

Abstract
Background
Despite medical therapies and surgical interventions for Parkinson's disease (PD), patients develop progressive disability. The role of physiotherapy is to maximise functional ability and minimise secondary complications through movement rehabilitation within a context of education and support for the whole person. The overall aim is to optimise independence, safety and wellbeing, thereby enhancing quality of life. Trials have shown that physiotherapy has short‐term benefits in PD. However, which physiotherapy intervention is most effective remains unclear.
Objectives
To assess the effectiveness of one physiotherapy intervention compared with a second approach in patients with PD.
Search methods
Relevant trials were identified by electronic searches of numerous literature databases (for example MEDLINE, EMBASE) and trial registers, plus handsearching of major journals, abstract books, conference proceedings and reference lists of retrieved publications. The literature search included trials published up to the end of January 2012.
Selection criteria
Randomised controlled trials of one physiotherapy intervention versus another physiotherapy intervention in patients with PD.
Data collection and analysis
Data were abstracted independently from each paper by two authors. Trials were classified into the following intervention comparisons: general physiotherapy, exercise, treadmill training, cueing, dance and martial arts.
Main results
A total of 43 trials were identified with 1673 participants. All trials used small patient numbers (average trial size of 39 participants); the methods of randomisation and concealment of allocation were poor or not stated in most trials. Blinded assessors were used in just over half of the trials and only 10 stated that they used intention‐to‐treat analysis.
A wide variety of validated and customised outcome measures were used to assess the effectiveness of physiotherapy interventions. The most frequently reported physiotherapy outcomes were gait speed and timed up and go, in 19 and 15 trials respectively. Only five of the 43 trials reported data on falls (12%). The motor subscales of the Unified Parkinson’s Disease Rating Scale and Parkinson’s Disease Questionnaire‐39 were the most commonly reported clinician‐rated disability and patient‐rated quality of life outcome measures, used in 22 and 13 trials respectively. The content and delivery of the physiotherapy interventions varied widely in the trials included within this review, so no quantitative meta‐analysis could be performed.
Authors' conclusions
Considering the small number of participants examined, the methodological flaws in many of the studies, the possibility of publication bias, and the variety of interventions, formal comparison of the different physiotherapy techniques could not be performed. There is insufficient evidence to support or refute the effectiveness of one physiotherapy intervention over another in PD.
This review shows that a wide range of physiotherapy interventions to treat PD have been tested . There is a need for more specific trials with improved treatment strategies to underpin the most appropriate choice of physiotherapy intervention and the outcomes measured.
Keywords: Humans, Physical Therapy Modalities, Gait, Gait/physiology, Parkinson Disease, Parkinson Disease/rehabilitation, Randomized Controlled Trials as Topic
Plain language summary
Physiotherapy for the treatment of Parkinson's disease
In spite of various medical and surgical treatments for Parkinson's disease (PD) patients gradually develop significant physical problems. Physiotherapists aim to enable people with PD to maintain their maximum level of mobility, activity and independence through the provision of the appropriate treatment. A range of approaches to movement rehabilitation are used, which aim to enhance quality of life by maximising physical ability and minimising secondary complications over the whole course of the disease. Evidence has shown that physiotherapy has short‐term benefits in PD, however which approach of physiotherapy is most effective remains unclear.
Only randomised controlled trials were included in this review. These were studies where a group of participants were given one physiotherapy intervention and were compared with another group who received a different physiotherapy intervention. The participants were assigned to a group in a random fashion to reduce the potential for bias.
A total of 43 randomised trials involving 1673 participants (average trial size of just 39 participants) were identified as suitable for this review. The trials assessed various physiotherapy interventions, so they were grouped according to the type of intervention being used (general physiotherapy, exercise, treadmill training, cueing, dance or martial arts). However, despite this grouping, the physiotherapy interventions delivered and the outcomes assessed varied so much that the results of the individual trials could not be combined.
This review highlights that a wide range of different physiotherapy techniques have been tested to treat PD. Considering the small number of participants, the wide variety of physiotherapy interventions and the outcomes assessed, there is insufficient evidence to support the use of one approach of physiotherapy intervention over another for the treatment of PD.
Background
Parkinson’s disease (PD) is a complex neurodegenerative disorder (Rubenis 2007) with wide reaching implications for patients and their families. Whilst disability can occur at all stages of the disease (Deane 2001a), PD is progressive in nature. Patients face increased difficulties with activities of daily living (ADL) (Kwakkel 2007) and mobility such as gait, transfers, balance and posture (Keus 2007). Ultimately this leads to decreased independence, inactivity and social isolation (Keus 2007), resulting in reduced quality of life (Schrag 2000).
The management of PD has traditionally centred on drug therapy with levodopa viewed as the 'gold standard' treatment (Rascol 2002). However, even with optimal medical management, patients with PD still experience a deterioration of body function, daily activities and participation (Nijkrake 2007). For this reason there has been increasing support for the inclusion of rehabilitation therapies as an adjuvant to pharmacological and neurosurgical treatment (Gage 2004; Nijkrake 2007) and a call for the move towards multidisciplinary management of this multidimensional condition (Robertson 2003; Rubenis 2007).
The physiotherapist is a member of the multidisciplinary team (Robertson 2008; Rubenis 2007) and strives to maximise functional ability and minimise secondary complications through movement rehabilitation within a context of education and support for the whole person (Deane 2001a; Plant 2000). Physiotherapy for PD focuses on transfers, posture, upper limb function, balance (and falls), gait, physical capacity and (in)activity utilising cueing strategies, cognitive movement strategies and exercise to optimise the patient’s independence, safety and wellbeing, thereby enhancing quality of life (Keus 2004; Keus 2007).
Referral rates to physiotherapy for people with PD have historically been low (Mutch 1986; Yarrow 1999). However, in recent years the number of referrals has increased, with a survey by Parkinson’s UK in 2008 reporting that 54% of the 13,000 members surveyed had seen a physiotherapist, compared with 27% in a survey undertaken in 1998 (PDS 2008; Yarrow 1999). This rise in referrals may be attributed to two factors. Firstly, guidelines such as those published by the National Institute for Health and Clinical Excellence (NICE) (NICE CG35 2006) recommend that physiotherapy be made available throughout all stages of the disease, raising the profile of the intervention. This has been further supported by the publication of Dutch physiotherapy guidelines (Keus 2004) (updated guidelines were due for publication in 2013), which provide specific information for physiotherapists involved in the management of PD. Secondly, there has been a substantial increase in the number of trials completed over the last decade (particularly in the last five years), offering supportive evidence for the inclusion of physiotherapy in the management of PD (Keus 2009).
A recent Cochrane review (Tomlinson 2012) assessed the effectiveness of physiotherapy intervention versus no physiotherapy intervention in patients with PD. The review provided evidence for the short‐term benefit (< three months) of physiotherapy intervention in the treatment of PD. Further, it suggested that there was no difference in treatment effect between the different types of physiotherapy interventions being used, though this was based on indirect comparisons. This now needs to be confirmed by examining head‐to‐head trials of physiotherapy interventions. This would be of interest to both clinicians and patients so that appropriate physiotherapy interventions which provide greater benefit can be delivered to PD patients (Tomlinson 2012).
The present Cochrane review was first published in 2001, and included only seven randomised controlled trials with a total of 142 participants (Deane 2001b). The methods of physiotherapy varied so widely across the trials that the data could not be combined. This, along with the presence of methodological flaws, small sample sizes, and the possibility of publication bias, led Deane et al to conclude that there was insufficient evidence to support or refute the efficacy of any given approach of physiotherapy over another in PD (Deane 2001b). This review updates the previous Cochrane review. It aims to compare the effectiveness of one approach of physiotherapy intervention versus another approach of physiotherapy intervention in patients with PD.
Objectives
To assess the effectiveness of one physiotherapy intervention compared with a second approach in patients with PD.
Methods
Criteria for considering studies for this review
Types of studies
All randomised controlled trials (including the first phase of cross‐over trials) comparing a physiotherapy intervention with another physiotherapy intervention were considered for inclusion in the review. Only trials that implemented random methods of treatment allocation were included.
Types of participants
Participants with a diagnosis of PD (as defined by the authors of the studies).
PD of any disease stage (i.e. early or diagnostic, maintenance, or complex phase).
Any duration of PD.
All ages.
Any drug therapy.
Any duration of physiotherapy treatment (although trials of less than one day of treatment were excluded).
Types of interventions
Physiotherapy interventions aim to maximise functional ability and minimise secondary complications through movement rehabilitation within a context of education and support for the whole person. Physiotherapy encompasses a wide range of techniques, so we were inclusive in our definition of physiotherapy intervention (including those not directly delivered by a physiotherapist) with trials of general physiotherapy, exercise, treadmill training, cueing, dance and martial arts being included.
Types of outcome measures
1. Gait outcomes such as:
a. two‐ or six‐minute walk test (m), measures the number of metres a person can walk in two or six minutes thereby providing a measurement of walking endurance (Kersten 2004);
b. walking speed:
i. 10‐ or 20‐metre walk test (s), measures the time in seconds that a person takes to walk 10 or 20 metres thereby providing a measurement of gait speed (Kersten 2004),
ii. velocity (m/s), measures the rate of change of position, recorded in metres per second (Trew 2005);
c. cadence (steps/min), measures the number of steps taken in a given period of time, which is then converted into the number of steps taken per minute (Trew 2005);
d. stride length (m), measures the average distance (in metres) between two successive placements of the same foot (Whittle 1996);
e. step length (m), measures the average distance (in metres) between successive foot to floor contact with the opposite feet (Trew 2005);
f. Freezing of Gait Questionnaire, a validated questionnaire for the assessment of freezing of gait. The questionnaire consists of six items and scores range from 0 to 24, with higher scores corresponding to more severe freezing of gait (Giladi 2000).
2. Functional mobility and balance outcomes such as:
a. timed up and go (s), measures the time taken in seconds for a person to get up from a chair, walk a certain distance (usually three metres), turn around and walk back to the chair and sit down (Podsiadlo 1991);
b. Functional Reach Test (cm), “the maximal distance one can reach forward beyond arm’s length, while maintaining a fixed base of support in the standing position” (Duncan 1990);
c. Berg Balance Scale, a validated questionnaire designed to measure functional standing balance of the older adult. The measure consists of 14 items and score ranges from 0 to 56; with 0 to 20 = high fall risk; 21 to 40 = medium fall risk; and 41 to 56 = low fall risk (Berg 1992; Qutubuddin 2005);
d. Activity Specific Balance Confidence. a 16‐item self‐report questionnaire that asks individuals to rate their confidence that they will maintain their balance in the course of daily activities. Each item is rated from 0% (no confidence) to 100% (complete confidence) (Powell 1995; Talley 2008).
3. Data on falls such as:
a. number of patients falling, e.g. falls diary;
b. Falls Efficacy Scale, a 10‐item patient‐reported questionnaire that measures how confident a person is at carrying out various ADL. Items are rated from 1 to 10, with higher scores correlating with lower levels of confidence, and a total score of 70 or more indicating that a person has a fear of falling (Tinetti 1990);
c. Falls Efficacy Scale International, a 16‐item questionnaire that includes the 10 original items of the standard Falls Efficacy Scale as well as six items regarding higher functioning and social activities. Each item is rated on a scale of 1 to 4, with 1 being ‘not concerned at all’ and 4 being ‘very concerned’ (maximum score out of 64) (Yardley 2005).
4. Clinician‐rated impairment and disability measures such as:
a. Hoehn and Yahr, a scale used to describe how symptoms of Parkinson's disease progress. Scale ranges from 0 to 5, with higher levels indicating greater disability (Hoehn 1967);
b. Unified Parkinson's Disease Rating Scale (UPDRS), designed to assess motor impairment and disability in Parkinson’s disease. Higher scores correspond to greater disability (Fahn 1987):
i. total, score ranges from 0 to 176,
ii. mental, score ranges from 0 to 16,
iii. ADL, score ranges from 0 to 52,
iv. motor, score ranges from 0 to 108;
c. Webster Rating Scale, an assessment of severity of disease and clinical impairment against 10 items using a scale of 0 = normal to 3 = maximum impairment (bradykinesia, rigidity, posture, upper extremity swing, gait, tremor at rest, facies, seborrhoea, speech, and self care). Scores ranges from 0 to 30, with higher scores indicating greater disease severity and disability (Webster 1968);
d. Columbia University Rating Scale, an assessment of motor impairment and ADL against 13 items, using a five‐point scale for each to give a total score between 0 = normal to 65 = maximum disability (Yahr 1969).
5. Patient‐rated quality of life such as:
a. Parkinson's Disease Questionnaire‐39 (PDQ‐39), a PD specific health‐related quality of life questionnaire containing 39 items divided into eight domains. Scores range from 0 to 100 with higher scores corresponding to poorer quality of life (Jenkinson 1997; Peto 1995);
b. PDQUALIF, a PD specific health‐related quality of life questionnaire containing 32 items in seven dimensions and one item of global health‐related quality of life. The total score ranges from 0 to 128 with higher scores indicating poorer quality of life (Welsh 2003);
c. PDQL, a PD specific health‐related quality of life questionnaire containing 37 items grouped into four subscales. Item scores range from 1 to 5. The PDQL‐Summary Index ranges from 37 to 185, with higher scores reflecting better quality of life (Deboer 1996);
d. Short Form‐36 (SF‐36) or 12 (SF‐12), a generic short form health survey consisting of 36 or 12 questions. The SF‐36 consists of eight scaled scores assessing vitality, physical functioning, bodily pain, general health perceptions, physical role functioning, emotional role functioning, social role functioning and mental health. Scores range from 0 to 100 with higher scores corresponding to better quality of life (Ware 1992).
6. Adverse events e.g. fractures, pain.
7. Compliance e.g. participant adherence, treatment fidelity.
8. Economic analysis.
Search methods for identification of studies
We undertook a systematic search of the literature up to the end of January 2012 for publications or abstracts describing relevant trials. This included searching the following.
1. General biomedical and science electronic databases (without date limiters) including the Cochrane Movement Disorders Specialised Register, The Cochrane Library, MEDLINE (1966 to 2012), EMBASE (1974 to 2012), CINAHL (1982 to 2012), ISI‐SCI (1981 to 2012); the rehabilitation databases AMED (1985 to 2012), REHABDATA (1995 to 2012), REHADAT (1990 to 2012), PEDro (1929 to 2012), GEROLIT (1979 to 2012); the English language databases of foreign language research and third world publications LILACS (1982 to 2012), MedCarib (17th Century to 2012) and IMEMR (1984 to 2012).
2. The Cochrane Central Register of Controlled Trials (CENTRAL), the CentreWatch Clinical Trials listing service, the metaRegister of Controlled Trials, ClinicalTrials.gov, RePORT, National Institute on Disability and Rehabilitation Research (NIDRR) and National Research Register (NRR).
3. Handsearching of general (Lancet, BMJ, JAMA) and specific journals (Movement Disorders,Neurology,Archives of Physical Medicine and Rehabilitation,Clinical Rehabilitation,Physiotherapy, Physical Therapy) from 2001 to the end of January 2012.
4. The reference lists of retrieved papers and review articles.
5. Abstract books and conference proceedings. This included The XIII International Congress on Parkinson's disease (1999), The International Congress of Parkinson's Disease and Movement Disorders (1990, 1992, 1994, 1996, 1998, 2000, 2002, 2004, 2005, 2006, 2007, 2008, 2009, 2010, 2011, 2012), World Congress on Parkinson's Disease and Related Disorders (2009) and The American Academy of Neurology 51st annual meeting (1999).
6. Grey literature databases (including theses): Conference Proceedings Citation Index (1982 to 2012), DISSABS (1999 to 2012), Conference Papers Index (1982 to 2012), Index to Theses (1970 to 2012), Electronic Theses Online Service (EThOS) (16th Century to 2012) and ProQuest dissertations and theses databases (1861 to 2012).
The search strategies are listed in full in Appendix 1.
Data collection and analysis
Selection of studies
From the search results, two review authors (CLT, CPH, SP or LS) independently screened the abstracts of potentially relevant studies, with the full paper being obtained if the abstract did not provide sufficient information to determine eligibility for inclusion in the review. Disagreement was resolved by referral to a third review author (RS, CM or NI). Authors of potentially eligible studies were contacted for further information if details of their trial were unclear.
Data extraction and management
Two review authors (CLT, CPH, SP or CM) independently assessed the eligible papers or abstracts for trial details and outcome data. These were validated by discussion with any discrepancies resolved by consensus. Trial details were recorded on a standard trial description form and included: trial name, trial group, authors, randomised comparison, treatment schedule (including duration, number of sessions, type of intervention), other therapy, eligibility criteria, method of randomisation, allocation concealment, blinding, accrual period, number of participants randomised, number of dropouts, duration of follow‐up, outcomes reported, use of intention‐to‐treat analysis and publication date(s). The outcome data extracted included data on gait, functional mobility and balance, falls, clinician‐rated disability scale and patient‐rated quality of life, adverse events, compliance or withdrawals and health economics where available.
Authors of any eligible unpublished studies were contacted to ask if further details and the data for their trial could be provided.
Assessment of risk of bias in included studies
Two review authors (CLT, CPH, SP or CM) assessed the methodological quality of the full papers by recording the eligibility criteria (for example specified inclusion (and exclusion) criteria ‐ low risk), method of randomisation (for example used computer random number generator ‐ low risk) and blinding (for example blinding of assessors ‐ low risk), concealment of allocation (for example use of central randomisation service ‐ low risk), similarity of participants in treatment groups at baseline (no difference in baseline characteristics between treatment groups as stated in trial publication ‐ low risk), co‐intervention(s) constant (for example drug therapy stable ‐ low risk), comparable treatment arms (for example similar treatment duration and frequency ‐ low risk), whether an intention‐to‐treat analysis was performed (intention‐to‐treat analysis and withdrawals < 10% ‐ low risk, withdrawals > 10% ‐ unclear risk, per protocol analysis ‐ all unclear risk) and the number of participants lost to follow‐up and missing values (withdrawals below 10% ‐ low risk) (see the risk of bias tables under 'Characteristics of included studies').
Data synthesis
Treatment arms of the included studies were classified and divided according to the types of interventions administered:
1. general physiotherapy;
2. exercise;
3. treadmill training;
4. cueing;
5. dance;
6. martial arts.
Disparate study designs in the included trials resulted in a lack of overlap in the collated physiotherapy methods and outcome measures such that data could not be combined in a meaningful way.
Results
Description of studies
A total of 78 randomised trials of physiotherapy intervention in PD patients were identified; 29 studies were excluded (see Characteristics of excluded studies). The reasons for excluding these trials were: not randomised or not properly randomised (n = 12), cross‐over study with data for the different phases not adequately separated (n = 4), treatment given in trial not usually used by physiotherapists (such as whole body vibration technique) (n = 4), no outcome measures relevant to our review (n = 2), multidisciplinary therapy rehabilitation trial (n = 2), trial duration under one day (n = 1), insufficient information available for inclusion in review (n = 1), unsuitable comparator arm (n = 1), study was confounded (n = 1) and comparison of physiotherapy delivery rather than technique (n = 1). There were also six ongoing trials for which data were not yet available (see Characteristics of ongoing studies). Therefore, there were 43 trials available for inclusion in the review, compared to seven in the 2001 review (Figure 1).
1.
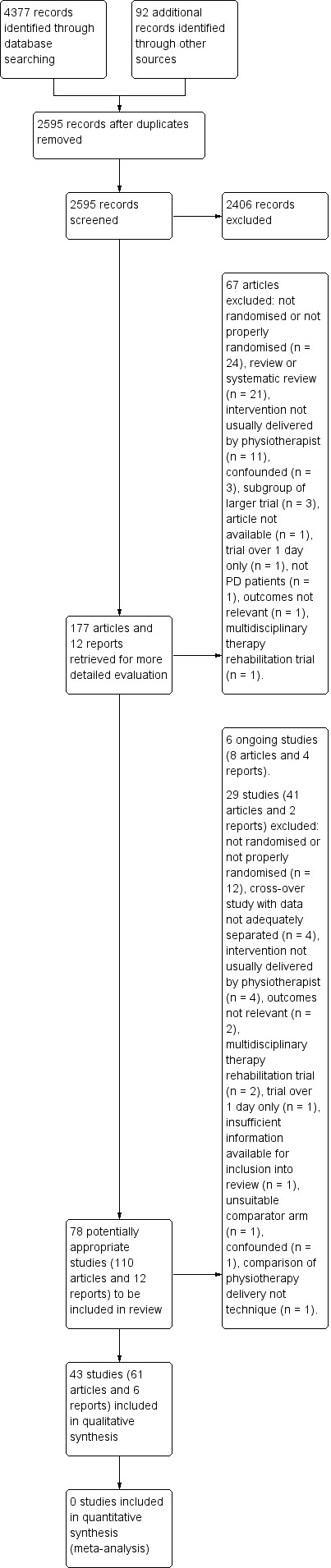
PRISMA flow diagram.
The number of participants randomised into each of the 43 trials ranged from eight to 210 participants, with 1673 participants randomised in total (giving an average trial size of 39 participants) (see Characteristics of included studies). The assessment period ranged from two weeks to 24 months. The mean age of the participants in the trials was 67 years, 62% were male, the mean Hoehn and Yahr stage was 2.4, and they had had PD for approximately seven years.
There were 14 three‐arm trials. Eight trials compared two different experimental physiotherapy interventions with placebo or no intervention (Almeida 2012; Fisher 2008; Li 2012; Mak 2008; McGinley 2012; Shankar 2009; Talakkad 2011; Thaut 1996). The placebo or no intervention arms of these trials were not included in any analysis for this review (see Tomlinson 2012). Six trials compared three different physiotherapy techniques (Chaiwanichsiri 2011; Ebersbach 2010; Juncos 2006; Reuter 2011; Schenkman 2012a; Toole 2005). There was also one four‐arm trial comparing two types of dance (waltz or foxtrot and tango) and martial arts with no intervention (Hackney 2009).
Risk of bias in included studies
See the Characteristics of included studies risk of bias in included studies tables, risk of bias graph (Figure 2) and risk of bias summary (Figure 3).
2.
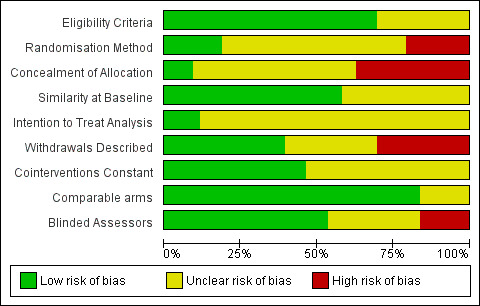
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
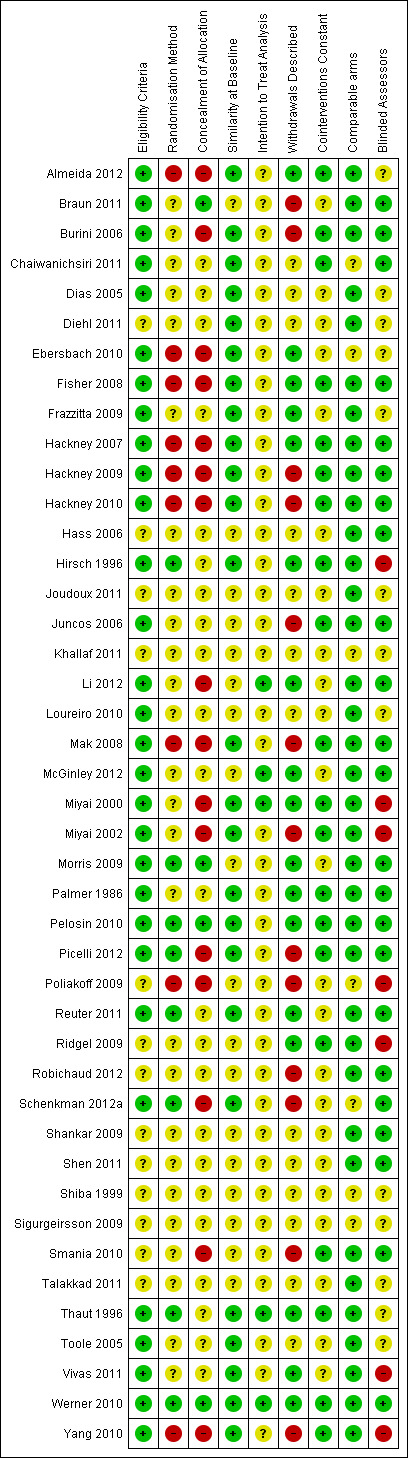
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Trial design
A total of 40 trials had a parallel design and three had a cross‐over design (Burini 2006; Miyai 2000; Shiba 1999). Most trials looked at the short‐term effect of therapy by assessing the participants at baseline and immediately or shortly after the physiotherapy intervention period (which ranged from two weeks to 24 months). Of the parallel design trials 21 reported additional data at assessment points after the treatment period had finished; this may have been at only two weeks or up to 12 months after the end of the treatment period.
Sample size
Only 13 studies (30%) (Braun 2011; Hackney 2007; Hackney 2009; Hackney 2010; Hirsch 1996; Li 2012; McGinley 2012; Morris 2009; Picelli 2012; Reuter 2011; Schenkman 2012a; Smania 2010; Yang 2010) reported a sample size calculation in the trial report, which was achieved by seven studies.
Eligibility criteria
The eligibility criteria for the trials were broad and varied considerably across the trials. The level of detail provided on the eligibility criteria was also variable, with some studies providing a detailed description of the entry criteria and others just stating 'patients with Parkinson’s disease'. Only four trials (Pelosin 2010; Reuter 2011; Schenkman 2012a; Yang 2010) stated that a diagnosis of PD by the United Kingdom Brain Bank Criteria (Gibb 1988) was required. It is vital that eligibility criteria are well‐defined so that the trial participant population can be determined.
Randomisation method and concealment of allocation
A total of 24 trials (56%) described the randomisation method used, of which only eight trials used low risk methods (for example computer random number generators). No details of the randomisation method used were provided for the remaining 19 trials. Further, only 20 trials (47%) either stated or gave adequate information that allowed the assessment of whether an adequate concealment of treatment allocation procedure had been used. Four trials were considered to be low risk by virtue of having used a central independent randomisation service, with the other 16 considered high risk (that is concealment of treatment allocation was potentially compromised as sealed envelopes, picking a card or picking from a hat were used).
Blinding of assessors
It would be impossible to blind participants and therapists to randomised treatment allocation in trials of physiotherapy. Therefore, such trials are open label by nature, and they are consequently liable to the possibility of both performance and attrition bias. However, blinding of assessors could be employed to try and reduce the possibility of bias; 23 (53%) of the 43 studies used blinded assessors, seven used unblinded assessors so were classed as high risk, and in the other 13 studies this information was not provided (classed as unclear risk).
Co‐interventions
Information on co‐interventions was provided in 24 trials (56%), with participants continuing with their standard PD medication. In 20 trials the drug therapy was kept stable (low risk) throughout the duration of the trial, whereas five trials allowed variation (unclear risk). The remaining trials did not describe drug therapy (unclear risk).
Similarity of treatment groups at baseline
A description of the baseline characteristics of the trial participants is important to determine whether the trial results are generalisable and to compare characteristics of the two arms to ensure that the randomisation methods were successful. Six trials (Diehl 2011; Joudoux 2011; Khallaf 2011; Shankar 2009; Shen 2011; Talakkad 2011) did not provide any information on the baseline characteristics of the participants entered into the trial; 31 (of the 37) trials that reported baseline data gave this information split by treatment group; 25 trials reported sufficient data that showed participants to be similar at baseline. In six trials the baseline characteristics of the withdrawn participants were not given (Hackney 2009; Mak 2008; Miyai 2002; Picelli 2012; Smania 2010; Yang 2010). Along with the six trials that did not supply baseline data, this meant that 274 (16%) of the 1693 randomised participants were not characterised.
Data analysis
Ten trials stated intention to treat as the primary method of analysis, although it was not always clear if participants who withdrew from the trial were included in the analysis. The number of participant withdrawals was classed as low risk (≤ 10% of trial participants withdrew) in five of the 10 trials. Four trials used per protocol as the method of analysis (unclear risk). In the other 29 trials the method of analysis was not described (unclear risk), of these trials seven were considered high risk in terms of the proportion of participants that withdrew (that is > 10%), and in 13 trials the number of participant withdrawals (if any) was not described (unclear risk).
Available trial information and data
A total of 13 trials were reported in abstract form; further information was requested from the authors (two were not contactable: Khallaf 2011; Shiba 1999) with four (Juncos 2006; Poliakoff 2009; Robichaud 2012; Shankar 2009) providing additional information and seven (Diehl 2011; Hass 2006; Joudoux 2011; Loureiro 2010; Shen 2011; Sigurgeirsson 2009; Talakkad 2011) being unsuccessful. A total of 30 trials were reported as full publications; further information was requested from authors for 26 trials with 13 providing additional information.
