

Abstract
This chapter provides an overview of the medical chart, and its sections. The neuropsychologist will be provided with detailed information about how to decipher some of the many abbreviations, and we also provide the neuropsychologist, who may not be familiar with common lab values with descriptions of the neurologic examination common grading systems such as motor and sensory functions. In addition, this chapter provides a brief overview of neurologic terms commonly encountered in general medical and more detailed neurological examinations along with figures and illustrations of some of these terms.
Keywords: Essential Tremor, Cerebellar Ataxia, Motor Movement, Physiological Tremor, Intention Tremor
Key Points and Chapter Summary
The medical chart has several components and familiarity with the basic structure of each section is important to both effective patient management and quality care
The History and Physical (H&P) is the initial evaluation of a patient upon admission to a hospital, service, or transfer, and is often the most comprehensive source of current patient information
While the basic structure of a H&P is similar across medical disciplines/specialties, elaboration within different sections is often discipline/specialty-specific
The Medical Chart
The quality of care rendered by medical personnel is proportional to the quality of the assessment, diagnosis and management of the patient. While the point of medical training is to ensure consistent high quality patient care, certain variables such as the information available to assist in this process often remain beyond our control. Good assessment and consultation often start with a review of the existing medical chart and records. In this chapter, a practical method for extracting information from often complex, chaotic medical records is reviewed with particular emphasis on information relevant for neuropsychological evaluation (see also Lezak et al. 2004; Victor and Ropper 2001; Zaidat and Lerner 2008, for review).
Inpatient Chart
Various state and federal guidelines mandate the prompt evaluation of an individual admitted to a hospital or longer-term health care facility. The admission note is often the most detailed source of information available in an entire chart, and therefore bears special scrutiny in helping with neuropsychological assessment. The basic form of the admission History and Physical includes the following sub-sections
Chief complaint. This is usually in the form of a succinct sentence often or ideally in the patient’s own words such as “shortness of breath” or “change in mental status” or “admitted for elective cardiac surgery.” The chief complaint encapsulates the reason for admission, at least on the initial basis.
History of present illness. This forms the main narrative of the admission history and physical and often starts with a brief review of past medical history. An example of this might be a “Chief complaint of left-sided weakness” followed by “The patient is a 68-year-old right-handed man with a history of hypertension, diabetes, coronary artery disease admitted for left-sided weakness of 1 day’s duration.” The History of Present Illness often contains additional important information such as who provided the history; whether it was the patient or family or other medical personnel. It may also contain cross-references to other portions of the medical chart such as records obtained from the Emergency Medical Services. More importantly, one needs to scrutinize the History of Present Illness section for what it does not contain, such as important demographic information or vague statements that need to be considered in making one’s own evaluation at a later date.
- Past medical history. Typically, this is a listing of medical conditions, frequently abbreviated. Regulatory agencies such as JCAHO have rightly criticized the practice of abbreviations in medical charts as they can be confusing or ambiguous, and this may impact patient quality of care. Caution should be given in considering the source of medical history and confirming the list of critical past illnesses, as these can be in error and, if so, may lead to erroneous conclusions about contributing factors in the patient’s current condition. For example, a patient with an erroneously reported history of Diabetes, Hypertension, or Coronary Artery Disease may be evaluated differently when presenting with stroke symptoms only to find out they have blood clots (phlebitis) after a long journey in a sedentary position.
Table 2.1.
