

Abstract
Diarrhea is the leading cause of death in neonatal calves and contributes to major economic losses. The objective of this double-blind randomized clinical trial was to evaluate the effect of oral inorganic or organic zinc supplementation as a treatment for neonatal diarrhea in calves. Seventy nine 1 to 8 day old male Holstein calves on a California calf ranch were block randomized to one of 3 treatments within 24 h from their first onset of diarrhea. Calves received a daily dose of either a placebo composed of 80 mg of zinc-free powder, 381.54 mg of zinc methionine (Met) (equivalent to 80 mg of zinc), or 99.69 mg of zinc oxide (ZO) (equivalent to 80 mg of zinc) in 2 L of a zinc-free oral rehydration solution (ORS). Calves were treated once daily until normal fecal consistency or for a maximum of 14 days. Upon enrollment and exit, calves were weighed, and blood, feces, and liver biopsies were collected for trace mineral analysis. Fecal samples at enrollment and exit were tested for E. coli K99, Cryptosporidium spp., rotavirus and coronavirus. Pre-treatment liver zinc concentrations for the 71 calves in the placebo, zinc Met, and ZO treatment groups were 710.6 (SEM = 147.7), 852.3 (SEM = 129.6), and 750.7 (SEM = 202.9) mg/kg dry weight (DW), respectively. Exit liver zinc concentrations for the calves in the placebo, zinc Met, and ZO treatment groups were 728.9 (SEM = 182.9), 1141.0 (SEM = 423.8), and 636.8 (SEM = 81.5) mg/kg dry weight, respectively. Although statistically non-significant, there were clinically important findings identified for each of zinc Met and ZO treatments. Calves treated with zinc Met gained on average 40 g/day during a diarrhea episode compared to a weight loss of 67 g/day on average in the placebo-treated calves (Power 19.9%). Calves treated with ZO had 1.4 times higher hazard of clinical cure compared to calves in the placebo group (Power 5.3%). Calves that were fecal positive to cryptosporidium spp. at enrollment and treated with zinc Met had higher odds of testing negative at exit compared to placebo calves (Odds Ratio (OR) = 16.0). In contrast, calves treated with ZO tended to recover (fecal score = 1) one day earlier compared to calves treated with a placebo (8.5 d vs. 9.7 d). The current trial identified clinically important findings that warrant further research to investigate zinc's therapeutic effect for calf diarrhea.
Keywords: Calf, Diarrhea, Zinc methionine, Zinc oxide, Cryptosporidium
1. Introduction
Considerable economic losses may be incurred from neonatal diseases during calf rearing. In 2006, 8% of pre-weaned heifers and 2% of weaned heifers died primarily due to diarrhea and other gastrointestinal illnesses (NAHMS, 2010). Similarly in pediatrics, diarrhea is the leading cause of death in children under the age of 5 years in developing countries and is estimated to cause 3 million deaths annually (Bhutta et al., 2000, Hoque et al., 2009). In 2004, based on numerous randomized clinical trials, the World Health Organization recommended zinc supplementation of oral rehydration solutions to decrease the duration and severity of infant diarrhea (Bhutta et al., 1999, Faruque et al., 1999, Penny et al., 1999). Infants with diarrhea for more than 10 days had significantly lower serum zinc levels compared to healthy infants or infants with other non-gastrointestinal illnesses (Naveh et al., 1982), suggesting gastrointestinal loss of zinc (Hoque et al., 2009). Zinc-supplemented ORS also resulted in increased recovery rates, reduced mortality and a reduction in use of antibiotics (Bhandari et al., 2008, Bhutta et al., 2000, Bhutta et al., 1999). Although the exact underlying mode of action of zinc is still not known, (Hoque et al., 2009) a mucosal-protective role, enhanced cell-mediated immunity, and modification of intra-luminal electrolyte secretion and absorption mechanisms have been proposed (Atia and Buchman, 2009, Fischer Walker et al., 2009, Hoque et al., 2009). Similar benefits of zinc-supplemented ORS on diarrhea in calves could significantly impact the economics and sustainability of the production system by reducing antibiotic use for treatment of calf diarrhea. Zinc studies have demonstrated its beneficial effects in piglets and rats, and on calf growth and fetal development (Graham et al., 2010, Graham et al., 1984, Owusu-Asiedu et al., 2003). However, the therapeutic use of zinc in calves with diarrhea has not been studied. A comparison of inorganic and organic formulations of zinc such as zinc oxide (ZO) and zinc methionine (Met), respectively, is warranted because of differences in zinc bioavailability (Wedekind et al., 1992). A greater effectiveness of an inorganic zinc formulation in treating calf diarrhea compared to an organic formulation may be evidence of zinc's local intra-luminal mode of action given its poor absorption in the intestines (absorption coefficient of ZO = 0.12 compared to 0.40 for zinc Met) (Cousins, 1985). On the other hand, if zinc Met is found to be more effective than ZO in treating diarrhea this may be evidence for a systemic mode of action given the greater bioavailability of zinc Met compared to ZO. In addition, because zinc is an antagonist of copper (NRC, 2001), a comprehensive assessment of trace minerals is necessary when administering zinc to calves.
The hypothesis of this block-randomized double-blind clinical trial is that neonatal Holstein calves with diarrhea supplemented with either zinc Met or ZO will experience reduced days to recovery from diarrhea, reduced mortality, and reduced weight lost during the diarrhea episode compared to the placebo treated calves. The objective of this clinical trial was to compare the effect of a daily dose of ZO or zinc Met equivalent to 80 mg of zinc, or a placebo for a maximum of 14 days on fecal output and recovery in otherwise untreated 1 to 8 day-old Holstein bull calves with neonatal diarrhea on a California calf ranch. A secondary objective was to assess the effect of zinc Met or ZO on serum and liver zinc, copper, and iron concentrations.
2. Materials and methods
2.1. Study population
All procedures were approved by the University of California Davis Institutional Animal Care and Use Committee (protocol number 16232). The clinical trial was conducted between June and September 2011 on a large California calf ranch in the San Joaquin Valley housing approximately 70,000 Holstein calves, 40,000 of which were of preweaning age. Calves enrolled included all male Holsteins that developed diarrhea for the first time between 1 and 8 days of age. Calves were excluded from the study if they had a previous incident of diarrhea since birth or signs of disease other than diarrhea, such as an umbilical abscess, pneumonia, or meningitis, or if they were previously treated with antimicrobial drugs. Calves with diarrhea were identified by a veterinarian (AG) prior to enrollment.
2.2. Sample size estimation
Due to lack of estimates in neonatal calves, the sample size estimation was based on the difference between serum zinc levels of infants with and without diarrhea. The increase in serum zinc levels post treatment in calves was assumed to be similar to that in infants (Naveh et al., 1982). Hence the sample size was calculated to detect a statistically significant difference in serum zinc concentrations in treated calves (mean ± SD, 87 ± 20 μg/dl) and placebo calves (100 ± 14 μg/dl) with a power of 80% and level of significance of 5%. A total of 22 calves per group were required. Allowing for a 15% loss to follow-up, a total of 26 calves per group (n = 78 total) were required in the study.