Effects of interventions
See 'Summary of results' table for included trials (Table 1).
1. Included trials: summary table of results.
| Study Group | Location | Interventions | Withdrawals at post‐test (with reasons) | Outcomes | Summary of results at post‐test | ||||||
| Arm 1 | Arm 2 | Arm 3 | Arm 4 | Arm 1 | Arm 2 | Arm 3 | Arm 4 | ||||
| Almeida 2012 | Waterloo, Canada | Visual cueing on the ground (n=14; 30 minutes, 3 times per week, 6 weeks) | Visual cueing on the treadmill (n=14; 30 minutes, 3 times per week, 6 weeks) | Control (n=14) | 0 | 0 | 0 | Primary: Step length Secondary: UPDRS III, timed up and go, gait speed, cadence, double support time, step time, step‐to‐step variability, step time variability, 30 second chair stand |
There was no difference between treatment arms | ||
| Braun 2011 | Netherlands | Physiotherapy with mental practice (n=25; 1 hour (or 2 x 30 minutes) weekly, 6 weeks) | Physiotherapy with relaxation (n=25; 1 hour (or 2 x 30 minutes) weekly, 6 weeks) | 3 (n=2; hospitalised with relapse, n=1; too confronting) | 4 (n=3; hospitalised with relapse, n=1 died) | Visual analogue scale, timed up and go, 10 m walk test | There was no difference between treatment arms | ||||
| Burini 2006 | Ancona, Italy | Aerobic training (n=13; 45 minutes, 3 times per week, 7 weeks) | Qigong group (n=13; 45 minutes, 3 times per week, 7 weeks) | 2 (n=1; poor compliance, n=1; back pain after 3rd session) | 2 (n=1; poor compliance, n=1; fall‐related fracture) | Primary: UPDRS III, UPDRS II, Brown's disability scale (BDS), 6 minute walk test, Borg scale for breathlessness, Beck depression inventory (BDI), PDQ‐39. Secondary: Spirometry test, Maximum cardiopulmonary exercise test |
There was no difference between treatment arms for primary outcomes | ||||
| Chaiwanichsiri 2011 | Bangkok, Thailand | Treadmill with music cue (n=10; 30 minutes, 3 times per week, 4 weeks) | Treadmill (n=10; 30 minutes, 3 times per week, 4 weeks) | Home walking (n=10; 30 minutes, 3 times per week, 4 weeks) | 0 | 0 | 0 | Timed up and go, Walking speed, Step length, Cadence, Stride length, 6‐minute walk test, 6 metre walk time, Single leg stance, UPDRS I, II, III |
There was no difference between treatment arms | ||
| Dias 2005 | Brasil, South America | Physiotherapy and cardiovascular exercise with visual cues (n=8; total 20 sessions) | Conventional physiotherapy (n=8; total 20 sessions) | 0 | 0 | UPDRS, Functional independence measurement scale, Berg balance scale, H&Y scale | Physiotherapy and cardiovascular exercise with visual cues significantly improved functional independent measure, step length, velocity (gait speed) and cadence compared to conventional physiotherapy | ||||
| Diehl 2011 | Indiana, USA | Group Box training (n=unknown, total n=20) | Traditional group exercise (n=unknown, total n=20) | unknown | unknown | Berg balance scale, Activities specific balance confidence scale, Functional reach test, Parkinson's disease quality of life scale |
There was no difference between treatment arms | ||||
| Ebersbach 2010 | Beelitz‐Heilsãtten, Germany | LSVT BIG training (n=20; 1 hour, 4 times per week, 4 weeks) | Nordic Walking (n=20; 1 hour, twice a week, 8 weeks) | Home exercise (n=20; 1 session) | 0 | 1 (n=1; withdrawal of consent) | 1 (n=1; withdrawn due to psychosis) | Primary: UPDRS III. Secondary: PDQ‐39, Timed up and go, time to walk 10 m |
Significant improvement of UPDRS, timed up and go and timed 10m walking in LSVT BIG group compared to Nordic walking and home exercise. There was no difference between treatment arms for PDQ‐39 | ||
| Fisher 2008 | Los Angeles, California | Treadmill group (n=10; 1 hour, 3 times per week, 8 weeks) | Physiotherapy group (n=10; 1 hour, 3 times per week, 8 weeks) | Control group (n=10; 1 hour, total of 6 sessions over 8 weeks) | 0 | 0 | 0 | UPDRS (Total, I, II and III subscores), Hoehn and Yahr, Functional assessments, Walking tests: average gait velocity, step length, stride length, cadence, double limb support time, ankle, knee, hip rotation. Sit‐to‐stand test, Transcranial magnetic stimulation (subset) |
There was no difference between treatment arms | ||
| Frazzitta 2009 | Montescano, Italy | Treadmill with auditory and visual cues (n=20; 20 minutes daily, 4 weeks) | Auditory and visual cues (n=20; 20 minutes daily, 4 weeks) | 0 | 0 | UPDRS III, Gait speed, Freezing of gait questionnaire, Stride length, 6 minute walking test |
The treadmill with auditory and visual cues had significant improvement in gait speed, freezing of gait questionnaire, stride length and 6 minute walking test when compared to the auditory and visual cues group. There were no differences between treatment arms for UPDRS III | ||||
| Hackney 2007 | St. Louis, Missouri, USA | Tango (n=9; 1 hour, 20 sessions within 13 weeks) | Exercise (n=10; 1 hour, 20 sessions within 13 weeks) | 0 | 0 | UPDRS III, Berg balance scale, Freezing of gait, Timed up and go, Velocity of walking and dual‐task walking |
There was no difference between treatment arms | ||||
| Hackney 2009 | St. Louis, Missouri, USA | Tango group (n=19; 1 hour, twice weekly, total 20 sessions in 13 weeks) | Waltz/foxtrot group (n=19; 1 hour, twice weekly, total 20 sessions in 13 weeks) | Tai Chi group (n=17; 1 hour, twice weekly, total 20 sessions in 13 weeks) | Control group (n=20; 13 weeks) | 5 (n= 1; personal problems, n=1; knee pain, n=2; transportation problems, n=1; change in medication) | 2 (n=1; injury at home, n=1; infrequent attendance (unknown)) | 4 (n=2; transportation problems, n=1; hospitalisation (unrelated), n=1; insufficiently intense exercise) | 3 (n=1; hospitalisation (unrelated), n=1; ankle injury, n=1; death in family) | PDQ‐39, UPDRS III, Berg balance scale, Tandem stance test, Timed up and go test, One leg stance test 6 minute walk test, Gait |
PDQ‐39 significantly improved in the tango arm compared to the waltz/foxtrot and Tai Chi arms. Timed up and go test was significantly improved in the tango arm compared to the waltz/foxtrot and Tai Chi arms. There was no difference between treatment arms in UPDRS III |
| Hackney 2010 | St. Louis, Missouri, USA | Partnered tango (n=19; 1 hour, twice weekly, 10 weeks) | Non‐partnered tango (n=20; 1 hour, twice weekly, 10 weeks) | 7 (n=1; progressive decline in mental status, n=2; excessive travelling distance, n=1; felt classes were too fatiguing, n=3; unable to return for follow‐up measures) | 5 (n=1; expressed lack of interest, n=1; new job interfered with class, n=1; unrelated medical problems, n=1; work commitments, n=1; unable to return for follow‐up measures) | Tandem stance, one leg stance, Timed up and go, 6 minute walk test, Gait velocity, Cadence, Stride length, Swing percentage, Double support percentage | There was no difference between treatment arms | ||||
| Hass 2006 | Florida, USA | Tai Chi (n=unknown, total n=23; 1 hour, twice weekly, 16 weeks) | Qi‐gong (n=unknown, total n=23; 1 hour, twice weekly, 16 weeks) | Unknown | Unknown | Gait initiation, Gait velocity, Stride length, Stance, Double limb support, Step duration | There was no difference between treatment arms | ||||
| Hirsch 1996 | North Carolina, USA | Combined balance and resistance training (n=6; 45 minutes, 3 times per week, 10 weeks) | Balance training group (n=9; 30 minutes, 3 times per week, 10 weeks) | 0 | 0 | Balance, Muscle strength (subset group): knee extensors, knee flexors, ankle plantar flexors. Latency to fall, % of trials resulting in falls |
Combined balance and resistance training improved balance scores significantly more than the balance training group. There were no differences between treatment arms for the falls outcomes | ||||
| Joudoux 2011 | Crétil, France | Asymmetric motor training program (n=unknown, total n=50; 1 hour, 3 times per week, 8 weeks) | Broad program (n=unknown, total n=50; 1 hour, 3 times per week, 8 weeks) | Unknown | Unknown | UPDRS III, GMT score, Rapid alternating movements, Handwriting and spiralography, PDQ‐39, Dpression (GDS‐15), Video recording of 8 activities of daily living and biomechanical evaluations |
Abatract describing methodology. No result data | ||||
| Juncos 2006 | Georgia, USA | Aerobic exercise (n=unknown, total n=56; 6 months) | Tai Chi (n=unknown, total n=56; 6 months) | Qi‐gong (n=unknown, total n=56; 6 months) | Unknown (total n=16: n=2; serious adverse events, n=14; unrelated medical or logistical problems) | Unknown (total n=16: n=2; serious adverse events, n=14; unrelated medical or logistical problems) | Unknown (total n=16: n=2; serious adverse events, n=14; unrelated medical or logistical problems) | UPDRS total, UPDRS motor, UPDRS ADL, PDQ‐39, Clinical global impression, Walking speed, Falls | UPDRS ADL scores improved significantly more with Qi‐gong than aerobic exercise. There was no difference between treatment arms for PDQ‐39 and UPDRS total and motor subscores. There was insufficient information on clinical global impression, walking speed and falls | ||
| Khallaf 2011 | Saudi Arabia | Physiotherapy and treadmill (n=15) | Physiotherapy (n=15) | Unknown | Unknown | UPDRS II & III, Hamilton rating scale of depression, Walking speed, Walking distance | Both treatment arms showed significant improvement in walking distance, speed and ADL. A significant improvement in depression only observed in physiotherapy and treadmill group. Unclear if there were any differences between treatment arms | ||||
| Li 2012 | Oregon, USA | Tai Chi (n=65; 1 hour, twice weekly, 24 weeks) | Resistance training (n=65; 1 hour, twice weekly, 24 weeks) | Control, stretching group (n=65; 1 hour, twice weekly, 24 weeks) | 9 (n=4; health problem, n=3; noncommittal/time conflict, n=2; relocating) | 6 (n=4; health problem, n=1; noncommittal/time conflict, n=1; relocating) | 4 (n=3; health problem, n=1; noncommittal/time conflict) | Primary: Two indicators of postural stability: maximum excursion and directional control. Secondary: Stride length, Walking velocity, Strength of bilateral knee extensors and flexors, Functional reach test, Timed up and go, UPDRS III, Number of falls |
The Tai Chi group performed significantly better than those in the resistance training and stretching groups on the primary outcomes. The Tai Chi group had significantly better performance/scores in many outcomes compared to the stretching group. The Tai Chi group out performed the resistance training group on the stride length and functional reach | ||
| Loureiro 2010 | Católica do Paraná, Brazil | Conventional physical therapy (n=6, sessions, twice weekly, total 12 sessions) | Complementary activities (n=6, sessions, twice weekly, total 12 sessions) | Unknown | Unknown | Timed up and go, Anterior functional reach | There was no difference between treatment arms | ||||
| Mak 2008 | Hong Kong, China | Audio‐visual cued task‐specific training (n=21; 20 minutes, 3 times per week, 4 weeks) | Conventional exercise (n=21; 45 minutes, twice weekly, 4 weeks) | Control (n=18; 4 weeks) | 2 (n=1; change of medication, n=1; heel pain) | 2 (n=1; fall with fracture, n=1; went overseas) | 4 (n=2; declined to come back, n=2; went overseas) | Peak horizontal velocity, Peak vertical velocity, Movement time,3 D Kinematics data of sit‐to‐stand | The audio‐visual cued task‐specific training group increased both peak horizontal and vertical velocities and reduced time taken to complete sit‐to‐stand. These improvements were greater than those of the conventional exercise group and control | ||
| McGinley 2012 | Carlton, Australia | Movement strategy training (n=69; 2 hours + 2 hours home practice program, once a week, 8 weeks) | Progressive strength training (n=70; 2 hours + 2 hours home practice program, once a week, 8 weeks) | Life skills control (n=71; 2 hours + 2 hours home practice program, once a week, 8 weeks) | 2 (n=1; unable or unwilling to attend, n=1; death) | 1 (n=1; health reasons) | 12 (n=2; unable or unwilling to attend, n=2; poor health, n=1; preference for exercise group, n=1; death, n=2; health reasons, n=1; unspecified, n=1; group was "depressing", n=2, not exercising or receiving falls education) | Primary: Falls: no. of fallers per group, no. of multiple fallers per group, falls rate over 12 months in each group. Secondary: Number of injurious falls, Walking speed, 6 minute walk test, Timed up and go, UPDRS II and III, PDQ‐39, EuroQol‐5D |
Time to first fall during the intervention phase did not differ across groups. Full trial results not yet published | ||
| Miyai 2000 | Osaka, Japan | Body weight supported treadmill training (n=5; 45 minutes, three times per week, 4 weeks) | Physical therapy (n=5; 45 minutes, three times per week, 4 weeks) | 0 | 0 | UPDRS, UPDRS subscales (mental, ADL, motor and complications), Overground ambulation endurance, Gait speed, No. steps taken for 10 metre walk | Cross‐over trial, combined data presented. Body weight‐supported treadmill training showed greater improvement in UPDRS total, ambulation speed and number of steps than physical therapy arm. Additional data supplied by author allowed data to be separated and there was no difference between arms | ||||
| Miyai 2002 | Osaka, Japan | Body weight supported treadmill training (n=11; 45 minutes, three times per week, 4 weeks) | Physical therapy (n=9; 45 minutes, three times per week, 4 weeks) | 1 (n=1, medication changed) | 3 (n=3, medication changed) | Primary: UPDRS, Gait speed, No. steps taken for 10 metre walk. Secondary: UPDRS subscales (mental, ADL, motor and complications) |
Body weight‐supported treadmill training had significantly greater improvement than the physical therapy group in gait speed at 1 month; and in the number of steps at 1, 3 and 4 months | ||||
| Morris 2009 | Melbourne, Australia | Movement strategy training (n=14; 45 minutes, max 16 sessions over 2 weeks) | Musculoskeletal exercise (n=14; 45 minutes, max 16 sessions over 2 weeks) | 0 | 2 (n=2; lost to follow up, no details) | Primary: UPDRS Motor and ADL (combined). Secondary: 10 m walk test, Timed up and go, 2 min walk test, Balance‐shoulder tug, PDQ‐39 |
The movement strategy training group had a significant improvement in balance compared to the musculoskeletal arm. There were no other differences between treatment arms | ||||
| Palmer 1986 | Minneapolis, Minnesota, USA | United Parkinson Foundation exercise program (n=7; 1 hour, three times per week, 12 weeks) | Upper body karate training program (n=7; 1 hour, three times per week, 12 weeks) | 0 | 0 | Forearm pronation/supination rate, Pursuit score walk index, Degree of activated rigidity, Degree of arm tremor, Activated rigidity, Grip strength, 9‐hole peg test, Minnesota placing and turning test, Arm swings test, Rapid alternating arm movement test, Button board, Putting shirt on and off, Putting shoes and socks on and off, Getting up from chair, Long latency stretch response | Study did not compare differences between treatment arms | ||||
| Pelosin 2010 | Genova, Italy | Action plus physical therapy group (n=9; 1 hour, three times per week, 4 weeks) | Landscape plus physical therapy group (n=9; 1 hour, three times per week, 4 weeks) | 1 (n=1; found to have past history of neurological conditions other than PD or implantation for deep brain stimulation) | 1 (n=1; found to have past history of neurological conditions other than PD or implantation for deep brain stimulation) | FOG Questionnaire and FOG diary, Timed up and go, 10 metre walking test, Tinetti scale part I and II, Berg balance scale, PDQ‐39 |
At post‐test there was no difference between treatment arms | ||||
| Picelli 2012 | Verona, Italy | Robot assisted gait‐training group (n=21; 45 minutes, three times per week, 4 weeks) | Physiotherapy group (n=20; 45 minutes, three times per week, 4 weeks) | 3 (n=3; lack of cooperation) | 2 (n=2; lack of cooperation) | Primary: 10 m walk test, 6 min walk test. Secondary: Spatiotemporal gait parameters including stride length, Parkinson's fatigue scale, UPDRS Total |
Robot assisted gait‐training significantly improved 10 m walk test, 6 min walk test, Parkinson's fatigue scale, UPDRS Total compared to the physiotherapy group |
||||
| Poliakoff 2009 | Manchester, UK | 20 week gym group (n=16; 1 hour, twice a week, 20 weeks) | 10 week gym group (n=16; 1 hour, twice a week, 10 weeks) | 4 (n=1; randomised but did not start intervention, n=3; did not complete or insufficient sessions) | 6 (n=1; randomised but did not start intervention, n=5; did not complete or insufficient sessions) | Simple, choice and serial reaction time, Videotaped motor performance, PDQ‐39, UPDRS III, Illness perceptions (BIPQ), Questionnaire assessing experiences of programme | No significant differences between arms, except for the learning sequence RT outcome | ||||
| Reuter 2011 | Giessen, Germany | Nordic walking group (n=30; 70 minutes, three times per week, 6 months) | Walking group (n=30; 70 minutes, three times per week, 6 months) | Flexibility and relaxation group (n=30; 70 minutes, three times per week, 6 months) | 0 | 0 | 0 | Max walking speed on treadmill, 12 m and 24 m walking test, Stride length, Gait variability, UPDRS, PDQ‐39, Physical activity in everyday life, Adverse effects | Main reported differences were that the Nordic walking group was superior to the walking and flexibility and relaxation programme in improving postural stability, stride length, gait pattern, and gait variability | ||
| Ridgel 2009 | Cleveland, Ohio, USA | Forced exercise group (n=5; 1 hour, 3 times per week, 8 weeks) | Voluntary exercise group (n=5; 1 hour, 3 times per week, 8 weeks) | 0 | 0 | UPDRS part III Manual functional dexterity, Bimanual dexterity, Centre of pressure (CoP) |
UPDRS motor scores showed a significantly greater improvement in the forced exercise arm compared to the voluntary exercise arm. Only forced exercise resulted in significant improvements in bimanual dexterity | ||||
| Robichaud 2012 | Chicago, Illinois, USA | Progressive resistance exercise (n=unknown (total n=48 at 6 month time point); 1 hour, twice per week, 24 months) | Fitness counts (n=unknown (total n=48 at 6 month time point); 1 hour, twice per week, 24 months) | Unknown | Unknown | UPDRS motor, Timed up and go, Berg balance scale, Modified physical performance test | There was no difference between treatment arms | ||||
| Schenkman 2012a | Denver, Colorado, USA | Flexibilty/balance/function exercise group (n=39; 1 hour, 3 times per week for the first 4 months then tapered for 1 month to once monthly sessions out to 16 months) | Aerobic exercise group (n=41; 1 hour, 3 times per week for the first 4 months then tapered for 1 month to once monthly sessions out to 16 months) | Home exercise group (n=41; once monthly supervised sessions) | 3 at 4 months (n=1; health problems, n=2; personal issues) | 7 at 4 months (n=1; not happy with the program, n=2; missed appointment, n=2; health problems, n=1; moved, n=1; deceased) | 6 at 4 months (n=3; not happy with the program, n=1; did not return calls, n=1 unable to commit the time, n=1; missed appointment) | Primary: Overall physical function, Balance ‐ functional reach, Walking economy ‐ VO2 Secondary: UPDRS ADL, UPDRS Motor, PDQ‐39 |
Overall physical function: improvement at 4 months was greater in the Flexibilty/balance/function exercise group than the aerobic and home exercise group. Functional reach was not different between groups. Walking economy: aerobic exercise improved compared to Flexibilty/balance/function exercise group. The only secondary outcome that showed significant differences was UPDRS ADL: Flexibilty/balance/function exercise group performed better than home exercise group at 4 months | ||
| Shankar 2009 | Calgary, Canada | Treadmill with cueing group (n=10; 30 minutes, twice a week, 8 weeks) | Treadmill without cueing (n=9; 30 minutes, twice a week, 8 weeks) | Cueing only group (n=10; 30 minutes, twice a week, 8 weeks) | 0 | 0 | 0 | Gait and Balance Scale, UPDRS III, PDQ‐39 | Limited data. There was no difference between treatment arms | ||
| Shen 2011 | Hong Kong, China | Balance group (n=23; treatment delivered over 12 weeks) | Strength training (n=22; treatment delivered over 12 weeks) | 0 | 0 | Limit of stability, Walking speed, One leg stance time, Activities‐specific balance confidence scale, UPDRS III | Limited data. The balance group improved significantly more than the strength group in movement velocity and one leg stance | ||||
| Shiba 1999 | Kanagawa, Japan | Visual stimulation (n=unknown, total n=8; treated for an unknown period of time) | Auditory stimulation (n=unknown, total n=8; treated for an unknown period of time) | 0 | 0 | Stride length | Stride length was significantly greater after visual stimulation than after auditory stimulation gait training | ||||
| Sigurgeirsson 2009 | Reykjalundur, Iceland | Walking with visual cues (n=unknown, total n=26; 30 minutes, 4 sessions per week, 4 weeks) | Walking without cues (n=unknown, total n=26; 30 minutes, 4 sessions per week, 4 weeks) | Unknown | Unknown | Timed up and go, PDQ‐39 | Limited data. There was no difference between treatment arms for Timed up and go | ||||
| Smania 2010 | Verona, Italy | Balance training (n=33; 50 minutes, 3 times per week, 7 weeks) | General physical exercise (n=31; 50 minutes, 3 times per week, 7 weeks) | 5 (n=2; uncooperativeness, n=3; medical complications) | 4 (n=2; uncooperativeness, n=2; medical complications) | Primary: Berg balance scale, Activities‐specific balance confidence, Postural transfer test, Self destabilization of the centre of foot pressure test, Falls diary. Secondary: UPDRS Total, Modified Hoehn and Yahr, Geriatric depression scale |
There was a significant difference in favour of the balance training arm in the Berg Balance Scale and the self destabilization of the centre of foot pressure test when compared to the general physical exercise group | ||||
| Talakkad 2011 | Bangalore, India | Conventional gait training (n=unknown, total n=60; 8 hours over 4 weeks) | Partial weight supported treadmill training: 20% unweighting (n=unknown, total n=60; 8 hours over 4 weeks) | Control: No specific intervention (n=unknown, total n=60) | Unknown | Unknown | Unknown | Dynamic posturography, UPDRS (total and motor subscore), Beat‐to‐beat finger blood pressure | Limited data. Partial weight supported (‐20%) treadmill training had a significantly greater improvement in UPDRS motor score compared to conventional gait training | ||
| Thaut 1996 | Colorado, USA | Novel rhythmic auditory stimulation group (n=15; 30 minutes per day, total 10.5 hours over 3 weeks) | Standard self paced training group (n=11; 30 minutes per day, total 10.5 hours over 3 weeks) | No treatment group (n=11) | 0 | 0 | 0 | Stride velocity, Stride cadence, Stride length, EMG analysis on leg muscles | Rhythmic auditory stimulation group improved significantly for flat and incline velocity compared to the self paced training. The rhythmic auditory stimulation group's improvements in stride length were only significantly better than the no treatment group and changes in cadence were only significantly higher than the self paced training group | ||
| Toole 2005 | Florida, USA | Standard treadmill group (n=unknown, total n=23; 20 minutes, 3 times per week, 6 weeks) | Unweighted treadmill group (n=unknown, total n=23; 20 minutes, 3 times per week, 6 weeks) | Weighted treadmill group (n=unknown, total n=23; 20 minutes, 3 times per week, 6 weeks) | Unknown | Unknown | Unknown | Balance from dynamic posturography, Berg balance scale, UPDRS, Biomechanical assessment of strength and range of motion, Gait | There was no difference between treatment arms for function and stability in gait and dynamic balance | ||
| Vivas 2011 | A Coruña, Spain | Water based exercise group (n=6; 45 minutes, twice weekly, 4 weeks) | Land based exercise group (n=6; 45 minutes, twice weekly, 4 weeks) | 1 (n=1; influenza ‐ did not receive intervention) | 0 | Functional reach test, Berg balance scale, Gait ‐turn time, velocity, cadence, step amplitude, Timed up and go, UPDRS | The water based exercise group significantly improved Berg Balance Scale and UPDRS compared to the land based exercise group. There was no difference between treatment arms for the remaining outcomes | ||||
| Werner 2010 | New York, USA | Verbal instruction with augmented feedback group (n=6; 90 minutes, 2 times per week, 2 weeks) | Verbal instruction only group (n=6; 90 minutes, 2 times per week, 2 weeks) | 0 | 0 | Stride length, Cadence, Gait velocity, Shoulder excursion | There was no difference between treatment arms | ||||
| Yang 2010 | Taipei, Taiwan | Downhill walking group (n=16; 30 minutes, 3 times per week, 4 weeks) | Physiotherapy group (n=17; 30 minutes, 3 times per week, 4 weeks) | 1 (n=1; low motivation) | 2 (n=1; conflicting work schedule, n=1; transport problem) | Speed, Candence, Stride length, Thoriacic kyphosis, Muscle strength | Downhill walking significantly improved gait speed, stride length and muscle strength of knee extensors compared to physiotherapy | ||||
The physiotherapy interventions were placed into one of the six categories (general physiotherapy, exercise, treadmill training, cueing, dance and martial arts) according to the type of treatment administered. However, the content and delivery of the interventions within each category were diverse and varied substantially. Further, a wide variety of validated and customised outcome measures were used to assess the effectiveness of the physiotherapy interventions. Consequently, it was inappropriate to combine the results of studies or perform any statistical analysis.
Nevertheless, results of the most regularly used outcome measures could be examined on a trial by trial basis. The most frequently reported physiotherapy outcome measures were gait speed and timed up and go. The motor subscales of the UPDRS and PDQ‐39 were the most commonly reported clinician‐rated disability and patient‐rated quality of life outcome measures respectively. Falls data were also considered to be an important outcome in PD. Even in the case of these more widely reported outcome measures, quantitative meta‐analysis could not be performed due to the wide variety of interventions employed by the included studies such that no two studies with comparable interventions assessed the same outcome measure.
Gait speed (m/s)
Gait speed was measured in 19 studies with data available from 15 studies; data were inadequately or not reported for four trials (Juncos 2006; Khallaf 2011; McGinley 2012; Shen 2011). Nine (Almeida 2012; Chaiwanichsiri 2011; Fisher 2008; Hackney 2007; Hass 2006; Li 2012; Miyai 2000; Vivas 2011; Werner 2010) of the 15 studies reported no difference between the two intervention arms. In five studies (Dias 2005 (mean difference between arms 0.34 m/s); Frazzitta 2009 (mean difference between arms 0.1 m/s); Miyai 2002 (mean difference between arms 0.16 m/s); Thaut 1996 (mean difference between arms 0.093 m/s); Yang 2010 (mean difference between arms 0.15 m/s)) the gait speed was significantly increased in the novel experimental arm compared to the comparator arm. The remaining study (Hackney 2009) was a three‐arm trial. Hackney (Hackney 2009) recorded significantly greater gait speed in the tango arm compared to the waltz/foxtrot arm (mean difference between arms 0.06m/s), but not the Tai Chi arm.
Timed up and go (s)
The timed up and go test was reported in 15 studies with data available from 14 studies; data were inadequately or not reported for one study (McGinley 2012). There was no difference between the two intervention arms for 12 studies (Almeida 2012; Braun 2011; Chaiwanichsiri 2011; Hackney 2007; Hackney 2010; Li 2012; Loureiro 2010; Morris 2009; Pelosin 2010; Robichaud 2012; Sigurgeirsson 2009; Vivas 2011). In the Ebersbach (Ebersbach 2010) study, the time taken to complete the timed up and go test was significantly improved (that is reduced) with the Lee Silverman voice treatment (LSVT) BIG arm compared to the Nordic walking and home exercise arms. In the Hackney (Hackney 2009) study, the timed up and go test was significantly improved in the tango arm compared to the waltz or foxtrot and Tai Chi arms.
Falls
Outcome measures that report data on falls are important and pertinent in PD studies. However, only five trials reported data on falls (11%) (Hirsch 1996; Juncos 2006; Li 2012; McGinley 2012; Smania 2010).
