

Abstract
Infection of the upper airways is very common and is the most common acute illness evaluated in the outpatient setting. The infection is usually caused by viruses including rhinoviruses, influenza viruses, parainfluenza and respiratory syncytial viruses. Influenza is the only viral infection preventable by vaccination and occurs predominately during annual winter epidemics. Bacterial infection such as acute rhinopharyngitis is uncommon and usually presents with either persistent symptoms of an URTI lasting over a week or worsening course after initial improvement or acute onset with high fever and inflammatory changes confined to the pharynx.
Fever is common in both bacterial and viral gastroenteritis. High fever is commonly present in many bacterial causes (e.g. Shigella, Salmonella, Shiga toxin-producing E. coli). Fever is often absent or low-grade in other diseases (e.g. enteropathogenic E. coli, cholera). Other febrile conditions cause diarrhoea and need to be differentiated.
Fever in CNS infection is the most common presenting symptom in children beyond the neonatal age owing to the presence of inflammatory mediators, particularly IL-1 and TNF in the blood or within the CNS. In MCD, fever was the first symptom in children younger than 5 years and 94% developed fever at some point.
Viral exanthems are common causes of febrile illness in children. More than 50 viral agents are known to cause a rash. Historically, exanthems were numbered in the order in which they were differentiated from other exanthems. Thus the first was measles; second, scarlet fever; third, rubella; forth, so-called Filatov-Dukes disease (no longer recognized as an entity); fifth, erythema infectiosum; and sixth, exanthema subitum. As more exanthems were described, numerical assignment became impractical.
Keywords: Fever in infections of respiratory tract, Pneumonia, Gastroenteritis, Hepatitis, Meningitis, Encephalitis, Viral exanthems
Core Messages
Infection of the respiratory tract is the most common reason for seeking medical advice and hospital admission in children. A viral upper respiratory tract infection (URTI) is the most common infection of the respiratory tract.
In developing countries, acute respiratory infection remains a leading cause of childhood mortality, causing an estimated 1.5–2 million deaths annually in children younger than 5 years of age.
In developed countries viruses are responsible for most upper and lower respiratory tract infections, including pharyngitis and pneumonia.
Although the degree of fever cannot differentiate between viral and bacterial diseases, high fever is associated with a greater incidence of serious bacterial diseases such as pneumonia or meningitis.
Worldwide, diarrhoeal disease is the leading cause of childhood deaths under 5 years of age.
If the fever does not have an evident source, urinary tract infection should be considered, particularly if the fever is greater than 39.0 °C and longer than 24–48 h.
Widespread vaccinations against bacteria causing meningitis, such as Hib, and vaccines against meningococci and pneumococci have dramatically reduced the incidence of meningitis.
A child with fever and non-blanching rash should be promptly evaluated to exclude meningococcal diseases.
Young children with malaria may present with irregular fever and not with typical paroxysms of fever, occurring particularly in early falciparum infection or as a consequence of previous chemoprophylaxis, which modifies the typical pattern of fever.
Acute Upper Airway Infections
An upper airway infection is the most common infection in children, accounting for half to two-thirds of all childhood infections. This term includes viral upper respiratory tract infection, tonsillopharyngitis, otitis media and epiglottic diseases.
Viral Upper Respiratory Tract Infection (URTI)
An URTI (known as the common cold) is an exceedingly frequent infection characterized by nasal obstruction and discharge, cough, sore throat, with or without fever, decreased appetite and restless sleep. The initial watery nasal discharge is followed rapidly by mucopurulent nasal discharge, which does not necessarily indicate bacterial infection. It has been estimated that young children may have as many as 12 respiratory infections per year if he or she attends nursery, 9 infections per year if a sibling attends school, and 6 or 7 per year if the child and a sibling are not at school.
Well over 100 viruses are known to cause respiratory tract infection, such as rhinoviruses (most common virus), influenza A and B, coronaviruses, parainfluenza 1, 2 and 3, adenoviruses and respiratory syncytial viruses (RSV). Infection may result from inhalation, self-inoculation to the nasal mucosa or airborne inoculation to the conjunctival mucosa. Children tend to have greater concentrations of viruses in the nasal secretion and shed them for longer periods of time than adults. Viraemia is less common and the infection is usually restricted to the mucosa, including the sinuses and Eustachian tube. Viral URTI may be complicated by secondary bacterial infections including acute otitis media and sinusitis. Acute idiopathic pericarditis (presents as chest pain and pericardial rubs on auscultation) is a rare complication that is usually preceded by a recent URTI. Infection with influenza viruses occurs during annual winter epidemics and is usually a self-limited illness. However, it can cause severe illness and deaths, particularly in children with high-risk medical conditions and neurological, genetic and chromosomal disorders.
Inflammatory cytokines such as interferons (INF) IL-1, IL-6 and IL-4 and TNF are involved in the inflammatory changes of URTI. Symptoms occur as a result of the effects of these cytokines rather than the virus itself. Injection of IFN-alpha to volunteers causes fever, malaise, headache and myalgia.
Fever in URTI:
Fever in URTI is present in about 50% of older children and in 90% of infants and young children.
Although high degrees of fever occur in viral and bacterial infections, high fever may predict serious bacterial infection.
High fever (>39.5 °C) is often associated with influenza A virus infections, occurring in more than 50% of children. Adenovirus infection causes fever exceeding 40 °C in about 20%, while fever in rhinovirus infection is usually absent or mild.
Fever associated with respiratory virus infection may last for 3–5 days. A prolonged duration of fever is however common. Fever lasting 5 days or longer occurs in over 30% of children with this infection. The longest duration of fever (>7 days) may occur in association with adenovirus. The shortest duration of fever is associated with parainfluenza 2 viruses.
Fever enhances body’s immunity against infection, and antipyretics may negatively affect the outcome of the illness. Therefore antipyretics should only be given for symptomatic children, such as discomfort, and not for fever per se.
Recurrent URTIs are mostly caused by viruses obtained from nursery attendance.
The knowledge that viruses can cause high and/or prolonged fever allows the physician to withhold antibiotic treatment and extensive investigations in children with prolonged fever who appear generally well, and common serious infections (e.g. UTI) have been excluded.
In the differential diagnosis, conditions mimicking URTI include:
Allergic rhinitis. There is often a family history of atopy, a history of nasal symptoms with exposure to potential allergens and the symptoms tend to be persistent. Nasal eosinophilia, increased serum IgE level and the finding of possible allergens in skin prick tests or blood may confirm the diagnosis.
Streptococcal throat infection. Children are usually >5 years. Fever tends to be higher than that in URTI. Nasal symptoms are usually absent.
Sinusitis should be considered in a child with purulent nasal discharge and fever (usual range 38–39 °C), localized pain and tenderness, mucosal erythema and headache, whereas a higher fever with chills may suggest an extension of the infection beyond the sinuses.
Management of a febrile child with an URTI:
No specific therapy is indicated for the majority of children, and the aim of treatment is to make the child comfortable.
The most commonly prescribed analgesic-antipyretic is paracetamol (81%) followed by combination of ibuprofen and paracetamol [1], and URTIs are the most common reason for the administration of antipyretics.
Symptomatic relief is obtained with antipyretics for pain, excessive myalgia and malaise. Paracetamol in a dose of 10–15 mg/kg, 4–6 h intervals may be given for children with fever ≥39.0 °C. Excessive paracetamol use can worsen asthma. The use of Ibuprofen is not recommended in children with dehydration. The practice of alternating antipyretics (paracetamol and ibuprofen) should be discouraged for there is no scientific evidence to support this practice.
Antibiotics are not indicated in uncomplicated cases and should be avoided, as should antihistamines and cough suppressants. The effect of antibiotics on fever in children who recovered with or without antibiotics is shown in Fig. 5.1.
Nasal decongestants are rarely required, except perhaps for those infants with feeding or sleeping difficulty caused by the nasal obstruction.
Vitamin C has been advocated for common cold, but its value is unproven. There is evidence that vitamin D can prevent acute viral URTI.
Herbal preparations are often used. Ivy leaf extract (Hedera helix) is popular as an antitussive in many European countries. It contains saponins that have mucolytic, spasmolytic, bronchodilatory and antibacterial effects.
Children, particularly those with high-risk medical conditions, may receive annual influenza vaccination to prevent the infection.
Oseltamivir and zanamivir reduce replication of influenza A and B viruses and can reduce the duration of influenza by a median of 36 h. They are also effective for prevention of influenza complications such as pneumonia or myocarditis. Oseltamivir is not licensed for use in children aged less than 1 year. For further information on the treatment of influenza (NICE guidelines).
The use of physical methods in reducing fever is discouraged.
Fig. 5.1.

Time to resolution of fever (days from consultation) according to virus detected and antibiotic prescribing. hmpv human metopneumovirus, RSV respiratory syncytial virus (obtained from Arch. Dis. Child. 2007; 92; 594–597; originally published online 16 Mar 2007; doi:10.1136/adc.2007. 116665)
Tonsillopharyngitis
The tonsils serve immune defence containing T-lymphocytes and macrophages. The main phase of immune acquisition continues until the age of 6 years, and therefore enlarged tonsils (hyperplasia) are physiological at this age to be followed by regression in size until the age of 12 years. Although most cases of tonsillopharyngitis are caused by viral agents, group A beta-haemolytic streptococci (GABHS) are the most common bacterial cause, occurring in 20–30% of cases. Less common causes are pneumococci and other groups of beta-haemolytic streptococci.
Streptococcal tonsillopharyngitis is primarily a disease of children 5–15 years of age. It may begin abruptly with fever (in over 90%), malaise, sore throat, swallowing difficulty, headaches and abdominal pain. The tonsils are oedematous and hyperaemic. There may be purulent exudates confined to the enlarged tonsils. The pillars are not enlarged as it is the cases in peritonsillar abscess. The uvula is red and swollen and the upper, anterior cervical lymph nodes are enlarged (>2 cm) and tender. There is usually an absence of conjunctivitis, coryza or cough. Diagnosis is made by throat culture and a more than twofold rise in antistreptolysin O titres between two serum samples taken 2 weeks apart. Rapid antigen detection and PCR tests are useful for providing rapid results.
