

Abstract
Severe acute respiratory syndrome (SARS), the first global epidemic in the 21st century, affected over 8500 people in approximately 30 countries 1, 2, 3, 4, 5, 6, 7. With a crude mortality of 9%, its cause was quickly identified as a novel coronavirus that jumped species from animals to man. The SARS coronavirus epidemic, which began in the Fall of 2002, was related to the exotic food industry in southern China, initially involving disproportionate numbers of animal handlers, chefs, and caterers. Subsequently, person-to-person transmission spawned the outbreak. What distinguished this illness clinically was the fact that approximately half of the victims were health care workers (8), infected while caring for recognized or unrecognized patients with SARS. There are many curiosities and uncertainties surrounding the epidemic of SARS with lessons that may be useful to the community of infectious diseases physicians, especially when looking ahead to the next epidemic. Herein we relate our perspectives on useful lessons derived from a review of the SARS epidemic.
Key Words: Severe acute respiratory syndrome, Infection control, Emergent infectious diseases, Health care workers
Recognition of a New Epidemic
A repeated theme in reviewing emergent outbreaks is that it is essential that astute clinicians with sufficient experience will recognize and distinguish something new. It is difficult to comment about clinicians in the early course of SARS in China, because nothing was reported. However, when the epidemic appeared in Vietnam, the team of physicians at the French Hospital of Hanoi led by Dr. Carlo Urbani immediately alerted the world (9). His colleagues in the Doctors without Borders group recognized a defining feature of the cluster of community-acquired pneumonias: 30 of the initial 60 cases involved health care workers. Sadly, within weeks Dr. Urbani and four of his colleagues themselves would die as victims of SARS. It later became apparent that whereas the 9% mortality was somewhat higher than the expected mortality for the usual causes of community-acquired pneumonias (approximately 2–4%), the 50% mortality for patients over age 60 also distinguished this pathogen (10). Diarrhea and dyspnea were common among populations studied with SARS (11), but each was not highly predictive of infection in any single patient with the novel coronavirus. Thus, the high transmissibility to nurses and physicians and the higher than expected mortality were key features strongly suggesting a new pathogen. Furthermore, SARS to many clinicians appeared to have a biphasic course, with cough and fever initially followed in 3–5 days with a normal temperature and increasing hypoxia. The point is that physicians and nurses need to be trained to be alert to the unusual, the unexpected, and the variant clinical presentation. The astute, frontline health care worker is the first defense against spread of an emerging pathogen.
Early Reporting of an Epidemic
Rapid containment of a serious infectious disease epidemic depends on early notification to the world at large. With respect to SARS, much has already been said of the delays caused by Chinese officials in delaying its reporting. Their reluctance and hesitation to notify the World Health Organization (WHO) stands in sharp contrast to the transparency and quick communication from Vietnam (12).
It is assumed that fear of nationally significant, economic downturns was one key factor in the lack of early reporting from China. This is neither new nor unique, and in the future other nations will be similarly concerned about financial losses should they acknowledge an outbreak in their country. Thus, the question is, how can incentives be designed to encourage early and transparent reporting?
We would suggest that the World Bank offer financial support to countries that agree to early reporting with full disclosure about new epidemics. It is likely that the global economy would be better preserved with such a positive financial incentive. Consider the fact that estimates of the cost of SARS ranged from $30 billion to $100 billion (13). A fraction of that cost could have been invested in China late in the Fall of 2002 to help limit the spread of SARS within Guangdong providence, where it originated. At least in retrospect this would seem to indicate a great return on investment.
In addition to the positive incentives, there may indeed need to be some international censure—perhaps from the United Nations—for countries that persist in hiding an epidemic in the face of the proposed World Bank incentives. It probably should not be tied to financial penalties, however, because government officials and not the general citizenry would make the decision to obscure the truth. For example, one could consider the banning of the country from participating in the subsequent Olympics, a situation that would cause national shame for the country's political leadership. Alternatively, the offending country might not be allowed to cast votes in the United Nations for a 1-year period. Of course, there are no guarantees that either the favorable financial incentives or an international rebuke would always lead to early reporting, but the ideas are testable.