2.3. Study design and zinc administration
Prior to initiation of the study, zinc concentrations of water, calf starter grain, milk replacer, and electrolyte powder were determined. All calves on the calf ranch received the same diet in the hutches consisting of 2 L of milk replacer twice daily, free access to water, and a calf starter grain mix. The electrolyte powder is a proprietary mix and was submitted for heavy metal analysis; it contains 4.5 ppm iron. All other heavy metals were not detected. Pretrial samples collected from the water contained no detectable zinc. Calf starter grain contained 22 mg/kg zinc DM, and milk replacer had 2.4 mg/kg zinc DM. Calves were randomized by a veterinarian (AG) to one of the 3 treatments in blocks that ranged from 3 to 15 calves depending on the number of calves eligible at each enrollment day. The randomization scheme was generated using Microsoft Excel 2010 by a different veterinarian (SA). Treatments (placebo, zinc Met, or ZO) were placed into 2.0 ml locking-lid microcentrifuge tubes with polypropylene snap-cap (Fisher Scientific, Pittsburgh, PA) and labeled 1, 2, or 3 (SA). Treatment allocation, administration and data recording were performed by AG while being blinded to the true treatments until completion of the trial. Success of blinding and randomization at producing comparable groups was evaluated by comparing baseline values at enrollment using ANOVA for clinical parameters (Table 1 ) and trace mineral concentrations (Table 2 ). Calves received a single daily oral dose of either 99.69 mg of a zinc-free placebo (electrolyte powder used to make ORS; group 1), 381.54 mg of zinc Met (equivalent to 80 mg of zinc; group 2), or 99.69 mg of ZO (equivalent to 80 mg of zinc; group 3) dissolved in 2 L of a zinc-free ORS solution. The dose of 80 mg zinc per day was based on the ratio of human zinc nutrient requirement (NHMRC, 2005) to zinc supplementation of ORS (1:6.7) (Bhandari et al., 2008, Bhutta et al., 1999, Patel et al., 2009). This was verified to be less than the ratio in calves of recommended zinc intake (NRC, 2001) to toxic levels (1:37.5) (Graham et al., 1988, Graham et al., 1987b).
Table 1.
Baseline clinical parameters (rectal temperature, weight, and attitude) of neonatal Holstein calves at enrollment (prior to treatment) into one of the three treatment groups (placebo, zinc methionine (Met), or zinc oxide (ZO)) from a double-blind block-randomized clinical trial on the effect of zinc as a treatment for diarrhea.
| Variable | Treatmenta, b |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo |
Zinc Met |
ZO |
|||||||||||
| N | Mean | SEM | 95% C.I. | Mean | SEM | 95% C.I. | Mean | SEM | 95% C.I. |
||||
| Lower | Upper | ||||||||||||
| Rectal temperature (°C) | 71 | 38.55 | 0.12 | 38.30 | 38.79 | 38.80 | 0.10 | 38.61 | 39.00 | 38.42 | 0.12 | 38.19 | 38.68 |
| Weight (kg) | 72 | 42.34 | 0.98 | 40.32 | 44.36 | 41.34 | 1.18 | 38.90 | 43.78 | 42.62 | 1.08 | 40.37 | 44.89 |
| Attitudec | 74 | 1.04 | 0.04 | 0.96 | 1.12 | 1.08 | 0.05 | 0.97 | 1.19 | 1.04 | 0.04 | 0.95 | 1.13 |
Treatment: Placebo = zinc-free oral rehydration solution (ORS); zinc Met = 80 mg of zinc/2 L of ORS (381.5 mg of zinc Met); ZO = 80 mg of zinc/2 L of ORS (99.7 mg of ZO).
No significant differences in means within the same row (P < 0.05).
Attitude Scores: 1 = calf was standing, bright, alert, responsive, and had a good suckle reflex; 2 = calf stood only after stimulation and had a moderate suckle reflex; 3 = calf was recumbent, did not stand with stimulation, and had a weak or absent suckle reflex.
Table 2.
Fecal zinc, serum zinc, and liver zinc, copper, and iron, concentrations expressed as means in neonatal Holstein calves before and after treatment with placebo, zinc methionine (Met), or zinc oxide (ZO) from a double-blind block-randomized clinical trial on the effects of zinc as a treatment for diarrhea.
| Samplec | Pre/Post | N | Treatmentsa, b |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo |
Zinc Met |
ZO |
||||||||||||
| Mean | SEM | 95% C.I. | Mean | SEM | 95% C.I. | Mean | SEM | 95% CI |
||||||
| Lower | Upper | |||||||||||||
| Fecal zinc | Pre | 71 | 135.9 A | 17.0 | 100.9 | 171.0 | 153.6 A | 21.9 | 108.5 | 198.8 | 153.0 A | 14.1 | 123.6 | 182.3 |
| Post | 71 | 378.4 A | 48.2 | 278.4 | 478.5 | 1128.9 B | 255.5 | 601.5 | 1656.3 | 651.3 AB | 53.4 | 540.5 | 762.0 | |
| Serum zinc | Pre | 71 | 0.95 A | 0.04 | 0.87 | 1.03 | 0.91 A | 0.04 | 0.82 | 1.00 | 0.91 A | 0.07 | 0.76 | 1.05 |
| Post | 71 | 1.09 A | 0.05 | 0.99 | 1.19 | 1.28 B | 0.05 | 1.18 | 1.39 | 1.16 AB | 0.05 | 1.05 | 1.26 | |
| Liver zincd | Pre | 71 | 710.6 A | 147.7 | 405.2 | 1016.1 | 852.3 A | 129.6 | 585.4 | 1119.1 | 750.7 A | 202.9 | 327.5 | 1173.9 |
| Post | 68 | 728.9 A | 182.9 | 349.6 | 1108.3 | 1141.0 A | 423.8 | 264.2 | 2017.7 | 636.8 A | 81.5 | 466.9 | 806.8 | |
| Liver copper | Pre | 73 | 483.9 A | 51.3 | 378.1 | 589.8 | 500.4 A | 68.9 | 358.6 | 642.3 | 477.3 A | 59.8 | 353.0 | 601.6 |
| Post | 70 | 683.0 A | 119.7 | 435.3 | 930.7 | 741.7 A | 211.5 | 304.2 | 1179.1 | 468.1 A | 63.5 | 336.1 | 600.0 | |
| Liver irond | Pre | 71 | 381.7 A | 72.4 | 232.2 | 531.2 | 363.3 A | 65.9 | 227.6 | 499.1 | 205.9 A | 33.3 | 136.3 | 275.5 |
| Post | 68 | 347.3 A | 90.6 | 159.9 | 534.6 | 254.1 A | 46.5 | 157.9 | 350.3 | 157.7 A | 24.4 | 106.7 | 208.8 | |
Treatments: Placebo = zinc-free oral rehydration solution (ORS); zinc Met = 80 mg of zinc/2 L of ORS (381.5 mg of zinc Met); ZO = 80 mg of zinc/2 L of ORS (99.7 mg of ZO).
Means with different letters within each row are significantly different (P < 0.05).
Fecal zinc (mg/kg of DW), serum zinc (mg/L), and liver zinc, copper, and iron (mg/kg of DW).
Liver zinc and iron concentration pre and post treatment: liver biopsy samples were insufficient for accurate zinc or iron determination in two samples. Thus, two calves had to be excluded from liver zinc and iron enrollment and exit analysis.
