

Abstract
Introduction:
The recent study aimed to assess the root canal morphology of mandibular canines in the Syrian population depending on the cone beam computed tomography (CBCT) images.
Materials and Methods:
A total of 418 fully developed mandibular canines in Syrian individuals aged between 16 and 60 years were included. The presence of at least one mandibular right or left canine with fully developed roots was recorded in each image. The root canal configurations were classified according to the method of Vertucci. The mandibular canines were examined in sagittal, coronal, and axial dimensions. The CBCT images were evaluated by three endodontists with at least 9 years of clinical experience in endodontics. Data were analyzed with descriptive analysis and Chi-square tests using the Statistical Package for the Social Sciences (SPSS) software version 25 (SPSS Inc, Chicago, IL, USA).
Results:
Out of the 418 mandibular canines, 409 (97.85%) were single-rooted canines while only 9 (2.15%) were double-rooted canines. The most common type of Vertucci in single-rooted canines was Type I (1-1) in the percentage of 95.87% and the least type was Type V (1-2) in the percentage of (0.24%). The Chi-square tests showed no significant association between gender and number of roots (P = 0.64) and gender and root canal configuration in single-rooted canine (P = 0.194).
Conclusion:
Single-rooted with Type I canal configuration was the most common anatomy in mandibular canines in the Syrian population. Incidence of more than one root canal foramen at the end of the single root was detected in one case only.
Keywords: Canal, canine, cone beam computed tomography, configuration, foramen, Vertucci
Introduction
The most important steps in a root canal treatment (RCT) are the biomechanical cleaning of the root canal space, preparation of this special system to be receptive to the filling materials, and creation of a tight sealing of the apical and coronal regions.[1,2] To achieve the previously mentioned objectives and guarantee the success of this kind of treatment, you should have a thorough understanding of the external and internal anatomy of the root canal system and its morphological variations.[3–5] The morphology of the root canal system has been studied and classified by several investigators, but the famous one was that of Vertucci.[6–8] The mandibular canine is usually single-rooted.[9,10] According to numerous studies, 1.7 to 6.2% of these teeth are double-rooted[10,11] and 10.6% have two or more canals.[1] Depending on several methods, the determination of the exact anatomy of a root canal system can be done. The group of used methods in scientific researches includes clinical evaluation during RCT, conventional radiography, retrospective assessment of patients’ records, cone beam computed radiography (CBCT),[12–14] tooth sectioning,[6] microscopic examination, and using three dimensional (3D) methods. CBCT has become a suitable tool to study the root canal system anatomy.[15] This method has many advantages, such as producing 3D images, noninvasive technique, reducing the overlapping of orofacial structures, and lower radiation doses and costs.[16] According to our knowledge and searching, no study has evaluated the root canal morphology of mandibular canines in Syrian population using CBCT. So, the aim of this study was to assess the root canal morphology of mandibular canines in a Syrian population using CBCT.
Materials and Methods
Patients who needed CBCT radiographic examinations for their routine examination, diagnosis, and treatment planning were included. Cases where the anatomy was damaged and original root canal morphology was unclear were excluded. A total of 418 fully developed mandibular canines in Syrian individuals aged between 16 and 60 years were included. Understanding and written consent of each patient was obtained, and the presence of at least one mandibular right or left canine with fully developed roots was recorded in each image. The following observations were recorded:
(i) Gender of patient
(ii) Number of roots
(iii) Canal configuration.
The root canal configurations were classified according to the method of Vertucci. The mandibular canines were examined in sagittal, coronal, and axial dimensions [Figure 1]. The CBCT images were evaluated by three endodontists with at least 9 years of clinical experience in endodontics. The CBCT images were analyzed with the Blue Sky Plan® software in a Dell Computer with a 32-inch Dell LCD screen with a resolution of 1280 × 1024 pixels in a darkroom. Data were analyzed with descriptive analysis and Chi-square tests using the Statistical Package for the Social Sciences (SPSS) software version 25(SPSS Inc., Chicago, IL, USA). The level of statistical significance was set at P < 0.05.
Figure 1.