Abbreviations for common medical diseases, conditions, and termsAbbreviation/Acronym Medical Term, Condition, Disease AD Alzheimer’s disease OR Attachment disorder ADD(-R) Attention deficit disorder(-resistant) ADEM Acute disseminated encephalopathy ADHD Attention deficit hyperactivity disorder AF Atrial fibrillation AIDS Acquired immune deficiency syndrome ALS Amyotrophic lateral sclerosis (Lou-Gehrig’s disease) APS Antiphospholipid syndrome ARDS Acute respiratory distress syndrome ASD Autism spectrum disorders (see also PDD) AVM/ AVMs Arteriovenous malformations BEB Benign essential bepharospasm BPH Benign prostatic hyperplasia BSE Bovine spongiform encephalopathy CAD Coronary artery disease CADASIL Cerebral autosomal dominant arteriopathy with sub-cortical infarcts and leukoencephalopathy CAT Computerized axial tomography study CCU Critical care unit OR Coronary care unit CF Cystic fibrosis CFS Chronic fatigue syndrome CH Cluster headache CHD Congenital heart disease OR Coronary heart disease OR Congenital hip dysplasia CHF Congestive heart failure CICU Cardiac intensive care unit CIPD Chronic inflammatory demyelinating polyneuropathy CJD Creutzfeldt-Jakob disease (see also SSE) COPD Chronic obstructive pulmonary disease CRF Chronic renal failure CSA Central sleep apnea CSF Cerebrospinal fluid CT Computerized tomography study CVD Cardiovascular disease DM (I or II) Diabetes mellitus, [Type I (juvenile); Type 2 (acquired) DLB Dementia with Lewy bodies (also DLBD) DTs Delirium tremens ED Emergency department OR emotionally disturbed EDS Ehlers-danlos syndrome OR excessive daytime sleepiness EMR Electronic medical record EPS Extrapyramidal symptoms ESRD End state renal disease FAE Fetal alcohol effects FAS (FASDs) Fetal alcohol syndrome (Disorders) FMA Focal muscular atrophies FMLA Family medical leave act FXS Fragile X syndrome GAD Generalized anxiety disorder GAS (disease) Group A streptococcal disease GBS (disease) Guillain-barre syndrome OR Group B streptococcal (disease) GD Gestational diabetes GERD Gastroesophageal reflux disease HA (H/A) Headaches HD Huntington’s disease HTN Hypertension HPV Infection Human papillomavirus infection HSV (infection) Herpes Simplex Virus IBD Inflammatory bowel disease OR Ichthyosis bullosa of siemens IS Infantile spasm JRA Juvenile rheumatoid arthritis LD Learning disability OR Legionnaires’ disease LKS Landau-Kleffner syndrome LP Lipoid proteinosis OR Little Person MD Muscular dystrophy MMR(V) Measles, mumps, rubella (varicella) MND Motor neuron disease MPS (I to VII) Mucopolysaccharoidosis (Type _) MR(/DD) (MRDD) Mentally retarded/Developmentally disabled MRI Magnetic resonance imaging MS Multiple sclerosis NCL Neuronal ceroid lipofuscinosis NF (1 or 2) Neurofibromatosis (type __) NICU Neonatal intensive care unit NLD (NVLD) Nonverbal learning disorder NP (NPC1) Niemann-pick disease (type C1) NPH Normal pressure hydrocephalus NSU Neurosciences (Neurological) intensive care unit OCD Obsessive-compulsive disorder ODD Oppositional defiant disorder OPCA Olivopontocerebellar atrophy OSA Obstructive sleep apnea PACU Post anesthesia care unit PCP Primary care physician PD Parkinson’s disease PICU Pediatric intensive care unit PDD (NOS) Pervasive developmental disorder (Not Otherwise Specified) PML Progressive multifocal leukoencephalopathy PMS Premenstrual syndrome POTS Postural orthostatic tachycardia syndrome PSP Progressive supranuclear palsy PVL Periventricular leukomalacia RA Rheumatoid arthritis RIND Reversible ischemic neurologic deficit RLS Restless legs syndrome ROP Retinopathy of prematurity RSD Reflex sympathetic dystrophy RTI Respiratory tract infection SARS Severe acute respiratory syndrome SB Spina bifida SBS (SIS) Shaken baby syndrome (Shaken infant syndrome) SIDS Sudden infant death syndrome SLE Systemic lupus erythematosus SMA Spinal muscular atrophy SPS Stiff person syndrome SSE Subacute spongiform encephalitis SSPE Subacute sclerosing panencephalitis STD Sexually transmitted disease SWS Sturge-weber syndrome TB Tuberculosis TBI Traumatic brain injury TCS Tethered cord syndrome TIA Transient ischemic attack TMJ (TMD) Temporomandibular joint disorder TS Tourette syndrome OR Tuberous sclerosis TSC Tuberous sclerosis TSE Transmissible spongiform encephalopathies UTI Urinary tract infection VD Venereal disease VHF Viral hemorrhagic fever VSD Ventricular septal defect WD Wilson’s disease Family and social history . Although this is usually a very truncated section of the history and physical, it is of importance in interpretation of any neuropsychological testing. This is one of the few sections that actually gives a sense of the person as living on a day-to-day basis. It will frequently contain information such as marital status or gender, tobacco, alcohol, and drug abuse. It may also contain information about the number of children, although in an inpatient setting this is often not specified. Of special importance is the patient’s educational history and primary language (if specified), as many neuropsychological skills and test performances vary considerably with education, and consideration should be given to evaluate a patient in his/her primary language. For example, the same memory capacity would not be expected of someone with 4 years of education compared to someone with a graduate degree. If not a Fluent English speaker, performances and expectations should be altered. For practitioners who do not speak the language of the patient, options may include identifying another practitioner who does speak the language or finding an interpreter (caution should be taken if a family member or friend of the patient is used as this may introduce bias). If unavailable basic cognitive testing using nonverbal tasks/tests may provide some useful information, but interpretation and conclusions should be viewed with caution.
Review of systems . The review of systems should ideally complement previous medical history. A complete review of systems encompasses constitutional symptoms as well as up to about 15 bodily systems. Frequently, this may be just marked as NC for noncontributory.
