatelet therapy in the specific context of SCAD is based on the idea of the existence of the associated thrombus within the true lumen in selected SCAD cases. A previous study reported the presence of thrombus within the true lumen in three out of 11 OCT-confirmed SCAD cases.[51] Recent data on a larger cohort of SCAD patients with OCT seem to corroborate these findings, showing the presence of some amount of thrombus in the true lumen in 36% of fenestrated and 14% of non-fenestrated SCAD lesions.[52] However, it is hard to justify that this usually tiny amount of intraluminal thrombus may play a major role in SCAD-related ischaemia. On the contrary, the thrombus probably plays a minor role as an epiphenomenon in SCAD. Some authors still recommend dual antiplatelet therapy (with aspirin plus clopidogrel) during the acute phase with continuing life-long aspirin therapy in conservatively managed SCAD patients. In patients where PCI with stent implantation is performed, 12-month dual antiplatelet therapy (avoiding potent P2Yrs other than clopidogrel) is recommended by current guidelines.[77] More information about different regimens and duration of dual antiplatelet therapy is needed.
Data on the use of anticoagulant therapy in the context of SCAD are lacking. In the context of ACS (a common presentation of SCAD), anticoagulant therapy with heparin or fondaparinux should be discontinued as soon as the diagnosis of SCAD is confirmed in the absence of any other indication for anticoagulant therapy.[2]
Statins
The rationale for lipid-lowering therapies in a condition not related to cholesterol deposition seems weak. Furthermore, retrospective data from the Mayo Clinic group even suggest a slightly higher risk of recurrence in patients taking statins.[78] Current guidelines recommend treatment with statins only for primary prevention.[1,2]
Beta-blockers
The potential benefit of beta-blockers in SCAD has been extrapolated from experience in acute aortic dissection and atherosclerotic-ACS. Moreover, data from a large cohort showed a lower risk of recurrences in SCAD survivors taking beta-blockers.[34] Based on this observational data, most experts recommend long-term treatment with beta-blockers for SCAD survivors.[2]
Revascularisation
Conservative Management
Observational data shows that most patients with SCAD have a benign clinical course when managed with a conservative, watchful waiting strategy without PCI.[3] This is coupled with the evidence of a high percentage of complete vessel healing at follow-up in SCAD survivors. The Canadian group described spontaneous healing in all 79 SCAD patients who had a repeat angiogram ≥26 days after the index event.[13] The same group has recently reported angiographic healing in 86% of SCAD lesions, a percentage that increased to 95% in patients who had a repeat angiogram >30 days after the event.[79] These findings, combined with reported high rates of complications and suboptimal results with PCI, lead to the current recommendation of conservative management in the absence of recurrent or ongoing ischaemia, high-risk anatomy or haemodynamic/electric instability.[1,2,43,67]
Percutaneous Coronary Interventions
While conservative management constitutes the preferred approach in the majority of SCAD patients, PCI may be required in some specific situations such as in the presence of ongoing or recurrent ischaemia, total vessel occlusion, haemodynamic/electric instability or high-risk anatomies where a great territory is at risk (as with left main or proximal involvement). PCI has poorer results in the treatment of SCAD than in atherosclerotic disease. The Mayo Clinic cohort study described a 53% rate of procedural PCI failure.[43] In the prospective Canadian cohort, 30% of PCI procedures were unsuccessful.[15] Furthermore, these interventions in weaker coronary artery walls have been associated with an increased risk of iatrogenic dissections or IMH propagation.[80,81]
Many strategies have been postulated as the preferable technique in the context of SCAD. However, head-to-head studies comparing different strategies have not been performed. With the high rate of total healing described above, a more conservative approach with the objective of restoring the distal coronary flow may be potentially beneficial. Thereby, in some cases, gentle, low-calibre balloon angioplasty can be enough to restore distal flow, avoiding the implantation of a permanent metallic layer in a young patient with no significant atherosclerotic burden. This is also the rationale underlying the isolated use of scoring or cuttings balloons to fenestrate the IMH, with the aim of reducing the compression of the true lumen.[58,82] When stent implantation is considered, it seems reasonable to use current generation drug-eluting stents (DES) over bare metal stents. In this regard, Conrotto et al. analysed the results of DES versus bare metal stents in 238 patients with SCAD.[83] The DES group showed a non-significant trend towards a lower primary endpoint, that was mainly driven by a reduction in target vessel revascularisation.
