

Abstract
Introduction:
Increasing age, long-term deleterious habits, and increased bone resorption leading to the gingival recession have become a significant reason for poor geriatric oral health among which root caries are the most prevalent ones among the Indian population.
Methodology:
A cross-sectional study was conducted among the geriatric population above 60 years of age and those who gave voluntary consent for participating in the study were included in the study and were briefed about the questionnaire. The self-administered questionnaire was given and complete oral examination was done. Results were analyzed using the SPSS 22 version using descriptive analysis and Chi-square test.
Result:
Percentage of deleterious habits amongst males was higher than that of females i.e. 56%. Thus, males were reported with root caries more than females. The percentage of married people suffering from root caries was 85%. The most prevalent occupation among the geriatric population was found to be the farmers with 37%. Religion with maximum percentage and frequency was found to be Hinduism with 84%. Educational statuses with 6th to 12th standards were reported with maximum root caries, i.e. 55%.
Conclusion:
The study showed that criteria including income, gender, marital status, occupation, religion, and educational status were significant in assessing the prevalence of root caries. Whereas the risk factors such as habits, methods of cleaning, and brushing techniques influenced the root caries among the geriatric population.
Keywords: Geriatric population, oral hygiene, risk factors, root caries, rural population
Introduction
Medical sciences have much improved in the present days which have increased the life expectancy of the recent population. The geriatric population above the age of 60 years, live a better quality of life than previous ages. Primary care for the oral health of the geriatric population should be maintained for better health. In the Indian population, due to lack of proper nutrition, there is an increased incidence of bone resorption leading to gingival recession leading to root caries. For long healthy life, people need to keep their teeth vital for a longer time span. Hence, there is an immediate need to curb the etiological factors causing root caries and the required treatment for this group of the population should be given.[1] Gingival recession exposes the root surface to the oral environment. This predisposes the exposed root surface to the microorganisms which cause demineralization of the cementum surface. This type of lesion has a distinct outline in contrast to the sound tooth structure of the noncarious portion of the tooth.
The geriatric population constitutes around 8.6%, who are above the age group of 60 years among the total population of India. The stomatognathic system plays a primary role in better well-being to have a better quality of life. Geriatric patients have an increased incidence of bone resorption for all the bones in the body and so it is the same for the oral cavity too. Due to the resorption of the alveolar ridge, there is an increased incidence of root caries. To avoid this pathology, primary care should be taken for a better quality of life.
There are various etiological and risk factors associated with root caries among the geriatric population. Etiological factors are gingival recession due to periodontitis or with age. Radiation therapy, abfraction, xerostomia, recurrent caries, abrasion, removable partial denture or overdenture, erosion, malocclusion of teeth which had tipped and increases food lodgement, diabetes, and disability, physical and psychological factors which decreases cleansing efficiency, diminished manual dexterity, and so on.[2] Risk factors are chronic medical conditions, radiation treatment for head/neck cancer, physical limitations, poor oral hygiene, changes in diet habit, previously root caries experience, cognitive defects due to mental illness, depression, Alzheimer's disease, dementia, Sjogren's syndrome, and so on.[1,3]
There are several microorganisms involved in causing root caries which include Streptococcus mutans, lactobacillus, actinobacillus and so on.[2] The rate of progression or demineralization of tooth structure is much higher in root caries compared to enamel caries because root has less mineral content than enamel.
There are few salient features of root caries, e.g., sex predilection where males more prone to root caries than females. It is mostly seen in cases where there is severe periodontal attachment loss exposing the tooth surface to the oral environment which leads to the initiation of root caries.[4,5] It appears as a white or discolored soft irregular and progressive lesion which occurs at or apical to the cement-enamel junction. The shape of root caries is oval or round, demarcated from the surrounded noncarious tooth. Root caries progresses rapidly and may join adjoining root caries lesion. In the maxillary arch, root caries in the tooth are more commonly spread in the following order, at first incisors, then canine, followed by premolar and molar tooth. In mandibular arch the usual sequence of affecting root caries is, first at molar, then premolar, followed by canine and incisor tooth.[6]
Treatment modality of root caries is similar to caries depending on the extent of the lesion into the tooth structure, i.e. excavation of infected tooth structure and replacement with help of restoration like GIC or composites. In some cases in which caries is deep but not extending till pulp can be treated with indirect pulp capping and then followed by restoration.
Prescribe regimens to stimulate salivary flow like chewing gum with or without sugar, the inclusion of other active ingredients, sucking sugarless candies, buffered citric food acid tablets, using cholinergic medication[7,8] Prescribing saliva substitutes such as gels, sprays, liquids with placement around denture as well as on the teeth and oral soft tissues.
