

Abstract
Influenza, measles, SARS, MERS, and smallpox illnesses are caused by highly infectious viral pathogens that induce critical illness. These biologically diverse viruses enter and replicate within host cells triggering viral- and host-mediated damage that results in pneumonia and multiorgan failure in severe cases. Early case identification and strict infection control limit healthcare transmission. Vaccination allowed smallpox eradication and limits global measles and seasonal influenza mortality. While SARS-coronavirus (CoV) is no longer circulating, MERS-CoV and zoonotic influenza viruses, with pandemic potential, remain persistent threats. Supportive critical care is the mainstay of treatment for severe disease due to these viral infections.
Keywords: Influenza, Measles, SARS, MERS, Smallpox, Pathogenesis, Treatment
The Viruses
Influenza Biology
Influenza viruses are spherical orfilamentous, enveloped, negative-sense, single-stranded RNA viruses of family Orthomyxoviridae of approximately 100 nm to 300 nm in diameter that include types A, B, C, and D [1, 2]. Influenza A and B viruses cause mild to severe illness during seasonal epidemics, and influenza A viruses cause intermittent pandemics. Influenza C viruses cause mild infections but not epidemics, and influenza D virus may cause subclinical infection [3, 4]. Influenza A viruses are classified into subtypes based on the combination of the surface glycoproteins hemagglutinin and neuraminidase, with 18 H and 11 N known subtypes [5–7]. Specific influenza strains are named according to the World Health Organization (WHO) convention designating influenza virus type, host of origin (if not human), geographic origin, strain number, year of isolation, and subtype (for influenza A viruses) (e.g., Influenza A/California/7/2009[H1N1]) [8].
Influenza A viruses have eight genome segments that code for structural and nonstructural proteins (Fig. 5.1a) [9]. Surface glycoproteins include hemagglutinin (HA), required for viral binding and entry, and neuraminidase (NA), required for viral budding. Matrix (M1) protein underlies the host-derived lipid envelope providing structure, and M2 protein is an ion channel integrated into the envelope. Eight single-stranded RNA viral genome segments are coated with nucleoprotein (N) and bound by the polymerase complex, composed of basic polymerase 1 (PB1), PB2, and acidic polymerase (PA). Nuclear export protein (NEP) mediates trafficking of viral RNA segments and nonstructural protein (NS1) inhibits host antiviral responses. The virus can also expressaccessory proteins PB1-F2 and PA-x.
Fig. 5.1.




Schematic of viral structures and key epidemiological features. (a) Influenza virus is spherical or filamentous in shape. Hemagglutinin (HA) and neuraminidase (NA) proteins are integrated into the host-derived lipid envelope and project from the viral surface. Matrix (M1) protein underlies the envelope, and M2 forms an ion channel within the envelope. Eight single-stranded RNA genome segments are coated with nucleoprotein (NP) and bound by the polymerase complex. Nuclear export protein (NEP) mediates export of viral RNA. Influenza has estimated reproductive number (R0) between 1 and 2. Standard, droplet, and contract precautions are recommended to prevent nosocomial transmission. (b) virus is pleomorphic in shape. Hemagglutinin (H) and fusion (F) proteins are integrated into the host-derived lipid envelope, and matrix (M) protein underlies the envelope. The single-stranded RNA genome is coated with nucleoprotein (N) and bound by the polymerase complex. Measles has an estimate R0 between 9 and 18. Standard, airborne, and contact precautions are recommended to prevent nosocomial transmission. (c) are spherical in shape. Spike (S), membrane (M), and envelope (E) proteins are integrated into the host-derived lipid envelope. The single-stranded RNA genome is coated with nucleoprotein (N). SARS and MERS have an estimated R0 of <1–2. Standard, airborne, and contact precautions are recommended to prevent nosocomial transmission. (d) are oval to brick shaped. The biconcave viral core contains double-stranded DNA and several proteins organized as a nucleosome and surrounded by a core membrane. Two proteinaceous lateral bodies flank the core, and a single lipid membrane surrounds the cell-associated form of the mature virion (MV). A second host-derived lipid envelope covers the extracellular virion (EV). Smallpox has an estimated R0 between 4 and 6. Standard, airborne, and contact precautions are recommended to prevent nosocomial transmission of smallpox
Measles (Rubeola Virus) Biology
Measles virus is a pleomorphic, enveloped, negative-sense, single-stranded RNA virus of family of approximately 100 nm to 300 nm in diameter [2]. Measles virus causes mild to severe illness during seasonal outbreaks in endemic areas and intermittent outbreaks in nonendemic area [10]. Measles virus codes for six structural and two nonstructural proteins (Fig. 5.1b) [11]. Hemagglutinin (H) and fusion (F) glycoproteins project from the viral surface and facilitateviral binding to cellular receptors and fusion with the host cell membrane, respectively. Matrix (M) protein underlies the envelope providing structure. The inner nucleocapsid is composed of RNA coated by nucleoprotein (N), bound by the polymerase complex which includes the large (L) polymerase protein, and phosphoprotein (P), a polymerase cofactor. The remaining nonstructuralproteins include C and V.
Coronavirus Biology
Coronaviruses are spherical, enveloped, positive-sense, single-stranded RNA viruses of family Coronaviridae of approximately 120 nm in diameter [12]. Coronaviruses are the causative agents of an estimated 30% of upper and lower respiratory tract infections in humans resulting in rhinitis, pharyngitis, sinusitis, bronchiolitis, and pneumonia [13]. While coronaviruses are often associated with mild disease (e.g., HCoV-229E, HCoV-OC43, HCoV-NL63, HCoV-HKU1), severe acute respiratory syndrome coronavirus (SARS-CoV), a lineage B betacoronavirus, and Middle East respiratory syndrome coronavirus (MERS-CoV), a lineage C betacoronavirus, are associated with severe and potentially fatal respiratory infection [14, 15].
SARS- and MERS-CoV transcribe 12 and 9 subgenomic RNAs, respectively, which encode for the spike (S), envelope (E), membrane (M), and nucleocapsid (N) structural proteins (Fig. 5.1c) [14]. S, E, and M are all integrated into the host-derived lipid envelope, and S facilitates host cell attachment to angiotensin-converting enzyme (ACE)-2 receptors for SARS-CoV and dipeptidyl peptidase (DPP)-4 receptors for MERS-CoV [16, 17]. The N protein encapsidates the viral genome to form the helical nucleocapsid. The viral replicase-transcriptase complex is made up of 16 nonstructural proteins (nsp1–16) including a unique proofreading exoribonuclease that reduces the accumulation of genomemutations [12].
Smallpox (Variola Virus) Biology
Poxviruses areoval-to-brick-shaped double-stranded DNA viruses of family Poxviridae that range in size from 200 to 400 nm [2]. Viruses within genus that cause human disease include cowpox virus (CPXV), monkeypox virus (MPXV), vaccinia virus (VACV), and variola virus (VARV), the etiologic agent of smallpox [18].
Poxviruses contain a biconcave viral core where the DNA genome, DNA-dependent RNA polymerase, and enzymes necessary for particle uncoating reside (Fig. 5.1d) [19]. This nucleosome is surrounded by a core membrane that is flanked by two proteinaceous lateral bodies. A singlelipid membrane surrounds the cell-associated form of the mature virion (MV). A second host-derived lipid envelope covers the extracellular virion (EV) [2, 19]. Poxvirus genomes are comprised of a large, linear double-stranded viral DNA genome that encodes ~200 genes. Highly conserved structural genes are predominantly found in the middle of the genome, whereas variable virulence factor genes that function in immune evasion, virulence,and viral pathogenesis are found at the termini of the genome [20].
Ecology and Epidemiology
Avian, Swine, Seasonal, and Pandemic Influenza A Viruses
Wild aquatic birds are natural reservoirsfor nearly all influenza A virus subtypes, which spread to domestic avian species and mammals, including humans [5]. H17N10 and H18N11 subtypes are exceptions in that they have only been isolated from bats [6, 7]. Certain H5 and H7 subtypes are highly pathogenic to domestic poultry when transmitted from wild birds, known as highly pathogenic avian influenza (HPAI) viruses [21]. HPAIviruses cause spillover infections in humans that may be severe or fatal. Examples include outbreaks of H5N1 and H7N9 HPAI viruses in Asia with high case fatality among humans, although limited human-to-human transmission [22, 23] has been reported. HPAI virus adaptations might lead to sustained human-to-human transmission, and so poultry outbreaks are managed by flock depopulation [24]. Influenza A subtypes isolated in swine include H1 to H5, H9, and N1 and N2. Subtypes that spillover into humans cause mild to severe illness and are known as swine “variant” viruses [25].
Currently circulating seasonalinfluenza A subtypes H1N1 and H3N2 and influenza B viruses, Yamagata or Victoria lineage, cause annual epidemics during fall through spring in temperate regions and infections throughout the year in the tropics [26]. Antigenic drift of H and N surface glycoproteins drives annual epidemics. From 2017 to 2018, seasonal influenza caused approximately 49 million illnesses, 1 million hospitalizations, and 79,000 deaths in the United States alone [27]. When two or more influenza A viruses infect a common host, such as a bird or pig, individual gene segments may recombine to form a novel virus, known as antigenic shift. Influenza pandemics occur when novel viruses emerge into an immunologically naïve population and become adapted for sustained human-to-human spread. The 1918 “Spanish” influenza pandemic was the most severe on record, resulting in anestimated 50 million deaths [28]. Less severe pandemics occurred in 1957, 1968, and 2009. In an effort to improve preparedness and response to seasonal, pandemic, and zoonotic influenza, the World HealthOrganization (WHO) conducts global surveillance of influenza A and B isolates (Fig. 5.2a) [29].
Fig. 5.2.
