

Abstract
Canine adenoviruses (CAVs) and canine herpesvirus (CHV) are pathogens of dogs that have been known for several decades. The two distinct types of CAVs, type 1 and type 2, are responsible for infectious canine hepatitis and infectious tracheobronchitis, respectively. In the present article, the currently available literature on CAVs and CHV is reviewed, providing a meaningful update on the epidemiologic, pathogenetic, clinical, diagnostic, and prophylactic aspects of the infections caused by these important pathogens.
Canine adenoviruses (CAVs) and canine herpesvirus (CHV) are pathogens of dogs that have been known for several decades. The two distinct types of CAVs, type 1 (CAV-1) and type 2 (CAV-2), are responsible for infectious canine hepatitis (ICH) and infectious tracheobronchitis (ITB), respectively [1], [2]. Systematic vaccination of dogs has considerably reduced circulation of CAVs in canine populations, although severe outbreaks can be still observed in countries in which CAV vaccines are not used routinely or as a consequence of uncontrolled importation of dogs from endemic areas. CHV can be detected in healthy dogs or in association with different clinical forms, chiefly with mortality in newborns and with respiratory disease or genital lesions in adult dogs [3]. CHV vaccination is not applied routinely, and the infection is common in kenneled dogs.
In the present article, the currently available literature on CAVs and CHV is reviewed, providing a meaningful update on the epidemiologic, pathogenetic, clinical, diagnostic, and prophylactic aspects of the infections caused by these important pathogens.
Canine Adenoviruses
Cause and History
ICH, formerly known as epizootic encephalitis of foxes [1], was first observed in dogs in 1930 [2]. The causative agent CAV-1 was isolated a decade later [4] and was attenuated through passages on canine and swine cell lines to produce vaccines [5], [6]. CAV-2 was first recovered in 1961 from dogs with laryngotracheitis [7]. The isolate, strain Toronto A26/61, was initially considered to be an attenuated strain of CAV-1; only subsequently was it proposed as the prototype of a distinct CAV designated as CAV-2 [8], [9], [10], [11], [12].
CAV-1 and CAV-2 are members of the genus Mastadenovirus, family Adenoviridae, and are closely related antigenically [13], [14] and genetically (75% identity at the nucleotide level) [15], [16]. Despite their antigenic and genetic relatedness, they are easily distinguishable by restriction endonuclease analysis [17], [18] and DNA hybridization [19]. They also exhibit different hemagglutination patterns and cell tropism. CAV-1 recognizes the vascular endothelial cells and hepatic and renal parenchymal cells as targets for viral replication, whereas CAV-2 replicates efficiently in the respiratory tract and, to a limited extent, in the intestinal epithelia [20], [21], [22].
Infection by CAVs has been described worldwide in several mammalian species. Dogs, red foxes, wolves, and coyotes are highly susceptible to CAV infection [3]. The overall prevalence of antibodies to CAVs in European red foxes (Vulpes vulpes) in Australia was 23.2%, with marked geographic, seasonal, and age differences [23], whereas the prevalence of antibody was 97% in island foxes (Urocyon littoralis) in the Channel Islands, California [24]. Antibodies to CAVs were also detected in free-ranging terrestrial carnivores and marine mammals in Alaska and Canada, including black bears (Ursus americanus), fishers (Martes pennanti), polar bears (Ursus maritimus), wolves (Canis lupus), walruses (Odobenus rosmarus), and Steller sea lions (Eumetopias jubatus) [25], [26]. Recently, a fatal CAV-1 infection has been reported in a Eurasian river otter (Lutra lutra) [27].
Canine Infectious Hepatitis: Clinical Signs and Pathologic Findings
Canine ICH is a systemic disease described in Canidae and Ursidae. CAV-1 replication in vascular endothelial cells and hepatocytes produces acute necrohemorrhagic hepatitis, and the disease is more severe in young animals [28], [29]. Transmission occurs through animal-to-animal contact or indirectly through exposure to infectious saliva, feces, urine, or respiratory secretions. CAV-1 is shed in urine up to 6 to 9 months after infection [30]. The incubation period in dogs is 4 to 6 days after ingestion of infectious material and 6 to 9 days after direct contact with infected dogs [31]. The mortality rate is 10% to 30% [32]. Coinfections with canine coronavirus (CCoV) [33], [34], canine distemper virus (CDV) [34], [35], [36], [37], or canine parvovirus [34] can exacerbate the disease, increasing the mortality rates.
Fever (>40°C) is the earliest clinical sign and displays a biphasic course. After the first febrile peak (1–2 days), some dogs recover from the infection. Dogs displaying a second peak of hyperthermia frequently undergo a more severe form of ICH. Commonly observed symptoms are depression, loss of appetite, increased heart rate, hyperventilation, vomiting, and diarrhea. Abdominal pain and distention can occur as a result of accumulation of serosanguineous or hemorrhagic fluid and enlargement of the liver. Frequently, hemorrhagic diathesis is observed with epistaxis, congestion, or hemorrhage of the mucous membranes and skin. Respiratory distress can also be observed as a consequence of laryngitis, tracheitis, and, less frequently, pneumonia. Neurologic signs (hypersalivation, ataxia, and seizures) are rare in dogs and are associated with vascular damage in the central nervous system (CNS) [28], [38]. Corneal opacity (“blue eye”; Fig. 1) and interstitial nephritis may occur 1 to 3 weeks after recovery because of deposition of immune complexes [39], [40], [41]. Hematologic findings include leukopenia (<2000 cells/μL of blood; mainly attributable to a decrease in neutrophil count), increase in the serum transaminases (only in the severe forms of disease) [42], and coagulation disorders associated with disseminated intravascular coagulation (DIC; thrombocytopenia, altered platelet formation, and prolonged prothrombin time) [43]. Proteinuria (albuminuria) can easily reach values greater than 50 mg/dL because of immunomediated glomerulonephritis [29].
Fig. 1.

Dog with ICH. Note bilateral corneal opacity.
At necropsy, the dogs that die during the acute phase of the disease often appear in good nutritional state. External examination can reveal ecchymoses and petechial hemorrhages, whereas the abdominal cavity contains abundant clear or serosanguineous fluid. The liver is enlarged, yellowish brown, congested, and spotted with small rounding areas of necrosis; the gallbladder appears thickened, edematous, and grayish or bluish white opaque in color ( Fig. 2). Edema of the gallbladder wall is a constant finding. Congestion and hemorrhagic lesions are observed in the spleen, lymph nodes ( Fig. 3), thymus, pancreas, and kidneys. Lungs show patchy areas of consolidation because of bronchopneumonia. Hemorrhagic enteritis can also be observed ( Fig. 4) [3], [28].