2.4. Data collection
Upon enrollment, each calf was weighed (kg; Salter Brecknell PS-500 scale, Fairmont, MN) and received a complete physical examination. As part of the physical examination the rectal temperature (°C), fecal consistency, and attitude were scored for each calf. Fecal output was scored by a single veterinarian (AG) after adapting fecal scores from the University of Wisconsin's calf health scoring chart (http://www.vetmed.wisc.edu/dms/fapm/fapmtools/8calf/calf_health_scoring_chart.pdf). A fecal sample that was solid, semi-formed/loose, or watery was assigned 1, 2 or 3, respectively. A decision was made to merge the original chart's semi-formed and loose categories for consistency given the potential for difficulty distinguishing between both on the raised slatted wooden floors of calf hutches. A similar simple scoring system for calf attitude was followed. A calf with an attitude score of 1 was standing, bright, alert, responsive and had a good suckle reflex; a score 2 calf stood only after stimulation and had a moderate suckle reflex; and a score 3 calf was recumbent, did not stand with stimulation and had a weak or absent suckle reflex. After enrollment, fecal consistency and attitude for all trial calves were recorded every other day. Fecal and venous blood samples were collected at enrollment, every other day thereafter, and at exit from trial. In addition, a liver biopsy (Swanson et al., 2000) was collected from each calf at enrollment and exit. Calves enrolled were followed up every other day (physical exam, blood and fecal samples collected) and continued receiving their allocated treatment until clinical signs resolved (normal rectal temperature, no diarrhea for 24–48 h, and attitude score of 1) or for a maximum of 14 days at which time calves were eligible for exit.
2.5. Liver biopsy procedure
The liver biopsy was collected as described elsewhere (Swanson et al., 2000). Briefly, hair was removed from the ribs between the 10th and 13th right intercostal space. The site was disinfected using povidone iodine scrub, alcohol and povidone iodine solution. The incision site was blocked with 2 ml of 2% lidocaine using an 18 gauge 1 ½ inch needle into the skin and thoracic muscles. A stab incision was made with a carbon steel #15 surgical blade approximately 10 cm from the dorsal midline between the 11th and 12th intercostal space. A 14 gauge 15 cm sterile CareFusion Tru-Cut biopsy needle (San Diego, CA) was inserted through the incision and a liver biopsy was collected. A rapid acting adhesive was used for skin closure. The liver biopsy was immediately placed into a 2.0 ml locking-lid microcentrifuge tube with polypropylene snap-cap and stored on ice for a period no more than 3 h before being stored at −80 °C until submission to the testing at the participating laboratory.
2.6. Blood collection
Blood was collected from the jugular vein using a 20 gauge 1 ½ inch needle and placed into 3.0-ml tubes (BD Vacutainer, Franklin, NJ) that either contained K2-EDTA to assess packed cell volume (PCV) and total plasma protein (TPP) concentration, or specialized trace element tubes (royal blue top tubes; RBTT) for trace mineral analysis. Sample PCV (%) was measured using microhematocrit centrifugation, and TPP (g/dl) was measured using a Reichert-Jung Refractometer. The trace element blood tubes were spun in a centrifuge for 10 min, serum decanted into a 2.0 ml locking-lid microcentrifuge tube with polypropylene snap-cap and stored at −80 °C. Fecal samples were placed in a sterile 50-ml polypropylene centrifuge tube and stored at −80 °C. All fecal and serum samples were tested within 3 months from collection.
2.7. Sample analyses
2.7.1. Infectious disease testing
Fecal samples collected at enrollment and exit were tested at the Dairy Epidemiology Laboratory, VMTRC for Cryptosporidium spp. oocysts, bovine rotavirus and coronavirus, and E. coli K99 using a commercial kit that is highly specific (greater than 90%) and sensitive (coronavirus, 77%; E. coli K99, 93%; rotavirus, 100%) (Biovet, Quebec, Canada) (Robert et al., 1990, Thorns et al., 1992). Fecal samples were not initially tested for Salmonella due to a historically low prevalence of Salmonella in bi-monthly screening routinely conducted on the study calf ranch.
2.7.2. Necropsy and tissue collection
Calves that died during the study were necropsied to determine the cause of death. Toxicological tests were conducted at California Animal Health and Food Safety (CAHFS) Laboratory in Davis, CA. For heavy metal analysis of liver samples, approximately 0.5 g (biopsy) or 50 g (carcass) of liver were placed into a sterile plastic Nasco Whirl-Pak (Thermo Fisher Scientific Inc., Wilmington, MA) and stored at −80 °C until analysis. Tissue samples were shipped frozen to the CAHFS Toxicology Laboratory. In order to determine percent of moisture, tissue samples were placed in a drying oven at 95 °C and weighed daily until constant weight indicated complete removal of moisture.
2.7.3. Trace mineral analysis: liver
Liver samples were digested with nitric acid and analyzed for lead, manganese, iron, mercury, arsenic, molybdenum, zinc, copper, and cadmium by inductively coupled argon plasma emission spectrometry (ICA-PES; ARL, Accuris Model, Thermo Optek Corporation, Franklin, MA). Accuracy of ICA-PES was measured by analyzing standard reference materials (SRM) such as bovine liver (National Bureau of Standards and Technology, SRM 1577b) and lobster hepatopancreas (National Research Council of Canada TORT-2). Data were accepted if values for standard reference material fell within 2 standard deviations of the certified reference value. Metal concentrations were determined on a wet weight basis and converted to concentrations per dry weight by dimensional analysis as follows, heavy metal in mg/kg dry mass = heavy metal in mg/kg wet weight × [100/(100 − % moisture)]. Calves were excluded from liver mineral analysis if the liver biopsy submitted was less than 5 mg of wet weight.
2.7.4. Trace mineral analysis: feed samples
Feed samples (DM) were digested with nitric acid and analyzed for lead, manganese, cadmium, copper, iron, zinc, molybdenum, arsenic, and mercury by ICA-PES. Accuracy of ICA-PES results was measured by analyzing SRM and over-spiked feed samples of similar matrix. The SRM included dogfish liver (National Research Council of Canada, DOLT-4) and lobster hepatopancreas (National Research Council of Canada, TORT-2). Data were accepted if analyzed SRM values were within 2 standard deviations of the certified reference values and over-spike recovery was 80–120%.
2.7.5. Trace mineral analysis: serum
Zinc, copper, iron, magnesium, sodium, phosphorus, calcium and potassium concentrations were measured in serum samples after precipitation of proteins by using ICA-PES (FISONS, Accuris Model, Thermo Optek Corporation, Franklin, MA). Accuracy of ICA-PES results for these elements was measured by analyzing quality assurance sera obtained from the Veterinary Laboratory Association Quality Assurance Program (Genzyme Diagnostics, Blaine, MD, USA). Data were accepted if analyzed quality assurance serum values were within 2 standard deviations of the reference values.
2.8. Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics software (version 21; Somers, NY) and STATA MP 11.2 (College Station, TX). Statistical differences were determined at the 5% level of significance using intention to treat analysis.
2.8.1. Baseline comparisons
An ANOVA was used to compare calves enrolled in each treatment group prior to administration of the first treatment with respect to rectal temperature (°C), weight (kg), attitude scores, and fecal, serum, and liver zinc, copper, and iron concentrations.