Global Surveillance
Even before the notification from Vietnam of SARS, the global web-based surveillance system overseen by the International Society for Infectious Diseases was suggesting a new epidemic. That system, called ProMed, had an unusual query approximately 2 weeks before the WHO notification of 28 February 2003:
February 10, 2003: This morning I received this e-mail and searched your archives and found nothing. Does anyone know anything about this problem? Have you heard of an epidemic in Guangdong? An acquaintance of mine from a teacher's chat room lives there and reports that the hospitals there have been closed and people are dying. Stephen O. Cummion, MD, PhD, MA. www.promed.org (14).
The question arises that since WHO has no such web-based global surveillance, could ProMed partner—at least informally with WHO—to enhance an early response after the recognition of a new epidemic. The nature of this partnership could be either in the form of a non-financial agreement or a financial agreement with an incentive for the early recognition and reporting of a new epidemic to WHO. There may be complementary, web-based systems worldwide that could be united to work on the issue of global notification.
New Role for WHO
The World Health Organization responded admirably to the SARS epidemic, taking international leadership in addressing questions to the public, coordinating scientific investigations, and quickly reporting all new advances from the laboratory and field epidemiological studies (15). There is no question that WHO emerged as a global leader in epidemic investigation and control, and their suggestions for management and prevention were quickly respected and adopted. They were especially effective in forging important partnerships with national public health authorities such as the Centers for Disease Control and Prevention in Atlanta, GA, as well as with basic scientific laboratories in Asia, Europe and the Americas.
There is, of course, no going back. The international community will anticipate the same commitment, leadership, expertise and favorable outcomes. WHO will surely have to examine its structure, activities and budget as it prepares for the next series of emerging pathogens. Equally important will be the need to reinforce and solidify the scientific relationships it made successfully and consider still new ones. A great deal of thought will have to go into its capacity to respond to future epidemics and to budget for appropriate responses.
The Global Village Concept
Those of us living in developed countries need continually to remind ourselves of the concept of a global village: within 24 h serous microbes infecting a distant population can be carried over oceans directly to our homes. With respect to SARS, the culinary delicacies of southern China—what we call exotic food choices—led initially to infections in animal handlers, chefs, and caterers and subsequently had a huge impact on the lives of people thousands of miles away.
Briefly stated, we need to make concerted efforts to be aware of and remain interested in the afflictions of individuals in remote villages. Global surveillance coupled with a sense of community are the starting points. These concepts need to be embraced and continually articulated by leaders of the Public Health System. These should be supplemented by federal research support for serious illnesses even if the illnesses are thought to belong to “other” people. The fact is that the boundaries between foreign or exotic and what is traditionally referred to as domestic or local have blurred. We in the developed world cannot afford to be disengaged or appear to show indifference to the health challenge of less fortunate populations living in remote sectors of the world. The noted ethicist Peter Singer argues that given the advances in transportation and communication, coupled with the emergence of transnational companies and universal problems, we must transcend national boundaries to embrace a new ethic of one world (16). Our ability to care and reach out defines our humanity and importantly may impact the health of our own communities.
Using Risk Factors to Choose Which Health Care Workers Manage the Patients
When the initial case control studies were reported, several analyses pointed to older age as an independent risk factor for dying. In fact, although the overall crude mortality was 9%, the mortality of those over age 60 was approximately 50% (10). The question arises, can we use such information to make policy? Specifically, should we not insist that there be an age threshold for health care workers managing patients with SARS? For example, hospitals might say that physicians and nurses older than age 45 should be exempt, and only younger colleagues should be allowed to work with suspected SARS cases.
While considering the question, we have previously suggested that should smallpox cases arrive at the hospital, only those older than 50 should manage their illnesses until younger health care workers become immune after vaccination. That suggestion was based on the likely protection of the older cohort who had received one or more vaccinations decades ago. Very likely this policy approach to smallpox would not receive much criticism or objections.