Fig. 2.
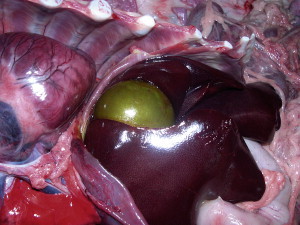
Dog with ICH. There is marked enlargement of the gallbladder.
Fig. 3.

Dog with ICH. The lymph node is enlarged and hemorrhagic.
Fig. 4.

Dog with ICH. There is segmental hemorrhagic enteritis.
Histologic changes in the liver are characterized by centrolobular necrosis, along with neutrophilic and mononuclear cell infiltration and intranuclear inclusions in the Kupffer's cells and hepatocytes. Multifocal areas of congestion, hemorrhage, and leukocyte infiltration can be observed in several organs, mainly in the liver and kidneys, because of vascular damage and inflammation. Interstitial nephritis and iridocyclitis with corneal edema are also present in dogs recovering from ICH [44].
Infectious Tracheobronchitis: Clinical Signs and Pathologic Findings
The route of infection by CAV-2 is oronasal. Respiratory signs are consistent with damage of bronchial epithelial cells. CAV-2 infections rarely result in overt clinical signs, however, despite the presence of extensive lung lesions. Clinical signs typical of ITB are observed when CAV-2 infection is complicated by other viral or bacterial pathogens of dogs, including canine parainfluenza 3 virus [45], CDV [46], [47], [48], Bordetella bronchiseptica [49], mycoplasmas [50], [51], and Streptococcus equi subsp. zooepidemicus [52], [53], [54]. In addition, other viruses with tropism for the respiratory tract have been recently identified and associated with ITB-like forms in dogs, such as influenza A virus [54], [55], a pantropic variant of CCoV [56], and the canine respiratory coronavirus (CRCoV) [57], [58]. CHV and mammalian reoviruses have rarely been reported from dogs with ITB and likely do not play a major role in the disease complex [59], [60].
ITB (kennel cough) is an acute and highly contagious respiratory disease of dogs affecting the larynx, trachea, bronchi, and, occasionally, lower respiratory tract [61]. Kennel cough is typically a complex of diseases caused by viral pathogens (eg, CAVs, CHV, canine parainfluenza virus, reoviruses) in association with bacteria, mainly B bronchiseptica and Mycoplasma spp. Most frequently, a dry hacking cough is observed as a consequence of an uncomplicated, self-limiting, and primarily viral infection of the trachea and bronchi. In complicated forms, which are more common in pups and immunocompromised dogs, secondary bacterial infections and involvement of pulmonary tissue overlap the viral infection. Cough is usually associated with mucoid discharges. The condition may progress to bronchopneumonia and, in the most severe instances, death [61]. Usually, CNS involvement is not seen, although death in pups with neurologic disease associated with CAV-2 infection has been reported [62].
At postmortem examination, red areas of consolidation can be observed in the lungs, especially in the complicated forms. Histologically, necrotizing bronchitis and bronchiolitis obliterans may be observed. Infection of type 2 alveolar cells is associated with interstitial pneumonia and the presence of viral inclusion bodies in their nuclei [63], [64], [65], [66], [67], [68].
Diagnosis, Treatment, and Vaccination
Hematologic findings (eg, leukopenia, prolonged blood clotting, increased activities of alanine aminotransferase [ALT] and aspartate aminotransferase [AST]) may be indicative of CAV-1 infection, although the increase of transaminases is commonly observed only in severely affected or moribund dogs. Postmortem findings and histopathologic changes are highly suggestive of CAV-1 infection. Confirmation of a diagnosis of ICH is obtained by virus isolation on permissive cell lines, such as Madin Darby canine kidney (MDCK) cells. A polymerase chain reaction (PCR) protocol has recently been developed for molecular diagnosis [69]. Ocular swabs, feces, and urine can be collected in vivo for virus isolation and PCR. Postmortem samples can be withdrawn from the kidney, lung, and lymphoid tissues. The liver is rich in arginase, which inhibits viral growth in cell cultures [70], but it represents the most important organ for histopathologic examination [28], [29]. Viral growth in cells is revealed by rounding cells that form clusters and detach from the monolayers [34]. Immunofluorescence (IF) can detect viral antigens in infected cell cultures and in acetone-fixed tissue sections or smears. Viral replication can also be demonstrated by detection of nuclear inclusion bodies in the cells after hematoxylin-eosin staining.
Neither virus isolation nor IF is able to distinguish between the two adenovirus types. Because CAV-2 can also be detected in the internal organs and feces of vaccinated or acutely infected dogs [46] and CAV-1 is also frequently isolated from respiratory secretions, trachea, and lungs, distinction between CAV-1 and CAV-2 necessarily deserves laboratory examination. Restriction fragment length polymorphism analysis on viral genomes using the endonucleases PstI and HpaII generates differential patterns [17], [18]. Detection and differentiation of CAV-1 and CAV-2 by PCR with a single primer pair are also possible [69]. Although CAVs agglutinate erythrocytes of several species, hemagglutination is not used in routine diagnosis [71]. Because most dogs are vaccinated and CAV-2 infection is frequent in dogs, serology has low diagnostic relevance [21], [39].
Treatment of ICH is primarily symptomatic and supportive. Dehydration and DIC require administration of fluids, plasma, or whole-blood transfusions and anticoagulants. Hyperammonemia attributable to hepatic and renal damages can be corrected by oral administration of nonabsorbable antibiotics and lactulose and by oral or parenteral administration of potassium and urinary acidificants (ascorbic acid). Supportive therapy may facilitate the clinical recovery of infected dogs, provided that there is time for hepatocellular regeneration [29].
Uncomplicated forms of CAV-2–associated ITB can be treated with glucocorticoids, antitussives, and bronchodilators as cough suppressants. Aerosol therapy can be effective in dogs displaying excessive accumulation of tracheal and bronchial secretions. Antimicrobial therapy is recommended in the complicated forms and when the lower respiratory tract seems to be involved [29].