Mechanisms of fever induction: Pyrogenic exotoxins, such as streptococcal pyrogenic exotoxin A, induce human mononuclear cells to produce numerous cytokines, in particular TNF-α, IL-1β and IL-6, which play a leading role in the pathogenesis of the inflammatory process and fever. High fever correlates with high levels of these two cytokines.
The differential diagnoses of streptococcal tonsillitis are:
Scarlet fever results from certain strains of haemolytic streptococci producing an erythrogenic toxin. The rash is an erythematous punctiform eruption that blanches on pressure and spares the area around the mouth. Initially the tongue has a thick white cover, which develops in a few days into typical strawberry tongue. Apart from the rash and the tongue, there is essentially no difference between streptococcal tonsillitis and scarlet fever. Fever in both conditions usually ranges from 39 to 40.5 °C peaking on the second day of illness. Without treatment, the temperature usually subsides on the fifth day, whereas penicillin therapy causes a rapid normalization of temperature within 12–24 h.
Peritonsillar abscess is a rare suppurative complication of tonsillitis causing a toxic appearance of the child, fluctuant peritonsillar mass and asymmetric deviation of the uvula.
Gingivostomatitis is usually caused by herpes simplex infection in infants and small children. It is characterized by irritability, anorexia and fever, which is usually in the range 38.5–39.5 °C (may also be as high as 40–40.5 °C). The child has painful oral vesicles that soon rupture. Submaxillary lymphadenitis may occur. The disease is self-limited and lasts about a week.
Coxsackievirus A may cause herpangina. The initial temperature ranges from normal up to 41 °C; the temperature tends to be higher in younger children. Other features include headache and vomiting. Throat inspection reveals discrete punctuate vesicles, surrounded by erythematous rings on the soft palate, anterior pillars and uvula.
Diphtheria, which develops insidiously, has a grey, thick membrane which bleeds easily if removed. The associated fever in diphtheria is typically low grade. Frequently, there is a pharyngeal erythematic and congestion (with or without tonsillar exudates). Anterior cervical adenitis is commonly present.
Treatment includes antipyretics (see above). Penicillin eradicates streptococci from the throat, bringing the symptoms, including fever, rapidly under control and effectively preventing suppurative and non-suppurative complications. Macrolides are used in case of penicillin allergy. Vitamin D is recommended to prevent recurrent tonsillopharyngitis.
Otitis Media (OM)
OM is one of the commonest infections in children, particularly during the first 2 years of life, affecting about 60% of all children. At risk are those who attend day-care centres and those whose parents smoke at home. The infection usually arises from an URTI, which spreads to the middle ear through the short and straight Eustachian tube. Streptococcus pneumoniae accounts for the majority of bacteria, followed by non-typeable Haemophilus influenza and Moraxella catarrhalis. Viruses (RSV, adenovirus, rhinovirus) are currently the most common cause of OM.
Bacterial OM often presents with a sudden febrile illness characterized by:
History of or the presence of viral URTI and sudden rise of fever.
High fever, irritability, ear pain and a prompt response to antibiotics. Fever of <39 °C occurs in about 25% and fever of >39 °C in about 75%. The highest fever is recorded in children less than 2 years of age. Only 4% of children persist with fever lasting longer than 48 h. Persistent fever suggests a viral cause, resistant bacteria, unsuitable antibiotic or a complication of OM.
Findings include intense erythema and various degrees of bulging of the tympanic membranes, with or without otorrhoea.
High cytokine levels, which correlate with the degrees of fever. In OM and middle ear effusion, high levels of cytokines exist, including IL-1β, Il-2, IL-4, IL-10 and TNF-α. High levels of IL-10 occur in infection by S. pneumoniae.
The absence of fever suggests a more insidious variety of OM characterized by mild lassitude and irritability. Conductive hearing loss is often present with this variety.
Complications include perforation of the drum, mastoiditis, chronic otitis, cholesteatoma, facial paresis, increased intracranial pressure (causing bulging of the fontanelle in infants), meningitis, brain abscess or lateral sinus thrombosis.
The introduction of pneumococcal vaccines has reduced the number of bacterial middle ear infections. The use of antibiotics is controversial except in cases with evidence of bacterial involvement. If antibiotics are prescribed, amoxicillin and a macrolide are sensible choices. The use of antihistamine, ear drops or decongestant is controversial. Analgesics are often needed to reduce the pain. For a bulging tympanic membrane or if the response to antibiotics is not prompt, myringotomy may rarely be considered for aspiration of fluid.
Infectious Mononucleosis (IM)
IM is an acute viral infection caused by Epstein-Barr virus. Symptoms, laboratory findings and complications are shown on Table 5.1. The virus targets memory B-lymphocytes and T-lymphocytes; the latter release a multitude of cytokines (e.g. IL-1β, IL-6, TNF-γ and IFN-γ) that cause the IM symptoms.
Table 5.1.
Features and complications of clinical data of infectious mononucleosisa
| Physical signs | % | Laboratory findings | % | Complication | % |
|---|---|---|---|---|---|
| Fever | 100 | EB-IgM | 100 | Pneumonia | 3 |
| Lymphadenopathy | 80 | Monospot test | 98 | Haemolytic anaemia | 3 |
| Pharyngitis | 80 | High transaminases | 90 | Agranulocytosis | 0.1 |
| Splenomegaly | 50 | >50% lymphocytes | 50 | Thrombocytopenia | 0.1 |
| Rash | Neurological | 1.5 | |||
| Palatal petechiae | 50 | Guillain-Barre syndrome | |||
| Exanthem | 10 | Meningoencephalitis | |||
| Transverse myelitis | |||||
| Hepatomegaly | 20 | ||||
| Jaundice | 5 | Other rare complications: | |||
| Ruptured spleen | |||||
| Airway obstruction | 1–3.5 | Myocarditis | |||
| Pericarditis | |||||
| Arthritis | |||||
| Nephritis | |||||
| Pancreatitis | |||||
A prodromal period of 3–5 days with malaise, fatigue and headache may precede the onset of fever. The majority (80%) of patients will have fever, pharyngitis and posterior cervical lymphadenopathy (pharyngeal form) and 20% present with fever alone (typhoidal form). Fever may last 4 days to 2 or 3 weeks (mean duration 2 week), peaking on the fifth day of illness. The pattern of fever is frequently intermittent, with a usual range between 38.5 and 39.5 °C, rarely higher.
IM commonly presents as:
Asymptomatic infection occurring in about 90% during early childhood.
Typical IM triad of abrupt onset of fever ranging from low-grade to high-grade fever, pharyngitis and cervical lymphadenopathy (especially posterior) occurring mainly in adolescents and young adults.
A case of pyrexia of unknown origin with fever as the only sign of the disease.
A complication listed in Table 5.1, including, rarely, malignancies, e.g. Burkitt’s lymphoma, Hodgkin’s lymphoma and nasopharyngeal carcinoma.
A cytomegalovirus mononucleosis characterized by prolonged fever, liver and haematological changes similar to those observed in Epstein-Barr infection. Heterophile antibodies are always absent. Pharyngitis is uncommon.
Tonsillopharyngitis not responding to antibiotic administration or as an extensive rash following the use of ampicillin or amoxicillin.
Leukocytosis in the range of 15,000–20,000 is frequent. Absolute lymphocytosis (greater than 50%) and at least 10% of atypical lymphocytes are usual findings. Tests to demonstrate heterophile antibodies (positive in more than 80%) have been superseded by several rapid slide tests (monospot). IgM is positive in almost 100%. PCR for detection of EBV is now in routine use to aid diagnosis.
Therapy: IM is usually self-limiting requiring only symptomatic treatment. Non-steroidal anti-inflammatory drugs (NSAIDs) reduce inflammatory features even at low doses. Paracetamol is used to reduce the fever and pain but should be used judiciously because of the liver status in IM. Aspirin should not be used because of bleeding risks and an association of IM with Reye’s syndrome. Steroids do not influence the extent or the duration of fever, but they are mainly indicated for impending airway obstruction. Hyperplasia of the lymphoid tissue in Waldeyer’s tonsillar ring may occasionally cause severe airway obstruction and will respond to steroids administered for 2 weeks. Antiviral and antibiotic treatment is not indicated. Close follow-up is recommended. Patients, particularly those with splenomegaly, should avoid excessive activity and trauma to minimize the risk of splenic rupture. Spontaneous splenic rupture and neurological complications are rare but account for the majority of fatalities.
Acute Upper Airway Obstruction
Croup ( laryngotracheobronchitis) is a common cause of upper respiratory tract obstruction of the subglottic area. It is characterized by inspiratory stridor, fever, cough, hoarse voice and a variable degree of respiratory distress. Although symptoms often appear alarming, the infection is a benign self-limited illness, which usually persists for 2–6 days. Parainfluenza viruses account for about 75% of all isolates. Other pathogens include influenza A and B, adenovirus and mycoplasma pneumonia. The attack rate is highest in the second year of life (usually 3 months to 3 years), and male children are predominately affected. Onset is sudden (usually at night) with loud stridor and barking cough, preceded by 24–72 h of an URTI. The severity of croup is assessed by a scoring system (Table 5.2).
Table 5.2.
Scoring system of severity for children with croup
| Mild-moderate | Severe | |
|---|---|---|
| Barky cough | Occasional | Frequent |
| Stridor | Minimal | Severe |
| Retraction | None | Obvious |
| Air entry | Normal | Decreased |
| Distress/agitation | Absent | Present |
| Level of consciousness | Normal | Disorientated, drowsy |
Fever is among the most common chief complaints in children presenting with upper respiratory infections. Variable degrees of fever are present in about 40% the patients with croup, ranging between 38 and 39 °C (mean 38.7 °C). Children with bacterial infection presenting with stridor (e.g. bacterial tracheitis) are mostly febrile with higher degrees of fever. Children with spasmodic croup are normally afebrile.
Management of a child with croup includes:
Children with croup usually recover rapidly with minimal medical intervention. Children with mild croup and minimal or no respiratory distress can be managed at home. If hospitalization is required, the mother should whenever possible be with the child to minimize stress.
