

Abstract
The healthcare industry is experiencing a major transformation towards e-healthcare, which delivers and enhances related information through the Internet among healthcare stakeholders and makes the electronic signature (e-signature) more and more important. This paper uses a mature framework, Technology–Organization–Environment (TEO), in information system discipline to identify factors that affect hospitals in adopting e-signature. A survey was conducted on regional hospitals and medical centers in Taiwan to verify the validity of the research framework. The results show that TEO framework is useful in distinguishing hospitals as adopters and non-adopters of e-signature. Based on the research findings, implications and limitations are discussed.
Keywords: Electronic Medical Records, Electronic signature, Healthcare Certification Authority, Technology–Organization–Environment framework
1. Introduction
Healthcare is believed to be an information intensive industry. However, the information technology (IT) change has been more rapid outside than within the healthcare industry [44]. The modern medical environment is now experiencing major transformation in its IT base with increasing in technological complexity and handling more patients with fewer resources, and resulting in higher demands on medical practitioners [14]. The information system (IS) discipline confronted similar transformations in other industries and developed theories and methods that should prove useful in healthcare applications [44]. Consequently, this study employed a mature framework available in IS discipline to explain the adoption decision of IT innovation in hospitals.
One of many ways to ease the workload of medical staff is Electronic Medical Records (EMR) to respond to the challenge for efficient and high-quality health care [1]. A completed EMR should include the authentication of a physician's e-signature and the electronic records of patients that can be transmitted within or between hospitals. Thereby, the lack of standardization of e-signatures impedes exchange and sharing of medical data [40]. There are at least three distinct motivations underlying our study. Firstly, a law pertaining to e-signature was enacted and was formally promulgated in 2002. Secondly, the Department of Health (DOH) of Taiwan adapted Public Key as an infrastructure and set up the Healthcare Certification Authority (HCA) in 2003. A total of 8000 IC cards were issued to medical institutes and more than 30,000 IC cards were issued to medical staff. Thirdly, the astonishing rapid spread of the intra-hospital transmission of Severe Acute Respiratory Syndrome (SARS) epidemic killed 84 people in Taiwan and speeds up the exchange of EMR between hospitals to track the potential contagion.
However, the adoption of e-signature was not satisfactory at the time this research was conducted and the reasons hospitals delayed e-signature adoption were not investigated. Adopting e-signature is not only a simple activity to purchase the required hardware and software, but rather a social interaction process among users, organizations, and the environment. While implementing IS, organizational managers are suggested to focus on critical success factors for promptly responding to important events [15], [25]. The process of making an innovation adoption decision is essentially an information-seeking and information-processing activity in which the adopter is motivated to reduce uncertainty about the advantages and disadvantages of an innovation. Therefore, the purpose of this study is to build an analysis framework to identify the critical factors that affect hospital adoption of e-signature for the further promotion of EMR.
2. Literature review
2.1. E-signature
In the network environment, e-government and e-commerce are dependent on electronic documents and signatures as the foundation of electronic communications and transactions. In order to encourage the development of digital economic activity, the norm for legal electronic documents and signatures according to the Law of E-Signature is required. Legitimizing e-signature to set up a safe and authentic environment for electronic transactions that incorporate e-commerce applications has become a global issue [27]. Nowadays, the technology of e-signature can be applied to purchase on the Internet, distance education, web entertainments, and Internet finance such as the electronic trading of stocks and bonds.
An e-signature consists of e-signature image and digital signature. E-signature is generally associated with a number of technologies, allows a person (or machine) to electronically mark a document [26], and can enable innovative document management processes [12]. In other words, e-signature provides electronic authentication and a process to verify the identity of users with a stand-alone mainframe, network, or Internet-based system to control access or authorize transactions [29].
There are many forms of e-signature. Benjamin Wright, a noted e-commerce attorney and co-author of The Law of Electronic Commerce, concluded that “How, where, and when e-signatures are used requires the same care and common sense that one would apply to the use of pen and ink signatures” [26] . In many states and industry sectors of the US, e-signatures attached to electronic records (documents created, stored, generated, received, or communicated by electronic means) are legally recognized in the same manner as handwritten signatures on paper [29].
2.2. Applying e-signature to medical institutes
Today's healthcare providers, faced with increasing competition, are exploring IT opportunities to reduce the overall cost of healthcare delivery while improving the quality. Junglas and Watson [19] indicate that the evolution of commerce through IT started from geographic commerce (g-commerce) and moved toward electronic commerce (e-commerce). In a similar way the healthcare industry is also transforming from g-healthcare toward e-healthcare. The medical information systems of g-healthcare range from physiological signals to Hospital Information Systems and are aimed at offering many benefits limited to a fixed time and location. E-healthcare delivers and enhances related information through the Internet among healthcare stakeholders and makes e-signature increasingly more important.
