

Abstract
Background
Autism spectrum disorders (ASD) include autistic disorder, Asperger's disorder and pervasive developmental disorder ‐ not otherwise specified (PDD‐NOS). Antipsychotics have been used as a medication intervention for irritability related to ASD. Aripiprazole, a third‐generation, atypical antipsychotic, is a relatively new drug that has a unique mechanism of action different from that of other antipsychotics. This review updates a previous Cochrane review on the safety and efficacy of aripiprazole for individuals with ASD, published in 2011 (Ching 2011).
Objectives
To assess the safety and efficacy of aripiprazole as medication treatment for individuals with ASD.
Search methods
In October 2015, we searched the Cochrane Central Register of Controlled Trials (CENTRAL), Ovid MEDLINE, Embase, the Cumulative Index to Nursing and Allied Health Literature (CINAHL) and seven other databases as well as two trial registers. We searched for records published in 1990 or later, as this was the year aripiprazole became available.
Selection criteria
Randomised controlled trials (RCTs) of aripiprazole (administered orally and at any dosage) versus placebo for treatment of individuals with a diagnosis of ASD.
Data collection and analysis
Two review authors independently collected, evaluated and analysed data. We performed meta‐analysis for primary and secondary outcomes, when possible. We used the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) approach to rate the overall quality of the evidence.
Main results
We included three trials in this review. Two were included in the previous published review, and the results of one, placebo‐controlled discontinuation study were added to this review. Although we searched for studies across age groups, we found only studies conducted in children and youth. Included trials had low risk of bias across most domains. High risk of bias was seen in only one trial with incomplete outcome data. We judged the overall quality of the evidence for most outcomes to be moderate.
Two RCTs with similar methods evaluated use of aripiprazole for a duration of eight weeks in 316 children/adolescents with ASD. Meta‐analysis of study results revealed a mean improvement of ‐6.17 points on the Aberrant Behavior Checklist (ABC) ‐ Irritability subscale (95% confidence intervals (CIs) ‐9.07 to ‐3.26, two studies, 308 children/adolescents, moderate‐quality evidence), ‐7.93 points on the ABC ‐ Hyperactivity subscale (95% CI ‐10.98 to ‐4.88, two studies, 308 children/adolescents, moderate‐quality evidence) and ‐2.66 points on the ABC ‐ Stereotypy subscale (95% CI ‐3.55 to ‐1.77, two studies, 308 children/adolescents, moderate‐quality evidence) in children/adolescents taking aripiprazole relative to children/adolescents taking placebo. In terms of side effects, children/adolescents taking aripiprazole had a greater increase in weight, with a mean increase of 1.13 kg relative to placebo (95% CI 0.71 to 1.54, two studies, 308 children/adolescents, moderate‐quality evidence), and had a higher risk ratio (RR) for sedation (RR 4.28, 95% CI 1.58 to 11.60, two studies, 313 children/adolescents, moderate‐quality evidence) and tremor (RR 10.26, 95% CI 1.37 to 76.63, two studies, 313 children/adolescents, moderate‐quality evidence). A randomised, placebo‐controlled discontinuation study found that 35% of children/adolescents randomised to continue intervention with aripiprazole relapsed with respect to their symptoms of irritability, compared with 52% of children/adolescents randomised to placebo, for a hazard ratio of 0.57 (95% CI 0.28 to 1.12, 85 children/adolescents, low‐quality evidence).
All three included trials were supported by Bristol‐Myers Squibb (Princeton, NJ) and Otsuka Pharmaceutical Company, Ltd. (Tokyo, Japan), with editorial support provided by Ogilvy Healthworld Medical Education and Bristol‐Myers Squibb.
Authors' conclusions
Evidence from two RCTs suggests that aripiprazole can be effective as a short‐term medication intervention for some behavioural aspects of ASD in children/adolescents. After a short‐term medication intervention with aripiprazole, children/adolescents showed less irritability and hyperactivity and fewer stereotypies (repetitive, purposeless actions). However, notable side effects, such as weight gain, sedation, drooling and tremor, must be considered. One long‐term, placebo discontinuation study found that relapse rates did not differ between children/adolescents randomised to continue aripiprazole versus children/adolescents randomised to receive placebo, suggesting that re‐evaluation of aripiprazole use after a period of stabilisation in irritability symptoms is warranted. Studies included in this review used criteria from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM‐IV) (APA 2000) for ASD diagnosis; however, the diagnostic criteria for ASD changed significantly with release of the fifth edition of the DSM (DSM‐5) in 2013 (APA 2013).
Keywords: Adolescent; Child; Female; Humans; Male; Antipsychotic Agents; Antipsychotic Agents/therapeutic use; Aripiprazole; Aripiprazole/therapeutic use; Child Development Disorders, Pervasive; Child Development Disorders, Pervasive/drug therapy; Hyperkinesis; Hyperkinesis/drug therapy; Irritable Mood; Irritable Mood/drug effects; Randomized Controlled Trials as Topic
Plain language summary
Aripiprazole for autism spectrum disorders (ASD)
Background
Aripirazole is an antipsychotic drug ‐ a type of medication used to treat serious mental disorders such as paranoia. It has also been used to treat behavioural problems (e.g. aggression, severe temper tantrums) in people with autism spectrum disorders (ASD). Aripiprazole has been shown to be well tolerated and to improve behavioural problems in other disorders such as schizophrenia and bipolar disorder. As aripiprazole is a relatively new drug, it is important to understand both the benefits and side effects of this drug in patients with ASD.
Review question
Do children and adults with ASD benefit from treatment with aripiprazole, compared with other children and adults with ASD who receive a drug with no active ingredient (placebo)?
Study characteristics
In this review, we included three studies that investigated effects of aripiprazole. Two were short‐term (eight weeks) studies that evaluated whether aripiprazole improved behavioural problems in a total of 316 children/adolescents. The third was a longer‐term (up to 16 weeks) study in which 85 children/adolescents whose symptoms initially improved on aripiprazole discontinued the medication to evaluate whether their behavioural problems recurred. All participants were between six and 17 years of age. All studies used multiple behavioural checklists to assess symptoms of ASD.
Key results and quality of evidence
Short‐term studies found improved irritability, hyperactivity and stereotypy (i.e. repetitive behaviours) and inappropriate speech in children/adolescents with ASD taking aripiprazole as compared with placebo. Researchers found no improvement in lethargy/withdrawal (i.e. lack of energy and reduced alertness). White children/adolescents were less likely to relapse (return to older, problematic behaviours) when taking aripiprazole, but this finding was not reported in children/adolescents of other races. Rates of movement disorder side effects such as tremor, muscle rigidity and involuntary movement were higher in children/adolescents taking aripiprazole in all trials. Results of this review suggest that short‐term use of aripiprazole may improve irritability, hyperactivity and repetitive movements in children/adolescents with ASD, although both weight gain and neurological side effects (e.g. involuntary movements of the face and jaw) can occur. Children and adolescents taking aripiprazole should be re‐evaluated periodically to monitor improvements in ASD symptoms and side effects. Overall, the quality of this evidence is moderate. Since the time these studies were conducted, an updated version of the manual for diagnosing ASD and other conditions has been published. Additional studies evaluating safety and benefits of long‐term use of aripiprazole would be helpful.
Summary of findings
for the main comparison.
| Aripiprazole compared with placebo for autism spectrum disorders (ASD)* | ||||
|
Patient or population: children/youth with ASD Settings: ambulatory care Intervention: aripiprazole Comparison: placebo | ||||
| Outcomes | Effect (95% confidence interval) |
Number of participants (studies) |
Quality of the evidence (GRADE) | Comments |
|
ABC ‐ Irritability subscale Mean score changes 8 weeks of treatment |
MD ‐6.17 (‐9.07 to ‐3.26) points relative to placebo, in favour of aripiprazole | 308 (2) |
⊕⊕⊕⊝ Moderatea | ‐ |
|
ABC ‐ Hyperactivity subscale Mean score changes 8 weeks of treatment |
MD ‐7.93 (‐10.98 to ‐4.88) points relative to placebo, in favour of aripiprazole | 308 (2) |
⊕⊕⊕⊝ Moderatea | ‐ |
|
ABC ‐ Stereotypy subscale Mean score changes 8 weeks of treatment |
MD ‐2.66 (‐3.55 to ‐1.77) points relative to placebo, in favour of aripiprazole | 308 (2) |
⊕⊕⊕⊝ Moderatea | ‐ |
|
Weight gain 8 weeks of treatment |
MD 1.13 (0.71 to 1.54) points relative to placebo | 308 (2) |
⊕⊕⊕⊝ Moderatea | ‐ |
|
Sedation 8 weeks of treatment |
RR 4.28 (1.58 to 11.60) | 313 (2) |
⊕⊕⊕⊝ Moderatea | ‐ |
|
Tremor 8 weeks of treatment |
RR 10.26 (1.37 to 76.63) | 313 (2) |
⊕⊕⊕⊝ Moderatea | ‐ |
|
Relapse rate 16 weeks of treatment |
HR 0.57 (0.28 to 1.12) | 85 (1) |
Lowb | ‐ |
| ABC: Aberrant Behavior Checklist; GRADE: Grades of Recommendation, Assessment, Development and Evaluation; HR: hazard ratio;MD: mean difference; RR: risk ratio | ||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||
aQuality was rated as moderate because of unclear risk of bias for some domains in Marcus 2009 and Owen 2009, and because of the overall small number of studies conducted using aripiprazole in ASD. bQuality of evidence for long‐term trials was rated as low because of high risk of attrition bias for incomplete outcome data in Findling 2014. Further research may have an important impact on our confidence in the estimate of effect and may change the estimate.
*A small number of studies have evaluated the use of aripiprazole for ASD. Only one study examined aripiprazole at a duration longer than eight weeks. Future trials of aripiprazole in children/adolescents with ASD are likely to impact the estimates found in this review.
Background
Description of the condition
Before 2013, autism spectrum disorders (ASD) represented pervasive developmental disorders of variable severity, defined as autistic disorder, Asperger's disorder and pervasive developmental disorder ‐ not otherwise specified (PDD‐NOS) in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition ‐ Text Revision (DSM‐IV‐TR) (APA 2000), and as childhood autism, atypical autism, Rett's syndrome, other childhood disintegrative disorder, Asperger's syndrome, other pervasive developmental disorder and pervasive developmental disorder unspecified in the International Statistical Classification of Diseases and Related Health Problems, Tenth Edition (ICD‐10) (WHO 1994). The three characteristic manifestations of ASD are (1) impaired social interaction, (2) impaired communication and (3) restricted repetitive and stereotyped patterns of behaviour. Diagnostic criteria for ASD changed significantly with the release of the fifth edition of the DSM (DSM‐5) in 2013 (APA 2013). Autistic disorder, Asperger's disorder and PDD‐NOS were collapsed into a single diagnosis of ASD ‐ a single diagnosis with considerable diagnostic variability. The social and communication domains of ASD were combined, leaving two key symptom domains: (1) social communication and (2) restricted and repetitive behaviours.
As a result of symptom variability, clinicians are encouraged to describe diagnostic specifics in detail, in particular, intelligence and speech and language level. Kanner first described autism in 1943 through his observations of several afflicted children, noting their affinity for extreme aloneness and sameness, and their inability to form purposeful relationships with other people (Kanner 1943). Secondary characteristics, such as emotional and behavioural problems, are extremely common; examples of these include irritability, aggression, poor temper, self injury and injury to others (Lecavalier 2006). As no biomarkers have been established, the diagnosis of ASD is based on behavioural features.
Autism spectrum disorder is a lifelong condition. Individuals with ASD are frequently affected by other neuropsychiatric conditions as well, the most common of which are attention deficit hyperactivity disorder (ADHD), oppositional defiant disorder (ODD) and anxiety disorders (Simonoff 2008). Autism spectrum disorder is a neurodevelopmental disorder, but the exact genetic and environmental factors contributing to its cause are unknown. Boys are three to four times more likely to have ASD than girls, again suggesting the importance of genetics in the disorder.
Estimates of the prevalence of ASD vary. A systematic review of prevalence studies of ASD from 1966 to 2004 identified an overall estimate of prevalence of 7.1 per 10,000 for autism (95% confidence interval (CI) 1.6 to 30.6) and 20 per 10,000 (95% CI 4.9 to 82.1) for all ASD (Williams 2006). Variation in the prevalence estimate of typical autism has been significantly affected by the diagnostic criteria used, the age of children screened and study location. More recent prevalence studies have yielded higher estimates. The 2007 National Survey of Children's Health (N (sample size) = 78,037) found the weighted ASD point prevalence to be 110 per 10,000 in the United States (Kogan 2009). In a UK school‐based population study in the Special Educational Needs register, the prevalence estimate for ASD was 94 per 10,000 (Baron‐Cohen 2009). Most recently, a 2014 report by the Centers for Disease Control and Prevention (CDC) found the point prevalence of ASD to be 14.7 per 1000 eight‐year‐olds (CDC 2014). A systematic review found that the median worldwide prevalence of autistic disorder was 17 per 100,000, with a range of 2.8 to 94 per 100,000; the median worldwide prevalence of pervasive developmental disorder was 62 per 100,000, with a range of 1 to 189 per 100,00 (Elsabbagh 2012).
Both pharmacological and non‐pharmacological interventions are available for children and adults with ASD. Non‐pharmacological interventions include educational, behavioural and social communication strategies that are used alone or in combination as part of an individual plan to enhance learning and community participation. These interventions strive to improve communication, social skills, daily living skills, play and leisure skills, academic achievement and maladaptive behaviours (Meyers 2007).
Description of the intervention
Aripiprazole is a novel, atypical, antipsychotic drug with distinct mechanisms of action through its receptor binding profile. Typical antipsychotic medications, such as haloperidol, are potent antagonists at D₂‐dopamine receptors. Second‐generation antipsychotics, such as risperidone, are high‐affinity antagonists at D₂‐dopamine receptors and serotonin 5‐HT₂A receptors. Aripiprazole has functionally significant interactions at D₂, D₃ and D₄ dopamine receptors, and at 5‐HT₁A, 5‐HT₂A, 5‐HT₂B, 5‐HT₂C, 5‐HT₆ and 5‐HT₇ serotonin receptors. Aripiprazole is postulated to work by being a dopamine‐serotonin partial agonist, or by working through the mechanism of functional selectivity, whereby D₂ functional effects are dependent on the cellular location of the D₂ receptor (Shapiro 2003). The functional selectivity hypothesis proposes that depending upon the cellular milieu, a mixture of agonist, partial agonist and antagonist actions is likely. Thus, the unique and robust mechanism of aripiprazole lies in its ability to be a dopamine agonist when levels are too low, and a dopamine antagonist when levels are too high (Goodnick 2002).
What is known about other antipsychotic medications in ASD?
Both typical (first‐generation) and atypical (second‐generation) antipsychotics have been evaluated for the treatment of behavioural symptoms in individuals with ASD. Although short‐term randomised controlled trials (RCTs) suggest efficacy for improving some symptoms of ASD, important side effects limit their use. Typical antipsychotics have been associated with drug‐induced movement disorders. Haloperidol, for example, has been evaluated for the treatment of ASD in several trials and has been associated with improvements in withdrawal and stereotypies (Anderson 1989), as well as positive effects on learning (Campbell 1982); however, it has also been associated with extrapyramidal side effects such as acute dystonic reactions, withdrawal dyskinesias and tardive dyskinesia in this population (Campbell 1997). A systematic review of risperidone for ASD demonstrated efficacy of this medication in treating symptoms of aggression, irritability and repetitive behaviour; notable side effects included weight gain, increased appetite and sedation (Jesner 2009) .