Parental education on signs of respiratory distress and when to seek medical help is important.
O2 in case of hypoxia (O2−saturation <94%) presenting as agitation or distress.
Dexamethasone 0.6 mg/kg orally reduces respiratory distress within an hour of oral administration; the effect lasts about 10 h.
Nebulized epinephrine (adrenalin) is effective in producing dramatic effects on airway obstruction and may be administered in severe croup before intubation.
Although humidification is commonly used, trials have not shown this to greatly influence the clinical course of croup.
Paracetamol 10–15 mg/kg is administered if the child is miserable with fever or sore throat.
Spasmodic croup is another entity of unknown aetiology. Onset is always at night. The characteristic presentation occurs in a child who previously has been well without associated upper respiratory infection and who awakens at night with sudden dyspnoea, croupy cough and inspiratory stridor. Fever is usually absent.
Bacterial tracheitis is an acute, potentially life-threatening bacterial infection caused mostly by Staphylococcus aureus of the tracheal mucosa, often producing thick purulent exudates. This infection usually begins as a viral-like illness or croup with stridor but progresses rapidly with high fever, toxicity and worsening respiratory distress. The diagnosis should be considered in any ill-looking child who does not respond to nebulised adrenaline.
Epiglottitis is an acute bacterial infection characterized by marked swelling of the glottis and arytenoids area. Septicaemia caused by H. influenzae type B is present in most cases. Epiglottitis is rarely seen nowadays following Hib vaccines. The infection has an abrupt onset with high fever, respiratory distress, dysphagia, drooling, irritability, restlessness, anxiety and a thick muffled voice. In a report of 100 consecutive admissions of children with epiglottitis, fever was noted in 88, with a range from 39 to 40.5 °C and a mean of 39.1 °C [1].
Differentiating epiglottitis from viral croup may be difficult. Epiglottitis is now very rare. Patients appear very unwell, with higher degrees of fever and respiratory distress, and there is usually leukocytosis and high CRP.
Acute Lower Airway Infection
Bronchiolitis
A clear distinction between bronchiolitis and bronchitis in the first 2 years of life is difficult and of no therapeutic significance. Both are preceded by URTI. About 20% of children develop bronchiolitis during their first year of life. The diagnosis of bronchiolitis is made in the presence of a history of an URTI followed by acute onset of respiratory distress with cough, breathlessness, wheezing, tachypnoea and clinical signs of chest inflation, occurring during a winter epidemic of bronchiolitis. RSV accounts for 60–80% of cases. Peak age is 4–6 months. Pre-existing chronic lung disease, congenital heart disease, immunodeficiency, prematurity and parental smoking are risk factors for severe presentation of bronchiolitis.
Fever in bronchiolitis: Information on the incidence of fever in bronchiolitis or on its relationship to clinical severity of bronchiolitis is limited. In a study of 90 children with bronchiolitis [2], fever (defined as a single recording of >38 °C or two successive recording >37.8 °C) was present in 28 infants (31%). Febrile children had a longer mean hospital stay and a more severe clinical course compared to those who were afebrile (Table 5.3). In infants with bronchiolitis, hypoxia is common and as many as 40–50% require oxygen supplementation. A rise of body temperature results in an increase in energy expenditure of about 10% for each 1 °C rise in temperature. These changes are accompanied by an increase in oxygen consumption of 10–12% for every 1 °C rise in temperature. The low incidence of fever in bronchiolitis may be due to low interferon production. Although interferon is known to be a potent endogenous pyrogen, this cytokine is significantly low during acute RSV bronchiolitis. RSV induces pro-inflammatory cytokines (IL-1β, IL-6, IL-8, IL-10 and TNF-ɑ) that cause fever and attract inflammatory leukocytes.
Table 5.3.
Summary of clinical data of 90 children hospitalized with bronchiolitis
| Group | Mean length of stay in days | Clinical severity | |
|---|---|---|---|
| Severe | Mild | ||
| Febrile (n = 28) | 4.2 (1–13) | 20 (71%) | 8 (28.6%) |
| Afebrile (n = 62) | 2.7 (1–10) | 18 (29%) | 44 (71) |
| P value | <0.005 | <0.005 | |
The mainstay of treatment is:
Adequate oxygenation and hydration. Hypoxia, as measured by pulse oximetry, requires oxygen administration.
Nasogastric tube feeding or intravenous fluid is often required in moderate or severe cases to maintain fluid balance, to replace fluid loss from insensible sweating or tachypnoea and to minimize aspiration.
Nebulized hypertonic saline (3%) may improve the clinical severity.
Inhalation of beta-2 agonist (salbutamol) or anticholinergic agent (Ipratropium) is effective if there are signs of bronchospasm (wheezing).
Antibiotics are of no value unless the disease is complicated by bacterial infection. Corticosteroids, antihistamine, cough suppressants and expectorants are also of unproven value. Ribavirin can be effective in reducing the shedding of virus and is used in immunocompromised patients. Palivizumab, an antibody directed against the virus, is recommended to prevent RSV in high-risk individuals such as immunocompromised children.
Asthma
Asthma is defined as reversible obstructive airway disease characterized by bronchospasm, mucosal oedema and mucosal plugging. The airway obstruction is unevenly distributed throughout the lungs, leading to ventilation-perfusion imbalance and hypoxia. There is increased airway responsiveness to various stimuli, including respiratory viruses (responsible for up to 90% in young children), house dusts, exercise, air pollutants, cigarette smoking and drugs. Cytokines enhance eosinophil differentiation and maturation as well as endothelial adherence and activation.
The clinical hallmarks of the disease are paroxysms of expiratory wheezing with prolonged expiratory phase, unproductive cough and dyspnoea. The predominant asthma type in school-age children (6–16 years) is the classic atopic variant that is associated with allergy problems as evidenced by strong correlation with serum IgE levels and with skin test reactivity to allergens. By contrast, asthma in children aged 1–5 years is characterized by recurrent, transient wheeze triggered by viral colds, a type previously termed as wheezy bronchitis and now as preschool viral wheeze. Physical examination reveals varying degrees of tachycardia, tachypnoea, use of accessory muscles of respiration and rhonchi on auscultation. Somnolence, fatigue, diminished wheezing and breath sounds usually signal respiratory failure.
Markers of asthma severity include an admission to hospital in the previous 12 months, less privileged social class, parental smoking and the frequency of prior and recent respiratory infections. Environmental factors such as climate and air pollution have been found to influence the prevalence and severity of asthma. Higher exposure rates to cockroaches and dust mites also correlated with asthma severity. There are three stages of asthma severity:
During early stage, hypoxia causes increased minute ventilation, a fall in PCO2 and normal or elevated pH (respiratory alkalosis).
Moderate asthma is associated with increased hypoxia, normal PCO2 and pH.
In severe asthma, hypercarbia, low pH and respiratory/metabolic acidosis (respiratory failure) ensue as a result of respiratory muscle fatigue, hypoxia and anaerobic cellular metabolism producing lactic acidosis.
Relationship between asthma and fever: There is a lack of information about fever and its relation to asthma. A Medline/PubMed search identified 65,993 articles on the subject of asthma published since 1966 [3]. There were only three reports related to the occurrence of fever in asthma, but none on the incidence of fever in children with asthma or its relationship to the severity of the disease.
Fever is not a frequent finding in acute exacerbations of asthma. It was recorded in only 18.8% on admission of 202 patients, mostly younger than 5 years of age (Table 5.4) [3]. In this study, the severity of asthma was found to be inversely related to the degree of fever: children with severe asthma were usually afebrile and mildly asthmatic children were often febrile. Fever can therefore be seen as a marker of mild asthma. Similar observations were made at the turn of the last century when patients were noted to obtain a temporary relief of their asthma in association with fever. Subsequently various methods (diathermy) were used to treat asthma. It is possible that:
Fever as a response to infection can limit the spread of infection by enhancing the host defence mechanisms to eliminate the viruses.
As airway inflammation is a cardinal feature of asthma, cortisol, a potent glucocorticoid, is known to be elevated in febrile illness and could play a role as an endogenous anti-inflammatory agent.
Table 5.4.
Clinical data of 202 children with asthma
| Mean age in months (range) | Mean stay in days in hospital (range) | Asthma severity | ||
|---|---|---|---|---|
| Severe | Mild | |||
| <5 years | ||||
| Febrile = 27 | 24 (12–42) | 1.7 (1–4) | 1 | 26 |
| Afebrile = 70 | 31 (12–58) | 1.9 (1–9) | 5 | 65 |
| p-value | 0.012 | 0.484 | 0.603 | |
| 95% CI | 1.6–12.7 | −0.3–0.7 | n/a | |
| >5 years | ||||
| Febrile = 11 | 113 (78–172) | 1.4 (1–2) | 1 | 10 |
| Afebrile = 94 | 118 (60–180) | 2.2 (1–6) | 18 | 76 |
| p-value | 0.700 | 0.065 | 0.688 | |
| 95% CI | 19.1, 28.3 | 0.65, 15 | n/a | |
The reasons why the majority of asthmatic children are afebrile may be due to:
Tachypnoea, which accompanies asthma, increases heat loss through evaporation.
Reduced interferon production has been reported in children with bronchiolitis and asthma. Interferon is known to be a potent endogenous pyrogen capable of inducing fever. Cytokines implicated in the pathogenesis of asthma, such as IL-5, IL-8, IL-4 and ECP, are not known to be potent pyrogens, and their presence is unlikely to induce fever in asthma [4].
Laboratory investigations such as full blood count, CRP and ESR are of little value in asthma. Leukocytosis is common in the absence of bacterial infection. A chest X-ray is rarely indicated unless the diagnosis is uncertain, in patients with fever >39 °C and in case of severe asthma. Measurement of oxygen saturation is always indicated when a child is admitted to hospital. For older children measurement of the peak flow is important and should be repeatedly performed. Allergy skin tests (to detect IgE antibody in the skin to inhalants such as pollens and house dust mites) and the radioallergosorbent test (RAST, detecting IgE to various allergens in the serum) are often performed, but they do not seem to be of great diagnostic or therapeutic value.
