

Abstract
Allergic diseases are common in all age groups and locations around the world. In the United States, allergic diseases affect 20 to 40 million people annually, including 10% to 30% of adults and close to 40% of children. An estimated 15 million people in the United States have been diagnosed as having asthma, with this number on the rise. Concomitant asthma affects 67% of patients who have allergic rhinitis. As a result of the increase in ventilation during exercise, athletes in particular experience significant symptoms of allergy triggered by exposure to aeroallergens. The allergic response causes nasal and conjunctival congestion, tearing, breathing difficulties, pruritus, fatigue, and mood changes, which affect athletic performance. Systemic symptoms of anaphylaxis from allergy, although rare, can be life threatening. Several decades ago it was inconceivable that an athlete who had asthma could perform competitively, let alone win Olympic gold medals. Today, with proper diagnosis, education, and optimal therapeutic management, the allergic athlete can achieve great strides in all sports endeavors. To avoid seasonal allergic flares and maximize performance, the physician providing care for an athlete who has seasonal allergies must be aware of the climatic patterns of aeroallergen expression, and adjust exercise and pharmacologic regimens accordingly. This article summarizes the effects of allergic disease on exercise and highlights the challenges that seasonal allergy place on athletic performance. Doping considerations grant additional complexity to this issue and underscore the need for a competent, skillful, informed, and ethical approach to treating seasonal allergy in the competitive athlete.
Allergic diseases are among the most common chronic diseases and have been increasing worldwide over the past several decades for reasons that are still not clearly understood [1], [2], [3], [4], [5], [6]. There has been considerable research elucidating the impact that allergic disease has on athletic performance. Athletes who have allergic disease can benefit from the tremendous progress that has been made in understanding the pathophysiologic basis of their disease. Accessing the host of international climatic and seasonal pollen reports available can enable athletes to be better prepared for training and performance. Additionally, athletes can benefit from an evolving repertoire of therapeutic modalities for allergic diseases that conform to current antidoping codes (www.wada-ama.org).
Pathophysiology of allergic disease
Atopic diseases such as asthma, allergic rhinitis, urticaria, and anaphylaxis are characterized by hypersensitivity to a particular allergen, resulting in secretion of specific immunoglobulin E (IgE) antibodies and acute, recurrent, or chronic inflammation. Certain individuals with an atopic predisposition synthesize IgE antibodies on initial exposure to allergen. IgE binding to mast cells and basophils sets the stage for the allergic response. On re-exposure, allergen cross-links IgE on cell surfaces, which causes the release of a host of inflammatory mediators. Early response mediators include granule mediators (eg, histamine, tryptase) and lipid mediators (eg, leukotrienes, prostaglandins). Cytokines such as tumor necrosis factor-alpha (TNF-α), interleukins, and chemokines (IL-8, MCP-1 and MIP-1α) are produced minutes to hours later (Fig. 1 ) [7], [8]. The type of allergen, the degree and length of exposure, and the atopic tendency of the individual determine the manifestation of symptoms.
Fig. 1.
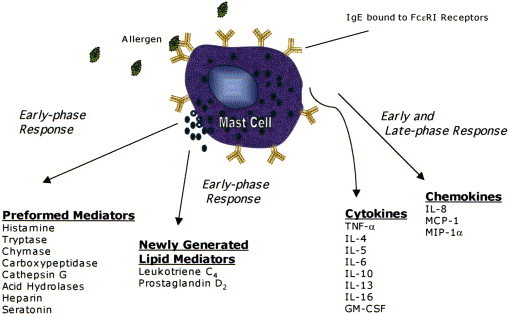
Mediators of mast cells and basophils. TNF, tumor necrosis factor; IL, interleukin; GM-CSF, granulocyte-macrophage colony-stimulating factor; MCP, monocyte chemotactic protein; MIP, monocyte inflammatory protein.
Sources of allergens include the environment (eg, tree, grass and weed pollen, dust, mold), foods, drugs, and stinging insects. Aeroallergens are further subdivided into seasonal aeroallergens, like tree, grass and weed pollen, and nonseasonal aeroallergens like mold and dust [9].
Pollen counts
The concentration of pollen in the atmosphere, which correlates with allergic manifestations, is reported and disseminated at multiple centers internationally. In the United States and Canada, a useful resource is The National Allergy Bureau, which provides pollen and mold counts from approximately 75 counting stations (www.aaaai.org/nab/).
Manifestations of allergy
Physical manifestation of allergy is often debilitating. In the lung there may be bronchoconstriction or asthma; in the nose, rhinitis; in the skin, urticaria; in the eyes, conjunctivitis. Systemic manifestations of allergy characterize anaphylaxis, which may be life threatening and require immediate medical attention. Anaphylaxis that occurs in conjunction with exercise, termed exercise-induced anaphylaxis, has been reported in certain individuals [10]. In addition to the inflammatory response, allergic disease manifestations have been associated with fatigue [11], depression [12], and decrements in cognition [13]. In fact, epidemiologic evidence suggests that seasonality of even extreme behavioral manifestation, such as suicide, may be associated with allergy [14] or with exposure to seasonal allergens, specifically tree pollen [15].
Diagnosis of allergy
In addition to the clinical manifestations of an allergic disorder, in vivo and laboratory-based testing for allergen sensitivity is used to strengthen the diagnosis of allergic disease. Skin-prick and intradermal testing provide a rapid and functional measure of IgE-mediated hypersensitivity in the skin with a resultant wheal and flare response that occurs within 15 minutes of allergen contact. In situations of decreased skin response from treatment with antihistamines, increased skin sensitivity from dermatographism, or logistical constrains, athletes may opt for the radioallergosorbent test (RAST), which detects specific IgE antibodies in serum with comparable sensitivity and specificity to skin-prick testing [16].
Seasonal effects of allergy on athletes
Environmental exposures
Athletes are particularly vulnerable to the effects of the environment, as many athletic activities—whether they are for leisure, training, or competition—occur outdoors. When athletes train and compete, often for long durations of time, they make intimate contact with the outdoor elements that are comprised of a host of topographical, seasonal, and climatic components. Exposure to the various elements is magnified by increased ventilation (up to 200 L/min during exercise), which intensifies the contact between the respiratory system and environment, and by inhalation of poor quality and cold air, which often affects those who train year-round in temperate climates [17], [18]. During the winter months, cold air inhalation during exercise exacerbates exercise-induced asthma in people with asthma [19]. Track and field athletes have extensive exposure to various seasonal pollen allergens during the spring (trees), summer (grass), and early fall (ragweed) [20]. Susceptible athletes may develop conjunctival inflammation, rhinitis, or bronchial inflammation as a consequence of these environmental conditions.