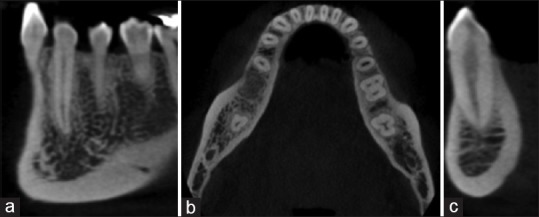
Cone beam computed tomography of mandibular canine (a) The sagittal plane, (b) the axial plane, and (c) the coronal plane
Results
Among the 418 examined mandibular canine (246 female and 172 male), most of the teeth had one root 409 (97.85%) distributed 171 (40.9%) for males and 238 (56.95%) for females while the two roots were present in 9 (2.15%) of all examined sample. Most (88.9%) of the two root cases were found in females [Table 1].
Table 1.
Distribution of examined mandibular canines according to the gender and number of roots
| Frequency (%) | |||
|---|---|---|---|
| One root | Two roots | Total | |
| Gender | |||
| Male | 171 (40.9%) | 1 (0.24%) | 172 (41.14%) |
| Female | 238 (56.95%) | 8 (1.91%) | 246 (58.86%) |
| Total | 409 (97.85%) | 9 (2.15%) | 418 (100%) |
According to the Vertucci classification, Type I was dominant in 95.87% of the participants, followed by Type III, which was present in 3.18%, Type II in 0.73%, and Type V was the least common type, found in 0.24% of the study participants [Table 2].
Table 2.
Distribution of examined mandibular canines according to the gender and root canal configuration (Vertucci types)
| Frequency (%) | |||||
|---|---|---|---|---|---|
| Type I (1-1) | Type II (2-1) | Type III (1-2-1) | Type V (1-2) | Total | |
| Gender | |||||
| Male | 168 (41.1%) | 1 (0.24%) | 2 (0.49%) | 0 (0%) | 171 (41.8%) |
| Female | 224 (54.77%) | 2 (0.49%) | 11 (2.69%) | 1 (0.24%) | 238 (58.2%) |
| Total | 392 (95.87%) | 3 (0.73%) | 13 (3.18%) | 1 (0.24%) | 409 (100%) |
The Chi-square tests revealed that there was no significant statistical association between gender and number of roots (P = 0.64) and also between gender and types of Vertucci in single-rooted canines (P = 0.194).
Discussion
Knowledge of root canal anatomy is one of the most important keys to RCT success. As each tooth type has certain common characteristics by which the operator can locate the initial access and the size of the first files to be used, it indicates a rational approach to solving any problems that arise during therapy. Canines are very long and stable teeth, there are four canines in the oral cavity (two maxillary and two mandibular) placed at corner of mouth; hence, they are called the “cornerstone” of the dentition. Typically, a canine has a single-pointed cusp, also called cuspid, and presents with single root and root canal. The canine's role in mastication is mainly tearing, which is intermediate between incising of anterior teeth and grinding of posterior teeth.[17]
Most teeth were studied anatomically and morphologically with variations have been existed and linked to various racial and genetic factors.[18–20] According to most of the previous studies, the lower canine usually has one root. The occurrence of two roots and even more than two root canals is rare. This finding is present in studies conducted by Ouellet and Kayaoglu in which the prevalence of two roots in the lower canine were 5% and 3.1%, respectively.[10,21] However, in our study, the occurrence of two roots in lower canine was 2.15%. This result is close to the previous studies, but it is less than the rate (12.08%) shown in the study by Rahimi.[22] Also, it has been found in the current study that females have a higher frequency (1.91%) of two roots occurrence in lower canine than males (0.24%) (P > 0.05). This result is in agreement with study by Kayaoglu,[21] but it is not contrary to Sert and Bayirli study and the study by Soleymani, in which the double-rooted canines and mandibular canine with two canals were significantly more common among men than women.[18,23] The majority of previous studies showed that Vertucci Type I configuration was the most common finding in the lower canine.[10,21,22] In the current study, 95.87% of the lower canine had a Type I canal configuration so there is consistency with those studies. On the other hand, Somalinga Amardeep et al. had found lesser rate of Type I configuration in their study conducted on Indian population (79.6%).[19] The other canal patterns found in our study were Type II (0.73%), Type III (3.18%), and Type V (0.24%). It is noted that Type II and III were found in most of the previous studies,[7,9,19,22,24,25] while Type V was found in lesser studies.[19,24] In our study, we have not found Vertucci Type IV configuration, whereas several studies showed this configuration pattern in lower canines.[7,9,18,24] Contrary to Somalinga Amardeep study,[19] the current study could not record the additional type of canal configuration, which is Type XIX (2-1-2-1) as per Se rt and Bayirli.[18] No significant difference was observed in this study among the prevalence of root canal type configuration in lower canine according to gender (P > 0.05).