Therapy aims at rapid reversal of the airway obstruction. Nebulised beta-2 agonists remain the first line of treatment. Corticosteroids are recommended for patients with acute severe asthma, but their effects are slow. Inhaled steroid (IS) therapy reduces symptoms and bronchial hyperresponsiveness and is currently widely used as an anti-inflammatory agent in asthma. For children taking steroid therapy who are still inadequately controlled, the use of long-acting inhaled beta-2 agonist or higher dose of IS is recommended. Children with mild asthma who are not taking adequate fluids by mouth and all children with severe asthma should have IV fluid therapy. Oxygen should be administered in all cases with hypoxia, that is, an oxygen saturation <92%.
Paracetamol and ibuprofen intake during pregnancy and during the first year of life has been reported to be associated with increased risk of asthma. Other reports found no evidence that paracetamol when used during febrile illness was associated with increased risk of asthma. Further studies are needed to ascertain this relationship between asthma and antipyretics.
Pneumonia
In 1900, pneumonia, called by Osler “the captain of the men of death”, is still the most common cause of deaths under the age of 5 years causing over a million deaths annually, mostly occurring in developing countries. In children, pneumonia is common, but its true incidence is not established owing to the lack of an accepted clinical definition of pneumonia. However, the bacterial incidence has significantly decreased after the introduction of Haemophilus influenzae type B and conjugate pneumonia vaccine PCV7. Peak incidence occurs between 6 months and 5 years. Factors that increase the risk of pneumonia include malnutrition, parental smoking, immunosuppression, low socio-economic status and prematurity. In recent years, HIV infection has contributed to increases in incidence and mortality.
The lungs are not only involved in gas exchange but also in mediating host defence. This includes non-immunological defence mechanisms (such as lysozyme secretion by macrophages) and immunological defence mechanisms (such as activation of macrophages and B- and T-lymphocytes). The alveolar macrophages respond to activation by exogenous pyrogens (such as endotoxin released by Gram-negative bacteria) by releasing potent inflammatory mediators, including interleukin-1 (IL-1), tumour necrosis factor (TNF) and IL-8. This leads to a febrile response, accumulation of neutrophils at the site of infection and inhibition and repair of tissue injury. IL-8 is particularly important for neutrophil chemotaxis.
Diagnosis of pneumonia is based on the following features:
Community-acquired pneumonia is defined: fever, clinical signs (cough, dyspnoea, tachypnoea, grunting and nasal flaring and referred pain) and chest X-ray infiltrates in a previously well child. Lower lobe pneumonia may cause lower abdominal pain mimicking acute appendicitis. Upper lobe pneumonia may cause meningism (increased CSF pressure, but CSF is otherwise normal).
Findings include inspiratory crepitations and bronchial breathing on auscultation. Tachypnoea (>40/min aged >1 year, >50/min aged 2–12 m and > 60/min aged <2 m) is the WHO-defined criterion to diagnose pneumonia.
Wheezing, cough and fever may occur with mycoplasma infection.
Chest X-ray is diagnostic, but it is often of limited value in distinguishing bacterial and viral. The presence of effusion and/or lobar consolidation suggests bacterial aetiology.
Isolation of the pathogens causing pneumonia is usually not possible in practice. Bacterial culture from the pharyngeal area or expectorated sputum is unreliable. However pathogens can be identified by:
Blood culture (positive in 10% of cases with bacterial pneumonia).
Serum or urine counter-immuno-electrophoresis is a rapid and more sensitive technique than blood culture for the detection of bacterial antigens.
Culture of aspirated pleural effusion.
High IgM, such as Mycoplasma pneumoniae.
Respiratory secretion for rapid virus antigens (e.g. RSV, parainfluenza).
Serological tests showing fourfold rise of antibody titres.
Polymerase chain reaction (PCR) is increasingly being used.
Marked leukocytosis, sometimes exceeding 40,000/mm3 (leukemoid reaction), is very suggestive of bacterial pneumonia, particularly pneumococcal or H. influenzae pneumonia. Although inflammatory markers (WBC, CRP) are usually normal in viral pneumonia, mild leukocytosis with a left shift in the differential count may occur, particularly in influenza pneumonia.
Fever in pneumonia: Fever is common in children with pneumonia older than 1 month of age. Reports [5] on fever and pneumonia indicated that:
Of the 100 febrile children with pneumonia, a temperature of >40 °C occurred in 45, while the remaining 55 children had a fever of <40 °C.
Fever was present in all children with H. influenzae pneumonia, with a mean temperature on admission of 39.9 °C (H. influenzae pneumonia is rarely seen nowadays).
The onset of pneumococcal pneumonia was usually abrupt with a temperature of 39.5–40.5 °C. The highest fever however tended to be with staphylococcal infection (A temperature of 41 °C is not an unusual finding).
The likelihood of pneumonia increased with increasing duration of fever longer than 3 days, e.g. during a febrile URTI. A study of 711 children with pneumonia from 13 hospitals in England found neither CRP, chest X-ray changes nor pyrexia was associated with increased severity of the disease.
In children <3 years old, a combination of >38.5 °C, chest recession and a respiratory rate of >50/min indicates pneumonia. Dyspnoea is a more reliable sign of pneumonia in older children (The British Thoracic Society guidelines).
Pneumonia in Newborn Infants
During the neonatal period, pneumonia is usually caused by organisms acquired during or before delivery, mainly E. coli and group B streptococci. The amniotic fluid may be infected or the mother is an asymptomatic carrier of these organisms. Predisposing factors are prolonged rupture of membrane, prolonged labour or an infected, febrile mother. The infection by these bacteria is mainly due to low levels of opsonizing antibodies directed at the polysaccharides of the organism, impaired function of the lung macrophages and polymorphonuclear leukocytes. Pneumonia may also accompany a generalized intrauterine infection by cytomegalovirus toxoplasmosis, listeria or rubella virus. Chlamydia trachomatis is classically an afebrile pneumonia with a dry cough and increasing tachypnoea. Conjunctivitis is present in about 50% of cases.
The newborn infant with pneumonia usually presents with signs of respiratory distress with tachypnoea and grunting. Body temperature is usually normal. If the mother has been febrile before delivery, an increased temperature may be detected in the infant in the first few hours of life owing to the constant temperature gradient between mother and infant during pregnancy.
Pneumonia at the Age 1 Month to 4 Years
During this age, the rate of viral pneumonia is high, particularly in children around 6 months of age. Respiratory syncytial virus (RSV) remains the most common cause of pneumonia in industrialized countries. Febrile pneumonias are commonly caused by RSV, influenza A and B, parainfluenza type B and adenoviruses, while afebrile pneumonias are usually due to chlamydia trachomatis, cytomegalovirus or Mycoplasma hominis. Commonly an URTI precedes the onset of pneumonia.
In developing countries, the causes and patterns of pneumonias are affected by malnutrition, poor housing, lack of early medical attention and immunization. Pneumococci, streptococci, coliforms, H. influenzae and staphylococci are more common causes of pneumonia with high mortality.
Staphylococcal pneumonia is a rather rare cause of pneumonia, occurring sometimes as a complication of influenza virus infection. Its presentation is with shaking chills and high fever>40 °C, pallor, tachypnoea, abdominal distension and rarely cyanosis. The diagnosis should be suspected in any child younger than 1 year of age who appears ill and does not respond rapidly to conventional antibiotics such as penicillin and ampicillin. Chest X-ray shows multiple nodules, which undergo cystic formation (pneumatocele) and empyema.
Pneumonia at the Age of >4 Years
Pneumococci and Mycoplasma pneumoniae are the most frequently identified organisms, while viruses are less common at this age. In pneumococcal pneumonia, patients have often flu-like symptoms for several days before the onset of pneumonia, which begins by an abrupt onset of rigor and high fever. The cough is not a feature initially but becomes intense later and is usually accompanied by chest pain. The sputum is classically rusty in colour due to alveolar haemorrhage, but this is seldom seen nowadays in children.
Mycoplasma pneumoniae is characterized by insidious onset of fever, headaches and abdominal pain, followed by cough. Transient skin rash is found in about 10% of cases. Mycoplasma pneumonia may also present with similar clinical and radiological features of pneumococcal and staphylococcal infection. In contrast to these infections, however, children with M. pneumoniae appear well despite the extent of the X-ray lesions. Fever is present in more than 90% of patients. In a study of 66 children with mycoplasma infection [11], the temperature distribution was as follows: temperature <38 °C was present in 22% of patients, 38.3–38.9 °C in 30%, 39.4–40 °C in 44% and >40.6 °C in 4%.
The diagnosis of M. pneumoniae is difficult, but it may be made by a combination of:
History of unresponsiveness to penicillin or amoxicillin.
A fourfold rise in antibody titre or a single titre of 128 or more.
IgM antibodies.
Serum cold agglutinins in 50–70% of the cases.
Chest X-ray is not diagnostic but commonly shows peribronchial and perivascular interstitial infiltrates.
A high CRP or ESR and a normal WBC count may be observed.
About 5% may develop neurological complications, such as encephalitis, meningitis, cerebellar ataxia, focal neuropathy or cerebral infarction. Other complications are haemolytic anaemia, arthritis, rash (popular, vesicular, erythema multiform) myocarditis, pericarditis and interstitial nephritis.
Pneumonia at any Age
Aspiration pneumonia may occur subsequent to aspiration of secretion from the oropharynx in weak or neurologically impaired children (e.g. in preterm infants, cerebral palsy) and in children with tachypnoea (e.g. bronchiolitis) or following inhalation or accidental ingestion of kerosene or aspiration of gastric acid. The child presents with dyspnoea, tachypnoea, subcostal recession, cough, wheezing and cyanosis. Children are usually afebrile with aspiration pneumonia, with possible exception of kerosene pneumonia, which is often associated with fever of 38–39.5 °C. Chest X-ray shows infiltrates usually involving the right upper lobe in infants and right lower lobe in older children.