The use of bioresorbable scaffolds (BRS) in the context of SCAD has clear appeal. The gradual and complete resorption of scaffolds over time would avoid the presence of a permanent metal layer when the coronary vessel wall is completely healed and, potentially, would obviate the risk of very-late device restenosis or thrombosis. A small series showed the good performance of first-generation BRS in the context of SCAD on mid- to long-follow-up.[84,85] However, these first-generation poly-L-lactide acid-based BRS are no longer available, owing to the observed higher incidence of thrombosis compared with second-generation, everolimus DES. Data on other BRS, such as as magnesium BRS, are still anecdotical.[86,87] Table 2 summarises several suggestions to avoid complications in SCAD PCI.
Table 2: Suggestions to Avoid Complications During Percutaneous Coronary Interventions in Spontaneous Coronary Artery Dissection.
|
|
|
|
|
|
|
|
|
|
Coronary Artery Bypass Grafting
Coronary artery bypass grafting may be necessary in the context of PCI failure with ongoing ischaemia and in some high-risk anatomic scenarios such as left main or multi-vessel proximal involvement. To date, available data on the results of bypass grafting in SCAD is limited to small case series. In general, these series described good acute results.[43,88,89] Of note, the Mayo Clinic paper showed a high prevalence (~70%) of late bypass graft occlusion, presumably due to competitive flow from the healed native coronary vessel.[43]
Exercise Recommendations and Cardiac Rehabilitation
Because of the association between SCAD episodes and acute physical stressors (especially isometric physical exercise) acting as a precipitating factor, concern has arisen about the prescription of physical activity in SCAD survivors. In the absence of robust data, it seems reasonable to keep an active lifestyle after SCAD, avoiding high-intensity exercise and competitive sports.[2] However, case reports have showed excellent outcomes in patients resuming high-intensity competitive sport activity.[90] The current American Heart Association statement recommends that all SCAD survivors should be referred to a cardiac rehabilitation programme.[2] In the absence of robust evidence of the prognostic benefit of cardiac rehabilitation on SCAD, Krittanawong et al. demonstrated that cardiac rehabilitation after SCAD is safe and reported physical and emotional benefits in a majority of SCAD survivors.[91]. The Canadian group also reported benefits of a specific SCAD rehabilitation program in the first 70 SCAD patients referred in terms of less chest pain, higher exercise capacity, better performance on depression questionnaires and a reduced incidence of major adverse cardiovascular events (MACE) on follow-up.[92]
Pregnancy in SCAD Survivors
Data evaluating the risk of SCAD recurrence with future pregnancies is scarce. To date, only one small series describes one pregnancy-related recurrence among eight SCAD survivors at a median follow-up of 36 months.[93] With this limited data, it does not seem reasonable to give a general recommendation to SCAD survivors to avoid pregnancy. Pregnancy after SCAD should be considered high risk, and patients should be closely monitored and receive adequate information about the potential increased risk of SCAD recurrence associated with pregnancy.
Follow-up: Prognosis and Risk of Recurrences
Reported mortality in SCAD is generally low. The Mayo Clinic group reported a 10-year mortality of 7.7% after SCAD.[78] The Canadian group described a 1.2% mortality at median follow-up of 3.1 years.[34] Lettieri et al. described a 5.6% 6-year mortality after SCAD.[14] In the Japanese series, the mortality rate was 1.6% at median follow-up of 2.8 years.[10] However, morbidity is significant after SCAD. Saw et al. described in-hospital major adverse events in 8.8% of 750 SCAD patients.[67] The composite was mainly driven by recurrent MI (4%), severe ventricular arrhythmia (4%) and unplanned revascularisation (3%). Overall, 30-day MACE in the same series was 8.8%, driven by recurrent MI (6%) and unplanned revascularisation (3%). In a previous paper by the same group with a longer follow-up, the overall MACE rate was 19.9% at median follow-up at 3.1 years, mostly driven by recurrent MI (16.8%) and recurrent SCAD (10.4%).[34] The Mayo Clinic group reported a 10-year rate of MACE as high as 47.4%, with 17% rate of recurrence during a median follow-up of 3.9 years.[78] Lettieri et al. described a 6-year MACE rate of 14.6%, driven by recurrent MI (5.2%) and repeated revascularisation (4.6%).[14] In the paper by Nakashima et al., the 5-year MACE rate was 37%, with 22% SCAD recurrence at median follow-up of 2.8 years.[10] Observational data by Saw et al. found that hypertension and beta-blocker treatment seem to modify the risk of recurrence.[34] Eleid et al. noted that increased coronary tortuosity might be associated with a higher risk of recurrence.[12]
Patient Groups
Recently, due to a greater awareness of this condition, SCAD survivor groups have been set up. Initiatives such as Beat SCAD (https://beatscad.org.uk) in the UK or SCAD Alliance (https://www.scadalliance.org) in North America support patients and families affected by the condition.
