

Abstract
Nikolsky's sign has been a very useful diagnostic tool in cases of skin disorders like pemphigus, toxic epidermal necrolysis, etc., The sign is demonstrated when lateral pressure is applied on the border of an intact blister, which results in the dislodgment of the normal epidermis and extension of the blister.
Keywords: Dislodgement, lateral pressure, Nikolsky's sign
Background
This famous clinicopathological sign was first described by Dr. Pyotr Vasilyewich Nikolsky (1858–1940). He was a dermatologist and later a professor and chief of dermatology at the University of Warsaw. Dr. Nikolsky described this sign in 1896 and presented an explanation for the phenomenon.[1]
The explanation was that the sign showed a weakening relationship and contact between the corneal and granular layers on all surfaces, even in places between the lesions on seemingly unaffected skin.[1]
Appearance
Nikolsky's sign is pathognomic for pemphigus, toxic epidermal necrolysis, and staphylococcal scalded skin syndrome (SSSS). This sign basically differentiates intraepidermal blisters from subepidermal blisters.
It is elicited by applying tangential/lateral pressure by a thumb or a finger in the perilesional skin, affected skin, or normal skin, which results in a force that dislodges upper layers of epidermis from lower layers.[2]
Various types
Nikolsky's sign has different types, and the notable ones include the “wet Nikolsky's sign” and “dry Nikolsky's sign”. The wet Nikolsky's sign is when a moist, glistening, and eroded base is seen after exerting pressure on the skin. Dry Nikolsky's sign just differs in the aspect that the base of the eroded skin is dry.[2,3,4,5]
Other types of Nikolsky's sign include the “marginal Nikolsky's sign” and “direct Nikolsky's sign.” The marginal Nikolsky's sign is described as the extension of erosion on surrounding normal skin. This is elicited by rubbing the skin surrounding the existing lesions. The direct Nikolsky's sign includes the inductions of the erosion on the normal skin that are far from the lesions.[2,3]
Another subclinical counterpart of the Nikolsky's sign is the “microscopic Nikolsky's sign.” In this case, upon exerting the tangential/lateral pressure, which is generally used for eliciting clinical Nikolsky's sign, it produces the classical microscopic changes for pemphigus vulgaris or pemphigus foliaceus in the epidermis, which can be confirmed by a skin biopsy. Recent studies have proposed that microscopic Nikolsky's sign may be a better and more sensitive method for rapid diagnosis and can also improve the efficacy of histopathological results.[3,6]
In further studies, different authors have further described few signs related to Nikolsky's sign, namely, the “false Nikolsky's sign” or “Sheklakov's sign” and “pseudo Nikolsky's sign” or “epidermal peeling sign.”
The “false Nikolsky's sign” is elicited and positive for subepidermal blistering disorders. It is seen in disorders like bullous pemphigoid, cicatricial pemphigoid, dermatitis herpetiformis, epidermolysis bullosa, porphyrias, bullous systemic lupus erythematosus (SLE). It is elicited by pulling the peripheral remnant roof of a ruptured blister, thus extending the erosion on the surrounding normal skin. The “false Nikolsky's sign” has a subepidermal cleavage that occurs in the skin surrounding the lesion. The subepidermal cleavage are limited in size, do not show a tendency of spontaneous extension, and heal rapidly.[2,3,4]
Another sign is the “pseudo Nikolsky's sign,” which is positive for Stevens–Johnson Syndrome, some burn cases, toxic epidermal necrolysis, and bullous ichthyyosiform erythroderma. Here, the underlying pathophysiology is necrosis and not acantholysis, which is seen in the “true Nikolsky's sign” it is elicited only on areas that are already involved and affected and also on erythematous areas.[2,3]
There is a phenomenon associated with this sign called “Nikolsky's phenomenon.” Here the superficial epidermis is felt to move over the deeper layers, and instead of an immediate reaction to form erosion as in Nikolsky's sign, the blisters develop after some time.[2,3]
Pathophysiology Related to Nikolsky’ Sign
The core pathophysiology behind this sign is acantholysis. “Acantholysis” term was described by Auspitz in 1881 and has been defined as the loss of coherence between epidermal cells because of the breakdown of their intercellular bridges. The acantholysis in this sign has been shown to be present in both affected as well as intact areas [Figures 1 and 2]. Nikolsky's sign is usually positive in diseases with dermoepidermal separation; thus, it helps us distinguish between pemphigus and bullous pemphigoid.[3,7]
Figure 1.