Dutta and Heda [7] find the success of managed care depends critically on the collection, analysis and seamless exchange of information within and across organizational borders. In the medical industry, adopting e-signature technology allows physicians to sign on medical records in a more timely and efficient manner and hence exchange EMR among different healthcare providers when it is necessary. According to Waegemann [41], when medical institutions attempt to accomplish EMR, they not only need to establish certification, access control, and an e-signature system, but also guarantee the completeness and safety in integrating medical data. In 2002, Lin [24] surveyed all 590 hospitals and 3162 clinics in Taiwan, and found that about 60% of hospital respondents and more than half of the clinic respondents felt that the Law of E-Signature would help develop EMR.
2.3. The factors affecting IT adoption
Healthcare is a large and growing industry that is experiencing major transformation in its IT base [44]. As mentioned above, the IT change has been more rapid outside than within the healthcare industry. The IS discipline has confronted similar technological transformation in other industries and has developed theories and methods to deal with the changes. Taking this into account, our study uses the mature framework of Technology–Organization–Environment (TOE) in IS discipline for adopting an innovative technology, and indicates the critical factors that affect the adoption decision. Tornatzky and Fleischer [39] developed the TOE framework to determine what factors influence a firm's adoption decision. TOE is consistent with Rogers' [35] theory of innovation adoption in technological characteristics and internal and external characteristics of the organization [46].
As e-signature is a brand new technology to Taiwan's hospitals, the TOE research framework is adapted in this study to identify the factors that influence hospitals' adoption of the innovative technology. Swanson [37] classifies IS innovations into three types: Type I innovations are confined to the technical tasks; Type II innovations support the administration of business; and Type III innovations are embedded in the core of the business. According to this typology, e-signature should be a combination of Types II and III innovation, in the sense that e-signatures are embedded in the EMR, which is a core operating process for hospitals. It also streamlines the hospital administration.
Within an organization, “User involvement” can positively affect the adoption of new technology [23], [34], [38]. While adopting innovative IT, adequate resources could enhance the success [30], [38]. A large organization has more resources for changing business strategy. Therefore, the “organizational size” can affect the adoption of innovative IT [17], [18], [36]. Meanwhile, “internal demands” also play an important role in the adoption decision of innovative IT [18], [31].
When good coordination exists between customers and their IT vendors, the customers usually favor the adoption of innovative technology [9]. Similarly, “government policy” influences the technological development of an organization [3], [16], [17]. Enterprises adopting security protection products with security certification can rely on their information security systems [8]. Therefore, “Security protection” will no doubt, influence the adoption of innovative IT [4], [17]. Finally, the adoption of innovative IT is related to the level of system complexity [6], [32], [38], [47].
3. Research methodology
Owing to the complexity involved in adopting e-signature, an expert panel was formed to guide the research process. The expert panel includes two medical informatics consultants and two experts with experience in the field. The medical informatics consultants have extensive consulting experience and background with e-signature and are professors in the medical informatics department of a national university in Taiwan. The other two experts played major roles in the government e-signature planning and promoting project, and consequently they have accumulated comprehensive experience in this subject area.
The expert panel helps us determine the appropriateness of the research framework, check the completeness and suitability of the questionnaire, and offer guidance for the research progress whenever there is a need. Questionnaires were mailed out to the executives and directors of the information departments of 86 hospitals to collect the needed information. Finally, a discriminant analysis was conducted to distinguish between those hospitals that adopted e-signature and those that did not.
3.1. Research framework and hypotheses
According to the TOE framework, the research dimensions are constructed with organizational, environmental, and e-signature characteristics. Each dimension with its own variables is summarized from literature reviews in Fig. 1 .
Fig. 1.
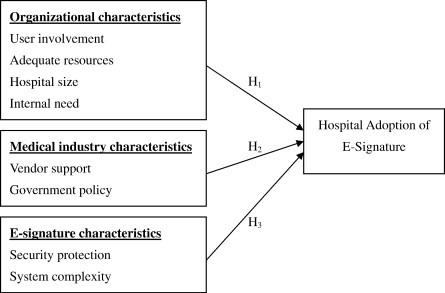
Research framework.
Based on our research framework, related literature, and the opinions of the expert panel, eight hypotheses grouped into three TEO categories are proposed to identify factors affecting the adoption of e-signature:
H1
The organizational characteristics of a hospital affect its adoption of e-signature.
H1.1
A hospital with a high degree of “User involvement” tends to adopt e-signature.
H1.2
A hospital that has “Adequate resources” tends to adopt e-signature.
H1.3
Larger hospitals tend to adopt e-signature.
H1.4
A hospital with a high degree of “Internal need” tends to adopt e-signature.