Allergies and Olympic athletes
Based on a 15-year database of aeroallergen records, an in-depth study reported the predicted aeroallergen counts that would be observed in association with the 2004 Olympic games in Athens, Greece. The study predicted that peak pollen concentrations would be observed during training in March and May, and high levels of goosefoot, mugwort, Alternaria, and Cladisporum spores would be observed in August and September during the Olympic games [21], thus highlighting the need for preparation, testing, and therapy.
An earlier survey of allergic disease in elite athletes reported that 20% of the 1984 Australian Olympic team had allergic disorders based on clinical evaluation (not including skin testing or RAST) [22]. Of 214 Australian Olympic athletes studied during the 2000 Sydney Olympics, which took place during the period of high tree pollen (over 5000 grains per CμM), a high prevalence of perennial and seasonal allergic disease was reported. Within that group, 56% reported a history of allergic rhinoconjunctivitis, 41% were symptomatic with a positive skin test to a potential allergen, 29% were diagnosed with seasonal allergic rhinoconjunctivitis based on history and skin testing, and 21% suffered from asthma [23]. Before the 2004 Olympics in Athens, Greece, information regarding circulating aeroallergens in neighboring cities was published to attempt to minimize the allergy symptoms and help athletes achieve peak performance. Understandably, the incidence of adverse responses to seasonal allergens is common amongst athletes. Although athletes with allergic diseases have successfully won many Olympic medals, the detrimental contribution of pollutants, allergens, or other environmental factors has occasionally produced severe exacerbations of allergic conditions, warranting medical attention and causing suboptimal performance.
Seasonal exposures to infectious agents may also induce seasonal decrements in athletic performance. Viral infections reviewed in Nelson et al [24], such as influenza, reovirus, and respiratory syncytial virus, manifest a seasonal peak in winter and early, cause significant morbidity, may trigger bronchial hyper-reactivity, and may result in secondary bacterial infections such as sinus or bronchial infections (Table 1 ).
Table 1.
Seasonality of infectious diseases
| Infection | Peak prevalence |
|---|---|
| Malaria | Winter–early spring |
| Leishmaniasis | Winter–early spring |
| Influenza | Winter–early spring |
| Human reovirus | Winter |
| Coronavirus | Winter–early spring |
| Respiratory syncytial virus | Winter–early spring, summer |
Adapted from Nelson RJ, Demas GE, Klein SL, et al. Seasonal patterns of stress, immune function, and disease. 1st edition. Cambridge, MA: Cambridge University Press; 2002.
Several studies have characterized the relationship between viral infection, which is primarily a T-helper type 1 (Th1) response, and enhancement of allergic disease, which is a T-helper type 2 (Th2) response. Viral infections like influenza A may trigger allergic asthma by interfering with tolerance to aeroallergens [25], inducing a concomitant Th1 response [26], and causing recruitment of Th2 cells into the lung [27]. In some people, seasonal allergy and mood vulnerability to inflammation may interact, and people with allergies may experience more post-flu mood worsening than those without allergies [28].
Allergic rhinitis
Allergic rhinitis in athletes
Often the initial contact of pollen and other airborne components is with nasal mucosal and eyes. Studies have shown that allergic rhinoconjunctivitis is under-recognized and certainly undertreated in elite athletes [18]. Helenius et al [29] reported the results of a survey of 49 athletes competing in summer events. The diagnosis of allergic rhinoconjunctivitis was more common among athletes than in a control group of nonathletes (P = .037). Helbling et al [30] surveyed 2961 Swiss athletes who participated in 68 sports. Of the 79% who responded to the questionnaire, 16.8% indicated they suffered from hay fever and 59% reported that they needed medication during the pollen season. Individuals who have allergic rhinitis also often have increased bronchial hyperresponsiveness [31], [32].
Pathophysiology and presentation
Allergic rhinitis (AR) is characterized by nasal mucosa edema as a result of IgE-mediated release of early- and late-phase mediators and Th2 cytokines, which promotes the infiltration of mucosa with inflammatory cells such as eosinophils, neutrophils, basophils, T cells, and macrophages [2], [33], [34]. AR is characterized by nasal congestion, rhinorrhea, sneezing, itching of the nose, or postnasal drainage and is often associated with allergic conjunctivitis manifested by ocular itch, tearing, redness, and sometimes swelling and photophobia. These and other signs and symptoms of AR are listed in Box 1 . Allergic, irritant, infectious, hormonal, occupational, and other factors are causative agents in nasal mucosal edema [35]. Peak presentations of allergic rhinoconjunctivitis occur between 10 to 25 years, which includes the age range of most elite athletes [3].
Box 1.
Signs and symptoms of allergic rhinitis
Itching of the nose, ears, palate, throat
Sneezing spells
Clear and watery rhinorrhea
Congestion
Sinus headache
Mouth breathing
Post-nasal drip
Sleep disturbance
Cough
Fatigue
Allergic rhinitis and athletic performance
Although exercise may increase nasal airway patency, likely by way of increased sympathetic nerve discharge [36], there are several reasons why AR may interfere with athletic performance. Rhinitis often causes changes in sleep patterns because of nasal obstruction, rhinorrhea, and sinus pressure that add to tiredness and fatigue and impair athletic performance [18]. Additionally, short bursts of sprinting require nasal breathing for optimal performance [36], implicating nasal obstruction as a deleterious factor in performance. AR has been associated with alteration in central nervous system (CNS) function, which may significantly affect the athlete's ability to perform. Using a standardized computer-based battery of cognitive processing tests, subjects who have AR experienced decrements in reaction time, attention, and vigilance when exposed to pollen [13]. Others associated AR with increased fatigue [11], depression [11], [37], and anxiety in women [38], which all pose a potential hindrance to performance.
The mechanism by which seasonal environmental exposures may affect these cognitive and emotional parameters has not been elucidated. Reichenberg et al [39] has shown activation of the innate immune response in humans by low-dose endotoxin exposure and subsequent release of pro-inflammatory cytokines (eg, IL-1, IL-6, TNF-α), some of which are also released by IgE-mediated responses in the nasal mucosa (see Fig. 1) [40], [41]. The exposure to endotoxins and secretion of cytokines induced depressive symptoms, anxiety, and cognitive impairment in the absence of constitutional symptoms (eg, decreased energy, anorexia, drowsiness) [39], [42]. Circulating cytokines may also induce activation of the HPA-axis [43], and elevation of corticotrophin-releasing factor (CRF) and cortisol have been shown to contribute to major affective illness [44]. Furthermore, cytokines in the respiratory tract may stimulate specific receptors present in the vagus nerve and affect brain function through this pathway [45]. As such, cytokine release could contribute to decrements in cognition and to the onset or exacerbation of depression or anxiety, thus having detrimental effects on athletic performance.