It is quite possible, however, that with respect to SARS, younger and less experienced health care workers may not easily embrace a policy that places them at risk, even if they faced a considerably lower risk of dying than older colleagues. Younger health care workers may assume that they are being asked to take a disproportionate risk in caring for SARS patients which those older than 50 are asked to avoid. Nevertheless, the facts speak for themselves, that epidemiological data clearly show age as a risk factor for death after SARS. The barrier—if it exists—is the need for a clear articulation of the issue in a sensitive manner. Furthermore, it may be reasonable to add financial incentives to health care workers—regardless of age—who take risks during the early stages of a new epidemic.
Although logical arguments can be made and should be placed into policy, the emotional responses will be formidable and very likely to make implementation difficult.
Psychological Support for Health Care Workers
An area that received so little attention was the psychological support of health care workers who came to work every day during the SARS outbreak (17). Surely they were aware of the risk of infection, the possibility of serious morbidity and even of dying from infection transmitted in the hospital as an occupational hazard. Several studies have documented the psychiatric morbidity among health workers associated with the SARS epidemic 18, 19, 20. Quarantined workers experienced stigma and fear (18), stress levels were raised (19), and feelings of extreme vulnerability, uncertainty and threat to life were perceived (20).
How can we prepare for the next epidemic that places our workforce at risk? How do we prepare physicians and nurses and comfort them and their worried families that we are doing our best to protect them? How do we respond in the face of the next epidemic early and appropriately? Academic centers have additional responsibilities to explore the fears of medical, nursing, and pharmacy students whose learning may be put on hold during an epidemic. Alternatively, the students may be in a panic way and plans for managing their exposures and concerns need to be formally addressed and managed. We suggest that institutions recognize the fear and uncertainty among health care workers when a new epidemic hits. Creating telephone hot lines with trained professionals would seem to be an important first step. Thereafter, a Psychological Support Response Team should be formed to outline appropriate procedures to manage the stresses expected and to define specific goals of intervention and therapy. Trained counselors who can explore the origins of individual fears need to be on the team and supported by infectious disease experts who can discuss the facts related to the disease, its incubation period, the risk of transmission and outcomes. Because we will continue to see new epidemics, hospitals might consider developing guidelines now that could be utilized in future introductions of new pathogens.
Use of Quarantine
The word quarantine derives from the Italian, quarantiana (40 days), which was the period of time a ship suspected of harboring plague in medieval times was forced to remain off the harbor in Venice. Unfortunately, the word also has a lurid history of being used with great prejudice in many outbreaks (21).
In SARS, the word applies to those people—including health care workers—who were identified to have been exposed but had not yet shown any signs of illness. They would be expected to remain secluded, usually at home, until the incubation period—usually 2–8 days—is exceeded.
Assume that a health care worker recognizes that he or she had an unprotected exposure to a SARS patient (see Figure 1). In our opinion, that health care worker should find alternative lodging for all family members and proceed to buy food and entertainment (books, movies, magazines) for the duration of the incubation period. He or she should have taken a mask home and agreed to take his/her temperature daily and report the reading each afternoon to the hospital's employee health program. If fever appears, the person should don the mask when entering the institution and proceed for an examination in a negative air pressure room. If no symptoms occur by the tenth day postexposure, the health care worker could return to work on the following day (22).
Figure 1.
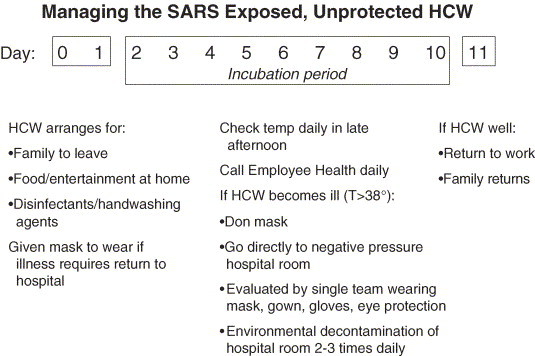
Proposal by the authors for quarantine of exposed health care workers (HCW) to SARS patients.
In theory, it may also be important to confine a population of exposed or ill people to a defined geographic location (e.g., a hotel or neighborhood). This too may be considered a quarantine. Such an action must be reserved for serious epidemics, explained clearly and empathetically by experts to those involved, and unconditionally supported by local authorities who agree to provide all needs such as food, water, heat, lodging, etc. and instituted without prejudice. Such quarantines were instituted in SARS with varying levels of success. However, in a recent report, Hawryluck and colleagues showed that of 129 previously quarantined people, symptoms of post-traumatic stress disorder were noted in 29% and depression in 31% (23).