Hirsch 1996 reported the effect of training on mean latency to fall (average number of seconds participants swayed before stepping or falling, touching the surrounding panels with hands, or needing assistance from the technician to keep from sitting in the harness) and the proportion of falls (number of trials resulting in falls). There were no significant differences between the combined balance and resistance arm and balance only arm for either outcome.
Juncos 2006 was published in abstract form. There was insufficient information on the falls data collected to allow a description of the manner in which falls were analysed or to give any indication of the result.
Li 2012 monitored falls using daily ‘falls calendars’ that were maintained by study participants. There were no differences between the Tai Chi and resistance training arms.
McGinley 2012 measured the number of fallers, the number of multiple fallers and falls rate. The number of falls during the intervention phase (eight weeks) was significantly lower in the progressive strength training arm compared to the movement strategy training arm (n = 10 versus n = 24; P = 0.006), with the frequency of falls varying markedly. However, the time to first fall did not differ significantly between groups (P = 0.4).
Smania 2010 reported the number of falls by means of a falls diary. A diary of the number of falls, their circumstances, and the consequences for the patient’s health were kept for one month prior to each evaluation session. There was no significant difference between the balance training experimental arm and the general physical exercises arm.
Clinician‐rated disability
UPDRS motor subscale
The motor subscale of the UPDRS was reported in 23 studies with data and information available from 17; data were inadequately or not reported for six studies (Joudoux 2011; Khallaf 2011; Reuter 2011; Shankar 2009; Shen 2011; Toole 2005). There was no difference between the two intervention arms for 14 studies (Almeida 2012; Burini 2006; Fisher 2008; Frazzitta 2009; Hackney 2007; Hackney 2009; Juncos 2006; Li 2012; McGinley 2012; Miyai 2000; Miyai 2002; Poliakoff 2009; Robichaud 2012; Schenkman 2012a). In the Ebersbach 2010 study, the UPDRS motor score was significantly improved in the LSVT BIG arm compared to the Nordic walking and home exercise arms. In the Ridgel 2009 study, UPDRS motor scores showed a significantly greater improvement in the forced exercise arm compared to the voluntary exercise arm. In the Talakkad 2011 study, partial weight supported (‐20%) treadmill training had a significantly greater improvement in UPDRS motor score compared to conventional gait training (no data in publication).
Patient‐rated quality of life
PDQ‐39 (Summary Index)
A total of 13 studies described using data from the PDQ‐39 but the data were only available from eight studies; data were inadequately or not reported in five studies (Joudoux 2011; McGinley 2012; Reuter 2011; Shankar 2009; Sigurgeirsson 2009). Seven studies (Burini 2006; Ebersbach 2010; Juncos 2006; Morris 2009; Pelosin 2010; Poliakoff 2009; Schenkman 2012a) reported no difference between the intervention arms. Only the Hackney 2009 trial reported a significant difference, with quality of life scores significantly improved in the tango arm compared to the waltz or foxtrot and Tai Chi arms.
Adverse events
Nine trials recorded adverse event data (Chaiwanichsiri 2011; Fisher 2008; Li 2012; McGinley 2012; Picelli 2012; Poliakoff 2009; Reuter 2011; Schenkman 2012a; Yang 2010). Minor adverse events such as muscle soreness, falls and dizziness were reported, with none of these trials reporting events significant enough to cause concern over the safety of the intervention.
Compliance
Only 18 of the 43 trials discussed participant compliance, with 13 (Burini 2006; Ebersbach 2010; Hackney 2007; Hackney 2009; Hirsch 1996; Li 2012; McGinley 2012; Miyai 2000; Miyai 2002; Poliakoff 2009; Reuter 2011; Thaut 1996; Toole 2005) quantifying it in some form; however this was difficult to analyse.
Health economics
Only one trial (McGinley 2012) intended to look at health economics. Watts 2008 (See McGinley 2012) published a protocol for economic analysis alongside the McGinley trial. They proposed to evaluate cost‐effectiveness using a three‐way comparison of the cost per fall averted and the cost per quality adjusted life year saved across two physical therapy interventions and a control group.
Discussion
Summary of main results
This review updates the previous Cochrane review published in 2001 (Deane 2001b) comparing the effectiveness of one approach of physiotherapy intervention versus a second approach of physiotherapy intervention for the treatment of PD. The review now includes 43 randomised trials and 1693 participants (compared with seven trials and 142 participants in the 2001 review). Many recent systematic reviews have focused on specific areas of physiotherapy such as exercise, cueing and treadmill training (Allen 2011; Crizzle 2006; Goodwin 2008; Lim 2005; Mehrholz 2010; Nieuwboer 2008). Physiotherapy for PD encompasses a wide range of methods and techniques ranging from standard UK National Health Service (NHS) physiotherapy to exercise regimens and martial arts (Tomlinson 2012). Therefore, it is important that all approaches of physiotherapy intervention are included. Physiotherapy interventions were placed into six categories according to the type of treatment administered. However, the content and delivery of the interventions within each category varied substantially. In view of the disparate study designs, variety of interventions, and the array of outcome measures used the results of individual studies could not be combined using quantitative meta‐analysis methods.
Comparison of different physiotherapy interventions
A recent Cochrane review provided evidence on the short‐term benefit of physiotherapy in the treatment of PD (Tomlinson 2012). However, it did not identify whether any specific type of physiotherapy intervention provides greater benefit. This review aimed to assess this by comparing the effectiveness of one approach of physiotherapy intervention with a second approach of physiotherapy intervention. The various physiotherapy interventions used in the trials included in this review were categorised according to the type of treatment administered to aid comparisons (general physiotherapy, exercise, treadmill training, cueing, dance, martial arts). However, despite categorisation, the techniques employed within each category were diverse. Therefore, it was not possible or appropriate to combine the results by meta‐analysis as any such analysis would be difficult to interpret. It is also difficult to summarise such large amounts of heterogeneous data using a qualitative approach. Consequently, we conclude that there is no robust trial evidence to support any one approach of physiotherapy over another in the treatment of PD.
The content and delivery of the interventions used in the trials included within this review were diverse in nature. Although attempts were made to compare trials that were 'like for like' through the creation of different categories, the interventions delivered varied substantially within these categories. In the future it may be useful to further subcategorise by the primary aim of the trial. For example, categories for the primary aim might be to improve gait or improve a specific problem such as gait freezing or balance, or improve overall PD performance or function. The variation in the therapy delivered is unsurprising. Physiotherapy is an autonomous profession. Physiotherapists use different sets of skills and work within their own scope of practice (Chartered Society of Physiotherapy), and so this variation in the interventions delivered within clinical trials may reflect the diversity of clinical practice. Over the past decade, steps have been taken to try and provide best practice consensus in the form of the Dutch KNGF guidelines for physical therapy in patients with Parkinson’s disease (Keus 2004). However, this publication provides a guidance framework rather than a 'recipe' for treatment. It is therefore important that physiotherapy interventions are compared against each other within rigorous trial designs to determine which are the most effective. This will provide therapists with a menu of treatment strategies that are known to be effective, from which they can devise individualised interventions. However, given the complexity of physiotherapy interventions, it is important that such trials follow the Medical Research Council guidelines for developing and evaluating complex interventions (MRC 2008), which will help standardise interventions. In addition, many of the trials included in this review had interventions that were intensive and for long durations, which may not be feasible in main stream care. Therefore, future trials should be designed such that the interventions are transferable and cost‐effective in main stream care.
Outcome measures
There was a large variety of outcome measures utilised in the different studies included in this review. The majority of the outcomes were standard physiotherapy and PD outcomes. Gait speed, timed up and go, UPDRS motor score and quality of life measured using the PDQ‐39 were the most frequently reported outcome measures within their respective categories. PD is a multidimensional disease and several important outcomes were either poorly or not reported; this includes data on the number of the falls, depression and anxiety and adverse events. Further, many of the outcomes measured were not relevant to the PD patient or carer. There is a need for the use of functional gait outcomes in future trials which look at the impact on the patient during everyday living rather than in a laboratory environment. Further, only one trial intended to look at a health economics analysis of physiotherapy intervention, therefore little is known about the cost‐effectiveness and economic value of this therapy. Future trials should include these outcomes.
Gait speed
Six trials (Dias 2005; Frazzitta 2009; Hackney 2009; Miyai 2002; Thaut 1996; Yang 2010) reported significant differences between the treatment arms for gait speed. The observed differences between treatment arms ranged from 0.06 to 0.34 m/s. In all these trials, with the exception of Hackney 2009, the intervention arm that used cueing or treadmill training methods, or both, was the better treatment arm. The Hackney trial (Hackney 2009) examined dance with the tango arm outperforming the waltz or foxtrot arm. The possible relevance and benefit of these significant differences to patients with PD must be put into context in terms of what is considered a minimally clinically important change (MCIC). Data on what is considered an MCIC are lacking for PD patients, but some data have been reported in stroke patients. In one study, it was reported that an increase in speed of just 0.03 and 0.13 m/s could translate into a change from a limited household to an unlimited household walker, and from an unlimited household walker to a most‐limited community walker, respectively (Perry 1995). Therefore, these differences in gait speed between arms are consistent with the findings reported by Perry (Perry 1995).
Timed up and go
The MCIC in PD patients is thought to be 11 seconds (Steffen 2008). The differences seen between treatment arms in the Ebersbach (Ebersbach 2010) and Hackney trials (Hackney 2009) were much smaller than this (the mean difference between arms ranged from 1.1 to 2 seconds).
UPDRS motor subscale
Three trials reported a significant benefit of one treatment arm in improving UPDRS motor over the other arms. The UPDRS motor score in the LSVT BIG arm in the Ebersbach (Ebersbach 2010) trial improved by 5.05 points, which was significantly different from the two other arms in which the score increased (that is got worse) by 0.53 and 1.68 points in the Nordic walking and home exercise arms, respectively. Ridgel (Ridgel 2009) reported a significant difference in UPDRS motor score between the forced exercise arm (‐16.6 points) and the voluntary exercise arm (3.6 points). Additionally, Talakkad (Talakkad 2011) reported a significantly greater improvement of the UPDRS motor score in the partial weight supported (‐20%) treadmill training compared to conventional gait training, although there were no data in the abstract publication. The MCIC for the UPDRS motor score has been reported in two studies. One analysed data from two independent randomised controlled trials and concluded that the MCIC was five points for the motor score (Schrag 2006). The second study performed a cross‐sectional analysis on 653 PD participants and reported a MCIC of 2.3 to 2.7 points for the motor score (Shulman 2010). Considering the recommendations of both Schrag (Schrag 2006) and Shulman et al (Shulman 2010) the improvements seen in the Ebersbach (Ebersbach 2010) and Ridgel (Ridgel 2009) trials may reflect a MCIC.
Patient‐rated quality of life
A study performed by Peto et al (Peto 2001) to determine the MCIC for the PDQ‐39 Parkinson’s questionnaire reported that a difference of 1.6 on the summary index was a meaningful change. Only the Hackney 2009 trial reported a significant difference, with quality of life scores significantly improved by 7.10 points in the tango arm, which was significantly different from the waltz or foxtrot arm that improved by 0.68 points and the Tai Chi arm which had an increased score of 1.55 points (that is got worse). This improvement in quality of life that was seen in the tango arm is therefore meaningful to patients.
Quality of the evidence
There has been an improvement in the trial methodological quality and reporting since the last Cochrane review (Deane 2001b). The use of more robust randomisation methods, blinding and intention‐to‐treat analyses has increased since the previous review, although it was still inadequate. Of the 43 trials, only 24 trials provided information on the randomisation method (of which eight were considered low risk) and only four used a central independent randomisation procedure to ensure concealment of treatment allocation; 23 trials used blinded assessors and only 10 stated that they used intention‐to‐treat analysis methods. The lack of information in many trial reports may not necessarily indicate lack of implementation within the trial, but without this information provided in the trial publications the level of bias within the individual trials is difficult to assess. The need for further improvement in the methodological quality of trials in physiotherapy for PD was noted recently (Kwakkel 2007; Tomlinson 2012). Future trials must be methodologically sound, large, randomised, and controlled with reporting following CONSORT guidelines (Boutron 2008a; Boutron 2008b).
The trials included in the review were relatively small, with the majority assessing the effect of one approach of physiotherapy intervention versus a second approach of physiotherapy intervention over a short period of time, with limited follow‐up. The overall size of trials has increased (with an average of 39 participants per trial in this review compared to 20 in the previous review), but the number of small and underpowered trials remains a problem. Small trials may be subject to ‘random error’ (Doll 1980) and consequently may give rise to false negative or positive results. Further, it must be noted that the mean age of onset of PD in the participants in the trials was 60 years. This is relatively young as the average age of onset in the PD MED trial is 67 to 69 years (Patel 2010), therefore the results of the trials may not be relevant to the general PD population, in particular older PD patients.
It should also be noted that only 18 of the 43 trials discussed participant compliance. This is surprising as compliance can be an important determinant of the outcomes measured and the acceptability of the interventions being assessed in the trials. Therefore, it would be beneficial if the level of compliance is measured in future trials.
Another limitation is that the follow‐up period in the trials included in this review was relatively short. Outcome measures were assessed in all trials at baseline and immediately or shortly after the intervention had ceased (one or two weeks, with one trial (Ebersbach 2010) assessing at 12 weeks post‐intervention). PD is a long‐term neurodegenerative disease, so it is important that the long‐term effect of treatment is assessed. Only half of the 43 trials followed‐up participants and reported further data during the post‐treatment period (but this could have been only two weeks or up to 12 months post‐treatment). The previous review’s recommendations were for participants to be followed‐up for at least six months. Only two trials did this, reporting follow‐up data at 12 months (McGinley 2012) and at both 6 and 12 months (Werner 2010) post‐treatment. Long‐term data will provide valuable information about the duration of any improvement following therapy.
Reporting biases
Many trials used multiple outcome measures, and in the majority of trials the primary outcome measure was not explicitly stated. Therefore, it was difficult to assess and identify if studies were free of selective outcome reporting.
In order to minimise the risk of publication bias, a comprehensive search was performed of multiple databases, including searching of unpublished and ongoing studies, without any language restrictions. Also, where necessary, authors were contacted to request additional information. However, as with any systematic review, publication bias should still be taken into consideration.
In summary, large, well‐designed randomised trials with improved specific treatment strategies and a follow‐up of at least 12 months that assess the impact of treatment on all aspects of a patient's PD, alongside a health economics assessment, are needed.
Authors' conclusions
Implications for practice.
Considering the small number of participants, the methodological flaws in many of the studies, the wide variety of physiotherapy interventions and outcome measures used, there is insufficient evidence to support the use of one approach of physiotherapy intervention over another for the treatment of PD.
Implications for research.
The majority of the studies included in this review were small and had a short follow‐up period. It is clear that larger randomised controlled trials with longer‐term follow‐up are required, particularly focusing on improving trial methodology and reporting. Rigorous methods of randomisation should be used and the allocation should be adequately concealed. Data should be analysed according to intention‐to‐treat principles and trials should be reported according to the guidelines set out in the CONSORT statement (Boutron 2008a; Boutron 2008b).
This review highlights the variety of physiotherapy interventions being tested for the treatment of PD. There is a need for more specific trials with improved treatment strategies to underpin the most appropriate choice of physiotherapy intervention and the outcomes measured. This review also reinforces the need for the universal employment of clinically relevant, reliable and sensitive outcome measures with a predefined outcome in each trial.
Future trials should, where appropriate, try to follow the Medical Research Council guidelines for developing and evaluating complex interventions (MRC 2008).
Future trials should be designed such that the interventions are transferable and cost‐effective in main stream care.
What's new
| Date | Event | Description |
|---|---|---|
| 13 May 2014 | New citation required but conclusions have not changed | Conclusions not changed |
| 13 May 2014 | New search has been performed | Search updated to 31 January 2012 New studies added, conclusions unchanged |
History
Protocol first published: Issue 4, 2000 Review first published: Issue 1, 2001
| Date | Event | Description |
|---|---|---|
| 29 November 2000 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
We recognise the contributions of all the original trialists and the individuals who performed the trials that contributed to this systematic review, and thank the participants who agreed to help improve the assessment of PD treatment by taking part in these trials.
We acknowledge Parkinson’s UK for funding and the Department of Health whose core support for BCTU made this review possible.
We would also like to thank Ana Verissimo who provided a translation for the Dias 2005 paper.
Appendices
Appendix 1. Search strategies
Cochrane Movement Disorders Specialised Register (search end of January 2012).
#1. SR‐Movement
#2. physiotherapy
#3. exercise
#4. physical therapy
#5. rehabilitation
#6. #2 or #3 or #4 or #5
#7. Parkinson
#8. Parkinsons disease
#9. parkinsonism
#10. #7 or #8 or #9
#11. #1 and #6 and #10
The Cochrane Library and The Cochrane Controlled Trials Register (Wiley online library) (Issue 1, 2012).
#1. MeSH descriptor: [Parkinson Disease] explode all trees
#2. parkinson*
#3. parkinsonism
#4. {or #1‐#3}
#5. MeSH descriptor Physical Therapy (Speciality) explode all trees
#6. MeSH descriptor Physical Therapy Modalities explode all trees
#7. physical therapy
#8. physiotherapy
#9. MeSH descriptor Exercise explode all trees
#10. exercise
#11. MeSH descriptor Rehabilitation explode all trees
#12. rehabilitation
#13. {or #5‐#13}
#14. #4 and #13
MEDLINE (Ovid) 1966 ‐ Jauary (Week 4) 2012.
1. randomized controlled trial.pt
2. controlled clinical trial.pt
3. randomized.ab.
4. placebo.ab.
5. drug therapy.fs.
6. randomly.ab.
7. trial.ab.
8. groups.ab.
9. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8
10. exp animals/ not humans.sh.
11. 9 not 10
12. exp Parkinson Disease/
13. "parkinson*".ab.ti.
14. 12 or 13
15.exp "Physical Therapy (Specialty)"/
16. physiotherapy.mp.
17. exp Exercise/
18. exp Rehabilitation/
19. exercise*.mp. [mp=title, original title, abstract, name of substance word, subject heading word, unique identifier]
20. rehabilitation*.mp. [mp=title, original title, abstract, name of substance word, subject heading word, unique identifier]
21. 15 or 16 or 17 or 18 or 19 or 20
22. 11 and 14 and 21
23. limit 22 to yr="2001 ‐Current"
EMBASE (Ovid) 1974 ‐ January (Week 4) 2012.
1. random$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
2. factorial$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
3. (crossover$ or cross‐over$).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
4. placebo$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
5. (doubl$ adj blind$).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
6. (singl$ adj blind$).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
7. assign$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
8. allocat$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
9. volunteer$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
10. crossover procedure.sh.
11. Double‐blind Procedure.sh.
12. Randomized Controlled Trial.sh.
13. Single‐blind Procedure.sh.
14. 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13
15. exp Parkinson Disease/
16. parkinson*.mp.
17. 15 or 16
18. exp physiotherapy/
19. physical therapy.mp.
20. exp Exercise/
21. exp Rehabilitation/
22. physiotherapy.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
23. exercise.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
24. rehabilitation.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer name]
25. 18 or 19 or 20 or 21 or 22 or 23 or 24
26. 14 and 17 and 25
27. limit 26 to yr="2001 ‐ Current"
CINAHL (EBSCO) (1982‐2012).
S1. (MH "Random Assignment")
S2. (MH "Comparative Studies")
S3. (MH "Clinical Research+")
S4. (MH "Clinical Trials+")
S5. (MH "Evaluation Research+")
S6. TX ((control* or clinic* or prospective*) adj5 (trial* or study or studies))
S7. TX cross*over*
S8. TX (compar* adj5 (trial* or study* or studies))
S9. "random$"
S10. "placebo"
S11. "RCT"
S12. (S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11)
S13. (MH "Parkinson Disease")
S14. "Parkinson*"
S15. "physiotherapy"
S16. (MH "Physical Therapy+")
S17. (MH "Exercise+")
S18. rehabilitation
S19. S13 or S14
S20. S15 or S16 or S17 or S18
S21. S12 and S19 and S20
ISI Web of Science: Science Citation Index Expanded (SCI‐EXPANDED) (1981 to January 2012), ISI Web of Science: Conference Proceedings Citation Index‐Science (CPCI‐S) (1982 to January 2012).
#1. TS=clinical trial*
#2. TS=research design
#3. TS=comparative stud*
#4. TS=evaluation stud*
#5. TS=controlled trial*
#6. TS=follow‐up stud*
#7. TS=prospective stud*
#8. TS=random*
#9. TS=placebo*
#10. TS=(single blind*)
#11. TS=(double blind*)
#12. #11 OR #10 OR #9 OR #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1
#13. TS=(parkinson disease)
#14. TS=parkinson*
#15. #13 OR #14
#16. TS=physiotherap*
#17. TS=(physical therap*)
#18. TS=exercise*
#19. TS=rehabilitation*
#20. #19 OR #18 OR #17 OR #16
#21. #20 AND #15 AND #12
AMED (EBSCO) (1985‐2012).
S1. (MH "Random Assignment")
S2. (MH "Comparative Studies")
S3. (MH "Clinical Research+")
S4. (MH "Clinical Trials+")
S5. (MH "Evaluation Research+")
S6. TX ((control* or clinic* or prospective*) adj5 (trial* or study or studies))
S7. TX cross*over*
S8. TX (compar* adj5 (trial* or study* or studies))
S9. "random$"
S10. "placebo"
S11. "RCT"
S12. (S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11)
S13. (MH "Parkinson Disease")
S14. "Parkinson*"
S15. "physiotherapy"
S16. (MH "Physical Therapy+")
S17. (MH "Exercise+")
S18. rehabilitation
S19. S13 or S14
S20. S15 or S16 or S17 or S18
S21. S12 and S19 and S20
REHABDATA (1995‐2012). Searched using the term Parkinson*
REHADAT (1990 ‐ 2012). Searched using the term Parkinson.
PEDro (1929‐2012). Searched using the term Parkinson.
GEROLIT (1979‐2012). Searched using the terms "parkinson*" AND "physi*", "parkinson*" AND "exercise*", "parkinson* AND rehabilitation*"
LILACS (Virtual Health Library) (1982‐2012); MedCarib (Virtual Health Library) (17th Century‐2012); IMEMR (1984‐2012). Searched using the terms "Parkinson$" AND "physi$", "Parkinson$" AND "exercise$", "Parkinson$" AND "rehabilitat$", "Parkinson$" AND "physiotherap$".
The Cochrane Controlled Trials Register. See the Cochrane Library.
The CentreWatch Clinical Trials listing service. Screened all entries under the Medical Condition 'Parkinson's Disease'.
The metaRegister of Controlled Trial; NIDRR. Searched using the term Parkinson.
ClinicalTrials.gov. Searched using the terms "parkinson" AND "(physical therapy OR physiotherapy OR exercise OR rehabilitation)".
RePORT. Searched using the terms "Parkinson" and "Rehabilitation", "Parkinson" and "Exercise", "Parkinson" and "Physical Therapy", "Parkinson" and "Physiotherapy".
NRR. Searched using the terms "Parkinson" and "Exercise", "Parkinson" and "Exercising", "Parkinson" and "Physiotherapy", "Parkinson" and "Physiotherapies", "Parkinson" and "Physical", "Parkinson" and "rehabilitation", "Parkinson" and "Rehabilitating", "Parkinson" and "Rehabilitate".
Conference Proceedings Citation Index (1982‐2012). See ISI Web of Science.
DISSABS (DISSertation ABStracts) (1999‐2012). Search using the term "parkinson".
Conference Papers Index (ProQuest) (1982‐2012); Index to Theses (1970‐2012); ProQuest dissertations and theses databases (1861‐2012).
Searched using the terms (all(Physical therapy*) OR all(physiotherap*) OR all(exercise) OR all(rehabilitation*)) AND all(parkinson*).
Electronic Theses Online Service (EThOS) (16th Century‐2012). Searched using the terms "parkinson" AND "physical therapy", "parkinson" AND "physiotherapy", "parkinson" AND "exercise", "parkinson" AND "rehabilitation".
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Almeida 2012.
| Methods | Parallel group design Randomised by pulling allocation out of a hat Analysed on a per protocol basis Treated as outpatients for 9 hours over 6 weeks Assessed at baseline, 6 weeks and 12 weeks Assessors were blinded for UPDRS III evaluation |
|
| Participants | 14 participants in the Overground walking group (OG), 14 in the Treadmill walking group (TM) and 14 in the control group (CL). 2 dropouts in TM group, 1 dropout in CL group. Participants' mean age 73.9 years (OG), 63.9 years (TM), 67.4 years (CL); male/female 12/2 (OG), 8/6 (TM), 11/3 (CL); Hoehn and Yahr stage not stated; duration of PD not stated. Inclusion criteria: Confirmed as having clinically typical Parkinson's disease by at least one movement disorders neurologist. Exclusion criteria: Past history of neurological conditions other than Parkinson's disease, orthopaedic or visual disturbances that severely impaired walking ability, unable to independently walk down an 8 metre GAITRite carpet for a total of 10 trials. |
|
| Interventions | OG: Walk down equally spaced transverse lines presented on a 16m carpet. The cues were white lines of tape. Participants asked to walk across the lines, turn and continue back. Spacings were set at 8% greater than the initial step length of any of the groups (70 cm). 30 minute session with mandatory 2 min break every 8 mins, additional rest allowed if necessary but a total of 24 mins walking was required to consider gait session complete. TM: Walk on a treadmill presented with equally distributed standardised transverse white lines. Spacings were set at 8% greater than the initial step length of any of the groups (70 cm). 30 minute session with mandatory 2 min break every 8 mins, additional rest allowed if necessary but a total of 24 mins walking was required to consider gait session complete. CL: Instructed to continue their usual activities. Participants were optimally medicated at time of all training and testing sessions and remained on stable regimen throughout trial period. |
|
| Outcomes | Step length UPDRS III Timed up and go Gait speed Cadence Double support time Step time Step‐to‐step variability, step time variability 30 second chair stand |
|
| Notes | CL arm not included in review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | High risk | Allocation pulled out of hat |
| Concealment of Allocation | High risk | Allocation pulled out of hat |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Analysed on a per protocol basis |
| Withdrawals Described | Low risk | Withdrawals at less than 10% |
| Cointerventions Constant | Low risk | Participants maintained stable drug regiment throughout trial period |
| Comparable arms | Low risk | Same time and attention given to both arms |
| Blinded Assessors | Unclear risk | Assessors blind for UPDRS III evaluation only |
Braun 2011.
| Methods | Parallel group design Random allocation list used for each site with block sizes of 4 Both intention‐to‐treat and per protocol analysis were carried out Treated as outpatients for either 1 hour per week (groups) or 30 mins per week (individuals) over 6 weeks Assessed at baseline (week 0‐1), at 7‐8 weeks and at 3 months (12‐13 weeks) Assessors were blinded |
|
| Participants | 25 participants in the physiotherapy with mental practice group (PT+MP) and 22 in the physiotherapy and relaxation group (PT+R). There were 3 dropouts PT+MP group and 4 in the PT+R group prior to the post‐intervention assessment, and a further 4 dropouts in the PT‐MP group and 3 in the PT‐R group prior to the 3 month follow‐up assessment. Participants' mean age 70 years (PT‐MP), 69 years (PT‐R); Male/female ratio, 17/8 (PT‐MP), 15/7 (PT‐R); Mean Hoehn and Yahr not given; Mean duration of PD 5.2 years (PT‐MP), 6.6 years (PT‐R). Inclusion criteria: Clinically diagnosed adults with PD, sufficient cognitive level and communication skills to engage mental practice. Exclusion criteria: Other conditions such as stroke, rheumatic disease or dementia prior to onset of PD and sufficient to cause persistent premorbid disability. |
|
| Interventions | Participants entering the trial were already receiving physiotherapy. This pre‐existing treatment was continued. The randomly allocated new treatment was incorporated into the participants existing program. PT‐MP: In half hour sessions 10 mins were spent on mental practice, in group sessions of 1 hour, 20 mins were spent on mental practice. Therapy was recorded in pre‐structured files which detailed content and duration. As soon as possible therapists encouraged unguided mental practice. Logs were given to participants to record unguided mental practice behaviour. The main goal of mental practice was to improve locomotor tasks like walking, standing up from a chair or the floor. This was achieved through four steps, explaining the concept, developing imagery techniques, applying mental practice and consolidating. During therapy imagery attempts and overt movements were combined. This information was embedded in the imagery attempts to make them as vivid as possible. The proportions of actual movements and imagery attempts were based on individual preferences. PT‐R: In half hour sessions 10 mins were spent on relaxation, in group sessions of 1 hour, 20 mins were spent on relaxation. Therapy was recorded in pre‐structured files. As soon as possible therapists encouraged unguided relaxation. Logs were given to participants to record unguided practice. Used to control for attention and consisted of treatment according to the national Dutch guidelines with relaxation therapy being incorporated into each session. The amount of relaxation incorporated matched the amount of mental practice in the experimental group. Relaxation followed the principles of progressive muscle relaxation. It was not stated whether drug therapy was kept constant during the trial. |
|
| Outcomes | Patient and therapist perceived effect on walking performance using visual analogue scale Timed up and go 10 m walk test |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria |
| Randomisation Method | Unclear risk | Random allocation list not clear how generated |
| Concealment of Allocation | Low risk | Lists kept by independent 3rd party |
| Similarity at Baseline | Unclear risk | Hoehn and Yahr not stated |
| Intention to Treat Analysis | Unclear risk | Primary analysis was ITT then per protocol was carried out |
| Withdrawals Described | High risk | Withdrawals > 15% prior to post‐intervention assessment |
| Cointerventions Constant | Unclear risk | Not stated whether drug therapy was kept constant during the trial |
| Comparable arms | Low risk | Same time and attention given in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Burini 2006.