Probably, 600 million people aged 60 years and over are affected by caries and it is expected that the number will be double by the year 2025. But globally poor oral hygiene is evident in terms of high caries experience in both coronal and root surface and high prevalence rate of periodontal diseases with increasing age. The prevalence of caries was 46.4% among which root caries 15%.[9,10] Oral health policies and preventive measures are needed focusing on the special needs of this neglected and socioeconomically deprived population to improve their oral health-related quality of life. Hence, the aim of this study was to access the prevalence and risk factors for the development of root caries in the geriatric population in a rural area.
Methodology
The research was based on the cross-sectional study design. The ethical approval of this study was obtained from the institutional ethical committee, Dated 15.09.2018. Inclusion criterions for the geriatric population were above 60 years of age and the subject should not be edentulous.[10] The study was supposed to be conducted among 120 population. The formula for determining the size of the sample is
n = z2(p (1-p))/e2 where
n = size of the sample
z = critical value at a specific level of confidence = 1.96
P = 0.05
e = difference between sample size proportion and population proportion = 25
The sample size derived using the above formula was rounded up to 113. Participants who gave voluntary consent for participating in the study were briefed on the questionnaire by the investigator. The participants were made to fill the questionnaire prior to the examination. The questionnaire mainly consisted of questions regarding oral hygiene maintenance, method of cleaning, and habits that are deleterious in nature, the form was filled by the subjects and further handed back to the investigator.
The questions were framed in the Marathi language for the ease of understanding among the rural population. The questionnaire was initially prepared in English, after which it was converted into Marathi by a bilingual translator who was fluent with Marathi and English. The questions were further converted into the English language by another bilingual translator. Both the English questions were analyzed for examination by a statistician. The validity of questions was analyzed in the questionnaire (Cronbach's alpha = 0.82).
Oral examination was conducted with the use of a diagnostic set consisting of plain mouth mirror, dental probe, and explorer. Descriptive statistics and Chi-square tests were used. Statistical analysis was done by SPSS version 22. The power of the study was considered 80%. The level of significance was set at P < 0.05.
Results
A total of 113 participants were included in the study. The age of the participants was considered to be above 60 years. In the study group, 68 (60.2%) brushed with toothbrush and 43 (38.1%) brushed with a finger, in which 97 (85.8%) subjects brushed once daily, 15 (13.3%) brushed twice daily. Majority of the subjects 85 (75.2%) brushed in horizontal method, and 13 (11.5%) subjects had a habit of mouth rinsing after every meal, 97 (85.8%) occasionally rinsed their mouth and 3 (2.7%) did not have a habit of mouth rinsing [Table 1].
Table 1.
Depicts statistical results of the questionnaire
| Question | Options | n | % | χ2 | P |
|---|---|---|---|---|---|
| How do you brush your teeth? | Toothbrush | 68 | 60.2 | 58.956 | <0.001* |
| Finger | 43 | 38.1 | |||
| Others | 2 | 1.8 | |||
| How many times do you brush? | Once | 97 | 85.8 | 142.796 | <0.001* |
| Twice | 15 | 13.3 | |||
| More than twice daily | 1 | 0.9 | |||
| Method of cleaning? | Horizontal | 85 | 75.2 | 92.619 | <0.001* |
| Vertical | 22 | 19.5 | |||
| Others | 6 | 5.3 | |||
| The material used for cleaning? | Toothpaste | 13 | 11.5 | 37.823 | <0.001* |
| Toothpowder | 66 | 58.4 | |||
| Others | 34 | 30.1 | |||
| Type of toothbrush used? | Soft | 53 | 46.9 | 9.575 | 0.008* |
| Medium | 28 | 24.8 | |||
| Hard | 32 | 28.3 | |||
| Do you rinse your mouth after every meal? | Always | 13 | 11.5 | 141.522 | <0.001* |
| Sometimes | 97 | 85.8 | |||
| Never | 3 | 2.7 | |||
| Do you clean your tongue daily? | Yes | 9 | 8 | 79.867 | <0.001* |
| No | 104 | 92 | |||
| Do you use mouth wash? | Yes | 3 | 2.7 | 101.319 | <0.001* |
| No | 110 | 97.3 |
*Significance at P<0.05.