Vital signs . Typically, this would include Temperature (recorded either in Centigrade or Fahrenheit), Pulse (per minute), Respirations (per minute) and Blood Pressure with systolic recorded over diastolic. In charting, these are often abbreviated as T, P, R, B/P, and often noted as numbers in that order. Caution is again warranted as the information provided here may have been copied from earlier in the chart (or another chart), such as the evaluation in the emergency room, and may not reflect information at the time of the writing of the admission History and Physical. It is also not uncommon in a busy inpatient hospital setting for the actual writing of the admission History and Physical to be delayed for several hours following the actual examination.
Rule of thumb: Outline of the H&P
Chief Complaint
- History of Present Illness
- Current medications
- Past History
- Medical history (including Psychiatric)
- Family and Social history
- Review of Systems
- Head, Eyes, Ears, Nose and Throat (HEENT)
- Neck
- Lungs
- Cardiovascular
- Abdominal
- Extremities
- Back
- Genito-urinary
- Neurologic
- Cranial Nerves
- Mental Status
- Motor
- Sensory
- Gait/Station
- Laboratory
The following subsections of the Review of Systems are often found:
HEENT. This stands for Head, Eyes, Ears, Nose, and Throat. A frequent abbreviation is NC/AT which stands for Normocephalic, Atraumatic. Ideally, this section will identify any observed defects and state of the skin, oral mucosa, dentition, use of hearing aides, or glasses. However, this information is often omitted. Again, cross-reference with the history as described above is often useful. Gross vision problems may be noted here (or in CN exam section), including strabismus, exotropia, esotropia, or ambylopia. Strabismus is the lack of muscle co-ordination between the eyes. Exotropia refers to an eye being deviated away from midline (deviated outward), and is a form of strabismus. Esotropia refers to an eye being deviated towards the midline (deviated inward), and is a form of strabismus. Amblyopia refers to when the brain does not process visual signals of a misaligned eye (the eye that is exotropic or esotropic), resulting in vision being based on one eye and a patient losing depth perception. Strabismus refers to the condition of misaligned eyes when looking ahead.
Neck . This is often described as supple, a rigid neck being a concerning finding regarding the possibility of meningitis in a patient particularly who is febrile. There may be referral to nuchal (neck) rigidity which may be accompanied by a Brudzinski’s sign (raising of the legs towards the chest when the head is bent forward at the neck) often associated with meningeal irritation or inflammation. Other abbreviations seen here would be JVD, standing for jugular venous distention, which may be increased with right heart failure as with pulmonary hypertension, for example. There may also be references to the size of the thyroid as well as the presence or absence of carotid bruits (an abnormal sound made by blood in the carotid arteries when it swirls past a stenotic or ulcerative plaque).
Lungs or chest. This may or may not include a breast examination. A variety of maneuvers are taught to medical students to describe chest findings. The most common abbreviation here is CTA (Clear To Auscultation) meaning the quadrants of the chest do not demonstrate any abnormal (i.e. different or atypical) sound when thumped or listened to (ausculated). It is less likely, particularly with more senior clinicians, to have a detailed chest examination unless they are performed by a pulmonologist or a cardiologist. Other findings of note may include findings suspicious for a pleural effusion such as dullness at the base or evidence for pneumonia such as crackles or decreased breath sounds. The presence of wheezes suggestive of obstructive airway disease is sometimes noted as well. These comparisons are often reported by chest or lung quadrant indicating a more precise area of abnormal findings.
Cardiovascular. This refers primarily to the heart sounds on auscultation, but may also contain information regarding peripheral arterial disease. Most commonly, it may say normal S1 S2 (S refers to sound and S1–4 refers to the 1st through 4th heart sounds in a normal heart beat) referring to the normal opening heart sounds. The presence of additional heart sounds which are nonspecific findings include the possibility of an abnormal S3 or S4. The presence of murmurs is often noted, and this may be abbreviated as an M. Pulses may also be included under cardiovascular. The dorsalis pedis pulse (or pedal pulse) is abbreviated as DP and often will be marked as +/+; the initial + referring to their right side and the second + to the left side.
Abdomen. Frequently abbreviated as ABD. The most common abbreviations here are BS for bowel sounds and NT for non-tender. Also noted is focal tenderness or masses, and sometimes the presence of an aortic or femoral bruit may be located here rather than under the cardiovascular examination.
Extremities. Frequently abbreviated as EXT. The most common abbreviation is C/C/E standing for cyanosis, clubbing, or edema. The presence of osteoarthritic changes may be noted here, as may be congenital or acquired deformities such as an amputation. This is sometimes accompanied by a drawing of an affected or infected extremity. Frequently, the pulse is recorded and relevant here, and may be obtained from two extremities (e.g., the dorsalis pedis pulses may be recorded here rather than under the cardiovascular examination). Evaluation is based not only on recording abnormalities but also symmetry. Differences in symmetry in either palor, size or functionality may be noted here. Limitations in movement, such as inability to abduct or adduct a limb may be noted here. Abduct(ion) is action that moves a body part away from the midline or center axis along an horizontal plane. Adduct(ion) is action moving a body part toward the midline or center axis.