2.8.2. Mean daily weight change
An ANOVA was used to compare mean daily weight change (g) between treatment groups. The mean daily weight change was calculated as the difference between exit and enrollment weights divided by number of days a calf was on the trial.
2.8.3. Fecal zinc, serum zinc, and liver zinc, copper, and iron concentrations at exit
An ANOVA was used to compare calves in each treatment group at exit from the trial with respect to the mean concentration of fecal zinc (mg/kg dry weight, DW), serum zinc (mg/L), and liver zinc, copper, and iron (mg/kg DW).
2.8.4. Clinical cure
Kaplan–Meier analysis was used to determine mean days to a clinical cure for calves that tested positive on fecal ELISA kit at enrollment (Cryptosporidium spp., E. coli K99, coronavirus, or rotavirus) and had a normal fecal score of 1 for at least 24 h. Calves that died or had a fecal score greater than 1 at exit were censored.
Cox Proportional Hazard (PH) regression analysis was used to estimate and compare the hazard for clinical cure as assessed every other day. The proportional hazard assumption that clinical cure hazard is independent of time was assessed using the log-minus-log (LML) survival plots generated for each of the treatment group variables with the placebo group as the reference. The full Cox model for the hazard of a clinical cure in a calf enrolled with diarrhea can be summarized as:
where λ 0 is a non-negative unspecified baseline hazard, independent variables (v1) composed of β i, the regression coefficients estimates for ZM (zinc Met) and ZO, each compared to the placebo, and X i are their respective observed covariate values. Cox proportional hazard regression models were estimated for clinical cure by pathogen at enrollment. Power calculations were performed for non-significant models using the global logrank test and assuming a 5% level of significance, baseline cumulative failure probabilities observed in the placebo group, and model estimates for the hazard ratios of the independent variables (Barthel et al., 2006).
2.8.5. Microbiological cure
Only enrollment and exit fecal samples were tested for pathogens making the exact time to microbiological cure unknown. Hence, logistic regression was used to estimate and compare the odds of microbiological cure at exit (fecal score = 1 or 14 days of treatment) for each treatment group. Microbiological cure was determined if a calf tested negative for all four pathogens at exit (E. coli K99, Cryptosporidium spp., coronavirus or rotavirus). In addition, logistic regression models were estimated for microbiological cure by pathogen at enrollment. Power calculations were performed for models with non-significant coefficients assuming a 5% level of significance and the observed sample sizes and proportion of calves that attained the respective outcome modeled.
3. Results
A total of 79 calves were enrolled with 26 calves in group 1 (placebo), 28 calves in group 2 (zinc Met), and 25 in group 3 (ZO). All the trial calves drank their morning and afternoon two quart daily milk bottles except for two of the calves that died. The enrollment blocks added up to 78 calves. In addition a calf was enrolled in group 2 on the last day bringing the total enrolled to 79 calves. A total of 5 calves were excluded from all analyses including: (1) one calf mistakenly enrolled in group 1 with normal fecal consistency; (2) two calves in group 2: one died immediately after enrollment and its necropsy revealed abomasal torsion; another was enrolled with an umbilical abscess; (3) two calves in group 3: one died after enrollment and necropsy revealed serous atrophy of fat, and the other was moribund at enrollment with severe systemic illness unable to drink milk or electrolyte treatment.
Of the 74 calves in the study, 3 died during the trial: (1) one in group 1 (placebo) with gross lesions of an infarct and perforating ulcer in the cecum; (2) one in group 2 (zinc Met) with enteritis; (3) one in group 3 (ZO) with bilateral bronchopneumonia. There was no evidence of peritonitis associated with the liver biopsies in any of the calves submitted for necropsy. Histology of the formalin-fixed pancreas of each calf that died revealed no damage to the exocrine pancreas, and therefore, no evidence of zinc toxicosis (Gabrielson et al., 1996, Smith and Embling, 1993). The remaining 71 calves were treated once daily with either a placebo, zinc Met, or ZO formulations and were removed from the trial when they developed a normal fecal score of 1, or at the end of a 14 day supplementation period.
3.1. Baseline comparisons
Baseline comparisons between the 3 treatment groups at enrollment showed no significant differences in rectal temperature (°C) (P = 0.06), enrollment weight (kg) (P = 0.65), or attitude (P = 0.82) (Table 1). There were no statistically significant differences between fecal zinc (P = 0.74), serum zinc (P = 0.84), liver zinc (P = 0.80), copper (P = 0.96) or iron (P = 0.13) concentrations at enrollment (Table 2).
3.2. Mean daily weight change
Weight data for 71 calves at enrollment and exit was available for analysis. There were no statistically significant differences in mean daily weight change for calves in the three treatment groups (P = 0.33). However, calves treated with zinc Met experienced a mean daily weight gain of 40.24 g (SD = 374.52) compared to a mean daily weight loss of 66.88 g (SD = 296.16) in the placebo group, or mean daily weight loss of 85.45 g (SD = 245.27) in the ZO group (Fig. 1 ). The power (1 − β) estimate for the comparison of the mean daily weight loss in the placebo group to the mean daily weight gain in the zinc Met was 19.9%. We estimate a sample size of 213 calves per group required to find a statistically significant difference using an α = .05 and a β = 0.10 (power of 90%).
Fig. 1.
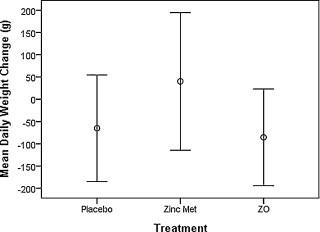
Means and 95% confidence intervals for daily weight change (grams) in neonatal Holstein calves diagnosed with diarrhea and randomly allocated to a placebo, zinc methionine (Met), or zinc oxide (ZO) treatment in a double-blind block-randomized clinical trial to study the effect of zinc as a treatment for diarrhea.
3.3. Fecal zinc, serum zinc, and liver zinc, copper, and iron concentrations at exit
Data for 71 calves was available from fecal and serum zinc, copper, and iron analysis at exit. Data for 3 calves did not exist because they died during the trial and serum and fecal samples were not able to be collected prior to death. At exit, there were no significant difference among calves in the three treatment groups regarding fecal copper (P = 0.67) and iron (P = 0.16). At exit, calves treated with zinc Met had a significantly higher fecal zinc concentration (1128.87 mg/kg DW, P < 0.01) when compared to the placebo calves, and there were no significant differences among calves supplemented with zinc Met and ZO (P = 0.12; Table 2).
At exit, there were no significant differences among calves in the three treatment groups regarding serum copper (P = 0.64) and iron (P = 0.90). Calves treated with zinc Met had significantly higher serum zinc concentrations compared to the placebo group (1.28 mg/L vs. 1.09 mg/L, P = 0.02), and there were no significant differences among calves treated with zinc Met and ZO (P = 0.24; Table 2).
Liver zinc analysis results existed for 71 calves at enrollment. Three calves died during the trial, thus there were only 68 calves available for liver zinc analysis at exit. Calves that died were necropsied and did not have any gross or histopathological signs suggestive of overexposure to zinc (Gabrielson et al., 1996, Smith and Embling, 1993). Liver zinc DW concentrations in calves treated with zinc Met or ZO did not differ significantly from calves treated with a placebo (P = 0.41). The mean (SEM) DW liver zinc concentrations at exit for the placebo, zinc Met and ZO groups were 728.9 (182.9), 1141.0 (423.8), and 636.8 (81.5) mg/kg, respectively. Calves treated with zinc Met had 64% higher DW liver zinc mean concentrations compared to the placebo group, although it was not significantly higher (P = 0.41; Table 2).