Use of vaccines has greatly reduced the burden of ICH in canine populations. Initial attempts were made with CAV-1 inactivated vaccines, which require repeated inoculations [72]. CAV-1–based modified-live virus (MLV) vaccines proved to be highly effective but were associated with interstitial nephritis and corneal opacity [22]. Administration of CAV-1 in conjunction with CDV vaccines was also associated with postvaccinal encephalitis [73]. Because CAV-1 and CAV-2 are able to confer cross-protection, the current vaccines contain MLV CAV-2, which is not able to induce renal or ocular damage. The CAV-2 attenuated strain Toronto A26/61 is contained in most vaccine formulations [22], [74]. In the absence of maternally derived antibodies (MDAs), a single dose administered subcutaneously or intramuscularly is protective against ICH and ITB. Because of the possible interference of MDAs, however, the vaccination schedule requires administration of at least two vaccine doses at a 3- to 4-week interval, starting when pups are 8 to 10 weeks old. Intranasal administration of an MLV CAV-2 vaccine has been proposed to overcome MDA interference, but it may be associated with the onset of mild respiratory disease [29].
Vaccination is usually repeated yearly, although after administration of two doses of CAV-2 vaccine, immunity seems to persist for more than 3 years [75], [76]. Although extensive vaccination has greatly reduced the incidence of CAV infections, re-emergence of ICH has been described in Italy, likely as the result of parallel trading of pups with uncertain sanitary status from Eastern European countries [34]. At the moment, there are few data on the molecular epidemiology of CAVs, but it is commonly accepted that vaccine breaks occur rarely with CAV vaccines, because the viruses are genetically stable. Accordingly, CAV infection in vaccinated dogs has been associated with MDA interference in the early life of the pups rather than with emergence of variants genetically distant from the prototype strains contained in CAV-2 vaccines [34].
Canine Herpesvirus
Cause
CHV was first described in the mid-1960s as the causative agent of a fatal septicemic disease of puppies [77]. CHV is included in the Alphaherpesvirinae subfamily, Herpesviridae family [78]. The virus is sensitive to lipid solvents, is readily inactivated at temperatures greater than 40°C, and is rapidly inactivated by common disinfectants.
CHV seems to be a monotypic virus, as defined by antigenic comparison of various isolates [77], [79]. The genome structure of CHV resembles that of other members of the Alphaherpesvirus subfamily [80], [81], [82], [83]. Southern blot hybridization and sequence analysis of various genes have shown a close genetic relatedness to feline herpesvirus (FHV-1), to phocid herpesvirus 1, and to the equid herpesviruses 1 and 4 [84], [85], [86].
Epidemiology
The host range of CHV is restricted to dogs [87]. Antibodies to CHV have been detected in sera of European red foxes (V vulpes) in Australia [23] and Germany [88], however, and in sera of North American river otters (Lontra canadensis) from New York [89], whereas a CHV-like virus has been isolated from captive coyote pups [90].
The virus seems to be present worldwide in domestic and wild dogs. Serologic surveys have shown a relatively high prevalence of CHV in household and colony-bred dogs. The prevalence of antibodies in dogs was 88% in England, 45.8% in Belgium, and 39.3% in The Netherlands [91], [92], [93]. Serologic studies in Italy have revealed a high prevalence in kenneled dogs (27.9%), whereas the prevalence was lower in pets (3.1%) [94]. In the United States, Fulton and colleagues [95] studied the prevalence of antibodies against CHV in Washington and found only a 6% seroprevalence. Transmission occurs by direct contact with oronasal or genital secretions, because CHV is quickly inactivated in the environment.
Clinical Signs and Pathogenesis
The age of the pups at the time of infection is critical for the outcome of the disease. Infection of susceptible puppies at 1 to 2 weeks of age may be associated with fatal generalized necrotizing and hemorrhagic disease, whereas infection of pups older than 2 weeks of age and adult dogs is often asymptomatic [77]. Infection in older dogs seems to be restricted to the upper respiratory tract [96]. Also, CHV has been identified in corneal swabs of adult dogs with corneal ulcerations [97]. Transplacental transmission of CHV and fetal death may also occur [98], and CHV infection is suspected in dogs with fertility disorders. The high susceptibility of newborn pups to fatal acute CHV-induced disease is likely related to the fact that pups have low and poorly regulated body temperature and CHV growth is optimal at lower than normal body temperature [99].
Neonatal mortality
CHV infection is generally fatal in neonatal pups lacking maternally derived immunity. Death of 1- to 4-week-old pups is most common. Neonatal pups may be infected during passage through the birth canal or by contact with oronasal secretions of other dogs. The duration of illness in newborn pups is 1 to 3 days. Signs include vocalization, anorexia, dyspnea, abdominal pain, incoordination, and soft feces, whereas the rectal temperature is not elevated and may be low. Serous or hemorrhagic nasal discharge and petechial hemorrhage on the mucous membranes may also be observed.
In pups less than 1 week of age at the time of infection, CHV replicates in the nasal mucosa, pharynx, and tonsils before spreading by means of the blood (in macrophages) to the liver, kidneys, lymphatic tissues, lungs, and CNS. The incubation period is approximately 6 to 10 days. Death in affected litters usually occurs over a period of a few days to a week. Litter mortality can reach a peak of 100%. In pups older than 2 to 3 weeks of age at the time of infection, CHV infection is generally asymptomatic, although CNS signs, including blindness and deafness, have been described [100].
Reproductive disorders
CHV can cause occasional in utero infections that result in death of the fetus or pup shortly after birth [77], [98]. Pregnant dogs infected at midgestation or later may abort weak or stillborn pups. Pups may seem normal at parturition but die within a few days of birth. The infected dams develop protective immunity, and CHV-related diseases are not observed in subsequent litters because maternally derived immunity protects the pups during the first week of life when they are most susceptible.
Primary genital infections in susceptible adult animals may be associated with lymphofollicular lesions and vaginal hyperemia ( Fig. 5). Male animals may have similar lesions over the base of the penis and the prepuce.
Fig. 5.

Dog with primary genital herpesvirus infection. There is lymphoid hyperplasia and hyperemia of the vaginal mucosa.
Respiratory disease
CHV has been detected in dogs with ITB [101], but its role remains controversial. Experimental infection has been shown to cause mild clinical symptoms of rhinitis and pharyngitis [96] or tracheobronchitis [102]. Experimental infection by the intravenous route in adult foxes resulted in fever, lethargy, and respiratory signs, although peroral infection did not [103].
A long-term survey in a population of dogs in a shelter has demonstrated CHV in 9.6% of lung and 12.8% of tracheal samples. CHV infections occurred later than other viral infections. CHV was detected more frequently at weeks 3 and 4 after a dog's introduction in the kennel, whereas CRCoV and canine parainfluenza were detected more frequently within the first and second weeks, respectively. Interestingly, CHV infection was apparently related to more severe respiratory signs [53]. In a 1-year study in training centers for working dogs, however, seroconversion to CHV seemed to be more frequent in dogs infected with CRCoV [104], suggesting virus reactivation after disease-induced stress.