Back. This may or may not be present. A common abbreviation is CVA or costovertebral angle (this refers to the angle of the spine and ribs) or CVAT for costovertebral angle tenderness which may or may not be present. The presence of scoliosis or kyphosis may also be noted here. Also noted here may be any complaints of pain and the distribution of the region of the pain, which may be helpful in differentiating central and peripheral from referred pain that may be associated with organ dysfunction.
Rectal. This may be included under the abdominal examination or it may be deferred. Often times, abbreviations here refer to the presence or absence of occult blood such as determined with the guaiac screening card or the presence of normal rectal reflexes indicative of normal sacral spinal cord function.
Genitourinary. Abbreviated as GU. This would include vaginal or external male genitalia examination including the penis, scrotum, and testes. This examination may also be deferred in inpatient evaluations.
Neurological. The neurologic examination is frequently replete with abbreviations. The importance of the neurologic examination to neuropsychological evaluation cannot be overstated. The most important piece of information available to the consulting neurologist or neuropsychologist is a prior neurological examination noted in sufficient depth to reassure the examiner that it was performed with more than cursory inspection. The components of the Neurologic examination are elaborated below.
Mental status. This is frequently abbreviated as AO × 3 standing for alert, oriented to person, place, and time. Occasionally one may see orientation described as AO × 4 with the “4” referring to situation or circumstances. Just as commonly, one will see AAO × 3 (or AAO × 4) which stands for Awake, Alert and Oriented to person, place, and time (and circumstances/situation). A more detailed listing of specific findings such as a score obtained for the Mini-Mental State Exam (MMSE; Folstein et al. 1975) may be found (e.g., 30/30), as well as descriptions of which items the patient failed. This section should include observations regarding attention, language, memory and insight/awareness of any current problems. Notation of defects in orientation, language problems (dysarthria, expressive/receptive aphasia, paraphasias) may be reported here. This section may also report about the patient’s mood and affect along with presence of hallucinations or delusions and risk of harm to self or others. The presence of more specific observations indicates the person was examined in depth, since the designation of “AO × 3 or AAO × 3” does not indicate a full or detailed exam was performed.
Cranial nerves . These are often summarized as “CN II-XII intact.” Cranial nerve I (olfactory nerve) is generally not tested. As with mental status, it is not always clear when this is a cursory evaluation versus a summation of a detailed examination. See 10.1007/978-0-387-76978-3_3 for review of anatomy of Cranial Nerves, and 10.1007/978-0-387-76978-3_4 for list of the Cranial Nerves and methods for assessment. Neurologists will often group cranial nerves into functional clusters including smell, taste, vision and eye movement, hearing, swallowing, and facial and neck strength and sensation. Sometimes, one will see “CN I–XII were intact (or WNL),” indicating sense of smell was evaluated. However, a more detailed exam will provide clear indication how the CN’s were tested (e.g., “each nostril tested separately, and pt. able to identify several common scents.”).
Motor examination. This includes muscle tone (resistance to passive movement), bulk, strength, often expressed according to the 0–5 Medical Research Council (MRC) grading scale (Table 2.2). Deep tendon reflexes (DTRs) should be noted here. Frequently, these are provided along with a stick drawing of a person with reflexes noted (see Fig. 2.1 and Table 2.3). Plantar responses may also be provided here, and may be noted along with DTRs (see Fig. 2.1). Figure 2.2 illustrates how the plantar response can be elicited.
Table 2.2.
Grading of muscle strength (MRC scale)
| Grading of muscle strength | Qualitative descriptor of muscle grading |
|---|---|
| 0 | No palpable muscle contraction |
| 1 | A flicker or trace of contraction |
| 2 | Active movement with gravity eliminated |
| 3 | Movement against gravity but not resistance |
| 4− | Active movement against gravity and slight resistance |
| 4 | Active movement against gravity and resistance |
| 4+ | Active movement against gravity and strong resistance |
| 5 | Full active range of motion and normal muscle resistance |
A muscle grading of 0 is verbally discussed as “muscle strength is/was zero or zero out of five”.
Fig. 2.1.
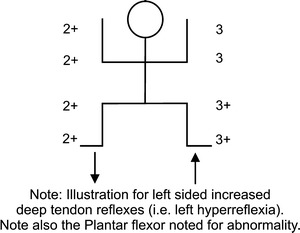
Common notation used to record reflexes as part of a neurological exam
Table 2.3.
Grading of deep tendon reflexes (DTRs)
| Grading of DTRs | Qualitative descriptor of reflex grading |
|---|---|
| 0 | Not present, even with facilitory procedure |
| 1 | Present but reduced or weak |
| 2 | Normal |
| 2+ | Normal, but somewhat brisk (high normal) |
| 3 | Brisk |
| 3+4 (or 3+) | Very brisk, but no clonus |
| 4 | Pathologically brisk with clonus |
Reflex grading of 2+ throughout, is discussed as “reflexes were 2+ throughout”.
Fig. 2.2.