Conclusion
SCAD is nowadays a well-known cause of ACS. Despite great advances in the recognition of this elusive disease in the last few years, significant gaps remain in our knowledge of the physiopathology, diagnosis, management and prognosis of this condition. In a sporadic and infrequent clinical entity such as SCAD (where randomised clinical trials are unlikely), information from further prospective registries and collaborative studies are required to advance in the knowledge of this fascinating condition.
References
- 1.Adlam D, Alfonso F, Maas A European Society of Cardiology, Acute Cardiovascular Care Association, SCAD study group: a position paper on spontaneous coronary artery dissection. Eur Heart J. 2018. pp. 3353–68. [DOI] [PMC free article] [PubMed]
- 2.Hayes SN, Kim CESH, Saw J et al. Spontaneous coronary artery dissection: current state of the science: a scientific statement from the American Heart Association. Circulation. 2018;137:e523–57. doi: 10.1161/CIR.0000000000000564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Saw J, Mancini GBJ, Humphries KH. Contemporary review on spontaneous coronary artery dissection. J Am Coll Cardiol. 2016;68:297–312. doi: 10.1016/j.jacc.2016.05.034. [DOI] [PubMed] [Google Scholar]
- 4.Waterbury TM, Tweet MS, Hayes SN et al. Early natural history of spontaneous coronary artery dissection. Circ Cardiovasc Interv. 2018;11:e006772. doi: 10.1161/CIRCINTERVENTIONS.118.006772. [DOI] [PubMed] [Google Scholar]
- 5.Pretty HC. Dissecting aneurysm of coronary artery in a woman aged 42: rupture. Br Med J. 1931;1:667. [Google Scholar]
- 6.Hering D, Piper C, Hohmann C et al. Prospective study of the incidence, pathogenesis and therapy of spontaneous, by coronary angiography diagnosed coronary artery dissection. Zeitschrift für Kardiol. 1998;87:961–70. doi: 10.1007/s003920050253. [in German] [DOI] [PubMed] [Google Scholar]
- 7.Vanzetto G, Berger-Coz E, Barone-Rochette G et al. Prevalence, therapeutic management and medium-term prognosis of spontaneous coronary artery dissection: results from a database of 11,605 patients. Eur J Cardio-Thoracic Surg. 2009;35:250–4. doi: 10.1016/j.ejcts.2008.10.023. [DOI] [PubMed] [Google Scholar]
- 8.Mortensen KH, Thuesen L, Kristensen IB, Christiansen EH. Spontaneous coronary artery dissection: a Western Denmark Heart Registry Study. Catheter Cardiovasc Interv. 2009;74:710–7. doi: 10.1002/ccd.22115. [DOI] [PubMed] [Google Scholar]
- 9.Nishiguchi T, Tanaka A, Ozaki Y et al. Prevalence of spontaneous coronary artery dissection in patients with acute coronary syndrome. Eur Hear J Acute Cardiovasc Care. 2016;5:263–70. doi: 10.1177/2048872613504310. [DOI] [PubMed] [Google Scholar]
- 10.Nakashima T, Noguchi T, Haruta S et al. Prognostic impact of spontaneous coronary artery dissection in young female patients with acute myocardial infarction: a report from the Angina Pectoris-Myocardial Infarction Multicenter Investigators in Japan. Int J Cardiol. 2016;207:341–8. doi: 10.1016/j.ijcard.2016.01.188. [DOI] [PubMed] [Google Scholar]
- 11.Saw J, Aymong E, Mancini GBJ et al. Nonatherosclerotic coronary artery disease in young women. Can J Cardiol. 2014;30:814–19. doi: 10.1016/j.cjca.2014.01.011. [DOI] [PubMed] [Google Scholar]
- 12.Eleid MF, Guddeti RR, Tweet MS et al. Coronary artery tortuosity in spontaneous coronary artery dissection angiographic characteristics and clinical implications. Circ Cardiovasc Interv. 2014;7:656–62. doi: 10.1161/CIRCINTERVENTIONS.114.001676. [DOI] [PubMed] [Google Scholar]
- 13.Saw J, Aymong E, Sedlak T et al. Spontaneous coronary artery dissection association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ Cardiovasc Interv. 2014;7:645–55. doi: 10.1161/CIRCINTERVENTIONS.114.001760. [DOI] [PubMed] [Google Scholar]
- 14.Lettieri C, Zavalloni D, Rossini R et al. Management and long-term prognosis of spontaneous coronary artery dissection. Am J Cardiol. 2015;116:66–73. doi: 10.1016/j.amjcard.2015.03.039. [DOI] [PubMed] [Google Scholar]