Management of allergic rhinitis
Prevention
Athletes must prepare themselves for the various climatic conditions they will encounter in their training locale and the competition destinations. Knowledge of the temperature, humidity, sunlight, altitude, season, and type and concentration of pollen they will be exposed to can help athletes achieve peak performance through the use of prophylactic measures [21].
Nonpharmacologic therapy
Various nonpharmacologic therapies have been effective under certain conditions. For the treatment of AR, saline nasal irrigation is a safe and effective method of cleansing the nasal mucosa of allergens, and improving nasosinus disease [46]. External nasal dilators have been used by athletes [47] to increase nasal valve area, which is the narrowest area in the nasal canal [46], [48], and to significantly decrease submaximal exercise-perceived exertion, heart rate, ventilation, and volume of oxygen use [47].
Pharmacologic treatment and doping concerns
Beginning with the earliest Olympic games, athletes have enhanced athletic performance through the use of foreign substances. In 1967, the International Olympic Commission developed a list of prohibited methods and substances to protect the health of, and foster equality for, all competing athletes [49]. In the realm of allergic diseases, these restrictions have generated significant challenges. For example, the overall Olympic champion in women's gymnastics at the 2000 Olympics was disqualified and her gold medal withdrawn because she used a medication for AR which contained pseudoephedrine, allegedly without the intent of doping. Pseudoephedrine is no longer on the Prohibited List (Table 2 ). In 1972, the winner of the 400-meter men's Freestyle was disqualified because significant levels of the banned drug ephedrine were detected in his post-race urinalysis. The swimmer had used a combination ephedrine/theophylline preparation for the prerace treatment of his asthma [22]. These examples highlight the importance for athletes, coaches, and team physicians to understand the potential that a particular medication, apparently innocuous, may contain or be contaminated by a particular banned substance. To establish a universal internationally standardized Olympic antidoping code, the World Anti-Doping Agency (WADA) was established in 1999. The WADA disseminates current information on substances prohibited for use by competitive athletes. WADA maintains and updates the World Anti-Doping Code Prohibited List, which includes substances that are prohibited only during competition, others that are always prohibited, and others that are on the monitoring list (see Table 2). More and current updated information regarding antidoping rules, regulations, and prohibited substance listings can be found at www.wada-ama.org.
Table 2.
Medical treatment of seasonal allergic diseases related to athletes
| Drug | Mode of action | Use | Comments | WADA statusa |
|---|---|---|---|---|
| Antihistamines | Histamine antagonist at H1 receptor site | Allergic rhinitis and conjunctivitis, urticaria, allergic asthma | First-line therapy for mild to moderate symptoms | Not prohibited |
| Oral first-generation | Often combined with oral decongestant | |||
| Oral second-generation | Very effective for symptoms of rhinorrhea, sneezing, and nasal and ocular itch | |||
| Intranasal | First-generation formulations have significant CNS adverse effects, second-generation preferred | |||
| Topical (optical) | ||||
| Corticosteroids | Antiinflammatory | Treatment of many allergic diseases: allergic rhinitis and conjunctivitis, asthma, urticaria, and atopic dermatitis | Potent antiinflammatory | Systemicb uses are prohibitedc; inhaled and intranasal only require abbreviated TUEd; topical are not prohibited |
| Oral | intranasal — first-line therapy for moderate to severe symptoms of rhinitis | |||
| Inhaled | oral — severe exacerbations of asthma, urticaria | |||
| Intranasal | ||||
| Topical (skin) | ||||
| Decongestants | α-adrenergic agonist | Rhinitis | Reduces nasal congestion | Ephedrine is prohibitede, phenylephrine, phenylpropanolamine, pseudoephedrine, and synephrine are on monitoring listf |
| Oral | Causes nasal vasoconstriction | May cause insomnia, loss of appetite, and nervousness | ||
| Intranasal | Intranasal may cause rebound nasal congestion (rhinitis medicamentosa) | |||
| Cromolyn/nedocromil sodium | Mast cell stabilizer | Asthma, allergic rhinitis | Nonsteroidal antiinflammatory | Not prohibited |
| Oral | Inhibits degranulation | Minimal adverse effects | ||
| Inhaled | Requires multiple daily dosing | |||
| Intranasal | ||||
| Anticholinergic | Muscarinic receptor antagonist | Asthma, rhinitis | Effectively reduce rhinorrhea | Not prohibited |
| Inhaled | Role in acute bronchospasm | |||
| Intranasal | ||||
| Leukotriene inhibitors | Inhibit phospholipid metabolism | Asthma | Nonsteroidal antiinflammatory | Not prohibited |
| Oral | Very effective in preventing EIA | |||
| Steroid sparing controller | ||||
| Allergen immunotherapy | Th2 response suppression | Allergic rhinitis and conjunctivitis, asthma | Very effective for allergic rhinitis | Not prohibited |
| Th1 response stimulated | ||||
| Anti-IgE antibody | Reduces serum IgE | Severe asthma, possibly allergic rhinitis | Approved for severe asthma | Not prohibited |
| IM injection | Requires multiple IM injections | |||
| Expensive | ||||
| β2 agonist | Bind β2 adrenergic receptor, ↑cAMP, relaxes bronchial smooth muscle | Asthma | First-line therapy in preventing EIA | Prohibited in general, some formulations with specific clinical indications require only an abbreviated TUEg |
| Inhaled | ||||
| Short-acting | ||||
| Long-acting | ||||
| Theophylline | Inhibits phosphodiesterase, causing bronchodilation | Asthma | Long-term controller | Not prohibited |
| Oral | Required serum level monitoring | |||
| Inhaled | ||||
| Epinephrine | α- and β-adrenergic agonist | Anaphylaxis | Universally recommended drug of choice for acute anaphylaxis | During competition requires a TUE |
| Adult dose: SQ or IM, 0.2–0.5 ml of 1/1000 (wt/vol) dilution |
Abbreviations: cAMP, cyclic adenosine monophosphate; EIA, exercise-induced asthma; IM, intramuscularly; SQ, subcutaneously; TUE, therapeutic use exemption.