Copper liver concentrations were available for 73 calves at enrollment and 70 calves at exit. Three calves died during the trial and thus their liver biopsy samples were not available for analysis at exit. The remaining calves had less than 5 mg tissue mass biopsied and hence were missing liver heavy metal concentration at exit. The mean (SEM) DW liver copper concentrations at exit for the placebo, zinc Met, and ZO groups were 683.0 (119.7), 741.7 (211.5), and 468.1 (63.5) mg/kg, respectively. There were no significant differences between the three groups regarding liver copper DW concentrations at exit (P = 0.41; Table 2).
Liver iron concentrations were available for 71 calves at enrollment and 68 calves at exit. Three calves died during the trial and thus there liver biopsy samples were not available for analysis at exit. Likewise, the mean (SEM) DW liver iron concentrations at exit for the placebo, zinc Met, and ZO groups were 347.3 (90.6), 254.1 (46.5), and 157.7 (24.4) mg/kg, respectively, and there were no significant differences in liver iron DW concentrations among the three treatment groups at exit (P = 0.13; Table 2).
3.4. Clinical cure
A total of 74 calves were included in the Kaplan–Meier survival analysis for mean days to a clinical cure. There were no significant differences in mean days to recovery between calves treated with either the placebo, zinc Met, or ZO (9.7, 9.7, 8.5), respectively; P = 0.21).
Cox regression model results for clinical cure are presented in Table 3, Table 4 . Although there were no significant differences in hazards of clinical cure between the treatment groups, calves that were treated with ZO had 1.4 times higher hazard of a clinical cure at exit (fecal score = 1) compared to calves in the placebo group (P = 0.272; power = 5.3%). For clinical cure by pathogen at enrollment, all 4 calves positive for E. coli K99 at enrollment (2 in the placebo group, 1 in each of the zinc MET and ZO groups) attained clinical cure, hence a survival analysis was not possible. Although not significant, the hazard ratios comparing clinical cure in calves positive for Cryptosporidium spp. or coronavirus at enrollment when treated with ZO in comparison to a placebo were greater than 1 (power = 66.1% and 5.2%, respectively). However, this was not the case for calves that tested positive for rotavirus at enrollment in either zinc Met or ZO groups (power = 5.1%).
Table 3.
Cox Regression model results from a double-blind block-randomized clinical trial on the effect of treatment with zinc methionine (Met) or zinc oxide (ZO) compared to a placebo on clinical curea in neonatal Holstein calves with diarrhea.
| Treatmentb | Enrollment (n) |
Clinical cure at exit (n) |
β | SE | Hazard ratio | 95% CI |
P-value | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Placebo | 24 | 21 | ||||||
| Zinc Met | 26 | 22 | −0.091 | 0.306 | 0.91 | 0.50 | 1.66 | 0.766 |
| ZO | 23 | 22 | 0.339 | 0.308 | 1.40 | 0.77 | 2.57 | 0.272 |
Clinical cure defined as normal fecal consistency for at least 24 h.
Treatment: Placebo = zinc-free oral rehydration solution (ORS); zinc Met = 80 mg of zinc/2 L of ORS (381.5 mg of zinc Met); ZO = 80 mg of zinc/2 L of ORS (99.7 mg of ZO).
Table 4.
Cox Regression model results from a double-blind block-randomized clinical trial on the effect of treatment with zinc methionine (Met) or zinc oxide (ZO) compared to a placebo on clinical curea in neonatal Holstein calves with diarrhea by pathogen at enrollment.
| ELISA status at enrollment | Treatmentb | Enrollment (n) | Clinical cure at exit (n) | β | SE | Hazard ratio | 95% CI |
P-value | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Cryptosporidium spp. | Placebo | 5 | 5 | Reference | |||||
| Zinc Met | 5 | 3 | −0.511 | 0.730 | 0.60 | 0.14 | 2.51 | 0.484 | |
| ZO | 10 | 10 | 1.249 | 0.716 | 3.49 | 0.86 | 14.18 | 0.081 | |
| Coronavirus | Placebo | 15 | 12 | Reference | |||||
| Zinc Met | 11 | 9 | −0.193 | 0.442 | 0.83 | 0.35 | 1.96 | 0.663 | |
| ZO | 11 | 10 | 0.196 | 0.435 | 1.22 | 0.52 | 2.86 | 0.652 | |
| Rotavirus | Placebo | 11 | 11 | Reference | |||||
| Zinc Met | 14 | 13 | −0.068 | 0.418 | 0.93 | 0.41 | 2.12 | 0.871 | |
| ZO | 11 | 11 | −0.123 | 0.429 | 0.88 | 0.38 | 2.05 | 0.774 | |
Clinical cure defined as normal fecal consistency for at least 24 h.
Treatment: Placebo = zinc-free oral rehydration solution (ORS); zinc Met = 80 mg of zinc/2 L of ORS (381.5 mg of zinc Met); ZO = 80 mg of zinc/2 L of ORS (99.7 mg of ZO).
3.5. Microbiological cure
Results of logistic regression models for microbiological cure are summarized in Table 5, Table 6 . Although not statistically significant, the odds of testing negative for all four pathogens at exit were 1.55 times higher in calves treated with zinc Met compared to calves treated with a placebo (P = 0.455; power = 47.9%). For pathogen specific cure, all calves that tested positive at enrollment for coronavirus (n = 37) or E. coli K99 (n = 4) tested negative at exit (fecal score = 1 or 14 days of treatment). Similarly, out of the 36 calves that tested positive for rotavirus at enrollment only 2 tested positive at exit (fecal score = 1 or 14 days of treatment). Hence, logistic regression analyses for microbiological cure in calves that tested positive for the latter pathogens was not possible. In contrast, calves that tested positive for Cryptosporidium spp. at enrollment and were treated with zinc Met had 16 times higher odds of being fecal ELISA negative at exit compared to the placebo group, however this difference was also not significant (P = 0.08; power = 72.3%).
Table 5.
Logistic regression model results from a double-blind block-randomized clinical trial on the effect of treatment with zinc methionine (Met) or zinc oxide (ZO) compared to a placebo on microbiological curea in neonatal Holstein calves with diarrhea.
| Treatmentb | Fecal ELISA positive at enrollment (n) | Fecal ELISA negative at exit (n) | β | SE | OR | 95% C.I. |
P-value | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Placebo | 23 | 9 | Reference | |||||
| Zinc Met | 24 | 12 | 0.442 | 0.591 | 1.55 | 0.49 | 4.95 | 0.455 |
| ZO | 21 | 4 | −1.01 | 0.701 | 0.37 | 0.09 | 1.45 | 0.152 |
Microbiological cure defined as fecal ELISA test negative for E. coli K99, Cryptosporidium spp., rotavirus, and coronavirus at exit from trial.
Treatment: Placebo = zinc-free oral rehydration solution (ORS); zinc Met = 80 mg of zinc/2 L of ORS (381.5 mg of zinc Met); ZO = 80 mg of zinc/2 L of ORS (99.7 mg of ZO).
Table 6.