According to a study conducted, frequency and percentage of root caries are highest in income strata of the population for INR 5001–10000 per month. The percentage of root caries amongst the income strata of the population belonging to INR 5001–10000 per month was 38% and the frequency was 44 [Graph 1]. Males showed a higher frequency rate than females for the consumption of tobacco, alcohol, and betel nut. The percentage of deleterious habits among males was higher than females i.e. 56% and frequency was 62. Males were reportedly observed with dry mouth and exposed root surfaces, which contributes more to root caries among males [Graph 2]. Farmers were reported with the highest frequency of root caries followed by housewives. The percentage of farmers suffering from root caries was 37% and the frequency was 44. Farmers had reportedly been associated with less income and lack of awareness regarding oral care maintenance [Graph 3]. The frequency of root caries was highest in married people. The percentage of married people suffering from root caries was 85% and the frequency was 102. According to our study, the frequency of root caries is highest in married people [Graph 4]. Hindus had the highest frequency of root caries. The percentage of Hindus suffering from root caries was 84%. The frequency of people in this category was 95 [Graph 5]. The population of the qualification level of the 6th-12th standard was suffering from root caries, i.e. 55% [Graph 6].
Graph 1.
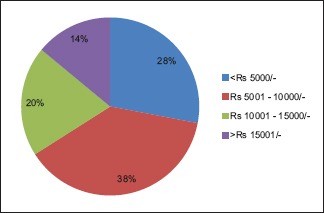
Prevalence of root caries with respect to income of the population
Graph 2.
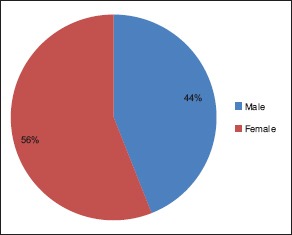
Prevalence of root caries with respect to gender
Graph 3.
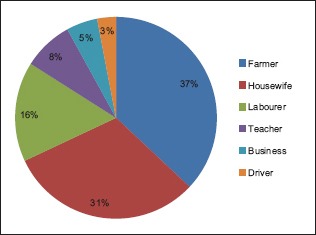
Prevalence of root caries with respect to the occupation of the population
Graph 4.
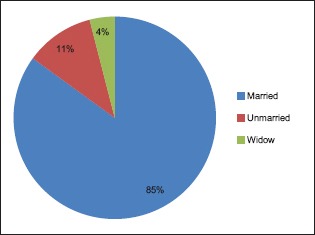
Prevalence of root caries with respect to the marital status of the population
Graph 5.
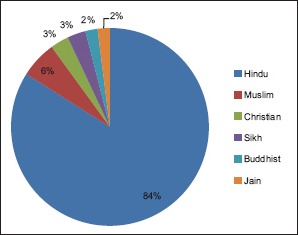
Prevalence of root caries with respect to the religion of the population
Graph 6.
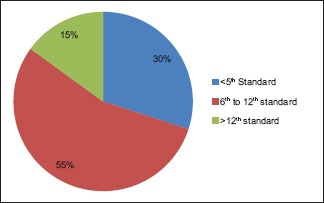
Prevalence of root caries with respect to the educational status of the population
Discussion
Root caries is a disease influenced by various factors such as sex, marital status, occupation, and habits. It is a preventable disease which if identified at an early stage, can be controlled and treated. In review, the 25 studies are taken as reference, root caries affects most commonly in older individuals of mean age above 60 years. The present study showed that age is a determining factor for root caries. Root caries was more frequently observed with advancing age, which was similar to studies done by Hintao et al.[11] In contrast Soni et al.[12] found root caries increased with the increasing age and considered the increasing prevalence of root decay with age may not be due to aging but might be a result of the general deterioration in oral health. The risk indicators for the disease have been found in common while reviewing 25 articles, out of which gingival recession and dry mouth have been found the most prevalent indicators. Medications that are prescribed to the elderly in fact can cause impaired salivary flow. Many medications, chemotherapy, radiation treatments, and some diseases can decrease salivary gland function, and therefore make caries and other oral diseases more likely to occur. Some common drugs that may cause dry mouth are high blood pressure drugs, cholesterol-lowering drugs, pain medications, muscle relaxants, allergy, and asthma medications.
The percentage of root caries in males was reported to be 56% and frequency was 62. The result of our study is in accordance with the study conducted by Chi et al.,[13] which stated that males were more prone to root caries than females. Deleterious habits such as smoking and paan chewing are more practised by males than females. The prevalence of root caries was more among tobacco chewers and smokers. This finding was in agreement with studies done by Tomar et al.[14] and Fure.[15] Robertson et al.[16] considered that the use of smokeless tobacco increased the prevalence of gingival recession with associated attachment loss, cervical abrasion, and root caries. Hence, this indirectly supports the fact that males reported with root caries more than females.