| Methods | Cross‐over design Participants coupled consecutively with list of random numbers. Numbers correspond to a sealed envelope containing group allocation Method of analysis not stated Treatment delivered to groups in 45‐50 minute sessions, 3 times per week up to a total of 20 sessions Assessed at Baseline, after 7 weeks of first treatment, after 8 weeks wash‐out period, after 7 weeks of second treatment Assessors were blinded |
|
| Participants | 13 participants in the aerobic training group and 13 in the Qi‐gong group. There were 2 dropouts in each group. Participants' mean age 65.7 years (aerobic training), 62.7 years (Qi‐gong); Male/female ratio, 5/8 (aerobic training), 4/9 (Qi‐gong); Mean Hoehn and Yahr 2.8 (aerobic training), 2.7 (Qi‐gong); Mean duration of PD 11.2 years (aerobic training), 10.6 years (Qi‐gong). Inclusion criteria: PD subjects, stable medication, Hoehn and Yahr stage II to III. Exclusion criteria: Severe cognitive impairment (MMSE < 24), concomitant severe neurologic cardiopulmonary or orthopaedic disorders, specific contraindication to the execution of a cardiopulmonary test or aerobic training, recent participation in any physiotherapy/rehabilitation program during 2 months prior to start of trial. |
|
| Interventions | Aerobic training: Cycle ergometer used with warm‐up, endurance and cool‐down phases in each 45 min session occurring 3 times per week. Qi‐gong: Breathing exercises, stretches, neck and trunk rotation exercises and balance training in the upright position, 50 minute sessions 3 times per week. Drug regimen remained constant throughout trial period. |
|
| Outcomes | UPDRS III UPDRS II Brown's disability scale (BDS) 6‐minute walk test Borg scale for breathlessness Beck depression inventory (BDI) PDQ‐39 Spirometry test Maximum cardiopulmonary exercise test |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Not stated how random number list was generated |
| Concealment of Allocation | High risk | Sealed envelopes |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | High risk | Dropouts at 15% |
| Cointerventions Constant | Low risk | Drug regimen remained constant throughout trial period |
| Comparable arms | Low risk | Same time and attention given to both groups |
| Blinded Assessors | Low risk | Assessors blinded, patients instructed not to discuss treatment schedule |
Chaiwanichsiri 2011.
| Methods | Parallel group design Randomisation method not stated Method of analysis not stated Treated as outpatients for 3 sessions per week and using home practice for 3 sessions per week each lasting 30 minutes over 4 weeks plus 4 week home program Assessed at baseline, immediately after treatment (4 weeks), and after home program at 8 weeks Assessors were blinded |
|
| Participants | 10 participants in the treadmill + music + home‐walking (TMH) group, 10 participants in the treadmill and home‐walking (TH) group, 10 participants in the home‐walking group (H). No dropouts described. Participants' mean age 67.1 years (TMH group), 67.9 years (TH group), 68.6 years (H group); Male/female ratio 10/0 (TMH group), 10/0 (TH group), 10/0 (H group); Mean Hoehn and Yahr score 2.3 (TMH group), 2.5 (TH group), 2.1 (H group); Mean duration of PD 3.7 years (TMH group), 7.4 years (TH group), 4.4 years (H group). Inclusion criteria: Male, 60‐80 years old, PD as diagnosed by attending neurologists, Thai Mental State Examination > 23, stable medications without freezing, no exercise program in last 2 months, no contraindication for exercise, H&Y II‐III, independent walking without use of gait aids. Exclusion criteria: Medication change during study, inability to walk on treadmill, cannot complete 80% of prescribed program. |
|
| Interventions | TMH: 10 minutes of stretching followed by 20 minutes of treadmill training with cueing (music) delivered 3 days per week and home‐walking practised 3 days per week. After treadmill speed was set, the step frequency would be identified by adjustable electrical metronome. The prepared music with the same rhythmic frequency was chosen. Then the participants were training to walk synchronised with the matched music rhythm on the treadmill. This music would be recorded in MP3 for the participants to take home and listen during home practice. Home program consisted of 10 minutes of stretching and 20 minutes walking. After 4 weeks treadmill training ceased but home program was continued for a further 4 weeks. TH: 10 minutes of stretching followed by 20 minutes of treadmill training without cueing delivered 3 days per week and home‐walking, as described above, practised 3 days per week. After 4 weeks treadmill training ceased but home program was continued for a further 4 weeks. H: Home‐walking practised 6 days per week. Patients were excluded if medication was changed during trial period. Patients did not participate in training in 2 months prior to study start. |
|
| Outcomes | Timed up and go Walking speed Step length Cadence Stride length 6‐minute walk test 6 metre walk time Single leg stance UPDRS I, II, III |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Analysis method not stated |
| Withdrawals Described | Unclear risk | Withdrawals not described |
| Cointerventions Constant | Low risk | Patients were excluded if medication changed during trial period |
| Comparable arms | Unclear risk | Home group no therapist time |
| Blinded Assessors | Low risk | Assessors were blinded |
Dias 2005.
| Methods | Parallel group design Randomisation method not stated Method of analysis not stated Treatment delivered in a total of 20 hour long sessions Assessed at baseline, immediately after treatment and 30 days after end of treatment Not stated whether assessors were blinded |
|
| Participants | 8 participants in the physiotherapy and cardiovascular exercise with visual cues (PTCV) group and 8 in the physiotherapy only (PT) group. No dropouts described. Participants mean age 61.5 years (PTCV group), 64.3 years (PT group); Male/female ratio 4/4 (PTCV group), 7/1 (PT group); Mean Hoehn and Yahr 1.6 (PTCV group), 1.7 (PT group); Mean duration of PD 7.4 years (PTCV group), 8.4 years (PT group). Inclusion criteria: Hoehn and Yahr stage ≤3. Exclusion criteria: Any degree of dementia, joint deformations, arthritis, severe pain, other neurological disturbance, submitted to neurological surgery, severe associated pathologies that would impair physiotherapy. |
|
| Interventions | PTCV: 20 sessions of physiotherapy following a protocol that included 15 mins muscular stretching, 30 mins gait training on stable ground with visual cues, 15 mins cardiovascular exercise using ergometric bicycle. PT: Conventional physiotherapy. It was not stated whether drug therapy was kept constant during the trial. |
|
| Outcomes | UPDRS Functional independence measurement scale Berg balance scale Hoehn and Yahr scale |
|
| Notes | Article in Portuguese | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Method of randomisation not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Number of dropouts not stated |
| Cointerventions Constant | Unclear risk | Not stated whether drug regimen remained constant throughout trial period |
| Comparable arms | Low risk | Same number of sessions of active therapy in both arms |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Diehl 2011.
| Methods | Parallel group design Randomisation method not stated Analysis method not stated Treated for 24‐36 sessions, lasting 90 mins each over 12 weeks Assessed at baseline and immediately after treatment Not stated whether assessors were blinded |
|
| Participants | 20 participants were recruited, group split not stated. Dropouts not stated. Baseline characteristics not stated but it was reported that no significant differences were found between groups in pre‐test demographic variables. Inclusion and exclusion criteria not stated. |
|
| Interventions | Group box training: Stretching, lateral foot work, punching various targets, resistance exercises and aerobic training. Traditional group exercises:Stretching, resistance exercises, aerobic and balance activities. It was not stated whether drug therapy was kept constant during the trial. |
|
| Outcomes | Berg balance scale Activities‐specific balance confidence scale Functional reach test Parkinson's disease quality of life scale |
|
| Notes | Abstract only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Eligibility criteria not stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Randomisation method not stated |
| Similarity at Baseline | Low risk | No significant differences were found between groups in pretest demographic variables |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Withdrawals not described |
| Cointerventions Constant | Unclear risk | Not stated whether drug therapy was kept constant during the trial |
| Comparable arms | Low risk | Same time and attention given to both groups |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Ebersbach 2010.
| Methods | Parallel group design Randomly allocated by drawing lots Analysed on a per protocol basis Treatment took place for 1 hour sessions 4 times per week for 4 weeks Assessed at baseline and at 16 weeks Assessors blinded for UPDRS III, not stated for other outcomes |
|
| Participants | 20 participants in LSVT BIG (BIG) group, 19 participants in Nordic walking (WALK) group and 19 participants in the Home exercise (HOME) group. 1 dropout in WALK group and 1 in HOME group. Participants mean age 67.1 years (LSVT BIG group), 65.5 years (WALK group), 69.3 years (HOME group); Male/female ratio 7/13 (LSVT‐BIG group), 7/12 (WALK group), 8/11 (HOME group); Mean Hoehn and Yahr 2.8 (LSVT BIG group), 2.6 (WALK group), 2.5 (HOME group); Mean duration of PD 6.1 years (LSVT‐BIG group), 7.8 years (WALK group), 7.4 years (HOME group). Inclusion criteria: Fulfil diagnostic criteria for IPD, Hoehn & Yahr stage I‐III outpatient treatment, stable medication 4 weeks prior to inclusion. Exclusion criteria: Dementia (MMSE<25), severe depression, disabling dyskinesias, comorbidity affecting mobility or ability to exercise. |
|
| Interventions | LSVT BIG: 50% of exercises consisted of standardized whole‐body movements with maximal amplitude, repetitive multidirectional movements and stretching. 50% of exercise included goal‐directed ADL according to individual needs and preferences. ADL were performed using high amplitude LSVT BIG movements. LSVT BIG was delivered one‐to‐one with intensive motivation and feedback. Participants were constantly encouraged to work with at least ‘80% of their maximal energy’ on every repetition and taught to use bigger movements in routine activities to provide continuous exercise in everyday movements. Participants in all groups were encouraged to exercise regularly at home. Diaries were used to document type and duration of exercise performed in addition to supervised LSVT BIG. WALK: Each session consisted of a standardized protocol for beginners including warming up, practicing Nordic walking and finally a cooling down. Sessions were performed in a local park in groups of 4 or 6 and constantly supervised by the therapist. Participants in all groups were encouraged to exercise regularly at home. Diaries were used to document type and duration of exercise performed in addition to supervised WALK sessions. HOME: 1 hours instruction of domestic training with practical demonstration and training. Exercises included stretching, high‐amplitude movements, as well as active workouts for muscular power and posture. Participants in all groups were encouraged to exercise regularly at home. They received a diary to document type and duration of exercise performed. Changes in medication occurred in 6 patients from each group. |
|
| Outcomes | UPDRS III PDQ‐39 Timed up and go Time to walk 10 m |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | High risk | Randomised by drawing lots |
| Concealment of Allocation | High risk | Randomised by drawing lots |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Analysed on a per protocol basis |
| Withdrawals Described | Low risk | Withdrawals <10% |
| Cointerventions Constant | Unclear risk | Minor changes to medication |
| Comparable arms | Unclear risk | Time and attention greater in LSVT BIG and WALK groups than in HOME group |
| Blinded Assessors | Unclear risk | Assessors blinded for primary outcome, not stated for secondary outcomes |
Fisher 2008.
| Methods | Parallel group design Subjects closed their eyes and selected a card corresponding to 1 of the 3 groups Analysis method not stated Treated as outpatients for 24 sessions over 8 weeks for both treatment arms, 6 sessions over 8 weeks for control group Assessed at baseline and immediately post‐treatment Assessors were blinded |
|
| Participants | 10 participants in treadmill group, 10 participants in physiotherapy group and 10 in the control arm. No dropouts. Participants' mean age, 64.0 years (treadmill), 61.5 years (physiotherapy), 63.1 years (control). Male/female ratio, 6/4 (treadmill), 5/5 (physiotherapy), 8/2 (control). Mean Hoehn and Yahr 1.9 in all 3 groups. Mean duration of PD 1.2 years (treadmill), 0.7 years (physiotherapy), 1.5 years (control). Inclusion criteria: Early stage PD, diagnosis of PD within 3 years of study participation, Hoehn and Yahr stage 1 or 2, 18 years or older, medical clearance from primary care physician to participate in exercise programme, ability to walk. Exclusion criteria: Medical or physical screening examination showed a score of less than 24 on the MMSE, there were physician determined major medical problems such as cardiac dysfunction that would interfere with participation, they had musculoskeletal impairments or excessive pain in any joint that could limit participation in an exercise programme, had insufficient endurance and stamina to participate in exercise 3 times per week for a 1 hour session. |
|
| Interventions | Treadmill: Level of intensity was defined by metabolic equivalents (MET). High intensity exercise greater than 3 METs. Body weight supported (BWS) treadmill training. Goal of each session was to reach and maintain a MET > 3. Exercise progressed by decreasing BWS (initially 10% of participants' bodyweight) and physical assistance, increasing the treadmill speed and time on the treadmill, with the end goal for each participant to walk on the treadmill continuously for 45 min within the MET range. Physiotherapy: Less than 3 METs. This group was representative of general or traditional physical therapy. Each 45 min session was individualised and consisted of activities from 6 categories 1) passive range of motion and stretching 2) active range of motion 3) balance activities 4) gait 5) resistance training 6) practice of functional activities and transitional movements. Control: Zero intensity group. Six 1 hour education classes taken over an 8 week period. All participants were allowed to continue their customary exercise routines and filled out a daily exercise diary. Drug therapy was constant during the trial. |
|
| Outcomes | UPDRS (Total, I, II and III subscores) Hoehn and Yahr Functional assessments Walking tests: average gait velocity, step length, stride length, cadence, double limb support time, ankle, knee, hip rotation Sit‐to‐stand test Transcranial magnetic stimulation (subset) All participants took their customary medications at the same time relative to each assessment |
|
| Notes | Control arm not included in this review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | High risk | Subjects self‐selected a card with eyes closed |
| Concealment of Allocation | High risk | Subjects self‐selected a card with eyes closed |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not described |
| Withdrawals Described | Low risk | No dropouts |
| Cointerventions Constant | Low risk | All medication kept stable during course of study |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded to group allocation |
Frazzitta 2009.
| Methods | Parallel group design Randomisation method not stated Analysis method not stated Treatment was delivered over 4 weeks in 28 sessions lasting 20 mins each Assessed at baseline and immediately after treatment Not stated whether assessors were blinded |
|
| Participants | 20 participants in treadmill with cues group, 20 in Auditory and visual cues group. No dropouts. Participants mean age 71 years for both groups; Male/female ratio not stated; Mean Hoehn and Yahr 3 for both groups; Mean duration of condition 13.2 years (treadmill group), 12.9 years (cued group). Inclusion criteria: Clinically probable IPD, ability to walk without assistance, visual and hearing capacity sufficient to perceive the cues, freezing of gait at the time of peak medication, stable pharmacological treatment, Hoehn & Yahr stage III, no cognitive impairment, MMSE > 26. Exclusion criteria: Neurological condition other than IPD, postural hypertension, cardiovascular disorders, musculoskeletal disorders, vestibular dysfunction limiting locomotion or balance. |
|
| Interventions | Treadmill: Rehabilitation protocol for gait disturbance & freezing that used treadmill training associated with auditory & visual cues. Maximum tolerated walking speed ‐40% used for 2 day warm‐up, then increased by 0.05 stride cycles/second. Visual cue of target on screen that participant had to reach with stride, auditory cue of music at matched frequency. Cued: Visual cue of lines spaced according to individual stride length for gait training coupled with auditory cue of music at frequency matching that used in Treadmill group. It was not stated whether drug therapy was kept constant during the trial. |
|
| Outcomes | UPDRS III Gait speed Freezing of gait questionnaire Stride length 6 minute walking test |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Randomisation method not stated |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Low risk | No dropouts |
| Cointerventions Constant | Unclear risk | Not stated whether drug regimen remained constant throughout trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Hackney 2007.
| Methods | Parallel group design Randomisation method not stated Method of analysis not given Treated as outpatients for 20 sessions each lasting 1 hour delivered over 13 weeks Assessed 1 week prior to treatment and 1 week after treatment Assessors were blinded |
|
| Participants | 9 participants in Tango group, 10 in Exercise group. No dropouts were reported. Participants mean age 72.6 years (Tango), 69.6 years (exercise); Male/female ratio 6/3 (Tango), 6/4 (exercise); Hoehn and Yahr 2.3 (Tango), 2.2 (exercise); Mean duration of condition 6.2 years (Tango), 3.3 years (exercise). Inclusion criteria: Diagnosed with clinically defined IPD, clear benefit from PD medications. |
|
| Interventions | Tango: Progressive Tango dance lessons with postural stretches, balance exercises, Tango‐style, footwork patterns and experimentation with timing of steps to music with and without partner. Exercise: Structured flexibility exercise classes designed for people with PD and/or elderly individuals. Breathing and stretching exercises progressed to resistance and dexterity exercises sometimes using water bottles or yard sticks to provide resistance or leverage. Some exercises done standing or using chair for support and last 10 minutes consisted of core strengthening exercises using floor matts or modified exercises in chair. Drug therapy was kept constant during the trial. |
|
| Outcomes | UPDRS III Berg balance scale Freezing of gait Timed up and go Velocity of walking and dual‐task walking |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion criteria stated, clear definition of disease |
| Randomisation Method | High risk | Numbers drawn from a hat |
| Concealment of Allocation | High risk | Numbers drawn from a hat |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not given |
| Withdrawals Described | Low risk | No dropouts reported |
| Cointerventions Constant | Low risk | Drug regimen remained constant throughout trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Hackney 2009.
| Methods | Parallel group design Randomised by selecting allocation from a hat, carried out by trial investigator Method of analysis not given Treatment delivered in 1 hour sessions twice weekly for a total of 20 sessions Assessed at baseline and within 1 week of completing 20 classes Assessors were blinded |
|
| Participants | 19 participants in tango group, 19 in Waltz/Foxtrot group , 17 in Tai Chi and 20 in control. 5 dropouts in Tango group, 2 dropouts in Waltz/Foxtrot, 4 dropouts in Tai Chi and 3 in control group. Participants mean age 68.2 years (Tango group), 66.8 years (Waltz/Foxtrot group), 64.9 (Tai Chi), 66.5 (control); Male/female ratio 11/3 (Tango group), 11/6 (Waltz/Foxtrot), 11/2 (Tai Chi),12/5 (control); Hoehn & Yahr 2.1 (Tango), 2.0 (Waltz/Foxtrot), 2.0 (Tai Chi), 2.2 (control); Mean duration of condition 6.9 years (Tango), 9.2 years (Waltz/Foxtrot), 8.7 (Tai Chi), 5.9 (control). Inclusion criteria: At least 40 years of age, could stand for at least 30 min, could walk independently 3 or more metres with or without assistive device, diagnosis of IPD using diagnostic criteria for critically defined "definite PD" based upon published standards, patients demonstrated clear benefit from L‐dopa, Hoehn & Yahr I‐III. Exclusion criteria: History of neurological deficit other than PD, patients had been previously screened for dementia by their neurologists and none were diagnosed with dementia. |
|
| Interventions | Waltz/Foxtrot and Progressive Tango: Experience professional ballroom dancer taught progressive Tango, Waltz/Foxtrot lessons. Instructor, equally versed in both dances, attempted to give all students equal time in leading and following dance roles. All steps done in closed practice position, participants maintain contact through upper extremities and face one another. Tai Chi: Progressive lessons on Tai Chi's 1st and 2nd circles of the Yang short style of Cheng Manching taught by experienced instructor. Control: No intervention. Drug therapy was constant during the trial or patients were excluded. |
|
| Outcomes | PDQ‐39 UPDRS III Berg balance scale Tandem stance test Timed up and go test One leg stance test 6 minute walk test Gait |
|
| Notes | Control arm not included in this review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | High risk | Allocation pulled out of hat |
| Concealment of Allocation | High risk | Allocation pulled out of hat |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not given |
| Withdrawals Described | High risk | Withdrawals at 19% |
| Cointerventions Constant | Low risk | Patients excluded if change in medication was required |
| Comparable arms | Low risk | Same time and attention given to both groups |
| Blinded Assessors | Low risk | Assessors blinded |
Hackney 2010.
| Methods | Parallel group design Randomised by selecting allocation from a hat Analysed on an intention‐to‐treat basis Treatment was delivered in 1 hour classes twice a week for 10 weeks Assessed in the week prior to start of treatment, the week following completion of 10 week treatment and 4 weeks after completion of treatment Assessors were blinded |
|
| Participants | 19 participants in the partnered tango group, 20 in the non‐partnered tango group. 7 dropouts in partnered group, 5 in non‐partnered group. Participants mean age 69.6 years in both groups; Male/female ratio 13/6 (partnered), 15/5 (non‐partnered); Mean Hoehn and Yahr 2.5 (partnered) 2.0 (non‐partnered); Duration of condition 9.5 years (partnered), 7.9 years (non‐partnered). Inclusion criteria: PD without a history of other neurological deficits, at least 40 years of age, able to stand for at least 30 minutes and walk independently for 3 or more metres with or without an assistive device, diagnosis of IPD Hoehn and Yahr stages I‐III using diagnostic criteria for clinically defined 'definite PD' and demonstrated clear benefit from L‐dopa. Exclusion criteria not stated. |
|
| Interventions | Both partnered and non‐partnered groups began with identical warm‐ups to upbeat latin music. After warm‐up both classes listened to and danced to identical commercial tango music selections in the same order of presentation. Partnered: both sexes spent equal time leading and following dance steps, performed in a ‘closed practice’ position, an adaptation of the traditional ballroom frame. Participants with PD always danced with individuals without PD. These individuals included caregivers and loved ones who elected to participate in classes as well as young adult volunteers. Non‐partnered: learned the same Argentine ‘leading’ and ‘following’ tango‐based steps as the partner group but performed them without a partner. Caregivers, loved ones and volunteers participated in the nonpartner class also. Participants remained on a steady drug regimen throughout the study |
|
| Outcomes | Tandem stance One leg stance Timed up and go 6 minute walk test Gait velocity Cadence Stride length Swing percentage Double support percentage |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion criteria stated |
| Randomisation Method | High risk | Randomised by selecting allocation from a hat |
| Concealment of Allocation | High risk | Randomised by selecting allocation from a hat |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Analysed on an intention‐to‐treat basis |
| Withdrawals Described | High risk | Withdrawals at 31% |
| Cointerventions Constant | Low risk | Participants remained on a steady drug regimen throughout the study |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Hass 2006.
| Methods | Parallel group design Randomisation method not stated Analysis method not stated Treatment delivered in 1 hour sessions twice a week for a total of 32 sessions Assessment intervals not stated Investigators were blinded |
|
| Participants | 23 participants were recruited into the study. Number of dropouts was not stated. Baseline characteristics for groups not stated. Total mean age 67 years; Hoehn Yahr 2.2. Inclusion criteria: IPD. Exclusion criteria not stated. |
|
| Interventions | Tai Chi: Emphasised physical movements, mind/body coordination & meditation. 8 forms of Tai Chi performed in sessions. Qi‐gong: Emphasised prolonged intense contemplative or deep meditation in 2 postures, seated or lying supine on floor mats. It was not stated whether drug therapy was kept constant during the trial. |
|
| Outcomes | Gait initiation Gait velocity Stride length Stance Double limb support Step duration |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Inclusion criteria IPD only |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Baseline characteristics not split by group |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Withdrawals not described |
| Cointerventions Constant | Unclear risk | Not stated whether drug therapies were kept constant throughout trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Single blind study |
Hirsch 1996.
| Methods | Parallel group design
Randomised according to a computer generated random number list but concealment of allocation not stated Analysed on a per protocol basis Treated as outpatients for an unspecified period of time (3 days/week) for 10 weeks Assessed at baseline, immediately after treatment and 4 weeks later Assessors were not blinded |
|
| Participants | 6 patients in novel combined balance and resistance training group and 9 patients in balance training group. No dropouts stated. Patients mean age 70.8 years (combined), 75.7 years (balance); Male/female ratio not stated; Hoehn and Yahr 1.8 (combined), 1.9 (balance); Duration of condition 5.5 years (combined), 8.3 years (balance). Inclusion criteria: Diagnosed with IPD by neurologist, not participated in any organised balance or muscle strengthening activities before being pre‐tested, ambulatory, not acutely ill, able to follow simple commands, not suffering from unstable cardiovascular disease. Exclusion criteria: Uncontrolled chronic conditions that would interfere with safety and conduct of the training and testing. | |
| Interventions | Combined: Group training in strengthening and balance exercises. Resistance exercises used Nautilus leg extension and side‐lying leg‐flexion machines and therabands. Balance training consisting of gentle sternal or dorsal perturbation and leaning movements designed to enhance limit of stability whilst standing on a firm or a compliant surface. Balance: 'standard' group balance therapy as described above. Medications kept stable throughout trial period. | |
| Outcomes | Balance Muscle strength (subset) : knee extensors, knee flexors, ankle plantar flexors Latency to fall % of trials resulting on falls |
|
| Notes | Randomisation violation; 1 patient who was allocated to the combined therapy group was reassigned to the balance group after 2 weeks of training due to an inguinal hernia making it impossible for him to carry out the strength training | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Low risk | Computer generated random number list |
| Concealment of Allocation | Unclear risk | Method not stated |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Per protocol analysis |
| Withdrawals Described | Low risk | 13% withdrawal rate for muscle strength outcomes only |
| Cointerventions Constant | Low risk | Medications kept stable throughout trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | High risk | Assessors not blinded |
Joudoux 2011.
| Methods | Parallel group design Randomisation method not stated Analysis method not stated Treated for 3 weekly 1 hour sessions for 8 weeks Assessed at baseline, after treatment and after 3 months follow‐up Not stated whether assessors were blinded |
|
| Participants | 50 participants recruited, group split not stated. Dropouts not stated. Patients baseline characteristics not stated. Inclusion criteria: Mild to moderate PD (Hoehn and Yahr II‐III). Exclusion criteria not stated. |
|
| Interventions | Assymmetric motor training Program: Designed to enhance only the agonist activity of the 'body openers' i.e. extension/supination/abduction/external rotation ‐ which is more reduced than their antagonist activity of flexion/protonation/adduction/internal rotation in PD ‐ aiming at re‐balancing forces around joints. Broad program: Standard techniques of passive and active joint mobilisations, balance and gait training, relaxation techniques and respiratory techniques and respiratory work. Not stated whether drug regimen remained constant throughout trial period. |
|
| Outcomes | UPDRS III GMT score Rapid alternating movements Hand writing and spiralography PDQ‐39 Dpression (GDS‐15) Video recording of 8 activities of daily living and biomechanical evaluations |
|
| Notes | Abstract only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Randomisation method not stated |
| Similarity at Baseline | Unclear risk | Group characteristics not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | No dropouts described |
| Cointerventions Constant | Unclear risk | Not stated whether drug regimen remained constant throughout trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Juncos 2006.
| Methods | Parallel group design Method of randomisation not stated Analysed on an intention‐to‐treat basis Treated for 6 months Assessed at baseline then monthly and after last training session Assessors were blinded |
|
| Participants | 56 participants were randomised into Aerobic exercise (AE), Tai Chi Chung (TCC) or Qi Gong (QG) groups. 16 dropouts in total. Group splits not stated. Baseline characteristics for groups not stated. Total mean age 65 years. Inclusion criteria: Ambulatory subjects with IPD, stable medication regimen, MMSE > 24/30. Exclusion criteria not stated. |
|
| Interventions | AE: Moderate intensity walk‐run program with moderate caloric expenditure. TCC: Intermediate intensity to that of AE, low caloric expenditure. QG: Meditation in stillness, minimal caloric expenditure. Drugs stable during therapy. |
|
| Outcomes | UPDRS total UPDRS motor UPDRS ADL PDQ‐39 Clinical global impression Walking speed Falls |
|
| Notes | Abstract and trial registration only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Hoehn and Yahr not stated |
| Intention to Treat Analysis | Unclear risk | Intention‐to‐treat analysis used |
| Withdrawals Described | High risk | Withdrawals to 29% |
| Cointerventions Constant | Low risk | Drugs stable during therapy |
| Comparable arms | Low risk | Same time and attention given to both groups |
| Blinded Assessors | Low risk | Assessors were blinded |
Khallaf 2011.