How the intervention might work
Alterations in dopaminergic and serotonergic neurotransmission have been implicated in ASD, and abnormalities in these systems have been demonstrated through neuroimaging and metabolic studies (Posey 2008). As aripiprazole has affinity for both dopamine and serotonin receptors, it is likely to exert its action through mechanisms similar to those of other antipsychotic medications. When compared, the 5‐HT₂ antagonism of aripiprazole is higher than most atypical antipsychotics but lower than ziprasidone or risperidone; however its degree of antagonist activity, along with partial D₂ agonist activity, is at an optimal level, reducing the risk of extrapyramidal signs such as tardive dyskinesia (Goodnick 2002). Aripiprazole has moderate H₁ receptor affinity, which results in decreased sedation and risk of weight gain, compared with clozapine and olanzapine, which have high affinities at this receptor (Goodnick 2002).
Aripiprazole use in other disorders
Aripiprazole has been shown in a placebo‐controlled trial to be an effective intervention for positive and negative symptoms of schizophrenia, with a lower propensity to induce certain movement disorders, weight gain or sedation, or to increase cholesterol and prolactin levels, compared with drugs such as olanzapine or risperidone (Komossa 2009). Studies have shown that antipsychotic medications can cause increased weight gain and increased risk of type 2 diabetes in children and adolescents (Bobo 2013; Correll 2009). Aripiprazole was well tolerated in a placebo‐controlled trial of adolescents with schizophrenia, causing few side effects (Findling 2008). Another placebo‐controlled trial has shown its efficacy and tolerability in treating adolescents with bipolar I disorder or mixed episodes, with no significant weight changes compared with placebo (Findling 2009). The half‐life of aripiprazole of 72 hours allows once‐daily dosing and increased assurance of full absorption (Goodnick 2002).
Why it is important to do this review
This review updates a previous Cochrane review on the safety and efficacy of aripiprazole for individuals with ASD published in 2011 (Ching 2011). Aripiprazole currently has United States (US) Food and Drug Administration (FDA)‐labelled indications for the treatment of schizophrenia, bipolar disorder, major depressive disorder and autistic disorder (FDA 2010). Although several antipsychotics have demonstrated benefit in the treatment of behavioural symptoms of ASD, all currently available medication interventions have side effects that limit their use. As aripiprazole is a relatively new drug, it is important to understand both the efficacy and the side effects of this intervention in individuals with ASD. It is also important to determine whether intervention effects are dependent on factors such as age, length of intervention or medication dosage. A synthesis of available data on aripiprazole in ASD will be useful for clinicians considering use of this agent for people with ASD.
Objectives
To assess the safety and efficacy of aripiprazole as medication treatment for individuals with ASD.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs), including both parallel‐group and cross‐over designs, of any duration.
Types of participants
Children and adults with a clinical diagnosis of ASD made by an established classification system. Diagnosis of ASD includes individuals with autistic disorder, Asperger's disorder and pervasive developmental disorder ‐ not otherwise specified (PDD‐NOS).
Diagnosis of ASD in trial participants was corroborated by administration of a standardised instrument such as the Autism Diagnostic Interview ‐ Revised (ADI‐R) (Lord 1994).
Given the high rate of co‐morbidity between ASD and other neuropsychiatric disorders, we did not exclude individuals with co‐morbid disorders. However, we did exclude participants receiving co‐interventions such as other antipsychotics, psychostimulants, antidepressants or mood stabilisers. We did not exclude participants receiving non‐pharmacological therapy (i.e. behaviour therapy) provided it was equally accessible to all study participants, stable before trial entry and consistent throughout the study.
Types of interventions
Aripiprazole administered orally for ASD at any dosage compared with placebo.
Types of outcome measures
Primary outcomes
-
Emotional and behavioural symptoms, as measured by validated clinician‐ or parent‐reported scales.
Irritability (e.g. Aberrant Behaviour Checklist (ABC) ‐ Irritability subscale (Aman 1986)).
Hyperactivity (e.g. ABC ‐ Hyperactivity subscale (Aman 1986)).
Stereotypy (e.g. ABC ‐ Stereotypy subscale (Aman 1986)).
Inappropriate speech (e.g. ABC ‐ Inappropriate Speech subscale (Aman 1986)).
Lethargy/withdrawal (e.g. ABC ‐ Lethargy/Withdrawal subscale (Aman 1986)).
Aggression (e.g. Overt Aggression Scale (OAS) (Yudofsky 1986)).
Clinical Improvement (e.g. Clinical Global Impression (CGI) ‐ Improvement scale (Guy 1976)).
Extrapyramidal side effects*, as measured by scales such as the modified Webster Scale (mWS) (Webster 1968), the Abnormal Involuntary Movements Scale (AIMS) (Guy 1976) or the Barnes Akathisia Scale (BARS) (Barnes 1989).
Secondary outcomes
Obsessive‐compulsive behaviours as rated by, for example, the Children’s Yale‐Brown Obsessive Compulsive Scale (CY‐BOCS) (Goodman 1989).
Weight gain and metabolic side effects*.
Other side effects*, for example, somnolence, insomnia, headache and constipation.
We planned to synthesise results for the following time points: less than three months, three to six months and over six months. We were able to synthesise two trials that were eight weeks in duration and to describe, in detail, a discontinuation study of 16 weeks' duration.
*Please note, we use the term 'side effects' to describe any harms, adverse effects or adverse drug reactions associated with aripiprazole.
Search methods for identification of studies
Electronic searches
Searches for the original review were run in May 2011. We limited the search to 1990 onwards, as this is the year in which aripiprazole first became available. We applied no language restrictions. We ran searches for this update in November 2014 and again in October 2015, using the search strategies presented in Appendix 1. We have reported in Appendix 2 additional details about the searches, including exact search dates for each database. We searched the following databases.
Cochrane Central Register of Controlled Trials (CENTRAL; 2015, Issue 9; part of The Cochrane Library), which also contains the Cochrane Developmental, Psychosocial and Learning Problems Group Specialised Register.
Ovid MEDLINE (1946 to October Week 1 2015).
Embase (1980 to Week 41 2015; Ovid).
CINAHL Plus (1937 to current; EBSCOhost).
PsycINFO (1806 to October Week 1 2015; Ovid).
Cochrane Database of Systematic Reviews (CDSR; 2015, Issue 10; The Cochrane Library).
Database of Abstracts of Reviews of Effects (DARE; 2015, Issue 2; The Cochrane Library).
Conference Proceedings Citation Index ‐ Science (CPCI‐S; 1990 to current; Web of Science).
Autism Data (all available years).
ZETOC (limited to conference proceedings; all available years).
WorldCat (limited to theses and dissertations; all available years).
ClinicalTrials.gov (all available years).
World Health Organisation International Clinical Trials Registry Platform (WHO ICTRP; all available years).
Searching other resources
We contacted the drug company that makes aripiprazole to determine whether any trials were ongoing or results unpublished in this area.
Data collection and analysis
Selection of studies
For the initial review, two review authors (TP, HC) independently reviewed titles and abstracts obtained from the searches and selected potentially relevant studies. Two review authors (TP, LH) followed the same procedure for this update. We obtained full‐text articles and read them in detail to determine whether they fulfilled inclusion criteria. In the event of any dispute as to whether a study met the inclusion criteria, a discussion between review authors took place. We did not need to refer any disagreement to an independent arbiter.
Data extraction and management
Both review authors (TP and HC original; TP and LH update) independently extracted data from included studies and entered them onto a pre‐designed data extraction form. We extracted and entered the following data.
Study procedures, including recruitment, diagnosis, medication, dosage, duration and clinical setting.
Study design.
Method of randomisation.
Method of allocation concealment.
Blinding of participants, personnel and outcome assessors.
Inclusion and exclusion criteria for participants.
Number of participants.
Age distribution.
Gender.
Loss to follow‐up.
Premature discontinuation and reasons for such.
Outcomes.
Incomplete outcome data and selective outcome reporting.
Method of analysis.
Comparability of groups at baseline.
We compared extracted data to ensure accuracy, and we resolved discrepancies through discussion between review authors. One review author (TP) entered data into Review Manager (RevMan 2014), and the other (LH) checked the data for accuracy.
Assessment of risk of bias in included studies
Two review authors (original review: TP and HC; this update: TP and LH) independently assessed the risk of bias of each included study according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a). Review authors assessed each included study against the seven domains described below and assigned a rating of low risk of bias, high risk of bias or unclear risk of bias (uncertain risk of bias). When risk of bias was unclear, we sought additional information from the study authors. When the two review authors disagreed, we consulted the original paper until we were able to make a decision.
Random sequence generation
Description: The method by which participants were randomly allocated to different intervention groups is described in sufficient detail as to determine whether comparable groups were produced.
Review authors’ judgement: Was the allocation sequence adequately generated?
Allocation concealment
Description: The method by which participants were notified of intervention schedules is described in sufficient detail to assess whether such schedules could be foreseen in advance of, or during, recruitment.
Review authors’ judgement: Was allocation adequately concealed?
Blinding of participants and personnel
Description: Any measures taken to blind participants and personnel were described in sufficient detail to determine whether knowledge of intervention type was revealed at any point during the study.
Review authors’ judgement: Was blinding adequate during the study?
Blinding of outcome assessment
Description: Any measures taken to blind outcome assessors were described in sufficient detail to determine whether knowledge of intervention type was revealed at any point during the study.
Review authors’ judgement: Was blinding adequate during the study?
Incomplete outcome data
Description: Intention‐to‐treat analysis (analysis comparing participants in the groups to which they were originally randomly assigned versus complete outcome data available for all randomised participants) was included in each study. Review authors extracted and reported data on the distribution across intervention groups, on attrition and exclusion, on reasons for missed outcomes and on re‐inclusion in analyses.
Review authors’ judgement: Were incomplete study data dealt with adequately by study authors?
Selective outcome reporting
Description: We attempted to assess the possibility of selective outcome reporting by study authors. We checked study protocols through trial registries and compared outcomes listed in the protocol versus the published report. We then compared outcomes listed in the methods section of the manuscript versus those those listed in the results section. We also assessed and reported which studies collected data on a small number of key outcomes that are routinely measured.
Review authors’ judgement: Are included studies free of any possibility of selective outcome reporting?
Other sources of bias
Description: We investigated any possibility of potential threats to validity in the included studies. Possible sources included:
design‐specific risk of bias;
early stopping;
baseline imbalance;
inappropriate administration of a co‐intervention; and
use of an insensitive instrument to measure outcomes.
Review authors’ judgement: Are included studies free of other problems that could put the investigation at high risk of bias?
Measures of treatment effect
Binary data
We used risk ratio (RR) estimations with 95% CIs for binary outcomes.
Continuous data
For continuous outcomes, we used the mean difference (MD) to pool outcomes measured on the same scale across studies. We also performed an intention‐to‐treat analysis and included all randomised participants in the analysis, retained in the groups to which they were allocated. For additional methods to be used in future updates of this review, please see our protocol (Ching 2011) and Appendix 3.
Time‐to‐event data
We used hazard ratio (HR) estimations with 95% CIs for time‐to‐event outcomes.
Unit of analysis issues
We did not encounter any unit of analysis issues. Please see our protocol (Ching 2011) and Appendix 3 for methods that we will use to deal with these issues when we update this review.
Dealing with missing data
When data were missing, we first attempted to contact the study authors. Neither of the included studies reported standard deviations for data on the Aberrant Behavior Checklist (ABC) (Aman 1986), the Clinical Global Impression ‐ Severity (CGI‐S) scale (Guy 1976) and the Children’s Yale‐Brown Obsessive Compulsive Scale (CY‐BOCS) (Goodman 1989). Furthermore, although study authors responded to our requests for further information, they were not able to provide us with the standard deviations that we requested. Correspondence with study authors and a statistician allowed us to use statistical methods, when necessary, to back‐calculate missing data. Therefore, for Marcus 2009, we back‐calculated standard deviations from given standard errors. For Owen 2009, we back‐calculated standard deviations from given 95% CIs. We performed back‐calculations using the methods specified in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011b). We described missing data and dropouts for each study included in the review in the 'Risk of bias' tables (beneath the Characteristics of included studies tables).
Assessment of heterogeneity
We assessed methodological heterogeneity by comparing trial designs, and clinical heterogeneity by comparing the distribution of important participant factors such as age. We estimated heterogeneity through the DerSimonian and Laird method. We then assessed statistical heterogeneity by examining the I² statistic, an approximate quantity that describes the proportion of variation in point estimates that is due to heterogeneity of studies rather than to sampling error. In addition, we performed a Chi² test of homogeneity to determine the strength of evidence that heterogeneity is genuine. We examined I² and Chi² statistics in conjunction with one another because of the limitations of each statistic independently, especially considering the small number of studies included in this review. We used a significance level of 0.10 for the Chi² test. We also described tau², an estimate of between‐study variability, when presenting results of the random‐effects model.
Assessment of reporting biases
As we found only three studies, we did not assess reporting bias. See our protocol (Ching 2011) and Appendix 3 for methods to be used for future updates of this review.
Data synthesis
We performed a meta‐analysis of the data, using both fixed‐effect and random‐effects models, which we compared to assess statistical heterogeneity. We used Mantel‐Haenszel methods for RRs because of the rarity of these events, as the Mantel‐Haenszel weighting scheme is preferable with sparse data (Higgins 2011c). We analysed time‐to‐event data and MDs using inverse variance methods. We did not plan to combine trials with important differences in methods, inclusion criteria, participants and administration of medication (e.g. trials with only adult participants would not be combined with trials of only children; trials lasting two weeks would not be combined with trials lasting one year). When we were unable to perform a meta‐analysis, we described trial data with respect to the review's primary and secondary outcomes. When significant heterogeneity was present in the fixed‐effect model, we presented results from the random‐effects model.
Summary of findings
We created a 'Summary of findings' table, which includes the effect estimate, 95% CIs, number of participants and quality of evidence for major outcomes included in the review (ABC ‐ Irritability subscale, ABC ‐ Hyperactivity subscale, ABC ‐ Stereotypy subscale, weight gain, sedation, tremor, relapse rate). We used the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) method to assess the quality of the body of evidence for each outcome (Guyatt 2011). Although we considered RCTs to provide high‐quality evidence, we downgraded the level of evidence to moderate for all outcomes because of the presence of limitations in the design of available studies, and the overall small number of studies in this area. It is thus likely that further research could have an important impact on our confidence in the estimate of effect and may change the estimate.
Subgroup analysis and investigation of heterogeneity
As we found only two studies, we did not perform a subgroup analysis. See our protocol (Ching 2011) and Appendix 3 for methods to be used for future updates of this review.
Sensitivity analysis
As we found only two studies, we did not perform a sensitivity analysis. See our protocol (Ching 2011) and Appendix 3 for methods to be used for future updates of this review.
Results
Description of studies
See Characteristics of included studies and Characteristics of excluded studies.
Results of the search
In 2011, we found 1569 records, discarded the duplicates and screened 1323 titles and abstracts. We obtained and reviewed 14 full‐text reports. Two studies fitted our inclusion criteria of being randomised, placebo‐controlled, and double‐blinded trials (Marcus 2009; Owen 2009). We excluded the remaining 12 studies because they were review articles, pooled analyses, open‐label retrospective studies or case series studies (Ching 2012).
For this update, we ran searches in November 2014 and found 468 records. From these, we reviewed eight full‐text reports. We excluded seven of the eight studies (see Excluded studies) and included data from one new study in the update of this review (see Figure 1). The included study was an RCT investigating the safety and efficacy of long‐term maintenance treatment with aripiprazole in ASD (Findling 2014). We updated the searches again in October 2015. Among the 111 records found, we identified no eligible studies.