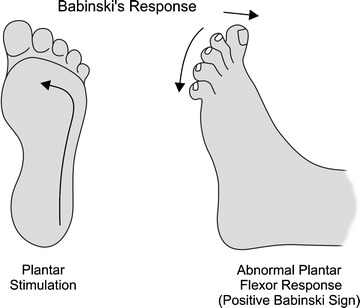
Illustration of the Plantar (Babinski) reflex
The presence of a abnormal movements/movement disorder (e.g., tremor, jerks, incoordination), apraxia, ataxia, hypertonicity (rigidity), hypotonicity (flaccidity) or other abnormalities of gait and station are also often noted here. Tremor description should indicate where the tremor is present (e.g., upper extremity, lower extremity, head), when it is present (i.e., continuous, under stress, only at rest), and the severity of the tremor (see Fig. 2.3 for illustration of tremors). A variety of terms may be used to describe when it is present, but the most common will be action tremor (including postural, kinetic, physiological, and intention tremors) or resting tremor (classically, Parkinsonian tremor). Among action tremors, the most common clinically diagnosed type is essential tremor (ET), which is a tremor of 4–8 Hz most predominant when a static limb posture is maintained, but may also be evident when moving (intention tremor). Classically, it affects the upper limbs bilaterally, but may present worse in one limb (typically dominant hand). It may also involve the head, termed titubation, with a nodding type of movement. Involvement can include jaw, lips, and larynx, such that the patient’s voice has a quavering quality. It is uncommon for lower extremities to be markedly affected by ET. It can progress to be disabling, making writing illegible and preventing a patient from holding a cup of water to drink (see also 10.1007/978-0-387-76978-3_19, this volume, for further review of ET and other movement disorders). Physiological tremor is present in all normal individuals, and is of high frequency (8–13 Hz) and low amplitude such that it is not seen by the naked eye nor appreciated by most people. When exaggerated, termed Enhanced Physiological tremor, by fright, anxiety, extreme exertion, withdraw from alcohol, toxic effects from some chemicals (caffeine, lithium, etc.) or metabolic dysfunction (e.g., hyperthyroidism or hypoglycemia), the physiological tremor increases to be seen and to disrupt routine activities. Enhanced physiological tremor can appear like ET, and is most easily appreciated when holding arms out with fingers outstretched. Intention tremor refers to a tremor distinguished from other action or postural tremor by its form and associated features. Intention tremor is absent at rest and the initial start of a movement. However, as increasingly fine movement is needed for an act (i.e., picking up a full cup of water), the tremor becomes present with a sideways oscillation at about 2–4 Hz of increasingly large amplitude that often continues after the target is reached. Intention tremor is always associated with cerebellar ataxia.
Fig. 2.3.
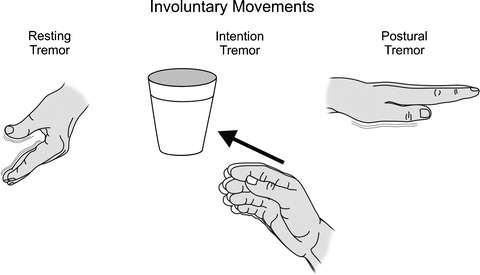
Illustration and descriptions for common types of tremors
Other abnormal movements, such as chorea, athetosis, dystonias, ballismus (often hemiballismus) or akinesia, are often noted here. Choreiform movements may involve the proximal or distal muscles and are involuntary, excessive, jerky, irregularly timed, and randomly distributed. These movements can vary from subtle (appearing as “restlessness” to unstable dance-like gait while walking), to more severe (disabling flow of continuous extreme and violent movements). They are frequently associated with basal ganglia diseases. Athetosis describes slow writhing-like movements that are slower than choreiform movements, but may be described as “slow choreiform movements.” Choreoathetosis is an “intermediate” form of choreiform movements. Ballismus describes an extreme of choreiform movement in which motor movements are rapid and include violent flinging movements. It typically involves an involuntary, continuous, uncoordinated movement involving proximal and distal muscle groups resulting in a limb being “flung out.” It typically involves one side of the body, termed hemiballismus, but bilateral paraballismus has been reported. Ballismus is considered an extreme choreiform motor movement. Akinesia is lack of movement.
Motor abnormalities of hypertonicity/rigidity [e.g., spasticity, cogwheel rigidity, lead pipe rigidity, paratonia (gegenhalten), etc.] or hypotonicity are also frequently noted here. Hypertonicity refers to excess motor tension, presence of spasticity, lead pipe rigidity (rigidity of a limb maintained during and after passive movement of muscle), cogwheel rigidity (passive movement results in a cogwheel or ratchet like catching and quickly releasing as limb moves), and paratonia (involuntary variable resistance to efforts at passive movement of a muscle, like a limb) (see 10.1007/978-0-387-76978-3_10 and 10.1007/978-0-387-76978-3_19, this volume, for more details).