Latency
After symptomatic and asymptomatic infections, dogs remain latently infected and virus may be excreted at unpredictable intervals over periods of several months or years. Reactivation of latent virus may be provoked by environmental or social stress or, experimentally, by immunosuppressive drugs (corticosteroids) or antilymphocyte serum. Latent virus persists in the trigeminal ganglia and other sites, such as lumbosacral ganglia, tonsils, and parotid salivary glands [3], [105], [106], [107]. Latently infected dogs represent a source of infection for susceptible animals, and this is of particular concern in breeding dogs that can ensure CHV transmission through genital secretions.
Pathologic Findings
Multifocal areas of necrosis and hemorrhage may be observed in most organs, including the lungs, liver, brain, and intestine, with the kidneys being the most classic organ affected. Circumscribed areas of hemorrhage and necrosis on a pale gray cortex give the organs a spotted appearance ( Fig. 6). Lymph nodes and spleens appear enlarged. Meningoencephalitis also is common. Necrosis in the placenta is observed in infected pregnant animals. Fetal lesions are similar to those seen in affected puppies.
Fig. 6.
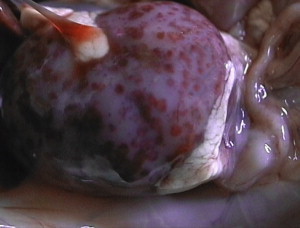
Puppy with neonatal herpesvirus infection. There is multifocal hemorrhage and necrosis of the kidneys.
Diagnosis, Treatment, and Vaccination
Diagnosis of CHV infection may be achieved by isolation of the virus on permissive cell lines. The virus can be adapted for growth on canine primary or secondary kidney or testicular cells and in canine cell lines. Growth is optimal at 34°C to 35°C, with diminished virus yields at temperatures higher than 36°C. In cell cultures, virus growth is revealed by formation of typical clusters of rounded cells that tend to detach, and for certain isolates, by formation of syncytia with type A intranuclear inclusions. PCR assays are available, significantly increasing diagnostic reliability and sensitivity [107]. Serologic screenings to evaluate the neutralizing antibodies may be useful to investigate the presence of CHV in kennels.
Because CHV growth is optimal at temperatures lower than 36°C [99], attempts were made to influence the evolution of CHV-induced disease in experimentally infected pups. Experimentally infected newborn pups reared at elevated temperatures that raised their body temperature to 38.5°C to 39.5°C survived CHV infection but presented with permanent neurologic damage [108]. Likewise, residual neurologic damage may be observed in infected dogs treated with antiviral drugs, such as vidarabine. Accordingly, neither artificial temperature nor vidarabine may be applied for the therapy of CHV.
An inactivated subunit vaccine is available commercially in Europe. The vaccine should be administered to bitches during heat or the initial stages of pregnancy and again at the sixth to seventh week of gestation. A temperature-resistant mutant of CHV attenuated through serial cell passages has been proposed as an MLV vaccine [109], but its safety and efficacy have not been evaluated and such a vaccine is not available commercially.
Summary
CAV infections have been satisfactorily controlled in the past decades as a consequence of the vaccination programs adopted in all developed countries. Nevertheless, there are some concerns about the possible introduction of infected dogs from areas of uncertain epidemiologic conditions, in which both CAV types are widespread as a result of the lack of systematic canine immunization [34]. CAV vaccines have been proved to be safe and effective for prevention of ICH and ITB, conferring protection against more recent CAV strains, albeit prepared with old CAV-2 strains [28], [110].
Conversely, CHV is still circulating in canine populations worldwide, mainly in shelters and breeding kennels. Active immunization is recommended in pregnant bitches to prevent fatal infections in newborn pups [111]. When the MDAs decrease, however, pups born to vaccinated bitches become susceptible and, along with unvaccinated dogs, maintain CHV infection. It is unclear whether vaccination prevents CHV infection and virus shedding through secretions. In addition, control of the infection is hindered by the fact that CHV is often associated with asymptomatic infections, and the real prevalence of CHV infection is likely underestimated [87].
The intensification of surveillance activity using new diagnostic techniques and molecular analysis tools may help to investigate the epidemiology of CAV and CHV infections more thoroughly and to plan adequate measures of control.
References
- 1.Green R.G., Ziegler N.R., Breen B.B. Epizootic fox encephalitis. I. General description. Am J Hyg. 1930;12:109–129. [Google Scholar]
- 2.Cowdry E.V., Scott G.H. A comparison of certain intranuclear inclusions found in the livers of dogs without history of infection with intranuclear inclusions characteristic of the action of filtrable viruses. Arch Pathol. 1930;9:1184–1196. [Google Scholar]
- 3.Carmichael L.E., Greene C.E. Canine herpesvirus infection. In: Greene C.E., editor. Infectious diseases of the dog and cat. WB Saunders Co; Philadelphia: 1998. pp. 28–32. [Google Scholar]
- 4.Cabasso V.J., Stebbins M.R., Nortor T.W. Propagation of infectious canine hepatitis virus in tissue culture. Proc Soc Exp Biol Med. 1954;85:239–245. doi: 10.3181/00379727-85-20843. [DOI] [PubMed] [Google Scholar]
- 5.Fieldsteel A.H., Emery J.B. Cultivation and modification of infectious canine hepatitis virus in roller tube cultures of dog kidney. Proc Soc Exp Biol Med. 1954;86:819–823. doi: 10.3181/00379727-86-21242. [DOI] [PubMed] [Google Scholar]
- 6.Cabasso V.J., Stebbins M.R., Avampato J.M. A bivalent live virus vaccine against canine distemper (CD) and infectious canine hepatitis (ICH) Proc Soc Exp Biol Med. 1958;99:46–51. doi: 10.3181/00379727-99-24242. [DOI] [PubMed] [Google Scholar]