Pneumocystis jiroveci pneumonia = PJP (previously known as Pneumocystis carinii) occurs almost exclusively in patients who are immunocompromised, including those who are receiving immunosuppressive drugs for malignancy or organ transplantation or HIV infection. About 85% of patients with HIV develop PJP during the course of their illness. Unlike most infectious complications in cancer patients, PJP may occur while the patient is in remission from the primary cause. Clinical manifestations include fever, cough, cyanosis, marked tachypnoea with intercostal retraction and a paucity of physical signs of pneumonia. Among 1251 children with malignancies, PJP was identified in 51 (4.1%) [12]. Fever was the first sign of abnormality and occurred in almost all patients with, or shortly preceding, tachypnoea. The extent of the fever varies from mild to severe.
The diagnosis is suggested by a chest X-ray showing a hazy, bilateral alveolar infiltration. Sputum examination and bronchoalveolar lavage (BAL) can identify PJP in the majority of cases. The diagnosis is confirmed by detecting PJP by histological or cytological demonstration of thick-walled cysts, as obtained by BAL or from percutaneous transthoracic needle aspiration of the lung.
Antibiotic therapy of pneumonia depends on the age of the child and likelihood of the causative agent. Neonates are treated with penicillin and gentamicin. Older children respond to amoxicillin and second- or third-generation cephalosporins or co-amoxiclav. Suspected cases of staphylococcal pneumonia should receive anti-staphylococcal agent such as flucloxacillin. Patients with mycoplasma pneumonia usually respond well to macrolides. The treatment of choice for patients with PJP is trimethoprim-sulfamethoxazole 20 mg/kg/day.
Gastroenteritis
Worldwide, diarrhoeal disease is the leading cause of death under 5 years of age. More than two million children die every year from gastroenteritis, almost all living in resource-constrained countries. In the absence of diarrhoeal diseases, the total infant and child mortality in the Third World would not differ significantly from that of developed countries. Data collected from 276 surveys on diarrhoea in 60 countries have shown that one-third of all deaths in children below 5 years of age were caused by diarrhoea. Approximately 1.5 billion diarrhoeal episodes and 4.6 million deaths in children occur per year (or 12,600 deaths/day), accounting for 21–29.3% of all childhood deaths [6].
In developing countries, bacterial (Escherichia coli, Salmonella, Shigella, Campylobacter and Yersinia enterocolitica) and parasitic (Entamoeba histolytica, Giardia lamblia, Cryptosporidium species) pathogens are the major causes of gastroenteritis, particularly in summer months (Table 5.5). In developed countries, viruses are responsible for approximately 70% of the gastroenteritis. Viral GE causes shorter illness than bacterial GE and is associated with increased risk of vomiting and dehydration compared to bacterial GE. Rotavirus is the most common causative pathogen followed by norovirus and adenovirus. Enteric adenovirus is associated with longer-lasting diarrhoea.
Table 5.5.
Major enteropathogenic agents in children with gastroenteritis
| Bacteria | Virus | Parasites |
|---|---|---|
| Salmonella | Rotavirus | Giardia lamblia |
| Shigella | Adenovirus | Entamoeba histolytica |
| E. coli | Other viruses | |
| Campylobacter jejuni | ||
| Yersinia | ||
| Vibrio cholerae | ||
| Other bacteria |
Fever is common in both bacterial and viral gastroenteritis. High fever is commonly present in many bacterial causes (e.g. Shigella, Salmonella, Shiga toxin-producing E. coli). Fever is often absent or low-grade in other diseases (e.g. enteropathogenic E. coli, cholera). Other febrile conditions that cause diarrhoea and need to be differentiated from GE are shown in Table 5.6.
Table 5.6.
Febrile non-enteritis conditions that cause diarrhoea
| Conditions | Diagnostic clue |
|---|---|
| Intussusception | Intermittent, colicky abdominal pain |
| HUS | Bloody diarrhoea, abdominal pain, vomiting |
| Appendicitis | Young age of 1–3, predominately diffuse abdominal pain |
| Neuroblastoma | Abdominal mass |
| Primary immunodeficiency | Associated recurrent infections |
| HIV infection | Commonly associated with thrush, recurrent infections, weight loss |
| Kawasaki disease | Lymphadenopathy, conjunctivitis, rash |
| Addison’s disease | Diarrhoea occurs in chronic adrenal insufficiency, abnormal electrolytes, pigmentation, adynamy |
| Crohn’s disease | Associated weight loss, anaemia, high CRP |
HUS Haemolytic uremic syndrome
Bacteria or viruses acting as exogenous pyrogens can cause fever by inducing endogenous pyrogens which raises the hypothalamic thermoregulatory set-point. Clinical and laboratory findings, which can differentiate bacterial from viral aetiology of acute gastroenteritis, are shown in Table 5.7.
Table 5.7.
Factors likely to predict the aetiology of acute gastroenteritis
| Bacterial aetiology | Viral aetiology |
|---|---|
| Fever >39 °C | No fever or low-grade fever |
| Presence of bloody stools | No bloody stools |
| Summer months | Winter months |
| High CRP, WBC, IL-6 | Normal or mildly elevated CRP, WBC, IL-6 |
| Hyponatraemia is common | Hyponatraemia is uncommon |
| Increased WBC in stool | None to few WBC in stool |
| High-serum TNF-alpha | Low serum TNF-alpha |
Dehydration, the most common cause of hyperthermia, leads to cutaneous vasoconstriction and decreased sweating, causing an increase in body temperature. In hypernatraemic dehydration, an increase in sodium pump activity needed to offset the high extracellular sodium concentration may further raise the body temperature. High sodium levels may also act directly upon the hypothalamus to increase the set-point. For every 1 °C increase of body temperature, there is an increase in insensible water loss of 10%. Table 5.8 shows typical water losses based on caloric expenditure of 100 kcal/kg/day for an infant weighing 10 kg body weight.
Table 5.8.
Typical water losses per 100 kcal of energy expended for a healthy 10 kg child
| Source of water loss | Approximate water loss (mL/kg/day) |
|---|---|
| Insensible | |
| Skin | 30 |
| Respiratory | 15–20 |
| Sensible | |
| Stool | 10 |
| Urine | 50–60 |
| Total | 105–120a |
aThe above average calculation. The sum of insensible water loss (average 50 mL/kg/day) with 16 mL/kg/day subtracted for endogenous water for oxidation produces 34 mL/kg/day. The addition of 66 mL/kg/day urinary loss would produce 100 mL/kg/day fluid requirement
Bacterial Gastroenteritis
Bacterial gastroenteritis is caused either by secretory pathogens (such as cholera, which causes watery diarrhoea through colonization and adherence to the small bowel mucosa) or invasive pathogens (such as Shigella, which cause inflammatory cell exudates in the distal bowel and/or colon). Secretory pathogens are likely to cause severe diarrhoea. Invasive organisms may cause watery or grossly bloody diarrhoea with cramps and tenesmus, but severe diarrhoea is infrequent.
Salmonellae are Gram-negative rods with over 1400 known species. The most common serotypes are S. typhimurium, S. enteritidis and S. infantis. In industrialized countries non-typhoidal salmonellae (NTS) infection is more common. This is usually a self-limiting and benign disease, and invasion beyond the gastrointestinal tract occurs in only about 5% of patients. In many African countries, bacteraemia is a major cause of death, and NTS account for 20–50% of cases, ranking second only to pneumococcal pneumonia as the leading bacterial cause of child mortality. Most human infections occur in late summer and early autumn and are caused by the ingestion of contaminated food (meat, poultry products, eggs) or water. Increased susceptibility to the infection occurs in children with sickle cell anaemia, impaired cellular immunity and achlorhydria. About 12–48 h following ingestion of contaminated ingestion of contaminated food, the onset is abrupt with nausea, fever, and crampy abdominal pain, followed by loose, watery diarrhoea, occasionally containing mucus, blood or both. The illness is indistinguishable from Shigella infection. Vomiting is a not a striking feature in salmonellosis. While salmonellosis in older children is usually self-limited disease requiring no antibiotic therapy, there is a significant incidence of bacteraemia (range 15–45%) and meningitis in infants younger than 3 months. Bacteraemia may occur in the absence of fever in this age group. The absence of fever usually excludes bacteraemia in older children.
Fever in Gastroenteritis
Endotoxin is a complex lipopolysaccharide structure that constitutes the outside portion of the cell wall of Salmonella. Endotoxin releases IL-1 from macrophage into the circulation, accounting for the fever and other systemic manifestations of the disease. Cytokines are responsible for the symptoms and development of the protective mechanisms in the disease. Mean serum concentrations of TNF-alpha, TNF-gamma and IL-12 are increased during the acute phase of the disease. IL-8 and IL-10 are involved in the pathogenesis of rotavirus GE.
Diarrhoea is usually more frequent in afebrile than in febrile cases.
Children with bacterial GE are more likely to develop high fever than those with viral GE, and there is a significant relation higher fever and shigella GE.
In a study from Finland [7] comprising 102 children salmonella gastroenteritis, 15 had a fever >40 °C, 66 had a fever of 38–39.9 °C and 21 had a temperature of <37.9 °C. There was a significant correlation between the degree of fever and the duration of organism excretion: a fever of >40 °C had the shortest and no fever the longest duration of excretion (Table 5.9). Fever therefore appears to have a favourable prognostic influenza on the duration of salmonella excretion. The gastrointestinal tract acts as a major barrier against the potentially noxious substances, such as microbes. Immunological defences include secretory IgA, macrophage and activated T-lymphocytes in the Peyer patches and lamina propria. Fever is beneficial to the infected host by enhancing macrophage and T- and B-cell activity.
Convulsion may occur during the diarrhoeal disease. About 10% develop febrile or afebrile seizures. Febrile seizures (FS) are particularly common with shigella infection. Occasionally, afebrile seizure may occur in association with dehydration, electrolyte imbalance, hypoglycaemia or hypocalcaemia. A third form of seizure is an afebrile seizure, particularly during viral GE, without dehydration of electrolyte imbalance. This type of seizure is usually benign. CSF and EEG are normal. Paracetamol has not been shown to prevent FS.
Ibuprofen is an antipyretic that is frequently administered for febrile children with GE. Acute renal insufficiency may occur in association with ibuprofen and should therefore be avoided.