Based on the WADA 2005 Prohibited List International Standard, see www.wada.com for current updated information.
Orally, rectally, IV, or IM.
In competition only. Any substance or method that is on the Prohibited List must be granted a Therapeutic Use Exemption (TUE) for use.
nonsystemic routes require the completion of an abbreviated TUE application. Dermatological preparations are not prohibited.
Prohibited when its concentration in urine is >5 mcg/mL.
These stimulants are no longer on the Prohibited List, but are on the 2005 monitoring program “in order to detect patterns of misuse in sports.”
All β2-agonists including their D- and L-isomers are currently (2005) prohibited in and out of competition and require a TUE for use. Formoterol, salbutamol, salmeterol, and terbutaline are permitted by inhalation to prevent and or/treat asthma and exercise-induced asthma/bronchoconstriction, with the completion of abbreviated TUE application.
Pharmacologic therapies
Oral decongestants, such as pseudoephedrine and phenylpropanolamine, are effective in reducing nasal congestion from rhinitis, although they can cause insomnia, loss of appetite, and excessive nervousness [3], [50]. These decongestants are no longer on the Prohibited List, but have been placed on the 2005 Monitoring Program to detect patterns of misuse in sports (see Table 2). Topical α-adrenergic nasal decongestants are commonly used, but may cause rhinitis medicamentosa, the syndrome of rebound nasal congestion, when overused [3]. Antihistamines are commonly used, have long been standard therapy for seasonal and perennial AR, and are effective in relieving symptoms of itching, sneezing and rhinorrhea, and allergic conjunctivitis [6], [51]. The older first-generation antihistamines are significantly limited by their sedative and anticholinergic adverse effects and may compromise important psychomotor skills (eg, reaction time, visual discrimination) [52], and therefore should be avoided. The newer second-generation antihistamines are preferred because of their longer duration of action and minimal, if any, CNS adverse effects [53], [54]. Intranasal steroids are likely the most effective therapy for AR and allergic conjunctivitis. Their efficacy is maximized with continuous use [53], but there are also proven as-need benefits [55]. They have the benefit over antihistamines of down-regulating numerous steps in the inflammatory process, including reducing the release of cytokines and chemokines [56]. Their use in Olympic athletes requires the application for an abbreviated therapeutic use exemption (TUE). Several studies have shown concurrent reduction with use of intranasal corticosteroids in bronchial hyperresponsiveness [5]. Leukotriene modifiers have confirmed benefit in allergic rhinitis comparable to antihistamines [57]. Other effective intranasal agents include intranasal antihistamines, ipratropium bromide, and cromolyn sodium [3]. To date, there have been no published reports of immunotherapy specifically targeting elite athletes [18]. However, allergen immunotherapy significantly decreases the severity of AR, reduces the requirement for pharmacotherapy, and improves quality of life [53].
Asthma
Asthma in athletes
Asthma is characterized by variable airflow obstruction, bronchial hyperresponsiveness, and airway inflammation. Respiratory viral infections (most common), allergens, irritants, drugs, climatic conditions, exercise, and other stimuli can induce asthmatic exacerbations. In a survey of 214 athletes representing 12 Olympic sports, 21% reported having experienced asthma [23]. The reason for the higher prevalence of asthma among athletes is because of their exposure to various climatic conditions (eg, cold in winter), pollen content (eg, grass, weed, trees), and various pathophysiologic changes that occur during exercise that may promote bronchial hyperresponsiveness [17], [19], [58], [59], [60], [61], [62], [63]. When strenuous exercise results in resistance to airflow, the phenomenon is called exercise-induced bronchospasm or exercise-induced asthma (EIA) [19].
Exercise-induced asthma
Pathogenesis and presentation
Various factors have been described in the development of EIA. The generally accepted pathogenesis of EIA involves the loss of heat and water from airway mucosa [59], [64], [65], [66]. During exercise and increased respiratory rate, large volumes of dry, cold air reduce airway cooling as it travels along the tracheobronchial tree, which may cause bronchial constriction through a reflex stimulation of airway receptors. This response may lead to changes in mucosal osmolarity and promote mast cell degranulation, consequently furthering bronchoconstriction [67]. Rapid airway rewarming after exercise may cause vascular congestion, increased permeability, and edema, leading to obstruction [19], [68].
EIA symptoms of chest tightness, wheezing, and shortness of breath generally follow a brief period of bronchodilation that occurs at initiation of exercise. Bronchoconstriction peaks 8 to 15 minutes after exercise and resolves in about 60 minutes. A refractory period of up to 3 hours after recovery, during which time repeat exercise causes less bronchospasm, has been observed.[68]. Although EIA generally commences following the cessation of physical exertion, it may also appear during sustained activity [69].
Seasonal consideration in exercise-induced asthma
Track and field athletes are extensively exposed to seasonal allergens. When the rate of breathing exceeds 30 L/min, there is a shift from nose breathing to combined mouth and nasal breathing, thereby increasing deposition of airborne allergens and other inhaled particles into the lower airway [20]. Asthmatic subjects who are allergic to birch pollen were shown to have aggravated EIA responses during the pollen season when compared with the response of asthmatic individuals who are not allergic to birch pollen [63].
Challenges in the diagnosis of exercise-induced asthma
In has been reported that 40% to 90% of asthmatics have EIA [61], [67], [70], [71], [72]. Before the 1984 Summer Olympics, 67 of 597 (11%) athletes screened for performance experienced symptoms of EIA, yet only 26% of theses athletes had a history of asthma [60]. However, 42 of 67 reported symptoms of asthma during strenuous exercise, thus emphasizing the importance of screening for EIA in well-conditioned individuals who appear to be in excellent health [73].
EIA is a common and often unrecognized problem among school-age participants in sports [74]. In a cohort of 256 adolescent athletes, 9.4% were diagnosed with EIA. Yet screening for EIA through physical examination and history did not accurately predict it and would have detected only about half of the children who were diagnosed as having EIA using spirometry [75]. Furthermore, 9% of individuals in the general population who have EIA have no history of asthma.
Management of asthma
Prophylaxis
Detailed prior knowledge of environmental exposures can help prevent or minimize exacerbation. Once a pattern of symptoms has been established, prophylaxis is the key to therapy in patients who have EIA. Physical warm-up can reduce EIA. Continuous, low-intensity warm-up is more effective than interval warm-up in preventing EIA in athletes [76]. In certain cold conditions, such as those experienced by cross-country skiers, breathing filters are being used [67]. Although there is no clear evidence that physical conditioning decreases EIA or improves pulmonary function, it does delay the symptoms of EIA from reaching threshold [77].