The presence of apraxia, ataxia and/or disorders associated with cerebellar function, such as dysmetria or dysdiadochokinesia, may be identified here or in the Gait and Balance section below. Apraxia refers to the loss of ability to complete previously learned purposeful motor movements, not due to motor weakness (see 10.1007/978-0-387-76978-3_9 for additional review). Examples include ideomotor and ideational apraxia. Ataxia refers to inability to coordinate muscle movements that is not due to motor weakness. Muscle movements will appear clumsy or “jerky.” Ataxia is typically associated with lesions to the cerebellum leading to gait abnormalities (see below), but may also occur due to sensory ataxia from damage to proprioception sensory pathways. Optic ataxia is the inability to coordinate eye–hand motor movements and is observed with Balint’s syndrome (see 10.1007/978-0-387-76978-3_9, this volume). Ataxic respiration is the poor coordination of muscles in chest and diagram, related to damage of the respiratory centers in the medulla oblongata or associated pathways.
Gait and balance. Sometimes included under the motor system, this includes rapid alternating movements (RAM), finger to nose testing (FTN), Romberg testing, and other gait and balance descriptions. Observations of ataxia (e.g., dysmetria, dysdiadochokinesia) may be noted here. Dysmetria is abnormal movements associated with cerebellar damage, and involves dysfunction in the ability to accurately control the range of movement needed for a muscular action. Dysmetria is commonly tested with finger-to-nose testing. The individual with dysmetria will be unable to guide his/her finger to the examiners finger or nose, in which the target is under- or overshot, with attempts at corrections which have a ‘jerky’ quality and overcorrection is often present. Dysdiadochokinesia is the inability to complete rapid alternating movements associated with cerebellar ataxia, and is often tested by having a patient rapidly alternate slapping the palm of each hand and back of the hand on a stable surface (i.e., pronation/supination test). Gait may be described with various terms, but some of the more common include: normal, spastic, apraxic (wide-based), ataxic (also wide-based), parkinsonian, steppage, or scissored gait (see Fig. 2.4 for illustration and summary description of common gait abnormalities).
Fig. 2.4.
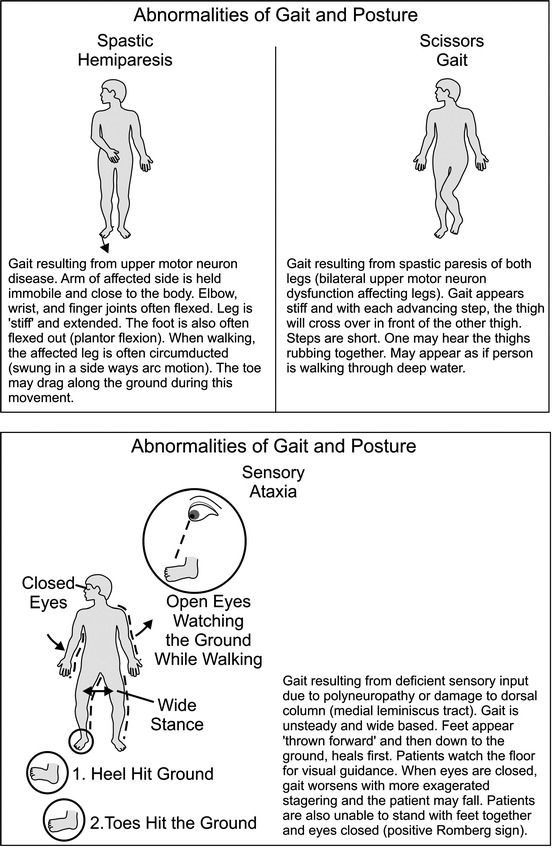
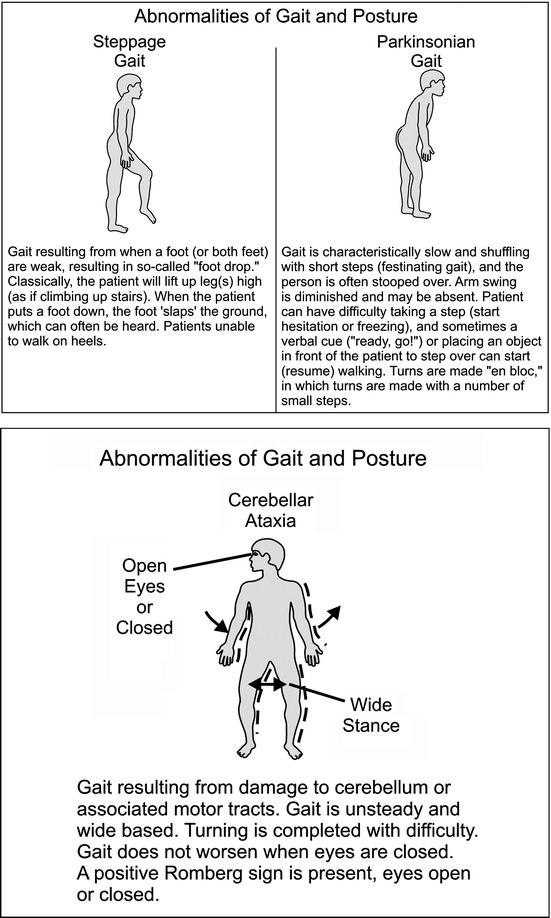
Illustration and description of common gait abnormalities
Sensory. Basic sensory modalities include light touch, pain sensation, vibratory sensation and joint position testing. “Higher order” sensory testing such as two point discrimination, sensory extinction, and/or graphesthesia may be included here. Figure 2.5 illustrates a bedside neurological examination to assess for graphesthesia. While this illustrates using the patient’s palm, it may also be tested on the patient’s finger tips. Presence of agraphasthesia is associated with contralateral parietal lobe damage.