| Methods | Parallel group design Randomisation method not stated Analysis method not stated Treatment dose not stated Assessment intervals not stated Not stated whether assessors were blinded |
|
| Participants | 15 participants in Physiotherapy and treadmill group (PT + T) and 15 in Physiotherapy only group (PT). Dropouts not described. Participant baseline characteristics not stated. Inclusion/exclusion criteria not stated. |
|
| Interventions | PT + T: Designed physiotherapy program in addition to 20 min of treadmill training. PT: Designed physiotherapy program only. Not stated whether drug therapies were kept constant throughout trial period. |
|
| Outcomes | UPDRS II and III Hamilton rating scale of depression Walking speed Walking distance |
|
| Notes | Abstract only, no contact details found for author | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Inclusion criteria not stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of Randomisation not stated |
| Similarity at Baseline | Unclear risk | Participant baseline characteristics not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Dropouts not described |
| Cointerventions Constant | Unclear risk | Not stated whether drug therapies were kept constant throughout trial period |
| Comparable arms | Unclear risk | No details of intervention schedules |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Li 2012.
| Methods | Parallel group design Randomised by permuted blocks, allocation delivered in sealed envelopes Analysed on an intention‐to‐treat basis Treatment delivered in 2 sessions per week each lasting an hour over 24 weeks Assessed at baseline and post intervention (at 6 months) and at 3 months follow‐up Assessors were blinded |
|
| Participants | 65 participants in Tai Chi group, 65 in resistance group, 65 in the stretching group. 9 dropouts in Tai Chi group, 6 in resistance group, 4 in stretching group. Participants mean age 68 years (Tai Chi), 69 years (resistance), 69 years (stretching); Male/female ratio 45/20 (Tai Chi), 38/27 (resistance), 39/26 (stretching); Mean Hoehn and Yahr not given; Duration of condition 8 years (Tai Chi), 8 years (resistance), 6 years (stretching). Inclusion criteria: Clinical diagnosis of PD, aged 40 ‐ 85 years, Hoehn and Yahr stage I ‐ IV, at least one score of at least 2 or more for at least one limb for the tremor, rigidity, postural stability or bradykinesia items in the motor section of the UPDRS, stable medication use, ability to stand unaided and walk with or without an assistive device, medical clearance for participation and willingness to be assigned to any of the three interventions. Exclusion criteria: Current participation in any other behavioural or pharmacologic study or instructor led exercise program, a MMSE score lower than 24, debilitating conditions or vision impairment that would impede full participation in the study, unavailability during the study period. |
|
| Interventions | Tai Chi: Six Tai Chi movements integrated into an eight‐form routine. The protocol was specifically designed to tax balance and gait by having participants perform symmetric and diagonal movements, such as weight shifting, controlled displacement of the centre of mass over the base of support, ankle sways an anterior –posterior and lateral stepping. The first 10 weeks emphasized the mastery of single forms through multiple repetitions; later weeks focused on repetitions to enhance balance and increase locomotion. Natural breathing was integrated into the training routine. Resistance: Focused on strengthening the muscles that are important for posture, balance and gait. Resistance (with weighted vests and ankle weights) was introduced at week 10. Weight vest resistance was initially set at 1% of body weight and was increased by approx. 1 to 2% of body weight, depending on each participants tolerance, every fifth week until 5% of body weight was achieved. Ankle weights started at 0.45 Kg per limb and were gradually increased to 1.36 Kg. the routine involved 8 to 10 exercises, including forward and side steps, squats, forward and side lunges, and heel and toe raises, performed in 1 to 3 sets of 10 to 15 repetitions. Progression was modified for participants with physical limitations. Natural breathing was emphasized during the training routine. Stretching: This control condition was designed to provide a low intensity exercise program with the social interaction and enjoyment inherent in the two other interventions but without similar training benefits in lower‐extremity weight bearing, strength or balance. The core activities encompassed a variety of seated and standing stretches involving the upper body (neck, upper back, shoulders, chest and arms) and lower extremities (quadriceps, hamstrings, calves and hips) with the use of gentle joint extension and flexion and trunk rotation. Abdominal breathing with an emphasis on inhaling and exhaling to maximum capacity and relaxation of major muscle were also included. There were no significant changes reported in outside physical activity or use of anti‐parkinsonian medication. |
|
| Outcomes | Two indicators of postural stability: maximum excursion and directional control Stride length Walking velocity Strength of bilateral knee extensors and flexors Functional reach test Timed up and go UPDRS III Number of falls |
|
| Notes | 122/195 participants continued with their exercise out to 3 month follow‐up so this is not a clean follow up comparison Stretching arm classed as attention control and not included in this review |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Permuted blocks |
| Concealment of Allocation | High risk | Sealed envelopes used |
| Similarity at Baseline | Unclear risk | Mean Hoehn and Yahr not given |
| Intention to Treat Analysis | Low risk | Intention‐to‐treat analysis used |
| Withdrawals Described | Low risk | Withdrawals <10% |
| Cointerventions Constant | Unclear risk | No significant change in medications |
| Comparable arms | Low risk | Same time and attention given to each group |
| Blinded Assessors | Low risk | Assessors blinded |
Loureiro 2010.
| Methods | Parallel group design Randomisation method not stated Analysis method not stated Treatment delivered in 2 sessions per week over 6 weeks Assessment intervals not stated Not stated whether assessors were blinded |
|
| Participants | 6 participants in conventional physiotherapy (Physio) group, 6 in complimentary activities (CA) group. Mean age 57 (Physio group), 65 (CA group). Inclusion criteria: Hoehn and Yahr II‐III. Exclusion criteria not stated. |
|
| Interventions | Physio: Conventional physiotherapy. CA: Wii fit in addition to conventional physiotherapy. Not stated whether the drug therapy was constant during trial. |
|
| Outcomes | Timed up and go Anterior functional reach |
|
| Notes | Abstract only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Hoehn and Yahr not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Dropouts not described |
| Cointerventions Constant | Unclear risk | Not stated whether drug therapies were kept constant throughout trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Mak 2008.
| Methods | Parallel‐group design Participants randomly allocated to groups by drawing lots Method of analysis not described Treated as outpatients for 4 hours (audio‐visual), 6 hours (exercise) over 4 weeks Assessed at baseline, at 2 weeks, immediately after and 2 weeks after treatment had ended Assessor was blinded |
|
| Participants | 21 participants in the cueing group, 21 participants in the exercise group and 18 in the control group. 2 dropouts from the cueing group, 2 from the exercise group and 4 from the control group. No baseline characteristics given for drop‐outs. Participants' mean age 63 (cueing), 66 (exercise), 63 (control). No data given for the sex of participants. Hoehn and Yahr stage 2.8 (cueing), 2.7 (exercise) and 2.7 (control). Duration of PD 5.9 years (cueing), 6.1 years (exercise), 5.9 years (control). Inclusion criteria: diagnosed with PD according to Quinn, stable on anti‐PD medications without dyskinesia, orthopaedic, arthritic or heart problems, aged between 50‐75 years old, perform sit to stand independently, can follow instructions. No exclusion criteria stated. |
|
| Interventions | Cueing: Audio‐visual cued task‐specific training for 20 min three times per week. Received cued sit‐to‐stand training using Equitest‐Balance Master. Visual cue was given on a computer screen with verbal command as auditory cue. Each task lasted 2 min, repeated once with a 30 second rests in between. Exercise: 45 min of conventional exercise twice a week. Conventional mobility and strengthening exercises for flexors and extensors of trunk, hips, knees and ankles followed by sit‐to‐stand practice. Control: No treatment. Drugs stable during therapy. |
|
| Outcomes | Peak horizontal velocity Peak vertical velocity Movement time 3D Kinematics data of sit‐to‐stand Not stated when during the day tests took place |
|
| Notes | Control group not included in this review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion criteria stated |
| Randomisation Method | High risk | Participants randomised by drawing lots |
| Concealment of Allocation | High risk | Participants randomised by drawing lots |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | High risk | Withdrawals at 13% |
| Cointerventions Constant | Low risk | Medications kept stable throughout trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors blinded |
McGinley 2012.
| Methods | Parallel group design Method of randomisation not stated Analysed on an intention‐to‐treat basis Treated as outpatients for a 2 hour session once per week for 8 weeks plus home practice Assessed at baseline, one week after intervention, at 3 months and 12 months after intervention Assessors blinded. |
|
| Participants | 69 participants in Movement strategy training group (MST), 70 in Progressive strength training group (PST), 71 in Life‐skills control group (LS). 14 dropouts prior to post‐intervention time point. Baseline characteristics not split by group. Participants mean age 67.9 years; Male/female ratio 140/70; Hoehn and Yahr mean score not stated; Duration of condition 6.7 years. Inclusion criteria: Confirmed Idiopathic Parkinson's disease, Hoehn & Yahr stages 0‐4, able to participate in an outpatient exercise program including strength training, willing to complete a falls calendar for 12 months after therapy, able to walk, willing and able to attend the therapy and assessment program. Exclusion criteria: Score less than 24 on mini‐mental state examination, rating greater than 4 on the modified Hoehn & Yahr scale, on major tranquillisers, other medical conditions that could limit or prevent exercising safely at the required intensity, other prior neurological conditions affecting and dementia. |
|
| Interventions | MST: Movement strategies emphasise task specific practice of everyday functional actions such as rolling over, standing up, walking, crossing obstacles and turning. These tasks are practised with strategies such as visual or auditory cues, mental rehearsal and movement planning, conscious attention during the task and breaking the task into a sequence of smaller components. The program is tailored to movement impairments, activity limitations, and cognitive status and learning ability. An individualised home practice session of strategies to practice within the home or community will be completed once a week. Structured falls risk education will also be provided each week. A single home visit will be conducted by a trained therapist or nurse to check compliance with the therapy program. PST: Strengthening exercises for quadriceps, hip and trunk extensor muscles, hip abductors, calf, and ankle dorsiflexors, tailored to individual’s strength and functional ability. Where possible training is performed in functional tasks such as standing up from a chair, stepping up onto a step etc, using body weight, weighted vests and Thera‐band® to progress the resistance. Structured falls risk education will be provided each week. An individualised home practice session of strengthening exercises will also be completed once a week. A single home visit will be conducted by a trained therapist or nurse to check compliance with the therapy program. LS: Equivalent duration to the MST and PST groups. Each session led by OTs, PTs, Speech pathologists or social workers and included content such as relaxation, games, or communication activities. Guided discussion. Guided discussion will also include topics such as the impact of PD on the individual and family, support and resources available and fatigue management. None of the content will relate to walking, balance or falls risk education. A home session of reflection activities and relaxation practice will also be completed once per week. Not stated whether the drug therapy was constant during treatment. |
|
| Outcomes | Falls: no. of fallers per group, no. of multiple fallers per group, falls rate over 12 months in each group Number of injurious falls Walking speed 6 minute walk test Timed up and go UPDRS II and III PDQ‐39 EuroQol‐5D |
|
| Notes | LS arm not included in this review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Baseline characteristics not split into groups |
| Intention to Treat Analysis | Low risk | Analysed on an intention‐to‐treat basis |
| Withdrawals Described | Low risk | Withdrawals at 7% for post‐intervention time point |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during treatment |
| Comparable arms | Low risk | Same time and attention given to participants in each physio group |
| Blinded Assessors | Low risk | Assessors were blinded |
Miyai 2000.
| Methods | Cross‐over design Randomisation using the envelope method Analysed on an intention‐to‐treat basis Inpatients treated for 12 sessions, each lasting 45 minutes, over 4 weeks Assessed at baseline, after first set of treatment at 4 weeks and after second set of treatment at 8 weeks Assessors were not blinded |
|
| Participants | 5 participants in body‐weight supported treadmill training (BWSTT) and 5 in conventional physiotherapy (PT). No dropouts described. Participants mean age 66 years (BWSTT), 69.3 years (PT); Male/female ratio 2/3 (BWSTT), 3/2 (PT); Hoehn and Yahr 2.8 (BWSTT), 2.9 (PT); Duration of condition 4.9 years (BWSTT), 3.6 years (PT). Inclusion criteria: Hoehn and Yahr stage 2.5 or 3 Parkinson's disease, no dementia MMSE >27. Exclusion criteria not stated. |
|
| Interventions | BWSTT: Walking with 20% bodyweight support (BWS) for 12 minutes, then 4.5 minutes rest, followed by 10% BWS for 12 minutes, another 4.5 minutes rest and finally 12 minutes walking with 0% BWS. Walking speed started at 0.5 km/hr and was ramped up in 0.5 km/hr increments to 3.0 km/hr as tolerated. PT: General conditioning, range of motion exercise, activities of daily living training and gait training. Drug therapy was stable during trial period. |
|
| Outcomes | UPDRS UPDRS subscales (mental, ADL, motor and complications) Overground ambulation endurance Gait speed No. steps taken for 10 metre walk |
|
| Notes | Pre‐crossover data only used | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | High risk | By the envelope method |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Low risk | Analysed on an intention‐to treat basis |
| Withdrawals Described | Low risk | No withdrawals |
| Cointerventions Constant | Low risk | Drug therapy was stable during therapy period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | High risk | Assessors were not blinded |
Miyai 2002.
| Methods | Parallel group design Randomisation was the envelope method Analysed on an intention‐to‐treat basis Treatment delivered for 12 sessions over 1 month, sessions lasted 45 minutes Assessed at baseline, at 1 month, 2 months, 3 months, 4 months, 5 months and 6 months Assessors were not blinded |
|
| Participants | 11 participants in body‐weight supported treadmill training (BWSTT) group and 9 in conventional physiotherapy (PT) group. 4 participants not analysed due to changes in their medication. Participants mean age 69.5 years (BWSTT), 69.8 years (PT); Male/female ratio 5/6 (BWSTT), 5/4 (PT); Hoehn and Yahr 2.9 (BWSTT), 2.8 (PT); Duration of condition 4.1 years (BWSTT), 4.5 years (PT). Inclusion criteria: Diagnosis of Parkinson's disease based on the presence of rest tremor, bradykinesia, rigidity, positive response to l‐dopa and no evidence of vascular lesions on MRI. Hoehn and Yahr stage 2.5 or 3. Exclusion criteria: Dementia, MMSE <27. |
|
| Interventions | BWSTT: Walking with 20% bodyweight support (BWS) for 12 minutes, then 4.5 minutes rest, followed by 10% BWS for 12 minutes, another 4.5 minutes rest and finally 12 minutes walking with 0% BWS. Walking speed started at 0.5 km/hr and was ramped up in 0.5 km/hr increments to 3.0 km/hr as tolerated. PT: General conditioning, range of motion exercise, activities of daily living training and gait training. Changes in medication not allowed. Participants who changed their medication were excluded. |
|
| Outcomes | UPDRS UPDRS subscales (mental, ADL, motor and complications) Gait speed No. steps taken for 10 metre walk |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | High risk | Envelope method used |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Analysed on an intention‐to‐treat basis |
| Withdrawals Described | High risk | Withdrawals at 17% |
| Cointerventions Constant | Low risk | Changes in medication not allowed. Participants who changed their medication were excluded |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | High risk | Assessors were not blinded |
Morris 2009.
| Methods | Parallel group design Randomised using generated random number sequences by an independent university source Method of analysis not stated Treated as inpatients for 2 weeks in 16 sessions each lasting 45 minutes Assessed at baseline, immediately after treatment and at 3 months Assessors were blinded |
|
| Participants | 14 participants in movement strategies (MS) group and 14 in exercise (Ex) group. 2 participants missing from follow‐up in exercise group. Participants mean age 68 years (MS), 66 years (Ex); Male/female ratio, disease severity and duration for groups were not stated. Inclusion criteria: Aged 21 ‐80 years, medically stable, diagnosis of IPD confirmed by a neurologist, >23 MMSE with a minimum of 2 out of 3 on the recall question, Hoehn & Yahr II or III, able to walk 10 metres 3 times without assistance. Exclusion criteria: Unsafe to participate in the therapy programs |
|
| Interventions | MS: Learn how to use cognitive strategies such as focusing their attention on movement and responding to external cues to enhance walking, turning, standing up from a chair and obstacle negotiation. Based on principles of Victorian comprehensive Parkinson's disease program. Ex: Lower limb and trunk strengthening exercises, spinal and lower limb flexibility exercises and receiving feedback on optimal postural alignment for a range positions. Not stated whether the drug therapy was constant during treatment. |
|
| Outcomes | UPDRS Motor UPDRS ADL 10 m walk test Timed up and go 2 min walk test Balance‐shoulder tug PDQ‐39 |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Low risk | Randomised using generated random number sequences by an independent university source |
| Concealment of Allocation | Low risk | Randomised using generated random number sequences by an independent university source |
| Similarity at Baseline | Unclear risk | Only average age of groups given |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Low risk | Withdrawals at 7% |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during treatment |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Palmer 1986.
| Methods | Parallel group design Randomised in pairs matched for stage of disease, sex and age, method not stated Method of analysis not stated Treated as outpatients for 12 weeks in 1 hour sessions 3 times per week Assessed at baseline and immediately after therapy Assessors were blinded |
|
| Participants | 7 participants in United Parkinson Foundation (UPF) exercise program, 7 in upper body karate (UBK) training program. No dropouts were described. Participants mean age 63.9 years (UPF), 65.9 years (UBK); Male/female ratio not stated; Hoehn and Yahr 2.4 (UPF), 2.4 (UBK); Duration of condition not stated. Inclusion criteria: IPD, stabilization on a regimen of pharmacologic therapy, ability to attend the scheduled evaluation and exercise sessions. Exclusion criteria: Physical problems that might cause them to risk injury during exercises. |
|
| Interventions | UPF: Stretch exercises from the UPF exercise program led by a corrective therapist. UBK: Trained in upper body Karate techniques by a rehabilitation nursing student who had a black belt in karate. All karate was done in a seated position. Each session consisted of approximately 15 mins warm‐up stretching exercises, 35 mins karate training and 10 mins cool down stretching exercises. Drug therapy was stable during therapy period. |
|
| Outcomes | Forearm pronation/supination rate Pursuit score walk index Degree of activated rigidity Degree of arm tremor Activated rigidity Grip strength 9‐hole peg test Minnesota placing and turning test Arm swings test Rapid alternating arm movement test Button board Putting shirt on and off Putting shoes and socks on and off Getting up from chair Long latency stretch response |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Randomisation method not stated |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Low risk | No withdrawals |
| Cointerventions Constant | Low risk | Drug therapy was stable during therapy period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Pelosin 2010.
| Methods | Parallel group design Randomised by computerised random‐number generator performed by an independent researcher Method of analysis not stated Treated as outpatients for 4 weeks with hour long sessions delivered 3 times per week Assessed at baseline, 2 days after completion of all therapy sessions and 4 weeks later Assessors were blinded |
|
| Participants | 9 participants in action group, 9 in landscape group. 2 additional patients were recruited but excluded due to past history of neurological conditions other than PD. No dropouts described. Participants mean age 68.8 years (action), 70.2 years (landscape); Male/female ratio not stated; Hoehn & Yahr 2.1 (action), 2.2 (landscape); Duration of condition 11.6 years (action), 9.5 years (landscape). Inclusion criteria: IPD according to the UK PDS BB criteria. All on stable medication regime. Mobile despite occurrence of freezing at least once a week (minimum score of 2 on item 3 of the FOG questionnaire) and for at least 2s (minimum score of 1 on item 4 of FOG‐Q). MMSE > 24. Exclusion criteria not stated. |
|
| Interventions | Action: Instructed to carefully watch 6 video clips (each clip lasting 6 mins) showing strategies useful in circumventing FOG episodes. During each training session 2 video clips (with different sequences of actions) were presented twice. The complexity of movements progressively increased from simple actions to more complex movements. All actions shown in the video clips were performed by a physical therapist. To ensure proper attention during the video presentation, patients were explicitly asked to concentrate on how the actions were performed and were not allowed to imitate any movement. After video clip observation, patients were asked to practice (for the remaining time of the session‐36 min) the observed actions repetitively and accurately according to the instructions of the physical therapist. Landscape: Matched the experimental protocol, with the exception that during each training sessions they watched 2 video clips (presented twice) containing sequences of static pictures of mountains and seaside, countryside, and desert scenes without any living (human or animal) representations. During training sessions, patients in the landscape group performed the same movements/ actions used for the Action group following the physical therapist’s instructions, in the exact order and for the same amount of time. Drug therapy was stable during trial period. |
|
| Outcomes | FOG Questionnaire and FOG diary Timed up and go 10 metre walking test Tinetti scale part I and II Berg balance scale PDQ‐39 |
|
| Notes | Only data for FOG could be extracted from paper | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion criteria stated |
| Randomisation Method | Low risk | Randomised by computerised random‐number generator |
| Concealment of Allocation | Low risk | Randomisation performed by an independent researcher |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated. ITT was not used |
| Withdrawals Described | Low risk | Withdrawals at 10% |
| Cointerventions Constant | Low risk | Drug therapy was stable during trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Picelli 2012.
| Methods | Parallel group design Participants randomised using list, generated by www.randomisation.com kept in locked desk draw Analysed on a per protocol basis Treated as outpatients for 45 minute sessions, 3 times per week for 4 weeks Assessed at baseline, post intervention, and 1 month after treatment Assessors were blinded |
|
| Participants | 21 participants in Robot assisted gait‐training group (RAGT) and 20 participants in physiotherapy group (PT). 3 dropouts in RAGT group and 2 in PT group. Participants' mean age 68.1 years (RAGT), 68.7 years (PT). Male/female ratio, 10/8 (RAGT), 6/12 (PT). Hoehn and Yahr 2.7 (RAGT), 2.7 (PT). Duration of PD 6.6 years (RAGT), 7.4 years (PT). Baseline data not given for drop‐outs. Inclusion criteria: Confirmed PD, Hoehn and Yahr score 2.5 or 3, MMSE score > 23. Exclusion criteria: Severe dyskinesias of "on‐off" phases, change of PD medications during the study, deficits of somatic sensation in the lower limbs, vestibular disorders or paroxysmal vertigo, other neurological orthopaedic conditions involving the lower limbs and cardiovascular comorbidity. |
|
| Interventions | RAGT: 2 motor driven footplates positioned on 2 bars that provide a Robot assisted propulsion by means of a planetary gear system, simulating stance and swing with a ratio of 60% to 40% between the two phases. A progressive reduction of body weight combined with an increase in gait speed. Each training session consisted of 3 parts (each one lasting 10 minutes), with a 5‐minute rest after each of them. Patients were first trained at 20% of body weight supported and at a speed of 1 km/h for 10 minutes; then at 10% of body weight supported and a speed of 1.3 km/hr for 10 mins; and finally, at 0% of body weight supported and a speed of 1.6 km/hr for 10 mins. Patients were instructed to “help” the gait trainer (GT1) gait‐like movement during training. Any patient unable to maintain the chosen pace was excluded from the study. PT: Program included active joint mobilization and conventional gait training. Each treatment session consisted of 2 parts with a 5‐minute rest between them. First patients performed active joint mobilization of the lower limbs (hip, knee and ankle) in the supine and prone positions (10 repetitions of 6 exercises) for 10 minutes (5 minutes per position). Then they performed conventional gait therapy based on the proprioceptive neuromuscular facilitation (PNF) concept for 30 minutes. Among the PNF techniques we facilitated pelvic motion to improve control of the pelvis as a “key point of control” for maintaining a gait pattern. Conventional gait therapy consisted of 10 minutes each of rhythmic initiation, slow reversal and agonistic reversal exercises applied to the pelvic region. The time spent in PNF was equal to that spent in RAGT. The same trained therapist treated all the patients in this group and standardized the duration of each part of the treatment. No changes in medications as this was a criterion for exclusion. |
|
| Outcomes | 10 m walk test 6 min walk test Spatiotemporal gait parameters including stride length Parkinson's fatigue scale UPDRS Total |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Low risk | List generated using www.randomization.com |
| Concealment of Allocation | High risk | List kept by principal investigator |
| Similarity at Baseline | Low risk | No significant difference between groups |
| Intention to Treat Analysis | Unclear risk | Per protocol analysis used |
| Withdrawals Described | High risk | Withdrawals at 12% |
| Cointerventions Constant | Low risk | No changes in medications as this was a criterion for exclusion |
| Comparable arms | Low risk | Same time and attention given to both groups |
| Blinded Assessors | Low risk | Assessors blinded |
Poliakoff 2009.
| Methods | Parallel group design Randomisation method was done by drawing lots and placing allocations in two sets of sealed envelopes for high and low severity of Parkinson's disease Method of analysis was unclear Treatment delivered in two 1 hour sessions per week for 10 or 20 weeks Assessed at baseline, at 10 weeks and 20 weeks Assessors were not blinded |
|
| Participants | 16 participants in 20 week gym group (gym), 16 in 10 week gym group (control). 4 dropouts from gym group and 6 dropouts from control group. Participant mean age 66.6 years (gym), 63.7 years (control); Male/female ratio, 11/5 (gym), 10/6 (control); Hoehn and Yahr not stated; Duration of condition 7.4 years (gym), 4.7 years (control). Inclusion criteria: mild to moderate PD. Exclusion criteria: diagnosed with dementia, attendance of a group exercise class for Parkinson's disease, other neurodegenerative disease, >2weeks holiday booked during the study period. |
|
| Interventions | 20 Week: 20 week biweekly gym training programme at local leisure complex. 1 hours weekly training in the studio and 1 hour in the gym, each run by gym staff with experience of working with PD. Gym sessions consisted of mainly cardiovascular activity, studio sessions emphasised on gait and agility. The patients used external stimuli (such as music) and team working was encouraged. 10 Week: 10 week programme as above starting 10 weeks after baseline assessment. Not clear whether the drug therapy was constant during treatment. |
|
| Outcomes | Simple, choice and serial reaction time Videotaped motor performance PDQ‐39 UPDRS III Illness perceptions (BIPQ) Questionnaire assessing experiences of programme |
|
| Notes | Abstract and manuscript accepted for publication in Neurorehabilitation Data used from assessments at baseline and 20 weeks |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Characteristics of included patients described but not stated whether these items were used for the selection of patients for trial |
| Randomisation Method | High risk | Drawing lots |
| Concealment of Allocation | High risk | Drawing lots |
| Similarity at Baseline | Unclear risk | Limited baseline data |
| Intention to Treat Analysis | Unclear risk | Attempted to assess all participants regardless of whether they had started or completed intervention. ITT not used |
| Withdrawals Described | High risk | Withdrawals at 31% |
| Cointerventions Constant | Unclear risk | Not clear whether the drug therapy was constant during treatment |
| Comparable arms | Unclear risk | Half the amount of time and attention spent with delayed start group |
| Blinded Assessors | High risk | Assessors were not blinded |
Reuter 2011.
| Methods | Parallel group design Randomisation was conducted using a computer generated sequence Method of analysis not stated Treatment delivered in 70 minute sessions 3 times per week for 6 months Assessed at baseline and post‐intervention Assessors were blinded |
|
| Participants | 30 participants in Nordic walking group (NW), 30 in walking group (W) and 30 in flexibility and relaxation group (FR). No dropouts from any group. Participant mean age 62.0 years (NW), 63.0 years (W), 62.1 years (FR); Male/female ratio not stated; Hoehn & Yahr 2.5 (NW), 2.5 (W), 2.4 (FR); Duration of condition 5.3 years (NW), 6.0 years (W), 5.2 years (FR). Inclusion criteria: PD diagnosed using UKBB criteria assessed by movement disorder specialist, Hoehn and Yahr stage II‐III. Exclusion criteria: Severe concomitant disease which limit physical performance, second neurological disease. |
|
| Interventions | NW: Consisted of warming up including some flexibility and strength exercises with and without the poles. One session per week was dedicated to practising NW technique, the other sessions focused on endurance training. Participants were encouraged to increase the intensity of the training by walking faster or uphill and to increase the distance walked. Each training session finished with a cooling down programme. Training sessions took place in a park and a forest near to the university hospital. W: Consisted of warming up, technique training, endurance training and cooling down. Instructors emphasised on arm swing and coordination of upper and lower limbs. One session per week included walking uphill to improve muscle strength. FR: Performed flexibility exercises and relaxation training. The training focused on stretching, improving balance and range of movements. The flexibility and relaxation programme did not include aerobic exercises. Medical treatment was optimised prior to study and minor changes were allowed in 5 patients during trial period. |
|
| Outcomes | Max walking speed on treadmill 12 m and 24 m walking test Stride length Gait variability UPDRS PDQ‐39 Physical activity in everyday life Adverse effects |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Low risk | Computer generated sequence |
| Concealment of Allocation | Unclear risk | Method not stated |
| Similarity at Baseline | Low risk | No significant difference in baseline demographic data |
| Intention to Treat Analysis | Unclear risk | Analysis method not stated |
| Withdrawals Described | Low risk | No dropouts |
| Cointerventions Constant | Unclear risk | Minor changes in 5 patients |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Ridgel 2009.