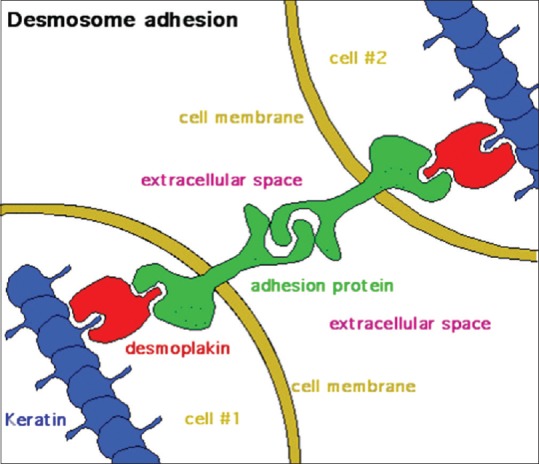
Ultra-structure of Desmosomes
Figure 2.

Normal and Disease structure of Oral Mucous Membrane
Acantholysis
Acantholysis can be broadly classified into two types, namely, primary and secondary. Primary acantholysis is dissociation and disintegration of desmosomes leading to the separation or disjunction of keratinocytes because of either direct injury to the desmosomes or hereditary defects in their development and construction [Figures 3 and 4].[3] Whereas, secondary acantholysis occurs because of alteration or damage to the structure of keratinocytes because of various factors. Primary acantholysis is seen in conditions like pemphigus, Hailey-Hailey disease, Darier's disease, SSSS, etc., and secondary acantholysis is seen in conditions like herpes simplex and herpes zoster infections, borderline-tuberculoid (BT) leprosy, epidermolysis bullosa, basal cell carcinoma, keratoacanthoma, adenoid squamous cell carcinoma, psoriasis, tinea corporis, etc., There are certain factors that trigger acantholysis like autoimmunity, drugs like thiol group of drugs, infections, heat, burns, sweating, friction, trauma, contact dermatitis, ultraviolet B (UVB) rays, etc.
Figure 3.
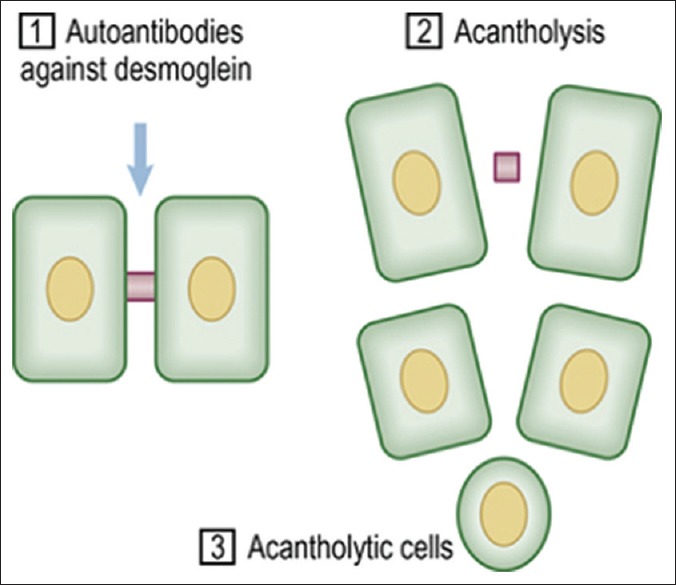
Pictorial representation of Acantholysis
Figure 4.