Fig. 2.5.
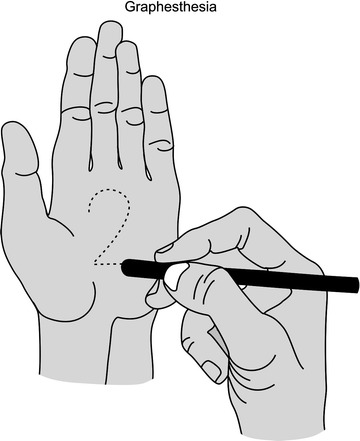
Bedside procedure to assess graphesthesia
Laboratory evaluations. Frequently listed after the physical examination in both the admission note and daily progress notes, laboratory evaluations include many abbreviations and common ways of recording the results. Tables 2.4–2.6 provide the abbreviations, descriptors, and purpose or function of common laboratory tests. Figures 2.6 and 2.7 illustrate how common laboratory values are diagramed in a chart.
Table 2.5.
Chemistry (routine) laboratory descriptors and abbreviations
| Laboratory abbreviation | Laboratory term | Purpose or function of test |
|---|---|---|
| Alb | Albumin | Major protein found in blood. Diminished with severe illness, kidney or liver dysfunction. Often measured with TP and Glob |
| Adult reference range: | ||
| 3.5–5.0 gm/dL | ||
| ALK or ALK Phos | Alkaline Phosphatase | Liver function. Elevated in conditions with increased bilirubin and in some bone diseases (e.g., Paget’s disease) |
| ALT | Alanine Aminotransferase | Liver function. Also found in cardiac and skeletal muscle. Elevated with liver damage |
| Adult reference range: | ||
| 1–21 units/L | ||
| AST | Aspartate Aminotransferase | Same purpose as ALT |
| Adult reference range: | ||
| 7–27 units/L | ||
| Bili | Bilirubin (total, direct, or indirect may be specified) | Bilirubin forms bile and is increased with cholestasis (blockage of bile excretion) |
| Adult reference range: | ||
| Total: 0.3–1.0 mg/dL | ||
| BUN | Blood urea nitrogen | Measures kidney function. Increased with kidney failure. Associated with Cr |
| Reference ranges: | ||
| −Adults = 6–20 mg/dL | ||
| −Higher in elderly (i.e., 8–23), lower in kids (5–18) | ||
| Ca (Ca+2) | Calcium | Involved in neural transmission and muscle function |
| Adult reference range: | ||
| 8.5–10.5 mg/mL | ||
| Cl (or Cl−) | Chloride | Major anion in body fluids. Often abnormal when sodium or potassium abnormal |
| Adult reference range: | ||
| 98–106 mEq/L | ||
| Cr | Creatinine | Measure of renal (kidney) excretion. Produced as part of energy metabolism in muscle |
| Adult reference ranges: | ||
| 0.6–1.2 mg/dL | ||
| GGT | Gamma Glutamyl transpeptidase | Abnormal with cholestasis; elevated in alcoholism |
| Glob | Globulins | Measure of antibodies. Associated with TP and Alb |
| Adult reference range: | ||
| 2.3–3.5 gm/dL | ||
| HCO3 (or HCO3) | Bicarbonate | Measure of acid – base balance |
| Adult reference range: | ||
| 18–23 mEq/L (CO2 content) | ||
| K (or K+) | Potassium | Involved in muscle contraction and function. Extreme low or high levels may be life threatening |
| Adult reference range: | ||
| 3.5–5.0 mEq/L | ||
| Na (Na+) | Sodium | Involved in muscle and nerve function. Low levels may be associated with seizures |
| PO4 or Phos | Phosphorus | Associated with bone metabolism and excreted renally. Related to calcium levels |
| Adult reference range: | ||
| 3.0–4.5 mg/dL (inorganic) | ||
| T4 | Thyroxine | Thyroid hormone level. |
| Adult reference range: | ||
| 4.6–12.0 μg/dL | ||
| TP | Total protein | Sum of albumin and globulin concentration. |
| Adult reference range: | ||
| 6.0–8.4 gm/dL | ||
| TSH | Thyroid stimulating hormone | Pituitary hormone whose levels are inversely related to thyroid function. |
| Adult reference range: | ||
| 0.5–5.0 microlU/mL |
Table 2.4.