Pharmacologic therapy
Long-term and more effective control is gained with pharmacologic intervention. The most common and effective prophylactic therapies used before exercise are β2 agonists, cromolyn, and nedocromil (see Table 2) [78], [79], [80]. Inhaled corticosteroids may be helpful in reducing bronchial hyperresponsiveness when used for their long-term antiinflammatory effects. Theophylline preparations and anticholinergics are used as tertiary agents when other agents are proven ineffective. However, the requirement for blood-level monitoring of a narrow therapeutic window makes theophylline a less desirable alternative agent for athletes [61]. Short-acting β2 agonists are considered first-line therapy and provide protection in 80% to 90% of subjects with minimal adverse effects [81], [82]. Long-acting β2 agonists can prevent bronchial obstruction for 10 to 12 hours [83] and provide athlete with a full day of protection. Formoterol, salbutamol, salmeterol, and terbutaline are permitted by inhalation with the completion of an abbreviated TUE, but all other β2 agonists, including their D- and L-isomers are prohibited in and out of competition, according to the 2005 Prohibited List (see Table 2). Regular use of β2 agonists without antiinflammatory treatment may increase airway responsiveness to irritants and foster allergen-induced late bronchoconstriction and airway inflammation [84].
Given the central role of IgE in the pathogenesis of allergic disease, inhibiting IgE responses through the use of anti-IgE antibodies would decrease its sensitizing effects on mast cells and basophils. Several studies indicate that anti-IgE therapy is effective in the treatment of asthma and allergic rhinitis [85], [86], [87], [88]. However, the implications for athletes are unknown.
In conclusion, evidence supports that seasonal allergy confers a seasonal vulnerability for performance decrements in competition and training. Specific interventions that prevent and directly address the allergic symptomatology, tailored to athletes' individual needs in specific circumstances, could prevent seasonal decompensation in performance or restore functioning to baseline levels.
Acknowledgments
We would like to thank Dr. Dean D. Metcalfe for his suggestions regarding the organization of this article.
References
- 1.Annesi-Maesano I. Epidemiological evidence of the occurrence of rhinitis and sinusitis in asthmatics. Allergy. 1999;54(Suppl 57):S7–S13. doi: 10.1111/j.1398-9995.1999.tb04401.x. [DOI] [PubMed] [Google Scholar]
- 2.Dykewicz M.S., Fineman S., Skoner D.P. Diagnosis and management of rhinitis: complete guidelines of the Joint Task Force on Practice Parameters in Allergy, Asthma and Immunology. American Academy of Allergy, Asthma, and Immunology. Ann Allergy Asthma Immunol. 1998;81:478–518. doi: 10.1016/s1081-1206(10)63155-9. [DOI] [PubMed] [Google Scholar]
- 3.International Consensus Report on the diagnosis and management of rhinitis. International Rhinitis Management Working Group. Allergy. 1994;49(Suppl 19):S1–S34. [PubMed] [Google Scholar]
- 4.Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet. 1998;351(9111):1225–1232. [PubMed] [Google Scholar]
- 5.Casale T.B., Amin B.V. Allergic rhinitis/asthma interrelationships. Clin Rev Allergy Immunol. 2001;21(1):27–49. doi: 10.1385/CRIAI:21:1:27. [DOI] [PubMed] [Google Scholar]
- 6.Rosenwasser L.J. Treatment of allergic rhinitis. Am J Med. 2002;113(Suppl 9A):S17–S24. doi: 10.1016/s0002-9343(02)01433-x. [DOI] [PubMed] [Google Scholar]
- 7.Boyce J.A. Mast cells: beyond IgE. J Allergy Clin Immunol. 2003;111(1):24–32. doi: 10.1067/mai.2003.60. [Quiz Review 33] [DOI] [PubMed] [Google Scholar]
- 8.Schwartz L.B. Effector cells of anaphylaxis: mast cells and basophils. Novartis Found Symp. 2004;257:65–74. [PubMed] [Google Scholar]
- 9.Solomon W.R. Airborne pollen: a brief life. J Allergy Clin Immunol. 2002;109(6):895–900. doi: 10.1067/mai.2002.125556. [DOI] [PubMed] [Google Scholar]
- 10.Castells M.C., Horan R.F., Sheffer A.L. Exercise-induced anaphylaxis. Curr Allergy Asthma Rep. 2003;3(1):15–21. doi: 10.1007/s11882-003-0005-x. [DOI] [PubMed] [Google Scholar]
- 11.Marshall P.S., O'Hara C., Steinberg P. Effects of seasonal allergic rhinitis on fatigue levels and mood. Psychosom Med. 2002;64(4):684–691. doi: 10.1097/01.psy.0000021944.35402.44. [DOI] [PubMed] [Google Scholar]
- 12.Timonen M., Jokelainen J., Herva A. Presence of atopy in first-degree relatives as a predictor of a female proband's depression: results from the Northern Finland 1966 Birth Cohort. J Allergy Clin Immunol. 2003;111(6):1249–1254. doi: 10.1067/mai.2003.1546. [DOI] [PubMed] [Google Scholar]
- 13.Wilken J.A., Berkowitz R., Kane R. Decrements in vigilance and cognitive functioning associated with ragweed-induced allergic rhinitis. Ann Allergy Asthma Immunol. 2002;89(4):372–380. doi: 10.1016/S1081-1206(10)62038-8. [DOI] [PubMed] [Google Scholar]
- 14.Timonen M., Viilo K., Hakko H. Is seasonality of suicides stronger in victims with hospital-treated atopic disorders? Psychiatry Res. 2004;126(2):167–175. doi: 10.1016/j.psychres.2004.02.005. [DOI] [PubMed] [Google Scholar]