H2
The medical industry characteristics of a hospital affect its adoption of e-signature.
H2.1
A hospital which perceives a high degree of “Vendor support” tends to adopt e-signature.
H2.2
A hospital which perceives “Government policy” as important tends to adopt e-signature.
H3
The e-signature characteristics affect a hospital's adoption of e-signature.
H3.1
A hospital which perceives a high degree of “Security protection” tends to adopt e-signature.
H3.2
A hospital which perceives a low degree of “System complexity” tends to adopt e-signature.
3.2. Measurements
The survey instrument contains four parts. The organizational dimension comprises fifteen questions; both environmental and e-signature dimensions contain nine questions each; and the fourth part includes six questions for collecting the basic information of the respondent and his/her hospital. Operational definition and the origin of each item in the questionnaire are shown in Appendix Table A.1. A five-point Likert scale is used to measure the respondent's agreement of each item where “one” represents strongly disagree and “five” represents strongly agree.
The sample of this study includes hospitals with certified accreditation as regional hospitals or medical centers in the 2002 official list given by the DOH. The list includes 17 medical centers and 69 regional hospitals for a total of 86 hospitals. Studies show that making prior notification calls [2] and mailing questionnaires to the specific subject can improve the response rates of mail surveys. A telephone call was conducted before mailing out the questionnaire to obtain the names of information department executives or directors for each hospital. Eighty five names were obtained since one director worked in two hospitals simultaneously. The 85 questionnaires were then mailed out.
4. Results
4.1. Basic data analysis
Out of 85 dispatched questionnaires 53 replies were received to make up a response rate of 62.35%. The majority of questionnaire respondents are male (94.12%), aged between 35 and 39 (23.53%) years old. Seventy-eight percent of the respondents have more than two years of experience in the IS department and 25.49% of the respondents are directors with over ten years experience. In other words, the sample data show that most respondents are experienced with medical information and therefore clearly understand the subject matter.
Among the respondent hospitals, 30.2% are medical centers while the remaining 69.8% are regional hospitals. Since the ratio of medical centers to regional hospitals in the population is 20% to 80% respectfully, our study has a higher response rate from medical centers. Ninety seven percent (31/32) of the non-respondents are regional hospitals and among them 84% (26/31) have not adopted e-signature since most of them have less IS personnel in their IS departments. Furthermore, among respondent medical centers, approximately 56.3% of them have adopted e-signature while only 27% of respondent regional hospitals have adopted. The proportion of hospitals that have adopted e-signature to those that have not is 29.4% to 70.6%, showing a slight difference compared with the proportion obtained through the DOH listing as being 30% to 70%. Meanwhile, mail surveys with a return of about 30% are often considered “satisfactory” [5]. Therefore, the respondents of this study may reasonably represent the population (see Table 1 ).
Table 1.
Comparison of respondent and not respondent
| Response rate | E-signature adopter | Hospital accreditation |
||
|---|---|---|---|---|
| Med center | Regional | |||
| Respondent 53 (62%) | No | 34 (62.7%) | 7 (20.6%) | 27 (79.4%) |
| Yes | 19 (37.3%) | 9 (47.4%) | 10 (52.6%) | |
| Total | 53 | 16 (30.2%) | 37 (69.8%) | |
| Non-respondent 32 (38%) | No | 26 (81.3%) | 0 (0%) | 26 (100%) |
| Yes | 6 (18.7%) | 1 (16.7%) | 5 (83.3%) | |
| Total | 32 | 1 (3.1%) | 31 (96.9%) | |
| Total: 85 | Adopter = 25 (29.4%) | Medical center = 17 (20%) | ||
| Non-adopter = 60 (70.6%) | Regional hospital = 68 (80%) | |||
4.2. Reliability and validity
Prior to data analysis, the research instrument was assessed for its reliability as well as construct validity. The measurement of this study was first derived from theoretical bases and references and then followed up by review of the expert panel to ensure the effectiveness of the questionnaire. In addition, discriminant validity focuses on whether one can empirically differentiate the construct from other constructs [21]. Since the sample size is less than 100, it is not suitable for factor analysis, which requires the sample size to be at least 100 or 5 times that of the number of variables to be analyzed [10], [13]. The Kaiser–Meyer–Olkin (KMO) [20] statistical analysis is used instead. The results show that the KMO for the organizational (0.729), environmental (0.812), and e-signature (0.804) dimensions are greater than the threshold of 0.50. Therefore, the factors used in this study are appropriate. Meanwhile, the Bartlett's Test of Sphericity correlative coefficients among measured items can be used to extract factors for factor analysis. In this study, the results of Bartlett's Test of Sphericity are all significant in the three dimensions (see Table 2 ).
Table 2.