- 15.Saw J, Starovoytov A, Humphries K et al. Canadian spontaneous coronary artery dissection cohort study: in-hospital and 30-day outcomes. Eur Heart J. 2019;40:1188–97. doi: 10.1093/eurheartj/ehz007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Saw J, Ricci D, Starovoytov A et al. Spontaneous coronary artery dissection: prevalence of predisposing conditions including fibromuscular dysplasia in a tertiary center cohort. JACC Cardiovasc Interv. 2013;6:44–52. doi: 10.1016/j.jcin.2012.08.017. [DOI] [PubMed] [Google Scholar]
- 17.Rogowski S, Maeder MT, Weilenmann D et al. Spontaneous coronary artery dissection: angiographic follow-up and long-term clinical outcome in a predominantly medically treated population. Catheter Cardiovasc Interv. 2017;89:59–68. doi: 10.1002/ccd.26383. [DOI] [PubMed] [Google Scholar]
- 18.Prasad M, Tweet MS, Hayes SN et al. Prevalence of extracoronary vascular abnormalities and fibromuscular dysplasia in patients with spontaneous coronary artery dissection. Am J Cardiol. 2015;115:1672–77. doi: 10.1016/j.amjcard.2015.03.011. [DOI] [PubMed] [Google Scholar]
- 19.Michelis KC, Olin JW, Kadian-Dodov D et al. Coronary artery manifestations of fibromuscular dysplasia. J Am Coll Cardiol. 2014;64:1033–46. doi: 10.1016/j.jacc.2014.07.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Saw J, Bezerra H, Gornik HL et al. Angiographic and intracoronary manifestations of coronary fibromuscular dysplasia. Circulation. 2016;133:1548–59. doi: 10.1161/CIRCULATIONAHA.115.020282. [DOI] [PubMed] [Google Scholar]
- 21.Sato C, Wakabayashi K, Suzuki H. Natural course of isolated spontaneous coronary artery dissection in Marfan syndrome. Int J Cardiol. 2014;177:20–2. doi: 10.1016/j.ijcard.2014.09.061. [DOI] [PubMed] [Google Scholar]
- 22.Nakamura M, Yajima J, Oikawa Y et al. Vascular Ehlers-Danlos syndrome – all three coronary artery spontaneous dissections. J Cardiol. 2009;53:458–62. doi: 10.1016/j.jjcc.2008.09.007. [DOI] [PubMed] [Google Scholar]
- 23.Anuwatworn A, Sethi P, Steffen K et al. Spontaneous coronary artery dissection: a rare manifestation of Alport syndrome. Case Rep Cardiol. 2017;2017:1–3. doi: 10.1155/2017/1705927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nizamuddin SL, Broderick DK, Minehart RD, Kamdar BB. Spontaneous coronary artery dissection in a parturient with Nail-Patella syndrome. Int J Obstet Anesth. 2015;24:69–73. doi: 10.1016/j.ijoa.2014.07.010. [DOI] [PubMed] [Google Scholar]
- 25.Henkin S, Negrotto SM, Tweet MS et al. Spontaneous coronary artery dissection and its association with heritable connective tissue disorders. Heart. 2016;102:876–81. doi: 10.1136/heartjnl-2015-308645. [DOI] [PubMed] [Google Scholar]
- 26.Nisar MK, Mya T. Spontaneous coronary artery dissection in the context of positive anticardiolipin antibodies and clinically undiagnosed systemic lupus erythematosus. Lupus. 2011;20:1436–38. doi: 10.1177/0961203311406765. [DOI] [PubMed] [Google Scholar]
- 27.Rekik S, Lanfranchi P, Jacq L, Bernasconi F. Spontaneous coronary artery dissection in a 35 year-old woman with systemic lupus erythematosus successfully treated by angioplasty. Heart Lung Circ. 2013;22:955–8. doi: 10.1016/j.hlc.2013.01.015. [DOI] [PubMed] [Google Scholar]
- 28.Reddy S, Vaid T, Ganiga Sanjeeva NC, Shetty RK. Spontaneous coronary artery dissection as the first presentation of systemic lupus erythematosus. BMJ Case Rep. 2016;2016:bcr2016216344. doi: 10.1136/bcr-2016-216344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kothari D, Ruygrok P, Gentles T, Occleshaw C. Spontaneous coronary artery dissection in an adolescent man with systemic lupus erythematosus. Intern Med J. 2007;37:342–3. doi: 10.1111/j.1445-5994.2007.01345.x. [DOI] [PubMed] [Google Scholar]