- 15.Postolache T.T., Stiller J.W., Herrell R., et al. Tree pollen peaks are associated with increased nonviolent suicide in women. Mol Psychiatry, in press [DOI] [PMC free article] [PubMed]
- 16.Hamilton R.G., Adkinson N.F., Jr 23. Clinical laboratory assessment of IgE-dependent hypersensitivity. J Allergy Clin Immunol. 2003;111(Suppl 2):S687–S701. doi: 10.1067/mai.2003.123. [DOI] [PubMed] [Google Scholar]
- 17.Helenius I.J., Tikkanen H.O., Haahtela T. Occurrence of exercise induced bronchospasm in elite runners: dependence on atopy and exposure to cold air and pollen. Br J Sports Med. 1998;32(2):125–129. doi: 10.1136/bjsm.32.2.125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Katelaris C.H., Carrozzi F.M., Burke T.V. Allergic rhinoconjunctivitis in elite athletes: optimal management for quality of life and performance. Sports Med. 2003;33(6):401–406. doi: 10.2165/00007256-200333060-00002. [DOI] [PubMed] [Google Scholar]
- 19.McFadden E.R., Jr, Gilbert I.A. Exercise-induced asthma. N Engl J Med. 1994;330(19):1362–1367. doi: 10.1056/NEJM199405123301907. [DOI] [PubMed] [Google Scholar]
- 20.Helenius I., Haahtela T. Allergy and asthma in elite summer sport athletes. J Allergy Clin Immunol. 2000;106(3):444–452. doi: 10.1067/mai.2000.107749. [DOI] [PubMed] [Google Scholar]
- 21.Gioulekas D., Damialis A., Papakosta D. 15-year aeroallergen records. Their usefulness in Athens Olympics, 2004. Allergy. 2003;58(9):933–938. doi: 10.1034/j.1398-9995.2003.00244.x. [DOI] [PubMed] [Google Scholar]
- 22.Fitch K.D. Management of allergic Olympic athletes. J Allergy Clin Immunol. 1984;73:722–727. doi: 10.1016/0091-6749(84)90314-2. [DOI] [PubMed] [Google Scholar]
- 23.Katelaris C.H., Carrozzi F.M., Burke T.V., Fitch K.D. A springtime Olympics demands special consideration for allergic athletes. J Allergy Clin Immunol. 2000;106(2):260–266. doi: 10.1067/mai.2000.108603. [DOI] [PubMed] [Google Scholar]
- 24.Nelson R.J., Demas G.E., Klein S.L. Seasonal patterns of stress, immune function, and disease. 1st edition. Cambridge University Press; Cambridge, MA: 2002. [Google Scholar]
- 25.Tsitoura D.C., Kim S., Dabbagh K. Respiratory infection with influenza A virus interferes with the induction of tolerance to aeroallergens. J Immunol. 2000;165(6):3484–3491. doi: 10.4049/jimmunol.165.6.3484. [DOI] [PubMed] [Google Scholar]
- 26.Dahl M.E., Dabbagh K., Liggitt D. Viral-induced T helper type 1 responses enhance allergic disease by effects on lung dendritic cells. Nat Immunol. 2004;5(3):337–343. doi: 10.1038/ni1041. [DOI] [PubMed] [Google Scholar]
- 27.Stephens R., Randolph D.A., Huang G. Antigen-nonspecific recruitment of Th2 cells to the lung as a mechanism for viral infection-induced allergic asthma. J Immunol. 2002;169(10):5458–5467. doi: 10.4049/jimmunol.169.10.5458. [DOI] [PubMed] [Google Scholar]
- 28.Bell I.R., Jasnoski M.L., Kagan J. Depression and allergies: survey of a nonclinical population. Psychother Psychosom. 1991;55(1):24–31. doi: 10.1159/000288404. [DOI] [PubMed] [Google Scholar]
- 29.Helenius I.J., Tikkanen H.O., Sarna S. Asthma and increased bronchial responsiveness in elite athletes: atopy and sport event as risk factors. J Allergy Clin Immunol. 1998;101(5):646–652. doi: 10.1016/S0091-6749(98)70173-3. [DOI] [PubMed] [Google Scholar]
- 30.Helbling A., Jenoure P., Muller U. [The incidence of hay fever in leading Swiss athletes] Schweiz Med Wochenschr. 1990;120(7):231–236. [German] [PubMed] [Google Scholar]
- 31.Prieto L., Gutierrez V., Linana J. Bronchoconstriction induced by inhaled adenosine 5′-monophosphate in subjects with allergic rhinitis. Eur Respir J. 2001;17(1):64–70. doi: 10.1183/09031936.01.17100640. [DOI] [PubMed] [Google Scholar]
- 32.Ramsdale E.H., Morris M.M., Roberts R.S. Asymptomatic bronchial hyperresponsiveness in rhinitis. J Allergy Clin Immunol. 1985;75(5):573–577. doi: 10.1016/0091-6749(85)90032-6. [DOI] [PubMed] [Google Scholar]
- 33.Berger W.E. Treatment update: allergic rhinitis. Allergy Asthma Proc. 2001;22(4):191–198. [PubMed] [Google Scholar]
- 34.Borish L. Allergic rhinitis: systemic inflammation and implications for management. J Allergy Clin Immunol. 2003;112(6):1021–1031. doi: 10.1016/j.jaci.2003.09.015. [DOI] [PubMed] [Google Scholar]
- 35.Dykewicz M.S. 7. Rhinitis and sinusitis. J Allergy Clin Immunol. 2003;111(Suppl 2):S520–S529. doi: 10.1067/mai.2003.82. [DOI] [PubMed] [Google Scholar]
- 36.Richerson H.B., Seebohm P.M. Nasal airway response to exercise. J Allergy. 1968;41(5):269–284. doi: 10.1016/0021-8707(68)90032-4. [DOI] [PubMed] [Google Scholar]
- 37.Hurwitz E.L., Morgenstern H. Cross-sectional associations of asthma, hay fever, and other allergies with major depression and low-back pain among adults aged 20–39 years in the United States. Am J Epidemiol. 1999;150(10):1107–1116. doi: 10.1093/oxfordjournals.aje.a009936. [DOI] [PubMed] [Google Scholar]
- 38.Addolorato G., Ancona C., Capristo E. State and trait anxiety in women affected by allergic and vasomotor rhinitis. J Psychosom Res. 1999;46(3):283–289. doi: 10.1016/s0022-3999(98)00109-3. [DOI] [PubMed] [Google Scholar]
- 39.Reichenberg A., Yirmiya R., Schuld A. Cytokine-associated emotional and cognitive disturbances in humans. Arch Gen Psychiatry. 2001;58(5):445–452. doi: 10.1001/archpsyc.58.5.445. [DOI] [PubMed] [Google Scholar]