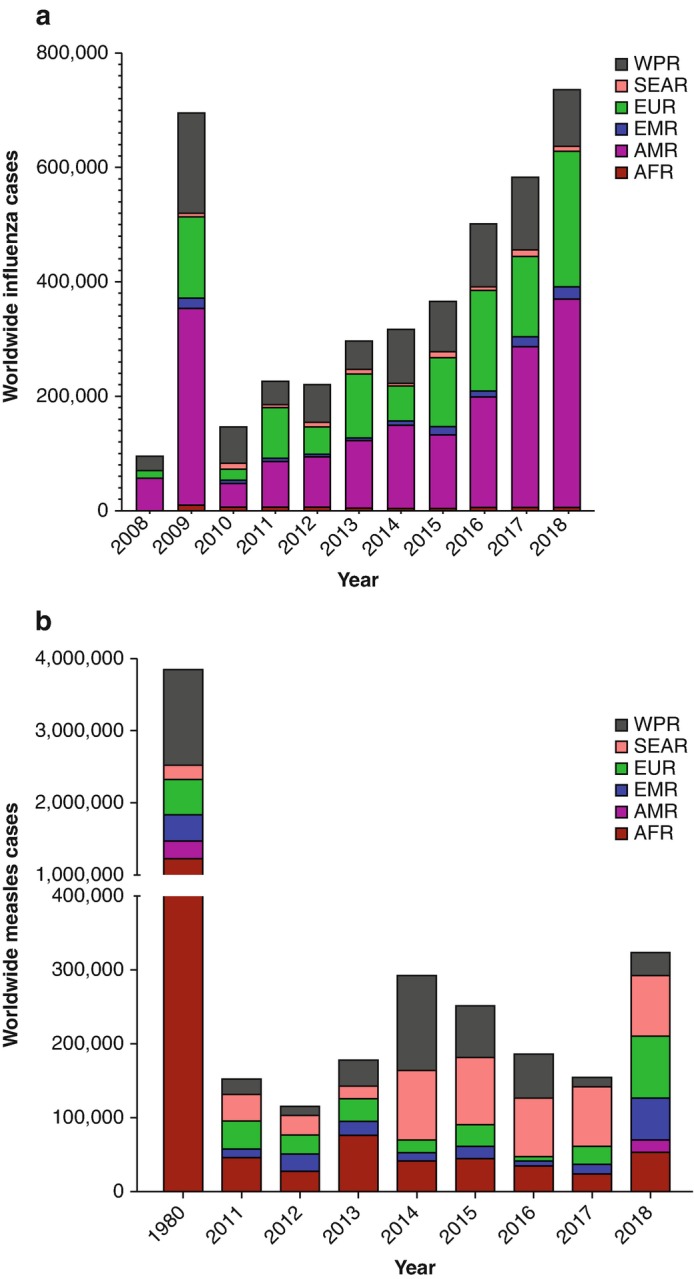
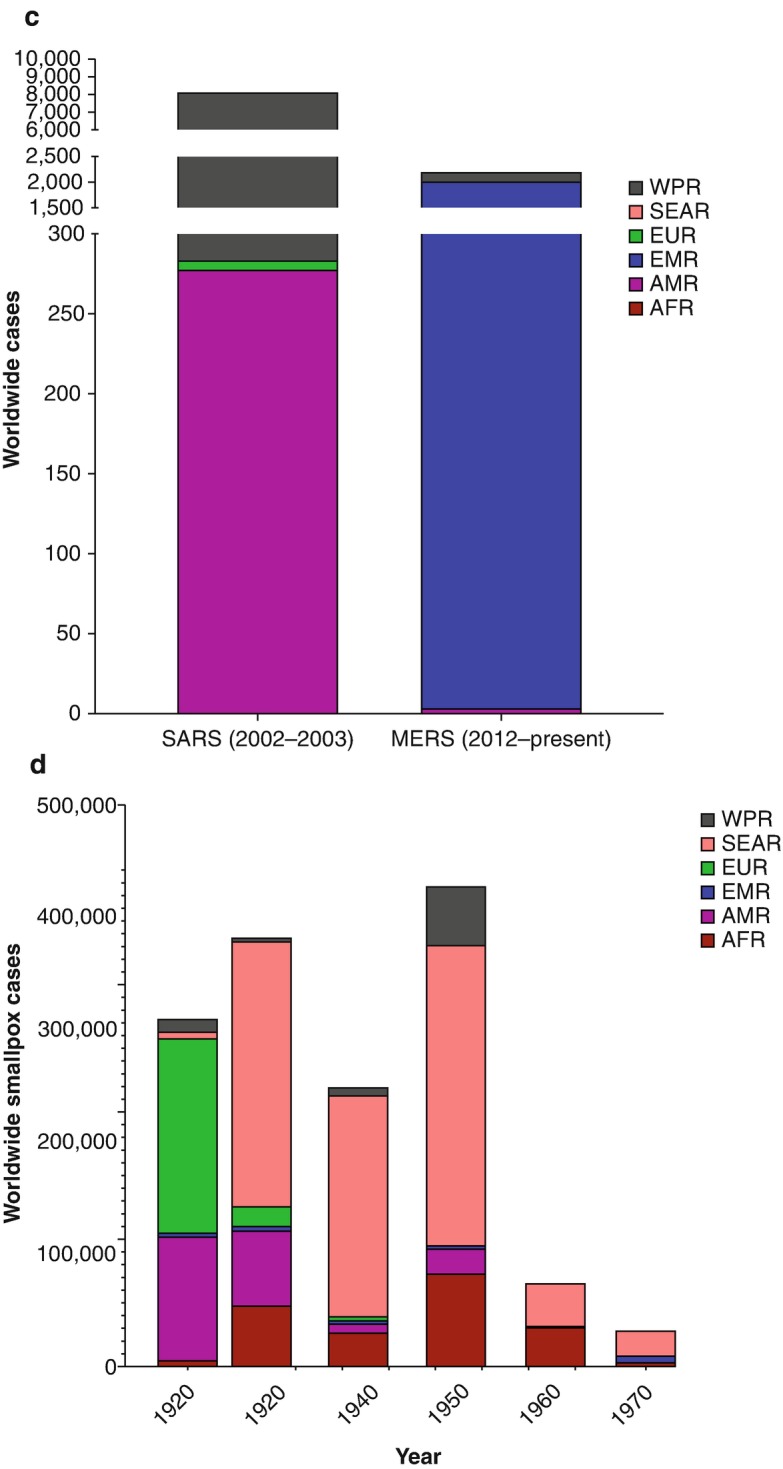
Viral disease burden reported by WHO region. (a) WHO global influenza surveillance of laboratory confirmed influenza A and B infections, 2008–2018. (b) Global measles cases reported to WHO, 2011–2018. Reported cases from 1980 are used as a reference. (c) Global cases of SARS- and MERS-CoV infections. (d) Global cases of smallpox from 1920 to 1970. Data represents the cumulative cases for that year. WHO regions are as follows: WPR Western Pacific Region, SEAR South-East Asia Region, EUR European Region, EMR Eastern Mediterranean Region, AMR Region of the Americas, AFR African Region. (Data courtesy of WHO)
Endemic and Epidemic Measles
Measles is pathogenic for humans and nonhuman primates, although sustained transmission occurs only among humans raising potential for global elimination [30]. Historically, measles infected an estimated 90% of children by age 5 years, resulting in approximately 2 million global deaths each year [10]. With the introduction of the measles vaccine in1963 and advances in global vaccination programs, measles cases and mortality have drastically declined (Fig. 5.2b). By 2017, 85% of children worldwide had received at least one dose of the measles vaccine by age 1 year, and during 2000–2017, global measles mortality decreased by 80%, preventing an estimated 21 million deaths [31]. Of the 24 known measles genotypes, only five were detected in circulation during2016–2017. Despite these gains, measles remains endemic in many regions of the world including Africa, Western Pacific, South East Asia, and Europe, and measles has resurged in previously low-incidence areas (e.g., regions within Europe and the Americas) with epidemics attributable to importation of cases and suboptimal immunization coverage [32–34]. An estimated 93% population immunity is required to preventmeasles transmission within communities, a prerequisite for global elimination [35].
SARS and MERS Epidemics
Chinese horseshoe bats are the putative reservoir for SARS-CoV, and dromedary camels are thought to be the reservoir for MERS-CoV [36–43]. Animal-to-human transmission likely occurs following direct contact with intermediate hosts [38, 44]. During the 2003–2004 SARS epidemic, 8096 cases and 774 deaths were reported from 26 countries with no cases reported since (Fig. 5.2c) [45]. Human-to-human transmission of SARS-CoV occurred primarily in healthcare settings with healthcare workers comprising 22% and >40% of reported cases in China and Canada, respectively [45]. MERS was first reported in Saudi Arabia in 2012 with >2000 cases and >800 deaths reported from 27 countries through 2018 [46]. While most cases have been reported from the Arabian Peninsula, an imported case to South Korea in 2015 resulted in a large outbreak in multiple healthcare facilities [47]. MERS transmission occurs primarily in healthcare facilities and to a lesser degree within households [48, 49].
Smallpox Eradication
While the only known reservoir forVARV is humans, it has been postulated that the virus emerged from an ancestral rodent-borne poxvirus more than 10,000 years ago [18, 50]. Numerous smallpox epidemics have occurred throughout recorded history including more than 300 million fatalities during the twentieth century alone [51–53]. Smallpox was eventually eradicated following the implementation of the Smallpox Eradication Program by the WHO from 1966 to 1980 (Fig. 5.2d) which was facilitated by the absence of a zoonotic reservoir for VARV [51].
Pathogenesis
Influenza Transmission and Mechanisms of Disease
Influenza viruses are transmitted bylarge respiratory droplets by coughing, sneezing, or talking or through contact with infected surfaces [54]. Influenza viruses bind to sugar moieties on the surface of airway epithelial cells where early viral replication, propagation, and shedding occur during an average 1–2 days of incubationperiod [55–57]. Peak viral replication typically occurs within 4 days of symptom onset and resolves within 7–10 days, lasting longer in children and immunocompromised hosts [58–60]. On average one person infects —one to two additional people; however, this reproductive number (R0) varies by viral strain and social and environmental factors [61]. Viral infection impairs the airway mucosal barrier and disrupts the alveolar-capillary membrane contributing to leakage of fluid and inflammatory cells into the alveolar space which impairs gas exchange resulting in hypoxemia [62, 63]. Bacterial coinfection often complicates severe cases contributing to respiratory failure and death, with Staphylococcus aureus and Streptococcus species as predominant copathogens [64]. Seasonal influenza virus infection is largely limited to the respiratory tract; however, H5 and H7 HPAI viruses have a polybasic cleave site within the hemagglutinin allowing for replication outside of the respiratory tract [65, 66]. Infectionwith one strain of influenza does not confer complete immunity to other strains or subtypes [67].