- 30.Sharma AK, Farb A, Maniar P et al. Spontaneous coronary artery dissection in a patient with systemic lupus erythematosis. Hawaii Med J. 2003;62:248–53. [PubMed] [Google Scholar]
- 31.Aldoboni AH, Hamza EA, Majdi K et al. Spontaneous dissection of coronary artery treated by primary stenting as the first presentation of systemic lupus erythematosus. J Invasive Cardiol. 2002;14:694–6. [PubMed] [Google Scholar]
- 32.Kanaroglou S, Nair V, Fernandes JR. Sudden cardiac death due to coronary artery dissection as a complication of cardiac sarcoidosis. Cardiovasc Pathol. 2015;24:244–6. doi: 10.1016/j.carpath.2015.01.001. [DOI] [PubMed] [Google Scholar]
- 33.Srinivas M, Basumani P, Muthusamy R, Wheeldon N. Active inflammatory bowel disease and coronary artery dissection. Postgrad Med J. 2005;81:68–70. doi: 10.1136/pgmj.2004.018952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Saw J, Humphries K, Aymong E et al. Spontaneous coronary artery dissection: clinical outcomes and risk of recurrence. J Am Coll Cardiol. 2017;70:1148–58. doi: 10.1016/j.jacc.2017.06.053. [DOI] [PubMed] [Google Scholar]
- 35.Pitliya A, Datta S, Kalayci A et al. Eosinophilic inflammation in spontaneous coronary artery dissection: a potential therapeutic target? Med Hypotheses. 2018;121:91–4. doi: 10.1016/j.mehy.2018.09.039. [DOI] [PubMed] [Google Scholar]
- 36.Camacho Freire SJ, Díaz Fernández JF, Gheorghe LL et al. Spontaneous coronary artery dissection and hypothyroidism. Rev Española Cardiol (Eng Ed) 2019;72:625–33. doi: 10.1016/j.rec.2018.06.031. [DOI] [PubMed] [Google Scholar]
- 37.Elkayam U, Jalnapurkar S, Barakkat MN et al. Pregnancy-associated acute myocardial infarction: a review of contemporary experience in 150 cases between 2006 and 2011. Circulation. 2014;129:1695–702. doi: 10.1161/CIRCULATIONAHA.113.002054. [DOI] [PubMed] [Google Scholar]
- 38.Tweet MS, Hayes SN, Codsi E et al. Spontaneous coronary artery dissection associated with pregnancy. J Am Coll Cardiol. 2017;70:426–35. doi: 10.1016/j.jacc.2017.05.055. [DOI] [PubMed] [Google Scholar]
- 39.Havakuk O, Goland S, Mehra A, Elkayam U. Pregnancy and the risk of spontaneous coronary artery dissection: an analysis of 120 contemporary cases. Circ Cardiovasc Interv. 2017;10:1–13. doi: 10.1161/CIRCINTERVENTIONS.117.004941. [DOI] [PubMed] [Google Scholar]
- 40.Goel K, Tweet M, Olson TM et al. Familial spontaneous coronary artery dissection. JAMA Intern Med. 2015;175:821. doi: 10.1001/jamainternmed.2014.8307. [DOI] [PubMed] [Google Scholar]
- 41.Adlam D, Olson TM, Combaret N et al. Association of the PHACTR1/EDN1 genetic locus with spontaneous coronary artery dissection. J Am Coll Cardiol. 2019;73:58–66. doi: 10.1016/j.jacc.2018.09.085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Fahmy P, Prakash R, Starovoytov A et al. Pre-disposing and precipitating factors in men with spontaneous coronary artery dissection. JACC Cardiovasc Interv. 2016;9:866–8. doi: 10.1016/j.jcin.2016.02.024. [DOI] [PubMed] [Google Scholar]
- 43.Tweet MS, Eleid MF, Best PJM et al. Spontaneous coronary artery dissection: revascularization versus conservative therapy. Circ Cardiovasc Interv. 2014;7:777–86. doi: 10.1161/CIRCINTERVENTIONS.114.001659. [DOI] [PubMed] [Google Scholar]
- 44.Luong C, Starovoytov A, Heydari M et al. Clinical presentation of patients with spontaneous coronary artery dissection. Catheter Cardiovasc Interv. 2017;89:1149–54. doi: 10.1002/ccd.26977. [DOI] [PubMed] [Google Scholar]
- 45.Saw J. Coronary angiogram classification of spontaneous coronary artery dissection. Catheter Cardiovasc Interv. 2014;84:1115–22. doi: 10.1002/ccd.25293. [DOI] [PubMed] [Google Scholar]
- 46.Al-Hussaini A, Adlam D. Spontaneous coronary artery dissection. Heart. 2017;103:1043–51. doi: 10.1136/heartjnl-2016-310320. [DOI] [PubMed] [Google Scholar]