KMO and Bartlett's test
| Dimensions | Organizational characteristics | Environmental characteristics | E-signature characteristics | |
|---|---|---|---|---|
| Kaiser–Meyer–Olkin value | .729 | .812 | .804 | |
| Bartlett's Test of Sphericity | Chi-square | 568.008 | 337.276 | 251.437 |
| df | 105 | 36 | 36 | |
| Sig. | .000 | .000 | .000 | |
In terms of reliability, Nunnally [28] suggested an index between 0.5 and 0.6, while Hair et al. [13] stated that the index has to be greater than 0.7 to be reliable. In general, if the index is smaller than 0.35, the test should be abandoned. As shown in Appendix A.2, the Cronbach's α for each variable is greater than 0.7. Thus, the reliability of the instrument is concluded. Summarizing from the above statistics, the questionnaires in this study were determined to be adequate.
4.3. Hypothesis testing results
The result of discriminant analysis shows that the overall model is acceptable (Wilks' lambda = 0.673, p = 0.022 < 0.05, see Table 3 ). In other words, the aforementioned factors in the analytic model can be used to distinguish the adopters and non-adopters of e-signature. For synchronic discriminant, two important indexes, which explain discriminant analysis results, are discriminant loading and standardized discriminant coefficient [13]. Using discriminant loading can avoid the collinear problem and is relatively stable when analyzing small samples. The standardized discriminant coefficient is used to compare the relative importance of predicting variables [7]. In general, discriminant loading has to be greater than 0.3 to be significant. Among the eight variables, the “hospital size”, “government policy”, “adequate resources”, and “vendor support” have discriminant loading greater than 0.3 and therefore contribute significant influence in discriminating the two groups. In other words, these variables have a significant effect on whether or not a hospital decides to adopt e-signature.
Table 3.
Results of discriminant analysis
| Wilks' lambda = .673, df = 8 | ||||||
| Chi-square = 17.842, Sig = .022⁎ | ||||||
| H | Factors | Discriminant loading | Adopter means | Non-adopter means | Conclusion—This | Conclusion—Previous |
| H1.1 | User involvement | 0.183 | 3.5789 | 3.3828 | Not support | Support |
| H1.2 | Adequate resources | 0.313 | 3.3263 | 3.0688 | Support | Support |
| H1.3 | Hospital size | 0.446 | 0.3602 (Z score) | − 0.2139 (Z score) | Support | Support |
| H1.4 | Internal need | 0.216 | 3.7193 | 3.4792 | Not support | Support |
| H2.1 | Vendor support | − 0.313 | 3.9684 | 4.2313 | Support | Support |
| H2.2 | Government policy | 0.327 | 4.1579 | 3.8906 | Support | Support |
| H3.1 | Security protection | − 0.039 | 3.9912 | 4.0260 | Not support | Support |
| H3.2 | System complexity | − 0.235 | 3.6316 | 3.8229 | Not support | Support |
⁎p < 0.05; Conclusion—This: conclusion of this study; Conclusion—Previous: conclusion of previous studies.
Both adopters and non-adopters of e-signature consider indifferently in “system complexity” (with means of 3.6316 and 3.7193), “internal need of a hospital” (with means of 3.5789 and 3.9912), “user involvement” (with means of 3.8229 and 3.4792), and “security protection” (with means of 3.3828 and 4.0260). In other words, the above four factors do not influence the willingness of adopting e-signature with insignificant discriminant loadings as − 0.235, 0.216, 0.183, and − 0.039, respectively.
5. Discussion
The research framework confirms some findings from previous IS studies in identifying critical factors affecting the technology adoption decision of an organization. Regarding the organizational dimension the finding of this study agrees with that of previous research on factors such as “adequate resources” and “hospital size” and disagrees on the “user involvement” and “internal need” of a hospital. Both vendor support and government policy factors are confirmed in this study. Regarding the technology characteristics dimension, the results of this study disagree with the previous research on system complexity and security protection. The comparisons of hypothesis testing results of this study and prior studies are summarized in Table 3.
The adopters of this study perceive significantly higher support in terms of “adequate resource” than non-adopters, and therefore tended to adopt e-signature. This finding is consistent with prior related research [32], [38]. The hospital size effect confirmed the prior research of organization size affecting innovation adoption [36]. According to this study, larger hospitals tend to adopt e-signature more than smaller hospitals do. Although vendor support is also a significant factor to distinguish e-signature adopters and non-adopters as indicated in the prior studies [45], non-adopters in this study value vendor support significantly higher than adopters. The possible reason may be that the adopters have gained experience during the cooperation and therefore rate the vendor support less important compared to non-adopters. Finally, adopters foresaw the impact of government policy higher than the non-adopters and therefore were willing to adopt e-signature. This finding also confirmed the results in the Ho and associates' study [16].