Measles Transmission and Mechanisms of Disease
Measles is among the most highlycontagious respiratory infections, spread by exposure to large respiratory droplets through coughing, sneezing, or talking; by indirect contact with infected surfaces; or by small infectious droplets that can remain suspended in air for up to 2 hours [10, 68]. Respiratory tract dendritic cells, lymphocytes, and alveolar macrophages are early targets of infection where during an average 8- to 12-day incubation period measles replicates and spreads to local lymphatics and respiratory epithelium and then disseminates in blood via infected lymphocytes to epithelial and endothelial cells in most organs [69–71]. The infectious period begins with fever onset and extends for several days after rash appears [72]. The estimated R0 of measles is 9–18 dependent upon host susceptibility and social and environmental factors [73]. Measles infects and disrupts tissues throughout the body;however, severe disease is primarily due to lower respiratory tract and neurological complications [72]. Natural measles infection confers lifelong immunity, and passive transfer of maternal antibodies protects newborns during the early postnatal period [74]. Individuals who recover from measles infection are at increasedrisk of secondary infection [75, 76].
SARS- and MERS-CoV Transmission and Mechanisms of Disease
SARS-CoV is transmitted by large respiratory droplets and by contact with infected surfaces. Epidemiologic data also support small droplet airborne transmission of SARS-CoV although the estimated R0 of 0.86–1.83 argues against this being a predominate route of spread [77, 78]. SARS-CoV binds to angiotensin-converting enzyme (ACE)-2 receptors on respiratory epithelial cells, pneumocytes, and alveolar macrophages resulting in diffuse alveolar damage and respiratory failure [79, 80]. SARS is a systemic infection with viremia detected in most cases affecting multiple cell types and organs [81, 82]. Acute kidney injury is multifactorial with evidence of acute tubule necrosis, vasculitis, and glomerular fibrosis, and central nervous system manifestations are at least in part attributable to direct infection of neurons resulting in edema and degeneration [83].
MERS-CoV is transmitted by large respiratory droplets and by contact with infected surfaces with an estimated R0 of <1 to >1 outside of versus within healthcare settings, respectively [84]. MERS-CoV binds dipeptidyl peptidase 4 (DPP4) on respiratory epithelial cells and pneumocytes where it undergoes productive replication during a 2–14 days incubation period [16]. Viral shedding from the lower respiratory tract may persist for weeks [85, 86]. Viremia, while not documented in all cases, is associated with severe disease and productive infection of DCs, and macrophages is thought to facilitate immune dysregulation [87, 88]. DPP4 is broadly expressed on cells outside of the lung; however, few autopsy data are available to define viral distribution [16, 89].
Variola Virus Transmission and Mechanisms of Disease
VARV is transmitted primarily by large respiratory droplets and to a lesser degree through contact with contaminated objects such as scabs, bedding, or clothing or by airborne small respiratory droplets [90, 91]. VARV is thought to replicate in airway epithelium and spread to regional lymph nodes [92, 93]. VARV replicates within lymph nodes and disseminates via the bloodstream seeding distant sightsincluding skin, spleen, bone marrow, liver, kidney, and other organs [94]. Fever manifests following an average 12 days incubation, and rash follows fever by 3–4 days, concurrent with high-level viral shedding from oropharyngeal secretions [95, 96]. The estimated R0 of smallpox is between 3.5 and 6 [97]. High-level viremia is detected more often with hemorrhagic compared with ordinary type smallpox, although exact mechanisms of organ failure observed in fatal case are not welldefined [98–101].
Clinical Findings
Influenza Illness and Complications
Influenza infection manifests as acute onset of fever, chills, malaise, headache, and myalgias following an average 1–2 days asymptomatic incubation period [9]. Most infections are self-limited resolving within 1–2 weeks. Upper or lower airway complications include otitis media, sinusitis, bronchitis, and pneumonia with or without bacterial coinfection [63, 64, 102]. Risk factors for severe infection include age >65 years or <5 years; pregnancy; preexisting respiratory, cardiac, neurologic, or metabolic conditions; immunosuppression; andobesity. Progressive lethargy and shortness of breath, typically within 5 days of symptom onset, suggest development of lower respiratory tract complications which may rapidly progress to respiratory failure and death in severe cases [64]. Pneumonia due to influenza infection alone versus influenza and bacterialcoinfection cannot be reliably distinguished by clinical or radiological grounds, and so a high index of suspicion is needed. Influenza complications outside of the respiratory tract include exacerbation of underlying heart disease including ischemic heart disease and heart failure, myocarditis, encephalopathy,and encephalitis [103].
Measles Illness and Complications
Measles infectionmanifests by acute onset fever, coryza, conjunctivitis, and cough [10]. Small white papules, Koplik spots, appear on the buccal mucosa within 3 days of fever onset, followed by development of diffuse maculopapular rash 1 or 2 days later. Diarrhea commonly begins shortly following rash onset and may result in dehydration. Symptoms typically resolve within 7 days of fever onset in self-limited illness. Groups at increased risk for measles complications include malnourished infants and those with vitamin A deficiency, adults >20 years old, and immunocompromised individuals [72]. Respiratory complications include otitis media, laryngotracheobronchitis (croup), and pneumonia. Pneumonia, often complicated by bacterial coinfection, is the most common severe complication of measles contributing to respiratory failure and death [72, 104]. Predominantbacterial copathogens include Streptococcus pneumonia, Staphylococcus aureus, and Haemophilus influenzae.
Three rare but severe neurologic complications occur [105]. Acute disseminated encephalomyelitis (ADEM) is a demyelinating autoimmune process that occurs within weeks of acute illness in approximately 1 in 1000 cases. ADEM is characterized by fevers, seizures, and neurologic deficits. Measles inclusion body encephalitis is a progressive lethal brain infection occurring within months of acute illness primarily among individuals with impaired cellular immunity. Subacute sclerosing panencephalitis (SSPE) occurs 5–10 years following initial infection resulting in seizures and cognitive and motor decline resulting in death. SSPE affects an estimated 1 in 10,000 infants under 1 year of age and is attributed to host responses to defective viral particleproduction in the brain.
SARS and MERS Illness and Complications
Following an average 5-day incubation period, SARS-CoV infection presents with fevers, chills, dry cough, headache, malaise, and dyspnea commonly followed by watery diarrhea [106–108]. Age >60 years and pregnancy are associated with severe disease manifested by progressive respiratory failure within 2 weeks of illness onset [108, 109]. Common laboratory features of SARS included lymphopenia, thrombocytopenia, abnormal coagulation parameters, and elevated lactate dehydrogenase, alanine aminotransferase, and creatine kinase levels [110–112]. Acute kidney injury and proteinuria were observed in 7% and 84% of patients, respectively [113].
Initial symptoms of MERS-CoV infection include fever, chills, cough, shortness of breath, myalgia, and malaise following a mean incubation period of 5 days [114]. Gastrointestinal symptoms, including vomiting and diarrhea, occur in one-third of patients [115–118]. The median times from symptom onset to hospitalization, ICU admission, and death are 4, 5, and 12 days, respectively [118]. MERS patients present with a rapidly progressing pneumonia requiring mechanical ventilation and additional organ support with the first week of illness [109]. Severe disease has been linked to comorbidities including diabetes mellitus (68%), chronic renal disease (49%), hypertension (34%), chronic cardiac disease (28%), chronic pulmonary disease (26%), and obesity (17%) [114]. The median age of those with confirmed MERS is 50 years with a male-to-female ratio of 3.3:1 [114]. Laboratory abnormalities include lymphopenia, leukopenia, thrombocytopenia, elevated serum creatinine levels consistent with acute kidney injury, and elevated liver enzymes [114, 115, 117, 119, 120]. High lactate levels and consumptive coagulopathy have also been reported [119, 121]. Chest radiographic abnormalities are due to viral pneumonitis with or without secondary bacterial pneumonia, and acute kidney injury occurs in up to 43% of patients [114, 119, 120, 122–124].
Smallpox Illness and Complications
As the smallpox disease coursewas related to the clinical presentation of disease, Rao proposed a clinical classification system [125] that was later adopted by the WHO in 1972 [51]. was the most common clinical type of smallpox. The incubation period was 7–19 days and was followed by fever onset (38.5–40.5 °C), headaches, backaches, vomiting, and diarrhea [51]. Lesions first appeared on mucous membranes (including the tongue, palate, and pharynx) ~1 day prior to macular rash development, where lesions began on the face followed by proximal regions of the extremities, the trunk, and the distal extremities. Lesion development followed a centrifugal dispersionpattern, typically most dense on the face, with papules appearing within 2 days of macular rash development. Papules became vesicular ~2–4 days later followed by a pustular stage (5–7 days postrash) that peaked ~10 days postrash. Pustule resolution quickly followed and was accompanied by lesion flattening, fluid reabsorption, hardening, and scab formation (14–21 days postrash). Rao proposed for ordinary type smallpox to be further subdivided based on the macular rash pattern [125]. These included discrete ordinary-type smallpox , characterized by discrete skin lesions; , where pustular skin lesions were confluent on the face and extremities; and , where skin lesions were confluent on the face but disparate over the rest of the body. Modified-type smallpox, where lesions were less numerous than in ordinary-type smallpox, was primarily associated with vaccinated individuals and had an accelerated nonfatal disease course [125]. Flat-type and hemorrhagic-type smallpox were the most lethalforms of the disease but were also very rare (~7% and 3% of patients, respectively) [51]. Flat-type smallpox had high CFRs in both unvaccinated and vaccinated patients (97% and 67%, respectively). Hemorrhagic-type smallpox was nearly 100% fatal in both vaccinated and unvaccinated individuals, and death normally came prior to macular rash development. The clinical symptoms of flat-type smallpox were more severe during the prodromal period and did not subside. Skin lesions were flat and often black or dark purple. Respiratory complications were common and patients were febrile throughout disease. Death typically occurred 8–12 days post-fever onset. Hemorrhagic-type smallpox could be divided into early and late hemorrhagic-type smallpox. The early form was characterized by hemorrhage (primarily subconjunctival) early in the disease course. Generalized erythema,petechiae, and ecchymosis within 2 days of fever and flat matter lesions formed across the entire body surface. Lesions turned purple by day 4 with death by day 6 as a result of cardiac and pulmonary complications. In the late form, hemorrhages occurred following rash development and death followed between8 and 10 days post-fever onset.
Diagnosis
Influenza: Infection Control and Confirmatory Testing
In healthcare settings, patients under evaluation for influenza should be isolated, and standard, droplet, and contact precautions should be implemented [126]. Traditional antigen-based rapid diagnostic assays (RDAs) for influenza lack sensitivity and cannot be relied upon to rule out infection [26]. Newer antigen-based RDAs that employ a digital scan of the test strip, and molecular assays that employisothermal amplification technology have improved sensitivity and specificity that more closely approximates highly sensitive and specific reverse transcriptase polymerase chain reaction (RT-PCR)-based assays [127]. Acceptable sample types for influenza testing include nasopharyngeal swab or wash and bronchoalveolar lavage specimens. Individuals suspected of zoonotic influenza infection should have case evaluation and specimen testing coordinated through local or state public health authorities.