Flowchart showing New Pathology of Acantholysis in Pemphigus
Nikolsky’ Sign and Associated Diseases
Most commonly this sign is seen in pemphigus. Pemphigus is an autoimmune disease which is characterized by acantholysis which subsequently results in the formation of mucocutaneous blisters and erosions. Circulating autoantibodies against Dsg3 (Desmoglein 3) or Dsg1 (Desmoglein 1) results in loss of adhesion between the keratinocytes and furthermore in blister formation.[7,8,9,10,11]
Nikolsky's sign has been pathognomic for pemphigus and is elicited by applying lateral or tangential pressure to the mucosa or skin in the peri-lesional area resulting in shearing away of the epidermis in the normal areas [Figure 5].
Figure 5.
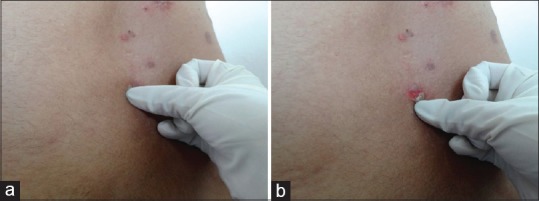
Nikolsky's Sign
The next syndromes where Nikolsky's sign has been of clinical importance is the SSSS.
SSSS in a potentially serious exfoliating cutaneous disease that occurs predominantly in children; particularly neonates. It is caused due to exfoliative toxins from a focus of infection with Staphylococcus aureus which specifically cleaves Desmoglein 1 (Dsg1) in the zona glomerulosa of epidermis and causes superficial cleavage of tissue with blistering. Here also in most of the cases upon applying tangential or lateral pressure in perilesional area the epidermis peels off from the normal-appearing skin area.[7,8,9]
The third disease on the list is toxic epidermal necrolysis or Lyell's disease. It is also a life-threatening mucocutaneous blistering eruption that is generally drug-induced eg: sulphonylureas, sulphonamides, NSAIDs, allopurinol, anti-retroviral therapy, etc., There is immense apoptosis of epidermal cells. This disease also shows a positive Nikolsky's sign most of the time.[7,8,9]
Nikolsky sign has also been reported in acute bullous lichen planus. It mainly occurs because of the loss of intercellular cohesion in basal and lower malphigian area which is the underlying cause of Nikolsky's sign in this case.[12]
Other Diseases With Signs Similar to True Nikolsky's Sign
False Nikolsky's sign has been seen in a variety of diseases as mentioned earlier. The most important of them are Bullous pemphigoid and Epidermolysis bullosa.
Bullous pemphigoid is an autoimmune dermatological disorder caused due to the action of autoantibodies BP230 and BP180 against hemidesmosomal BP antigens namely BPAg-1 and BPAg-2.[13] Here there is dermoepidermal separation rather than true acantholysis thus the sign here is named as False Nikiolsky's sign.[3,14]
Epidermolysis bullosa acquisita is an autoimmune disorder caused by actions of autoantibodies directed against collagen VII.[7,8] It was first described by Colcott (1897) and Kablitz (1904).[15]
Here also there is bulla formation is due to separation of epidermal areas from connective tissue leading to False Nikolsky's sign rather than the true one. But there have been cases of this disorder with positive Nikolsky's sign.[15]
Another sign that very closely resembles Nikolsky's sign is Pseudo Nikolsky's sign seen mainly in Stevens–Johnson syndrome.
It is a rare and severe form of bullous erythema multiforme with marked mucosal involvement including mouth, eyes, genitalia and constitutional disturbances that are mainly caused due to drug reactions rather than infection.[7,8] Its main pathophysiological cause has been underlying necrosis and apoptosis rather than true acantholysis so the sign here is named pseudo Nikolsky's sign.[16]
Asboe-Hansen sign
It was named after a Danish physician Dr. Gustav Asboe-Hansen. Also called a bulla spread sign. It is the ability to enlarge a blister in the direction of periphery by applying mechanical pressure on the roof of the intact blister. In pemphigus Vulgaris, the blister extension has a sharp angle and in bullous pemphigoid the border is rounded.[2,3]
Help in general practice
This sign has been one of the prominent clinical features of Pemphigus and few other blistering diseases as mentioned in this review. This sign is easy to elicit and can help a general practitioner to diagnose these conditions; which they may encounter in course of their practice. Just the basic knowledge on how to elicit the sign is required by the diagnosticians and it is not very difficult or complex. In general, the diagnosticians around the globe should have a clear idea about the different dermatological signs and their associated conditions.