1.
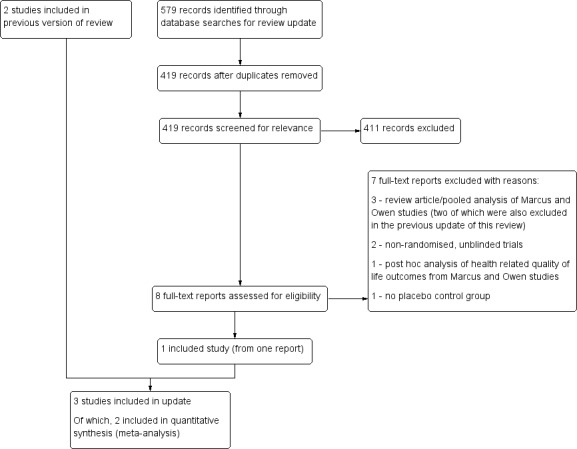
Study flow diagram.
We found no cluster‐randomised or cross‐over trials. Also, no studies conducted repeated observations on participants.
Included studies
See Characteristics of included studies tables.
Two studies included within this review were described as randomised, placebo‐controlled, double‐blinded trials; each lasted eight weeks (Marcus 2009; Owen 2009). The third study was a randomised, placebo‐controlled, double‐blinded relapse prevention trial, which included two phases (Findling 2014). Phase one ‐ the stabilisation phase ‐ consisted of 13 to 26 weeks of single‐blind aripiprazole, and phase two ‐ the randomisation phase ‐ consisted of up to 16 weeks of double‐blinded treatment with aripiprazole or placebo. Participants whose symptoms of irritability demonstrated a stable response to aripiprazole therapy for 12 consecutive weeks in phase one were eligible for randomisation into phase two.
Study location
All three studies were multi‐centre studies conducted in the United States (Findling 2014; Marcus 2009; Owen 2009).
Study participants
All participants in the studies were individuals (children or young people) younger than 18 years of age (age range six to 17 years) (Findling 2014; Marcus 2009; Owen 2009). Although the search was not restricted to children/adolescents, results of the search yielded appropriate studies involving only children/adolescents. Every child/adolescent had been diagnosed with autistic disorder. Both boys and girls were included and the number of children/adolescents ranged from 85 (Findling 2014) to 218 (Marcus 2009).
Study interventions and dosage
The intervention used was aripiprazole in several doses, ranging from 2 mg to 15 mg per day. In the Findling 2014 study, during phase one ‐ the stabilisation phase ‐ aripiprazole was flexibly dosed between 2 mg and 15 mg per day. During phase two ‐ the randomisation phase ‐ children/adolescents randomised to aripiprazole continued at the dose prescribed at the end of phase one.
Study outcomes
Primary outcomes
Emotional and behavioural symptoms
All three studies used the Aberrant Behaviour Checklist (ABC) to assess five categories of emotional and behavioural symptoms of ASD, notably, irritability, hyperactivity, stereotypy, inappropriate speech and lethargy/withdrawal. The ABC, developed by Aman 1986, consists of 58 items, organised within five subscales: irritability, hyperactivity, stereotypy, inappropriate speech and withdrawal/lethargy. Each item is scored on a scale from zero (not a problem) to three (severe). In interpreting results of this scale, a decreased score correlates with an improvement in the category, and an increased score correlates with a decline in that category. For example, the highest possible number of points for the irritability subscale is 45 (15 items × three points) and would depict the most severe case.
Studies by Marcus 2009 and Owen 2009 used the illness severity and global improvement subscales of the Clinical Global Impression (CGI) scale (Guy 1976) to measure clinical improvement. Illness severity is rated from one through seven, with one indicating normal, four moderately ill and seven most severely ill. Thus, a decrease in score for CGI‐S (severity) marks an improvement in disease state. Global improvement (illness change) is also rated from one through seven, with one meaning very much improved, four meaning no change and seven meaning very much worse. Thus, a decrease in score for CGI‐C (change) also marks an improvement in disease state.
The Findling 2014 relapse prevention trial evaluated time from randomisation to relapse of behavioural symptoms. Relapse was defined in one of the following ways.
Aberrant Behavior Checklist ‐ irritability (ABC‐I) score increase > 25% compared with end‐of‐phase one score, and Clinical Global Impressions ‐ Improvement (CGI‐I) rating of “much worse” or “very much worse” relative to the end of phase one, for two consecutive visits.
ABC‐I and CGI‐I scores as per definition above at one visit, plus “lost‐to‐follow‐up” at the next visit.
ABC‐I and CGI‐I scores as per definition above at one visit, plus initiation of a prohibited drug to treat worsening symptoms of irritability associated with autistic disorder at the next visit.
Child discontinued because of hospitalisation for worsening symptoms of irritability associated with autistic disorder or because of lack of efficacy based on the investigator's assessment.
Extrapyramidal side effects
All three studies used the Simpson Angus Scale (SAS) (Simpson 1970), the Abnormal Involuntary Movement Scale (AIMS) (Guy 1976) and the Barnes Akathisia Scale (BARS) (Barnes 1989) to measure extrapyramidal symptoms.
Secondary outcomes
Obsessive‐compulsive behaviours
Both Marcus 2009 and Owen 2009 used the Children's Yale‐Brown Obsessive Compulsive Scale (CY‐BOCS) (Scahill 1997) to assess obsessive‐compulsive behaviours. The CY‐BOCS is an adapted version of the Yale‐Brown Obsessive Compulsive Scale (Goodman 1989). It requires two informants ‐ child and parent ‐ to rate 10 items on a scale of zero to four. In general, a score of zero on each item shows no symptoms, and a score of four shows extreme symptoms (Scahill 1997); the total maximum score is 40. Therefore, as a higher number corresponds with greater severity of illness, a decrease in mean score on this particular scale shows improvement in symptoms. Both trials looked at the MD in scores between aripiprazole and placebo on these outcome scales.
Findling 2014 did not provide data related to this outcome.
Weight gain and metabolic side effects
The three studies also reported data on weight gain. As weight gain is a common occurrence for patients taking antipsychotic medications, more than one way of looking at this outcome was presented. Absolute weight gain in kilograms (kg) was presented in all studies, in addition to change in body mass index (BMI). Clinically relevant weight gain was defined in studies as an increase in weight of 7% or more of baseline body weight.
Other side effects
All three studies measured cholesterol, triglycerides and blood sugar. Studies also measured other side effects, including sedation, drooling and tremor.
Excluded studies
Overall, we excluded 19 out of 22 studies.
In the original review, we excluded 12 of 14 studies because they were review articles, pooled analyses, open‐label retrospective studies or case series studies (Ching 2011).
In this updated review, we excluded seven of eight studies: two because they used unblinded, non‐randomised, controlled study designs (D'Alessandro 2012, Maloney 2014), three because they were review articles or pooled analyses of the Marcus 2009 and Owen 2009 studies (Benton 2011; Douglas‐Hall 2011; Robb 2011), one randomised trial because it did not include a placebo control (Ghanizadeh 2014) and one study because it provided quality of life data (Varni 2012) from the two original studies included in our review (Marcus 2009; Owen 2009); however, this was not an outcome of interest in our review. Two of these studies were also excluded from the previous version of this review (Benton 2011; Robb 2011).
Risk of bias in included studies
See Figure 2 and 'Risk of bias' tables beneath the Characteristics of included studies tables.
2.
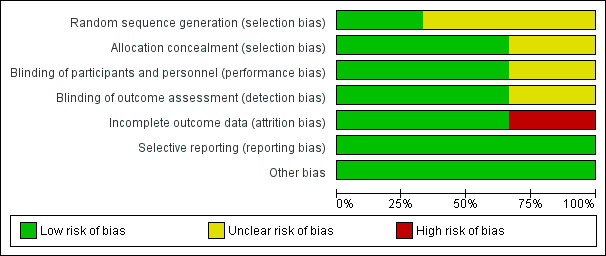
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Random sequence generation
In Findling 2014, eligible children/adolescents were randomly assigned (1:1) to placebo or aripiprazole (continued at the dose prescribed), but the randomisation sequence generation was not described in the manuscript. In Marcus 2009, children/adolescents were randomised to receive placebo or aripiprazole (5, 10 or 15 mg/d) in a 1:1:1:1 ratio, but the randomisation sequence generation was not described in the manuscript. We emailed each of the study authors for clarification but received no response. Consequently, we rated both of these studies as having unclear risk of selection bias. In Owen 2009, eligible children/adolescents were randomly assigned (1:1) to flexibly dosed aripiprazole or placebo according to a computer‐generated randomisation schedule prepared by Bristol‐Myers Squibb, using a permuted block design. We rated this study as having low risk of bias.
Allocation concealment
In Findling 2014, investigational sites accessed a centralised, call‐in system for randomisation. In Owen 2009, investigational sites accessed a call‐in, interactive voice response system when children/adolescents were ready to be randomly assigned. This system assigned a medication bottle number to each child/adolescent. We rated both of these studies as having low risk of bias in this domain. However, in Marcus 2009, allocation concealment was not described; thus it is unclear whether knowledge of assignment was adequately prevented.
Blinding
Performance bias
In all studies, children/adolescents were reported to be blinded to intervention type. We rated both Findling 2014 and Owen 2009 as having low risk of bias. For Marcus 2009, a double‐blind trial was described, but the study did not describe assurance of blinding, and so we rated this study as having unclear risk of bias.
Detection bias
In all studies, outcome assessors were reported to be blinded to intervention type. We rated both Findling 2014 and Owen 2009 as having low risk of bias. For Marcus 2009, a double‐blind trial was described, but the study did not describe assurance of blinding, and so we rated this study as having unclear risk of bias.
Incomplete outcome data
All studies gave details of attrition. Intention‐to‐treat analyses were performed in all three studies. Below, we describe missing data and dropouts for each study included in the review.
In Findling 2014, 19 out of 44 children/adolescents completed the placebo arm of the trial. Twenty‐five discontinued ‐ 23 because of lack of efficacy. Out of 41 children/adolescents, 22 completed the aripiprazole arm of the trial. Nineteen discontinued, 13 because of lack of efficacy, five withdrew consent and one was lost to follow‐up. We rated this study as having high risk of attrition bias. All study participants were included in the analysis of effect. If a participant dropped out of the study, investigators used the last observation carried forward (LOCF) method.
In Marcus 2009, 38 out of 52 children/adolescents completed the placebo arm of the trial. Fourteen discontinued for various reasons: lack of efficacy (n = 3), side effects (n = 4), withdrawal of consent (n = 2), loss to follow‐up (n = 3), non‐compliance (n = 1) and no longer meeting study criteria (n = 1). Out of 164, 140 children/adolescents completed the aripiprazole arm of the trial, whether 5 mg, 10 mg or 15 mg/d. In total, 26 discontinued for various reasons: side effects (n = 17), withdrawal of consent (n = 3), loss to follow‐up (n = 2), non‐compliance (n = 3) and other (n = 1). None discontinued because of lack of efficacy. The safety sample included all children/adolescents who took at least one dose of study medication, whereas the efficacy sample included all children/adolescents who had at least one post‐randomisation efficacy evaluation performed and compared with baseline values. Study authors performed a LOCF analysis for any child who discontinued. Despite the slightly higher percentage of dropouts in the aripiprazole arm, we rated this study as having low risk of attrition bias, as discontinuations due to side effects were generally higher in active treatment groups compared with placebo groups.
In Owen 2009, 36 out of 51 children/adolescents completed the placebo arm of the trial. Fifteen discontinued for various reasons: lack of efficacy (n = 6), side effects (n = 3), withdrawal of consent (n = 2) and loss to follow‐up (n = 4). Thirty‐nine out of 47 children/adolescents finished the aripiprazole arm of the trial. Eight discontinued for various reasons: lack of efficacy (n = 1), side effects (n = 5), withdrawal of consent (n = 1) and loss to follow‐up (n = 1). The safety sample included all but one child who was lost to follow‐up before entering the intervention phase. In the efficacy sample, two children were excluded (withdrawal of consent and side effects), as they did not complete a post‐baseline efficacy evaluation. We rated this study as having low risk of attrition bias.
Selective reporting
All three studies pre‐specified primary and secondary outcomes and reported expected measures of outcomes. Study protocols are available online at clinicaltrials.gov (NCT00332241, NCT00337571, NCT01227668); thus, we judged these studies to be at low risk of selective reporting bias.
Please see our protocol (Ching 2011) and Appendix 3 for additional methods that we would have used to assess small‐study effects had we identified 10 or more studies.
Other potential sources of bias
Although all three studies received funding from pharmaceutical companies, we did not judge this to be a matter of concern and thus rated all three studies as having low risk of bias.
Effects of interventions
See: Table 1
We were able to perform a meta‐analysis of data from Marcus 2009 and Owen 2009, as no important clinical heterogeneity was found. Furthermore, because both trials used the same measures and reported changes in scores and endpoint data in the same way, we were able to perform meta‐analyses for most of the outcomes listed below. The Findling 2014 trial had important differences in methods; therefore, we have described the results of this trial separately. For the study by Findling 2014, if a participant dropped out of the study, investigators used the LOCF method for their analysis.
We used both fixed‐effect and random‐effects models, which we then compared to assess statistical heterogeneity. Random‐effects and fixed‐effect models yielded nearly identical results in all analyses performed, with no difference greater than 0.1 point for any measure. Below, we present results from random‐effects models.
Minimal clinically important differences are not listed, as they are difficult to define because they vary depending on who is making the judgement and how severe underlying symptoms are determined to be. Thus, when combined with variation in our estimates (95% CIs), these differences will not lead to an accurate interpretation of study results. Instead, we have given information about the rating scales used, including maximum number of points possible, so that clinicians can make their own judgement as to whether the amount of change seen is clinically important.
Primary outcomes
Emotional and behavioral symptoms
Irritability
All three studies (Findling 2014; Marcus 2009; Owen 2009) assessed irritability using the ABC ‐ Irritability subscale (15 items yielding a maximum of 45 points) (Aman 1986).
A meta‐analysis of two studies (Marcus 2009; Owen 2009) yielded an MD of ‐6.17 points (change from baseline) between aripiprazole and placebo, in favour of aripiprazole (95% CI ‐9.07 to ‐3.26, tau² = 1.47, I² = 33%, P value < 0.00001, 308 children/adolescents, moderate‐quality evidence; Analysis 1.1).
1.1. Analysis.
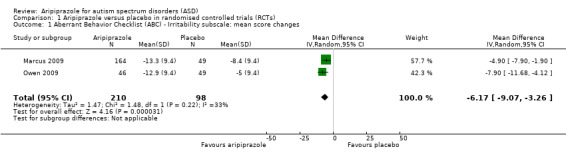
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 1 Aberrant Behavior Checklist (ABC) ‐ Irritability subscale: mean score changes.
Findling 2014 found no differences in scores between children/adolescents treated with aripiprazole and those treated with placebo from the end of phase one to week 16 of phase two.
Hyperactivity
All three studies (Findling 2014; Marcus 2009; Owen 2009) assessed hyperactivity using the ABC ‐ Hyperactivity subscale (16 items yielding a maximum of 48 points) (Aman 1986).
A meta‐analysis of two studies (Marcus 2009; Owen 2009) yielded an MD of ‐7.93 points (change from baseline) between aripiprazole and placebo, in favour of aripiprazole (95% CI ‐10.98 to ‐4.88, tau² = 2.27, I² = 44%, P value < 0.00001, 308 children/adolescents, moderate‐quality evidence; Analysis 1.2).