Measles: Infection Control and Confirmatory Testing
Measles should be consideredin patients without preexisting immunity and a compatible febrile rash illness. Travel to a region with ongoing measles transmission or exposure to other individuals with a febrile rash illness should raise suspicion. Patients under evaluation for measles require isolation and implementation of standard, airborne, and contact precautions. Local or state health authorities should be contacted within 24 hours to assist with confirmatory testing, case finding, and infection control. Measles is typically confirmed by measles-specific IgM serology or detection of measles RNA in a nasopharyngeal, throat, or urine specimen by RT-PCR [10]. A fourfold or greater rise in measles IgG titers between acute and convalescent samples tested 2 or more weeks apart can assist with diagnostic uncertainty. Virus can also be cultured from respiratory, blood, and urine specimens in appropriate public health laboratories.
SARS and MERS: Infection Control and Confirmatory Testing
While SARS is no longer circulating, MERS should be suspected in individuals with a compatible febrile illness and an epidemiological risk factor [128]. Risk factors include travel to the Arabian Peninsula or contact with a confirmed or suspected case within 14 days of symptom onset. Patients under evaluation for MERS require isolation and implementation of standard, airborne, and contact precautions. Confirmatory testing and infection control should be coordinated through local or state health authorities. MERS may be confirmed in designated public health laboratories by RT-PCR testing of lower respiratory tract specimens [129]. Multiple other specimen types including upper respiratory tract samples, serum, and stool should also be collected for testing. Serologic testing can be used to evaluate for suspected infection among individuals no longer shedding virus [129, 130].
Smallpox: Infection Control and Confirmatory Testing
Smallpox has not been observedin over 40 years; however, concerns remain for use as a bioweapon. Major and minor criteria have been established to assist clinicians in recognition of smallpox [131]. Individuals under evaluation should be isolated, and standard, airborne, and contact precautions should be implemented. Local or state health authorities should be contacted to assist with confirmatory testing and public health interventions. PCR identification of variola DNA or isolation of the virus from a clinical specimen isrequired to confirm a diagnosis in specialized high-containment laboratories.
Clinical Management
Influenza Prevention and Treatment
Annual seasonal influenza vaccination is recommended in the United States for all individuals aged 6 months or older and has been associated with decreased risk of pneumonia and death, particularly among high-risk groups [132–134]. Seasonal influenza vaccination does not provide protection against novel strains. Consequently, efforts are underway to develop a vaccine that would protect against most or all influenza strains [135]. Three classes of drugs are licensed for the treatment of influenza in the United States [136]. Adamantanes, including amantadine and rimantadine,are not currently recommended given resistance of circulating seasonal strains. Baloxavir morboxil, a cap-dependent endonuclease inhibitor, was recently approved for the treatment of uncomplicated influenza [137]. Neuraminidase inhibitors (NAI) include oral oseltamivir, inhaled zanamivir, and intravenous peramivir. Prophylactic use of NAIs is recommended in unvaccinated individuals with risk factors for severe disease and during institutional outbreaks to limit spread. Therapeutic use is recommended for individuals with suspected or confirmed influenza that have developed or are at high risk for influenza complications [26]. Influenza complications,including respiratory and multiorgan failure, are managed with supportive care. Bacterial coinfection should be considered and empirically treated early pending results of microbiologic testing among severe cases.
Measles Prevention and Treatment
Measles can be effectively prevented through vaccination, typically given in combination with vaccines for rubella (MR), mumps (MMR), or varicella (MMR-V). WHO recommends the first dose of measles vaccine be administered at 9 or 12 months of age in high and low prevalence settings, respectively [138]. A second dose should be administered after a minimum of 4-week interval. Nonimmune individuals that have been exposed to measles should receive post-exposure prophylaxis with MMR or immunoglobulin within 72 hours or 6 days, respectively, although not concurrently [139]. Clinical management of patients with measles consists of fluid, electrolyte, and nutritional support and early recognition and treatment of bacterial coinfection [10]. Two doses of vitamin A inchildren under 2 years have been associated with reduced risk of pneumonia and death [140]. WHO recommends administering 200,000 IU of vitamin A daily for 2 days in children aged 1 year and older, with reduced dosingin younger infants [141].
SARS and MERS Treatment
There are currently no licensed therapeutics or vaccines for SARS or MERS. Consequently, supportive care is the mainstay of treatment [142]. Renal replacement therapy is frequently required in severe illness [119, 143, 144]. Empiric antibiotics are often administered given potential for secondary bacterial infection. Ribavirin and pegylated interferon alpha 2b have been administered to MERS patients, although effectiveness data is lacking [144]. Aerosol-generating procedures including endotracheal intubation are associated with increased risk of healthcare worker infection necessitating strict adherence to infection control measures, including use of eye protection in addition to standard, airborne, and contact precautions [145].
Smallpox Prevention and Treatment
While routine smallpox vaccinationceased at the end of the smallpox eradication program, it is still employed for those at increased risk for exposure. First-generation vaccines comprise a significant proportion of both the US national and global vaccine stockpiles [146]. However, first-generation vaccines carry high risk of adverse events due to use of replication-competent VACV and potential manufacturing contaminants. Second-generation smallpox vaccines have reduced concerns for contaminants and are expected to have similar protective efficacy as first-generation vaccines. ACAM2000® has garnered US Food and Drug Administration licensure for vaccination of those at high risk for exposure and is part of the US strategic national stockpile [147]. ACAM2000® and the Lister-derived vaccines RIVM and Elstree-BN also contribute to the global stockpile. IMVAMUNE (MVA), a third-generation vaccine, is licensed in Europe and Canada and is part of the US national stockpile. Passive immunization with VIG has been employed to treat complications of vaccinations [148, 149]. There has also been increasing interest in the development and licensure of small molecule antivirals for treatment of Orthopoxvirus infections. CMX001 (brincidofovir), a DNA synthesis inhibitor, has demonstrated protection against lethal VARV in nonhuman primates [150] and has been granted ophan drug designation while also being included in the US Strategic National Stockpile. ST-246 (tecovirimat), which inhibits viral egress, has potent (IC50 < 0.010 μM) and selective (CC50 > 40 mM) inhibitory activities against multiple orthopoxvirues [151], is the only antipoxvirus therapeutic that has been granted approval in the US and has been added to the Strategic National Stockpile.
Contributor Information
Jorge Hidalgo, Email: jlhmmd@gmail.com.
Laila Woc-Colburn, Email: woccolbu@bcm.edu.
Daniel S. Chertow, Email: chertowd@cc.nih.gov
Jason Kindrachuk, Email: Jason.Kindrachuk@umanitoba.ca.
References
- 1.Centers for Disease Control and Prevention. Types of influenza viruses. [cited 2019 March 1]. Available from: https://www.cdc.gov/flu/about/viruses/types.htm.
- 2.Knipe DM, Howley PM. Fields virology. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health; 2013. [Google Scholar]
- 3.White SK, Ma W, McDaniel CJ, Gray GC, Lednicky JA. Serologic evidence of exposure to influenza D virus among persons with occupational contact with cattle. J Clin Virol. 2016;81:31–33. doi: 10.1016/j.jcv.2016.05.017. [DOI] [PubMed] [Google Scholar]
- 4.Hause BM, Collin EA, Liu R, Huang B, Sheng Z, Lu W, Wang D, Nelson EA, Li F. Characterization of a novel influenza virus in cattle and Swine: proposal for a new genus in the Orthomyxoviridae family. MBio. 2014;5:e00031-00014. doi: 10.1128/mBio.00031-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Krauss S, Webster RG. Avian influenza virus surveillance and wild birds: past and present. Avian Dis. 2010;54:394–398. doi: 10.1637/8703-031609-Review.1. [DOI] [PubMed] [Google Scholar]
- 6.Tong S, Li Y, Rivailler P, Conrardy C, Castillo DA, Chen LM, Recuenco S, Ellison JA, Davis CT, York IA, Turmelle AS, Moran D, Rogers S, Shi M, Tao Y, Weil MR, Tang K, Rowe LA, Sammons S, Xu X, Frace M, Lindblade KA, Cox NJ, Anderson LJ, Rupprecht CE, Donis RO. A distinct lineage of influenza A virus from bats. Proc Natl Acad Sci U S A. 2012;109:4269–4274. doi: 10.1073/pnas.1116200109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tong S, Zhu X, Li Y, Shi M, Zhang J, Bourgeois M, Yang H, Chen X, Recuenco S, Gomez J, Chen LM, Johnson A, Tao Y, Dreyfus C, Yu W, McBride R, Carney PJ, Gilbert AT, Chang J, Guo Z, Davis CT, Paulson JC, Stevens J, Rupprecht CE, Holmes EC, Wilson IA, Donis RO. New world bats harbor diverse influenza A viruses. PLoS Pathog. 2013;9:e1003657. doi: 10.1371/journal.ppat.1003657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.A revision of the system of nomenclature for influenza viruses: a WHO memorandum. Bull World Health Organ. 1980;58:585–91. [PMC free article] [PubMed]
- 9.Krammer F, Smith GJD, Fouchier RAM, Peiris M, Kedzierska K, Doherty PC, Palese P, Shaw ML, Treanor J, Webster RG, Garcia-Sastre A. Influenza. Nat Rev Dis Primers. 2018;4:3. doi: 10.1038/s41572-018-0002-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Moss WJ. Measles. Lancet. 2017;390:2490–2502. doi: 10.1016/S0140-6736(17)31463-0. [DOI] [PubMed] [Google Scholar]
- 11.Horikami SM, Moyer SA. Structure, transcription, and replication of measles virus. Berlin, Heidelberg: Springer; 1995. [DOI] [PubMed] [Google Scholar]
- 12.Fehr AR, Perlman S. Coronaviruses: an overview of their replication and pathogenesis. Methods Mol Biol. 2015;1282:1–23. doi: 10.1007/978-1-4939-2438-7_1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jevsnik M, Ursic T, Zigon N, Lusa L, Krivec U, Petrovec M. Coronavirus infections in hospitalized pediatric patients with acute respiratory tract disease. BMC Infect Dis. 2012;12:365. doi: 10.1186/1471-2334-12-365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.de Wit E, van Doremalen N, Falzarano D, Munster VJ. SARS and MERS: recent insights into emerging coronaviruses. Nat Rev Microbiol. 2016;14:523–534. doi: 10.1038/nrmicro.2016.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Graham RL, Donaldson EF, Baric RS. A decade after SARS: strategies for controlling emerging coronaviruses. Nat Rev Microbiol. 2013;11:836–848. doi: 10.1038/nrmicro3143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Raj VS, Mou H, Smits SL, Dekkers DH, Muller MA, Dijkman R, Muth D, Demmers JA, Zaki A, Fouchier RA, Thiel V, Drosten C, Rottier PJ, Osterhaus AD, Bosch BJ, Haagmans BL. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature. 2013;495:251–254. doi: 10.1038/nature12005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Li W, Moore MJ, Vasilieva N, Sui J, Wong SK, Berne MA, Somasundaran M, Sullivan JL, Luzuriaga K, Greenough TC, Choe H, Farzan M. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature. 2003;426:450–454. doi: 10.1038/nature02145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Diven DG. An overview of poxviruses. J Am Acad Dermatol. 2001;44:1–16. doi: 10.1067/mjd.2001.109302. [DOI] [PubMed] [Google Scholar]
- 19.Buller RM, Palumbo GJ. Poxvirus pathogenesis. Microbiol Rev. 1991;55:80–122. doi: 10.1128/mr.55.1.80-122.1991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Harrison SC, Alberts B, Ehrenfeld E, Enquist L, Fineberg H, McKnight SL, Moss B, O’Donnell M, Ploegh H, Schmid SL, Walter KP, Theriot J. Discovery of antivirals against smallpox. Proc Natl Acad Sci U S A. 2004;101:11178–11192. doi: 10.1073/pnas.0403600101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.World Health Organization. Avian influenza: assessing the pandemic threat. [cited 2019 March 11]. Available from: https://apps.who.int/iris/bitstream/handle/10665/68985/WHO_CDS_2005.29.pdf?sequence=1.