The Continuing Role for Infection Control
In the beginning of all epidemics with new pathogens, the degree of infectiousness and mode(s) of transmission are unknown (24). There may or may not be known effective therapies, vaccines or drugs to prevent illness. SARS is a perfect example.
The only way that we as health care experts have to control epidemics early is optimal infection control. Initially, if deaths are associated with new pathogens, the presumption should be that airborne and/or large droplet transmission is possible. A private room with a negative air pressure ventilation system—if available—should be used for all suspected patients. Health care workers should use masks, gowns, eye protection, and two sets of gloves until the modes of transmission are identified. What we are emphasizing is that maximal protection should be employed early with all new, life-threatening infectious diseases. Only later if the data suggest that less stringent control measures are warranted, less should be done. Because proper use of masks was shown to be protective among health care workers exposed to unrecognized SARS, it may be that early and consistent use would have reduced both infections and mortality.
Laboratory-Associated Infections
In late 2003, the initial two laboratory-associated infections with the SARS coronavirus—one in Singapore (25) and one in Taiwan (26)—were not associated with secondary transmission. Although initial concerns related to the large number of laboratories that housed the virus, there was an unwarranted optimism that single cases would be the rule and that subsequent person-to-person transmission might not occur. The focus was appropriately placed on improving techniques in the laboratories, because in both instances carelessness led to the infections.
Much changed in the Spring of 2004 with the report from Beijing of a third laboratory-associated SARS infection (27) ( Figure 2). This time, two young laboratory workers contracted the infection and, sadly, the mother of the one of the two laboratory workers who helped take care of her ill daughter also contracted SARS and died quickly. Furthermore, a nurse who cared for one of the victims also developed SARS. These contacts represent secondary transmissions of the novel coronavirus. Four contacts of the nurse became ill with SARS, thus representing tertiary transmission of the infection. Herein is the lesson: laboratory-associated cases will occur after epidemics of new pathogens, and assiduous procedures for managing all stored laboratory specimens are essential to avoid such infections. Additionally, secondary and tertiary transmissions can occur and lead to death in some instances. All laboratories with the new pathogen should review their protocols for strict adherence to procedures that will preclude transmission to those handling such agents. These procedures should be reevaluated at least annually.
Figure 2.
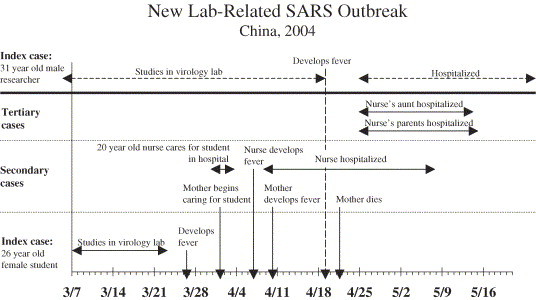
Timeline of person-to-person spread of SARS after two laboratory-associated infections in 2004 28, 29, 30, 31, 32, 33, 34.
Infection Control
In Sebastian Junger's book, The Perfect Storm (35), the author describes the improbable convergence of three low-pressure weather systems that created a terrifying storm off the coast of Nova Scotia. The swordfishing vessel, the Andrea Gail, and its crew of six who failed to take every precaution possible to avoid its path, perished in the maelstrom with crushing 100-ft waves.
As infectious disease epidemiologists tracking the course of SARS, we have enormous respect for the novel coronavirus that has incited a global torrent of worries. Scientists have good data to show that the epidemic emerged as a zoonosis, a disease primarily of animals. The SARS coronavirus, which has a crown-like appearance when seen through the electron microscope (36), became an accidental tourist, leaping from animals to nearby people—exotic animal handlers, chefs, and caterers initially. Epidemiologists had suspected this early because these same occupations among people in southern China were five-times over-represented compared to controls (37). Subsequently, microbiological confirmation came after an almost identical virus was isolated from the civit cat, a member of the mongoose family considered to be a culinary delicacy in the Guandong Province. Other exotic animals were also found to harbor the virus, and healthy animal handlers were shown to have a high prevalence of antibodies to the SARS coronavirus. However, the most important animal source of the epidemic that sparked the initial human infections remains uncertain. Thereafter, person-to-person spread occurred from patients to health care workers and both family members and other contacts. Almost 8500 people in 30 countries were infected, and 9% of the victims died.