- 7.Ditchfield J., MacPherson L.W., Zbitnew A. Association of a canine adenovirus (Toronto A26/61) with an outbreak of laryngotracheitis (kennel cough). A preliminary report. Can Vet J. 1962;3:238–247. [PMC free article] [PubMed] [Google Scholar]
- 8.Yamamoto R., Marusyk R.G. Morphological studies of a canine adenovirus. J Gen Virol. 1968;2:191–194. doi: 10.1099/0022-1317-2-1-191. [DOI] [PubMed] [Google Scholar]
- 9.Fairchild G.A., Cohen D. Serologic study of a canine adenovirus (Toronto A26/61) infection in dog. Am J Vet Res. 1969;30:923–928. [PubMed] [Google Scholar]
- 10.Swango L.J., Eddy G.A., Binn L.N. Serologic comparisons of infectious canine hepatitis and Toronto A26/61 canine adenoviruses. Am J Vet Res. 1969;30:1381–1387. [PubMed] [Google Scholar]
- 11.Marusyk R.G., Norrby E., Lundqvist U. Biophysical comparison of two canine adenoviruses. J Virol. 1970;5:507–512. doi: 10.1128/jvi.5.4.507-512.1970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Marusyk R.G. Comparison of the immunological properties of two canine adenoviruses. Can J Microbiol. 1972;18:817–823. doi: 10.1139/m72-127. [DOI] [PubMed] [Google Scholar]
- 13.Matthews R.E.F. Classification and nomenclature of viruses. Intervirology. 1982;17:4–199. [Google Scholar]
- 14.Wigand R., Bartha A., Dreizin R.S. Adenoviridae: second report. Intervirology. 1982;18:169–176. doi: 10.1159/000149322. [DOI] [PubMed] [Google Scholar]
- 15.Morrison M.D., Onions D.E., Nicolson L. Complete DNA sequence of canine adenovirus type 1. J Gen Virol. 1997;78:873–878. doi: 10.1099/0022-1317-78-4-873. [DOI] [PubMed] [Google Scholar]
- 16.Davison A.J., Benko M., Harrach B. Genetic content and evolution of adenoviruses. J Gen Virol. 2003;84:2895–2908. doi: 10.1099/vir.0.19497-0. [DOI] [PubMed] [Google Scholar]
- 17.Assaf R., Marsolais G., Yelle J. Unambiguous typing of canine adenovirus isolates by deoxyribonucleic acid restriction-endonuclease analysis. Can J Comp Med. 1983;47:460–463. [PMC free article] [PubMed] [Google Scholar]
- 18.Hamelin C., Marsolais G., Assaf R. Interspecific differences between DNA restriction profiles of canine adenovirus. Experientia. 1984;40:482. doi: 10.1007/BF01952396. [DOI] [PubMed] [Google Scholar]
- 19.Marusyk R.G., Hammarskjold M.L. The genetic relationship of two canine adenoviruses as determined by nucleic acid hybridization. Microbios. 1972;5:259–264. [PubMed] [Google Scholar]
- 20.Swango L.J., Wooding W.L., Binn L.N. A comparison of the pathogenesis and antigenicity of infectious canine hepatitis virus and the A26/61 virus strain (Toronto) J Am Vet Med Assoc. 1970;156:1687–1696. [PubMed] [Google Scholar]
- 21.Marusyk R.G., Yamamoto T. Characterization of canine adenovirus hemagglutinin. Can J Microbiol. 1971;17:151–155. doi: 10.1139/m71-026. [DOI] [PubMed] [Google Scholar]
- 22.Appel M., Bistner S.I., Menegus M. Pathogenicity of low-virulence strains of two canine adenoviruses. Am J Vet Res. 1973;34:543–550. [PubMed] [Google Scholar]
- 23.Robinson A.J., Crerar S.K., Waight Sharma N. Prevalence of serum antibodies to canine adenovirus and canine herpesvirus in the European red fox (Vulpes vulpes) in Australia. Aust Vet J. 2005;83:356–361. doi: 10.1111/j.1751-0813.2005.tb15634.x. [DOI] [PubMed] [Google Scholar]
- 24.Garcelon D.K., Wayne R.K., Gonzales B.J. A serologic survey of the island fox (Urocyon littoralis) on the Channel Islands, California. J Wildl Dis. 1992;28:223–229. doi: 10.7589/0090-3558-28.2.223. [DOI] [PubMed] [Google Scholar]
- 25.Burek K.A., Gulland F.M., Sheffield G. Infectious disease and the decline of Steller sea lions (Eumetopias jubatus) in Alaska, USA: insights from serologic data. J Wildl Dis. 2005;41:512–524. doi: 10.7589/0090-3558-41.3.512. [DOI] [PubMed] [Google Scholar]
- 26.Philippa J.D.W., Leighton P.J., Nielsen O. Antibodies to selected pathogens in free-ranging terrestrial carnivores and marine mammals in Canada. Vet Rec. 2004;155:135–140. doi: 10.1136/vr.155.5.135. [DOI] [PubMed] [Google Scholar]
- 27.Park N.Y., Lee M.C., Kurkure N.V. Canine adenovirus type 1 infection of a Eurasian river otter (Lutra lutra) Vet Pathol. 2007;44:536–539. doi: 10.1354/vp.44-4-536. [DOI] [PubMed] [Google Scholar]
- 28.Appel M. Canine adenovirus type 1 (infectious canine hepatitis virus) In: Appel M., editor. Virus infections of carnivores. Elsevier Science Publishers; Amsterdam: 1987. pp. 29–43. [Google Scholar]
- 29.Greene C.E. Infectious canine hepatitis. In: Greene C.E., editor. Infectious diseases of the dog and cat. WB Saunders; Philadelphia: 1990. pp. 242–251. [Google Scholar]
- 30.Poppensiek G.C., Baker J.A. Persistence of virus in urine as factor in spread of infectious hepatitis in dogs. Proc Soc Exp Biol Med. 1951;77:279–281. doi: 10.3181/00379727-77-18749. [DOI] [PubMed] [Google Scholar]
- 31.Baker J.A., Richards M.G., Brown A.L. Proc Am Vet Med Assoc 87th Ann. Mtg. 1950. Infectious hepatitis in dogs; pp. 242–248. [Google Scholar]
- 32.Cabasso V.J. Infectious canine hepatitis virus. Ann N Y Acad Sci. 1962;101:498–514. doi: 10.1111/j.1749-6632.1962.tb18891.x. [DOI] [PubMed] [Google Scholar]
- 33.Pratelli A., Martella V., Elia G. Severe enteric disease in an animal shelter associated with dual infection by canine adenovirus type 1 and canine coronavirus. J Vet Med B Infect Dis Vet Public Health. 2001;48:385–392. doi: 10.1046/j.1439-0450.2001.00466.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Decaro N., Campolo M., Elia G. Infectious canine hepatitis: an “old” disease reemerging in Italy. Res Vet Sci. 2007;83:269–273. doi: 10.1016/j.rvsc.2006.11.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Stookey J.L., VanZwieten M.J., Witney G.D. Dual viral infections in two dogs. J Am Vet Med Assoc. 1972;61:1117–1121. [PubMed] [Google Scholar]
- 36.Ducatelle R., Maenhout D., Coussement W. Dual adenovirus and distemper virus pneumonia in a dog. Vet Q. 1982;4:84–88. doi: 10.1080/01652176.1982.9693844. [DOI] [PubMed] [Google Scholar]