Table 5.9.
Fever on admission and duration of bacterial excretion after salmonella gastroenteritis in 102 children (Ref [7])
| Degree of fever (°C) | No of children | Duration of salmonella excretion (weeks) | ||
|---|---|---|---|---|
| Range | Mean | Mean (SD) | ||
| (A) > 40 0 | 15 | 0–10 | 0 | 1.9 (2.9) |
| (B) 38–38.9 | 66 | 0–18 | 3 | 4.1 (4.0) |
| (C) <37.9 | 21 | 2–60 | 7 | 11.7 (15.1) |
P value: (A) vs. (B), p = 0.160; (B) vs. (C), p = 0.0011; (A) vs. (C), p = 0.0001
Typhoid fever includes infection with S. typhi and S. paratyphi A, B and C, rarely S. choleraesuis, S. heidelberg and S. typhimurium. The incidence of typhoid fever in the USA is 0.2 cases per 100,000 population, with a case fatality rate of 1.3% [8].
Elevated pro-inflammatory pyrogenic cytokines, particularly tumour necrosis factor-α and IL-6, are responsible for the prolonged fever, which is characteristic of the disease. High serum levels of these cytokines have been linked to disease severity. High level of IL-6 suggests poorer response to antibiotic therapy and its decline correlates with successful therapy. Vigorous antipyretic use may lead to shock.
In older children, presentation of a typical case follows the following steps:
Onset is insidious with fever (without shaking chills), which is present in all patients, and is associated with headache, cough and abdominal pain. Symptoms then gradually increase over 2–3 days. The child is often constipated, nauseated and anorexic. The temperature continues to rise in a stepwise fashion to reach 40–41 °C. In young children the onset of fever is more often abrupt, then becoming sustained or intermittent. The stepwise pattern of fever is less common. In all ages, fever may continue for many days despite successful antibiotic therapy, and the child does not become afebrile until the end of the therapy. At the end of the first week, patients remain febrile with hot, dry skin, abdominal tenderness, hepatosplenomegaly and relative bradycardia. Roseate spots may be detected in about 20–40%, characterized by a few discrete popular erythematous lesions confined to the anterior chest and abdomen. Delirium, convulsion, meningeal irritation, psychosis and ataxia may be noted. If untreated with antibiotics, fever remains continuous at 39–40.5 °C for 2–3 weeks before abating slowly. By the end of 2 weeks, perforation or haemorrhage (in about 5%) may occur due to typhoid ulceration and defects in coagulation. This serious complication is associated with 50% mortality. Typhoid bacilli persist indefinitely in the bile passage in about 3–5% who recover from the infection.
Laboratory findings include leucopenia, anaemia, thrombocytopenia and increased serum aspartate transaminase (SGOT). Elevated agglutination titres of O and H antigens at 1:160 are significant. The diagnosis is based on isolation of S. typhi or other salmonella strains from blood or bone marrow culture.
Shigellae are Gram-negative rods with worldwide distribution. Humans are the principal host for shigellosis (bacillary dysentery). The majority of patients are under 5 years of age; the infection is rarely seen in infants under 6 months of age.
Four serotypes are known: Shigella flexneri, S. dysenteriae, S. sonnei and S. boydii. The first two species are more common in developing countries, whereas S. boydii and S. sonnei usually cause a self-limiting febrile illness in developed countries. Shigella must penetrate the mucosa in order to cause dysentery.
The disease onset is usually acute with fever and malaise, often progressing to dysentery consisting of cramps, tenesmus and frequent stools composed largely of blood and mucosa. Severe dehydration is not a typical feature of the infection. High fever is common. Of 57 children with Shigella gastroenteritis, 27 (47%) had a fever greater than 40 °C at presentation, 21 (37%) had a fever between 38 and 40 °C and the remaining 9 (16%) were afebrile [9].
Complications include toxic megacolon, protein-losing enteropathy, hyponatraemia due to inappropriate antidiuretic hormone secretion, disseminated intravascular coagulation, renal failure, haemolytic uraemic syndrome and bacteraemia. Shigella bacteraemia occurs in 4.0% of patients. Neurological symptoms, particularly convulsion are among the most frequent extra-intestinal manifestations of shigellosis occurring with or without evidence of the production of Shiga toxin (neurotoxin). Death can occur in children with poor nutritional state.
Amoebic dysentery, caused by Entamoeba histolytica, may cause colitis simulating shigellosis. Virulence of E. histolytica depends on the trophozoites being able to bind to colonic epithelium. The infection tends to run a more chronic course with intermittent watery or semiformed diarrhoea (containing blood and mucosa) without or with a low-grade fever. Young children tend to present with acute symptoms similar to cases with Shigella infection. Liver abscess may occur a few months after the intestinal infection, causing discomfort over the liver, intermittent fever with chills and sweats and weight loss. Findings suggestive of amoebic liver abscess include an elevated right diaphragm, hepatomegaly and a history of colitis. The diagnosis of amoebiasis is confirmed by demonstration of E. histolytica in a stool (motile trophozoites during the diarrhoea, cyst if the diarrhoea is not present) or in tissues. The indirect haemagglutination (HA) test and enzyme-linked immunosorbent assays (ELISA) are positive in almost all patients with amoebic liver abscess and in majority of those with intestinal infection.
Escherichia coli cause either non-bloody diarrhoea (e.g. enterotoxigenic E. coli, ETEC; enteropathogenic E. coli, EPEC) or bloody diarrhoea (e.g. Shiga toxin-producing E. coli, STEC; enteroinvasive E. coli, EIEC). E. coli cause significant fluid loss and dehydration, but bloody stools are relatively infrequent.
ETEC produce enterotoxins that cause copious, watery diarrhoea in developing countries. In severe form, the illness resembles cholera and is responsible for high mortality among young children. It is an uncommon cause of diarrhoea in industrial countries, but it is the most common cause of traveller’s diarrhoea. EPEC infection was in the past a common cause of outbreaks of infantile diarrhoea in industrialized countries, usually occurring in neonates and young children <2 years of age. Since the 1970s the infection has been reported less frequently, and the severity of the illness has lessened in children of these countries. It can cause protracted diarrhoea.
EIEC and STEC produce Shiga toxins, causing a dysentery-like diarrhoea and haemolytic uraemic syndrome (HUS) by the strain 0157:H7.
Fever occurs frequently in the range of 38–40 °C. Fever, very often low-grade, is reported in only one third of patients in children infected with EIEC and STEC. EPEC usually does not cause systemic manifestations because the organisms remain confined to the bowel lumen. Fever was found in only 5 of the infected 49 children from Addis Ababa [10].
Campylobacter enteritis is an important cause of enteritis in both developed and developing countries. C. jejuni is the most important species. The enteritis is a zoonosis and a man-to-man transmission is unusual. Raw cow’s milk and incompletely cooked poultry meat have caused most of outbreaks in the UK. Contaminated water is another cause of outbreaks in developing countries.
Infection is usually self-limited in industrialized countries, lasting 2–4 days, following an incubation time that averages 5 days. Children present with an acute illness accompanied by fever, diarrhoea and bloody stools in about 90% of cases. Abdominal pain occurs almost universally, but vomiting is mild and occurs in about 30%. In a study from Canada, all 32 children with this infection who were older than 12 weeks develop fever up to 40.5 °C, whereas all five children who were younger than 12 weeks remained afebrile. In a study from Iraq, 202 children with diarrhoea, C. Jejuni was found in 13.86% and fever was detected in 82.14% [11].
Yersinia enterocolitica is an anaerobic, Gram-negative bacillus that causes an infection mostly in cooler climates such as Scandinavia and Canada. Serotype O:3 is the most common isolate. Transmission of Y. enterocolitica to humans occurs from ingestion of contaminated foods (particularly contaminated pork), water and milk.
Presentation is characterized by bloody diarrhoea in about one third of patients. The fever is usually mild, ranging between 38 and 39 °C. The associated abdominal pain sometimes mimics appendicitis (pseudo-appendicitis). The disease is usually mild although it can be prolonged (1 day to 3 weeks). A Canadian study of 181 children with Yersinia infection (45) reported that diarrhoea occurred in 98%, fever in 88%, abdominal pain in 64.5% and vomiting in 38% [12].
Rare complications are arthritis and erythema nodosum. Other rare complications include intestinal perforation, diffuse ulceration, ileocolic intussusception, peritonitis, glomerulonephritis, meningitis and peri-myocarditis. The infection can occur as septicaemia and patients then have high fever, toxic appearance and confusion.
Viral Gastroenteritis
Rotavirus infection is responsible for 30–60% of all cases of dehydration and diarrhoea in young children (peak age 3–15 months) in both developed and developing countries. The infection is prevalent in winter months. Approximately 125 million cases of rotavirus diarrhoea occur annually in developing countries, leading to an estimated 800,000–900,000 deaths a year [13]. Although viraemia is rare in healthy individuals, this was reported in 67% of immunocompetent children with rotavirus diarrhoea.
Nosocomial acquired outbreaks of rotavirus have occurred in newborn nurseries and paediatric hospital wards. The virus can be detected in oropharyngeal aspirates with or without diarrhoea. Spread occurs via the faecal-oral route. The virus is shed in faeces in high concentration, which allows its easy identification by electron microscopy.
There is often a preceding or accompanying upper respiratory tract infection or otitis media. Within 2 days of exposure, there is fever and vomiting, which last 1–3 days, and usually preceding the onset of watery diarrhoea, which lasts 4–7 days. Dehydration occurs as a result of marked faecal fluid loss.
Most children with rotavirus diarrhoea have fever. A study from Finland [14] reported that 14% of 336 infants had fever of 39–40.2 °C and 65% had less than 39 °C. Many cytokines, particularly IL-6, IL-10 and INF-γ, play an important role in the pathogenesis of as well as protection against rotavirus reinfection. IL-6 is elevated in children with fever.