The root canal morphologies of the lower canine have been reported based on studies of various population groups, including Chinese,[26] Turkish,[18,21,25] Iranian,[22,23] Brazilian,[14] Indian,[19] and Saudis.[27] So, several authors claimed that the morphology of the root canal systems of the mandibular canine may vary according to geographical or ethnic differences and origin.[18,19,20,21,23] It has been noticed that the occurrence of two roots or root canal in lower canine was higher among Iranian[19,22] and Turkish[18,25] populations, whereas there was very low rate of incidence of two roots or root canal in the lower canine among the Chinese[26] and Saudis[27]. However, the current study found a low rate of occurrence of two root or root canals in lower canine in a sample of Syrian people. According to Sert and Bayirli,[18] gender is an important factor for assessing root canal morphology before treatment. But, other studies considered that gender affects root length and also the number of lower canine canals. In those studies, the average length of mandibular canine root was significantly longer in men than in women.[24,28] Kayaoglu assessed the effect of age on the number of canals and found a lower frequency of two root canals being detected among older patients because of continuous dentin deposition by odontoblasts after eruption that may totally obliterate the canal space in older patients.[21]
A mandibular canine with two roots can present bifurcation at different root levels. It has been found that the bifurcation point in two-rooted canines was mostly located at the middle third of the root followed by the apical third and coronal third.[21] This unusual situation may imply difficulties to clinicians during endodontic treatment. When the division is located apically, there is a higher degree of difficulty during the localization and mechanical preparation of the root canals. In contrast, when the division is located more cervically, there are increased risks of perforating the bifurcation during the search for the additional canal. In this case, the clinician may need to modify the coronal access. Additionally, it is helpful to use magnification tools, such as an endodontic microscope, to facilitate access cavity preparation, location, and negotiation of the root canal system.
Conclusion
Within the limitations of this study, it can be concluded that:
I. Most mandibular canines had one root with Type I configuration. But, the clinicians should be aware of the likelihood of extra root or root canal presence in lower canines, which leads to endodontic therapy failure if it does not treat.
II. CBCT has become a successful tool to explore and understand the anatomical and morphological characteristics of the root canal system.
III. Clinically, it is advised to use magnification tools like an endodontic microscope during management of lower canine with extra root or root canal as it facilitates finding hidden and accessory canals without excessive removal of tooth structure.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Ehsani M, Abesi F, Tajik F, Khafri S. Evaluation of the number of canals in mandibular canines using radiographic and clearing methods in an Iranian population. J Mash Dent Sch. 2013;37:1–10. [Google Scholar]
- 2.Asgary S, Fazlyab M. A successful endodontic outcome with non-obturated canals. Iran Endod J. 2015;10:208–10. doi: 10.7508/iej.2015.03.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10:3–29. [Google Scholar]
- 4.Peikoff MD, Trott JR. An endodontic failure caused by an unusual anatomical anomaly. J Endod. 1977;3:356–9. doi: 10.1016/S0099-2399(77)80066-6. [DOI] [PubMed] [Google Scholar]
- 5.Kenneth M, Hargreaves SC. Cohen's Pathways of the Pulp. Missouri: Mosby Elsevier; 2011. p. 231. [Google Scholar]
- 6.Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol. 1969;28:419–25. doi: 10.1016/0030-4220(69)90237-0. [DOI] [PubMed] [Google Scholar]
- 7.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 8.Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J. 2001;34:359–70. doi: 10.1046/j.1365-2591.2001.00399.x. [DOI] [PubMed] [Google Scholar]