- 22.Lai S, Qin Y, Cowling BJ, Ren X, Wardrop NA, Gilbert M, Tsang TK, Wu P, Feng L, Jiang H, Peng Z, Zheng J, Liao Q, Li S, Horby PW, Farrar JJ, Gao GF, Tatem AJ, Yu H. Global epidemiology of avian influenza A H5N1 virus infection in humans, 1997–2015: a systematic review of individual case data. Lancet Infect Dis. 2016;16:e108–e118. doi: 10.1016/S1473-3099(16)00153-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Li Q, Zhou L, Zhou M, Chen Z, Li F, Wu H, Xiang N, Chen E, Tang F, Wang D, Meng L, Hong Z, Tu W, Cao Y, Li L, Ding F, Liu B, Wang M, Xie R, Gao R, Li X, Bai T, Zou S, He J, Hu J, Xu Y, Chai C, Wang S, Gao Y, Jin L, Zhang Y, Luo H, Yu H, He J, Li Q, Wang X, Gao L, Pang X, Liu G, Yan Y, Yuan H, Shu Y, Yang W, Wang Y, Wu F, Uyeki TM, Feng Z. Epidemiology of human infections with avian influenza A(H7N9) virus in China. N Engl J Med. 2014;370:520–532. doi: 10.1056/NEJMoa1304617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jhung MA, Nelson DI, Centers for Disease Control and Prevention (CDC) Outbreaks of avian influenza A (H5N2), (H5N8), and (H5N1) among birds--United States, December 2014-January 2015. MMWR Morb Mortal Wkly Rep. 2015;64:111. [PMC free article] [PubMed] [Google Scholar]
- 25.Centers for Disease Control and Prevention (CDC) Influenza A (H3N2) variant virus-related hospitalizations: Ohio, 2012. MMWR Morb Mortal Wkly Rep. 2012;61:764–767. [PubMed] [Google Scholar]
- 26.Paules C, Subbarao K. Influenza. Lancet. 2017;390:697–708. doi: 10.1016/S0140-6736(17)30129-0. [DOI] [PubMed] [Google Scholar]
- 27.Centers for Disease Control and Prevention. Estimated influenza illnesses, medical visits, hospitalizations, and death in the United States — 2017–2018 influenza season. [cited 2019 March 11]. Available from: https://www.cdc.gov/flu/about/burden/2017-2018.htm#References.
- 28.Taubenberger JK, Morens DM. 1918 influenza: the mother of all pandemics. Emerg Infect Dis. 2006;12:15–22. doi: 10.3201/eid1209.05-0979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.World Health Organization. Global influenza surveillance and response system (GISRS). https://www.who.int/influenza/gisrs_laboratory/en/. Accessed 19 Apr 2019.
- 30.Moss WJ, Strebel P. Biological feasibility of measles eradication. J Infect Dis. 2011;204(Suppl 1):S47–S53. doi: 10.1093/infdis/jir065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Dabbagh A, Laws RL, Steulet C, Dumolard L, Mulders MN, Kretsinger K, Alexander JP, Rota PA, Goodson JL. Progress toward regional measles elimination – worldwide, 2000–2017. MMWR Morb Mortal Wkly Rep. 2018;67:1323–1329. doi: 10.15585/mmwr.mm6747a6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Thornton J. Measles cases in Europe tripled from 2017 to 2018. BMJ. 2019;364:l634. doi: 10.1136/bmj.l634. [DOI] [PubMed] [Google Scholar]
- 33.Gastanaduy PA, Budd J, Fisher N, Redd SB, Fletcher J, Miller J, DJ MF, 3rd, Rota J, Rota PA, Hickman C, Fowler B, Tatham L, Wallace GS, de Fijter S, Parker Fiebelkorn A, DiOrio M. A measles outbreak in an underimmunized Amish Community in Ohio. N Engl J Med. 2016;375:1343–1354. doi: 10.1056/NEJMoa1602295. [DOI] [PubMed] [Google Scholar]
- 34.Patel MK, Gacic-Dobo M, Strebel PM, Dabbagh A, Mulders MN, Okwo-Bele JM, Dumolard L, Rota PA, Kretsinger K, Goodson JL. Progress toward regional measles elimination – worldwide, 2000–2015. MMWR Morb Mortal Wkly Rep. 2016;65:1228–1233. doi: 10.15585/mmwr.mm6544a6. [DOI] [PubMed] [Google Scholar]
- 35.Wallinga J, Heijne JC, Kretzschmar M. A measles epidemic threshold in a highly vaccinated population. PLoS Med. 2005;2:e316. doi: 10.1371/journal.pmed.0020316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Haagmans BL, Al Dhahiry SH, Reusken CB, Raj VS, Galiano M, Myers R, Godeke GJ, Jonges M, Farag E, Diab A, Ghobashy H, Alhajri F, Al-Thani M, Al-Marri SA, Al Romaihi HE, Al Khal A, Bermingham A, Osterhaus AD, AlHajri MM, Koopmans MP. Middle East respiratory syndrome coronavirus in dromedary camels: an outbreak investigation. Lancet Infect Dis. 2014;14:140–145. doi: 10.1016/S1473-3099(13)70690-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Reusken CB, Haagmans BL, Muller MA, Gutierrez C, Godeke GJ, Meyer B, Muth D, Raj VS, Smits-De Vries L, Corman VM, Drexler JF, Smits SL, El Tahir YE, De Sousa R, van Beek J, Nowotny N, van Maanen K, Hidalgo-Hermoso E, Bosch BJ, Rottier P, Osterhaus A, Gortazar-Schmidt C, Drosten C, Koopmans MP. Middle East respiratory syndrome coronavirus neutralising serum antibodies in dromedary camels: a comparative serological study. Lancet Infect Dis. 2013;13:859–866. doi: 10.1016/S1473-3099(13)70164-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Azhar EI, El-Kafrawy SA, Farraj SA, Hassan AM, Al-Saeed MS, Hashem AM, Madani TA. Evidence for camel-to-human transmission of MERS coronavirus. N Engl J Med. 2014;370:2499–2505. doi: 10.1056/NEJMoa1401505. [DOI] [PubMed] [Google Scholar]
- 39.Hemida MG, Chu DK, Poon LL, Perera RA, Alhammadi MA, Ng HY, Siu LY, Guan Y, Alnaeem A, Peiris M. MERS coronavirus in dromedary camel herd, Saudi Arabia. Emerg Infect Dis. 2014;20:1231–1234. doi: 10.3201/eid2007.140571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Raj VS, Farag EA, Reusken CB, Lamers MM, Pas SD, Voermans J, Smits SL, Osterhaus AD, Al-Mawlawi N, Al-Romaihi HE, AlHajri MM, El-Sayed AM, Mohran KA, Ghobashy H, Alhajri F, Al-Thani M, Al-Marri SA, El-Maghraby MM, Koopmans MP, Haagmans BL. Isolation of MERS coronavirus from a dromedary camel, Qatar, 2014. Emerg Infect Dis. 2014;20:1339–1342. doi: 10.3201/eid2008.140663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ge XY, Li JL, Yang XL, Chmura AA, Zhu G, Epstein JH, Mazet JK, Hu B, Zhang W, Peng C, Zhang YJ, Luo CM, Tan B, Wang N, Zhu Y, Crameri G, Zhang SY, Wang LF, Daszak P, Shi ZL. Isolation and characterization of a bat SARS-like coronavirus that uses the ACE2 receptor. Nature. 2013;503:535–538. doi: 10.1038/nature12711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Li W, Shi Z, Yu M, Ren W, Smith C, Epstein JH, Wang H, Crameri G, Hu Z, Zhang H, Zhang J, McEachern J, Field H, Daszak P, Eaton BT, Zhang S, Wang LF. Bats are natural reservoirs of SARS-like coronaviruses. Science. 2005;310:676–679. doi: 10.1126/science.1118391. [DOI] [PubMed] [Google Scholar]
- 43.Rota PA, Oberste MS, Monroe SS, Nix WA, Campagnoli R, Icenogle JP, Penaranda S, Bankamp B, Maher K, Chen MH, Tong S, Tamin A, Lowe L, Frace M, DeRisi JL, Chen Q, Wang D, Erdman DD, Peret TC, Burns C, Ksiazek TG, Rollin PE, Sanchez A, Liffick S, Holloway B, Limor J, McCaustland K, Olsen-Rasmussen M, Fouchier R, Gunther S, Osterhaus AD, Drosten C, Pallansch MA, Anderson LJ, Bellini WJ. Characterization of a novel coronavirus associated with severe acute respiratory syndrome. Science. 2003;300:1394–1399. doi: 10.1126/science.1085952. [DOI] [PubMed] [Google Scholar]
- 44.Alshukairi AN, Zheng J, Zhao J, Nehdi A, Baharoon SA, Layqah L, Bokhari A, Al Johani SM, Samman N, Boudjelal M, Ten Eyck P, Al-Mozaini MA, Zhao J, Perlman S, Alagaili AN. High prevalence of MERS-CoV infection in camel workers in Saudi Arabia. MBio. 2018;9:e01985-18. doi: 10.1128/mBio.01985-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Skowronski DM, Astell C, Brunham RC, Low DE, Petric M, Roper RL, Talbot PJ, Tam T, Babiuk L. Severe acute respiratory syndrome (SARS): a year in review. Annu Rev Med. 2005;56:357–381. doi: 10.1146/annurev.med.56.091103.134135. [DOI] [PubMed] [Google Scholar]
- 46.World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV). https://www.who.int/emergencies/mers-cov/en/. Accessed 10 Apr 2019.