Conclusion
For many years now Nikolsky's sign has been one of the most common pathological signs to be elicited and to be used for diagnosis in pemphigus group of disorders and other autoimmune diseases. Its clinical utility has really been boon for diagnosticians around the globe for the diagnosis of pemphigus, SSSS, and Lyell's disease.
If we see in real sense it is a mark of a qualitative standard rather than a quantitative one. Lack of standardization may have limited its usefulness but it still continues to be a boon and blessing for medical practitioners all over the world as it helps in diagnosis of a group of threatening diseases in very easy and simpler way.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Urbano FL. Nikolsky's sign in autoimmune skin disorders. Hosp Physician. 2001:23–4. [Google Scholar]
- 2.Sachdev D. Sign of Nikolsky and related signs. IJDVL. 2003;69:243–4. [Google Scholar]
- 3.Seshadri D, Kumaran MS, Kanwar JA. Acantholysis revisited: Back to basics. IJDVL. 2013;79:220–45. doi: 10.4103/0378-6323.104688. [DOI] [PubMed] [Google Scholar]
- 4.Salopek TG. Nikolsky's sign: Is it ‘Dry’ or is it ‘wet’? Br J Dermatol. 1997;136:762–7. [PubMed] [Google Scholar]
- 5.Uzun S, Durdu M. The specificity and sensitivity of Nikolskiy sign in the diagnosis of pemphigus. J Am Acad Dermatol. 1999:312–4. doi: 10.1016/j.jaad.2005.10.019. [DOI] [PubMed] [Google Scholar]
- 6.Barzegari M, Valikhani M, Esmaiti N, Naraghi Z, Nikoo A, Kamyab K, et al. Microscopic Nikolsky's sign: Is it useful for diagnosis of pemphigus vulgaris. Iran J Dermatol. 2008;11:64–6. [Google Scholar]
- 7.Neviile BW, Damn DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology. 2nd ed. India: W.B Saunders Company; 2010. [Google Scholar]
- 8.Nicki CR, Brian WR, Stuart RH. Davidson's Principles and Practice of Medicine. 21st ed. Churchill Livingstone Elsevier; 2010. [Google Scholar]
- 9.Rajendran R, Sivapathasundram B. Shafer's Textbook of Oral Pathology. 7th ed. India: Elsevier; 2012. [Google Scholar]
- 10.Didona D, Maglie R, Eming R, Hertl M. Pemphigus: Current and future therapeutic strategies. Front Immunol. 2019;10:1–28. doi: 10.3389/fimmu.2019.01418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Banerjee I, Bhowmik B, Maji A, Sinha R. Pemphigus vulgaris- A report of three cases and review of literature. J Family Med Prim Care. 2018;7:1109–12. doi: 10.4103/jfmpc.jfmpc_133_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kaur S, Singh M, Radotra BD, Sehgal S. Positive Nikolsky's and bulla-spread signs in acute bullous lichen planus. Arch Dermatol. 1987;123:1122–3. [PubMed] [Google Scholar]
- 13.Grando SA. Pemphigus autoimmunity: Hypotheses and realities. Autoimmunity. 2012;45:7–12. doi: 10.3109/08916934.2011.606444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Grunwald MH, Ginzburg A, David M, Feuerman EJ. Nikolsky's or Pseudo-Nikolsky's sign in bullous pemphigoid. Int J Dermatol. 1984;23:629. doi: 10.1111/j.1365-4362.1984.tb05707.x. [DOI] [PubMed] [Google Scholar]
- 15.Nair VL, Ganga P. Epidermolysis bullosa aquisita. IJDVL. 1990;56:310–1. [Google Scholar]
- 16.Ariana E, Kena S, Casey W, Guha K. Stevens- Johnson syndrome and toxic epidermal necrolysis. Ann Allergy Asthma Immunol. 2017;118:143–7. doi: 10.1016/j.anai.2016.11.019. [DOI] [PubMed] [Google Scholar]