Logistic regression model results from a double-blind block-randomized clinical trial on the effect of treatment with zinc methionine (Met) or zinc oxide (ZO) compared to a placebo on microbiological curea in neonatal Holstein calves with diarrhea and Cryptosporidium spp. ELISA positive at enrollment.
| Treatmentb | Cryptosporidium spp. positiveat enrollment (n) | Cryptosporidium spp. negative at exit (n) | β | SE | OR | 95% C.I. |
P-value | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Placebo | 5 | 1 | Reference | |||||
| Zinc Met | 5 | 4 | 2.773 | 1.581 | 16.00 | 0.72 | 354.80 | 0.080 |
| ZO | 10 | 1 | −0.811 | 1.537 | 0.44 | 0.02 | 9.03 | 0.598 |
Microbiological cure defined as fecal ELISA test negative for E. coli K99, Cryptosporidium spp., rotavirus, and coronavirus at exit from trial.
Treatment: Placebo = zinc-free oral rehydration solution (ORS); zinc Met = 80 mg of zinc/2 L of ORS (381.5 mg of zinc Met); ZO = 80 mg of zinc/2 L of ORS (99.7 mg of ZO).
4. Discussion
Data collected from the current trial showed that a daily zinc dose of 80 mg did not result in zinc toxicosis or copper or iron deficiency. The current trial results did not provide evidence for a beneficial effect of either zinc Met or ZO as a treatment for diarrhea in neonatal Holstein calves. This is in contrast to studies on infants that reported a significant reduction in diarrhea-associated mortality after oral zinc supplementation (Bhandari et al., 2008, Bhutta et al., 2000). The difference in findings between the pediatric trials and our calf trial may be explained by the differences in pathogens or disease severity since pediatric research was conducted on diseased infants with more severe clinical signs and a greater risk of mortality compared to calves in our trial. Other explanations for the lack of significant differences among the treatment groups may be due to a sub-therapeutic zinc dose (trial dose provided 80 mg of available zinc/day), or a small sample size. Indeed, estimates of power analyses from the current data show evidence of low sample size.
At exit, calves treated with zinc Met had significantly higher fecal and serum zinc concentrations compared to the placebo treated group, however there were no significant differences in liver zinc concentrations at exit among the three treatment groups. Stratified analysis by duration of treatment (1–5, 6–10, or 11–14 days) showed that calves on treatment for up to 10 days and supplemented with zinc Met had significantly higher fecal zinc concentrations compared to the placebo treated calves, but there were no differences in liver or serum zinc concentrations among the three groups (data not shown). Total zinc was measured in feces (mg/kg DW), and thus we are not able to differentiate between the different forms of zinc. It is known that fecal excretion of zinc increases as the intake of zinc increases in humans, so it is possible that zinc Met was absorbed, metabolized to other forms of zinc, and then excreted via the intestine and bile (Cousins, 1985, Spencer et al., 1985). This trend did not continue for calves treated for more than 10 days. Calves in the trial for more than 10 days and supplemented with zinc Met had significantly higher serum and liver zinc concentrations than the placebo treated calves. These findings are consistent with the increased bioavailability of zinc Met compared to ZO (absorption coefficient of zinc Met = 0.40 compared to 0.12 for ZO) reported by Cousins (1985).
It is known that the bovine fetus is completely dependent on the placenta during gestation for supply of essential trace elements (Hidiroglou and Knipfel, 1981). In addition, liver zinc mean (SEM) concentrations vary from 1110 (193) mg/kg DW during 120–170 days of gestation to 716 (385) mg/kg DW during 221–270 days of gestation (Abdelrahman and Kincaid, 1993). The zinc concentration of bovine colostrum and milk is 15 μg/ml and 3–5 μg/ml, respectively. In the current study, all calves were fed formulated milk replacer containing 2.4 mg/kg zinc DW, the equivalent of 0.29 μg zinc/ml as fed (Abdelrahman and Kincaid, 1993). The National Research Council (NRC) daily zinc recommendation for calves is 40 mg/kg of total diet. There is a significant effect of age on liver zinc concentrations in calves in that the liver zinc concentrations decrease with time after birth (Puschner et al., 2004a). The low levels found in colostrum and milk replacer may reflect adequate tissue reserves of zinc in the bovine neonate (Abdelrahman and Kincaid, 1993, NRC, 2001). Thus if calves are born with adequate zinc stores in the liver and do not require much in the diet, our trial dose of 80 mg of zinc/day was likely too low to have an effect. At exit, trial calves treated with zinc Met had significantly higher fecal (P < 0.01) and serum zinc (P = 0.02) concentrations compared to the placebo group. Despite zinc Met being more bioavailable, it was excreted in the feces. This further indicates that calves have adequate zinc body stores and our trial dose may have been too low to have an effect.
The current trial's zinc dose of 80 mg/day in Holstein calves aged 1–22 days did not result in zinc toxicosis. It is known that clinical signs and death from zinc toxicosis can occur in pre-ruminant calves fed 700 μg zinc/g (mg/kg) diet for 30 days (Graham et al., 1987a). In previous studies where 3–38 day old male Holstein calves were fed milk replacers containing 40, 200, 500, 700, or 1000 mg/kg of zinc, weight gains, DM intakes, and feed efficiencies were reduced at the 700 and 1000 mg/kg level (Jenkins and Hidiroglou, 1991). The calves in the current trial were being fed a formulated milk replacer made on the calf ranch that contained 2.4 mg/kg zinc. The addition of an additional 80 mg of zinc resulted in a total zinc level well below the toxic dose of 700 μg/g of zinc assuming they were fed 1 gallon or 3.79 kg of milk per day. Approximately, total zinc intake level was (3.79 kg × 2.4 mg) + 80 mg = 89.1 mg. Previous research indicated that calves require anywhere from 9 to 14 mg/kg of zinc in their total diet to maintain adequate plasma levels, but that up to 40 mg/kg of dietary zinc may be required according to the NRC (Herrick, 1974, NRC, 2001). Thus, the therapeutic dose is not known for this age of Holstein calves, and this information suggests that there may be a wide range among tolerance, therapeutic, and toxic levels.
An important finding of the current study was that calves treated with either zinc Met or ZO did not experience clinical or laboratory evidence of zinc toxicity. The mean (SEM) liver zinc wet weight concentrations of the placebo, zinc Met, and ZO treated calves at exit were 145.3 (95.6), 179.1 (114.4), and 137.6 (72.3) mg/kg, respectively, which are below reported mean liver zinc wet weight concentrations of 345.7 (16.1) mg/kg in neonatal Holstein calves with clinical signs of zinc toxicosis (Graham et al., 1988). It has been reported in calves up to one year of age, without clinical signs of zinc deficiency or toxicosis, that acceptable liver zinc concentrations range from 49 to 117 mg/kg wet weight (Puschner et al., 2004a). Based on these data, calves in our trial did not have liver zinc concentrations suggestive of zinc deficiency (24–28 mg/kg wet weight) or toxicosis, but it is possible that there is a wide range of liver zinc concentrations during the first three weeks of life, from birth to weaning, and from weaning to breeding age.