1.2. Analysis.
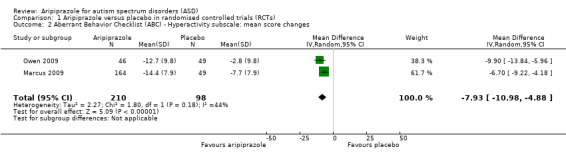
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 2 Aberrant Behavior Checklist (ABC) ‐ Hyperactivity subscale: mean score changes.
Findling 2014 reported differences in scores between children/adolescents treated with aripiprazole and those treated with placebo (MD ‐5.2, 95% CI ‐10.2 to ‐0.2, P value = 0.041, 85 children/adolescents).
Stereotypy
All three studies (Findling 2014; Marcus 2009; Owen 2009) assessed stereotypy using the ABC ‐ Stereotypy subscale (seven items yielding a maximum 21 points) (Aman 1986).
A meta‐analysis of two studies (Marcus 2009; Owen 2009) yielded an MD of ‐2.66 points (change from baseline) between aripiprazole and placebo, in favour of aripiprazole (95% CI ‐3.55 to ‐1.77, tau² = 0.00, I² = 0%, P value < 0.00001, 308 children/adolescents, moderate‐quality evidence; Analysis 1.3).
1.3. Analysis.
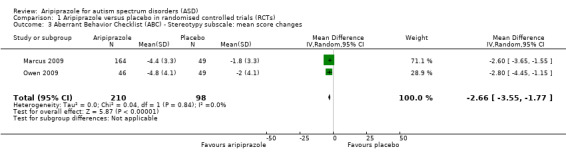
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 3 Aberrant Behavior Checklist (ABC) ‐ Stereotypy subscale: mean score changes.
Findling 2014 reported differences in scores between children/adolescents treated with aripiprazole and those treated with placebo (MD ‐2.0, 95% CI ‐3.70 to ‐0.40, P value = 0.018, 85 children/adolescents).
Inappropriate speech
All three studies (Findling 2014; Marcus 2009; Owen 2009) assessed inappropriate speech using the ABC ‐ Inappropriate Speech subscale (four items yielding a maximum 12 points) (Aman 1986).
A meta‐analysis of two studies yielded an MD of ‐1.43 points (change from baseline) between aripiprazole and placebo, in favour of aripiprazole (95% CI ‐2.60 to ‐0.27, tau² = 0.51, I² = 71%, P value = 0.02, 308 children/adolescents; Analysis 1.4).
1.4. Analysis.
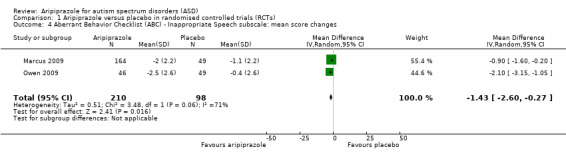
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 4 Aberrant Behavior Checklist (ABC) ‐ Inappropriate Speech subscale: mean score changes.
Findling 2014 reported differences in scores between children/adolescents treated with aripiprazole and those treated with placebo (MD ‐1.5, 95% CI ‐2.6, ‐0.3, P value = 0.013).
Lethargy/withdrawal
Marcus 2009 and Owen 2009 assessed lethargy/withdrawal using the lethargy/withdrawal subscale of the ABC (16 items yielding a maximum of 48 points) (Aman 1986). We combined these studies in a meta‐analysis. Results yielded an MD of ‐1.19 points (change from baseline) between aripiprazole and placebo, in favour of aripiprazole (95% CI ‐2.77 to 0.40, tau² = 0.00, I² = 0%, P value = 0.14, 308 children/adolescents; Analysis 1.5).
1.5. Analysis.
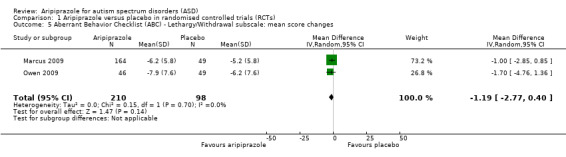
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 5 Aberrant Behavior Checklist (ABC) ‐ Lethargy/Withdrawal subscale: mean score changes.
Aggression
No studies provided data on this outcome.
Clinical improvement
All three studies (Findling 2014; Marcus 2009; Owen 2009) assessed severity using the CGI‐S subscale (Guy 1976). A meta‐analysis of two studies (Marcus 2009; Owen 2009) found an MD of ‐0.57 point (mean change from baseline) between aripiprazole and placebo, in favour of aripiprazole (95% CI ‐0.96 to ‐0.18, tau² = 0.05, I² = 63%, P value = 0.004, 308 children/adolescents; Analysis 1.6). Findling 2014 found no differences in scores between children treated with aripiprazole and those treated with placebo from the end of phase one to week 16 of phase two.
1.6. Analysis.
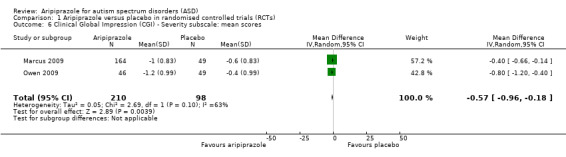
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 6 Clinical Global Impression (CGI) ‐ Severity subscale: mean scores.
Two studies (Marcus 2009; Owen 2009) assessed clinical improvement using the CGI‐I subscale (Guy 1976). A meta‐analysis of these studies yielded an MD of ‐1.33 points between aripiprazole and placebo, which approximates a one‐point change on the scale (of one to seven), in favour of aripiprazole (95% CI ‐1.75 to ‐0.92, tau² = 0.00, I² = 0%, P value < 0.00001, 308 children/adolescents; Analysis 1.7).
1.7. Analysis.
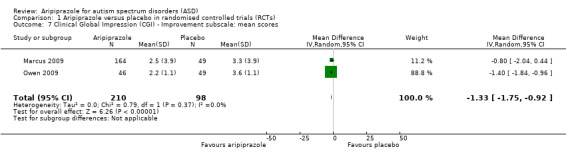
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 7 Clinical Global Impression (CGI) ‐ Improvement subscale: mean scores.
Findling 2014 reported no differences between aripiprazole and placebo for the primary endpoint ‐ time from randomisation to relapse (P value = 0.097). Kaplan‐Meier relapse rates at week 16 were 35% for aripiprazole and 52% for placebo, for a hazard ratio (aripiprazole/placebo) of 0.57 (95% CI 0.28 to 1.12, low‐quality evidence). A treatment‐by‐race interaction was explored and was found (P value = 0.034). Among white children/adolescents (n = 59), aripiprazole treatment resulted in a lower relapse rate (25.8%) than placebo (60.7%), with a hazard ratio of 0.33 (95% CI 0.14 to 0.78, P value = 0.011), whereas among non‐white children/adolescents (n = 26), the two treatment arms did not differ. An age‐interaction test found no evidence of an age interaction.
Extrapyramidal side effects
Extrapyramidal side effects are adverse, movement‐related symptoms, which include drug‐induced parkinsonism, dystonia, akathisia and tardive dyskinesia.
A meta‐analysis of two studies (Marcus 2009; Owen 2009) found no difference in rates of extrapyramidal symptom events among children/adolescents treated with aripiprazole compared with placebo (RR 1.89, 95% CI 0.98 to 3.66, tau² = 0.00, I² = 0%, P value = 0.06, 313 children/adolescents; Analysis 1.8). The result may not have reached statistical significance because the analysis lacked power with only two included studies. We were not able to perform a meta‐analysis on extrapyramidal side effects, as neither study provided standard deviations, standard errors or CIs for data from SAS (Simpson 1970), AIMS (Guy 1976) and BARS (Barnes 1989). Owen 2009 did not find differences between intervention groups with respect to mean change from baseline on these three measures. Marcus 2009 reported no differences between placebo‐ and aripiprazole‐treated children/adolescents in the mean change from baseline on BARS. On SAS, children/adolescents treated with a 10 mg dose of aripiprazole had significantly greater change from baseline (+ 0.7) compared with placebo‐treated children/adolescents (‐0.4) (P value = 0.006). Marcus 2009 also reported a significant change from baseline on the AIMS in all aripiprazole‐treated children/adolescents compared with placebo‐treated children/adolescents. Children/adolescents taking aripiprazole showed a decrease in scores (‐0.1 to ‐0.2 points) compared with placebo‐treated children/adolescents, who had an increase in score of 0.2 points (P value < 0.05).
1.8. Analysis.
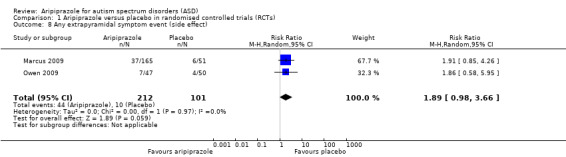
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 8 Any extrapyramidal symptom event (side effect).
Findling 2014, in phase one (the single‐blind phase), reported that 27 children/adolescents (17.4%) had treatment‐emergent extrapyramidal symptom‐related side effects. Extrapyramidal symptom‐related side effects occurred in 7.7% of children/adolescents treated with aripiprazole and in 7% of children/adolescents treated with placebo. Investigators reported no differences between groups on SAS, AIMS and BARS. Movement disorders were also common in phase two (5.1% for aripiprazole versus 0% for placebo).
Secondary outcomes
Obsessive‐compulsive behaviours
Two studies (Marcus 2009; Owen 2009) used the Children's Yale‐Brown Obsessive Compulsive Scale (CY‐BOCS) (Scahill 1997) to assess obsessive‐compulsive behaviours in 308 children/adolescents. We combined these studies in a meta‐analysis (Analysis 1.9). Results yielded an MD of ‐1.93 points (mean change from baseline) between aripiprazole and placebo, in favour of aripiprazole (95% CI ‐3.86 to 0.00, tau² = 1.65, I² = 84%, P value = 0.05).
1.9. Analysis.
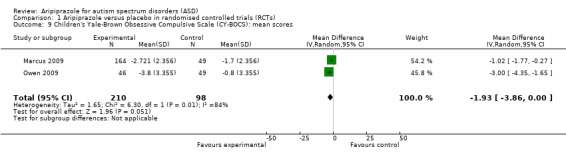
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 9 Children's Yale‐Brown Obsessive Compulsive Scale (CY‐BOCS): mean scores.
Weight gain and metabolic side effects
In a meta‐analysis of two studies (Marcus 2009; Owen 2009), the RR of clinically relevant weight gain while taking aripiprazole was approximately 3.78 kg compared with placebo (95% CI 1.78 to 8.02, tau² = 0.00, I² = 0%, P value = 0.0005, 308 children/adolescents; Analysis 1.10). The MD in weight gain between the aripiprazole group and the placebo group was 1.13 kg (95% CI 0.71 to 1.54, tau² = 0.00, I² = 0%, P value < 0.00001, two studies, 308 children/adolescents, moderate‐quality evidence; Analysis 1.11). We noted no difference between study groups as regards change in body mass index (BMI) (MD 0.44, 95% CI ‐0.27 to 1.16, tau² = 0.00, I² = 0%, P value = 0.22, two studies, 313 children/adolescents; Analysis 1.12). Both Marcus 2009 and Owen 2009 (313 children/adolescents) reported no differences in rates of abnormal triglycerides between children/adolescents treated with placebo and those treated with aripiprazole (Analysis 1.13), nor in low‐density lipoprotein (Analysis 1.14), high‐density lipoprotein (Analysis 1.15) or blood sugar (Analysis 1.16).
1.10. Analysis.
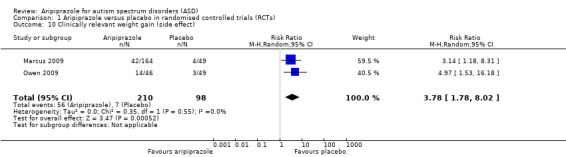
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 10 Clinically relevant weight gain (side effect).
1.11. Analysis.
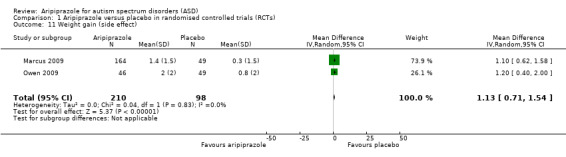
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 11 Weight gain (side effect).
1.12. Analysis.
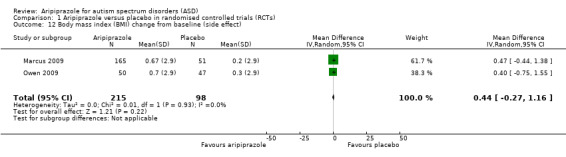
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 12 Body mass index (BMI) change from baseline (side effect).
1.13. Analysis.
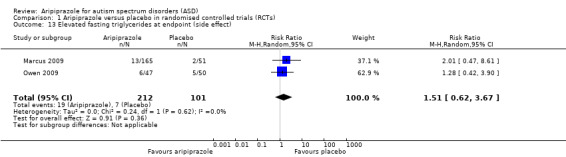
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 13 Elevated fasting triglycerides at endpoint (side effect).
1.14. Analysis.
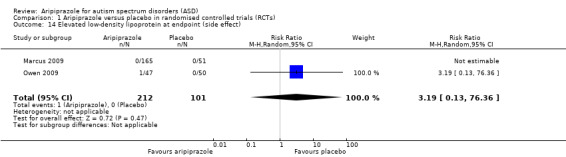
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 14 Elevated low‐density lipoprotein at endpoint (side effect).
1.15. Analysis.
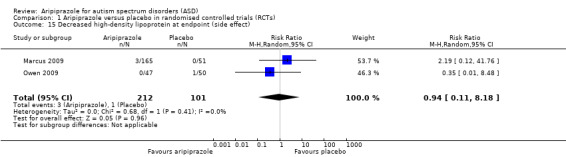
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 15 Decreased high‐density lipoprotein at endpoint (side effect).
1.16. Analysis.
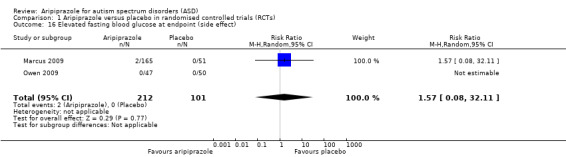
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 16 Elevated fasting blood glucose at endpoint (side effect).
Findling 2014 reported an increase of 25.2% in weight in phase one (all children/adolescents took aripiprazole during phase one). At week 16 of phase two, children/adolescents treated with aripiprazole gained a mean of 2.2 kg and placebo recipients gained 0.6 kg. Investigators reported no changes on metabolic laboratory tests (cholesterol, triglycerides and glucose) from baseline to week 16, during phase two, between children/adolescents treated with aripiprazole and those treated with placebo.
Other side effects
For the two studies included in the meta‐analysis (Marcus 2009; Owen 2009), we chose clinically relevant effects of concern, such as sedation, drooling and tremor. Such side effects were common in the aripiprazole group. In comparison with the control group, the RR of experiencing sedation was 4.28 times more likely if taking aripiprazole (95% CI 1.58 to 11.60, tau² = 0.00, I² = 0%, P value = 0.004, two studies, 313 children/adolescents, moderate‐quality evidence; Analysis 1.17). A person was 9.64 times more likely to experience drooling if taking aripiprazole (95% CI 1.29 to 72.10, tau² = 0.000, I² = 0%, P value = 0.03, two studies, 313 children/adolescents; Analysis 1.18) and was 10.26 times more likely to experience tremor (95% CI 1.37 to 76.63, tau² = 0.00, I² = 0%, P value = 0.02, two studies, 313 children/adolescents, moderate‐quality evidence; Analysis 1.19) compared with placebo.