It is believed that system complexity [11], [32], internal need [33], user involvement [23], and security protection [8] are key considerations for organizations deciding to adopt a new technology. However, these four factors were not supported in this study which reveals some insights about the nature of the healthcare industry. There are two possible reasons why the findings of this study vary from prior studies. Firstly, previous studies surveyed multiple organizations in multiple industries. Unlike for-profit organizations, hospitals in Taiwan are consistently centralized to a high degree [3] therefore the user involvement is deemed to be less important compared to that in other industries. Secondly, vendors of healthcare technology in Taiwan habitually provide total solution from adding gateways to on-site training or consulting to link the new technology to the buyers' IS. Therefore, all hospitals perceived system complexity is low. In terms of security, all the respondents perceived similar importance with means of 3.99 and 4.03 for adopter and non-adopter respectively. In other words, both adopters and non-adopters considered security indifferently. Summarized from the results of this study, the research model is refined as Fig. 2 shown below.
Fig. 2.
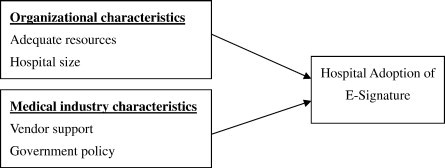
Modified research framework.
Although our data set revealed a reasonable fit (p = 0.022) of the TEO framework in identifying factors that influence the adoption of e-signature in Taiwan hospitals, three limitations should be noticed. Firstly, the respondents might tend to favor the technology and are therefore more willing to mail back the questionnaire. Secondly, all the variables in our framework are selected from the IS related literature. In other words, the important variables concerning the healthcare industry might not be included in this study. Lastly, this study uses static cross sectional approach, which may not reveal the dynamics of the technology adoption processes. Considering the ability to adopt IT, this study limited the scope to all regional hospitals and medical centers in Taiwan that have an IS department. Meanwhile, the surveyed subjects are executives or directors of each hospital information department. The users in practice that include physicians, system designers, and other employees may obtain different view-points about the technology. Therefore, more rigorous study is needed to further explore issues uncovered by this study. For instance a longitudinal study would provide more insight into the adoption process.
6. Conclusion
By the completion time of this research, 70% of the research hospitals in Taiwan are delaying their adoption of e-signature, which further delays the development of computerized medical records as planned by the Taiwan government under its digital hospital project. The future functions of a digital hospital can be listed as long distance treatments, Internet virtual hospitals, and medical e-commerce. Without e-signature, the above future function may not be easily achieved.
The four significant factors in distinguishing e-signature adopters from non-adopters are hospital size, adequate resources, vendor support, and government policy. Suggestions to increase the e-signature diffusion rate are as follows. Firstly, to enlarge hospital size is to increase the number of patient beds, to hire more medical employees, or to increase business volume of a hospital by the definition of this study. However, the number of beds to population in Taiwan is twice that number in the US, which may represent a waste of medical resources [22]. Therefore, to increase medical employees or business volume of a hospital is a more acceptable suggestion.
In terms of government policy and support, a 2003 worldwide report [43] ranked Taiwan the fifth in e-government service among 198 countries. This report also confirmed the effort of the Taiwanese government to build its electronic services infrastructure and the possibility of constructing EMR. Although the SARS threat has subsided provisionally, other epidemics such as Avian Influenza may cause a serious threat anytime and anywhere. This study suggests the government take a stronger position to provide financial aid and educate the non-adopters. Especially for the underprivileged hospitals, such as smaller hospitals without sufficient IS personnel, more cooperation or direct supports from the government are needed in order to help them adopt e-signature. Secondly, reducing uncertainty of policies, not only regulations for e-signature but also the reimbursement related to the promotion of e-signature, is needed. As the majority of hospital funds come from the Bureau of National Health Insurance (BNHI) reimbursement, stable and favorable e-signature BNHI policies are very important to a hospital's decision to adopt e-signature. With EMR, a patient who is infected with a disease or who has visited a contaminated hospital can be tracked or identified at the beginning of the medical care process to alert the medical care staff of the need for precaution.
Adopting e-signature is not just a simple activity to purchase the required hardware and software, but rather a social and economic interaction process among organizations and the environment. The contributions of this research are two-folded. Firstly, an analysis framework for adopting healthcare innovation was established to identify the critical factors on e-signature in the early stages of innovation diffusion. Secondly, this study illustrates the applicability of the IS model in the healthcare industry and sheds some light for future IS and healthcare interdisciplinary research in the e-healthcare area.
Biographies
I-Chiu Chang is an associate professor of MIS at National Chung Cheng University, Taiwan. She received her PhD from the University of Texas at Arlington, USA. Her research interests include Decision Support Systems, Healthcare Information Systems, and Electronic Medical Records. Her published works have appeared in Decision support systems, Industrial Management and data Systems, Medical Informatics and the Internet in Medicine, OMAGA, and Government Information Quarterly.