- 47.Motreff P, Malcles G, Combaret N et al. How and when to suspect spontaneous coronary artery dissection: novel insights from a single-centre series on prevalence and angiographic appearance. EuroIntervention. 2017;12:e2236–43. doi: 10.4244/EIJ-D-16-00187. [DOI] [PubMed] [Google Scholar]
- 48.Alfonso F, Bastante T. Spontaneous coronary artery dissection: novel diagnostic insights from large series of patients. Circ Cardiovasc Interv. 2014;7:638–41. doi: 10.1161/CIRCINTERVENTIONS.114.001984. [DOI] [PubMed] [Google Scholar]
- 49.Alfonso F. Spontaneous coronary artery dissection. Circulation. 2012;126:667–70. doi: 10.1161/CIRCULATIONAHA.112.122093. [DOI] [PubMed] [Google Scholar]
- 50.De-Giorgio F, Grassi VM, Abbate A et al. Causation or coincidence? A case of sudden death due to spontaneous coronary artery dissection in presence of myocardial bridging. Int J Cardiol. 2012;159:e32–4. doi: 10.1016/j.ijcard.2011.11.056. [DOI] [PubMed] [Google Scholar]
- 51.Alfonso F, Paulo M, Gonzalo N et al. Diagnosis of spontaneous coronary artery dissection by optical coherence tomography. J Am Coll Cardiol. 2012;59:1073–9. doi: 10.1016/j.jacc.2011.08.082. [DOI] [PubMed] [Google Scholar]
- 52.Jackson R, Al-Hussaini A, Joseph S et al. Spontaneous coronary artery dissection. JACC Cardiovasc Imaging. 2019;12:2475–88. doi: 10.1016/j.jcmg.2019.01.015. [DOI] [PubMed] [Google Scholar]
- 53.Arnold JR, West NE, van Gaal WJ et al. The role of intravascular ultrasound in the management of spontaneous coronary artery dissection. Cardiovasc Ultrasound. 2008;6:24. doi: 10.1186/1476-7120-6-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Kalra A, Aggarwal A, Kneeland R, Traverse JH. Percutaneous coronary intervention in spontaneous coronary artery dissection: role of intravascular ultrasound. Cardiol Ther. 2014;3:61–6. doi: 10.1007/s40119-014-0029-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Mahmood MM, Austin D. IVUS and OCT guided primary percutaneous coronary intervention for spontaneous coronary artery dissection with bioresorbable vascular scaffolds. Cardiovasc Revasc Med. 2017;18:53–7. doi: 10.1016/j.carrev.2016.09.005. [DOI] [PubMed] [Google Scholar]
- 56.Paulo M, Sandoval J, Lennie V et al. Combined use of OCT and IVUS in spontaneous coronary artery dissection. JACC Cardiovasc Imaging. 2013;6:830–2. doi: 10.1016/j.jcmg.2013.02.010. [DOI] [PubMed] [Google Scholar]
- 57.Cerrato E, Tomassini F, Rolfo C et al. Spontaneous coronary artery dissection treated with biovascular scaffolds guided by intravascular ultrasounds imaging. Cardiovasc Interv Ther. 2017;32:186–9. doi: 10.1007/s12928-016-0391-3. [DOI] [PubMed] [Google Scholar]
- 58.Ito T, Shintani Y, Ichihashi T et al. Non-atherosclerotic spontaneous coronary artery dissection revascularized by intravascular ultrasonography-guided fenestration with cutting balloon angioplasty. Cardiovasc Interv Ther. 2017;32:241–3. doi: 10.1007/s12928-016-0397-x. [DOI] [PubMed] [Google Scholar]
- 59.Tsutsui H, Chino C, Komatsu M et al. Resolution of spontaneous coronary artery dissection within 3 weeks detected by computed tomography angiography and intravascular ultrasound. Cardiovasc Interv Ther. 2017;32:77–81. doi: 10.1007/s12928-015-0373-x. [DOI] [PubMed] [Google Scholar]
- 60.Song L, Mintz GS, Kadohira T et al. Spontaneous coronary artery dissection with intra-adventitial hematoma detected by high-definition intravascular ultrasound. Coron Artery Dis. 2016;27:707–8. doi: 10.1097/MCA.0000000000000427. [DOI] [PubMed] [Google Scholar]
- 61.Garcia-Guimaraes M, Bastante T, Cuesta J et al. Multifaceted presentation of recurrent spontaneous coronary artery dissection: angiography and optical coherence tomography findings. Circ Cardiovasc Interv. 2017;10:e004696. doi: 10.1161/CIRCINTERVENTIONS.116.004696. [DOI] [PubMed] [Google Scholar]
- 62.Fabris E, Kennedy MW, Sinagra G et al. Optical coherence tomography for strategy planning and staged optimization of spontaneous coronary artery dissection. Eur Hear J Cardiovasc Imaging. 2017;18:939. doi: 10.1093/ehjci/jex058. [DOI] [PubMed] [Google Scholar]