For the most part, close contact is required for human transmission: the victim has to be within 3 ft of a patient to transfer the virus via a large droplet 38, 39. This is similar to what usually happens after a cough or sneeze in the spread of Streptococcus pyogenes pharyngitis and most agents of pneumonia. Ro represents the mathematical symbol for the average number of secondary cases occurring after each index case, and it is referred to as the case reproduction number. The relatively low case reproduction number for SARS, an Ro of 2–4, also supports transmission mostly by large droplets (39).
Sometimes, however, superspreaders were identified, passing the virus to those not in close proximity. This raises the likelihood of airborne spread by droplet nuclei (40), microscopic hot air balloons that encase the virus and allow it to stay suspended in the air currents for hours. This situation would be analogous to what happens with influenza, measles or tuberculosis. Eventually, the tiny droplets can be inhaled and reach all the way to the alveoli.
Early in the disease, the SARS coronavirus was found in blood, raising the hazardous possibility that blood transfusion or accidental needlestick injuries could be active modes of transmission (41). The virus is also found in saliva, urine, sweat and tears of infected people 42, 43. Furthermore, since the virus is shed in the feces for 30 days (44) and can survive for over 24 h on hard surfaces, environmental contact with the hands could occur with subsequent self-inoculation, should a health care worker or visitor touch his/her eyes or nasal mucosa. Hand transmissions of the virus to previously uninfected patients also might occur.
It should be no surprise that with such a varied portfolio of transmission possibilities in hospitals approximately 50% of the victims of SARS were nurses, physicians and other health care workers. One can begin to understand the angst of infection-control experts who worked diligently to avert the epidemic: imploring health care workers to wear gowns, gloves, masks, as well as face shields to protect their eyes, to wash their hands assiduously, to clean the environment with a disinfectant, refuse to allow blood transfusions from the victims, and to avoid needlesticks early in the disease course. Fortunately, those broad efforts appear to have worked.
While there is a lull in the action, we might re-examine some general principles, because the next wave of respiratory pathogens is just off the horizon: 1) Do we have sufficient capacity to manage such infections effectively in our hospitals? Probably not, yet with the annual visits of influenza and its 36,000 deaths in the U.S., the continuing threat of bioterror, the arrival of monkeypox in the U.S., and recent experience with SARS, which may return, large hospitals need to provide a geographically clustered area with an additional 10 or more rooms with negative air pressure (negative to the hallway) so that a variety of respiratory pathogens can be contained to the patients' rooms. Such steps would go a long way to create a new era of preparedness, not focused only on the latest pathogen. 2) There can be no excuse for health care workers who fail to wash hands between patients. Unfortunately, the current compliance rates in U.S. critical care units are only 40–60%. Better rates of hand washing need to be realized. Hand-washing rates should become an issue for the annual evaluation of health care workers and a necessary component for continued employment. 3) There are a limited number of occasions when the hospital environment needs to be disinfected and not just cleaned. It is recognized that transmission of most infections in the hospital is not from the environment. Nevertheless, we pay insufficient attention to this aspect of infection control when we are beset with specific problems. In all ongoing challenges with multi-antibiotic resistant, hospital-acquired infections (now common in the U.S.), antibiotic-associated diarrheal infections, and now SARS, we have several unique situations in which it is useful to decontaminate the hard surfaces that are commonly touched, such as bedside tables, door knobs, and IV poles. 4) To avoid needlestick injuries and the spread of bloodborne infections, we need to champion the available technology of non-sharp devices such as retractable needles after blood draws. If these technologies are affordable and effectively used, they will have the benefit of reducing in-hospital transmission of hepatitis C, HIV infection, and others—possibly including SARS.
The psychological impact of new diseases has received scant attention, and hospitals need to develop effective programs for counseling its healthcare workers who are at risk of infection and death and who sense personal danger when novel and frightening pathogens arrive.