| Methods | Parallel group design Randomisation method not stated Method of analysis not stated Treatment delivered in 1 hour sessions, 3 times per week for 8 weeks Assessed at baseline, immediately after completion of treatment, and four weeks after completion of treatment Assessors blinded for UPDRS outcome only |
|
| Participants | 5 participants in forced exercise group, 5 in voluntary exercise. No dropouts described. Participants mean age 58 years (forced), 64 years (voluntary); Male/female ratio not stated; Hoehn and Yahr stage not stated; Duration of condition 7.9 years (forced), 4.4 years (voluntary). Inclusion criteria: IPD. Exclusion criteria not stated. |
|
| Interventions | Forced: Tandem stationary bicycle with trainer. Lower extremity forced exercise (FE) intervention using a stationary tandem bicycle. Patient’s pedaling rate was increased to approximately 30% more than their preferred rate. Voluntary: Exercise on a stationary single bicycle. Drug therapy was stable during trial period. |
|
| Outcomes | UPDRS part III Manual functional dexterity Bimanual dexterity Centre of pressure (CoP) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Criteria not stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Hoehn and Yahr not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Low risk | Withdrawals at 10% |
| Cointerventions Constant | Low risk | Drug therapy was stable during trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | High risk | Assessors blinded for UPDRS outcome only |
Robichaud 2012.
| Methods | Parallel group design Method of randomisation not stated Method of analysis not stated Treatment was delivered in 1 hour sessions twice per week for 24 months Assessed at baseline, 6, 12, 18 and 24 months Assessors were blinded |
|
| Participants | Number randomised not stated. 48 patients assessed at 6 months, down to 38 at 24 months. Group split not stated. Group baseline characteristics not stated. Total mean age 59 years, total mean duration of condition 7 years. Eligibility criteria not stated. |
|
| Interventions | Progressive resistance exercise: Weight lifting program. Fitness counts: Flexibility, balance and strengthening program. Not stated whether the drug therapy was constant during treatment. |
|
| Outcomes | UPDRS motor Timed up and go Berg balance scale Modified physical performance test |
|
| Notes | Abstracts and trial registrations only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Eligibility criteria not stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Group baseline characteristics not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | High risk | 21% lost between 6 and 24 months |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during treatment |
| Comparable arms | Low risk | Same time and attention given to both groups |
| Blinded Assessors | Low risk | Assessors blinded |
Schenkman 2012a.
| Methods | Parallel group design Randomised using computer generated assignments kept in opaque, sealed envelopes, unsealed by research assistant after baseline assessment Analysed on an intention‐to‐treat basis Treatment was delivered in 1 hour sessions, 3 times per week for the first 4 months then tapered for 1 month to once monthly sessions out to 16 months. Home exercise group received just once monthly supervised sessions throughout Assessed at baseline, 4 months, 10 months and 16 months Assessors blinded |
|
| Participants | 39 participants in Flexibilty/balance/function exercise group (FBF), 41 in Aerobic exercise group (AE) and 41 in Home exercise group (HE). Participant mean age 64.5 years (FBF), 63.4 years (AE), 66.3 years (HE); Male/female ratio 24/15 (FBF), 26/15 (AE), 26/15 (HE); Hoehn and Yahr 2.3 (FBF), 2.2 (AE), 2.3 (HE); Duration of condition 4.9 years (FBF), 3.9 years (AE), 4.5 years (HE). Inclusion criteria: Primary PD diagnosed by a movement disorders specialist using the UKBBC, lived in the community, ambulated independently, Hoehn & Yahr stage II‐III. Exclusion criteria: Uncontrolled hypertension, on‐state freezing or exercise limitations from other disorders, MMSE<24. |
|
| Interventions | FBF: Individualised spinal and extremity flexibility exercises followed by group balance/functional training. 2 months of flexibility training one‐on‐one with a physical therapist followed by 2 months of small group exercise (up to 6 participants) that included flexibility, balance and functional exercise. AE: Treadmill, bike and/or elliptical trainer. Included 5‐10 min of warm‐up, 30 minutes exercise at 65% to 80% HR max and 5‐10min of cool down. Participants were encouraged to use a treadmill but were permitted to use a stationary bicycle or elliptical trainer. HE: Exercised at home using the National PD Foundation ‘Fitness counts’ program. Consisted of exercises in the home setting utilizing Fitness Counts with a single monthly group exercise session supervised by a physical therapist. Flexibility and strengthening exercises in sitting and standing. Daily walking (no specific guidelines). All participants regardless of group assignment were assisted to develop long term exercise habits. After randomisation and before beginning to exercise, participants met with their trainer to discuss motivation to exercise, potential barriers and strategies to develop exercise habits. Participants were asked to record supervised and home exercise throughout the 16 months. Drug therapy was kept constant for the first 4 months. |
|
| Outcomes | Overall physical function Balance ‐ functional reach Walking economy ‐ VO2 UPDRS ADL UPDRS Motor PDQ‐39 |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Low risk | Computer generated assignment |
| Concealment of Allocation | High risk | Sealed envelopes |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Intention‐to‐treat analysis used |
| Withdrawals Described | High risk | Withdrawals at 21% |
| Cointerventions Constant | Unclear risk | Drug therapy kept constant for first four months only |
| Comparable arms | Unclear risk | HE group received less time and attention than experimental groups |
| Blinded Assessors | Low risk | Assessors were blinded |
Shankar 2009.
| Methods | Parallel group design Randomisation method not stated Method of analysis not stated Treatment was delivered in 30 min sessions, twice a week for 8 weeks Assessed at baseline and at 2 months Assessors were blinded |
|
| Participants | 10 participants in Treadmill with Cueing (TwC) group, 9 in Treadmill without Cueing (T) group and 10 in Cueing only (C) group. No dropouts described. Baseline characteristics not stated for groups. Inclusion criteria: Moderate Parkinson's disease. No exclusion criteria. |
|
| Interventions | TwC: Walking on the treadmill with music for 30 min twice a week. Music was selected based upon participant input and cadence‐matched to the participant's preferred walking speed. T: Walking on the treadmill without music for 30 min twice a week. C: Listening to music for 30 min twice a week. Not stated whether the drug therapy was constant during trial. |
|
| Outcomes | Gait and Balance Scale UPDRS III PDQ‐39 Not stated when examinations took place |
|
| Notes | Abstract only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Criteria not stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Baseline characteristics not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Withdrawals not described |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during trial |
| Comparable arms | Low risk | Same time and attention given to participants in both T and TwC arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Shen 2011.
| Methods | Parallel group design Randomisation method not stated Method of analysis not stated Treatment delivered over 12 weeks Assessed at baseline and immediately after training and at 12 weeks follow‐up Assessors were blinded |
|
| Participants | 23 participants in balance group, 22 in control group. No dropouts described. Participants baseline characteristics not stated. Inclusion criteria: PD patients. Exclusion criteria not stated. |
|
| Interventions | Balance: Task specific to facilitate reaction time and length of compensatory steps during activities with self‐induced perturbation and in response to external perturbation. Control: Strength training of lower limb muscles with moderate intensity. Not stated whether the drug therapy was constant during trial. |
|
| Outcomes | Limit of stability Walking speed One leg stance time Activities‐specific balance confidence scale UPDRS III |
|
| Notes | Abstract only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Criteria not stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Group characteristics not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Withdrawals not described |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during trial |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Shiba 1999.
| Methods | Cross‐over group design
Method of randomisation not stated Method of analysis of the data not stated Treated as outpatients for an unknown period of time. 1 week between each training regimen. Assessed at baseline and immediately after treatment Not stated whether the assessors were blinded |
|
| Participants | 8 participants took part in the study. No dropouts described. Baseline characteristics not stated for groups. Total mean age 65 years; total male/female ratio 3/5. Inclusion criteria: Stable mild to moderate Parkinson's disease. Exclusion criteria not stated. |
|
| Interventions | Visual training: Patients walked over parallel lines at 90 degrees to the direction of travel. Distance apart of lines dependant on patients normal stride length. Auditory stimulation: Patients walked to a rhythm that was 30% of their comfortable walking rhythm. Not stated whether the drug therapy was constant during trial. |
|
| Outcomes | Stride length | |
| Notes | Abstract only. No numerical data available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Criteria not stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Baseline characteristics not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Dropouts not described |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during trial |
| Comparable arms | Unclear risk | Treatment schedules not stated |
| Blinded Assessors | Unclear risk | Not stated whether the assessors were blinded |
Sigurgeirsson 2009.
| Methods | Parallel group design Method of randomisation not stated Method of analysis not stated Treatment delivered in 30 min sessions, 4 sessions per week for 4 weeks Assessed at baseline, immediately after treatment and 3 months after treatment Not stated whether the assessors were blinded |
|
| Participants | 26 participants randomised, group split not stated. No dropouts described. Baseline characteristics of groups not stated.Total mean Hoehn Yahr 2.1. Inclusion and exclusion criteria not stated. |
|
| Interventions | Exercise: Walking with visual cues. Control: Walking without cues. Not stated whether the drug therapy was constant during trial. |
|
| Outcomes | Timed up and go PDQ‐39 |
|
| Notes | Abstract only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Criteria not stated |
| Randomisation Method | Unclear risk | Method not described |
| Concealment of Allocation | Unclear risk | Method of randomisation not described |
| Similarity at Baseline | Unclear risk | Baseline characteristics of groups not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Withdrawals not described |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during trial |
| Comparable arms | Unclear risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Unclear risk | Not stated whether the assessors were blinded |
Smania 2010.
| Methods | Parallel group design Randomisation list used Method of analysis not stated Treated as outpatients in 50 min sessions, 3 times per week for 7 weeks Assessed at baseline, immediately post treatment and 1 month post‐treatment Assessors were blinded |
|
| Participants | 33 participants in balance group, 31 in control group. 5 dropouts in balance group, 4 in control group. Participants mean age 67.6 years (balance), 67.3 years (control); Male/female 14/14 (balance), 15/12 (control); Hoehn and Yahr not stated; Duration of condition 10.4 years (balance), 8.6 years (control). Inclusion criteria: Idiopathic PD and postural instability, Hoehn & Yahr 3‐4, did not require assistance to rise from chairs or beds. Exclusion criteria: Unstable cardiovascular disease or other chronic conditions that could interfere with their safety during testing or training procedures, other neurological conditions or mental deterioration (MMSE <23), severe dyskinesias or ‘on‐off’ phases. |
|
| Interventions | Balance: Each patient was submitted to balance training consisting of exercises aimed at improving both feedforward and feedback postural reactions. Patients were required to repeat exercises from 3 different groups. Group 1: self‐destabilisation of the centre‐of‐body mass (feedforward), group 2 : externally induced destabilisation of the centre‐of‐body mass (feedback), group 3: emphasis of coordination between leg and arm movements during walking as well as locomotor dexterity over an obstacle course and other potentially destabilising activities (continuous feedback and feedforward adjustments). During each session 10 exercises were undertaken, 4 from group 1, 4 from group 2 and 2 from group 3. 5 – 10 repeats of each for 5 mins. Complexity of exercises was increased with patient’s ability. Support was provided by therapist at pelvis or chest when required. Control: Exercises not specifically designed to improve postural reactions. Active joint mobilisation, muscle stretching and motor coordination exercises. During each session 10 exercises were undertaken, 6 in supine position, 2 in the sitting position and 2 in the standing position. 5 – 10 repeats of each for 5 mins. Complexity of exercises was increased with patient’s ability. Drug therapy was stable during trial period. |
|
| Outcomes | Berg balance scale Activities specific balance confidence Postural transfer test Self destabilization of the centre of foot pressure test Falls diary UPDRS Total Modified Hoehn and Yahr Geriatric depression scale |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Charateristics of included patients described but not stated whether these items were used for the selection of patients for trial |
| Randomisation Method | Unclear risk | Randomisation list used |
| Concealment of Allocation | High risk | Randomisation list kept in locked desk of principal investigator |
| Similarity at Baseline | Unclear risk | Hoehn and Yahr scores not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | High risk | Withdrawals at 14% |
| Cointerventions Constant | Low risk | Drug therapy was stable during trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Low risk | Assessors were blinded |
Talakkad 2011.
| Methods | Parallel group design Method of randomisation not stated Method of analysis not described Treated for 8 hours over 4 weeks Assessed at baseline and after 4 weeks of intervention Not stated whether assessors were blinded |
|
| Participants | 60 participants were randomised into this trial. Dropouts were not described. Baseline characteristics of participants were not stated. Eligibility criteria not stated. |
|
| Interventions | Conventional gait training (CGT). Partial weight supported treadmill training: 20% unweighting. Control: No specific intervention. Drug therapy not described. |
|
| Outcomes | Dynamic posturography UPDRS (total and motor subscore) Beat‐to‐beat finger blood pressure |
|
| Notes | Abstract only Control arm not included in this review |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Unclear risk | Eligibility criteria not stated |
| Randomisation Method | Unclear risk | Method of randomisation not stated |
| Concealment of Allocation | Unclear risk | Method of randomisation not stated |
| Similarity at Baseline | Unclear risk | Baseline characteristics not stated |
| Intention to Treat Analysis | Unclear risk | Method of analysis not described |
| Withdrawals Described | Unclear risk | Dropouts not described |
| Cointerventions Constant | Unclear risk | Drug therapy not described |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Thaut 1996.
| Methods | Parallel group design
Randomised using a computerised random number generator
Analysed on an intention‐to‐treat basis
Treated at home or in the community, for 10.5 hours over 3 weeks. Assessed in laboratory, at baseline and immediately after treatment Not stated whether assessors were blinded |
|
| Participants | 15 patients in novel rhythmic auditory stimulation group (RAS), 11 in standard self paced training group (SPT) and 11 in no treatment group (NT). No dropouts noted. Patients mean age 69 years (RAS), 74 years (SPT), 71 (NT); Male/female 10/5 (RAS), 8/3 (SPT), 8/3 (NT); Hoehn and Yahr 2.4 (RAS), 2.5 (SPT), 2.6 (NT); Duration of condition 7.2 years (RAS), 5.4 years (SPT), 8.5 years (NT). Inclusion criteria: IPD with significant gait deficits but able to walk without physical assistance. Exclusion criteria not stated. |
|
| Interventions | RAS: Individual. 30 min/day walking to 3 different tempos of music. For 1st week; normal tempo = pretest cadence, quick = 5‐10% faster, fast = an additional 5‐10% faster. After each week each tempo was increased by 5‐10% to a maximum pace of 130 steps/min.
SPT: Individual. 30 min/day walking at normal, quick and fast speeds. NT: No treatment. Drug therapy was stable during trial period. |
|
| Outcomes | Stride velocity Stride cadence Stride length EMG analysis on leg muscles | |
| Notes | 3 arms to trial; RAS, SPT and no treatment. SPT versus no treatment are compared in 'Physiotherapy for patients with Parkinson's disease' Cochrane review. New correspondence with author on randomisation method | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria confirmed with author correspondence |
| Randomisation Method | Low risk | Randomised using a computerised random number generator |
| Concealment of Allocation | Unclear risk | Method not stated |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Low risk | Analysed on an intention‐to‐treat basis |
| Withdrawals Described | Low risk | No withdrawals |
| Cointerventions Constant | Low risk | Drug therapy was stable during trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Toole 2005.
| Methods | Parallel group design Randomised using table of random numbers Method of analysis not stated Treatment delivered in 20 mins sessions, 3 times per week for 6 weeks Assessed at baseline, within 1 week of completing intervention and 4 weeks later Not stated whether assessors were blinded |
|
| Participants | 23 participants randomised, group split not stated. No dropouts described. Participants mean age 75.4 years standard treadmill group (ST), 76.4 years unweighted treadmill group (UT), 72.0 years weighted treadmill group (WT); Male/female ratio not stated; Hoehn & Yahr 4.8 (ST), 3.6 (UT), 3.4 (WT); Duration of condition not stated. Inclusion criteria: Parkinsonism, Hoehn and Yahr 1‐4. Exclusion criteria: Uncompensated cardiovascular disease, uncontrolled high blood pressure, leg claudication, significant dementia, other disorders of comprehension and/or other medical conditions that would interfere with the participants safety and comfort during submaximal exercise. |
|
| Interventions | ST: Treadmill training with no loading or unloading. UT: Treadmill training assisted by the biodex unweighting system at a 25% body weight reduction for 15 mins then 5 mins with system removed. WT: Treadmill training wearing weighted scuba‐diving belt which increased normal body weight by 5% for 15 mins then 5 mins without belt. Not stated whether the drug therapy was constant during trial. |
|
| Outcomes | Balance from dynamic posturography Berg balance scale UPDRS Biomechanical assessment of strength and range of motion Gait |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Criteria stated |
| Randomisation Method | Unclear risk | Table of random numbers, unclear how generated |
| Concealment of Allocation | Unclear risk | Randomised using table of random numbers |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | Unclear risk | Withdrawals not described |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during trial |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | Unclear risk | Not stated whether assessors were blinded |
Vivas 2011.
| Methods | Parallel group design Randomisation method not stated Method of analysis not stated Treated as outpatients with twice weekly 45 minute sessions for 4 weeks Assessed at baseline, after 4 weeks treatment and at 17 days follow‐up Assessors were not blinded |
|
| Participants | 6 participants in water based exercise group (Water), 6 in land based exercise group (Land). 1 dropout in Water group. Participant mean age 65.7 years (Water), 68.3 years (Land); Male/female ratio 3/3 (Water), 4/2 (Land); Hoehn and Yahr 2.7 (Water), 2.4 (Land); Duration of condition 4.2 (Water), 7.8 (Land). Inclusion criteria: IPD, ability to follow a stable medication schedule, Hoehn & Yahr stage II‐III (Off medication), lack of dementia (MMSE ≥ 24). Exclusion criteria: unable to walk independently, undergone surgical treatment for PD. |
|
| Interventions | Water: Warm‐up exercises, trunk mobility exercises, postural stability exercises, transferring oneself and changing body positions, all carried out in water. Progression was encouraged with introduction of more complex exercises as appropriate. Land: Warm‐up exercises, trunk mobility exercises, postural stability exercises, transferring oneself and changing body positions, all carried out on land. Progression was encouraged with introduction of more complex exercises as appropriate. Medication withheld for 12 hours before evaluations, for OFF‐dose performance. |
|
| Outcomes | Functional reach test Berg balance scale Gait ‐ turn time, velocity, cadence, step amplitude Timed up and go UPDRS |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Unclear risk | Method not stated |
| Concealment of Allocation | Unclear risk | Randomisation method not stated |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Analysis method not stated |
| Withdrawals Described | Low risk | Withdrawals at 8% |
| Cointerventions Constant | Unclear risk | Not stated whether the drug therapy was constant during trial |
| Comparable arms | Low risk | Same time and attention given to both groups |
| Blinded Assessors | High risk | Assessors not blinded |
Werner 2010.
| Methods | Parallel group design Randomised by individual not involved in testing or treatment using a computer generated number list for allocation Analysed on an Intention‐to‐treat basis Treatment delivered in 90 min sessions, 2 times per week for 2 weeks Assessed at baseline (4‐5 days prior to start of intervention), 1 week after training and at 3, 6 and 12 months Assessors were blinded |
|
| Participants | 6 participants in Verbal instruction with augmented feedback group (VIAF), 6 in Verbal instruction only group (VI). 5 dropouts at follow‐up time‐points, group split not stated. Participant mean age 72.8 years (VIAF), 69.3 years (VI); Male/female ratio 5/1 (VIAF), 5/1 (VI); Hoehn and Yahr 2.3 (VIAF), 2.5 (VI); Duration of condition not stated. Inclusion criteria: Adequate vision. Exclusion criteria: MMSE<21, marked dyskinesia or other neurological impairments in addition to PD. Cardiac or musculoskeletal pathology that might impact gait, required an assistive device to walk, had video feedback or gait training previously or had difficulty understanding English. |
|
| Interventions | VIAB: 15 trials, of walking 7.5 m then returning to starting position with instruction to 'Walk as well as you can', per session. Verbal instruction and augmented feedback before each trial and 3 minutes of seated rest between each trial. Verbal instructions were to 'take big step' prior to each trial, during rest period participants were given 3 viewings of video playback of their walking performance from prior trial. On each viewing they were asked to a) focus on step length and comment on what they observed, b) indicate what they planned to do on next attempt. If subject did not comment accurately after viewing video or did not verbalise what they planned to do next, additional verbal 'knowledge of performance' (KP) or suggestions/corrections ('transitional information' (TI)) were provided by the experimenter. VI: Trials conducted in same manner as for VIAB group but during rest period the group engaged in discussion or were given something to read. Drug therapy was stable during trial period. |
|
| Outcomes | Stride length Cadence Gait velocity Shoulder excursion |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion and exclusion criteria stated |
| Randomisation Method | Low risk | Computer generated randomisation |
| Concealment of Allocation | Low risk | Randomised by individual not involved in testing or treatment |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Low risk | Analysed on an intention‐to‐treat basis |
| Withdrawals Described | Low risk | No withdrawals at post‐intervention time point. Withdrawals at 42% for follow up |
| Cointerventions Constant | Low risk | Drug therapy was stable during trial period |
| Comparable arms | Low risk | Same time and attention given to both groups |
| Blinded Assessors | Low risk | Assessors were blinded |
Yang 2010.
| Methods | Parallel group design Randomised by independent arbiter who picked out a sealed envelopes 30 mins before the start of the intervention Method of analysis not stated Treatment delivered in 30 mins sessions, 3 times per week for 4 weeks Assessed at baseline, within 7 days of completion of treatment, 1 month after treatment Assessors were not blinded |
|
| Participants | 16 participants in downhill walking group (DW), 17 in physiotherapy group (PT). 2 dropouts in DW group, 5 dropouts in PT group. Participants mean age 68.1 years (DW), 66.3 years (PT); Male/female 9/6 (DW), 7/8 (PT); Hoehn and Yahr 2.2 (DW), 2.2 (PT); Duration of condition 4.8 years (DW), 5.3 years (PT). Inclusion criteria: Diagnosed with IPD (as defined by the UK Brain Bank Criteria) by a neurologist, Hoehn and Yahr stages I through III, ability to walk independently, stable medication usage, freedom from any other problems that might affect training and ability to understand instructions and follow commands. Exclusion criteria not stated. |
|
| Interventions | DW: Downhill walking training using a treadmill. Subjects walked on a motorized treadmill with a body weight support (BWS) system under the close supervision of a physical therapist. Initially the downhill grade was set at 3%. If subjects could walk with correct erect posture and large strides without stumbling during the training period, the downhill grade was then increased by 1% per training period. Treadmill speed was set at a level that was comfortable for each participant. A BWS of <40% of the body weight was provided and decreased to the maximum extent possible. Rest periods were provided as needed. PT:Conventional therapy training program consisted of flexibility exercises (5 mins), strengthening exercises (7 mins), proprioceptive neuromuscular facilitation, coordination training, balance training (8 mins) and overground walking training (10 mins). Drug therapy was stable during trial period. |
|
| Outcomes | Speed Cadence Stride length Thoriacic kyphosis Muscle strength |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Eligibility Criteria | Low risk | Inclusion criteria stated |
| Randomisation Method | High risk | Randomised by independent arbiter who picked out a sealed envelopes |
| Concealment of Allocation | High risk | Randomised by sealed envelopes |
| Similarity at Baseline | Low risk | Group characteristics similar at baseline |
| Intention to Treat Analysis | Unclear risk | Method of analysis not stated |
| Withdrawals Described | High risk | Withdrawals at 21% |
| Cointerventions Constant | Low risk | Drug therapy was stable during trial period |
| Comparable arms | Low risk | Same time and attention given to participants in both arms |
| Blinded Assessors | High risk | Assessors were not blinded |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Byl 2009 | After contacting the author it was found that the study was not properly randomised |
| Cheon 2012 | Not stated whether patients were randomised into trial. Author contacted but no response |
| Chouza 2011 | Whole body vibration technique not usually used by physiotherapists |
| Cianci 2010 | Excluded as confounded due to use of rolling walker |
| Donovan 2011 | Quasi randomised using alternate allocation |
| Farley 2005 | Insufficient information available from abstract for review and no author correspondence was achieved |
| Filippin 2010 | Single arm study, so not randomised trial |
| Frazzitta 2012 | Comparator arm consists of suggested home exercise and usual care only |
| Gobbi 2009 | Insufficient information available from abstract for review and not stated whether randomisation was carried out |
| Haase 2011 | Single short session of intervention; treatment under one day. Not rehabilitative therapy |
| Kamsma 1995 | Partially randomised with a portion of patients placed in a convenient group based on practical grounds such as availability of transport |
| Klassen 2007 | Difference between the two physiotherapy arms is multidisciplinary education for which the physiotherapy component is unknown |
| Knobl 2011 | Not properly randomised, placed in groups |
| Lee 2011 | Outcomes not relevant, stroke outcomes used and patients trained on one side of the body only |
| Ma 2009 | Crossover trial carried out over one day only |
| Marchese 2000 | Not properly randomised, pseudo‐random number list used |
| Modugno 2010 | Trial included a theatre training arm which could not be considered solely as physiotherapy |
| Munneke 2010 | Randomised trial of systems of care for delivery of physiotherapy, not comparing different physiotherapy techniques |
| Pacchetti 2000 | Two arm trial included active music therapy arm, not considered to be solely physiotherapy intervention |
| Pohl 2003 | Randomised multiple intervention cross‐over, over 4 consecutive days. Randomisation was of the sequence of the interventions, therefore not RCT |
| Rochester 2011 | Excluded as the study was a randomised crossover over a couple of hours |
| Sage 2009a | After contacting the author it was found that the study was not properly randomised |
| Sage 2009b | After contacting the author it was found that the study was not properly randomised |
| Sage 2010 | After contacting the author it was found that the study was not properly randomised |
| Stallibrass 2001 | The method of therapy used ‐ Alexander Technique ‐ is not used by physiotherapists. Therefore this trial was excluded |
| Tamir 2007 | Quasi‐randomised trial using alternate allocation of patients to arms |
| Tickle‐Degnen 2010 | Multidisciplinary rehabilitation trail. Percentage component of physiotherapy was not specified, therefore unable to differentiate the contribution of physiotherapy to any change in the outcome measures |
| Wulf 2009 | Multiple cross‐over trial over a short period of time |
| Yen 2011 | No outcome measures relevant to our review |
Characteristics of ongoing studies [ordered by study ID]
Brauer 2011.
| Trial name or title | Single and dual task gait training in people with Parkinson's disease: A protocol for a randomised controlled trial |
| Methods | Parallel group design Randomised with opaque envelopes containing allocations from a computer generated random number sequence prepared by offsite investigator not involved in recruitment, intervention or data collection Analysed on an intention‐to‐treat basis Treated as outpatients for 40 ‐ 60 minutes session 3 times a week for 4 weeks, setting not stated Assessed at baseline, immediately after treatment and after 6 months follow‐up Assessors blinded |
| Participants | Planning to recruit 60 participants. Inclusion criteria: 18 years or older, IPD diagnosed using UKBB criteria, able to walk 100 m independently with or without gait aids, report reduced step length or slowed gait speed, confirmed by clinical examination, Hoehn and Yahr stage I‐IV. Exclusion criteria: Neurological condition other than PD, musculoskeletal or cardiopulmonary conditions that affect the ability to safely walk, had surgery for PD such as deep brain stimulation, score <24 on the mini‐mental status examination. |
| Interventions | Single task training: One‐to‐one therapy sessions with therapist. Individually progressed program of gait training aimed at improving step length via repeated practice of straight line walking, turning, obstacle negotiation and challenging gait tasks such as increasing speed and altering surface challenges. External cues to increase step length will be used when needed. Instructions will not be given while participant is walking to avoid dual tasking. A home program will be incorporated at week 2 for 6 months, which includes a walking program and a range of balance, strengthening and postural exercises. Dual task training: One‐to‐one therapy sessions with therapist. Aim to improve step length under dual task conditions that is when concurrently performing added cognitive or motor tasks. Participants will undertake repeated practice of walking aiming to improve step length using external cueing techniques including verbal, visual or auditory approaches. Progressing to internal concurrent cueing of appropriate step length. The gait tasks undertaken will be progressed from simple to more complex tasks as outlined for the single task group. In addition a variety of added tasks will be progressively integrated into the training program. These include tasks such as listening, speaking, conversing, generation of simple and complex lists, language, calculation and motor tasks increasing in complexity. Tasks will include those designed to reflect functional everyday activities such as carrying bags, getting keys out of a pocket, counting money, recalling directions or making a shopping list. Complexity will be progressively integrated as more complex tasks result in greater dual task interference with gait in people with PD. If able, participants will be progressed to performing increasingly complex cognitive tasks while concurrently walking. Motor tasks such as carrying and manipulation will also be included as added tasks. |
| Outcomes | Step length Gait speed Cadence Stride length Step length coefficient of variation Double support time Trail making A&B tests Strop colour‐word interference test Digit span test Timed up and go 6‐minute walk test Measures of community mobility questionnaire Activity measured using ActivPAL Quality of life PDQ‐39 EQ‐5D Hoehn and Yahr UPDRS III Freezing of Gait questionnaire Ambulatory self confidence questionnaire Compliance |
| Starting date | |
| Contact information | s.brauer@uq.edu.au |
| Notes | Protocol only |
Protas 2005.