When supplementing zinc in the diet of calves, interaction with other metals, especially copper and iron must be considered (Graham et al., 1988). There were 70 calves that had measurable liver copper concentrations at exit from the trial. The mean (SEM) liver copper wet weight concentrations for the placebo, zinc Met, and ZO treated calves were 175.6 (105.6), 143.5 (60.4), and 110.1 (62.0) mg/kg, respectively. It has been reported that newborn calves without clinical signs of copper deficiency or toxicosis can be expected to have liver copper concentrations ranging from 62 to 125 mg/kg wet weight or 190 to 380 mg/kg DW (Puschner et al., 2004b). Calves in the placebo, zinc Met, and ZO treatment groups had mean liver copper DW values higher than this range at exit, indicating that the zinc supplementation did not cause a deficiency in liver copper concentrations.
In the current trial, calves treated with zinc Met had a mean daily gain of 40.24 g compared to a daily loss in the other two treatment groups. The observations recorded from this trial do not prove that calves treated with zinc Met tend to gain rather than lose weight but the direction of point estimates for weight change between groups is worth further investigation. The sample size at the current study permitted a power of 19.9% to detect significant daily weight gain in the zinc MET group compared to the placebo group. As discussed earlier, sample size determination for this study was based on a study in infants that detected a statistically significant difference between children with gastro-intestinal illness and healthy infants and infants with diseases other than diarrhea (Naveh et al., 1982). This approach may be inappropriate for detecting a significant difference in neonatal Holstein calves. Given our study findings, the sample size needed to detect a statistically significant difference in mean daily weight change between the placebo group (−66.88 g/day, SD 296.16) and the zinc Met group (40.24 g/day, SD 374.53) given a power of 90% is 213 calves per group. Such a number can be easily attained on most dairy or calf ranches in California.
Although the data collected did not prove a positive association between ZO and clinical cure, calves supplemented with ZO had a higher hazard of a clinical cure compared to the placebo. In addition, the hazard for clinical cure in calves that tested positive for Cryptosporidium spp. or coronavirus at enrollment when treated with ZO were greater than the respective hazards in calves treated with a placebo. With respect to microbiological cure, calves that tested positive for Cryptosporidium spp. at enrollment and treated with zinc Met had 16 times higher odds of microbiological cure (being pathogen test negative at exit) than calves in the placebo group. Given the magnitude of the association (OR = 16) and it is respective power estimate of 72.3%, further studies are required to investigate the effect of zinc Met on microbiological prevention and cure from cryptosporidiosis in dairy calves. The lethal dose (LD 50) for such zinc formulation for different age groups would need to be estimated through formal toxicity studies to guide the dairy industry in the use of an optimal dose for zinc therapeutic treatment in calf diarrhea to avoid accidental intoxication.
The current study results are limited by the finding of only clinically important differences between treatment groups which were not statistically significant. Furthermore, the study was conducted on a large calf ranch in California which may differ in preweaned calf management on dairies. Important differences may include less variability in preweaned calf diets and more closely followed standard protocols for calf health monitoring and treatments. Despite such limitations, results of the current double blind clinical trial show that there may be a positive impact of zinc on calf health management including decrease in use of antimicrobial drugs.
5. Conclusions
This is the first randomized clinical trial testing the effect of a daily oral zinc supplementation in neonatal Holstein calves with diarrhea. Data collected from the current trial did not provide evidence for a beneficial effect of daily oral 80 mg of zinc as either zinc Met or ZO treatment on days to recovery, fecal consistency, or microbiological and clinical cures in Holstein calves with diarrhea. A total daily dose of 80 mg of available zinc did not result in a zinc toxicity or mineral deficiency. Although statistically not significant, the current trial identified clinically important differences in weight change during the course of diarrhea in calves and other potentially interesting contrasts between effect of organic versus inorganic zinc formulations on clinical and microbial cures in neonatal Holstein calves which differed by pathogen.
Acknowledgements
Funding for this study was made possible by the Center for Food Animal Health, and the Dairy Epidemiology Laboratory (S.S. Aly), Veterinary Medicine Teaching and Research Center, School of Veterinary Medicine, University of California, Davis. The authors thank the calf ranch manager and personnel for their assistance.
Footnotes
This manuscript represents the thesis submitted by Dr. Glover to the University of California at Davis, School of Veterinary Medicine as partial fulfillment of the requirements for the Master of Preventative Veterinary Medicine Degree.
References
- Abdelrahman M.M., Kincaid R.L. Deposition of copper, manganese, zinc, and selenium in bovine fetal tissue at different stages of gestation. J. Dairy Sci. 1993;76:3588–3593. doi: 10.3168/jds.S0022-0302(93)77698-5. [DOI] [PubMed] [Google Scholar]
- Atia A.N., Buchman A.L. Oral rehydration solutions in non-cholera diarrhea: a review. Am. J. Gastroenterol. 2009;104:2596–2604. doi: 10.1038/ajg.2009.329. [DOI] [PubMed] [Google Scholar]
- Barthel F.M., Babiker A., Royston P., Parmar M.K. Evaluation of sample size and power for multi-arm survival trials allowing for non-uniform accrual, non-proportional hazards, loss to follow-up and cross-over. Stat. Med. 2006;25:2521–2542. doi: 10.1002/sim.2517. [DOI] [PubMed] [Google Scholar]
- Bhandari N., Mazumder S., Taneja S., Dube B., Agarwal R., Mahalanabis D., Fontaine O., Black R.E., Bhan M.K. Effectiveness of zinc supplementation plus oral rehydration salts compared with oral rehydration salts alone as a treatment for acute diarrhea in a primary care setting: a cluster randomized trial. Pediatrics. 2008;121:e1279–e1285. doi: 10.1542/peds.2007-1939. [DOI] [PubMed] [Google Scholar]
- Bhutta Z.A., Black B.S., Brown R.E., Gardner K.H., Hidayat J.M., Khatun A., Martorell F., Ninh R., Penny N.X., Rosado M.E., Roy J.L., Ruel S.K., Sazawal M., Shankar S.A. Therapeutic effects of oral zinc in acute and persistent diarrhea in children in developing countries: pooled analysis of randomized controlled trials. Am. J. Clin. Nutr. 2000;72:1516–1522. doi: 10.1093/ajcn/72.6.1516. [DOI] [PubMed] [Google Scholar]