- 63.Ramalho AR, Silva Marques J, Oliveira Santos M, Matos V. Optical coherence tomography-guided full plastic jacket in spontaneous coronary artery dissection. JACC Cardiovasc Interv. 2017;10:413–14. doi: 10.1016/j.jcin.2016.10.028. [DOI] [PubMed] [Google Scholar]
- 64.Nishiguchi T, Tanaka A, Taruya A et al. Prognosis of spontaneous coronary artery dissection treated by percutaneous coronary intervention with optical coherence tomography. J Cardiol. 2017;70:524–9. doi: 10.1016/j.jjcc.2017.03.009. [DOI] [PubMed] [Google Scholar]
- 65.Eleid MF, Tweet MS, Young PM et al. Spontaneous coronary artery dissection: challenges of coronary computed tomography angiography. Eur Hear J Acute Cardiovasc Care. 2017;7:609–13. doi: 10.1177/2048872616687098. [DOI] [PubMed] [Google Scholar]
- 66.Roura G, Ariza-Solé A, Rodriguez-Caballero IF et al. Noninvasive follow-up of patients with spontaneous coronary artery dissection with CT angiography. JACC Cardiovasc Imaging. 2016;9:896–7. doi: 10.1016/j.jcmg.2015.06.011. [DOI] [PubMed] [Google Scholar]
- 67.Saw J, Starovoytov A, Humphries K et al. Canadian spontaneous coronary artery dissection cohort study: in-hospital and 30-day outcomes. Eur Heart J. 2019;40:1188–97. doi: 10.1093/eurheartj/ehz007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Liang JJ, Prasad M, Tweet MS et al. A novel application of CT angiography to detect extracoronary vascular abnormalities in patients with spontaneous coronary artery dissection. J Cardiovasc Comput Tomogr. 2014;8:189–97. doi: 10.1016/j.jcct.2014.02.001. [DOI] [PubMed] [Google Scholar]
- 69.Toggweiler S, Puck M, Thalhammer C et al. Associated vascular lesions in patients with spontaneous coronary artery dissection. Swiss Med Wkly. 2012;142:w13538. doi: 10.4414/smw.2012.13538. [DOI] [PubMed] [Google Scholar]
- 70.Niccoli G, Scalone G, Crea F. Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management. Eur Heart J. 2015;36:475–81. doi: 10.1093/eurheartj/ehu469. [DOI] [PubMed] [Google Scholar]
- 71.Agewall S, Beltrame JF, Reynolds HR et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J. 2017;38:143–53. doi: 10.1093/eurheartj/ehw149. [DOI] [PubMed] [Google Scholar]
- 72.Duran JM, Naderi S, Vidula M Spontaneous coronary artery dissection and its association with takotsubo syndrome: Novel insights from a tertiary center registry. Catheter Cardiovasc Interv. 2019. epub ahead of press. [DOI] [PubMed]
- 73.Siddiqui F, Briasoulis A, Siddiqui S et al. Spontaneous distal right coronary artery dissection in a patient with massive pulmonary embolism. Am J Ther. 2016;23:e249–51. doi: 10.1097/MJT.0000000000000108. [DOI] [PubMed] [Google Scholar]
- 74.Leclercq F, Messner-Pellenc P, Carabasse D et al. Successful thrombolysis treatment of a spontaneous left main coronary artery dissection without subsequent surgery. Eur Heart J. 1996;17:320–1. doi: 10.1093/oxfordjournals.eurheartj.a014853. [DOI] [PubMed] [Google Scholar]
- 75.Andreou AY, Georgiou PA, Georgiou GM. Spontaneous coronary artery dissection: report of two unsuspected cases initially treated with thrombolysis. Exp Clin Cardiol. 2009;14:e89–92. [PMC free article] [PubMed] [Google Scholar]
- 76.Jović Z, Obradović S, Djenić N et al. Does thrombolytic therapy harm or help in ST elevation myocardial infarction (STEMI) caused by the spontaneous coronary dissection? Vojnosanit Pregl. 2015;72:536–40. doi: 10.2298/VSP1506536J. [DOI] [PubMed] [Google Scholar]
- 77.Valgimigli M, Bueno H, Byrne RA et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur Heart J. 2018;39:213–60. doi: 10.1093/eurheartj/ehx419. [DOI] [PubMed] [Google Scholar]
- 78.Tweet MS, Hayes SN, Pitta SR et al. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation. 2012;126:579–88. doi: 10.1161/CIRCULATIONAHA.112.105718. [DOI] [PubMed] [Google Scholar]