Blood count and coagulation descriptors and abbreviations
| Laboratory abbreviation | Laboratory term | Purpose of function of test (what abnormal value may mean) |
|---|---|---|
| Complete blood count | ||
| Hb | Hemoglobin | To assess for anemia. Transports O2 to cells and CO2 away |
| Adult Reference Ranges: | ||
| −Females = 12–16 g/dL | ||
| −Males = 13–18 g/dL | ||
| Hct | Hematocrit | To assess for anemia; Hematocrit is the percentage of blood volume occupied by cells |
| Adult Reference Ranges: | ||
| −Females = 35–48% | ||
| −Males = 39–54% | ||
| Plt | Platelet count (in thousands) | Primary hemostasis. Initial blood clotting ability |
| RBC | Red blood cells | Density of Red Blood cells. Scales with Hb and Hct |
| Adult Normal Range: | ||
| Males = 4.2–5.4 × 106/μL | ||
| Females = 3.6–5.0 × 106/μL | ||
| WBC | White blood cell count | Assessment for infection; > 11,000/μL very elevated, can reflect infection, bone marrow disease (leukemia), trauma, etc.; <4,300/μL very low, can reflect bone marrow disease (leukemia), infection, chemotherapy, etc. |
| Coagulation/sedimentation | ||
| INR | International normalized ratio | Measure of anticoagulation (normal = 1.0) based on PT |
| PT | Prothrombin time | Measures function of vitamin K dependent clotting factors |
| PTT | Partial thromboplastin time | Measure of clotting function; measured with PT |
| Adult reference range: 25–41 s | ||
| ESR | Erythrocyte sedimentation rate | Measure of rate RBC’s settle out of whole blood in 1 h |
| Adult reference ranges: | ||
| −Females = 1–20 mm/h | ||
| −Males = 1–13 mm/h | ||
Table 2.6.
Cerebral spinal fluid and other body fluid laboratory descriptors and abbreviations
| Laboratory abbreviation | Laboratory term | Purpose or function of test |
|---|---|---|
| Cell ct | Cell count | Increased in meningitis or cerebral hemorrhage |
| Diff | Differential | Assesses for type of white blood cells found in body fluid (blood, CSF, etc.) |
| Prot | Protein | In CSF, elevations are nonspecific; elevated with neuropathy, stroke, MS and other conditions |
| Glu | Glucose | Low levels seen with bacterial meningitis. Usually 60% of serum value |
| Adult Reference Range: | ||
| 70–110 mg/dL (fasting) | ||
| U/A | Urinanalysis | Screen for urinary tract infection, and measure of kidney function |
| C + S | Culture and sensitivity | Identification of pathogens (usually bacterial) |
| Cx | Culture | As above |
| 14-3-3 protein | used for evaluating for prion disorders | |
| Oligoclonal bands | Antibodies that appear as discrete “bands” on staining | Evaluates for inflammatory conditions (such as Multiple Sclerosis, but are non-specific) |
Fig. 2.6.
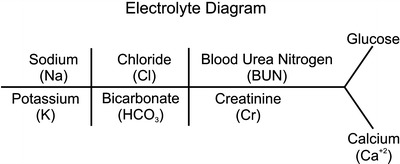
Basic chemistry notation diagram(The serum glucose is often appended at the right hand side of this figure as illustrated)
Fig. 2.7.
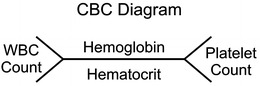
Basic Blood Chemistry diagram
Outpatient Medical Chart
The outpatient medical chart is often very similar to the inpatient chart, although follow-up visit notes may note less detail than above for some medical subspecialties. However, like the inpatient medical chart, the beginning consultation (office visit) report generally will include a detailed written report of the patients presenting history and medical evaluation similar in format (often identical to) that reviewed above for the inpatient medical record. However, return office visits may not re-review all the patient’s history again and note changes in the patient’s history as necessary for the patient’s ongoing care with the treatment provider. Thus, we will not re-review the sections noted above.
Contributor Information
Mike R. Schoenberg, Phone: 216844-5820, Email: mschoenb@health.usf.edu
James G. Scott, Phone: 405271-5253, FAX: 405271-5367, Email: jim-scott@ouhsc.edu
Alan J. Lerner, Email: Alan.Lerner@UHhospitals.org
References
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research. 1975;12:189–98. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- Lezak MD, Howieson DB, Loring DW. Neuropsychological assessment. 4. New York: Oxford; 2004. [Google Scholar]
- Victor M, Ropper AH. Adams and Victor’s principals of neurology. 7. New York: McGraw-Hill; 2001. [Google Scholar]
- Zaidat OO, Lerner AJ. The little black book of neurology. 5. Philadelphia: Elsevier Health Sciences; 2008. [Google Scholar]