- Bhutta Z.A., Nizami S.Q., Isani Z. Zinc supplementation in malnourished children with persistent diarrhea in Pakistan. Pediatrics. 1999;103:e42. doi: 10.1542/peds.103.4.e42. [DOI] [PubMed] [Google Scholar]
- Cousins R.J. Absorption, transport, and hepatic metabolism of copper and zinc: special reference to metallothionein and ceruloplasmin. Physiol. Rev. 1985;65:238–309. doi: 10.1152/physrev.1985.65.2.238. [DOI] [PubMed] [Google Scholar]
- Faruque A.S., Mahalanabis D., Haque S.S., Fuchs G.J., Habte D. Double-blind, randomized, controlled trial of zinc or vitamin A supplementation in young children with acute diarrhoea. Acta Paediatr. 1999;88:154–160. doi: 10.1080/08035259950170312. [DOI] [PubMed] [Google Scholar]
- Fischer Walker C.L., Fontaine O., Young M.W., Black R.E. Zinc and low osmolarity ORS for diarrhoea: a renewed call to action. Bull. World Health Organ. 2009;87:780–786. doi: 10.2471/BLT.08.058990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabrielson K.L., Remillard R.L., Huso D.L. Zinc toxicity with pancreatic acinar necrosis in piglets receiving total parenteral nutrition. Vet. Pathol. 1996;33:692–696. doi: 10.1177/030098589603300608. [DOI] [PubMed] [Google Scholar]
- Graham T.W., Breher J.E., Farver T.B., Cullor J.S., Kehrli M.E., Oberbauer A.M. Biological markers of neonatal calf performance: the relationship of insulin-like growth factor-I, zinc, and copper to poor neonatal growth. J. Anim. Sci. 2010;88:2585–2593. doi: 10.2527/jas.2009-2610. [DOI] [PubMed] [Google Scholar]
- Graham T.W., Goodger W.J., Christiansen V., Thurmond M.C. Economic losses from an episode of zinc toxicosis on a California veal calf operation using a zinc sulphate-supplemented milk replacer. J. Am. Vet. Med. Assoc. 1987;190:668–671. [PubMed] [Google Scholar]
- Graham T.W., Holmberg C.A., Keen C.L., Thurmond M.C., Clegg M.S. A pathologic and toxicological evaluation of veal calves fed large amounts of zinc. Vet. Pathol. 1988;25:484–491. doi: 10.1177/030098588802500612. [DOI] [PubMed] [Google Scholar]
- Graham T.W., Thurmond M.C., Clegg M.S., Keen C.L., Holmberg C.A., Slanker M.R., Goodger W.J. An epidemiologic study of mortality in veal calves subsequent to an episode of zinc toxicosis on a California veal calf operation using zinc sulphate-supplemented milk replacer. JAVMA. 1987;190:1296–1301. [PubMed] [Google Scholar]
- Graham T.W., Thurmond M.C., Mohr C., Holmberg C.A., Anderson M.L., Keen C.L. Relationships between maternal and fetal liver copper, iron, manganese, and zinc concentrations and fetal development in California Holstein dairy cows. J. Vet. Diagn. Invest. 1984;6:77–87. doi: 10.1177/104063879400600114. [DOI] [PubMed] [Google Scholar]
- Herrick J.B. The role of zinc in nutrition of food-producing animals. Vet. Med. Small Anim. Clinician: VM, SAC. 1974;69:85–89. [PubMed] [Google Scholar]
- Hidiroglou M., Knipfel J.E. Maternal–fetal relationships of copper, manganese, and sulfur in ruminants. A review. J. Dairy Sci. 1981;64:1637–1647. doi: 10.3168/jds.S0022-0302(81)82741-5. [DOI] [PubMed] [Google Scholar]
- Hoque K.M., Sarker R., Guggino S.E., Tse C.-M. A new insight into pathophysiological mechanisms of zinc in diarrhea. Ann. N.Y. Acad. Sci. 2009;1165:279–284. doi: 10.1111/j.1749-6632.2009.04442.x. [DOI] [PubMed] [Google Scholar]
- Jenkins K.J., Hidiroglou M. Tolerance of the preruminant calf for excess manganese or zinc in milk replacer. J. Dairy Sci. 1991;74:1047–1053. doi: 10.3168/jds.S0022-0302(91)78254-4. [DOI] [PubMed] [Google Scholar]
- NAHMS . USDA: APHIS: VS, CEAH; Fort Collins, CO: 2010. Heifer Calf Health and Management Practices on U.S. Dairy Operations, 2007. [Google Scholar]
- Naveh Y., Lightman A., Zinder O. Effect of diarrhea on serum zinc concentrations in infants and children. J. Pediatr. 1982;101:730–732. doi: 10.1016/s0022-3476(82)80303-x. [DOI] [PubMed] [Google Scholar]
- NHMRC . 2005. Nutrient Reference Values For Australia And New Zealand. [Google Scholar]
- NRC . 7th rev. ed. National Academy Press; Washington, DC: 2001. Nutrient Requirements of Dairy Cattle. [Google Scholar]
- Owusu-Asiedu A., Nyachoti C.M., Marquardt R.R. Response of early-weaned pigs to an enterotoxigenic Escherichia coli (K88) challenge when fed diets containing spray-dried porcine plasma or pea protein isolate plus egg yolk antibody, zinc oxide, fumaric acid, or antibiotic. J. Anim. Sci. 2003;81:1790–1798. doi: 10.2527/2003.8171790x. [DOI] [PubMed] [Google Scholar]
- Patel A., Dibley M.J., Mamtani M., Badhoniya N., Kulkarni H. Zinc and copper supplementation in acute diarrhea in children: a double-blind randomized controlled trial. BMC Med. 2009;7:22. doi: 10.1186/1741-7015-7-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Penny M.E., Peerson J.M., Marin R.M., Duran A., Lanata C.F., Lonnerdal B., Black R.E., Brown K.H. Randomized, community-based trial of the effect of zinc supplementation, with and without other micronutrients, on the duration of persistent childhood diarrhea in Lima, Peru. J. Pediatr. 1999;135:208–217. doi: 10.1016/s0022-3476(99)70024-7. [DOI] [PubMed] [Google Scholar]
- Puschner B., Choi Y.K., Tegzes J.H., Thurmond M.C. Influence of age, sex, and production class on liver zinc concentration in calves. J. Vet. Diagn. Invest. 2004;16:278–282. doi: 10.1177/104063870401600404. [DOI] [PubMed] [Google Scholar]
- Puschner B., Thurmond M.C., Choi Y.K. Influence of age and production type on liver copper concentrations in calves. J. Vet. Diagn. Invest. 2004;16:382–387. doi: 10.1177/104063870401600503. [DOI] [PubMed] [Google Scholar]
- Robert B., Ginter A., Antoine H., Collard A., Coppe P. Diagnosis of bovine cryptosporidiosis by an enzyme-linked immunosorbent assay. Vet. Parasitol. 1990;37:1–8. doi: 10.1016/0304-4017(90)90020-C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith B.L., Embling P.P. Sequential changes in the development of the pancreatic lesion of zinc toxicosis in sheep. Vet. Pathol. 1993;30:242–247. doi: 10.1177/030098589303000304. [DOI] [PubMed] [Google Scholar]
- Spencer H., Kramer L., Osis D. Zinc metabolism in man. J. Environ. Pathol. Toxicol. Oncol. 1985;5:265–278. [PubMed] [Google Scholar]
- Swanson K.S., Merchen N.R., Erdman J.W., Jr., Drackley J.K., Orias F., Douglas G.N., Huhn J.C. Technical note: a technique for multiple liver biopsies in neonatal calves. J. Anim. Sci. 2000;78:2459–2463. doi: 10.2527/2000.7892459x. [DOI] [PubMed] [Google Scholar]
- Thorns C.J., Bell M.M., Chasey D., Chesham J., Roeder P.L. Development of monoclonal-antibody Elisa for simultaneous detection of bovine coronavirus, rotavirus serogroup-a, and Escherichia-Coli K99 antigen in feces of calves. Am. J. Vet. Res. 1992;53:36–43. [PubMed] [Google Scholar]
- Wedekind K.J., Hortin A.E., Baker D.H. Methodology for assessing zinc bioavailability: efficacy estimates for zinc-methionine, zinc sulfate, and zinc oxide. J. Anim. Sci. 1992;70:178–187. doi: 10.2527/1992.701178x. [DOI] [PubMed] [Google Scholar]