- 47.Cho SY, Kang JM, Ha YE, Park GE, Lee JY, Ko JH, Lee JY, Kim JM, Kang CI, Jo IJ, Ryu JG, Choi JR, Kim S, Huh HJ, Ki CS, Kang ES, Peck KR, Dhong HJ, Song JH, Chung DR, Kim YJ. MERS-CoV outbreak following a single patient exposure in an emergency room in South Korea: an epidemiological outbreak study. Lancet. 2016;388:994–1001. doi: 10.1016/S0140-6736(16)30623-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Chowell G, Abdirizak F, Lee S, Lee J, Jung E, Nishiura H, Viboud C. Transmission characteristics of MERS and SARS in the healthcare setting: a comparative study. BMC Med. 2015;13:210. doi: 10.1186/s12916-015-0450-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hunter JC, Nguyen D, Aden B, Al Bandar Z, Al Dhaheri W, Abu Elkheir K, Khudair A, Al Mulla M, El Saleh F, Imambaccus H, Al Kaabi N, Sheikh FA, Sasse J, Turner A, Abdel Wareth L, Weber S, Al Ameri A, Abu Amer W, Alami NN, Bunga S, Haynes LM, Hall AJ, Kallen AJ, Kuhar D, Pham H, Pringle K, Tong S, Whitaker BL, Gerber SI, Al Hosani FI. Transmission of Middle East respiratory syndrome coronavirus infections in healthcare settings, Abu Dhabi. Emerg Infect Dis. 2016;22:647–656. doi: 10.3201/eid2204.151615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Li Y, Carroll DS, Gardner SN, Walsh MC, Vitalis EA, Damon IK. On the origin of smallpox: correlating variola phylogenics with historical smallpox records. Proc Natl Acad Sci U S A. 2007;104:15787–15792. doi: 10.1073/pnas.0609268104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Fenner FHD, Isao A, Zdenek J, Ladnyi ID. Smallpox and its eradication. Geneva: World Health Organization; 1988. [Google Scholar]
- 52.Koplow DA. Smallpox: the fight to eradicate a global scourge. Berkeley: University of California Press; 2004. [Google Scholar]
- 53.Riedel S. Edward Jenner and the history of smallpox and vaccination. Proc (Bayl Univ Med Cent) 2005;18:21–25. doi: 10.1080/08998280.2005.11928028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Killingley B, Nguyen-Van-Tam J. Routes of influenza transmission. Influenza Other Respir Viruses. 2013;7(Suppl 2):42–51. doi: 10.1111/irv.12080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Bridges CB, Kuehnert MJ, Hall CB. Transmission of influenza: implications for control in health care settings. Clin Infect Dis. 2003;37:1094–1101. doi: 10.1086/378292. [DOI] [PubMed] [Google Scholar]
- 56.van Riel D, Munster VJ, de Wit E, Rimmelzwaan GF, Fouchier RA, Osterhaus AD, Kuiken T. Human and avian influenza viruses target different cells in the lower respiratory tract of humans and other mammals. Am J Pathol. 2007;171:1215–1223. doi: 10.2353/ajpath.2007.070248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Shinya K, Kawaoka Y. Influenza virus receptors in the human airway. Uirusu. 2006;56:85–89. doi: 10.2222/jsv.56.85. [DOI] [PubMed] [Google Scholar]
- 58.Baccam P, Beauchemin C, Macken CA, Hayden FG, Perelson AS. Kinetics of influenza A virus infection in humans. J Virol. 2006;80:7590–7599. doi: 10.1128/JVI.01623-05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Ng S, Lopez R, Kuan G, Gresh L, Balmaseda A, Harris E, Gordon A. The timeline of influenza virus shedding in children and adults in a household transmission study of influenza in Managua, Nicaragua. Pediatr Infect Dis J. 2016;35:583–586. doi: 10.1097/INF.0000000000001083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Lehners N, Tabatabai J, Prifert C, Wedde M, Puthenparambil J, Weissbrich B, Biere B, Schweiger B, Egerer G, Schnitzler P. Long-term shedding of influenza virus, parainfluenza virus, respiratory syncytial virus and nosocomial epidemiology in patients with hematological disorders. PLoS One. 2016;11:e0148258. doi: 10.1371/journal.pone.0148258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Biggerstaff M, Cauchemez S, Reed C, Gambhir M, Finelli L. Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: a systematic review of the literature. BMC Infect Dis. 2014;14:480. doi: 10.1186/1471-2334-14-480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Herold S, Becker C, Ridge KM, Budinger GR. Influenza virus-induced lung injury: pathogenesis and implications for treatment. Eur Respir J. 2015;45:1463–1478. doi: 10.1183/09031936.00186214. [DOI] [PubMed] [Google Scholar]
- 63.Taubenberger JK, Morens DM. The pathology of influenza virus infections. Annu Rev Pathol. 2008;3:499–522. doi: 10.1146/annurev.pathmechdis.3.121806.154316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Chertow DS, Memoli MJ. Bacterial coinfection in influenza: a grand rounds review. JAMA. 2013;309:275–282. doi: 10.1001/jama.2012.194139. [DOI] [PubMed] [Google Scholar]
- 65.Ke C, Mok CKP, Zhu W, Zhou H, He J, Guan W, Wu J, Song W, Wang D, Liu J, Lin Q, Chu DKW, Yang L, Zhong N, Yang Z, Shu Y, Peiris JSM. Human infection with highly pathogenic avian influenza A(H7N9) virus, China. Emerg Infect Dis. 2017;23:1332–1340. doi: 10.3201/eid2308.170600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Luczo JM, Stambas J, Durr PA, Michalski WP, Bingham J. Molecular pathogenesis of H5 highly pathogenic avian influenza: the role of the haemagglutinin cleavage site motif. Rev Med Virol. 2015;25:406–430. doi: 10.1002/rmv.1846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Gomez Lorenzo MM, Fenton MJ. Immunobiology of influenza vaccines. Chest. 2013;143:502–510. doi: 10.1378/chest.12-1711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Remington PL, Hall WN, Davis IH, Herald A, Gunn RA. Airborne transmission of measles in a physician’s office. JAMA. 1985;253:1574–1577. doi: 10.1001/jama.1985.03350350068022. [DOI] [PubMed] [Google Scholar]
- 69.Laksono BM, de Vries RD, McQuaid S, Duprex WP, de Swart RL. Measles virus host invasion and pathogenesis. Viruses. 2016;8:210. doi: 10.3390/v8080210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Ludlow M, McQuaid S, Milner D, de Swart RL, Duprex WP. Pathological consequences of systemic measles virus infection. J Pathol. 2015;235:253–265. doi: 10.1002/path.4457. [DOI] [PubMed] [Google Scholar]
- 71.de Swart RL, Ludlow M, de Witte L, Yanagi Y, van Amerongen G, McQuaid S, Yuksel S, Geijtenbeek TB, Duprex WP, Osterhaus AD. Predominant infection of CD150+ lymphocytes and dendritic cells during measles virus infection of macaques. PLoS Pathog. 2007;3:e178. doi: 10.1371/journal.ppat.0030178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Perry RT, Halsey NA. The clinical significance of measles: a review. J Infect Dis. 2004;189(Suppl 1):S4–16. doi: 10.1086/377712. [DOI] [PubMed] [Google Scholar]
- 73.Guerra FM, Bolotin S, Lim G, Heffernan J, Deeks SL, Li Y, Crowcroft NS. The basic reproduction number (R0) of measles: a systematic review. Lancet Infect Dis. 2017;17:e420–e428. doi: 10.1016/S1473-3099(17)30307-9. [DOI] [PubMed] [Google Scholar]
- 74.Leuridan E, Hens N, Hutse V, Ieven M, Aerts M, Van Damme P. Early waning of maternal measles antibodies in era of measles elimination: longitudinal study. BMJ. 2010;340:c1626. doi: 10.1136/bmj.c1626. [DOI] [PubMed] [Google Scholar]
- 75.Griffin DE. Measles virus-induced suppression of immune responses. Immunol Rev. 2010;236:176–189. doi: 10.1111/j.1600-065X.2010.00925.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Mina MJ, Metcalf CJ, de Swart RL, Osterhaus AD, Grenfell BT. Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Science. 2015;348:694–699. doi: 10.1126/science.aaa3662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Yu IT, Li Y, Wong TW, Tam W, Chan AT, Lee JH, Leung DY, Ho T. Evidence of airborne transmission of the severe acute respiratory syndrome virus. N Engl J Med. 2004;350:1731–1739. doi: 10.1056/NEJMoa032867. [DOI] [PubMed] [Google Scholar]
- 78.Chowell G, Castillo-Chavez C, Fenimore PW, Kribs-Zaleta CM, Arriola L, Hyman JM. Model parameters and outbreak control for SARS. Emerg Infect Dis. 2004;10:1258–1263. doi: 10.3201/eid1007.030647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Liu L, Wei Q, Alvarez X, Wang H, Du Y, Zhu H, Jiang H, Zhou J, Lam P, Zhang L, Lackner A, Qin C, Chen Z. Epithelial cells lining salivary gland ducts are early target cells of severe acute respiratory syndrome coronavirus infection in the upper respiratory tracts of rhesus macaques. J Virol. 2011;85:4025–4030. doi: 10.1128/JVI.02292-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Kuba K, Imai Y, Rao S, Gao H, Guo F, Guan B, Huan Y, Yang P, Zhang Y, Deng W, Bao L, Zhang B, Liu G, Wang Z, Chappell M, Liu Y, Zheng D, Leibbrandt A, Wada T, Slutsky AS, Liu D, Qin C, Jiang C, Penninger JM. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat Med. 2005;11:875–879. doi: 10.1038/nm1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Gu J, Gong E, Zhang B, Zheng J, Gao Z, Zhong Y, Zou W, Zhan J, Wang S, Xie Z, Zhuang H, Wu B, Zhong H, Shao H, Fang W, Gao D, Pei F, Li X, He Z, Xu D, Shi X, Anderson VM, Leong AS. Multiple organ infection and the pathogenesis of SARS. J Exp Med. 2005;202:415–424. doi: 10.1084/jem.20050828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol. 2004;203:631–637. doi: 10.1002/path.1570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Gu J, Korteweg C. Pathology and pathogenesis of severe acute respiratory syndrome. Am J Pathol. 2007;170:1136–1147. doi: 10.2353/ajpath.2007.061088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Middle East Respiratory Syndrome Coronavirus (MERS-CoV). WHO MERS-CoV Global Summary and risk assessment. https://www.who.int/emergencies/mers-cov/mers-summary-2016.pdf. Accessed 19 Apr 2017.