Hsin-Ginn Hwang is a professor of MIS at National Chung Cheng University, Taiwan. He received his PhD from the University of Texas at Arlington, USA. His research interests include Decision Support Systems, Security, Healthcare Information Systems, and Electronic Medical Records. His published works have appeared in Information Management and Computer Security, Medical Informatics and the Internet in Medicine, Government Information Quarterly, and DSS.

Ming-Chien Hung is a lecturer of the Department of E-Business at WuFeng Institute of Technology, Taiwan. His research interests are information management, hospital information systems management, and electronic commerce. He has been publishing papers on academic journals, conference proceedings and books.

Ming-Hui Lin is a deputy director of Information Department at Chi Mei Medical Center, Taiwan. His Research interests include hospital information systems, and management information systems.

David C. Yen is Raymond E. Glos Professor of the Department of Decision Sciences and Management Information Systems at Miami University, USA. He received a Ph.D. in MIS and Master of Sciences in Computer Science from the University of Nebraska, USA. Professor Yen is active in research, he has published articles which have appeared in Communications of the ACM, Decision Support Systems, Information and Management, International Journal of Information Management, Information Sciences, Journal of Computer Information Systems, Interfaces, Telematics and Informatics, Computer Standards and Interfaces, Information Society, Omega, International Journal of Organizational Computing and Electronic Commerce, Communications of AIS, and Internet Research among others.
Contributor Information
I-Chiu Chang, Email: misicc@mis.ccu.edu.tw.
Hsin-Ginn Hwang, Email: mishgh@mis.ccu.edu.tw.
Ming-Chien Hung, Email: chemy@mail.wfc.edu.tw.
Ming-Hui Lin, Email: lmh@mail.chimei.org.tw.
David C. Yen, Email: yendc@muohio.edu.
Appendix A.
Appendix A.1Operational definitions and measurement of research variables
| Dimensions | Factors | Operational definitions (scale item) | References |
|---|---|---|---|
| Organizational characteristics | User involvement | The degree of user's involvement during phases of Information requirements analysis (USER 1); Reviewing consultant's recommendations (USER 2); Project meetings (USER 3); and Decision-making (USER 4) | [45] |
| Adequate resources | The resources available for adopting e-signature in terms of usual encouragement (RES 1); Abundant time (RES 2); Abundant funding (RES 3); Abundant human resources (RES 4); and Executive involvement (RES 5) | [42] | |
| Hospital size | In terms of number of beds (SIZE 1); Number of employees (SIZE 2); and Business volume of a hospital (SIZE 3) | [32] | |
| Internal need | In terms of reducing paperwork (NEED1); Cutting cost in operations (NEED2); and Offering differentiated service for efficiency (NEED3) | [31] | |
| Environmental characteristics | Vendor support | In terms of quality of technical support (VEND1); Quality of training (VEND2); Adequate technical support during adoption (VEND3); Abundant training (VEND4); and Adequate technical support after adoption (VEND5) | [45] |
| Government policy | In terms of setting up HCA (GOV 1); Health insurance IC card (GOV 2); EMR trend (GOV 3); Government's assistance (GOV 4) | [16] | |
| E-signature characteristics | Security protection | Degree of security in terms of security training (SECUR1); Classified management (SECUR2); Security of entity/environment (SECUR3); Access control (SECUR4); Organization of information security (SECUR5); Continuity of operational activity (SECUR6) | [2] |
| System complexity | Degree of complexity in terms of work practices in operating the system (SYS1); Complexity in developing the system process (SYS2); Used complexity in integrating the system (SYS3) | [11], [32] |
Appendix A.2 Principal component analysis of each dimension
| Dimensions | Factors | Measured Items | Factor loading | Eigen-values | % of Var. (Cum.%) | Cronbach's α value |
|---|---|---|---|---|---|---|
| Organizational characteristics | User involvement | USER1 | .911 | 3.306 | 22.038% (22.038%) | .9284 |
| USER2 | .891 | |||||
| USER3 | .867 | |||||
| USER4 | .820 | |||||
| Adequate resources | RES1 | .821 | 3.278 | 21.852% (43.889%) | .8603 | |
| RES2 | .817 | |||||
| RES3 | .817 | |||||
| RES4 | .793 | |||||
| RES5 | .707 | |||||
| Hospital size | SIZE1 | .961 | 2.720 | 18.131% (62.020%) | .9383 | |
| SIZE2 | .939 | |||||