- 40.Schwartz L.B. Mediators of human mast cells and human mast cell subsets. Ann Allergy. 1987;58(4):226–235. [PubMed] [Google Scholar]
- 41.Schwartz L.B., Bradford T.R., Irani A.M. The major enzymes of human mast cell secretory granules. Am Rev Respir Dis. 1987;135(5):1186–1189. doi: 10.1164/arrd.1987.135.5.1186. [DOI] [PubMed] [Google Scholar]
- 42.Pollmacher T., Haack M., Schuld A. Low levels of circulating inflammatory cytokines–do they affect human brain functions? Brain Behav Immun. 2002;16(5):525–532. doi: 10.1016/s0889-1591(02)00004-1. [DOI] [PubMed] [Google Scholar]
- 43.Turnbull A.V., Rivier C. Regulation of the HPA axis by cytokines. Brain Behav Immun. 1995;9(4):253–275. doi: 10.1006/brbi.1995.1026. [DOI] [PubMed] [Google Scholar]
- 44.Gold P.W., Chrousos G.P. Organization of the stress system and its dysregulation in melancholic and atypical depression: high vs low CRH/NE states. Mol Psychiatry. 2002;7(3):254–275. doi: 10.1038/sj.mp.4001032. [DOI] [PubMed] [Google Scholar]
- 45.Goehler L.E., Gaykema R.P., Hansen M.K. Vagal immune-to-brain communication: a visceral chemosensory pathway. Auton Neurosci. 2000;85(1–3):49–59. doi: 10.1016/S1566-0702(00)00219-8. [DOI] [PubMed] [Google Scholar]
- 46.Tomooka L.T., Murphy C., Davidson T.M. Clinical study and literature review of nasal irrigation. Laryngoscope. 2000;110(7):1189–1193. doi: 10.1097/00005537-200007000-00023. [DOI] [PubMed] [Google Scholar]
- 47.Griffin J.W., Hunter G., Ferguson D. Physiologic effects of an external nasal dilator. Laryngoscope. 1997;107(9):1235–1238. doi: 10.1097/00005537-199709000-00014. [DOI] [PubMed] [Google Scholar]
- 48.Portugal L.G., Mehta R.H., Smith B.E. Objective assessment of the breathe-right device during exercise in adult males. Am J Rhinol. 1997;11(5):393–397. doi: 10.2500/105065897781286061. [DOI] [PubMed] [Google Scholar]
- 49.Fraser A.D. Doping control from a global and national perspective. Ther Drug Monit. 2004;26(2):171–174. doi: 10.1097/00007691-200404000-00015. [DOI] [PubMed] [Google Scholar]
- 50.Chait L.D. Factors influencing the reinforcing and subjective effects of ephedrine in humans. Psychopharmacology (Berl) 1994;113(3–4):381–387. doi: 10.1007/BF02245213. [DOI] [PubMed] [Google Scholar]
- 51.Meltzer E.O., Weiler J.M., Widlitz M.D. Comparative outdoor study of the efficacy, onset and duration of action, and safety of cetirizine, loratadine, and placebo for seasonal allergic rhinitis. J Allergy Clin Immunol. 1996;97(2):617–626. doi: 10.1016/s0091-6749(96)70307-x. [DOI] [PubMed] [Google Scholar]
- 52.Montgomery L.C., Deuster P.A. Effects of antihistamine medications on exercise performance. Implications for sportspeople. Sports Med. 1993;15(3):179–195. doi: 10.2165/00007256-199315030-00004. [DOI] [PubMed] [Google Scholar]
- 53.Bousquet J., Van Cauwenberge P., Khaltaev N. Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol. 2001;108(Suppl 5):S147–S334. doi: 10.1067/mai.2001.118891. [DOI] [PubMed] [Google Scholar]
- 54.Wilken J.A., Kane R.L., Ellis A.K. A comparison of the effect of diphenhydramine and desloratadine on vigilance and cognitive function during treatment of ragweed-induced allergic rhinitis. Ann Allergy Asthma Immunol. 2003;91(4):375–385. doi: 10.1016/S1081-1206(10)61685-7. [DOI] [PubMed] [Google Scholar]
- 55.Jen A., Baroody F., de Tineo M. As-needed use of fluticasone propionate nasal spray reduces symptoms of seasonal allergic rhinitis. J Allergy Clin Immunol. 2000;105(4):732–738. doi: 10.1067/mai.2000.105225. [DOI] [PubMed] [Google Scholar]
- 56.Howarth P.H. A comparison of the anti-inflammatory properties of intranasal corticosteroids and antihistamines in allergic rhinitis. Allergy. 2000;55(Suppl 62):S6–S11. doi: 10.1034/j.1398-9995.2000.00702.x. [DOI] [PubMed] [Google Scholar]
- 57.Meltzer E.O., Malmstrom K., Lu S. Concomitant montelukast and loratadine as treatment for seasonal allergic rhinitis: a randomized, placebo-controlled clinical trial. J Allergy Clin Immunol. 2000;105(5):917–922. doi: 10.1067/mai.2000.106040. [DOI] [PubMed] [Google Scholar]
- 58.McFadden E.R., Jr Exercise-induced airway obstruction. Clin Chest Med. 1995;16(4):671–682. [PubMed] [Google Scholar]
- 59.McFadden E.R., Jr, Ingram R.H., Jr Exercise-induced airway obstruction. Annu Rev Physiol. 1983;45:453–463. doi: 10.1146/annurev.ph.45.030183.002321. [DOI] [PubMed] [Google Scholar]
- 60.Pierson W.E., Voy R.O. Exercise-induced bronchospasm in the XXIII summer Olympic games. N Engl Reg Allergy Proc. 1988;9(3):209–213. doi: 10.2500/108854188779023405. [DOI] [PubMed] [Google Scholar]
- 61.Randolph C. Exercise-induced asthma: update on pathophysiology, clinical diagnosis, and treatment. Curr Probl Pediatr. 1997;27(2):53–77. doi: 10.1016/s0045-9380(97)80002-3. [DOI] [PubMed] [Google Scholar]
- 62.Tan R.A., Spector S.L. Exercise-induced asthma: diagnosis and management. Ann Allergy Asthma Immunol. 2002;89(3):226–235. doi: 10.1016/S1081-1206(10)61948-5. [DOI] [PubMed] [Google Scholar]
- 63.Karjalainen J., Lindqvist A., Laitinen L.A. Seasonal variability of exercise-induced asthma especially outdoors. Effect of birch pollen allergy. Clin Exp Allergy. 1989;19(3):273–278. doi: 10.1111/j.1365-2222.1989.tb02383.x. [DOI] [PubMed] [Google Scholar]