- 37.Kobayashi Y., Ochiai K., Itakura C. Dual infection with canine distemper virus and infectious canine hepatitis virus (canine adenovirus type 1) in a dog. J Vet Med Sci. 1993;55:699–701. doi: 10.1292/jvms.55.699. [DOI] [PubMed] [Google Scholar]
- 38.Caudell D., Confer A.W., Fulton R.W. Diagnosis of infectious canine hepatitis virus (CAV-1) infection in puppies with encephalopathy. J Vet Diagn Invest. 2005;17:58–61. doi: 10.1177/104063870501700111. [DOI] [PubMed] [Google Scholar]
- 39.Carmichael L.E. The pathogenesis of ocular lesions of infectious canine hepatitis. I. Pathology and virological observation. Pathol Vet. 1964;1:73–95. doi: 10.1177/030098586500200403. [DOI] [PubMed] [Google Scholar]
- 40.Carmichael L.E. The pathogenesis of ocular lesions of infectious canine hepatitis. II. Experimental ocular hypersensitivity produced by the virus. Pathol Vet. 1965;2:344–359. doi: 10.1177/030098586500200403. [DOI] [PubMed] [Google Scholar]
- 41.Wright N.G. Canine adenovirus: its role in renal and ocular disease: a review. J Small Anim Pract. 1976;17:25–33. doi: 10.1111/j.1748-5827.1976.tb06543.x. [DOI] [PubMed] [Google Scholar]
- 42.Beckett S.D., Burns M.J., Clark C.H. A study of the blood glucose, serum transaminase, and electrophoretic patterns of dogs with infectious canine hepatitis. Am J Vet Res. 1964;25:1186–1190. [PubMed] [Google Scholar]
- 43.Wigton D.H., Kociba G.J., Hoover E.A. Infectious canine hepatitis: animal model for viral-induced disseminated intravascular coagulation. Blood. 1976;47:287–296. [PubMed] [Google Scholar]
- 44.Carmichael L.E., Medic B.L.S., Bistner S.I. Viral-antibody complexes in canine adenovirus type 1 (CAV 1) ocular lesion: leukocyte chemotaxis and enzyme release. Cornell Vet. 1975;65:331–351. [PubMed] [Google Scholar]
- 45.Binn L.N., Eddy G.A., Lazar E.C. Viruses recovered from laboratory dogs with respiratory disease. Proc Soc Exp Biol Med. 1967;126:140–145. doi: 10.3181/00379727-126-32386. [DOI] [PubMed] [Google Scholar]
- 46.Decaro N., Camero M., Greco G. Canine distemper and related diseases: report of a severe outbreak in a kennel. New Microbiol. 2004;27:177–181. [PubMed] [Google Scholar]
- 47.Chvala S., Benetka V., Mostl K. Simultaneous canine distemper virus, canine adenovirus type 2, and Mycoplasma cynos infection in a dog with pneumonia. Vet Pathol. 2007;44:508–512. doi: 10.1354/vp.44-4-508. [DOI] [PubMed] [Google Scholar]
- 48.Rodriguez-Tovar L.E., Ramirez-Romero R., Valdez-Nava Y. Combined distemper-adenoviral pneumonia in a dog. Can Vet J. 2007;48:632–634. [PMC free article] [PubMed] [Google Scholar]
- 49.Bemis D.A., Carmichael L.E., Appel M. Naturally occurring respiratory disease in a kennel caused by Bordetella bronchiseptica. Cornell Vet. 1977;67:282–293. [PubMed] [Google Scholar]
- 50.Randolph J.F., Moise N.S., Scarlett J.M. Prevalence of mycoplasmal and ureaplasmal recovery from tracheobronchial lavages and of mycoplasmal recovery from pharyngeal swab specimens in cats with or without pulmonary disease. Am J Vet Res. 1993;54:897–900. [PubMed] [Google Scholar]
- 51.Chalker V.J., Owen W.M., Paterson C. Mycoplasmas associated with canine infectious respiratory disease. Microbiology. 2004;150:3491–3497. doi: 10.1099/mic.0.26848-0. [DOI] [PubMed] [Google Scholar]
- 52.Chalker V.J., Brooks H.W., Brownlie J. The association of Streptococcus equi subsp. zooepidemicus with canine infectious respiratory disease. Vet Microbiol. 2003;95:149–156. doi: 10.1016/S0378-1135(03)00155-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Erles K., Dubovi E.J., Brooks H.W. Longitudinal study of viruses associated with canine infectious respiratory disease. J Clin Microbiol. 2004;42:4524–4529. doi: 10.1128/JCM.42.10.4524-4529.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Yoon K.-J., Cooper V.L., Schwartz K.J. Influenza virus infection in racing greyhounds. Emerg Infect Dis. 2005;11:1974–1975. doi: 10.3201/eid1112.050810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Crawford P.C., Dubovi E.J., Castleman W.L. Transmission of equine influenza virus to dogs. Science. 2005;310:482–485. doi: 10.1126/science.1117950. [DOI] [PubMed] [Google Scholar]
- 56.Buonavoglia C., Decaro N., Martella V. Canine coronavirus highly pathogenic for dogs. Emerg Infect Dis. 2006;12:492–494. doi: 10.3201/eid1203.050839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Erles K., Toomey C., Brooks H.W. Detection of a group 2 coronavirus in dogs with canine infectious respiratory disease. Virology. 2003;310:216–223. doi: 10.1016/S0042-6822(03)00160-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Decaro N., Desario C., Elia G. Serological and molecular evidence that canine respiratory coronavirus is circulating in Italy. Vet Microbiol. 2007;121:225–230. doi: 10.1016/j.vetmic.2006.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Karpas A., King N.W., Garcia F.G. Canine tracheobronchitis; isolation and characterization of the agent with experimental reproduction of the disease. Proc Soc Exp Biol Med. 1968;127:45–52. doi: 10.3181/00379727-127-32618. [DOI] [PubMed] [Google Scholar]
- 60.Lou T.Y., Wenner H.A. Natural and experimental infection of dogs with reovirus type 1: pathogenicity of the strain for other animals. Am J Hyg. 1963;77:293–304. [Google Scholar]
- 61.Appel M., Binn L.N. Canine infectious tracheobronchitis. Short review: kennel cough. In: Appel M., editor. Virus infections of carnivores. Elsevier Science Publisher; Amsterdam: 1987. pp. 201–211. [Google Scholar]
- 62.Benetka V., Weissenbock H., Kudielka I. Canine adenovirus type 2 infection in four puppies with neurological signs. Vet Rec. 2006;158:91–94. doi: 10.1136/vr.158.3.91. [DOI] [PubMed] [Google Scholar]
- 63.Appel M, Picherill RH, Menegus M, et-al. Current status of canine respiratory disease. In: Proc. 20th Gaines Vet Symp. Manhattan: 1970. p. 15–23.