Enteric adenovirus: Several studies have shown that adenovirus is second to rotavirus as the most common cause of viral gastroenteritis, occurring commonly during the first year of life. The infection was identified in 8.6% of 900 paediatric inpatients with diarrhoea, serotypes 40 and 41 being the most common isolates [15]. In contrast to enteric adenoviruses, other respiratory adenoviruses are not associated with diarrhoea. Watery diarrhoea is the most common presentation, usually followed by 1–2 days of vomiting. Illness typically lasts 5–12 days (mean 9 days). The duration of the diarrhoea usually lasts longer compared to that caused by rotavirus. Severe dehydration is less common compared to rotavirus infection.
A low-grade fever for 1–3 days is commonly recorded with adenovirus enteritis. A Canadian study [16] of 127 children with adenovirus enteritis found that 41% of them had a rectal temperature of >38 °C. The range of body temperature was 36.2–40.8 °C (mean 38 °C). The average duration of fever was 1.6 days (range 1–30 days).
The outcome of adenovirus gastroenteritis is generally good. Adenovirus is now more frequently diagnosed (due to PCR) in immunocompromised patients and is an important cause of mortality.
Other viruses: Norfolk virus and Norwalk-like viruses are major causes of small and large outbreaks of winter vomiting in older children and adults with or without diarrhoea. These outbreaks occur commonly in recreational camps, communities or schools in the USA. Presentation is similar to that of other types of viral gastroenteritis and includes anorexia, malaise, fever and abdominal cramps, followed within 48 h by vomiting and watery diarrhoea. Symptoms usually last 2–3 days and full recovery is the usual outcome. Astrovirus can also cause gastroenteritis. The infection is frequently asymptomatic in the newborn infants.
Treatment: Breast milk is the best prophylaxis against gastroenteritis, and exclusively breast-fed children remain remarkably free of severe diarrhoea in developed and developing countries.
The standard treatment of all diarrhoeal diseases is the replacement of fluid and electrolyte loss. This is best accomplished by oral rehydration solution (ORS) which has revolutionized the management of diarrhoeal diseases in developing countries. This is safe, cheap, convenient to use and superior to IV fluids because it can be started early at home. The sugar-electrolyte mixture recommended by the WHO contains (mmol/L water) sodium 90, chloride 80, potassium 20, sodium bicarbonate 30 and glucose 111, with an osmolality of 331 mosmol/L. A hypotonic solution with a sodium concentration of as low as 50–60 mmol/L and an osmolality of 224 mosmol/L has been shown in Finland to have clinical advantages over the standard ORS. Rice-based ORS compared with standard ORS reduced the 24 h stool volume. Intravenous electrolyte-glucose solution should be used for children with moderate to severe dehydration and persist vomiting.
Antibiotic therapy is usually not required for patients with gastroenteritis because it does not affect the clinical course of the majority of cases. Severe systemic manifestations associated with bacterial gastroenteritis (notably Shigella, Campylobacter, Yersinia and cholera) probably require antibiotics. Infants with salmonella gastroenteritis less than 3 months of age should be treated with an antibiotic, such as third-generation cephalosporin or a quinolone depending on the regional resistance pattern. Patients with typhoid fever and E. histolytica should also receive antibiotic treatment.
Viral Hepatitis
Hepatitis occurs as a result of a variety of causes, including viruses (hepatitis viruses, Epstein-Barr viruses, cytomegalovirus), bacteria (leptospirosis), parasitic infection (amoebiasis) and drugs.
Hepatitis A Virus (HAV)
HAV is a highly contagious infection, spreading mostly by faecal-oral contact from person to person.
The clinical features are usually mild, and most infected children have an anicteric illness with flu-like symptoms or gastroenteritis with lethargy, nausea, vomiting, abdominal pain and anorexia. Clinical findings often reveal a tender and enlarged liver. Splenomegaly is present in about 20% of cases. About 99% of children recover completely from the infection. Fulminant hepatic failure may occur in the remaining 1%. Chronic hepatitis or cirrhosis is not part of the HAV infection.
Fever, usually low-grade between 38 and 39 °C, is found in about 40% of cases. The low incidence of fever in hepatitis is probably due to impaired production of IL-1β, which increases slightly during the first week of illness, reaching a peak during the second and third week and thereafter decreasing to a normal level. IL-1, IL-6 and TNF-ɑ are mediating the inflammatory process, while IL-10 suppresses it.
Diagnosis rests on detection of the specific IgM, which is a marker of recent infection. It is usually positive before the onset of jaundice, peaking at 1 week and is undetectable 4–8 weeks later. IgG anti-HAV indicates previous exposure and is detectable approximately 1 week later than IgM and persists for years as a sign of immunity. High transaminases enzymes are characteristic of the disease. These enzymes are elevated during the anicteric phase of the illness and usually persist for a few weeks. Serum bilirubin and alkaline phosphatase are mildly or moderately elevated. Prothrombin time is usually normal.
Standard immunoglobulin preparations administered within 2 weeks of exposure have proved effective in preventing hepatitis A. Vaccine against HAV is effective.
Hepatitis B Virus (HBV)
Approximately 350 million people are chronically infected with HBV worldwide. Transmission of this virus usually occurs via vertically from mother-to-child at birth or any bodily secretion or fluid. Children exposed to multiple blood transfusions are at high risk of contracting the virus. The incubation period for HBV infection ranges from 6 weeks to 6 months (mean 90 days). The HB surface antigen (HBsAg) appears during the incubation period several weeks before clinical or biochemical illness develops and is usually undetectable after 6 months. The core antigen (HBcAg) and e antigen (HBeAg) are other antigens of HBV associated with greater infectivity. HBeAg is the only HBV virus that crosses the placenta.
Neonates are at high risk if the mother has acute hepatitis or carries HBsAg (chronic carrier) at delivery. Viral acquisition may follow swallowing of maternal blood during delivery, rarely via the transplacental route or through ingestion of breast milk. Most infants born to HBsAg-positive mothers remain asymptomatic for months and years.
Clinical manifestations are usually absent or mild without evidence of fever. The vast majority of children (>90%) infected with this virus develop a chronic carrier state, and less than 5% develop hepatitis. Children are at risk of developing hepatocellular carcinoma and should therefore be regularly monitored with serial ultrasound scan and serum alpha-fetoprotein. Patients have substantial abnormalities of cell-mediated immunity and cytokine production, including a decreased production of TNF-alpha.
In HBV infection in older children, prodromal symptoms may include urticaria and arthralgia, which precedes a spectrum of clinical presentations ranging from acute viral hepatitis, severe or fulminant hepatitis, chronic persistent hepatitis, chronic active hepatitis to the asymptomatic chronic carrier state.
Urinary Tract Infection (UTI)
UTI is a common cause of an acutely febrile illness in children affecting 7% of girls and 2% of boys. The infection is mainly caused by ascending faecal bacteria from the perineum to the bladder. UTI is frequently the result of sepsis during the first 3 months of age, occurring more commonly in males. Known predisposing factors for UTI include maternal febrile UTI, congenital malformation of the urinary tract, urolithiasis, indwelling urinary catheter, constipation and uncircumcised males. The principal sequence of UTI is vesicoureteric reflux found in 30% of acute cases, which may lead to chronic renal failure and/or hypertension in adults.
The most common organisms are:
Uropathogenic E. coli, which contain lipopolysaccharide, lipoprotein and proteoglycan. By attachment of the bacteria to the urinary tract, these substances are capable of inducing an inflammatory response and fever.
Less common aetiological agents include Proteus mirabilis, Klebsiella pneumoniae, Enterococci and Staphylococcus epidermidis.
The pro-inflammatory cytokines IL-6 and IL-8 play an important role in the inflammatory process of UTI. Serum and urine IL-6 and urine IL-1β positively correlate with fever in UTI. The cytokines sequester the bacteria in the bladder and reduce ascent to the kidneys.
UTI presents in one of the following ways:
High fever, rigor, vomiting, meningism and abdominal discomfort, loin pain and tenderness, usually affecting infants and young children.
As sepsis with or without fever, occurring in about 30% of neonates, 20% of infants aged 1–2 months and 5.0% of infants >3 months of age.
Febrile seizure as the first symptom of an underlying UTI.
As lower UTI (cystitis) with dysuria, frequency, urgency or dribbling, occurring in older children, particularly in girls who are usually afebrile.
Asymptomatic (without fever) bacteriuria is common in school girls (1–2%), but the infection is of little clinical or prognostic significance.
Diagnosis of UTI rests on the following findings:
A febrile child without a focus whose urine showed positive nitrite and leukocytes in the urine dipsticks, which are very suggestive of the diagnosis. Negative result of these two indicators virtually excludes it. A positive urinalysis is defined as five or more WBC per high-power field.
Urine culture as the ultimate tool to confirm or refute the diagnosis. UTI is diagnosed if the urine shows a colony count of 100,000 colonies/mL of a single bacterial species. Suprapubic puncture is important for accurate diagnosis during infancy, and a culture of 50,000 colonies is diagnostic. In older children midstream urine sample is sufficient.
Laboratory tests: Leukocytosis >15,000, high CRP (>40 mg/L to support the diagnosis. CRP is particularly valuable when fever has been present >12 h. IL-6 is a useful diagnostic tool for early recognition of UTI. Procalcitonin (PCT) > 0.5 ng/mL is a major predictor (compared to WBC count and CRP) for identifying children with acute upper urinary tract infection (pyelonephritis) during early stages of UTI.
Once UTI is confirmed, recent NICE guidelines recommend a renal ultrasound scan for all children <6 months of age within 6 months of the infection and no ultrasound scan in children >6 months with uncomplicated febrile UTI. Ultrasound should be arranged early in case of severe or recurrent infections. Micturating cystourography (MCUG) is currently less commonly performed than previously and should be reserved (along with DMSA isotope scan) for atypical presentation or recurrent infections occurring in infancy.
Fever in UTI has the following significance:
About 5% of highly febrile infant and young children have UTI (pyelonephritis), and 20% of children without a focus of infection have UTI.
About 95% of children with UTI are feverish, usually >39.0 °C.
The diagnosis of UTI should be considered in every febrile child, particularly when the fever is without a focus and of duration longer than 24–48 h. A delay in diagnosis and treatment increases the risk of renal scarring.