- 85.Corman VM, Albarrak AM, Omrani AS, Albarrak MM, Farah ME, Almasri M, Muth D, Sieberg A, Meyer B, Assiri AM, Binger T, Steinhagen K, Lattwein E, Al-Tawfiq J, Muller MA, Drosten C, Memish ZA. Viral shedding and antibody response in 37 patients with Middle East respiratory syndrome coronavirus infection. Clin Infect Dis. 2016;62:477–483. doi: 10.1093/cid/civ951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Oh MD, Park WB, Choe PG, Choi SJ, Kim JI, Chae J, Park SS, Kim EC, Oh HS, Kim EJ, Nam EY, Na SH, Kim DK, Lee SM, Song KH, Bang JH, Kim ES, Kim HB, Park SW, Kim NJ. Viral load kinetics of MERS coronavirus infection. N Engl J Med. 2016;375:1303–1305. doi: 10.1056/NEJMc1511695. [DOI] [PubMed] [Google Scholar]
- 87.Song Z, Xu Y, Bao L, Zhang L, Yu P, Qu Y, Zhu H, Zhao W, Han Y, Qin C. From SARS to MERS, thrusting coronaviruses into the spotlight. Viruses. 2019;11:59. doi: 10.3390/v11010059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Kim SY, Park SJ, Cho SY, Cha RH, Jee HG, Kim G, Shin HS, Kim Y, Jung YM, Yang JS, Kim SS, Cho SI, Kim MJ, Lee JS, Lee SJ, Seo SH, Park SS, Seong MW. Viral RNA in blood as indicator of severe outcome in Middle East respiratory syndrome coronavirus infection. Emerg Infect Dis. 2016;22:1813–1816. doi: 10.3201/eid2210.160218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Widagdo W, Raj VS, Schipper D, Kolijn K, van Leenders G, Bosch BJ, Bensaid A, Segales J, Baumgartner W, Osterhaus A, Koopmans MP, van den Brand JMA, Haagmans BL. Differential expression of the Middle East respiratory syndrome coronavirus receptor in the upper respiratory tracts of humans and dromedary camels. J Virol. 2016;90:4838–4842. doi: 10.1128/JVI.02994-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Wehrle PF, Posch J, Richter KH, Henderson DA. An airborne outbreak of smallpox in a German hospital and its significance with respect to other recent outbreaks in Europe. Bull World Health Organ. 1970;43:669–679. [PMC free article] [PubMed] [Google Scholar]
- 91.Eichner M, Dietz K. Transmission potential of smallpox: estimates based on detailed data from an outbreak. Am J Epidemiol. 2003;158:110–117. doi: 10.1093/aje/kwg103. [DOI] [PubMed] [Google Scholar]
- 92.Breman JG, Henderson DA. Diagnosis and management of smallpox. N Engl J Med. 2002;346:1300–1308. doi: 10.1056/NEJMra020025. [DOI] [PubMed] [Google Scholar]
- 93.Stanford MM, McFadden G, Karupiah G, Chaudhri G. Immunopathogenesis of poxvirus infections: forecasting the impending storm. Immunol Cell Biol. 2007;85:93–102. doi: 10.1038/sj.icb.7100033. [DOI] [PubMed] [Google Scholar]
- 94.Martin DB. The cause of death in smallpox: an examination of the pathology record. Mil Med. 2002;167:546–551. doi: 10.1093/milmed/167.7.546. [DOI] [PubMed] [Google Scholar]
- 95.Sarkar JK, Mitra AC, Mukherjee MK, De SK, Mazumdar DG. Virus excretion in smallpox. 1. Excretion in the throat, urine, and conjunctiva of patients. Bull World Health Organ. 1973;48:517–522. [PMC free article] [PubMed] [Google Scholar]
- 96.Guerrant RL, Walker DH, Weller PF. Tropical infectious diseases: principles, pathogens and practice. Saunders/Elsevier: Edinburgh; 2011. [Google Scholar]
- 97.Gani R, Leach S. Transmission potential of smallpox in contemporary populations. Nature. 2001;414:748–751. doi: 10.1038/414748a. [DOI] [PubMed] [Google Scholar]
- 98.Downie AW, Mc CK, Macdonald A. Viraemia in smallpox. Lancet. 1950;2:513–514. doi: 10.1016/S0140-6736(50)91496-6. [DOI] [PubMed] [Google Scholar]
- 99.Downie AW, McCarthy K, Macdonald A, Maccallum FO, Macrae AE. Virus and virus antigen in the blood of smallpox patients; their significance in early diagnosis and prognosis. Lancet. 1953;265:164–166. doi: 10.1016/S0140-6736(53)90107-X. [DOI] [PubMed] [Google Scholar]
- 100.Mitra AC, Chatterjee SN, Sarkar JK, Manji P, Das AK. Viraemia in haemorrhagic and other forms of smallpox. J Indian Med Assoc. 1966;47:112–114. [PubMed] [Google Scholar]
- 101.Moore ZS, Seward JF, Lane JM. Smallpox. Lancet. 2006;367:425–435. doi: 10.1016/S0140-6736(06)68143-9. [DOI] [PubMed] [Google Scholar]
- 102.Buchman CA, Doyle WJ, Skoner DP, Post JC, Alper CM, Seroky JT, Anderson K, Preston RA, Hayden FG, Fireman P, et al. Influenza A virus--induced acute otitis media. J Infect Dis. 1995;172:1348–1351. doi: 10.1093/infdis/172.5.1348. [DOI] [PubMed] [Google Scholar]
- 103.Sellers SA, Hagan RS, Hayden FG, Fischer WA., 2nd The hidden burden of influenza: a review of the extra-pulmonary complications of influenza infection. Influenza Other Respir Viruses. 2017;11:372–393. doi: 10.1111/irv.12470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Quiambao BP, Gatchalian SR, Halonen P, Lucero M, Sombrero L, Paladin FJ, Meurman O, Merin J, Ruutu P. Coinfection is common in measles-associated pneumonia. Pediatr Infect Dis J. 1998;17:89–93. doi: 10.1097/00006454-199802000-00002. [DOI] [PubMed] [Google Scholar]
- 105.Griffin DE. Measles virus and the nervous system. Handb Clin Neurol. 2014;123:577–590. doi: 10.1016/B978-0-444-53488-0.00027-4. [DOI] [PubMed] [Google Scholar]
- 106.Peiris JS, Lai ST, Poon LL, Guan Y, Yam LY, Lim W, Nicholls J, Yee WK, Yan WW, Cheung MT, Cheng VC, Chan KH, Tsang DN, Yung RW, Ng TK, Yuen KY, SARS Study Group Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet. 2003;361:1319–1325. doi: 10.1016/S0140-6736(03)13077-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Leung WK, To KF, Chan PK, Chan HL, Wu AK, Lee N, Yuen KY, Sung JJ. Enteric involvement of severe acute respiratory syndrome-associated coronavirus infection. Gastroenterology. 2003;125:1011–1017. doi: 10.1016/j.gastro.2003.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Leung GM, Hedley AJ, Ho LM, Chau P, Wong IO, Thach TQ, Ghani AC, Donnelly CA, Fraser C, Riley S, Ferguson NM, Anderson RM, Tsang T, Leung PY, Wong V, Chan JC, Tsui E, Lo SV, Lam TH. The epidemiology of severe acute respiratory syndrome in the 2003 Hong Kong epidemic: an analysis of all 1755 patients. Ann Intern Med. 2004;141:662–673. doi: 10.7326/0003-4819-141-9-200411020-00006. [DOI] [PubMed] [Google Scholar]
- 109.Hui DS, Memish ZA, Zumla A. Severe acute respiratory syndrome vs. the Middle East respiratory syndrome. Curr Opin Pulm Med. 2014;20:233–241. doi: 10.1097/MCP.0000000000000046. [DOI] [PubMed] [Google Scholar]
- 110.Hui DS, Sung JJ. Severe acute respiratory syndrome. Chest. 2003;124:12–15. doi: 10.1378/chest.124.1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Lee N, Hui D, Wu A, Chan P, Cameron P, Joynt GM, Ahuja A, Yung MY, Leung CB, To KF, Lui SF, Szeto CC, Chung S, Sung JJ. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1986–1994. doi: 10.1056/NEJMoa030685. [DOI] [PubMed] [Google Scholar]
- 112.Wong GW, Hui DS. Severe acute respiratory syndrome (SARS): epidemiology, diagnosis and management. Thorax. 2003;58:558–560. doi: 10.1136/thorax.58.7.558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Chu KH, Tsang WK, Tang CS, Lam MF, Lai FM, To KF, Fung KS, Tang HL, Yan WW, Chan HW, Lai TS, Tong KL, Lai KN. Acute renal impairment in coronavirus-associated severe acute respiratory syndrome. Kidney Int. 2005;67:698–705. doi: 10.1111/j.1523-1755.2005.67130.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Assiri A, Al-Tawfiq JA, Al-Rabeeah AA, Al-Rabiah FA, Al-Hajjar S, Al-Barrak A, Flemban H, Al-Nassir WN, Balkhy HH, Al-Hakeem RF, Makhdoom HQ, Zumla AI, Memish ZA. Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: a descriptive study. Lancet Infect Dis. 2013;13:752–761. doi: 10.1016/S1473-3099(13)70204-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Guery B, Poissy J, el Mansouf L, Sejourne C, Ettahar N, Lemaire X, Vuotto F, Goffard A, Behillil S, Enouf V, Caro V, Mailles A, Che D, Manuguerra JC, Mathieu D, Fontanet A, van der Werf S, MERS-CoV Study Group Clinical features and viral diagnosis of two cases of infection with Middle East respiratory syndrome coronavirus: a report of nosocomial transmission. Lancet. 2013;381:2265–2272. doi: 10.1016/S0140-6736(13)60982-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Hijawi B, Abdallat M, Sayaydeh A, Alqasrawi S, Haddadin A, Jaarour N, Alsheikh S, Alsanouri T. Novel coronavirus infections in Jordan, April 2012: epidemiological findings from a retrospective investigation. East Mediterr Health J. 2013;19(Suppl 1):S12–S18. doi: 10.26719/2013.19.supp1.S12. [DOI] [PubMed] [Google Scholar]
- 117.Memish ZA, Zumla AI, Al-Hakeem RF, Al-Rabeeah AA, Stephens GM. Family cluster of Middle East respiratory syndrome coronavirus infections. N Engl J Med. 2013;368:2487–2494. doi: 10.1056/NEJMoa1303729. [DOI] [PubMed] [Google Scholar]
- 118.Who Mers-Cov Research Group. State of knowledge and data gaps of Middle East respiratory syndrome coronavirus (MERS-CoV) in humans. PLoS Curr. 2013;5. [DOI] [PMC free article] [PubMed]
- 119.Arabi YM, Arifi AA, Balkhy HH, Najm H, Aldawood AS, Ghabashi A, Hawa H, Alothman A, Khaldi A, Al Raiy B. Clinical course and outcomes of critically ill patients with Middle East respiratory syndrome coronavirus infection. Ann Intern Med. 2014;160:389–397. doi: 10.7326/M13-2486. [DOI] [PubMed] [Google Scholar]
- 120.Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367:1814–1820. doi: 10.1056/NEJMoa1211721. [DOI] [PubMed] [Google Scholar]
- 121.Al-Tawfiq JA, Hinedi K, Ghandour J, Khairalla H, Musleh S, Ujayli A, Memish ZA. Middle East respiratory syndrome coronavirus: a case-control study of hospitalized patients. Clin Infect Dis. 2014;59:160–165. doi: 10.1093/cid/ciu226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Ajlan AM, Ahyad RA, Jamjoom LG, Alharthy A, Madani TA. Middle East respiratory syndrome coronavirus (MERS-CoV) infection: chest CT findings. AJR Am J Roentgenol. 2014;203:782–787. doi: 10.2214/AJR.14.13021. [DOI] [PubMed] [Google Scholar]
- 123.Zumla A, Hui DS, Perlman S. Middle East respiratory syndrome. Lancet. 2015;386:995–1007. doi: 10.1016/S0140-6736(15)60454-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Saad M, Omrani AS, Baig K, Bahloul A, Elzein F, Matin MA, Selim MA, Al Mutairi M, Al Nakhli D, Al Aidaroos AY, Al Sherbeeni N, Al-Khashan HI, Memish ZA, Albarrak AM. Clinical aspects and outcomes of 70 patients with Middle East respiratory syndrome coronavirus infection: a single-center experience in Saudi Arabia. Int J Infect Dis. 2014;29:301–306. doi: 10.1016/j.ijid.2014.09.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Rao AR. Smallpox. Bombay: The Kothari Book Depot; 1972. [Google Scholar]
- 126.Centers for Disease Control and Prevention. Prevention strategies for seasonal influenza in healthcare settings. https://www.cdc.gov/flu/professionals/infectioncontrol/healthcaresettings.htm. Accessed 17 Apr 2019.