- 64.Curtis R., Jemmet J.E., Furminger I.G.S. The pathogenicity of an attenuated strain of canine adenovirus type 2 (CAV-2) Vet Rec. 1978;103:380–381. doi: 10.1136/vr.103.17.380. [DOI] [PubMed] [Google Scholar]
- 65.Appel M. Canine infectious tracheobronchitis (kennel cough): a status report. Compendium on Continuing Education. 1981;3:70–79. [Google Scholar]
- 66.Appel M. Canine adenovirus type 2 (infectious laryngotracheitis virus) In: Appel M., editor. Virus infections of carnivores. Elsevier Science Publisher; Amsterdam: 1987. pp. 45–51. [Google Scholar]
- 67.Koptopoulos G., Cornwell H.J.C. Canine adenoviruses: a review. Vet Bull. 1981;51:135–142. [Google Scholar]
- 68.Castleman W.L. Bronchiolitis obliterans and pneumonia induced in young dogs by experimental adenovirus infection. Am J Pathol. 1985;119:495–504. [PMC free article] [PubMed] [Google Scholar]
- 69.Hu R.L., Huang G., Qiu W. Detection and differentiation of CAV-1 and CAV-2 by polymerase chain reaction. Vet Res Commun. 2001;25:77–84. doi: 10.1023/a:1006417203856. [DOI] [PubMed] [Google Scholar]
- 70.Carmichael L.E. Identification of a canine adenovirus (infectious canine hepatitis virus) inhibitor in dog liver extracts as arginase. Infect Immun. 1972;6:348–354. doi: 10.1128/iai.6.3.348-354.1972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Fastier L.B. Studies on the hemagglutinin of infectious canine hepatitis virus. J Immunol. 1957;78:413–418. [PubMed] [Google Scholar]
- 72.Miller A.S.H., Curtis R., Furminger I.G.S. Persistence of immunity to infectious canine hepatitis using a killed vaccine. Vet Rec. 1980;106:343–344. doi: 10.1136/vr.106.15.343. [DOI] [PubMed] [Google Scholar]
- 73.Cornwell H.J., Thompson H., McCandlish I.A. Encephalitis in dogs associated with a batch of canine distemper (Rockborn) vaccine. Vet Rec. 1998;122:54–59. doi: 10.1136/vr.122.3.54. [DOI] [PubMed] [Google Scholar]
- 74.Appel M., Carmichael L.E., Robson D.S. Canine adenovirus type 2-induced immunity to two canine adenoviruses in pups with maternal antibody. Am J Vet Res. 1975;36:1199–1202. [PubMed] [Google Scholar]
- 75.Gill M., Srinivas J., Morozov I. Three-year duration of immunity for canine distemper, adenovirus, and parvovirus after vaccination with a multivalent canine vaccine. International Journal of Applied Research in Veterinary Medicine. 2004;2:227–234. [Google Scholar]
- 76.Gore T.C., Coyne M.J., Duncan K.L. Three-year duration of immunity in dogs following vaccination against canine adenovirus type-1, canine parvovirus, and canine distemper virus. Vet Ther. 2005;6:5–14. [PubMed] [Google Scholar]
- 77.Carmichael L.E., Squire R.A., Krook L. Clinical and pathologic features of a fatal viral disease of newborn pups. Am J Vet Res. 1965;26:803–814. [PubMed] [Google Scholar]
- 78.van Regenmortel M.H.V., Fauquet C.M., Bishop D.H.L., editors. Academic Press; New York: 2000. Virus taxonomy. Seventh report of the International Committee on Taxonomy of Viruses. [Google Scholar]
- 79.Poste G., Lecatsas G., Apostolov K. Electron microscope study of the morphogenesis of a new canine herpesvirus in dog kidney cells. Arch Gesamte Virusforsch. 1972;39:317–329. doi: 10.1007/BF01241010. [DOI] [PubMed] [Google Scholar]
- 80.Rémond M., Sheldrick P., Lebreton F. Gene organization in the UL region and inverted repeats of the canine herpesvirus genome. J Gen Virol. 1996;77:37–48. doi: 10.1099/0022-1317-77-1-37. [DOI] [PubMed] [Google Scholar]
- 81.Haanes E.J., Tomlinson C.C. Genomic organization of the canine herpesvirus US region. Virus Res. 1998;53:151–162. doi: 10.1016/s0168-1702(97)00152-4. [DOI] [PubMed] [Google Scholar]
- 82.Limbach K.J., Limbach M.P., Conte D. Nucleotide sequence of the genes encoding the canine herpesvirus gB, gC and gD homologues. J Gen Virol. 1994;75:2029–2039. doi: 10.1099/0022-1317-75-8-2029. [DOI] [PubMed] [Google Scholar]
- 83.Reubel G.H., Pekin J., Webb-Wagg K. Nucleotide sequence of glycoprotein genes B, C, D, G, H and I, the thymidine kinase and protein kinase genes and gene homologue UL24 of an Australian isolate of canine herpesvirus. Virus Genes. 2002;25:195–200. doi: 10.1023/a:1020118003743. [DOI] [PubMed] [Google Scholar]
- 84.Rota P.A., Maes R.K. Homology between feline herpesvirus-1 and canine herpesvirus. Arch Virol. 1990;115:139–145. doi: 10.1007/BF01310631. [DOI] [PubMed] [Google Scholar]
- 85.Willoughby K., Bennett M., McCracken C.M. Molecular phylogenetic analysis of felid herpesvirus 1. Vet Microbiol. 1999;69:93–97. doi: 10.1016/s0378-1135(99)00094-2. [DOI] [PubMed] [Google Scholar]
- 86.Martina B.E., Harder T.C., Osterhaus A.D. Genetic characterization of the unique short segment of phocid herpesvirus type 1 reveals close relationships among alpha herpesviruses of hosts of the order Carnivora. J Gen Virol. 2003;84:1427–1430. doi: 10.1099/vir.0.19005-0. [DOI] [PubMed] [Google Scholar]
- 87.Appel M.J. Canine herpesvirus. In: Appel M.J., editor. Virus infections of carnivores. Elsevier; Amsterdam: 1987. pp. 5–15. [Google Scholar]