| Trial name or title | Gait and step training to prevent falls in Parkinson's disease |
| Methods | Parallel group design Treatment delivered for 1 hour per day, 3 times per week for 8 weeks Assessed at baseline, at 8 weeks, at 1 month follow‐up and 5 month follow‐up Assessors blinded |
| Participants | Planning to recruit 90 participants. Inclusion criteria: Diagnosis of PD, postural instability ‐ gait disorder predominant PD, history of falls, gait freezing or a positive pull test, stable regimen of medications, ability to stand and walk 3 m without assistance, stage 2 or 3 of the Hoehn and Yahr disability scale and moderate or higher cognitive scores. |
| Interventions | GSP: Gait and step perturbation. Gait training on a treadmill and in a safety harness while walking in four directions: frontwards, backwards, left sideways and right sideways. Training will start with a treadmill speed that is equivalent to fastest overground walking speed for forward walking and fastest possible for other directions and will increase during training. This group will also receive step training while positioned in 4 directions consisting of suddenly turning the treadmill on/off. The subjects will be required to maintain their balance during perturbations. SPT: Seated exercise. This group will receive seated active range of motion, and upper and lower extremity aerobic training. |
| Outcomes | Usual and fastest gait speed 5‐step test UPDRS Gait and balance scale Center for Epidemiological Studies depression scale Cognistat ‐ a co‐morbidity scale Activities balance confidence Physical activity scale for the elderly Limits of stability Falls frequency |
| Starting date | 25th September 2006 |
| Contact information | shinowara@nih.gov |
| Notes |
Schenkman 2012b.
| Trial name or title | Endurance exercise in Parkinson's disease |
| Methods | Parallel group design Randomisation method not stated Treatment was delivered four times a week for 6 months Assessors were blinded |
| Participants | Estimated total enrolment, 126 participants. Three arm trial: No intervention control group (NT), vigorous exercise group (VE), moderate exercise group (ME). Inclusion Criteria: Clinical diagnosis of primary Parkinson's disease, in a Hoehn and Yahr stage less than stage III, disease duration is less than 5 years, not likely to require dopaminergic therapy within 6 months. Exclusion Criteria: Use of any PD medication within 60 days prior to the beginning the study, including levodopa, direct dopamine agonists, amantadine, Rasagiline (Azilect), Selegiline (Eldepryl), Artane (trihexyphenidyl). Duration of previous use of medications for PD that exceeds 90 days. Expected to require dopaminergic therapy in the next 6 months. Poorly controlled or unstable cardiovascular disease. Uncontrolled hypertension. Hypo‐ or hyperthyroidism, abnormal liver function, abnormal renal function. Mild cognitive impairment (Montreal Cognitive Assessment score<26/30). Depression that precludes ability to exercise (Beck depression score>13). Disorders that interfere with ability to perform endurance exercises. Regular participation in vigorous endurance exercise. Evidence of serious arrhythmias or ischemic heart disease. Any clinically significant medical condition, psychiatric condition, drug or alcohol abuse, or laboratory abnormality that would, in the judgment of the investigators, interfere with the ability to participate in the study. |
| Interventions | NT: Control Group. Wait listed to moderate or vigorous exercise after 6 months of no exercise. VE: Endurance exercise at 80‐85% HR max. ME: Endurance exercise at 60 ‐ 65% HR max. |
| Outcomes | Adherence to exercise UPDRS Motor Adverse events |
| Starting date | April 2012 |
| Contact information | lindsey.pederson@ucdenver.edu |
| Notes |
Smith 2009.
| Trial name or title | Strength training and medication effects in Parkinson's disease: effects on hypokinesia in Parkinson's disease |
| Methods | Treated for 12 weeks |
| Participants | Inclusion criteria: Male or female at least 40 years of age, neurologist diagnosed idiopathic PD (using UK Brain Bank Criteria), ambulatory and medically cleared by their physician to participate in an exercise regimen, clinical signs of hypokinesia or postural instability, Folstein Mini‐Mental State Examination score > 23, currently taking dopamine replacement medication. Exclusion criteria: Previous surgical management of PD (pallidotomy, DBS), motor fluctuations and/or dyskinesias uncontrolled by medications, central nervous system disorder (other than PD), myopathic disease (e.g. focal myopathy) that affects skeletal muscle structure/function rheumatological disease that has an effect on muscle and/or mobility, unstable cardiovascular disease that limits exercise abilities, impaired knee flexion, <90°, extreme claustrophobia (secondary to the inability to perform the MRI scans) regular (2‐3 times/week) aerobic or resistance exercise performed over the past 6 months. |
| Interventions | High force resistance training Standard care |
| Outcomes | Muscle structure Muscle force output Hypokinesia |
| Starting date | August 2007 |
| Contact information | sheldon.smith@hsc.utah.edu |
| Notes |
Uc 2010.
| Trial name or title | Effects of aerobic exercise in Parkinson's disease |
| Methods | Assessors blinded |
| Participants | 100 participants to be enrolled. Inclusion criteria: Veteran or non‐veteran, presence of all 3 cardinal features of Parkinson's disease (resting tremor, bradykinesia and rigidity) which must be asymmetrical, Hoehn & Yahr stage I‐III, men or women aged 50‐80 capable of performing the planned exercise programs, intention to remain in the local area over the study period, stable dopaminergic treatment regimen for at least 4 weeks prior to baseline without any clinical need for medication adjustment at the time of screening. Exclusion criteria: Secondary parkinsonism, Parkinson‐plus syndromes, MMSE score<24, participating in an aerobic exercise program, an unstable dosage of drugs active in the central nervous system during the 60 days before the baseline visit, participation in drug studies or the use of investigational drugs within 30 days before screening, structural brain disease, active epilepsy, acute illness or active confounding medical, neurological or musculoskeletal conditions, alcoholism or other forms of drug addiction, inability to complete the graded exercise test, lack of medical clearance from our pulmonologist, intention to move or take > 1 month vacation during the study period, contraindications to MRI or claustrophobia requiring sedation. |
| Interventions | Aerobic exercise in the form of brisk walking using different training formats, four arms: group/continuous, group/interval, single/continuous and single/interval. |
| Outcomes | Cycle ergonometry Functional and morphometric MRI Trophic factor Biomarker assays Safety exams Lab results (ECG, biochemistry, CBC) Tests for Parkinsonism and cognition Questionnaires about quality of life, mood and activities of daily living |
| Starting date | February 2009 |
| Contact information | ergun‐uc@uiowa.edu |
| Notes |
van Nimwegen 2010.
| Trial name or title | ParkFit study: A randomised controlled trial evaluating the effectiveness of a multifaceted behavioural program to increase physical activity in Parkinson patients |
| Methods | Parallel group design Randomised assigned using minimisation algorithm Treatment delivered over 2 years, offered a maximum of 35 sessions per year, each session lasting 30 mins Assessed at baseline, at 6 months, 12 months 18 months and 24 months Assessors were blinded |
| Participants | 586 participants randomised, 299 in ParkFit group and 287 in ParkSafe group. No dropouts described. Baseline characteristics for groups not stated Inclusion criteria: PD according to UKBB criteria, aged between 40 and 75 years, sedentary lifestyle (<3 times a week vigorous‐intensity physical activity for <60 mins or <3 times a week moderate‐intensity physical activity for <150 mins), Hoehn & Yahr score ≤3. Exclusion criteria: Unclear diagnosis (no gratifying and sustained response to dopaminergic therapy), MMSE score <24, unable to complete dutch questionnaires, severe co‐morbidity interfering with daily functioning, daily institutionalised care, deep brain surgery. |
| Interventions | Both interventions were delivered exclusively by experienced therapists who participate in the Dutch ParkinsonNet. ParkFit: Brochure provided, ParkFit, covering specific strategies to promote behavioural change. Physical therapists serve as personal activity coaches who guide patients towards a more active lifestyle, during specific coaching sessions. Patient and coach create activity goals in order to obtain the 6‐month goals. Patients receive a personal ambulatory monitor with automated visual feedback showing the amount of actually delivered daily physical activity, recorded by a triaxial accelerometer. The ParkFit program also included a maximum of 19 physical therapy sessions in year 1 and 23 in year 2. Based on individual disabilities, therapist and patient jointly formulate treatment aims based on the evidence‐based guideline of physical therapy for PD. ParkSafe: Patients receive a brochure, ParkSafe with information about the benefits of physical therapy. Specific emphasis is given to the importance of safety when performing daily activities. Patients receive an individualised physical therapy program. Total of 35 sessions per year: 19 physiotherapy plus 16 coach sessions). Physical therapist and patient jointly formulate the aims of the projected treatment plan, based on individual problems and disabilities. Not stated whether the drug therapy was constant during trial. |
| Outcomes | Level of physical activity 6 minute walk test PDQ‐39 |
| Starting date | September 2008 |
| Contact information | m.munneke@neuro.umcn.nl |
| Notes | Subgroup analysis of those who succeeded in increasing their activity levels versus those who didn't, assessed for disease progression and physical fitness |
Contributions of authors
Claire Tomlinson was involved in searching and selection of studies, data extraction, analysis and interpretation of the review.
Clare Herd was involved in searching and selection of studies, data extraction, analysis and interpretation of the review.
Smitaa Patel was involved in selection of studies, data extraction.
Charmaine Meek was involved in selection of studies, data extraction and provided expert physiotherapy input into the interpretation of the review.
Carl Clarke contributed to the design of the protocol and was involved in the interpretation of the review providing clinical input.
Rebecca Stowe contributed to the design of the protocol and was involved in searching and selection of studies and interpretation of the review.
Laila Shah was involved in searching and selection of studies for the review.
Catherine Sackley contributed to the design of the protocol and provided expert physiotherapy input into the interpretation of the review.
Katherine Deane undertook the 2001 Cochrane Review, and was involved in the interpretation of this review.
Keith Wheatley contributed to the design of the protocol and was involved in the interpretation of the review.
Natalie Ives contributed to the design of the protocol and was involved in the analysis and interpretation of the review.
Sources of support
Internal sources
No sources of support supplied
External sources
Parkinson's UK, UK.
Department of Health, UK.
Declarations of interest
Carl Clarke, Natalie Ives, Charmaine Meek, Smitaa Patel, Catherine Sackley and Keith Wheatley are either recruiting for or involved in the running of the UK PD REHAB trial.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Almeida 2012 {published and unpublished data}
- Almeida QJ, Bhatt H. A manipulation of visual feedback during gait training in Parkinson's disease. Parkinsons Disease 2012:508720. [DOI] [PMC free article] [PubMed] [Google Scholar]
Braun 2011 {published data only}
- Braun S, Beurskens A, Kleynen M, Schols J, Wade D. Rehabilitation with mental practice has similar effects on mobility as rehabilitation with relaxation in people with Parkinson's disease: a multicentre randomised trial. Journal of Physiotherapy 2011;57(1):27‐34. [DOI] [PubMed] [Google Scholar]
Burini 2006 {published and unpublished data}
- Burini D, Farabollini B, Iacucci S, Rimatori C, Riccardi G, Capecci M, et al. A randomised controlled cross‐over trial of aerobic training versus Qigong in advanced Parkinson's disease. Europa Medicophysica 2006;42(3):231‐8. [PubMed] [Google Scholar]
Chaiwanichsiri 2011 {published data only}
- Chaiwanichsiri D. Treadmill and music cueing for gait training in mild to moderate Parkinson's disease. clinicaltrials.gov 2009.
- Chaiwanichsiri D, Wangno W, Kitisomprayoonkul W, Bhidayasiri R. Treadmill training with music cueing: a new approach for Parkinson's gait facilitation. Asian Biomedicine 2011;5(5):649‐54. [Google Scholar]
Dias 2005 {published data only}
- Dias NP, Fraga DA, Cacho EWA, Oberg TD. Training of gait with visual cues in the patient with Parkinson's disease. Fisioterapia em Movimento 2005;18(4):43‐51. [Google Scholar]
Diehl 2011 {published data only}
- Diehl D, Combs S, Staples B. Comparison of boxing training and traditional exercise on balance and quality of life outcomes in persons with Parkinson's disease: a pilot study. Movement Disorders 2011;26:S124. [Google Scholar]
Ebersbach 2010 {published and unpublished data}
- Ebersbach G, Ebersbach A, Edler D, Kaufhold O, Kusch M, Kupsch A, et al. Comparing exercise in Parkinson's disease ‐ The Berlin LSVT (R) BIG study. Movement Disorders 2010;25(12):1902‐8. [DOI] [PubMed] [Google Scholar]
Fisher 2008 {published data only}
- Fisher BE, Wu AD, Salem GJ, Song J, Lin CH, Yip J, et al. The effect of exercise training in improving motor performance and corticomotor excitability in people with early Parkinson's disease. Archives of Physical Medicine and Rehabilitation 2008;89(7):1221‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Frazzitta 2009 {published data only}
- Frazzitta G, Maestri R, Uccellini D, Bertotti G, Abelli P. Rehabilitation treatment of gait in patients with Parkinson's disease with freezing: A comparison between two physical therapy protocols using visual and auditory cues with or without treadmill training. Movement Disorders 2009;24(8):1139‐43. [DOI] [PubMed] [Google Scholar]
Hackney 2007 {published and unpublished data}
- Hackney ME, Kantorovich S, Levin R, Earhart GM. Effects of tango on functional mobility in Parkinson's disease: A preliminary study. Journal of Neurologic Physical Therapy 2007;31(4):173‐9. [DOI] [PubMed] [Google Scholar]
Hackney 2009 {published and unpublished data}
- Hackney ME, Earhart GM. Effects of Dance on Movement Control in Parkinson's Disease: A Comparison of Argentine Tango and American Ballroom. Journal of Rehabilitation Medicine 2009;41(6):475‐81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackney ME, Earhart GM. Health‐related quality of life and alternative forms of exercise in Parkinson disease. Parkinsonism & Related Disorders 2009;15(9):644‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackney ME, Earhart GM. Tai Chi improves balance and mobility in people with Parkinson disease. Gait & Posture 2008;28(3):456‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hackney 2010 {published and unpublished data}
- Hackney ME, Earhart GM. Effects of dance on gait and balance in Parkinson's disease: A comparison of partnered and nonpartnered dance movement. Neurorehabilitation and Neural Repair 2010;24(4):384‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hass 2006 {published data only}
- Hass CJ, Waddell DE, Wolf SL, Juncos JL, Gregor RJ. The influence of tai chi training on locomotor ability in Parkinson's disease. American Society of Biomechanics (www.asbweb.org/conferences/2006/pdfs/154.pdf). 2006:154.
Hirsch 1996 {published and unpublished data}
- Hirsch MA. Activity dependent enhancement of balance following strength and balance training. PhD Thesis, Florida State University 1996. [UMI Number: 9622856]
- Hirsch MA, Toole T, Maitland CG, Rider RA. The effects of balance training and high‐intensity resistance training on persons with idiopathic Parkinson's disease. Archives of Physical Medicine and Rehabilitation 2003;84(8):1109‐17. [DOI] [PubMed] [Google Scholar]
Joudoux 2011 {published data only}
- Joudoux S, Santiago T, Hutin E, Bayle N, Gracies JM. Randomised controlled single‐blind trial comparing two rehabilitation programs in Parkinson's disease at a moderate stage: Methodology. Annals of Physical and Rehabilitation Medicine. Conference proceeding 2011;54:e104. [Google Scholar]
Juncos 2006 {published and unpublished data}
- Juncos JL. Chinese exercise modalities in Parkinson's disease. controlled‐trials.com 2010.
- Juncos JL, Haber M, Waddell D, Gregor R, Wohl SL. A controlled study of aerobic exercise and Chinese exercise modalities in Parkinson disease. Neurology 2006;66(5 Suppl 2):A314. [Google Scholar]
Khallaf 2011 {published data only}
- Khallaf MES, Fathy H. Influence of moderate aerobic exercises on activities of daily living and depression in patients with Parkinson's disease. European Journal of Neurology. Conference proceeding 2011;18:439. [Google Scholar]
Li 2012 {published data only}
- Li F, Fitzgerald K. Postural stability in Parkinson's disease patients after Tai Chi training: A randomised controlled trial. WFN XIX World Congress on Parkinson's Disease and Related Disorders. 2012; Vol. 18:s155.
- Li F, Harmer P, Fitzgerald K, Eckstrom E, Stock R, Galver J, et al. Tai chi and postural stability in patients with Parkinson's disease. New England Journal of Medicine 2012;366(6):511‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sieber B, Fuzhong L. Tai Chi and Parkinson's disease. Report Database 2008.
Loureiro 2010 {published data only}
- Loureiro APC, Stori FR, Chen R, Ribas CG, Loureiro CC. Comparative study of conventional physiotherapy and virtual rehabilitation using Wii Fit for improvement of balance in Parkinson's disease patients. Movement Disorders 2010; Vol. 25 Suppl 3:S714.
Mak 2008 {published data only}
- Mak MK, Hui‐Chan CW. Effect of 4‐week training with audio‐visual cues on sit‐to‐stand in Parkinsonian patients. Movement Disorders 2005;20 Suppl 10:388. [Google Scholar]
- Mak MKY, Hui‐Chan CWY. Cued task‐specific training is better than exercise in improving sit‐to‐stand in patients with Parkinson's disease: A randomized controlled trial. Movement Disorders 2008;23(4):501‐9. [DOI] [PubMed] [Google Scholar]
McGinley 2012 {published and unpublished data}
- McGinley JL, Martin C, Huxham FE, Menz HB, Danoudis M, Murphy AT, et al. Feasibility, safety, and compliance in a randomized controlled trial of physical therapy for Parkinson's disease. Parkinson's Disease 2012:795294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris ME, Menz HB, McGinley JL, Huxham FE, Murphy AT, Iansek R, et al. Falls and mobility in Parkinson's disease: protocol for a randomised controlled clinical trial. BMC Neurology 2011;11:93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watts JJ, McGinley JL, Huxham F, Menz HB, Iansek R, Murphy AT, et al. Cost effectiveness of preventing falls and improving mobility in people with Parkinson disease: protocol for an economic evaluation alongside a clinical trial. BMC Geriatrics 2008;8:23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Miyai 2000 {published and unpublished data}
- Miyai I, Fujimoto Y, Ueda Y, Yamamoto H, Nozaki S, Saito T, et al. Treadmill training with body weight support: Its effect on Parkinson's disease. Archives of Physical Medicine and Rehabilitation 2000;81(7):849‐52. [DOI] [PubMed] [Google Scholar]
Miyai 2002 {published and unpublished data}
- Miyai I, Fujimoto Y, Yamamoto H, Ueda Y, Saito T, Nozaki S, et al. Long‐term effect of body weight‐supported treadmill training in Parkinson's disease: A randomized controlled trial. Archives of Physical Medicine and Rehabilitation 2002;83(10):1370‐3. [DOI] [PubMed] [Google Scholar]
Morris 2009 {published data only}
- Martin CL, Morris ME, Iansek R. Carry‐over effects of inpatient rehabilitation in Parkinson's disease. Movement Disorders 2008;23 Suppl 1:675. [Google Scholar]
- Morris ME, Iansek R. Effects of strategy training compared to exercises for gait rehabilitation in Parkinson disease: A randomized controlled trial. Movement Disorders 2006;21:688. [Google Scholar]
- Morris ME, Iansek R, Kirkwood B. A randomized controlled trial of movement strategies compared with exercise for people with Parkinson's disease. Movement Disorders 2009;24(1):64‐71. [DOI] [PubMed] [Google Scholar]
- Morris ME, Iansek R, Kirkwood B, Danoudis M, Martin CL. Carry‐over effects of movement strategy training in Parkinson's disease. Movement Disorders 2009;24 Suppl 1:S270. [Google Scholar]
- Schenkman M. Reply: A randomized controlled trial of movement strategies compared with exercise for people with Parkinson's disease. Movement Disorders 2010;25(4):524. [DOI] [PubMed] [Google Scholar]
Palmer 1986 {published data only}
- Palmer SS, Mortimer JA, Webster DD, Bistevins R, Dickinson GL. Comparison of stretch exercises and karate training as therapy for Parkinson's disease. Archives of Physical Medicine and Rehabilitation 1984;65(10):626. [DOI] [PubMed] [Google Scholar]
- Palmer SS, Mortimer JA, Webster DD, Bistevins R, Dickinson GL. Exercise therapy for Parkinson's disease. Archives of Physical Medicine and Rehabilitation 1986;67(10):741‐5. [DOI] [PubMed] [Google Scholar]
Pelosin 2010 {published data only}
- Pelosin E, Avanzino L, Bove M, Stramesi P, Nieuwboer A, Abbruzzese G. Action observation improves freezing of gait in patients with Parkinson's disease. Neurorehabilitation and Neural Repair 2010;24(8):746‐52. [DOI] [PubMed] [Google Scholar]
Picelli 2012 {published data only}
- Picelli A, Melotti C, Origano F, Waldner A, Fiaschi A, Santilli V, et al. Robot‐assisted gait training in patients with Parkinson's disease: A randomized controlled trial. Neurorehabilitation and Neural Repair 2012;26(4):353‐61. [DOI] [PubMed] [Google Scholar]
Poliakoff 2009 {published and unpublished data}
- Poliakoff E, Galpin A, McDonald K, Dick J, Kellett M, Hayes S, et al. The effect of gym training on multiple outcomes in Parkinson's disease: A pilot randomised waiting‐list controlled trial. Movement Disorders 2009;24 Suppl 1:S374. [DOI] [PubMed] [Google Scholar]
Reuter 2011 {published data only}
- Reuter I, Mehnert S, Leone P, Kaps M, Oechsner M, Engelhardt M. Effects of a flexibility and relaxation programme, walking, and nordic walking on Parkinson's disease. Journal of Aging Research 2011;2011:232473. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ridgel 2009 {published data only}
- Ridgel AL, Vitek JL, Alberts JL. Forced, not voluntary, exercise improves motor function in Parkinson's disease patients. Neurorehabilitation and Neural Repair 2009;23(6):600‐8. [DOI] [PubMed] [Google Scholar]
Robichaud 2012 {published and unpublished data}
- Chen D, Corcos DM. Motor deficits ‐ Experimental and clinical correlates. Report Database 2009.
- Corcos D, Robichaud JA, David FJ, Vaillancourt DE, Poon C, Rafferty M, et al. 24 months of exercise improves the motor symptoms in Parkinson's disease. Neurology 2012;78:S02.003. [Google Scholar]
- Rafferty MR, Robichaud JA, David FJ, Poon C, Vaillancourt DE, Comella CL, et al. Long‐term exercise improves and maintains physical function in people with Parkinson's disease. Movement Disorders 2012;27 Suppl 1:S135. [Google Scholar]
- Robichaud JA, Corcos D. The effect of exercise on individuals with Parkinson's disease. ClinicalTrials.gov 2007.
- Robichaud JA, Corcos D. The effect of exercise on individuals with Parkinson's disease. controlled‐trials.gov 2009.
- Robichaud JA, David FJ, Poon C, Rafferty M, Vaillancourt DE, Comella CL, et al. Long‐term progressive exercise improves bradykinesia and muscle weakness. Movement Disorders 2012;27 Suppl 1:S136. [Google Scholar]
Schenkman 2012a {published data only}
- Schenkman M, Hall DA, Baron AE, Schwartz RS, Mettler P, Kohrt WM. Exercise for people in early‐ or mid‐stage Parkinson disease: a 16‐month randomized controlled trial. Physical Therapy 2012;92(11):1395‐410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schenkman M, Shinowara N. Exercise, physical function and Parkinson's disease. Report Database 2009.
- Shinowara N. Gait and step training to prevent fall in Parkinson's disease. Report Database 2009.
Shankar 2009 {published data only}
- Shankar A, Labelle N, Derwent L, Bonfield S, Eliasziw M, Hu B, et al. Treadmill‐walking with music shows a synergistic improvement in gait and balance in patients with Parkinson's disease: A randomized controlled trial. Movement Disorders 2009;24 Suppl 1:S281‐2. [Google Scholar]
Shen 2011 {published and unpublished data}
- Shen X, Mak MKY. Effects of 12‐week strategy‐focused balance training on balance performance and balance confidence in patients with Parkinson's disease. Hong Kong Physiotherapy Journal 2011;29(2):100. [Google Scholar]
Shiba 1999 {published data only}
- Shiba Y, Obuchi S, Toshima H, Yamakita H. Comparison between visual and auditory stimulation in gait training of patients with idiopathic Parkinson's disease. World Congress of Physical Therapy Conference. 1999.
Sigurgeirsson 2009 {published data only}
- Sigurgeirsson AT, Bjarnadottir OH, Thorsteinsdottir MH, Ingvarsson PE. The effect of high‐volume walking with visual cues on gait in Parkinson's patients. A randomised controlled trial. Parkinsonism & Related Disorders 2009; Vol. 15 Suppl 2:S192.
Smania 2010 {published data only}
- Smania N, Corato E, Tinazzi M, Stanzani C, Fiaschi A, Girardi P, et al. Effect of balance training on postural instability in patients with idiopathic Parkinson's disease. Neurorehabilitation and Neural Repair 2010;24(9):826‐34. [DOI] [PubMed] [Google Scholar]
Talakkad 2011 {published data only}
- Gupta A, Ganesan M, Pal P, Talakkad S. Effect of partial weight‐supported treadmill gait training on balance in patients with Parkinson disease. 2011 Annual Assembly of the American Academy of Physical Medicine and Rehabilitation 2011; Vol. 3, issue 10:S163‐4.
- Talakkad S, Ganesan M, Gupta A, Pal PK, Trichur R. Effect of partial weight supported treadmill gait training on cardiovascular dynamics in patients with Parkinson's disease. Movement Disorders 2011;26 Suppl 2:s173. [Google Scholar]
Thaut 1996 {published and unpublished data}
- Thaut MH, McIntosh GC, Rice RR, Miller RA, Rathbun J, Brault JM. Rhythmic auditory stimulation in gait training for Parkinson's disease patients. Movement Disorders 1996;11(2):193‐200. [DOI] [PubMed] [Google Scholar]
Toole 2005 {published data only}
- Maitland CG, Toole T, Warren E, Hubmann MF. The effects of loading and unloading on gait and balance control in Parkinsonism. Archives of Physical Medicine and Rehabilitation 2004;85:E13. [Google Scholar]
- Toole T, Maitland CG, Warren E, Hubmann MF, Panton L. The effects of loading and unloading treadmill walking on balance, gait, fall risk, and daily function in Parkinsonism. NeuroRehabilitation 2005;20(4):307‐22. [PubMed] [Google Scholar]
Vivas 2011 {published data only}
- Vivas J, Arias P, Cudeiro J. Aquatic therapy versus conventional land‐based therapy for Parkinson's disease: an open‐label pilot study. Archives of Physical Medicine & Rehabilitation 2011;92(8):1202‐10. [DOI] [PubMed] [Google Scholar]
Werner 2010 {published and unpublished data}
- Werner WG, Gentile AM. Improving gait and promoting retention in individuals with Parkinson's disease: a pilot study. Journal of Neurology 2010;257(11):1841‐7. [DOI] [PubMed] [Google Scholar]
Yang 2010 {published data only}
- Yang YR, Lee YY, Cheng SJ, Wang RY. Downhill walking training in individuals with Parkinson's disease: A randomized controlled trial. American Journal of Physical Medicine & Rehabilitation 2010;89(9):706‐14. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Byl 2009 {published data only}
- Byl N. Enhancing safe mobility in patients with Parkinson's disease: effect of dual task training during aerobic and moderate exercise. Parkinsonism & Related Disorders 2009;15 Suppl 2:S122. [Google Scholar]
Cheon 2012 {published data only}
- Cheon SM, Sung HR, Chae BK, Kim JW. Effects of different exercises in the patients with Parkinson's disease. Parkinsonism & Related Disorders 2012;18:s154. [Google Scholar]
Chouza 2011 {published data only}
- Chouza M, Arias P, Vinas S, Cudeiro J. Acute effects of whole‐body vibration at 3, 6, and 9 hz on balance and gait in patients with Parkinson's disease. Movement Disorders 2011;26:920‐1. [DOI] [PubMed] [Google Scholar]
Cianci 2010 {published data only}
- Cianci H, Robinson K, Bunting‐Perry L, Sollenberger J, Nooregian J, Duda J. Are wheeled walkers with visual cues efficacious to treat freezing of gait in Parkinson's disease?. Parkinsonism & Related Disorders 2010; Vol. 16 Suppl 1:S64.