- 127.Merckx J, Wali R, Schiller I, Caya C, Gore GC, Chartrand C, Dendukuri N, Papenburg J. Diagnostic accuracy of novel and traditional rapid tests for influenza infection compared with reverse transcriptase polymerase chain reaction: a systematic review and meta-analysis. Ann Intern Med. 2017;167:394–409. doi: 10.7326/M17-0848. [DOI] [PubMed] [Google Scholar]
- 128.Centers for Disease Control and Prevention. Middle East Respiratory Syndrome (MERS). Interim Patient under Investigation (PUI) guidance and case definitions. https://www.cdc.gov/coronavirus/mers/case-def.html. Accessed 17 Apr 2019.
- 129.Memish ZA, Al-Tawfiq JA, Makhdoom HQ, Assiri A, Alhakeem RF, Albarrak A, Alsubaie S, Al-Rabeeah AA, Hajomar WH, Hussain R, Kheyami AM, Almutairi A, Azhar EI, Drosten C, Watson SJ, Kellam P, Cotten M, Zumla A. Respiratory tract samples, viral load, and genome fraction yield in patients with Middle East respiratory syndrome. J Infect Dis. 2014;210:1590–1594. doi: 10.1093/infdis/jiu292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Woo PC, Yuen KY, Lau SK. Epidemiology of coronavirus-associated respiratory tract infections and the role of rapid diagnostic tests: a prospective study. Hong Kong Med J. 2012;18(Suppl 2):22–24. [PubMed] [Google Scholar]
- 131.Centers for Disease Control and Prevention. Evaluating patients for smallpox: acute, generalized vesicular or pustular rash illness protocol. https://www.cdc.gov/smallpox/clinicians/algorithm-protocol.html. Accessed 17 Apr 2019.
- 132.Chan TC, Fan-Ngai Hung I, Ka-Hay Luk J, Chu LW, Hon-Wai CF. Effectiveness of influenza vaccination in institutionalized older adults: a systematic review. J Am Med Dir Assoc. 2014;15:226.e1–226.e6. doi: 10.1016/j.jamda.2013.10.008. [DOI] [PubMed] [Google Scholar]
- 133.Beck CR, McKenzie BC, Hashim AB, Harris RC, University of Nottingham Influenza and the ImmunoCompromised (UNIIC) Study Group. Nguyen-Van-Tam JS. Influenza vaccination for immunocompromised patients: systematic review and meta-analysis by etiology. J Infect Dis. 2012;206:1250–1259. doi: 10.1093/infdis/jis487. [DOI] [PubMed] [Google Scholar]
- 134.Grohskopf LA, Sokolow LZ, Broder KR, Walter EB, Fry AM, Jernigan DB. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices-United States, 2018-19 influenza season. MMWR Recomm Rep. 2018;67:1–20. doi: 10.15585/mmwr.rr6703a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Paules CI, Marston HD, Eisinger RW, Baltimore D, Fauci AS. The pathway to a universal influenza vaccine. Immunity. 2017;47:599–603. doi: 10.1016/j.immuni.2017.09.007. [DOI] [PubMed] [Google Scholar]
- 136.Centers for Disease Control and Prevention. Influenza antiviral medications: summary for clinicians. https://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm. Accessed 19 Apr 2019.
- 137.Hayden FG, Sugaya N, Hirotsu N, Lee N, de Jong MD, Hurt AC, Ishida T, Sekino H, Yamada K, Portsmouth S, Kawaguchi K, Shishido T, Arai M, Tsuchiya K, Uehara T, Watanabe A, Baloxavir Marboxil Investigators G. Baloxavir marboxil for uncomplicated influenza in adults and adolescents. N Engl J Med. 2018;379:913–923. doi: 10.1056/NEJMoa1716197. [DOI] [PubMed] [Google Scholar]
- 138.World Health Organization Measles vaccines: WHO position paper, April 2017–recommendations. Vaccine. 2019;37:219–222. doi: 10.1016/j.vaccine.2017.07.066. [DOI] [PubMed] [Google Scholar]
- 139.Centers for Disease Control and Prevention. Measles (Rubeola): for healthcare professionals. https://www.cdc.gov/measles/hcp/index.html. Accessed 19 Apr 2019.
- 140.Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005:CD001479. [DOI] [PMC free article] [PubMed]
- 141.World Health Organization. Measles and vitamin A. https://www.who.int/wer/2009/wer8435.pdf#page=3. Accessed 19 Apr 2019.
- 142.Chan JF, Lau SK, To KK, Cheng VC, Woo PC, Yuen KY. Middle East respiratory syndrome coronavirus: another zoonotic betacoronavirus causing SARS-like disease. Clin Microbiol Rev. 2015;28:465–522. doi: 10.1128/CMR.00102-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Albarrak AM, Stephens GM, Hewson R, Memish ZA. Recovery from severe novel coronavirus infection. Saudi Med J. 2012;33:1265–1269. [PubMed] [Google Scholar]
- 144.Omrani AS, Saad MM, Baig K, Bahloul A, Abdul-Matin M, Alaidaroos AY, Almakhlafi GA, Albarrak MM, Memish ZA, Albarrak AM. Ribavirin and interferon alfa-2a for severe Middle East respiratory syndrome coronavirus infection: a retrospective cohort study. Lancet Infect Dis. 2014;14:1090–1095. doi: 10.1016/S1473-3099(14)70920-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7:e35797. doi: 10.1371/journal.pone.0035797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Arita I. Smallpox vaccine and its stockpile in 2005. Lancet Infect Dis. 2005;5:647–652. doi: 10.1016/S1473-3099(05)70242-5. [DOI] [PubMed] [Google Scholar]
- 147.Petersen BW, Damon IK, Pertowski CA, Meaney-Delman D, Guarnizo JT, Beigi RH, Edwards KM, Fisher MC, Frey SE, Lynfield R, Willoughby RE. Clinical guidance for smallpox vaccine use in a postevent vaccination program. MMWR Recomm Rep. 2015;64:1–26. doi: 10.15585/mmwr.rr6404a1. [DOI] [PubMed] [Google Scholar]
- 148.Feery BJ. The efficacy of vaccinial immune globulin. A 15-year study. Vox Sang. 1976;31:68–76. doi: 10.1159/000467368. [DOI] [PubMed] [Google Scholar]
- 149.Sharp JC, Fletcher WB. Experience of anti-vaccinia immunoglobulin in the United Kingdom. Lancet. 1973;1:656–659. doi: 10.1016/S0140-6736(73)92215-0. [DOI] [PubMed] [Google Scholar]
- 150.Mucker EM, Goff AJ, Shamblin JD, Grosenbach DW, Damon IK, Mehal JM, Holman RC, Carroll D, Gallardo N, Olson VA, Clemmons CJ, Hudson P, Hruby DE. Efficacy of tecovirimat (ST-246) in nonhuman primates infected with variola virus (smallpox) Antimicrob Agents Chemother. 2013;57:6246–6253. doi: 10.1128/AAC.00977-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Yang G, Pevear DC, Davies MH, Collett MS, Bailey T, Rippen S, Barone L, Burns C, Rhodes G, Tohan S, Huggins JW, Baker RO, Buller RL, Touchette E, Waller K, Schriewer J, Neyts J, DeClercq E, Jones K, Hruby D, Jordan R. An orally bioavailable antipoxvirus compound (ST-246) inhibits extracellular virus formation and protects mice from lethal orthopoxvirus challenge. J Virol. 2005;79:13139–13149. doi: 10.1128/JVI.79.20.13139-13149.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]