- 88.Truyen U., Muller T., Heidrich R. Survey on viral pathogens in wild red foxes (Vulpes vulpes) in Germany with emphasis on parvoviruses and analysis of a DNA sequence from a red fox parvovirus. Epidemiol Infect. 1998;121:433–440. doi: 10.1017/s0950268898001319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Kimber K.R., Kollias G.V., Dubovi E.J. Serologic survey of selected viral agents in recently captured wild North American river otters (Lontra canadensis) J Zoo Wildl Med. 2000;31:168–175. doi: 10.1638/1042-7260(2000)031[0168:SSOSVA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 90.Evermann J.F., LeaMaster B.R., McElwain T.F. Natural infection of captive coyote pups with a herpesvirus antigenically related to canine herpesvirus. J Am Vet Med Assoc. 1984;185:1288–1290. [PubMed] [Google Scholar]
- 91.Reading M.J., Field H.J. Detection of high levels of canine herpes virus-1 neutralising antibody in kennel dogs using a novel serum neutralisation test. Res Vet Sci. 1999;66:273–275. doi: 10.1053/rvsc.1998.0222. [DOI] [PubMed] [Google Scholar]
- 92.Ronsse V., Verstegen J., Onclin K. Seroprevalence of canine herpesvirus-1 in the Belgian dog population in 2000. Reprod Domest Anim. 2002;37:299–304. doi: 10.1046/j.1439-0531.2002.00363.x. [DOI] [PubMed] [Google Scholar]
- 93.Rijsewijk F.A., Luiten E.J., Daus F.J. Prevalence of antibodies against canine herpesvirus 1 in dogs in The Netherlands in 1997–1998. Vet Microbiol. 1999;65:1–7. doi: 10.1016/s0378-1135(98)00285-5. [DOI] [PubMed] [Google Scholar]
- 94.Sagazio P., Cirone F., Pratelli A. Infezione da herpesvirus del cane: diffusione sierologica in Puglia. Obiettivi e Documenti Veterinari. 1998;5:63–67. [Google Scholar]
- 95.Fulton R.W., Ott W.L., Duenwald J.C. Serum antibodies against canine respiratory viruses: prevalence among dogs of eastern Washington. Am J Vet Res. 1974;35:853–855. [Google Scholar]
- 96.Appel M.J., Menegus M., Parsonson I.M. Pathogenesis of canine herpesvirus in specific-pathogen-free dogs: 5- to 12-week-old pups. Am J Vet Res. 1969;30:2067–2073. [PubMed] [Google Scholar]
- 97.Ledbetter E.C., Riis R.C., Kern T.J. Corneal ulceration associated with naturally occurring canine herpesvirus-1 infection in two adult dogs. J Am Vet Med Assoc. 2006;229:376–384. doi: 10.2460/javma.229.3.376. [DOI] [PubMed] [Google Scholar]
- 98.Hashimoto A., Hirai K., Yamaguchi T. Experimental transplacental infection of pregnant dogs with canine herpesvirus. Am J Vet Res. 1982;43:844–850. [PubMed] [Google Scholar]
- 99.Lust G., Carmichael L.E. Suppressed synthesis of viral DNA, protein and mature virions during replication of canine herpesvirus at elevated temperature. J Infect Dis. 1971;124:572–580. doi: 10.1093/infdis/124.6.572. [DOI] [PubMed] [Google Scholar]
- 100.Carmichael L.E. Herpesvirus canis: aspects of pathogenesis and immune response. J Am Vet Med Assoc. 1970;156:1714–1721. [PubMed] [Google Scholar]
- 101.Binn L.N., Alford J.P., Marchwicki R.H. Studies of respiratory disease in random-source laboratory dogs: viral infections in unconditioned dogs. Lab Anim Sci. 1979;29:48–52. [PubMed] [Google Scholar]
- 102.Karpas A., Garcia F.G., Calvo F. Experimental production of canine tracheobronchitis (kennel cough) with canine herpesvirus isolated from naturally infected dogs. Am J Vet Res. 1968;29:1251–1257. [PubMed] [Google Scholar]
- 103.Reubel G.H., Pekin J., Venables D. Experimental infection of European red foxes (Vulpes vulpes) with canine herpesvirus. Vet Microbiol. 2001;83:217–233. doi: 10.1016/s0378-1135(01)00419-9. [DOI] [PubMed] [Google Scholar]
- 104.Erles K., Brownlie J. Investigation into the causes of canine infectious respiratory disease: antibody responses to canine respiratory coronavirus and canine herpesvirus in two kennelled dog populations. Arch Virol. 2005;150:1493–1504. doi: 10.1007/s00705-005-0533-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Miyoshi M., Ishii Y., Takiguchi M. Detection of canine herpesvirus DNA in the ganglionic neurons and the lymph node lymphocytes of latently infected dogs. J Vet Med Sci. 1999;61:375–379. doi: 10.1292/jvms.61.375. [DOI] [PubMed] [Google Scholar]
- 106.Okuda Y., Ishida K., Hashimoto A. Virus reactivation in bitches with a medical history of herpesvirus infection. Am J Vet Res. 1993;54:551–554. [PubMed] [Google Scholar]
- 107.Burr P.D., Campbell M.E., Nicolson L. Detection of canine herpesvirus 1 in a wide range of tissues using the polymerase chain reaction. Vet Microbiol. 1996;53:227–237. doi: 10.1016/s0378-1135(96)01227-8. [DOI] [PubMed] [Google Scholar]
- 108.Carmichael L.E., Barnes F.D., Percy D.H. Temperature as a factor of resistance of young puppies to canine herpesvirus. J Infect Dis. 1969;120:669–678. doi: 10.1093/infdis/120.6.669. [DOI] [PubMed] [Google Scholar]
- 109.Carmichael L.E., Medic B.L.S. Small-plaque variant of canine of canine herpesvirus with reduced pathogenicity for newborn pups. Infect Immun. 1978;20:108–114. doi: 10.1128/iai.20.1.108-114.1978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Day M.J., Horzinek M.C., Schultz R.D. Guidelines for the vaccination of dogs and cats. Compiled by the vaccination guidelines group (VGG) of the world small animal veterinary association (WSAVA) J Small Anim Pract. 2007;48:528–541. doi: 10.1111/j.1748-5827.2007.00462.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Poulet H., Guigal P.M., Soulier M. Protection of puppies against canine herpesvirus by vaccination of the dams. Vet Rec. 2001;148:691–695. doi: 10.1136/vr.148.22.691. [DOI] [PubMed] [Google Scholar]