- 64.Tsai C.L., Saidel G.M., McFadden E.R., Jr Radial heat and water transport across the airway wall. J Appl Physiol. 1990;69(1):222–231. doi: 10.1152/jappl.1990.69.1.222. [DOI] [PubMed] [Google Scholar]
- 65.Gilbert I.A., Fouke J.M., McFadden E.R., Jr Heat and water flux in the intrathoracic airways and exercise-induced asthma. J Appl Physiol. 1987;63(4):1681–1691. doi: 10.1152/jappl.1987.63.4.1681. [DOI] [PubMed] [Google Scholar]
- 66.McFadden E.R., Jr, Nelson J.A., Skowronski M.E. Thermally induced asthma and airway drying. Am J Respir Crit Care Med. 1999;160(1):221–226. doi: 10.1164/ajrccm.160.1.9810055. [DOI] [PubMed] [Google Scholar]
- 67.Carlsen K.H. Exercise induced asthma in children and adolescents and the relationship to sports. Pediatr Allergy Immunol. 1998;9(4):173–180. doi: 10.1111/j.1399-3038.1998.tb00369.x. [DOI] [PubMed] [Google Scholar]
- 68.Tan R.A., Spector S.L. Exercise-induced asthma. Sports Med. 1998;25(1):1–6. doi: 10.2165/00007256-199825010-00001. [DOI] [PubMed] [Google Scholar]
- 69.Wallace J.M., Stein S., Au J. Special problems of the asthmatic patient. Curr Opin Pulm Med. 1997;3(1):72–79. [PubMed] [Google Scholar]
- 70.Poppius H., Muittari A., Kreus K.E. Exercise asthma and disodium cromoglycate. Br Med J. 1970;4(731):337–339. doi: 10.1136/bmj.4.5731.337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Jones R.S., Buston M.H., Wharton M.J. The effect of exercise on ventilatory function in the child with asthma. Br J Dis Chest. 1962;56:78–86. doi: 10.1016/s0007-0971(62)80005-9. [DOI] [PubMed] [Google Scholar]
- 72.Rupp N.T., Brudno D.S., Guill M.F. The value of screening for risk of exercise-induced asthma in high school athletes. Ann Allergy. 1993;70(4):339–342. [PubMed] [Google Scholar]
- 73.Milgrom H., Taussig L.M. Keeping children with exercise-induced asthma active. Pediatrics. 1999;104(3):e38. doi: 10.1542/peds.104.3.e38. [DOI] [PubMed] [Google Scholar]
- 74.Mehta H., Busse W. Prevalence of exercise-induced asthma in the athlete. In: Weiler J.M., editor. Allergic and respiratory disease in sports medicine. Marcel Dekker, Inc; New York: 1997. pp. 81–86. [Google Scholar]
- 75.Hallstrand T.S., Curtis J.R., Koepsell T.D. Effectiveness of screening examinations to detect unrecognized exercise-induced bronchoconstriction. J Pediatr. 2002;141(3):343–348. doi: 10.1067/mpd.2002.125729. [DOI] [PubMed] [Google Scholar]
- 76.McKenzie D.C., McLuckie S.L., Stirling D.R. The protective effects of continuous and interval exercise in athletes with exercise-induced asthma. Med Sci Sports Exerc. 1994;26(8):951–956. [PubMed] [Google Scholar]
- 77.Carroll N., Sly P. Exercise training as an adjunct to asthma management? Thorax. 1999;54(3):190–191. doi: 10.1136/thx.54.3.190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Latimer K.M., O'Byrne P.M., Morris M.M. Bronchoconstriction stimulated by airway cooling. Better protection with combined inhalation of terbutaline sulphate and cromolyn sodium than with either alone. Am Rev Respir Dis. 1983;128(3):440–443. doi: 10.1164/arrd.1983.128.3.440. [DOI] [PubMed] [Google Scholar]
- 79.Tullett W.M., Tan K.M., Wall R.T. Dose-response effect of sodium cromoglycate pressurised aerosol in exercise induced asthma. Thorax. 1985;40(1):41–44. doi: 10.1136/thx.40.1.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Roberts J.A., Thomson N.C. Attenuation of exercise-induced asthma by pretreatment with nedocromil sodium and minocromil. Clin Allergy. 1985;15(4):377–381. doi: 10.1111/j.1365-2222.1985.tb03006.x. [DOI] [PubMed] [Google Scholar]
- 81.Bundgaard A., Buch D., Schmidt A. Pretreatment of exercise-induced asthma in children using disodium cromoglycate and fenoterol inhalation powder. Eur J Respir Dis Suppl. 1983;130:36–41. [PubMed] [Google Scholar]
- 82.American Academy of Pediatrics: Section on Allergy and Immunology; Section on Diseases of the Chest Exercise and the asthmatic child. Pediatrics. 1989;84(2):392–393. [PubMed] [Google Scholar]
- 83.Green C.P., Price J.F. Prevention of exercise induced asthma by inhaled salmeterol xinafoate. Arch Dis Child. 1992;67(8):1014–1017. doi: 10.1136/adc.67.8.1014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Cockcroft D.W., McParland C.P., Britto S.A. Regular inhaled salbutamol and airway responsiveness to allergen. Lancet. 1993;342(8875):833–837. doi: 10.1016/0140-6736(93)92695-p. [DOI] [PubMed] [Google Scholar]
- 85.Lanier B.Q., Corren J., Lumry W. Omalizumab is effective in the long-term control of severe allergic asthma. Ann Allergy Asthma Immunol. 2003;91(2):154–159. doi: 10.1016/S1081-1206(10)62170-9. [DOI] [PubMed] [Google Scholar]
- 86.Busse W., Corren J., Lanier B.Q. Omalizumab, anti-IgE recombinant humanized monoclonal antibody, for the treatment of severe allergic asthma. J Allergy Clin Immunol. 2001;108(2):184–190. doi: 10.1067/mai.2001.117880. [DOI] [PubMed] [Google Scholar]
- 87.Milgrom H., Fick R.B., Jr, Su J.Q. Treatment of allergic asthma with monoclonal anti-IgE antibody. rhuMAb-E25 Study Group. N Engl J Med. 1999;341(26):1966–1973. doi: 10.1056/NEJM199912233412603. [DOI] [PubMed] [Google Scholar]
- 88.Kaliner M.A. Omalizumab and the treatment of allergic rhinitis. Curr Allergy Asthma Rep. 2004;4(3):237–244. doi: 10.1007/s11882-004-0032-2. [DOI] [PubMed] [Google Scholar]