The versatile SARS coronavirus has stunned the economic and health care institutions around the world. It has its broad repertoire of options for transmission in hospitals, which have traditionally had too few respiratory airborne isolation units, poor hand-washing compliance, too little investment in avoiding sharps injuries, and no commitment to the psychological preparation of its staff for dealing with life-threatening infections. The current circumstances have conspired to create a perfect hospital pathogen. In response, we need to seize the opportunity to prepare not just for a return of this single agent, but to a host of pathogens that will mimic its modes of transmission. The unsettling winds of the next disturbance are heading our way.
Conclusions
There are many lessons from SARS that apply generally to all epidemics. We would summarize by emphasizing the following: the importance of clinicians recognizing a new syndrome, the need for individuals and countries to report epidemics, the role of information technology to communicate, and the key role for the WHO. Quarantine must be employed with care and compassion. The obligation to be interested in the health of all people, the use of assiduous infection control and the need for psychological support of health care workers must be integral components of our approach to SARS and future epidemics.
(ARCMED-D-05-00112)
References
- 1.World Health Organization. Cumulative number of reported probable cases of severe acute respiratory syndrome (SARS). Available at: http://www.who.int/csr/sars/country/table2004_04_21/en/. Accessed July 14, 2004.
- 2.Avendano M., Derkach P., Swan S. Clinical course and management of SARS in health care workers in Toronto: a case series. CMAJ. 2003;168:1649–1660. [PMC free article] [PubMed] [Google Scholar]
- 3.Poutanen S.M., Low D.E., Henry B., Finkelstein S., Rose D., Green K., Tellier R., Draker R., Adachi D., Ayers M., Chan A.K., Skowronski D.M., Salit I., Simor A.E., Slutsky A.S., Doyle P.W., Krajden M., Petric M., Brunham R.C., McGeer A.J., National Microbiology Laboratory, Canada, Canadian Severe Acute Respiratory Syndrome Study Team Identification of severe acute respiratory syndrome in Canada. N Engl J Med. 2003;248:1995–2005. doi: 10.1056/NEJMoa030634. [DOI] [PubMed] [Google Scholar]
- 4.Chan-Yeung M., Yu W.C. Outbreak of severe acute respiratory syndrome in Hong Kong Special Administrative Region: case report. BMJ. 2003;326:850–852. doi: 10.1136/bmj.326.7394.850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.World Health Organization Outbreak news—severe acute respiratory syndrome (SARS) Wkly Epidemiol Rec. 2003;78:81–83. [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention Severe acute respiratory syndrome: Singapore, 2003. MMWR Morb Mortal Wkly Rep. 2003;52:405–411. [PubMed] [Google Scholar]
- 7.Lee N., Hui D., Wu A., Chan P., Cameron P., Joynt G.M., Ahuja A., Yung M.Y., Leung C.B., To K.F., Lui S.F., Szeto C.C., Chung S., Sung J.J. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1986–1994. doi: 10.1056/NEJMoa030685. [DOI] [PubMed] [Google Scholar]
- 8.Centers for Disease Control and Prevention Cluster of Severe Acute Respiratory Syndrome Cases Among Protected Health Care Workers—Toronto, Canada, April 2003. MMWR Morb Mortal Wkly Rep. 2003;52:433–438. [PubMed] [Google Scholar]
- 9.Reilley B., VanHerp M., Sermand D., Dentico N. SARS and Carlo Urbani. N Engl J Med. 2003;348:1951–1952. doi: 10.1056/NEJMp030080. [DOI] [PubMed] [Google Scholar]
- 10.Choi K.W., Chau T.N., Tsang O., Tso E., Chiu M.C., Tong W.L., Lee P.O., Ng T.K., Ng W.F., Lee K.C., Lam Y., Yu W.C., Lai J.Y., Lai S.T., Princess Margaret Hospital SARS Study Group Outcomes and prognostic factors in 267 patients with severe acute respiratory syndrome in Hong Kong. Ann Intern Med. 2003;139:715–723. doi: 10.7326/0003-4819-139-9-200311040-00005. [DOI] [PubMed] [Google Scholar]
- 11.Peiris J.S.M., Chu C.M., Cheng V.C., Chan K.S., Hung I.F., Poon L.L., Law K.I., Tang B.S., Hon T.Y., Chan C.S., Chan K.H., Ng J.S., Zheng B.J., Ng W.L., Lai R.W., Guan Y., Yuen K.Y., HKU/UCH SARS Study Group Clinical progression and viral load in a community outbreak of pneumonia: a prospective study. Lancet. 2003;361:1767–1772. doi: 10.1016/S0140-6736(03)13412-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rosenthal E. NY Times; April 10, 2003. A Beijing doctor questions data on illness. A8. [Google Scholar]
- 13.Assessing the Impact and Cost of SARS in Developing Asia. Asian Development Outbreak 2003. Update. R003. pp 75–92.