1.17. Analysis.
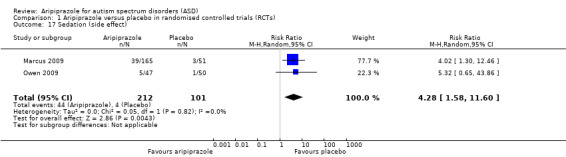
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 17 Sedation (side effect).
1.18. Analysis.
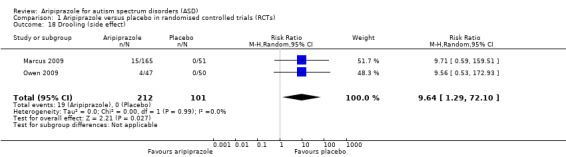
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 18 Drooling (side effect).
1.19. Analysis.
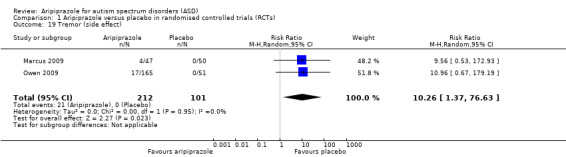
Comparison 1 Aripiprazole versus placebo in randomised controlled trials (RCTs), Outcome 19 Tremor (side effect).
Findling 2014 reported that somnolence (14.8%) and vomiting (14.2%) were common side effects in phase one (all children/adolescents treated with aripiprazole during phase one), and in phase two, the most common side effects with aripiprazole were upper respiratory tract infection (10.3% for aripiprazole versus 2.3% for placebo) and constipation (5.1% for aripiprazole versus 0% for placebo).
Discussion
Summary of main results
Both short‐term studies showed that aripiprazole can improve some symptoms of autism spectrum disorders (ASD). From these results, we can suggest that aripiprazole appears effective for the short‐term medication intervention of children/adolescents with ASD. Several significant results point towards efficacy of aripiprazole as a short‐term medication intervention for children/adolescents with ASD. Most of the primary outcomes specified were significantly better with aripiprazole as compared with placebo intervention. These primary outcomes, as stated earlier in the Types of outcome measures section, include score changes on the Aberrant Behaviour Checklist (ABC) (Aman 1986) and Clinical Global Impression (CGI) scales (Guy 1976).
Meta‐analysis of mean changes in scores on the ABC ‐ Irritability subscale and the CGI ‐ Improvement scale from both Marcus 2009 and Owen 2009 shows efficacy of aripiprazole in treating this behavioural symptom (see Analysis 1.1 and Analysis 1.7). Significant improvements also occurred in the hyperactivity and stereotypy subscales of the ABC. Changes on remaining ABC subscales pertaining to social withdrawal and inappropriate speech were not expected, as no evidence suggests that antipsychotic therapy is helpful in treating the core social and communication impairments of ASD. The magnitude of change on the ABC ‐ Irritability subscale was 6.17 points with aripiprazole relative to placebo. With mean baseline scores in the study group ranging from 25 to 30 out of a total of 45 points on this scale, a six‐point reduction in symptoms may be considered clinically meaningful by caregivers. Similarly, for the ABC ‐ Hyperactivity subscale, the magnitude of change was 7.93 points with aripiprazole relative to placebo, with baseline scores in the study group on this subscale ranging from 30 to 35 out of a total of 48 points. This change in hyperactivity score may be clinically meaningful for caregivers. Changes in stereotypy scores were more modest, with a decrease of 2.66 points with aripiprazole relative to placebo. Stereotypy subscale baseline scores ranged from 10 to 12 among study groups at baseline, out of a total of 21 points.
Secondary outcomes included results from the Children's Yale‐Brown Obsessive Compulsive Scale (CY‐BOCS) (Scahill 1997), metabolic side effects such as weight gain, extrapyramidal symptoms and other side effects such as sedation, drooling and tremor. We noted no improvement in obsessive‐compulsive behaviours. Multiple children/adolescents in the aripiprazole group experienced side effects compared with those in the placebo group. Evidence was consistent for both an increase and a decrease in extrapyramidal symptoms. Risk of experiencing side effects of sedation, drooling and tremor was higher if treated with aripiprazole. Individuals treated with aripiprazole gained more weight relative to placebo, and clinically significant weight gain was more likely to occur if treated with aripiprazole than placebo.
The Findling 2014 relapse prevention trial found no difference between aripiprazole and placebo during maintenance treatment (P value = 0.097). However, evidence showed a treatment‐by‐race relationship (P value = 0.034), wherein white children/adolescents demonstrated lower relapse rates on aripiprazole than placebo, although no difference was noted between non‐white children/adolescents. These results suggest that some children/adolescents may benefit from continued use of aripiprazole, and others may not. For secondary endpoints, the most clinically important effect observed was a deterioration in scores on the ABC ‐ Hyperactivity subscale, among children/adolescents treated with placebo compared with aripiprazole. Greater weight gain and increased movement disorders were associated with continued aripiprazole. In combination with results from Marcus 2009 and Owen 2009, it is suggested that children/adolescents taking aripiprazole should be re‐evaluated periodically to determine whether aripiprazole remains appropriate for treatment of ASD symptoms.
Overall completeness and applicability of evidence
Although the two short‐term use studies are complete in their reporting, and provide highly applicable findings, world literature on the use of aripiprazole for ASD is small. Only one long‐term use study has been conducted and is at high risk of bias due to attrition. Short‐term use studies found clinically important moderate improvements in irritability and hyperactivity, and small improvements in stereotypies, with aripiprazole compared with placebo. This review aimed to determine the safety and efficacy of aripiprazole for any ASD, but data were available only on children/adolescents with a diagnosis of autistic disorder, and failed to include those with Asperger's syndrome or pervasive developmental disorders ‐ not otherwise specified (PDD‐NOS), or adults with ASD. Although classification of these disorders changed in 2013, studies included only those at the most severe end of the spectrum. Data from a 14‐week open‐label study of aripiprazole, which was not eligible for inclusion (Stigler 2009), provided information on participants with Asperger's syndrome and PDD‐NOS and found similar trends of efficacy as the studies included in this review. Furthermore, all included studies were performed in the United States and were sponsored by pharmaceutical companies.
No trials examined the specific link between medication and behavioural interventions. Trials that include behavioural interventions and the addition of medication for families in crisis, or with behavioural interventions that are not sufficient, would provide the most applicable evidence related to current guidelines for treatment of ASD.
One study, which did not meet our inclusion criteria for the review, provided information on comparative efficacy of aripiprazole. Ghanizadeh 2014 randomised 59 children/adolescents with ASD to risperidone or aripiprazole twice daily. Investigators assessed outcomes using the ABC (Aman 1986), the CGI ‐ Improvement scale (Guy 1976) and systematic examination for extrapyramidal symptoms and other side effects. Both aripiprazole and risperidone decreased all ABC subscale scores significantly (P value < 0.05), but no significant difference between intervention groups was evident. Researchers also reported no difference between intervention groups on the CGI‐I subscale scores at endpoint. Both interventions were well tolerated, and the most common side effects were increased appetite, drooling and drowsiness. One child from each intervention arm withdrew because of side effects. Therefore, this study found that aripiprazole and risperidone show similar efficacy and side effects for treatment of ASD symptoms in children/adolescents.
Another study that did not meet our inclusion criteria for the review provided information on the impact of aripiprazole on quality of life. In a post hoc analysis of data from Marcus 2009 and Owen 2009, Varni 2012 evaluated the effects of use of aripiprazole in children/adolescents with ASD on health‐related quality of life (HRQoL). A total of 316 children/adolescents were randomised to aripiprazole or placebo and were evaluated at baseline and at eight weeks by means of three Pediatric Quality of Life Inventory (PedsQL) scales (Varni 1999). Aripiprazole was associated with greater improvement in the PedsQL combined scale total score (MD 7.8, 95% CI 3.8 to 11.8, P value < 0.001), and in all three PedsQL scales (emotional functioning: MD 7.8, 95% CI 3.4 to 12.2, P value < 0.05; social functioning: MD 6.2, 95% CI 0.7 to 11.8, P value < 0.05; and cognitive functioning: MD 9.3, 95% CI 3.8 to 14.9; P value < 0.05). These findings suggest that short‐term treatment with aripiprazole is associated with increased HRQoL in children/adolescents with ASD.
Quality of the evidence
The quality of studies performed on the use of aripiprazole in ASD was moderate. We rated quality as moderate because of unclear risk of bias for some domains in Marcus 2009 and Owen 2009, and because of the overall small number of studies conducted on the use of aripiprazole in ASD. We rated quality of evidence for long‐term trials as low because risk of attrition bias for incomplete outcome data was high in Findling 2014. Further research may have an important impact on our confidence in the estimate of effect and may change the estimate.
Potential biases in the review process
We have no other potential biases to report in the review process. Although we have synthesised all existing RCTs of aripiprazole for the treatment of behavioural symptoms in ASD, it must be recognised that available evidence is limited.
Agreements and disagreements with other studies or reviews
No other formal systematic reviews on use of aripiprazole for the treatment of ASD have been published to our knowledge. A pooled analysis of data on side effects from Marcus 2009 and Owen 2009 has been published (Robb 2011). Results and conclusions of our study with respect to side effects of aripiprazole are similar to those provided by Robb and colleagues.
Authors' conclusions
Implications for practice.
Evidence from this review shows that use of aripiprazole for the short‐term treatment of irritability in children/adolescents with ASD may be worth considering. If the decision is made to use aripiprazole, clinicians should follow established best practice and provide information about side effects such as weight gain, tremor, drooling and sedation to children/adolescents and their families, so they can consider the benefits and risks of treatment before commencing a medication trial. Children/adolescents undergoing a trial of therapy with aripiprazole should be monitored for clinical effectiveness of the medication, as well as for side effects. In the absence of high‐quality evidence, and given that similar relapse rates are observed for both aripiprazole and placebo, evidence suggests that the use of aripiprazole should be re‐evaluated periodically for continued efficacy, and that it might be appropriate to consider discontinuation of aripiprazole after successful treatment for 12 weeks.
Implications for research.
Additional trials should be conducted to investigate use of aripiprazole versus placebo for longer than three months. Only one trial compared aripiprazole head‐to‐head with another medication, risperidone. Future trials comparing aripiprazole versus other medications should be conducted to improve our understanding of the efficacy and safety of aripiprazole relative to other pharmacological interventions. Trials of these medications in older individuals with continuing symptoms should also be performed. Furthermore, trials that use behavioural interventions as a first‐line approach and medication interventions as an adjunct should be performed. Future reviews should include health‐related quality of life as an outcome measure.
What's new
| Date | Event | Description |
|---|---|---|
| 15 May 2015 | New citation required but conclusions have not changed | We found a new study that evaluates risk of relapse after discontinuation of aripiprazole once symptoms have improved during treatment |
| 20 November 2014 | New search has been performed | We updated the review following a new search in November 2014 and a top‐up search in October 2015 |
Acknowledgements
The review authors wish to acknowledge the Departments of Clinical Neurosciences and Pediatrics, at the University of Calgary, and the Cochrane Developmental, Psychosocial and Learning Problems Group.