Another probable reason for males being more susceptible to root caries than females is that males are also found to be maintaining less oral hygiene as compared to females which leads to a higher incidence of root caries amongst them. Males are associated with dry mouth and exposed root surfaces more than females. As saliva is associated with the remineralization and anti-cariogenic properties, the dry mouth (xerostomia) is highly associated with caries. The gingival recession exposes the root and makes it susceptible to decay and abrasion. However, according to a study conducted by Khan et al.,[17] females are more prone to caries than males, which is not in agreement with our study. This can be attributed to facts, including the early eruption of teeth in girls in comparison to boys, due to lack of financial independence and fear of dentists amongst females.
According to a study conducted, frequency and percentage of root caries are highest in income strata of the population for INR 5001–10000. The percentage of root caries amongst the income strata of the population belonging to INR 5001–10000 was 38% and frequency was 44. According to a study conducted by Sanders et al.,[8] root caries is associated with population belonging to lower socioeconomic strata, which is in agreement with the result obtained in our study. This is due to a lack of oral hygiene maintenance amongst the population with lower income strata.
The prevalence of root caries amongst farmers was the highest as compared to other occupations. The percentage of farmers suffering from root caries was 35% and the frequency was 44. The literacy rate amongst farmers and laborer's is significantly low. Thus, awareness regarding oral health is low as well. Lack of income and awareness pose a barrier for them to approach a dentist for oral care.
According to our study, the frequency of root caries was highest in married people. It is believed that married individuals are more organized and aware of oral healthcare than unmarried. Studies suggest that living alone seems to have an influence on the disease. It is known that elders who live with a partner have better overall health status than those living alone or with no partner.[18] However, Islas-Granillo et al.,[18] in their study concluded that the prevalence of root caries amongst unmarried was 96.5%. Hence, this is not in agreement with our study.
Our study has been conducted among populations belonging to diverse ethnic and religious backgrounds. Results obtained in our study showed Hindus having the highest prevalence rate. The percentage of Hindus suffering from root caries was found to be 84% and frequency was 95.
In our study, the population of the qualification level of the 6th–12th standard pass was suffering from root caries. This could be due to low awareness of oral healthcare among low-educational status people. According to a study conducted by Siukosaari et al.,[19] High levels of education had more teeth and root surfaces at risk than those with low educational status. Hence, this is not in accordance with the result of our study. Individuals with high educational status are associated with a high-income level. Such people are commonly reported to consume more on fast food, sticky food, and sweet beverages lacking roughage in the diet. Henceforth, the sweet and sticky food items may be the resulting factor of root caries in old people with high educational and income levels. Whereas the study conducted by Chi[13] found no correlation of root caries with educational level.
In view of all the risk indicators and causes, the required awareness and education for root caries are mandatory. Governmental interventions for providing treatment at low cost and required awareness in regard to oral healthcare should be done. All the respective dental institutions must extend their services for screening and treating caries in underserved rural areas of India.
Conclusion
Dental caries is a multifactorial disease affecting the general population in today's generation being prevalent in the geriatric population, affecting males who are more associated with the habit of tobacco chewing, alcohol consumption. The prevalence of root caries is more in Hindus where the frequency of root caries is highest in married people. Although in several other studies, it has been found that the prevalence of root caries is high amongst unmarried people. Married people are considered to be more organized in terms of maintaining a healthy lifestyle and diet. However, in our study, the result is contradictory to the commonly observed notion.
Factors like gingival recession, poor oral hygiene, and improper brushing technique are the common causes of root caries in the geriatric population. Treatment of root caries is similar to caries depending on the extent of the lesion into the tooth structure. The treatment procedure is the excavation of infected tooth structure and replacement with help of restoration like GIC or composites. In some cases in which carries is deep but not extending till pulp can be treated with indirect pulp capping and then with restoration.
Surface recontouring is the earliest form of interception which should include the removal of softened tissue followed by recontouring the root surface to give it a smooth and cleanable surface.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflict of interest
There is no conflict of interest.