| SIZE3 | .910 | |||||
| Internal need | NEED1 | .857 | 2.359 | 15.730% (77.750%) | .8319 | |
| NEED2 | .831 | |||||
| NEED3 | .804 | |||||
| Environmental characteristics | Vendor support | VEND1 | .946 | 4.079 | 45.318% (45.318%) | .9379 |
| VEND2 | .924 | |||||
| VEND3 | .895 | |||||
| VEND4 | .889 | |||||
| VEND5 | .813 | |||||
| Environmental characteristics | Government policy | GOV 1 | .833 | 2.617 | 29.083% (74.401%) | .8078 |
| GOV 2 | .819 | |||||
| GOV 3 | .767 | |||||
| GOV 4 | .760 | |||||
| E-signature characteristics | Security protection | SECUR1 | .875 | 4.029 | 44.766% (44.766%) | .9042 |
| SECUR2 | .859 | |||||
| SECUR3 | .845 | |||||
| SECUR4 | .776 | |||||
| SECUR5 | .761 | |||||
| SECUR6 | .735 | |||||
| System complexity | SYS1 | .825 | 2.027 | 22.527% (67.292%) | .7199 | |
| SYS2 | .808 | |||||
| SYS3 | .717 |
References
- 1.Blobel B. Advanced tool kits for EPR security. International Journal of Medical Informatics. 2000;60(2):169–175. doi: 10.1016/s1386-5056(00)00117-9. [DOI] [PubMed] [Google Scholar]
- 2.BSI . British Standards Institution (BSI); 1999. Information Security Management — Part 2: Specification for Information Security Management Systems, BS 7799-2. [Google Scholar]
- 3.Chang I.C., Hwang H.G., Yen D.C., Lian J.W. Critical factors for adopting PACS in Taiwan: views of radiology department directors. Decision Support Systems. 2006;42:1042–1053. [Google Scholar]
- 4.Cheng T.C.E., Lam D.Y.C., Yeung A.C.L. Adoption of internet banking: an empirical study in Hong Kong. Decision Support Systems. 2006;42:1558–1572. [Google Scholar]
- 5.Cooper D.R., Schindler P. McGraw Hill; 2003. Business Research Methods. [Google Scholar]
- 6.Cooper R.B., Zmud R.W. Information technology implementation research: a technological diffusion approach. Management Science. 1990;36(2):123–139. [Google Scholar]
- 7.Dutta A., Heda S. Information systems architecture to support managed care business processes. Decision Support Systems. 2000;30:217–225. [Google Scholar]
- 8.Eloff M.M., Solms S.H. Information security management: an approach to combine process certification and product evaluation. Computers & Security. 2000;19(8):698–709. [Google Scholar]
- 9.Gatignon H., Robertson T.S. Technology diffusion: an empirical test of competitive effects. Journal of Marketing. 1989;53(1):35–49. [Google Scholar]
- 10.Gorsuch R.L. Lawrence Erlbaum; Hillsdale, NJ: 1983. Factor Analysis. [Google Scholar]
- 11.Grover V. An empirically derived model for the adoption of customer-based interorganizational systems. Decision Sciences. 1993;24(3):603–640. [Google Scholar]
- 12.Gupta A., Tung Y.A., Marsden J.R. Digital signature: use and modification to achieve success in next generational e-business processes. Information & Management. 2004;41(5):561–575. [Google Scholar]
- 13.Hair J.F., Anderson R.E., Tatham R.L., Black W.C. 5th ed. Prentice Hall; New Jersey: 1998. Multivariate Data Analysis. [Google Scholar]
- 14.Hajdukiewicz J.R., Vicente K.J., Doyle D.J., Milgram P., Burns C.M. Modeling a medical environment: an ontology for integrated medical informatics design. International Journal of Medical Informatics. 2001;62(1):79–99. doi: 10.1016/s1386-5056(01)00128-9. [DOI] [PubMed] [Google Scholar]
- 15.Hartono E., Santhanam R., Holsapple C.W. Factors that contribute to management support system success: an analysis of field studies. Decision Support Systems. 2007;43:256–268. [Google Scholar]
- 16.Ho K.C., Hui P.C.L., Tao X., Yeung P.K.W. Measuring the technological development of the textiles and clothing industry in Hong Kong. International Journal of Services Technology and Management. 2003;4(3):255–286. [Google Scholar]
- 17.Huang S.M., Hung Y.C., Yen D.C. A study on decision factors in adopting an online stock trading system by brokers in Taiwan. Decision Support Systems. 2005;40:315–328. [Google Scholar]
- 18.Hwang H.G., Ku C.Y., Yen D.C., Cheng C.C. Critical factors influencing the adoption of data warehouse technology: a study of the banking industry in Taiwan. Decision Support Systems. 2004;37:1–21. [Google Scholar]
- 19.Junglas I.A., Watson R.T. International Conference on Information Systems (Dec 14–17th, Seattle, WA) 2003. U-commerce: a conceptual extension of E- and M-commerce. [Google Scholar]
- 20.Kaiser H.F. An index of factorial simplicity. Psychometrika. 1974;39:31–36. [Google Scholar]
- 21.Kerlinger F.N., Lee H.B. 4th ed. Thomson Learning; New York: 2000. Foundations of Behavioral Research. [Google Scholar]
- 22.KFSYSCC, http://www.kfsyscc.org/index.php?menu_id=735, 2005 (In Chinese).