Appendices
Appendix 1. Search strategies
Cochrane Central Register of Controlled Trials (CENTRAL; part of The Cochrane Library)
#1MeSH descriptor Antipsychotic Agents, this term only #2aripiprazol* or abilify or abilitat #3atypical Near/3 antipsychotic* #4(#1 OR #2 OR #3) #5MeSH descriptor Child Development Disorders, Pervasive explode all trees #6asperger* #7autis* or ASD or ASDs #8kanner* #9rett* #10childhood near/3 schizophren* #11(pervasiv* NEXT development* NEXT disorder*) OR PDD or PDDs #12MeSH descriptor Social Behavior Disorders, this term only #13MeSH descriptor Child Behavior Disorders, this term only #14MeSH descriptor Speech Disorders, this term only #15MeSH descriptor Language Development Disorders, this term only #16(speech or language) near/3 (disorder* or delay*) #17MeSH descriptor Communication Disorders, this term only #18(behav* or communicat*) NEXT (disorder* or impair*) #19(#5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18) #20(#4 AND #19)
Ovid MEDLINE
1 ( aripiprazol$ or abilify or abilitat).mp. 2 (atypical adj3 antipsychotic$).mp. 3 antipsychotic agents/ 4 or/1‐3 5 exp Child Development Disorders, Pervasive/ 6 asperger$.tw. 7 (autis$ or ASD or ASDs).tw. 8 kanner$.tw. 9 rett$.tw. 10 (childhood adj3 schizophren$).tw. 11 (pervasive development$ disorder$ or PDD or PDDs).tw. 12 Social Behavior Disorders/ 13 Child Behavior Disorders/ 14 speech disorders/ 15 language development disorders/ 16 ((speech or language) adj3 (delay$ or disorder$)).tw. 17 Communication Disorders/ 18 ((behav$ or communicat$) adj (disorder$ or impair$)).tw. 19 or/5‐18 20 randomised controlled trial.pt. 21 controlled clinical trial.pt. 22 randomi#ed.ab. 23 placebo$.ab. 24 drug therapy.fs. 25 randomly.ab. 26 trial.ab. 27 groups.ab. 28 or/20‐27 29 exp animals/ not humans.sh. 30 28 not 29 31 4 and 19 and 30
Embase (Ovid)
1 aripiprazole/ 2 (aripiprazol$ or abilify or abilitat).mp. 3 atypical antipsychotic agent/ 4 (atypical adj3 antipsychotic$).mp. 5 or/1‐4 6 exp autism/ 7 asperger$.tw. 8 (autis$ or ASD or ASDs).tw. 9 kanner$.tw. 10 rett$.tw. 11 (childhood adj3 schizophren$).tw. 12 (pervasive development$ disorder$ or PDD or PDDs).tw. 13 sociopathy/ 14 behavior disorder/ 15 speech disorder/ 16 language disability/ 17 ((speech or language) adj3 (delay$ or disorder$)).tw. 18 communication disorder/ 19 ((behav$ or communicat$) adj (disorder$ or impair$)).tw. 20 or/6‐19 21 exp Clinical trial/ 22 Randomization/ 23 Single blind procedure/ 24 Double blind procedure/ 25 Crossover procedure/ 26 Placebo/ 27 Randomi#ed.tw. 28 RCT.tw. 29 (random$ adj3 (allocat$ or assign$)).tw. 30 randomly.ab. 31 groups.ab. 32 trial.ab. 33 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw. 34 Placebo$.tw. 35 Prospective study/ 36 (crossover or cross‐over).tw. 37 prospective.tw. 38 or/21‐37 39 5 and 20 and 38
CINAHL Plus: Cumulative Index to Nursing and Allied Health Literature (EBSCOhost)
S39 S18 and S23 and S38 S38 S24 or S25 or S26 or S27 or S28 or S29 or S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 S37 TI (evaluat* study or evaluat* research) or AB (evaluate* study or evaluat* research) or TI (effectiv* study or effectiv* research) or AB (effectiv* study or effectiv* research) OR TI (prospectiv* study or prospectiv* research) or AB(prospectiv* study or prospectiv* research) or TI (follow‐up study or follow‐up research) or AB (follow‐up study or follow‐up research) S36 "cross over*" S35 crossover* S34 (MH "Crossover Design") S33 (tripl* N3 mask*) or (tripl* N3 blind*) S32 (trebl* N3 mask*) or (trebl* N3 blind*) S31 (doubl* N3 mask*) or (doubl* N3 blind*) S30 (singl* N3 mask*) or (singl* N3 blind*) S29 (clinic* N3 trial*) or (control* N3 trial*) S28 (random* N3 allocat* ) or (random* N3 assign*) S27 randomis* or randomiz* S26 (MH "Meta Analysis") S25 (MH "Clinical Trials+") S24 MH random assignment S23 S19 or S20 or S21 or S22 S22 atypical N3 antipsychotic* S21 (MH "Antipsychotic Agents") S20 Aripiprazol* or abilify or abilitat S19 (MH "Aripiprazole") S18 (S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11 or S12 or S13 or S14 or S15 or S16 or S17) S17 TI (speech N3 delay*) or TI (speech N3 disorder*) or AB (speech N3 delay*) or AB (speech N3 disorder*) S16 TI (language N3 delay*) or TI (language N3 disorder*) or AB (language N3 delay*) or AB (language N3 disorder*) S15 TI (communicat* disorder*) or TI (communicat* impair*) S14 AB (communicat* disorder*) or AB (communicat* impair*) S13 AB (behav* disorder*) or AB (behav* impair*) S12 TI (behav* disorder*) or TI (behav* impair*) S11 (MH "Speech Disorders") S10 (MH "Language Disorders") S9 (MH "Communicative Disorders") S8 TI(childhood schizophrenia) or AB(childhood schizophrenia) S7 TI(Kanner*) or AB (Kanner*) S6 TI (Rett* ) or AB (Rett*) S5 TI (Asperger* ) or AB (Asperger*) S4 TI (autis* or ASD or ASDs) or AB (autis* or ASD or ASDs) S3 AB (pervasive development* disorder* or PDD or PDDs) S2 TI (pervasive development* disorder* or PDD or PDDs) S1 (MH "Child Development Disorders, Pervasive+")
PsycINFO
PsycINFO (Ovid) was searched from 2014 onwards for the review update
1 exp pervasive developmental disorders/ 2 Developmental disabilities/ 3 pervasive development$ disorder$.tw. 4 (pervasive adj3 child$).tw. 5 autis$.tw. 6 asperger$.tw. 7 (autis$ or ASD or ASDs).tw. 8 (ASD or ASDs or PDD or PDDs).tw. 9 Rett$.tw. 10 Kanner$.tw. 11 or/1‐10 12 aripiprazole/ 13 Neuroleptic Drugs/ 14 (atypical adj3 (antipsychotic$ or anti‐psychotic$)).tw. 15 aripiprazol$.tw. 16 Abilify.tw. 17 Abilitat.tw. 18 (second generation adj (antipsychotic$ or anti‐psychotic$)).tw. 19 or/12‐18 20 clinical trials/ 21 random$.tw. 22 ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).tw. 23 (crossover$ or "cross over$").tw. 24 trial$.tw. 25 group$.ab. 26 control.ab. 27 exp program evaluation/ 28 treatment effectiveness evaluation/ 29 treatment outcome clinical trial.md. 30 ((effectiveness or evaluat$) adj3 (stud$ or research$)).tw. 31 (allocat$ or assign$).tw. 32 placebo.ab. 33 or/20‐32 34 11 and 19 and 33
PsycINFO (EBSCOhost) was searched in 2011 for the original review
S41 S21 and S26 and S40 S40 S27 or S28 or S29 or S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 or S38 or S39 S39 (evaluation N3 stud* or evaluation N3 research*) S38 (effectiveness N3 stud* or effectiveness N3 research*) S37 DE "Placebo" or DE "Evaluation" or DE "Program Evaluation" OR DE "Educational Program Evaluation" OR DE "Mental Health Program Evaluation" S36 (DE "Random Sampling" or DE "Clinical Trials") or (DE "Experiment Controls") S35 "cross over*" S34 crossover* S33 (tripl* N3 mask*) or (tripl* N3 blind*) S32 (trebl* N3 mask*) or (trebl* N3 blind*) S31 (doubl* N3 mask*) or (doubl* N3 blind*) S30 (singl* N3 mask*) or (singl* N3 blind*) S29 (clinic* N3 trial*) or (control* N3 trial*) S28 (random* N3 allocat* ) or (random* N3 assign*) S27 randomis* or randomiz* S26 S22 or S23 or S24 or S25 S25 (atypical N3 antipsychotic*) S24 DE "Neuroleptic Drugs" S23 (aripiprazol* or abilify or abilitat S22 DE "Aripiprazole" S21 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11 or S12 or S13 or S14 or S15 or S16 or S17 or S18 or S19 or S20 S20 TI (speech N3 disorder*) Or TI (speech N3 delay*) S19 AB (speech N3 disorder*) Or Ab (speech N3 delay*) S18 AB (language N3 disorder*) Or Ab (language N3 delay*) S17 TI (language N3 disorder*) Or TI (language N3 delay*) S16 TI(communicat* disorder*) or TI (communicat* impair*) S15 AB (communicat* disorder*) or AB (communicat* impair*) S14 AB (behav* disorder*) or AB (behav* impair*) S13 TI (behav* disorder*) or TI (behav* impair*) S12 DE "Behavior Disorders" S11 DE "Language Disorders" OR DE "Language Delay" S10 DE "Speech Disorders" S9 DE "Communication Disorders" S8 TI(childhood schizophrenia) or AB(childhood schizophrenia) S7 TI(Kanner*) or AB (Kanner*) S6 TI (Rett* ) or AB (Rett*) S5 TI (Asperger* ) or AB (Asperger*) S4 TI (autis* ) or AB (autis*) S3 TI (pervasive development* disorder* or PDD or PDDs) S2 AB (pervasive development* disorder* or PDD or PDDs) S1 DE "Pervasive Developmental Disorders" OR DE "Pervasive Developmental Disorders" OR DE "Aspergers Syndrome" OR DE "Autism" OR DE "Rett Syndrome"
Cochrane Database of Systematic Reviews (CDSR; part of The Cochrane Library)
#1MeSH descriptor: [Antipsychotic Agents] this term only #2(aripiprazol* or abilify or abilitat):ti,ab #3(atypical near/3 (antipsychotic* or anti‐psychotic*)):ti,ab #4#1 or #2 or #3 #5MeSH descriptor: [Child Development Disorders, Pervasive] explode all trees #6MeSH descriptor: [Developmental Disabilities] this term only #7asperger*:ti,ab #8(autis* or ASD or ASDs):ti,ab #9kanner*:ti,ab #10rett*:ti,ab #11(childhood near/3 schizophren*):ti,ab #12(pervasiv* next development* next disorder* or PDD or PDDs):ti,ab #13#5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 #14#4 and #13
Database of Abstracts of Reviews of Effects (DARE; part of The Cochrane Library)
#1MeSH descriptor: [Antipsychotic Agents] this term only #2(aripiprazol* or abilify or abilitat):ti,ab #3(atypical near/3 (antipsychotic* or anti‐psychotic*)):ti,ab #4#1 or #2 or #3 #5MeSH descriptor: [Child Development Disorders, Pervasive] explode all trees #6MeSH descriptor: [Developmental Disabilities] this term only #7asperger*:ti,ab #8(autis* or ASD or ASDs):ti,ab #9kanner*:ti,ab #10rett*:ti,ab #11(childhood near/3 schizophren*):ti,ab #12(pervasiv* next development* next disorder* or PDD or PDDs):ti,ab #13#5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 #14#4 and #13 #15#1
Conference Proceedings Citation Index ‐ Science (CPCI‐S; Web of Science)
#3 2 AND #1 #2 TS=(aripiprazol* or abilify or abilitat or "atypical antipsychotic*" or "atypical anti‐psychotic*" ) #1 TS=(autis* or asperger* or kanner* or childhood schizophren* or ASD or ASDs or "childhood pervasive disorder* " or "pervasive disorder* of childhood" or PDD or PDDs)
Autism Data
autism.org.uk/autismdata
aripiprazole or abilify or abilitat
ZETOC (limited to conferences)
zetoc.mimas.ac.uk
conference: aripiprazole autis*
WorldCat (limited to theses and dissertations)
worldcat.org/
(kw: autis* or kw: asperger* or kw: pervasiv*) AND (kw: aripiprazole OR kw: abilify OR kw: abilitat or kw: atypical) and yr: 1990‐2011 and mt: deg.
ClinicalTrials.gov
clinicaltrials.gov
aripiprazole OR abilify OR abilitat OR atypical antipsychotics AND autis* OR pervasive OR asperge*
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP)
who.int/ictrp/en
Condition : autism OR autistic or asperger or aspergers or pervasive or ASD or ASDs or PDD or PDDS
AND
Intervention: aripiprazole OR abilify OR abilitat OR atypical antipsychotic*
Appendix 2. Search summary
| Database | Search date | Database date range/issue/volume | Number of records | Limits |
| Cochrane Central Register of Controlled Trials (CENTRAL) | 04/05/2011 | 2011 Issue 11 | 84 | limit to 1990‐ |
| 20/11/2014 | 2014 Issue 10 | 26 | limit to 2011‐current | |
| 14/10/2015 | 2015 Issue 9 | 8 | limit to 2014‐2015 | |
| Ovid MEDLINE | 04/05/2011 | 1948 to April Week 3 2011 | 567 | limit to 1990‐ |
| 20/11/2014 | 1946 to November Week 2 2014 | 150 | ed=20110401‐20141120 | |
| 14/10/2015 | 1946 to October Week 1 2015 | 23 | ed=20141101‐20151001 | |
| Embase (Ovid) | 04/05/2011 | 1980 to 2011 Week 17 | 710 | limit to 1990‐ |
| 20/11/2014 | 1980 to 2014 Week 46 | 144 | limit to 2011‐current | |
| 14/10/2015 | 1980 to 2015 Week 41 | 27 | em=201446‐201541 | |
| CINAHL Plus (EBSCOhost) | 04/05/2011 | 1937 to current | 45 | limit to 1990‐ |
| 20/11/2014 | 1937 to current | 31 | EM 20110430‐ | |
| 14/10/2015 | 1937 to current | 5 | EM 20141101‐ | |
| PsycINFO (EBSCOost) | 04/05/2011 | 1887 to current | 83 | limit to 1990‐ |
| PsycINFO (Ovid) | 20/11/2014 | 1887 to current | 59 | up=20110502‐20141117 |
| 14/10/2015 | 1806 to October Week 1 2015 | 10 | up=20141117‐20151005 | |
| Cochrane Database of Systematic Reviews (CDSR) | 20/11/2014 | 11 of 12, November 2014 | 4 | no limits as not searched previously |
| 14/10.2015 | 10 of 12 October 2015 | 0 | 2014‐2015 | |
| Database of Abstracts of Reviews of Effects (DARE) | 20/11/2014 | Issue 4 of 4, October 2014 | 8 | no limits as not searched previously |
| 14/10/2015 | Issue 2 of 4, April 2015 | 1 | 2014‐2015 | |
| Conference Proceedings Citation Index ‐ Science (CPCI‐S, Web of Science) | 04/05/2011 | 1990 to current | 22 | limit to 1990‐ |
| 20/11/2014 | 1990 to current | 2 | limit to 2011‐2014 | |
| 14/10/2015 | 1990 to current | 1 | limit to 2014‐2015 | |
| AutismData | 04/05/2011 | all available years | 20 | no limits |
| 20/11/2014 | all available years | 21 | 2011‐2014 | |
| 14/10/2015 | all available years | 0 | 2014‐2015 | |
| ZETOC (conference proceedings) | 04/05/2011 | all available years | 0 | no limits |
| 20/11/2014 | all available years | 0 | no limits | |
| 14/10/2015 | all available years | 0 | no limits | |
| WorldCat.org (limited to theses and dissertations) | 04/05/2011 | all available years | 11 | 1990‐ |
| 20/11/2014 | all available years | 1 | 2011‐2014 | |
| 14/10/2015 | all available years | 0 | 2014‐2015 | |
| ClinicalTrials.gov | 04/05/2011 | all available years | 20 | no limits |
| 24/11/2014 | all available years | 16 | no limits | |
| 14/10/2015 | all available years | 16 | no limits | |
| World Health Organisation International Clinical Trials Registry Platform (WHO ICTRP) | 04/05/2011 | all available years | 7 | no limits |
| 24/11/2014 | all available years | 6 | no limits | |
| 14/10/2015 | all available years | 20 | no limits | |
| Total records up to 2011 | 1569 | |||
| Total records 2011 to 2015 | 579 |
Appendix 3. Planned methods archived for future updates of this review
| Measures of treatment effect |
Continuous outcomes We will use standardised mean differences (SMDs) for continuous outcomes that are measured with similar, but not identical, instruments. |
|
Unit of analysis issues |
Cluster‐randomised trials We do not anticipate finding cluster‐randomised trials. Cross‐over trials If we find any cross‐over trials, we will conduct a meta‐analysis to combine results using the inverse variance method as recommended by Elbourne 2002. In the case that data from a cross‐over trial are limited and restricted, we will use available data within the first phase, only up to the point of cross‐over. Repeated observations on participants If studies report repeated observations on participants, we will extract time points closer to 3 and 6 months and at the end of the study. |
|
Assessment of reporting bias |
If we find enough studies (n = 10), we will draw funnel plots (effect size versus standard error) to assess the presence of small‐study effects. Although asymmetry may represent the relationship between trial size and effect size, it can also demonstrate publication bias. If we find funnel plot asymmetry, we will investigate clinical diversity as a possible explanation for asymmetry. |
|
Subgroup analysis and investigation of heterogeneity |
Assuming a sufficient number of included studies, we will undertake a subgroup analysis to explore the possibility of differential responses to aripiprazole based on:
If data are presented in unuseable forms, we will attempt to contact study authors for raw data. If we cannot obtain these data, we will not include the study in the meta‐analysis but instead will describe the results individually. |
| Sensitivity analysis | We will conduct sensitivity analyses to assess the impact of risk of bias on results in the event that we find a sufficient number of studies. For example, we will exclude studies rated as having high risk of bias for sequence generation or allocation concealment, or both, to find any impact on results of the meta‐analysis. |
Data and analyses
Comparison 1. Aripiprazole versus placebo in randomised controlled trials (RCTs).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Aberrant Behavior Checklist (ABC) ‐ Irritability subscale: mean score changes | 2 | 308 | Mean Difference (IV, Random, 95% CI) | ‐6.17 [‐9.07, ‐3.26] |
| 2 Aberrant Behavior Checklist (ABC) ‐ Hyperactivity subscale: mean score changes | 2 | 308 | Mean Difference (IV, Random, 95% CI) | ‐7.93 [‐10.98, ‐4.88] |
| 3 Aberrant Behavior Checklist (ABC) ‐ Stereotypy subscale: mean score changes | 2 | 308 | Mean Difference (IV, Random, 95% CI) | ‐2.66 [‐3.55, ‐1.77] |
| 4 Aberrant Behavior Checklist (ABC) ‐ Inappropriate Speech subscale: mean score changes | 2 | 308 | Mean Difference (IV, Random, 95% CI) | ‐1.43 [‐2.60, ‐0.27] |
| 5 Aberrant Behavior Checklist (ABC) ‐ Lethargy/Withdrawal subscale: mean score changes | 2 | 308 | Mean Difference (IV, Random, 95% CI) | ‐1.19 [‐2.77, 0.40] |
| 6 Clinical Global Impression (CGI) ‐ Severity subscale: mean scores | 2 | 308 | Mean Difference (IV, Random, 95% CI) | ‐0.57 [‐0.96, ‐0.18] |
| 7 Clinical Global Impression (CGI) ‐ Improvement subscale: mean scores | 2 | 308 | Mean Difference (IV, Random, 95% CI) | ‐1.33 [‐1.75, ‐0.92] |
| 8 Any extrapyramidal symptom event (side effect) | 2 | 313 | Risk Ratio (M‐H, Random, 95% CI) | 1.89 [0.98, 3.66] |
| 9 Children's Yale‐Brown Obsessive Compulsive Scale (CY‐BOCS): mean scores | 2 | 308 | Mean Difference (IV, Random, 95% CI) | ‐1.93 [‐3.86, 0.00] |
| 10 Clinically relevant weight gain (side effect) | 2 | 308 | Risk Ratio (M‐H, Random, 95% CI) | 3.78 [1.78, 8.02] |
| 11 Weight gain (side effect) | 2 | 308 | Mean Difference (IV, Random, 95% CI) | 1.13 [0.71, 1.54] |
| 12 Body mass index (BMI) change from baseline (side effect) | 2 | 313 | Mean Difference (IV, Random, 95% CI) | 0.44 [‐0.27, 1.16] |
| 13 Elevated fasting triglycerides at endpoint (side effect) | 2 | 313 | Risk Ratio (M‐H, Random, 95% CI) | 1.51 [0.62, 3.67] |
| 14 Elevated low‐density lipoprotein at endpoint (side effect) | 2 | 313 | Risk Ratio (M‐H, Random, 95% CI) | 3.19 [0.13, 76.36] |
| 15 Decreased high‐density lipoprotein at endpoint (side effect) | 2 | 313 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.11, 8.18] |
| 16 Elevated fasting blood glucose at endpoint (side effect) | 2 | 313 | Risk Ratio (M‐H, Random, 95% CI) | 1.57 [0.08, 32.11] |
| 17 Sedation (side effect) | 2 | 313 | Risk Ratio (M‐H, Random, 95% CI) | 4.28 [1.58, 11.60] |
| 18 Drooling (side effect) | 2 | 313 | Risk Ratio (M‐H, Random, 95% CI) | 9.64 [1.29, 72.10] |
| 19 Tremor (side effect) | 2 | 313 | Risk Ratio (M‐H, Random, 95% CI) | 10.26 [1.37, 76.63] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Findling 2014.