References
- 1.Gupta B, Marya S, Juneja V, Dahiya V. Root caries: An aging problem. Internet J Dent Sci. 2006;5:1–6. [Google Scholar]
- 2.MacDonald DE. Principles of geriatric dentistry and their application to the older adult with a physical disability. Clin Geriatr Med. 2006;22:413–34. doi: 10.1016/j.cger.2005.12.009. [DOI] [PubMed] [Google Scholar]
- 3.Neville BW. Oral and Maxillofacial Pathology. 2nd ed. Vol. 3. Philadelphia, Pa: Saunders WB; 2002. pp. 500–6. [Google Scholar]
- 4.Perdigon HT, Schneiderman E, Opperman LA. Oral health assessment of independent elders in Texas. Spec Care Dentist. 2019;39:515–23. doi: 10.1111/scd.12409. [DOI] [PubMed] [Google Scholar]
- 5.Göstemeyer G, da Mata C, McKenna G, Schwendicke F. Atraumatic vs conventional restorative treatment for root caries lesions in older patients: Meta- and trial sequential analysis. Gerodontology. 2019;36:285–93. doi: 10.1111/ger.12409. [DOI] [PubMed] [Google Scholar]
- 6.Urquhart O, Tampi MP, Pilcher L, Slayton RL, Araujo MWB, Fontana M. Nonrestorative treatments for caries: Systematic review and network meta-analysis. J Dent Res. 2019;98:14–26. doi: 10.1177/0022034518800014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Katz RV. Clinical signs of root caries: Measurement issues from epidemiologic perspective. J Dent Res. 1990;69:1211–5. doi: 10.1177/00220345900690051801. [DOI] [PubMed] [Google Scholar]
- 8.Saunders RH, Jr, Meyerowitz C. Dental caries in older adults. Dent Clin N Am. 2005;49:293–308. doi: 10.1016/j.cden.2004.10.004. [DOI] [PubMed] [Google Scholar]
- 9.Anusavice KJ. Dental caries: Risk assessment and treatment solutions for elderly population. Compend Contin Educ Dent. 2002:2312–20. [PubMed] [Google Scholar]
- 10.Bourgeosis D, Nithlia A, Mersel A. Prevalence of caries and edentulousness among 65-74 years in Europe. Bull World Health Organ. 1998;76:413–7. [PMC free article] [PubMed] [Google Scholar]
- 11.Hintao J, Teanpaisan R, Chongsuvivatwong V, Dahlen G, Rattarasarn C. Root surface and coronal caries in adults with type-2 diabetes mellitus. Community Dent Oral Epidemol. 2007;35:302–9. doi: 10.1111/j.1600-0528.2007.00325.x. [DOI] [PubMed] [Google Scholar]
- 12.Soni S, Mehta M, Devi A, Radha P, Pallavi, Kadanakuppe S, et al. Root caries among type 2 diabetes mellitus patient visiting a hospital. Spec Care Dentist. 2014;34:273–8. doi: 10.1111/scd.12065. [DOI] [PubMed] [Google Scholar]
- 13.Chi DL, Berg JH, Kim AS, Scott J. Correlates of root caries experiences in middle aged and older adults within northwest precedent. J Am Dent Assoc. 2013;144:507–16. doi: 10.14219/jada.archive.2013.0153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tomar SL, Winn DM. Chewing tobacco use and dental caries among U.S. men. J Am Dent Assoc. 1999;130:1601–10. doi: 10.14219/jada.archive.1999.0099. [DOI] [PubMed] [Google Scholar]
- 15.Fure S. Ten years cross sectional and incidence study of coronal and root caries and some related factors in elderly Swedish individuals. Gerdontology. 2004;21:130–40. doi: 10.1111/j.1741-2358.2004.00025.x. [DOI] [PubMed] [Google Scholar]
- 16.Robertson PB, Walsh MM, Greene JC. Oral effects of smoke- less tobacco use by professional baseball players. Adv Dent Res. 1997;11:307–12. doi: 10.1177/08959374970110030101. [DOI] [PubMed] [Google Scholar]
- 17.Khan AA, Jain SK, Shrivatsav A. Prevalence of dental caries among the population of Gwalior in relation of different associated factors. Eur J Dent. 2008;2:81–5. [PMC free article] [PubMed] [Google Scholar]
- 18.Islas-Granillo H, Borges-Yanez SA, Medina-Solis CE, Casanova- Rosado AJ, Minaya-Sanchez M, Villalobos Rodelo JJ, et al. Sociodemographic, and clinical variables associated with root caries in a group of persons age 60 years and older in Mexico. Geriatr Gerontol Int. 2012;12:271–6. doi: 10.1111/j.1447-0594.2011.00764.x. [DOI] [PubMed] [Google Scholar]
- 19.Siukosaari P, Ainamo A, Narhi TO. Level of education and incidence of caries in the elderly: A 5-year follow-up study. Gerodontology. 2005;22:130–6. doi: 10.1111/j.1741-2358.2005.00070.x. [DOI] [PubMed] [Google Scholar]