- 14.International Society for Infectious Diseases. ProMED-mail. Available at: http://www.promedmail.org/pls/askus/f?p=2400:1000. Accessed July 14, 2004.
- 15.World Health Organization. Communicable Disease Surveillance and Response: Severe Acute Respiratory Syndrome. Available at: http://www.who.int/csr/sars/en/. Accessed July 14, 2004.
- 16.Singer P. 2nd ed. Yale University Press; New Haven, CT: 2004. One World: The Ethics of Globalization. [Google Scholar]
- 17.Maunder R., Hunter J., Vincent L., Bennett J., Peladeau N., Leszcz M., Sadavoy J., Verhaeghe L.M., Steinberg R., Mazzulli T. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ. 2003;168:1245–1251. [PMC free article] [PubMed] [Google Scholar]
- 18.Robertson E., Hershenfield K., Grace S.L., Stewart D.E. The Psychosocial Effects of Being Quarantined Following Exposure to SARS: A Qualitative Study of Toronto Health Care Workers. Can J Psychiatry. 2004;49:403–407. doi: 10.1177/070674370404900612. [DOI] [PubMed] [Google Scholar]
- 19.Chua S.E., Cheung V., Cheung C., McAlonan G.M., Wong J.W., Cheung E.P., Chan M.T., Wong M.M., Tang S.W., Choy K.M., Wong M.K., Chu C.M., Tsang K.W. Psychological effects of the SARS outbreak in Hong Kong on high-risk health care workers. Can J Psychiatry. 2004;49:391–393. doi: 10.1177/070674370404900609. [DOI] [PubMed] [Google Scholar]
- 20.Chong M.Y., Wang W.C., Hsieh W.C., Lee C.Y., Chiu N.M., Yeh W.C., Huang O.L., Wen J.K., Chen C.L. Psychological impact of severe acute respiratory syndrome on health care workers in a tertiary hospital. Br J Psychiatry. 2004;185:127–133. doi: 10.1192/bjp.185.2.127. [DOI] [PubMed] [Google Scholar]
- 21.Verghese A. NY Times Magazine; April 20, 2003. Viral Terrors. 15–16. [Google Scholar]
- 22.Wenzel R.P., Edmond M.B. Listening to SARS: lessons for infection control. Ann Intern Med. 2003;139:592–593. doi: 10.7326/0003-4819-139-7-200310070-00012. [DOI] [PubMed] [Google Scholar]
- 23.Hawryluck L., Gold W.L., Robinson S., Pogorski S., Galea S., Styra R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg Infect Dis. 2004;10:1206–1212. doi: 10.3201/eid1007.030703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wenzel R.P., Edmond M.B. Managing SARS amidst uncertainty. N Engl J Med. 2003;348:1947–1948. doi: 10.1056/NEJMp030072. [DOI] [PubMed] [Google Scholar]
- 25.Normile D. SARS Experts want labs to improve safety practices. Science. 2003;302:31. doi: 10.1126/science.302.5642.31a. [DOI] [PubMed] [Google Scholar]
- 26.Normile D. Second lab accident fuels fears about SARS. Science. 2004;303:26. doi: 10.1126/science.303.5654.26. [DOI] [PubMed] [Google Scholar]
- 27.Yardley J. NY Times; April 23, 2003. China Reports Suspected Case of SARS in Beijing. A5. [Google Scholar]
- 28.Xinhua News Agency. China's new SARS cases may have resulted from lab infection, spokesman says. April 23, 2004.