- 23.Lawrence M., Low G. Exploring individual user satisfaction within user-led development. MIS Quarterly. 1993;17(2):195–208. [Google Scholar]
- 24.Lin T.M. Survey of current development on computerized medical records with hospitals. 2003. http://www.doh.gov.tw/EN/Webpage/index.aspx
- 25.Liu R.L., Lu Y.L. Distributed agents for cost-effective monitoring of critical success factors. Decision Support Systems. 2003;35:353–366. [Google Scholar]
- 26.Minihan J. Electronic signature technologies: a tutorial. Information Management Journal. 2001;35(4):4–8. [Google Scholar]
- 27.MOEA Electronic signatures act, Ministry of Economic Affairs, R.O.C. 2002. http://www.esign.org.tw/English.asp
- 28.Nunnally J.C. 2nd ed. McGraw-Hill; New York: 1978. Psychometric Theory. [Google Scholar]
- 29.Nunno R.M. Electronic signatures: technology developments and legislative issues. Government Information Quarterly. 2000;17(4):395–401. [Google Scholar]
- 30.Poon P., Wagner C. Critical success factors revisited: success and failure cases of information systems for senior executives. Decision Support Systems. 2001;30:393–418. [Google Scholar]
- 31.Premkumar G., Ramamurthy K. The role of interorganizational and organizational factors on the decision mode for adoption of interorganizational systems. Decision Sciences. 1995;26(3):303–336. [Google Scholar]
- 32.Premkumar G., Roberts M. Adoption of new information technologies in rural small business. Omega. 1999;27(4):467–484. [Google Scholar]
- 33.Premkumar G., Ramamurthy K., Nilakanta S. Implementation of electronic data interchange: an innovation diffusion perspective. Journal of Management Information Systems. 1994;11(2):157–186. [Google Scholar]
- 34.Rainer R.K., Watson H.J. The keys to executive information system success. Journal of Management Information Systems. 1995;12(2):83–98. [Google Scholar]
- 35.Rogers E.M. The Free Press; New York: 1995. Diffusion of Innovations. [Google Scholar]
- 36.Romeo A. Interindustry & interfirm differences in the rate of diffusion of an innovation. The Review of Economics and Statistics. 1975;57(53):311–319. [Google Scholar]
- 37.Swanson E.B. Information systems innovation among organizations. Management Science. 1994;40(9):1069–1092. [Google Scholar]
- 38.Tait P., Vessey I. The effect of user involvement on system success: a contingency approach. MIS Quarterly. 1988;12(1):91–108. [Google Scholar]
- 39.Tornatzky L.G., Fleischer M. Lexington Books; Lexington, MA: 1990. The Process of Technology Innovation. [Google Scholar]
- 40.van Ginneken A.M. The computerized patient record: balancing effort and benefit. International Journal of Medical Informatics. 2002;65(2):97–119. doi: 10.1016/s1386-5056(02)00007-2. [DOI] [PubMed] [Google Scholar]
- 41.Waegemann C.P. Spotlight on healthcare: document imaging in healthcare: one piece of the puzzle in creating electronic patient record systems. Inform. 2000;14(1):8–10. [Google Scholar]
- 42.Watson H.J., Haley B.J. Data warehousing: a framework and survey of current practices. Journal of Data Warehousing. 1997;2(1):10–17. [Google Scholar]
- 43.West D.M. Global e-government. 2004. http://www.insidepolitics.org/egovt03int.html
- 44.Wilson E.V., Lankton N.K. Interdisciplinary research and publication opportunities in information systems and healthcare. Communications of the Association for Information Systems. 2004;14:332–343. [Google Scholar]
- 45.Yap C.S., Thong J.Y.L., Raman K.S. Effect of government incentives on computerization in small business. European Journal of Information Systems. 1994;3(3):191–206. [Google Scholar]
- 46.Zhu K., Kraemer K., Xu S. Electronic business adoption by European firms: a cross-country assessment of the facilitators and inhibitors. European Journal of Information Systems. 2003;12(4):251–268. [Google Scholar]
- 47.Zmud R.W. An examination of ‘push–pull’ theory applied to process innovation in knowledge work. The Institute of Management Sciences. 1984;30(6):727–738. [Google Scholar]