- 79.Hassan S, Prakash R, Starovoytov A, Saw J. Natural history of spontaneous coronary artery dissection with spontaneous angiographic healing. JACC Cardiovasc Interv. 2019;12:518–27. doi: 10.1016/j.jcin.2018.12.011. [DOI] [PubMed] [Google Scholar]
- 80.Prakash R, Starovoytov A, Heydari M et al. Catheter-induced iatrogenic coronary artery dissection in patients with spontaneous coronary artery dissection. JACC Cardiovasc Interv. 2016;9:1851–3. doi: 10.1016/j.jcin.2016.06.026. [DOI] [PubMed] [Google Scholar]
- 81.García-Guimaraes M, Bastante T, Cuesta J, Alfonso F. Hybrid percutaneous treatment of iatrogenic coronary artery dissection complicating a spontaneous coronary artery dissection. EuroIntervention. 2018;14:e1038–9. doi: 10.4244/EIJ-D-18-00035. [DOI] [PubMed] [Google Scholar]
- 82.Alkhouli M, Cole M, Ling FS. Coronary artery fenestration prior to stenting in spontaneous coronary artery dissection. Catheter Cardiovasc Interv. 2016;88:E23–7. doi: 10.1002/ccd.26161. [DOI] [PubMed] [Google Scholar]
- 83.Conrotto F, D’Ascenzo F, Cerrato E et al. Safety and efficacy of drug eluting stents in patients with spontaneous coronary artery dissection. Int J Cardiol. 2017;238:105–9. doi: 10.1016/j.ijcard.2017.03.027. [DOI] [PubMed] [Google Scholar]
- 84.Ielasi A, Cortese B, Tarantini G et al. Sealing spontaneous coronary artery dissection with bioresorbable vascular scaffold implantation: data from the prospective “registro Absorb Italiano” (RAI Registry) Int J Cardiol. 2016;212:44–6. doi: 10.1016/j.ijcard.2016.03.043. [DOI] [PubMed] [Google Scholar]
- 85.Macaya F, Salinas P, Gonzalo N et al. Long-term follow-up of spontaneous coronary artery dissection treated with bioresorbable scaffolds. EuroIntervention. 2019;14:1403–5. doi: 10.4244/EIJ-D-18-00519. [DOI] [PubMed] [Google Scholar]
- 86.Quadri G, Tomassini F, Cerrato E, Varbella F. First reported case of magnesium-made bioresorbable scaffold to treat spontaneous left anterior descending coronary artery dissection. Catheter Cardiovasc Interv. 2017;90:768–72. doi: 10.1002/ccd.27214. [DOI] [PubMed] [Google Scholar]
- 87.Quadri G, Cerrato E, Rolfo C, Varbella F. Spontaneous coronary artery dissection treated with magnesium-made bioresorbable scaffold: 1-year angiographic and optical coherence tomography follow-up. Catheter Cardiovasc Interv. 2019;93:E130–3. doi: 10.1002/ccd.27971. [DOI] [PubMed] [Google Scholar]
- 88.Vanzetto G, Berger-Coz E, Barone-Rochette G et al. Prevalence, therapeutic management and medium-term prognosis of spontaneous coronary artery dissection: results from a database of 11,605 patients. Eur J Cardiothorac Surg. 2009;35:250–4. doi: 10.1016/j.ejcts.2008.10.023. [DOI] [PubMed] [Google Scholar]
- 89.Unal M, Korkut AK, Kosem M et al. Surgical management of spontaneous coronary artery dissection. Texas Heart Inst J. 2008;35:402–5. [PMC free article] [PubMed] [Google Scholar]
- 90.Weber N, Weber A, Carbone P et al. High-intensity, sport-specific cardiac rehabilitation training of a 22-year-old competitive cyclist after spontaneous coronary artery dissection. Proc (Bayl Univ Med Cent) 2018;31:207–9. doi: 10.1080/08998280.2017.1415509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Krittanawong C, Tweet MS, Hayes SE et al. Usefulness of cardiac rehabilitation after spontaneous coronary artery dissection. Am J Cardiol. 2016;117:1604–9. doi: 10.1016/j.amjcard.2016.02.034. [DOI] [PubMed] [Google Scholar]
- 92.Chou AY, Prakash R, Rajala J et al. The first dedicated cardiac rehabilitation program for patients with spontaneous coronary artery dissection: description and initial results. Can J Cardiol. 2016;32:554–60. doi: 10.1016/j.cjca.2016.01.009. [DOI] [PubMed] [Google Scholar]
- 93.Tweet MS, Hayes SN, Gulati R et al. Pregnancy after spontaneous coronary artery dissection: a case series. Ann Intern Med. 2015;162:598–600. doi: 10.7326/L14-0446. [DOI] [PubMed] [Google Scholar]