- 29.Yardley J., Altman L.K. NY Times; April 24, 2004. China is scrambling to curb SARS cases after a death. A4. [Google Scholar]
- 30.Xinhua News Agency. Official: Beijing's first SARS patient can be discharged fro hospital in 10 days. May 1, 2004.
- 31.Xinhua News Agency. Two more SARS patients discharged from hospital. May 13, 2004.
- 32.Xinhua News Agency. One SARS patient discharged from hospital. May 21, 2004.
- 33.Xinhua News Agency. Laboratory pinpointed as source of China's SARS outbreak. July 1, 2004.
- 34.World Health Organization. Summary of China's investigation into the April outbreak. Available at: http://www.wpro.who.int/sars/docs/update/update_07022004_revisedfinal.asp. Accessed July 14, 2004.
- 35.Junger S. WW Norton and Company; New York: 1997. The Perfect Storm: A True Story of Men against the Sea. [Google Scholar]
- 36.Kuiken T., Fouchier R.A.M., Schultien M., Rimmelzwaan G.F., van Amerongen G., van Riel D., Laman J.D., de Jong T., van Doomum G., Lim W., Ling A.E., Chan P.K., Tam J.S., Zambon M.C., Gopal R., Drosten C., van der Werf S., Escriou N., Manuguerra J.C., Stohr K., Peiris J.S., Osterhaus A.D. Newly discovered coronavirus as the primary cause of severe respiratory syndrome. Lancet. 2003;362:263–270. doi: 10.1016/S0140-6736(03)13967-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rosenthal E. NY Times; April 27, 2003. From China's provinces, a crafty germ spreads. A1. [Google Scholar]
- 38.Peiris J.S.M., Yuen K.Y., Osterhaus A.D., Stohr K. The severe acute respiratory syndrome. N Engl J Med. 2003;349:2431–2441. doi: 10.1056/NEJMra032498. [DOI] [PubMed] [Google Scholar]
- 39.Dye C., Gay N. Modeling the SARS Epidemic. Science. 2003;300:1884–1885. doi: 10.1126/science.1086925. [DOI] [PubMed] [Google Scholar]
- 40.Yu I.T.S., Li Y., Wong T.W., Tam W., Chan A.T., Lee J.H., Leung D.Y., Ho T. Evidence of airborne transmission of the severe acute respiratory syndrome virus. N Engl J Med. 2004;350:1731–1739. doi: 10.1056/NEJMoa032867. [DOI] [PubMed] [Google Scholar]
- 41.Ng L.F.P., Wong M., Koh S., Ooi E.E., Tang K.F., Leong H.N., Ling A.E., Agathe L.V., Tan J., Liu E.T., Ren E.C., Ng L.C., Hibberd M.L. Detection of severe acute respiratory syndrome coronavirus in blood of infected patients. J Clin Microbiol. 2004;42:347–350. doi: 10.1128/JCM.42.1.347-350.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ding Y., He L., Zhang Q., Huang Z., Che X., Hou J., Wang H., Shen H., Qiu L., Li Z., Geng J., Cai J., Han H., Li X., Kang W., Weng D., Liang P., Jiang S. Organ distribution of severe acute respiratory syndrome (SARS) associated coronavirus (SARS-CoV) in SARS patients: implications for pathogenesis and virus transmission pathways. J Pathol. 2004;203:622–630. doi: 10.1002/path.1560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Loon S.C., Teoh S.C., Oon L.L., Se-Thoe S.Y., Ling A.E., Leo Y.S., Leong H.N. The severe acute respiratory syndrome coronavirus in tears. Br J Ophthalmol. 2004;88:861–863. doi: 10.1136/bjo.2003.035931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lau S.K., Woo P.C., Wong B.H., Tsoi H.W., Woo G.K., Poon R.W., Chan K.H., Wei W.I., Peiris J.S., Yuen K.Y. Detection of severe acute respiratory syndrome (SARS) coronavirus nucleocapsid protein in SARS patients by enzyme linked immunosorbent assay. J Clin Microbiol. 2004;42:2884–2889. doi: 10.1128/JCM.42.7.2884-2889.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]