| Methods |
Phase 1: single‐blind, aripiprazole, flexibly dosed, to aripiprazole (2 to 15 mg/d) for 13 to 26 weeks. Chldren and adolescents with a stable response (> 25% decrease in ABC‐I subscale score and rating of "much improved" or "very much improved" on CGI‐I subscale score for 12 weeks randomised into phase 2) Phase 2: 1:1 randomisation to titrated dose of aripiprazole (2 to 15 mg/d) or placebo for 16 weeks in this double‐blind, randomised, placebo‐controlled, parallel‐group study |
|
| Participants |
Sample size: 85 children/adolescents entered phase 2 (double‐blind randomisation), from 157 in phase 1 (single‐blind stabilisation) Particpants randomised in phase 2 Sample size: 85 (intervention 41, placebo 44) Sex: 17 girls (intervention 11, placebo 6), 68 boys (intervention 30, placebo 38) Mean age: overall 10.4 (SD 2.8); intervention 10.1 (SD 2.80); placebo 10.8 (SD 2.77) Race: 59 white (intervention 31, placebo 28), 19 black/African American (intervention 8, placebo 11), 3 Asian (0 intervention, 3 placebo), 1 American Indian/Alaskan Native (0 intervention, 1 placebo), 3 other (2 intervention, 1 placebo) Inclusion criteria (both phases)
Inclusion criteria (phase 2)
|
|
| Interventions | Aripiprazole 2, 5, 10 or 15 mg/d or placebo | |
| Outcomes |
Primary outcome
Secondary outcomes
|
|
| Notes |
Study dates: March 2011 to June 2012 Study location: United States Funding: Bristol‐Myers Squibb Conflicts of interest
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation was not described in the manuscript |
| Allocation concealment (selection bias) | Low risk | Randomisation was performed via a centralised call‐in system |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded aripiprazole or matching placebo was taken once daily |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blinded aripiprazole or matching placebo was taken once daily |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Not all raw data were provided |
| Selective reporting (reporting bias) | Low risk | All outcomes in protocol were reported in the study |
| Other bias | Low risk | From the report, it does not appear that any other sources of bias are present |
Marcus 2009.
| Methods | Randomised 1:1:1:1 to aripiprazole (5, 10 or 15 mg/d) or placebo in this 8‐week double‐blind, randomised, placebo‐controlled, parallel‐group study | |
| Participants |
Sample size: 218 children and adolescents (intervention 166 (54 = 15 mg, 59 = 10 mg, 53 = 5 mg), placebo 52) Sex: 23 girls (intervention 19 (4 = 15 mg, 9 = 10 mg, 6 = 5 mg), placebo 4), 195 boys (intervention 147 (50 = 15 mg, 50 = 10 mg, 47 = 5 mg), placebo 48) Age: 166 between 6 and 12 years of age (intervention 131 (42 = 15 mg, 45 = 10 mg, 44 = 5 mg), placebo 35), 52 between 13 and 17 years of age (intervention 35 (12 = 15 mg, 14 = 10 mg, 9 = 5 mg), placebo 17) Race: 155 white (intervention = 120 (42 = 15 mg, 41 = 10 mg, 37 = 5 mg), placebo = 35), 50 black (intervention = 37 (9 = 15 mg, 13 = 10 mg, 15 = 5 mg), placebo = 13), 46 Asian (intervention = 43 (0 = 15 mg, 42 = 10 mg, 1 = 5 mg), placebo = 3), 7 other (intervention = 6 (3 = 15 mg, 1 = 10 mg, 2 = 5 mg), placebo = 1) Inclusion criteria
|
|
| Interventions | Aripiprazole (5, 10 or 15 mg/day) versus placebo | |
| Outcomes |
Primary outcome
Secondary outcomes
|
|
| Notes |
Study dates: June 2006 to June 2008 Study location: United States Funding: Bristol‐Myers Squibb and Otsuka Pharmaceutical Conflicts of interest
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Although a double‐blind placebo‐controlled trial was described, the study did not describe how randomisation occurred |
| Allocation concealment (selection bias) | Unclear risk | Although a double‐blind placebo‐controlled trial was described, the study did not describe the method of concealment of allocation of intervention type |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Although a double‐blind trial was described, the study did not describe assurance of blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Although a double‐blind trial was described, the study did not describe assurance of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Sufficient information was provided to address incomplete outcome data and how LOCF analysis of such data was performed. Excluded children and adolescents and reasons for exclusion were reported fully |
| Selective reporting (reporting bias) | Low risk | Study protocol is available; its pre‐specified, primary outcomes have been reported online to reduce the likelihood of selective reporting |
| Other bias | Low risk | From the report, it seems clear that no other risks of bias are present |
Owen 2009.
| Methods | Randomised 1:1 to flexibly dosed aripiprazole (target dose 5, 10 or 15 mg/d) or placebo in this 8‐week, double‐blind, randomised, placebo‐controlled, parallel‐group study | |
| Participants |
Sample size: 98 children/adolescents (intervention 47, placebo 51) Sex: 12 girls (intervention 7, placebo 5), 86 boys (intervention 40, placebo 46) Age: 83 between 6 and 12 years of age (intervention 46, placebo 37), 15 between 13 and 17 years of age (intervention 10, placebo 5) Race: 73 white (intervention 41, placebo 32), 18 black (intervention 11, placebo 7), 2 Asian (2 intervention, 0 placebo), 5 other (intervention 2, placebo 3) Inclusion criteria
|
|
| Interventions | Aripiprazole (5, 10 or 15 mg/d) versus placebo | |
| Outcomes |
Primary outcome
Secondary outcomes
|
|
| Notes |
Study dates: June 2006 to April 2008 Study location: United States Funding: Bristol‐Myers Squibb and Otsuka Pharmaceutical Conflicts of interest
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A computer‐generated randomisation schedule using permuted block design was used for randomisation |
| Allocation concealment (selection bias) | Low risk | A call‐in interactive voice response system was readily available for participating intervention sites when children and adolescents were ready to be randomly assigned |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Medication bottle numbers were assigned to children and adolescents, thus reducing the risk that blinding could have been broken |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigators and caregivers were blinded to the intervention; dosage increases were made incrementally |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Sufficient information was provided to address incomplete outcome data and the way LOCF analysis of such data was performed. Excluded children and adolescents and reasons for exclusion were reported fully. 3 randomised children were excluded from the analysis ‐ 1 child randomised to placebo was lost to follow‐up before entering the double‐blind intervention phase, 1 child randomised to placebo withdrew consent and 1 child randomised to aripiprazole discontinued on day 2 of the study before completing a post‐baseline efficacy evaluation. We do not think exclusion of these 3 children would alter study results, even if extreme results were obtained in all 3 cases |
| Selective reporting (reporting bias) | Low risk | Study protocol is available; its pre‐specified primary outcomes have been reported online to reduce the likelihood of selective reporting |
| Other bias | Low risk | From the report, it seems clear that no other risks of bias are present |
ABC: Aberrant Behavior Checklist. ABC‐I: Aberrant Behavior Checklist ‐ Irritability. ADI‐R: Autism Diagnostic Interview ‐ Revised. ASD: autism spectrum disorders. BMI: body mass index. CGI: Clinical Global Impressions scale. CGI‐I: Clinical Global Impressions ‐ Improvement scale. CGI‐S: Clinical Global Impressions ‐ Severity scale. CY‐BOCS: Children’s Yale‐Brown Obsessive Compulsive Scale. DSM‐IV‐TR: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision LOCF: last observation carried forward. SD: standard deviation.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aman 2010 | Post hoc analysis of pooled results of Marcus 2009 and Owen 2009 |
| Benton 2011 | Review article |
| Blankenship 2010 | Review article |
| D'Alessandro 2012 | Non‐randomised controlled trial |
| Douglas‐Hall 2011 | Review article |
| Erickson 2010 | Review article |
| Farmer 2011 | Review article |
| Ghanizadeh 2014 | No placebo control group |
| Huang 2010 | Case series |
| Lewis 2009 | Pooled analysis of results of Marcus 2009 and Owen 2009 |
| Maloney 2014 | Non‐randomised controlled trial |
| Masi 2009 | Retrospective naturalistic study |
| Narasimhan 2006 | Open‐label study |
| Robb 2011 | Pooled analysis of results of Marcus 2009 and Owen 2009 |
| Stigler 2004 | Open‐label study |
| Stigler 2006 | Open‐label study |
| Varni 2012 | Post hoc HRQoL analysis of results of Marcus 2009 and Owen 2009 |
HRQoL: health‐related quality of life.
Differences between protocol and review
We choose not to exclude participants receiving non‐pharmacological therapy (i.e. behaviour therapy), provided it was equally accessible to all study participants, stable before trial entry and consistent throughout the study. This was not specified in the protocol (Ching 2011) and therefore reflects a post hoc decision.
We have specified in the Types of outcome measures section that we use the term 'side effects' to describe any harms, adverse effects or adverse drug reactions associated with aripiprazole.
We added Conference Proceedings Citation Index ‐ Science and WorldCat to the electronic sources listed in our protocol (Ching 2011) to increase the chance of finding conference papers and theses. We also added Autism Data to search the holdings of the National Autistic Society Information Centre Library. For this update, we also searched the Cochrane Database of Systematic Reviews (CDSR) and the Database of Abstracts of Reviews of Effects (DARE) to check the reference lists of previous reviews related to our topic.
In the Assessment of risk of bias in included studies, we reported separately methods for assessing the risk of performance bias due to inadequate blinding of participants and personnel, and methods for assessing the risk of detection bias due to inadequate blinding of outcome assessment.
We analysed time‐to‐event data using hazard ratios and their associated 95% CIs. This type of data analysis was not listed in the protocol (Ching 2011) and therefore reflects a post hoc decision.
We reported tau² ‐ an estimate of between‐study variance ‐ when reporting results from the random‐effects model. This was not specified in the protocol (Ching 2011) and therefore reflects a post hoc decision.
We added a section on 'Summary of findings', beneath the section on 'Data synthesis'.
Contributions of authors
For the original Cochrane review, Heidi Ching drafted the protocol, selected trials for inclusion, extracted data from trials, entered data into RevMan, drafted the final review and carried out the analysis. For this version only, Lauren Hirsch selected trials for inclusion, extracted data from trials, entered data into RevMan and drafted and edited the final review. For both the original Cochrane review (Ching 2012) and this version, Tamara Pringsheim edited the protocol, selected trials for inclusion, extracted data from trials, interpreted the analysis and drafted the final review. Tamara has overall responsibility for the review and will keep the review up‐to‐date.
Sources of support
Internal sources
-
University of Calgary, Department of Clinical Neurosciences, Canada.
Salary support for Dr. Pringsheim
External sources
None, Other.
Declarations of interest
Lauren Hirsch has no conflicts of interest to declare.
Tamara Pringsheim (TP) has received direct financial gain from:
Teva Canada Innovation, on one occasion in 2014, for consulting. TP declares that Teva does not make or market any products relevant to this review.
TP has received indirect financial gain from:
Shire Canada, in 2015. TP received an unrestricted educational grant to create an educational curriculum on assessment and treatment of aggression in youth. TP declares that Shire does not make or market any products relevant to this review.
TP declares that the entities listed below are funding agencies that do not make treatments for ASD or any other disease.
Canadian Institutes of Health Research, for research funding to create a patient decision aid in 2014 and 2015.
Alberta Mental Health Strategic Clinical Network, for research funding on off‐label prescribing of antipsychotics in 2015.