- 9.Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol. 1972;33:101–10. doi: 10.1016/0030-4220(72)90214-9. [DOI] [PubMed] [Google Scholar]
- 10.Ouellet R. Mandibular permanent cuspids with two roots. J Can Dent Assoc. 1995;61:159–61. [PubMed] [Google Scholar]
- 11.Green D. Double canals in single roots. Oral Surg Oral Med Oral Pathol. 1973;35:689–96. doi: 10.1016/0030-4220(73)90037-6. [DOI] [PubMed] [Google Scholar]
- 12.Atieh MA. Root and canal morphology of maxillary first premolars in a Saudi population. J Contemp Dent Prac. 2008;9:46–53. [PubMed] [Google Scholar]
- 13.Pattanshetti N, Gaidhane M, Al Kandari AM. Root and canal morphology of the mesiobuccal and distal roots of permanent first molars in a Kuwait population – A clinical study. Int Endod J. 2008;41:755–62. doi: 10.1111/j.1365-2591.2008.01427.x. [DOI] [PubMed] [Google Scholar]
- 14.De Oliveira SH, de Moraes LC, Faig-Leite H, Camargo SE, Camargo CH. In vitro incidence of root canal bifurcation in mandibular incisors by radiovisiography. J Appl Oral Sci. 2009;17:234–9. doi: 10.1590/S1678-77572009000300020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Han X, Yang H, Li G, Yang L, Tian C, Wang Y. A study of the distobuccal root canal orifice of the maxillary second molars in Chinese individuals evaluated by cone-beam computed tomography. J Appl Oral Sci. 2012;20:563–7. doi: 10.1590/S1678-77572012000500012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007;40:818–30. doi: 10.1111/j.1365-2591.2007.01299.x. [DOI] [PubMed] [Google Scholar]
- 17.Fuller TL, Denehy GE, Schulein TM. Concise Dental Anatomy and Morphology. 4th ed. Iowa City, IA: University of Iowa College of Dentistry; 2001. pp. 59–65. [Google Scholar]
- 18.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30:391e398. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 19.Somalinga Amardeep N, Raghu S, Natanasabapathy V. Root canal morphology of permanent maxillary and mandibular canines in Indian population using cone beam computed tomography. Anat Res Int 2014. 2014:731859. doi: 10.1155/2014/731859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Habib AH, Kalaji MN, Al saysd TJ, Al Jawfi KA. Root canal configurations of the first and second mandibular premolars in the population of north Syria. J Taibah Univ Med Sci. 2015;10:391e395. [Google Scholar]
- 21.Kayaoglu G, Peker I, Gumusok M, Sarikir C, Kayadugun A, Ucok O. Root and canal symmetry in the mandibular anterior teeth of patients attending a dental clinic: CBCT study. Braz Oral Res. 2015;29:1–7. doi: 10.1590/1807-3107BOR-2015.vol29.0090. [DOI] [PubMed] [Google Scholar]
- 22.Rahimi S, Milani AS, Shahi S, Sergiz Y, Nezafati S, Lotfi M. Prevalence of two root canals in human mandibular anterior teeth in an Iranian population. Indian J Dent Res. 2013;24:234–6. doi: 10.4103/0970-9290.116694. [DOI] [PubMed] [Google Scholar]
- 23.Soleymani A, Nafiseh Namaryan N, Ehsan Moudi E, Gholinia A. Root canal morphology of mandibular canine in an Iranian population: A CBCT assessment. Iran Endod J. 2017;12:78–82. doi: 10.22037/iej.2017.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pécora JD, Sousa Neto MD, Saquy PC. Internal anatomy, direction and number of roots and size of human mandibular canines. Braz Dent J. 1993;4:53–7. [PubMed] [Google Scholar]
- 25.Çalişkan MK, Pehlivan Y, Sepetçioǧlu F, Türkün M, Tuncer SŞ. Root canal morphology of human permanent teeth in a Turkish population. J. Endod. 1995;21:200–4. doi: 10.1016/S0099-2399(06)80566-2. [DOI] [PubMed] [Google Scholar]
- 26.Han T, Ma Y, Yang L, Chen X, Zhang X, Wang Y. A study of the root canal morphology of mandibular anterior teeth using cone-beam computed tomography in a Chinese subpopulation. J Endod. 2014;40:1309–14. doi: 10.1016/j.joen.2014.05.008. [DOI] [PubMed] [Google Scholar]
- 27.Al-Dahman Y, Alqedairi A, Alfawaz H, Alnassar F, Al-Jebaly A. Cone-beam computed tomographic evaluation of root canal morphology of mandibular canines in a Saudi subpopulation. Saudi Endod J. 2019;9:113–8. [Google Scholar]
- 28.Versiani MA, Pécora JD, Sousa-Neto MD. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int Endod J. 2013;46:800–7. doi: 10.1111/iej.12061. [DOI] [PubMed] [Google Scholar]