Donovan 2011 {published data only}
- Donovan S, Lim C, Diaz N, Browner N, Rose P, Sudarsky LR, et al. Laserlight cues for gait freezing in Parkinson's disease: An open‐label study. Parkinsonism & Related Disorders 2011;17(4):240‐5. [DOI] [PubMed] [Google Scholar]
Farley 2005 {published data only}
- Farley BG, Koshland GF. Learning Big (TM): Efficacy of a large‐amplitude exercise approach for patients with Parkinson's disease‐bradykinesia to balance. Movement Disorders 2005;20 Suppl 10:466. [Google Scholar]
Filippin 2010 {published data only}
- Filippin NT, Costa PHL, Mattioli R. Effects of treadmill‐walking training with additional body load on quality of life in subjects with Parkinson's disease. Revista Brasileira de Fisioterapia 2010;14(4):344‐50. [DOI] [PubMed] [Google Scholar]
Frazzitta 2012 {published data only}
- Frazzitta G, Bertotti G, Riboldazzi G, Turla M, Uccellini D, Boveri N, et al. A new approach to rehabilitation of Parkinsonian patients: The intensive rehabilitation treatment. Movement Disorders 2011;26:s127. [Google Scholar]
- Frazzitta G, Bertotti G, Riboldazzi G, Turla M, Uccellini D, Boveri N, et al. Effectiveness of intensive inpatient rehabilitation treatment on disease progression in Parkinsonian patients: A randomized controlled trial with 1‐year follow‐up. Neurorehabilitation and Neural Repair 2012;26(2):144‐50. [DOI] [PubMed] [Google Scholar]
Gobbi 2009 {published data only}
- Gobbi L, Oliveira‐Ferreira M, Aetano MJ, irani‐Silva E, Arbieri F, Tella F, et al. Exercise programs improve mobility and balance in people with Parkinson's disease. Parkinsonism & Related Disorders 2009; Vol. 15 Suppl 2:S6. [DOI] [PubMed]
- Gobbi LTB, Oliveira‐Ferreira MDT, Caetano MJD, Lirani‐Silva E, Barbieri FA, Stella F, et al. Exercise programs improve mobility and balance in people with Parkinson's disease. Parkinsonism & Related Disorders 2009;15 Suppl 3:S49‐52. [DOI] [PubMed] [Google Scholar]
Haase 2011 {published data only}
- Haase M. The immediate effects of rhythmic arm swing and finger tapping exercises on gait of Parkinson's patients. ProQuest 2011.
Kamsma 1995 {published data only}
- Kamsma YPT, Brouwer WH, Lakke JPWF. Training of compensational strategies for impaired gross motor skills in Parkinson' disease. Physiotherapy Theory and Practice 1995;11(4):209‐29. [Google Scholar]
Klassen 2007 {published data only}
- Klassen L, Dal Bello‐Haas V, Sheppard M, Metcalfe A. Evaluating the benefits of group exercise and group exercise and education programs for individuals with Parksinson's disease (PD). Physiotherapy 2007;93 Suppl 1:S91. [Google Scholar]
Knobl 2011 {published data only}
- Knobl PE. An evaluation of motor imagery and exercise interventions in Parkinson's disease. ProQuest 2011.
- Knobl PE, Almeida QJ. Rehabilitation for Parkinson's disease: Is it the sensory or attention focus that improves disease severity in sensory‐attention focused interventions?. Movement Disorders 2011;26 Suppl 2:s153. [Google Scholar]
Lee 2011 {published data only}
- Lee KS, Lee WH, Hwang S. Modified constraint‐induced movement therapy improves fine and gross motor performance of the upper limb in Parkinson disease. American Journal of Physical Medicine & Rehabilitation 2011;90(5):380‐6. [DOI] [PubMed] [Google Scholar]
Ma 2009 {published data only}
- Ma HI, Hwang WJ, Lin KC. The effects of two different auditory stimuli on functional arm movement in persons with Parkinson's disease: a dual‐task paradigm. Clinical Rehabilitation 2009;23(3):229‐37. [DOI] [PubMed] [Google Scholar]
Marchese 2000 {published data only}
- Abbruzzese G, Diverio M, Zucchi F, Marchese R. Comparison of two physical therapy approaches in the rehabilitation of parkinsonian patients. Parkinsonism and Related Disorders 1999;5 Suppl:S49. [DOI] [PubMed] [Google Scholar]
- Marchese R, Diverio M, Zucchi F, Lentino C, Abbruzzese G. Comparison of two physical therapy approaches in the rehabilitation of parkinsonian patients: a comparison of two physical therapy protocols. Movement Disorders 2000;15(5):879‐83. [DOI] [PubMed] [Google Scholar]
Modugno 2010 {published data only}
- Modugno N. Long‐term program of social theatre for the management of motor and motor symptoms of Parkinson's disease. Movement Disorders 2010; Vol. 25 Suppl 3:S721.
- Modugno N, Iaconelli S, Fiorilli M, Lena F, Kusch I, Mirabella G. Active theater as a complementary therapy for Parkinson's disease rehabilitation: A pilot study. The Scientific World Journal 2010;10:2301‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
Munneke 2010 {published data only}
- Keus SH, Bloem BR, Nijkrake M, Lim LI, Munneke M. The ParkNet trial: Implementation of an evidence‐based guideline for physical therapy in Parkinson's disease. Movement Disorders 2006;21:S122. [Google Scholar]
- Keus SHJ, Nijkrake MJ, Borm GF, Kwakkel G, Roos RAC, Berendse HW, et al. The ParkinsonNet trial: design and baseline characteristics. Movement Disorders 2010;25(7):830‐7. [DOI] [PubMed] [Google Scholar]
- Munneke M, Kens S, Nijkrake M, Kwakkel G, Berendse H, Roos R, et al. Efficiency of evidence‐based physiotherapy for Parkinson's disease: the ParkinsonNet Trial. Movement Disorders 2008;23 Suppl 1:669. [Google Scholar]
- Munneke M, Nijkrake M, Keus SHJ, Kwakkel G, Berendse HW, Roos RAC, et al. Efficacy of community‐based physiotherapy networks for patients with Parkinson's disease: a cluster‐randomised trial. Lancet Neurology 2010;9(1):46‐54. [DOI] [PubMed] [Google Scholar]
- Munneke M, Nijkrake MJ, Keus SHJ, Lim IIK, Borm GF, Wilt GJ, et al. Efficiency of physiotherapy in Parkinson's disease: The ParkNet trial. Movement Disorders 2007;22 Suppl 16:629. [Google Scholar]
- Nijkrake MJ, Keus SHJ, Overeem S, Oostendorp RAB, Vlieland TPMV, Mulleners W, et al. The ParkinsonNet concept: development, implementation and initial experience. Movement Disorders 2010;25(7):823‐9. [DOI] [PubMed] [Google Scholar]
Pacchetti 2000 {published data only}
- Pacchetti C, Mancini F, Aglieri R, Fundaro C, Martignoni E, Nappi G. Active music therapy in Parkinson's disease: An integrative method for motor and emotional rehabilitation. Psychosomatic Medicine 2000;62(3):386‐93. [DOI] [PubMed] [Google Scholar]
Pohl 2003 {published data only}
- Pohl M, Rockstroh G, Ruckriem S, Mrass G, Mehrholz J. Immediate effects of speed‐dependent treadmill training on gait parameters in early Parkinson's disease. Archives of Physical Medicine and Rehabilitation 2003;84(12):1760‐6. [DOI] [PubMed] [Google Scholar]
Rochester 2011 {published data only}
- Rochester L, Baker K, Nieuwboer A, Burn D. Targeting dopa‐sensitive and dopa‐resistant gait dysfunction in Parkinson's disease: selective responses to internal and external cues. Movement Disorders 2011;26(3):430‐5. [DOI] [PubMed] [Google Scholar]
Sage 2009a {published data only}
- Sage MD, Almeida QJ. Symptom and gait changes after sensory attention focused exercise vs aerobic training in Parkinson's disease. Movement Disorders 2009;24(8):1132‐8. [DOI] [PubMed] [Google Scholar]
Sage 2009b {published and unpublished data}
- Sage MD, Almeida QJ. A Canadian approach to exercise rehabilitation: a systematic evaluation of strategies to reduce the symptoms of Parkinson's disease. Movement Disorders 2009;24 Suppl 1:S276‐7. [Google Scholar]
Sage 2010 {published data only}
- Sage MD, Almeida QJ. A positive influence of vision on motor symptoms during sensory attention focused exercise for Parkinson's disease. Movement Disorders 2010;25(1):64‐9. [DOI] [PubMed] [Google Scholar]
Stallibrass 2001 {published data only}
- Stallibrass C. Controlled trial to evaluate the effects of lessons in the Alexander Technique on the management of disability by people with Parkinson's disease. National Research Register 2001.
Tamir 2007 {published data only}
- Tamir R, Dickstein R, Huberman M. Integration of motor imagery and physical practice in group treatment applied to subjects with Parkinson's disease. Neurorehabilitation and Neural Repair 2007;21(1):68‐75. [DOI] [PubMed] [Google Scholar]
Tickle‐Degnen 2010 {published data only}
- Tickle‐Degnen L, Ellis T, Saint‐Hilaire M, Thomas CA, Wagenaar RC. Efficacy of self‐management rehabilitation on quality of life outcomes in Parkinson's disease. Movement Disorders 2009;24 Suppl 1:S377‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tickle‐Degnen L, Ellis T, Saint‐Hilaire M, Thomas CA, Wagenaar RC. Self‐management rehabilitation and health‐related quality of life in Parkinson's disease: a randomized controlled trial. Movement Disorders 2010;25(2):194‐204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White DK, Wagenaar RC, Ellis TD, Tickle‐Degnen L. Changes in walking activity and endurance following rehabilitation for people with Parkinson disease. Archives of Physical Medicine and Rehabilitation 2009;90(1):43‐50. [DOI] [PubMed] [Google Scholar]
Wulf 2009 {published data only}
- Wulf G, Landers M, Lewthwaite R, Tollner T. External focus instructions reduce postural instability in individuals with Parkinson's disease. Physical Therapy 2009;89(2):162‐8. [DOI] [PubMed] [Google Scholar]
Yen 2011 {published data only}
- Yen CY, Lin KH, Hu MH, Wu RM, Lu TW, Lin CH, et al. Effects of virtual reality‐augmented balance training on sensory organization and attentional demand for postural control in people with Parkinson disease: a randomized controlled trial. Physical Therapy 2011;91(6):862‐78. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
Brauer 2011 {published and unpublished data}
- Brauer SG, Woollacott MH, Lamont R, Clewett S, O'Sullivan J, Silburn P, et al. Single and dual task gait training in people with Parkinson's disease: a protocol for a randomised controlled trial. BMC Neurology 2011;11:90. [DOI] [PMC free article] [PubMed] [Google Scholar]
Protas 2005 {published data only}
- Protas EJ, Mitchell K, Williams A, Qureshy H, Caroline K, Lai EC. Gait and step training to reduce falls in Parkinson's disease. NeuroRehabilitation 2005;20(3):183‐90. [PubMed] [Google Scholar]
Schenkman 2012b {published data only}
- Schenkman M. Endurance exercise in Parkinson's disease. controlled_trials.com 2012.
- Schenkman M. Study in Parkinson's disease of exercise (SPARX). ClinicalTrials.gov 2011.
Smith 2009 {published data only}
- Smith S, Dibble L. High force resistance training and dopamine replacement effects on hypokinesia in Parkinson disease. ClinicalTrials.gov 2009.
Uc 2010 {published data only}
- Uc EY, Newman SR. Effects of aerobic exercise in Parkinson's disease. ClinicalTrials.gov 2010.
van Nimwegen 2010 {published and unpublished data}
- Speelman AD, Nimwegan M, Smulders K, Overeem S, Borm G, Backx F, et al. Rationale and design of the Parkfit study: a randomized controlled trial to increase physical activity in patients with Parkinson's disease. Parkinsonism & Related Disorders 2010; Vol. 16 Suppl 1:S58.
- Speelman AD, Nimwegen ML, Smulders K, Overeem S, Borm GF, Backx FJG, et al. Design of a randomized controlled trial evaluating the effectiveness of a multifaceted program to increase physical activity in Parkinson patients. Movement Disorders 2010; Vol. 25 Suppl 3:S679. [DOI] [PMC free article] [PubMed]
- Nimwegen M, Speelman A, Smulders S, Overeem S, Borm G, Backx F, et al. Rationale and design of the ParkFit study: A randomized controlled trial to increase physical activity in patient with Parkinson's disease. Movement Disorders 2009;24 Suppl 1:S284. [Google Scholar]
- Nimwegen M, Speelman AD, Smulders K, Overeem S, Borm GF, Backx FJG, et al. Design and baseline characteristics of the ParkFit study, a randomized controlled trial evaluating the effectiveness of a multifaceted behavioral program to increase physical activity in Parkinson patients. BMC Neurology 2010;10:70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nimwegen ML, Speelman AD, Gerrits MS, Bloem BR, Munneke M. Monitoring treatment fidelity in the ParkFit Study, a multifaceted behavioral program to increase physical activity in Parkinson patients. Movement Disorders 2010; Vol. 25 Suppl 3:S678.
Additional references
Allen 2011
- Allen NE, Sherrington C, Paul SS, Canning CG. Balance and falls in Parkinson's disease: a meta‐analysis of the effect of exercise and motor training. Movement Disorders 2011;26(9):1605‐15. [DOI] [PubMed] [Google Scholar]
Berg 1992
- Berg KO, Wooddauphinee SL, Williams JI. Measuring balance in the elderly ‐ validation of an instrument. Canadian Journal of Public Health‐Revue Canadienne de Sante Publique 1992;83:S7‐S11. [PubMed] [Google Scholar]
Boutron 2008a
- Boutron I, Moher D, Altman DG, Schulz K, Ravaud P, for the CONSORT group. Methods and processes of the CONSORT Group: example of an extension for trials assessing nonpharmacologic treatments. Annals of Internal Medicine 2008;148(4):W60‐6. [DOI] [PubMed] [Google Scholar]
Boutron 2008b
- Boutron I, Moher D, Altman DG, Schulz K, Ravaud P, for the CONSORT group. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaboration. Annals of Internal Medicine 2008;148(4):295‐309. [DOI] [PubMed] [Google Scholar]
Chartered Society of Physiotherapy
- The Chartered Society of Physiotherapy. In: The Chartered Society of Physiotherapy, editor(s). Rules of professional conduct. 2nd Edition. London: The Chartered Society of Physiotherapy, 2002. [Google Scholar]
Crizzle 2006
- Crizzle AM, Newhouse IJ. Is physical exercise beneficial for persons with Parkinson's disease?. Clinical Journal of Sports Medicine 2006;16(5):422‐5. [DOI] [PubMed] [Google Scholar]
Deane 2001a
- Deane K, Jones DE, Playford ED, Ben‐Shlomo Y, Clarke CE. Physiotherapy versus placebo or no intervention in Parkinson's disease. Cochrane Database of Systematic Reviews 2001, (3):CD002817. [Google Scholar]
Deboer 1996
- Deboer AGEM, Wijker W, Speelman JD, Dehaes JCJM. Quality of life in patients with Parkinson's disease: Development of a questionnaire. Journal of Neurology, Neurosurgery, and Psychiatry 1996;61(1):70‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Doll 1980
- Doll R, Peto R. Randomized controlled trials and retrospective controls. British Medical Journal 1980;280(6206):44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Duncan 1990
- Duncan PW, Weiner DK, Chandler J, Studenski S. Functional Reach ‐ A new clinical measure of balance. Journals of Gerontology 1990;45(6):M192‐7. [DOI] [PubMed] [Google Scholar]
Fahn 1987
- Fahn S, Elton RL. UPDRS Development Committee. Unified Parkinson's Disease Rating Scale. In: Fahn S, Marsden CD, Calne DB, Goldestein M editor(s). Recent developments in Parkinson's disease. Florham Park, NJ: Macmillan Health Care Information, 1987:153‐63. [Google Scholar]
Gage 2004
- Gage H, Storey L. Rehabilitation for Parkinson's disease: a systematic review of available evidence. Clinical Rehabilitation 2004;18(5):463‐82. [DOI] [PubMed] [Google Scholar]
Gibb 1988
- Gibb WRG, Lees AJ. The relevance of the Lewy Body to the pathogenesis of idiopathic Parkinsons disease. Journal of Neurology, Neurosurgery, and Psychiatry 1988;51(6):745‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Giladi 2000
- Giladi N, Shabtai H, Simon ES, Biran S, Tal J, Korczyn AD. Construction of freezing of gait questionnaire for patients with Parkinsonism. Parkinsonism & Related Disorders 2000;6(3):165‐70. [DOI] [PubMed] [Google Scholar]
Goodwin 2008
- Goodwin VA, Richards SH, Taylor RS, Taylor AH, Campbell JL. The effectiveness of exercise interventions for people with Parkinson's disease: A systematic review and meta‐analysis. Movement Disorders 2008;23(5):631‐40. [DOI] [PubMed] [Google Scholar]
Hoehn 1967
- Hoehn MM, Yahr MD. Parkinsonism ‐ onset, progression and mortality. Neurology 1967;17(5):427‐42. [DOI] [PubMed] [Google Scholar]
Jenkinson 1997
- Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson's Disease Questionnaire (PDQ‐39): development and validation of a Parkinson's disease summary index score. Age and Ageing 1997;26(5):353‐7. [DOI] [PubMed] [Google Scholar]
Kersten 2004
- Kersten P. Principles of physiotherapy assessment and outcome measures. In: Stokes M editor(s). Physical management in neurological rehabilitation. 2nd Edition. London: Elsevier Mosby, 2004:29‐46. [Google Scholar]
Keus 2004
- Keus S, Hendriks HJ, Bloem BR, Bredero‐Cohen AB, Goede CJ, Haaren M, et al. Clinical practice guidelines for physical therapy in patients with Parkinsons disease. Dutch Journal of Physiotherapy 2004;114 Suppl 3:1‐94. [Google Scholar]
Keus 2007
- Keus SHJ, Bloem BR, Hendriks EJM, Bredero‐Cohen AB, Munneke M. Evidence‐based analysis of physical therapy in Parkinson's disease with recommendations for practice and research. Movement Disorders 2007;22(4):451‐60. [DOI] [PubMed] [Google Scholar]
Keus 2009
- Keus SHJ, Munneke M, Nijkrake MJ, Kwakkel G, Bloem BR. Physical therapy in Parkinson's disease: Evolution and future challenges. Movement Disorders 2009;24(1):1‐14. [DOI] [PubMed] [Google Scholar]
Kwakkel 2007
- Kwakkel G, Goede CJT, Wegen EEH. Impact of physical therapy for Parkinson's disease: A critical review of the literature. Parkinsonism & Related Disorders 2007;13:S478‐87. [DOI] [PubMed] [Google Scholar]
Lim 2005
- Lim I, Wegen E, Goede C, Deutekom M, Nieuwboer A, Willems A, et al. Effects of external rhythmical cueing on gait in patients with Parkinson's disease: a systematic review. Clinical Rehabilitation 2005;19(7):695‐713. [DOI] [PubMed] [Google Scholar]
Mehrholz 2010
- Mehrholz J, Friis R, Kugler J, Twork S, Storch A, Pohl M. Treadmill training for patients with Parkinson's disease. Cochrane Database of Systematic Reviews 2010, (1):CD007830. [DOI] [PubMed] [Google Scholar]
MRC 2008
- Medical Research Council. Developing and evaluating complex interventions: new guidance. http://www.mrc.ac.uk/Utilities/Documentrecord/index.htm?d=MRC004871 2008.
Mutch 1986
- Mutch WJ, Strudwick A, Roy SK, Downie AW. Parkinson's Disease ‐ disability, review and management. British Medical Journal 1986;293(6548):675‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
NICE CG35 2006
- National Institute for Health and Clinical Excellence. NICE clinical guideline 35. Parkinson's disease: diagnosis and management in primary and secondary care. www.nice.org.uk 2006.
Nieuwboer 2008
- Nieuwboer A, Rochester L, Jones D. Cueing gait and gait‐related mobility in patients with Parkinson's disease ‐ Developing a therapeutic method based on the international classification of functioning, disability, and health. Topics in Geriatric Rehabilitation 2008;24(2):151‐65. [Google Scholar]
Nijkrake 2007
- Nijkrake MJ, Keus SH, Kalf JG, Sturkenboom IH, Munneke M, Kappelle AC, Bloem BR. Allied health care interventions and complementary therapies in Parkinson's disease. Parkinsonism & Related Disorders 2007;13 Suppl 3:S488‐94. [DOI] [PubMed] [Google Scholar]
Patel 2010
- Patel S, Cheed V, Ives N, Clarke C, Rick C, Wheatley K, Gray R, on behalf of the PD MED Collaborators. A large randomised assessment of the relative cost‐effectiveness of different classes of drugs for Parkinson's disease (PD MED Trial). Movement Disorders 2010;25 Suppl 3:S681. [Google Scholar]
PDS 2008
- PDS. Life with Parkinson's today ‐ room for improvement. Parkinson's Disease Society, London 2008.
Perry 1995
- Perry J, Garrett M, Gronley JK, Mulroy SJ. Classification of walking handicap in the stroke population. Stroke 1995;26(6):982‐9. [DOI] [PubMed] [Google Scholar]
Peto 1995
- Peto V, Jenkinson C, Fitzpatrick R, Greenhall R. The development and validation of a short measure of functioning and well‐being for individuals with Parkinson's disease. Quality of Life Research 1995;4(3):241‐8. [DOI] [PubMed] [Google Scholar]
Peto 2001
- Peto V, Jenkinson C, Fitzpatrick R. Determining minimally important differences for the PDQ‐39 Parkinson's disease questionnaire. Age and Ageing 2001;30:299‐302. [DOI] [PubMed] [Google Scholar]
Plant 2000
- Plant R, Jones D, Walton G, Ashburn A, Lovgreen B, Handford F, Kinnear E. Physiotherapy for people with Parkinson's disease: UK best practice short report. Institution of Rehabilitation, University of Northumbria 2000.
Podsiadlo 1991
- Podsiadlo D, Richardson S. The Timed Up and Go ‐ A test of basic functional mobility for frail elderly persons. Journal of the American Geriatrics Society 1991;39(2):142‐8. [DOI] [PubMed] [Google Scholar]
Powell 1995
- Powell LE, Myers AM. The Activities‐Specific Balance Confidence (Abc) Scale. Journals of Gerontology Series A, Biological Sciences and Medical Sciences 1995;50(1):M28‐34. [DOI] [PubMed] [Google Scholar]
Qutubuddin 2005
- Qutubuddin AA, Pegg PO, Cifu DX, Brown R, McNamee S, Carne W. Validating the Berg Balance Scale for patients with Parkinson's disease: A key to rehabilitation evaluation. Archives of Physical Medicine and Rehabilitation 2005;86(4):789‐92. [DOI] [PubMed] [Google Scholar]
Rascol 2002
- Rascol O, Payoux P, Ferreira J, Brefel‐Courbon C. The management of patients with early Parkinson's disease. Parkinsonism & Related Disorders 2002;9(1):61‐7. [DOI] [PubMed] [Google Scholar]
Robertson 2003
- Robertson D. Developing and delivering services. In: Playford D, Thompson AJ editor(s). Neurological Rehabilitation of Parkinson's Disease. London: Martin Dunitz, 2003. [Google Scholar]
Robertson 2008
- Robertson D, Aragon A, Moore G, Whelan L. Rehabilitation and the interdisciplinary team. In: Playfer J, Hindle J editor(s). Parkinson's Disease in the Older Patient. 2nd Edition. Oxford: Radcliffe Publishing Ltd, 2008. [Google Scholar]
Rubenis 2007
- Rubenis J. A rehabilitational approach to the management of Parkinson's disease. Parkinsonism & Related Disorders 2007;13 Suppl 3:S495‐7. [DOI] [PubMed] [Google Scholar]
Schrag 2000
- Schrag A, Jahanshahi M, Quinn N. How does Parkinson's disease affect quality of life? A comparison with quality of life in the general population. Movement Disorders 2000;15(6):1112‐8. [DOI] [PubMed] [Google Scholar]
Schrag 2006
- Schrag A, Sampaio C, Counsell N, Poewe W. Minimal clinically important change on the Unified Parkinson's Disease Rating Scale. Movement Disorders 2006;21(8):1200‐7. [DOI] [PubMed] [Google Scholar]
Shulman 2010
- Shulman LM, Gruber‐Baldini AL, Anderson KE, Fishman PS, Reich SG, Weiner WJ. The clinically important difference on the Unified Parkinson's Disease Rating Scale. Archives of Neurology 2010;67(1):64‐70. [DOI] [PubMed] [Google Scholar]
Steffen 2008
- Steffen T, Seney M. Test‐retest reliability and minimal detectable change on balance and ambulation tests, the 36‐Item Short‐Form Health Survey, and the Unified Parkinson Disease Rating Scale in people with parkinsonism. Physical Therapy 2008;88(6):733‐46. [DOI] [PubMed] [Google Scholar]
Talley 2008
- Talley KMC, Wyman JF, Gross CR. Psychometric properties of the activities‐specific balance confidence scale and the survey of activities and fear of falling in older women. Journal of the American Geriatrics Society 2008;56(2):328‐33. [DOI] [PubMed] [Google Scholar]
Tinetti 1990
- Tinetti ME, Richman D, Powell L. Falls efficacy as a measure of fear of falling. Journals of Gerontology 1990;45(6):239‐43. [DOI] [PubMed] [Google Scholar]
Tomlinson 2012
- Tomlinson CL, Patel S, Meek C, Clarke CE, Stowe R, Shah L, et al. Physiotherapy versus placebo or no intervention in Parkinson's disease. Cochrane Database of Systematic Reviews 2012, (8):CD002817. [DOI] [PubMed] [Google Scholar]
Trew 2005
- Trew M, Everett T. Human movement: an introductory text. 5th Edition. Edinburgh: Churchill Livingstone, 2005. [Google Scholar]
Ware 1992
- Ware JE, Sherbourne CD. The MOS 36‐Item Short‐Form Health Survey (Sf‐36) .1. Conceptual framework and item selection. Medical Care 1992;30(6):473‐83. [PubMed] [Google Scholar]
Webster 1968
- Webster DD. Critical analysis of disability in Parkinson's disease. Modern Treatment 1968;5(2):257‐82. [PubMed] [Google Scholar]
Welsh 2003
- Welsh M, McDermott MP, Holloway RG, Plumb S, Pfeiffer R, Hubble J, et al. Development and testing of the Parkinson's disease quality of life scale. Movement Disorders 2003;18(6):637‐45. [DOI] [PubMed] [Google Scholar]
Whittle 1996
- Whittle M. Gait analysis: an introduction. 2nd Edition. Oxford: Butterworth‐Heinemann, 1996. [Google Scholar]
Yahr 1969
- Yahr MD, Duvoisin RC, Schear MJ, Barrett RE, Hoehn MM. Treatment of Parkinsonism with levodopa. Archives of Neurology 1969;21(4):343‐54. [DOI] [PubMed] [Google Scholar]
Yardley 2005
- Yardley L, Beyer N, Hauer K, Kempen G, Piot‐Ziegler C, Todd C. Development and initial validation of the Falls Efficacy Scale‐International (FES‐I). Age and Ageing 2005;34(6):614‐9. [DOI] [PubMed] [Google Scholar]
Yarrow 1999
- Yarrow S. Members' 1998 survey of the Parkinson's Disease Society of the United Kingdom. In: Percival R, Hobson P editor(s). Parkinson's disease: Studies in psychological and social care. Leicester: BPS Books, 1999:79‐92. [Google Scholar]
References to other published versions of this review
Deane 2001b
- Deane K, Jones DE, Ellis‐Hill C, Clarke CE, Playford ED, Ben‐Shlomo Y. Physiotherapy for Parkinson's disease: a comparison of techniques. Cochrane Database of Systematic Reviews 2001, (1):CD002815. [DOI] [PubMed] [Google Scholar]