Mathison Centre for Mental Health Research and Education, for research funding for the Canadian Schizophrenia Guidelines in 2015.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Findling 2014 {published data only}
- Findling RL, Mankosi R, Timko K, Lears K, McCartney T, McQuade RD, et al. Randomized controlled trial investigating the safety and efficacy of aripiprazole in the long‐term maintenance treatment of pediatric patients with irritability associated with autistic disorder. Journal of Clinical Psychiatry 2014;75(1):22‐30. [PUBMED: 24502859] [DOI] [PubMed] [Google Scholar]
Marcus 2009 {published data only}
- Marcus RN, Owen R, Kame L, Manos G, McQuade RD, Carson WH, et al. A placebo‐controlled, fixed‐dose study of aripiprazole in children and adolescents with irritability associated with autistic disorder. Journal of the American Academy of Child and Adolescent Psychiatry 2009;48(11):1110‐9. [PUBMED: 19797985] [DOI] [PubMed] [Google Scholar]
Owen 2009 {published data only}
- Owen R, Sikich L, Marcus RN, Corey‐Lisle P, Manos G, McQuade RD, et al. Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder. Pediatrics 2009;124(6):1533‐40. [PUBMED: 19948625] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Aman 2010 {published data only}
- Aman M, Kasper W. Line‐item analysis of the Aberrant Behaviour Checklist: results from two studies of aripiprazole in the treatment of irritability associated with autistic disorder. Journal of Child and Adolescent Psychopharmacology 2010;20(5):415‐22. [PUBMED: 20973712] [DOI] [PubMed] [Google Scholar]
Benton 2011 {published data only}
- Benton T. Aripiprazole to treat irritability associated with autism: a placebo‐controlled, fixed‐dose trial. Current Psychiatry Reports 2011;13(2):77‐9. [DOI: 10.1007/s11920-010-0172-0] [DOI] [PubMed] [Google Scholar]
Blankenship 2010 {published data only}
- Blankenship K, Erickson C, Stigler KA, Posey DJ, McDougle CJ. Aripiprazole for irritability associated with autistic disorder in children and adolescents aged 6‐17 years. Pediatric Health 2010;4(4):375‐81. [DOI] [PMC free article] [PubMed] [Google Scholar]
D'Alessandro 2012 {published data only}
- D'Alessandro TMM. Low‐dose Abilify and the Treatment of Disruptive Behaviours in Children with Autism Spectrum Disorders [PhD thesis]. Florida: University of Florida, 2012. [Google Scholar]
Douglas‐Hall 2011 {published data only}
- Douglas‐Hall P, Curran S, Bird V, Taylor D. Aripiprazole: a review of its use in the treatment of irritability associated with autistic disorder patients aged 6‐17. Journal of Central Nervous System Disease 2011;3:143‐53. [DOI: 10.4137/JCNSD.S4140] [DOI] [PMC free article] [PubMed] [Google Scholar]
Erickson 2010 {published data only}
- Erickson C, Stigler K, Posey DJ, McDougle CJ. Aripiprazole in autism spectrum disorders and fragile X syndrome. Neurotherapeutics 2010;7(3):258‐63. [DOI: 10.1016/j.nurt.2010.04.001] [DOI] [PMC free article] [PubMed] [Google Scholar]
Farmer 2011 {published data only}
- Farmer CA, Aman MG. Aripiprazole for the treatment of irritability associated with autism. Expert Opinion on Pharmacotherapy 2011;12(4):635‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ghanizadeh 2014 {published data only}
- Ghanizadeh A, Sahraeizadeh A, Berk M. A head‐to‐head comparison of aripiprazole and risperidone for safety and treating autistic disorders, a randomized double blind clinical trial. Child Psychiatry and Human Development 2014;45(2):185‐92. [PUBMED: 23801256] [DOI] [PubMed] [Google Scholar]
Huang 2010 {published data only}
- Huang SC, Tsai SJ, Yang HJ. Aripiprazole improves social interaction in Taiwanese children with pervasive developmental disorder. Chang Gung Medical Journal 2010;33(2):211‐5. [PubMed] [Google Scholar]
Lewis 2009 {published data only}
- Lewis D, Owen R. Efficacy and safety of aripiprazole for the treatment of irritability associated with autistic disorder in children and adolescents (6‐17 years): results from two 8‐week, randomized, double‐blind, placebo controlled trials. Neurology 2009;72(11 Suppl 3):A428. [Google Scholar]
Maloney 2014 {published data only}
- Maloney A, Mick EO, Frazier J. Aripiprazole decreases irritability in 12 out of 14 youth with autism spectrum disorder. Journal of Child and Adolescent Psychopharmacology 2014;24(6):357‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Masi 2009 {published data only}
- Masi G, Cosenza A, Millepiedi S, Muratori F, Pari C, Salvadori F. Aripiprazole monotherapy in children and young adolescents with pervasive developmental disorders: a retrospective study. CNS Drugs 2009;23(6):511‐21. [DOI] [PubMed] [Google Scholar]
Narasimhan 2006 {published data only}
- Narasimhan T, Bruce T, BallardJF, Patkar A, Masand P, Rech R. Poster session III: an open label trial of aripiprazole in the treatment of autism and its correlation to whole blood serotonin levels and serotonin transporter (5HTTPLR) function. Neuropsychopharmacology. Proceedings of the American College of Neuropsychopharmacology 45th Annual Meeting; 2006 December 3‐7; Hollywood, Florida. 2006; Vol. 31 (Suppl 1s):S259‐60.
Robb 2011 {published data only}
- Robb A, Andersson C, Bellocchio EE, Manos G, Rojas‐Fernandez C, Mathew S, et al. Safety and tolerability of aripiprazole in the treatment of irritability associated with autistic disorder in pediatric subjects (6‐17 years): results from a pooled analysis of 2 studies. Primary Care Companion for CNS Disorders 2011;13(1):e1‐9. [PUBMED: 21731831] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stigler 2004 {published data only}
- Stigler K, Posey D, McDougle CJ. Aripiprazole for maladaptive behaviour in pervasive developmental disorders. Journal of Child and Adolescent Psychopharmacology 2004;14(3):455‐63. [PUBMED: 15650503] [DOI] [PubMed] [Google Scholar]
Stigler 2006 {published data only}
- Stigler KA, Diener JT, Kohn AE, Erickson CA, Posey DJ. McDougle CJ. Poster session II: a prospective open‐label study of aripiprazole in youth with Asperger's disorder and pervasive developmental disorder not otherwise specified. Neuropsychopharmacology. Proceedings of the American College of Neuropsychopharmacology 45th Annual Meeting; 2006 December 3‐7; Hollywood, Florida. 2006; Vol. 31 (Suppl 1s):S194.
Varni 2012 {published data only}
- Varni, JW, Handen, BL, Corey‐Lisle P, Guo Z, Manos G, Ammerman DK, et al. Effect of aripiprazole 2 to 15 mg/d on health‐related quality of life in the treatment of irritability associated with autistic disorder in children: a post hoc analysis of two randomized controlled trials. Clinical Therapeutics 2012;34(4):982‐92. [PUBMED: 22444782] [DOI] [PubMed] [Google Scholar]
Additional references
Aman 1986
- Aman M, Singh N. Aberrant Behaviour Checklist: Manual. New York: Slosson Educational Publications, 1986. [Google Scholar]
Anderson 1989
- Anderson LT, Campbell M, Adams P, Small AM, Perry R, Shell J. The effects of haloperidol on discrimination learning and behavioural symptoms in autistic children. Journal of Autism and Developmental Disorders 1989;19(2):227‐39. [DOI] [PubMed] [Google Scholar]
APA 2000
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th Edition. Washington, DC: American Psychiatric Association, 2000. [Google Scholar]
APA 2013
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th Edition. Arlington, VA: American Psyciatric Publishing, 2013. [Google Scholar]
Barnes 1989
- Barnes TR. A rating scale for drug‐induced akathisia. British Journal of Psychiatry 1989;154:672‐6. [PUBMED: 2574607] [DOI] [PubMed] [Google Scholar]
Baron‐Cohen 2009
- Baron‐Cohen S, Scott FJ, Allison C, Williams J, Bolton P, Matthews FE, et al. Prevalence of autism spectrum conditions: UK school based population study. British Journal of Psychiatry 2009;194(6):500‐9. [DOI] [PubMed] [Google Scholar]
Bobo 2013
- Bobo WV, Cooper WO, Stein CM, Olfson M, Graham D, Daugherty J, et al. Antipsychotics and the risk of type 2 diabetes mellitus in children and youth. JAMA Psychiatry 2013;70(10):1067‐75. [PUBMED: 23965896] [DOI] [PubMed] [Google Scholar]
Campbell 1982
- Campbell M, Anderson LT, Small AM, Perry R, Green WH, Caplan R. The effects of haloperidol on learning and behaviour in autistic children. Journal of Autism and Developmental Disorders 1982;12(2):167‐75. [PUBMED: 7174605] [DOI] [PubMed] [Google Scholar]
Campbell 1997
- Campbell M, Armenteros JL, Malone RP, Adams PB, Eisenberg ZW, Overall JE. Neuroleptic‐related dyskinesias in autistic children: a prospective, longitudinal study. Journal of the American Academy of Child and Adolescent Psychiatry 1997;36(6):835‐43. [PUBMED: 9183140] [DOI] [PubMed] [Google Scholar]
CDC 2014
- Centers for Disease Control and Prevention. Community Report from the Autism and Developmental Disabilities Monitoring (ADDM) Network: a snapshot of autism spectrum disorder among 8‐year‐old children in multiple communities across the United States in 2010. http://www.cdc.gov/ncbddd/autism/documents/community_report_autism.pdf (accessed 4 September 2015).
Correll 2009
- Correll CU, Manu P, Olshanskiy V, Napolitano B, Kane JM, Malhotra AK. Cardiometabolic risk of second‐generation antipsychotic medications during first‐time use in children and adolescents. JAMA 2009;302(16):1765‐73. [PUBMED: 19861668] [DOI] [PMC free article] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne DR, Altman DG, Higgins JP, Curtin F, Worthington HV, Vail A. Meta‐analysis involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [PUBMED: 11914310] [DOI] [PubMed] [Google Scholar]
Elsabbagh 2012
- Elsabbagh M, Divan G, Koh Y, Kim YS, Kauchali S, Marcin C, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Research 2012;5(3):160‐79. [PUBMED: 22495912] [DOI] [PMC free article] [PubMed] [Google Scholar]
FDA 2010
- Food, Drug Administration. Label and approval history: ability. www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseraction=Search.Label_ApprovalHistory#apphist (accessed 28 February 2010).
Findling 2008
- Findling RL, Robb A, Nyilas M, Forbes RA, Jin N, Ivanova S, et al. A multiple‐center, randomized, double‐blind, placebo‐controlled study of oral aripiprazole for treatment of adolescents with schizophrenia. American Journal of Psychiatry 2008;165(11):1432‐41. [PUBMED: 18765484] [DOI] [PubMed] [Google Scholar]
Findling 2009
- Findling RL, Nyilas M, Forbes RA, McQuade RD, Jin N, Iwamoto T, et al. Acute treatment of pediatric bipolar I disorder, manic or mixed episode, with aripiprazole: a randomized, double‐blind, placebo‐controlled study. Journal of Clinical Psychiatry 2009;70(10):1441‐51. [PUBMED: 19906348] [DOI] [PubMed] [Google Scholar]
Goodman 1989
- Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, Hill CL, et al. The Yale‐Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Archives of General Psychiatry 1989;46(11):1006‐11. [PUBMED: 2684084] [DOI] [PubMed] [Google Scholar]
Goodnick 2002
- Goodnick PJ, Jerry JM. Aripiprazole: profile on efficacy and safety. Expert Opinion on Pharmacotherapy 2002;3(12):1773‐81. [PUBMED: 12472374] [DOI] [PubMed] [Google Scholar]
Guy 1976
- Guy W. Early Clinical Drug Evaluation Unit (ECDEU) Assessment Manual for Psychopharmacology. National Institute Mental Health. Bethesda, MD: National Institute of Mental Health, 1976. [Google Scholar]
Guyatt 2011
- Guyatt G, Oxman AD, Aki EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction ‐ GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383‐94. [DOI] [PubMed] [Google Scholar]
Higgins 2011a
- Higgins JPT, Altman DG, Sterne J on behalf of the Cochrane Statistical Methods Group and the Cochrane Bias Methods Group. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Intervention Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from http://handbook.cochrane.org.
Higgins 2011b
- Higgins JPT, Deeks JJ, Altman DG on behalf of the Cochrane Statistical Methods Group. Chapter 16: Special topics in statistics. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from http://handbook.cochrane.org.
Higgins 2011c
- Deeks JJ, Higgins JPT, Altman DG on behalf of the Cochrane Statistical Methods Group. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jesner 2009
- Jesner OS, Aref‐Adib M, Coren E. Risperidone for autism spectrum disorder. Cochrane Database of Systematic Reviews 2007, Issue 1. [DOI: 10.1002/14651858.CD005040.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kanner 1943
- Kanner L. Autistic disturbances of affective contact. Nervous Child 1943;2:217‐50. [PubMed] [Google Scholar]
Kogan 2009
- Kogan MD, Blumberg SJ, Schieve LA, Boyle CA, Perrin JM, Ghandour RM, et al. Prevalence of parent‐reported diagnosis of autism spectrum disorders among children in the US, 2007. Pediatrics 2009;124(5):1395‐403. [DOI] [PubMed] [Google Scholar]
Komossa 2009
- Komossa K, Rummel‐Kluge C, Schmid F, Hunger H, Schwarz S, El‐Sayeh HGG, et al. Aripiprazole versus other atypical antipsychotics for schizophrenia. Cochrane Database of Systematic Reviews 2009, Issue 4. [DOI: 10.1002/14651858.CD006569.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lecavalier 2006
- Lecavalier L. Behavioral and emotional problems in young people with pervasive developmental disorders: relative prevalence, effects of subject characteristics, and empirical classification. Journal of Autism and Developmental Disorders 2006;36(8):1101‐14. [PUBMED: 16897387] [DOI] [PubMed] [Google Scholar]
Lord 1994
- Lord C, Rutter M, Couteur A. Autism Diagnostic Interview ‐ Revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders 1994;24(5):659‐85. [DOI] [PubMed] [Google Scholar]
Meyers 2007
- Myers S, Johnson C, Council on Children with Disabilities. Management of children with autism spectrum disorders. Pediatrics 2007;120(5):1162‐82. [DOI] [PubMed] [Google Scholar]
Posey 2008
- Posey DJ, Stigler SKA, Erickson CA, McDougle CJ. Antipsychotics in the treatment of autism. Journal of Clinical Investigation 2008;118(1):6‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Scahill 1997
- Scahill L, Riddle M, McSwiggin‐Hardin M, Ort SI, King RA, Goodman WK, et al. Children's Yale‐Brown Obsessive Compulsive Scale: reliability and validity. Journal of the American Academy of Child and Adolescent Psychiatry 1997;36(6):844‐52. [PUBMED: 9183141] [DOI] [PubMed] [Google Scholar]
Shapiro 2003
- Shapiro DA, Renock S, Arrington E, Chiodo LA, Liu LX, Sibley DR, et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology 2003;28(8):1400‐11. [PUBMED: 12784105] [DOI] [PubMed] [Google Scholar]
Simonoff 2008
- Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, Baird G. Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity and associated factors in a population derived sample. Journal of the American Academy of Child and Adolescent Psychiatry 2008;47(8):921‐9. [PUBMED: 18645422] [DOI] [PubMed] [Google Scholar]
Simpson 1970
- Simpson GM, Agnus JWS. A ratings scale for extrapyramidal side effects. Acta Psychiatrica Scandinavica 1970;45(S212):11‐9. [DOI] [PubMed] [Google Scholar]
Stigler 2009
- Stigler KA, Diener, JT, Kohn AE, Li L, Erickson CA, Posey DJ, et al. Aripiprazole in pervasive development disorder not otherwise specified and Asperger's disorder: a 14‐week, prospective, open‐label study. Journal of Child and Adolescent Psychopharmacology 2009;19(3):265‐74. [PUBMED: 19519261] [DOI] [PMC free article] [PubMed] [Google Scholar]
Varni 1999
- Varni JW, Seid M, Rode CA. The PedsQL: measurement model for the pediatric quality of life inventory. Medical Care 1999;37(2):126‐39. [PUBMED: 10024117] [DOI] [PubMed] [Google Scholar]
Webster 1968
- Webster DD. Critical analysis of the disability in Parkinson's disease. Modern Treatment 1968;5(2):279‐81. [PUBMED: 5655944] [PubMed] [Google Scholar]
WHO 1994
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision. Vol. 1‐3, Geneva: World Health Organization, 1994. [Google Scholar]
Williams 2006
- Williams JG, Higgins JP, Brayne CE. Systematic review of prevalence studies of autism spectrum disorders. Archives of Diseases in Childhood 2006;91(1):8‐15. [PUBMED: 15863467] [DOI] [PMC free article] [PubMed] [Google Scholar]
Yudofsky 1986
- Yudofsky SC, Silver JM, Jackson W, Endicott J, Williams D. The Overt Aggression Scale for the objective rating of verbal and physical aggression. American Journal of Psychiatry 1986;143(1):35‐9. [PUBMED: 3942284] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Ching 2011
- Ching H, Pringsheim T. Aripiprazole for Autism Spectrum Disorders (ASD). Cochrane Database of Systematic Reviews 2011, Issue 3. [DOI: 10.1002/14651858.CD009043] [DOI] [PubMed] [Google Scholar]
Ching 2012
- Ching H, Pringsheim T. Aripiprazole for autism spectrum disorders (ASD). Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD009043.pub2] [DOI] [PubMed] [Google Scholar]