Resolution of fever after initiating antibiotic therapy indicates adequate therapy.
Persistent fever of >48 h is an indication to admit the child to hospital (if he/she was treated as an outpatient), arranging an ultrasound scan and commencing IV antibiotic treatment.
Afebrile status is a criterion for discharge from hospital.
Therapy: There are no significant differences in persistent renal damage or duration of fever between oral antibiotics (a second-generation cephalosporin or co-amoxiclav) for 7–10 and short courses (2–4 days) of IV therapy followed by oral therapy for the same period. Dysfunctional voiding (e.g. ineffective bladder emptying) should be eliminated. Circumcision should be considered for recurrent UTIs in boys. Probiotics may be useful.
HIV Infection
Over three million children <15 years are estimated to be HIV-infected. This accounts for more than 10% of the total HIV-infected population. Some 50–60,000 HIV-infected infants are born every year. The fast majority of children (90–95%) are infected through vertical transmission mother-to-child (in utero, intrapartum and breast milk). Typical presenting symptoms are fever, asthenia, failure to thrive, prolonged diarrhoea, recurrent infections and lymphadenopathy.
Fever in HIV infection: Fever occurs in 85% and is caused by:
Common viral or bacterial infections, similar to children without HIV infection. Fever >7 days is more likely to be due to bacterial or parasitic infections rather than viral infections. More prolonged fever could be due to TB, connective tissue disease or malignancies.
The HIV infection itself. Acute retroviral syndrome may occur 2–4 weeks after the infection, mainly in teens, as a febrile illness resembling glandular fever.
Immune reconstitution syndrome (IRS). This is a transient deterioration or emergence of new manifestations (such as high fever, worsening of CNS lymphadenitis lesions) of an opportunistic infection occurring after the initiation of antiretroviral therapy (ART). The syndrome also occurs after initiating anti-TB treatment in patients already on ART.
Secondary infections (such as tuberculosis).
Drug fever, commonly associated with ART.
Unknown causes of fever, which may present as a case of pyrexia of unknown origin (PUO).
The incidence of fever is higher with a coinfection such as TB. Children with fever >39.0 °C are at high risk of bacteraemia with S. pneumonia. Unexplained persistent and/or recurrent fever (>37.5 °C intermittent or constant) for >1 month is considered as a moderate severe HIV.
In a study [17] of 316 febrile children with advanced HIV disease, the diagnoses were disseminated mycobacteria avium complex (MAC) infection in 36%, tuberculosis in 16%, B lymphoma (6%), disseminated CMV infection (4%), extrapulmonary cryptococcus (3.5%) and 17% of cases presented as PUO. Other less frequent diagnoses were drug fever, endocarditis, HIV primary infection, pancreatic abscess, pseudomonas aeruginosa bacteraemia and visceral leishmaniasis.
The majority of these patients (about 75%) were receiving co-trimoxazole prophylaxis with or without antiretroviral treatment.
Children with HIV infection often present with:
Fever without focal signs and duration <14 days in HIV (Table 5.10)
Fever without focal signs and duration >14 days (Table 5.11)
Table 5.10.
Differential diagnosis of fever without focal signs and duration <14 days in HIV infected children
| Differential diagnosis | Diagnostic clues |
| Malaria |
• Living or a history of visiting malaria area • Blood film/dipstick positive • The presence of anaemia, low platelets |
| Typhoid fever |
• Seriously ill without apparent cause • Abdominal tenderness • Relative bradycardia in relation to body temperature • Maculopapular rash, often sparing palms |
| Urinary tract infection |
• Dysuria, frequency, pyuria, tenderness in renal angles • Positive nitrate and WBC dipstick |
| Dengue |
• Patient from areas at risk • Sudden onset of high fever with headache, pain behind eyes, joint and muscle pain • Macular rash in 50% (centrifugal, itching) (In dengue haemorrhagic fever, there is in addition bleeding tendency, e.g. from the nose, bowel, fingers) |
| Septicaemia | • Seriously ill with no apparent cause |
| Immune reconstitution inflammatory syndrome |
• Recent start of HAART • CD4% < 10% at start of HAART • Rise in CD4+ lymphocyte count |
| Drug-induced fever | • Nevirapine, cotrimoxazole, dapsone, ß-lactams, isoniazid, anticonvulsants, abacavir, efavirenz |
HAART highly active antiretroviral treatment
Table 5.11.
Differential diagnosis of fever without focal signs and duration >14 days in HIV infected children
| Differential diagnosis | Diagnostic clues |
| Disseminated TB |
• Advanced HIV/AIDS, with anaemia • AFB seen on sputum, gastric aspirate, CSF, pleural fluid and/or fine needle aspirate of lymph nodes • Enlarged mediastinal or hilar lymph nodes, pulmonary infiltrates or miliary lesions on chest X-ray. Enlarged liver or spleen or enlarged lymph nodes on abdominal ultrasound |
| Mycobacterium Avium Complex (MAC) |
• Severe immunosuppression or WHO stage 4 disease • Symptoms compatible with disseminated TB but failing to respond to TB medicines • Absence of peripheral lymphadenopathy • Severe anaemia and neutropenia |
| Cytomegalovirus (CMV) | • Very low CD4 count (CD4 < 50 cells/mm3 in children >5 years) or WHO stage 4 disease. Blind spots in one or both eyes, with signs of retinitis |
| Disseminated cryptococcal infection |
• Very low CD4 count (CD4 < 50 cells/mm3 in children >5 years) or WHO stage 4 disease • Headache, molluscum-like skin lesions • Positive serum cryptococcal antigen tests • Isolation of the pathogen from CSF, lymph nodes, sputum or skin ulcers (Indian ink) |
| Visceral leishmaniasis |
• Splenomegaly, lymphadenopathy. Pancytopenia • Amastigotes seen in samples of tissue or body fluid under the microscope (Giemsa stain) |
| Bacterial endocarditis |
• Enlarged spleen, heart murmur • Petechiae on skin and mucosa, anaemia • Splinter haemorrhages in nail bed |
| Relapsing fever |
• Exposure to ticks or body lice • Recurrent pattern of fever. Headache, muscle pain, enlarged liver and spleen, red eyes and photophobia |
| Abscesses | • Tender or fluctuant mass, often detected by ultrasound |
| Trypanosomiasis |
• Travel to or living in region with tsetse flies • History of painful trypanosomal chancre at site of inoculation of the parasite • Bouts of high fever lasting several days are separated by afebrile periods, lymphadenopathy, itching and maculopapular rashes |
Evaluation of fever among patients with HIV infection requires a detailed history, focusing on:
Duration of fever
Recent travel to an area of malaria or dengue disease
Skin rash, cough, pain during swallowing, headache, diarrhoea, dysuria
Weight loss
The last CD4 cell count? (normal CD count: 600–1000)
Current treatment (e.g. ART) and adherence
Examination should include routine physical examination focusing on areas likely to be involved in the infection, such as thorough palpation of the lymph nodes, neurological examination and fundoscopy for cytomegalovirus (CMV) and TB.
Laboratory investigations should include the following:
Blood tests: complete blood count with differential counts; blood chemistry (transaminases, alkaline phosphatase, LDH); blood smear for malaria; serum cryptococcal antigen test (SCrAg); dipstick for malaria (rapid tests), if in endemic zone; viral load, CD4 count; dengue serology (if patient is living or have travelled to endemic areas)
Urinalysis
Chest X-ray, abdominal ultrasound
Stool examination for bacterial culture and AFB
Lumbar puncture
Mantoux Test or INF gamma assay
Management of newly diagnosed children who present with PUO entails:
A thorough search and adequate treatment of the secondary infections should be carried out prior to starting the antiretroviral therapy.
The above investigations should be initiated prior to any treatment.
Antibiotics to cover the likely infections, particularly Streptococcus pneumoniae while waiting for results may be required.
Patients with confirmed or probable TB (abnormal chest X-ray, positive gastric aspirate/ sputum AFB, abdominal lymphadenopathy, positive IFN gamma release assay) should start on antituberculous treatment. This treatment is also indicated as an empirical therapy in cases of unexplained weight loss and fever in advanced AIDS.
If a patient is not improving on anti-TB treatment, alternative diagnoses such as MAC should be considered.
Patients responding to mycobacteria avium complex (MAC) therapy should continue until CD4 cells have adequately recovered. This may takes months/years.
During the whole period of treatment, patients should repeatedly be re-evaluated for the appearance of new symptoms and signs, which may indicate additional infections.
Management of HIV patients with PUO while taking antiretroviral therapy:
An associated skin rash should arouse the suspicion of drug fever. Nevirapine is a frequent cause of this. Abacavir is also a cause of hypersensitivity reactions.
Patients who initially responded to treatment for opportunistic infections (OI) prior to the start of antiretroviral therapy, and then developed a worsening of the OI after the start of antiretroviral therapy (e.g. reappearing of fever), should be considered as having IRS (if other obvious causes of fever are excluded). Patients should continue OI and ART, but steroids treatment should be considered.
Infections of the CNS
Meningitis
Meningitis remains one of the most important infectious causes of neurodisability and death in childhood. Newborn infants and children between 6 and 12 months of age are at greater risk of meningitis than older children; 90% of reported cases occur below 5 years of age. Congenital and acquired T- and B-cell defects, sickle-cell anaemia, splenectomy and malnutrition all predispose to meningitis.
Definitions of the clinical variations of the CNS (central nervous system) infections are provided in the Table 5.12.
Table 5.12.
Definitions of meningitis, meningococcal disease and encephalitis
| • Confirmed meningitis: isolation of bacteria from CSF, blood or DNA detection through PCR from a patient with a CSF pleocytosis of white cells >10 cells/mm3. In neonates a pleocytosis of >20 white cells is accepted. Diagnosis is also accepted in case of postmortem diagnosis. |
| • Probable meningitis: the presence of clinical symptoms and signs of bacterial meningitis in the absence of laboratory confirmation. |
| • Meningococcal disease: a clinical condition caused by Neisseria meningitidis with purulent conjunctivitis, septic arthritis and septicaemia with or without meningitis. |
| • Aseptic meningitis: the presence of CSF white cell count >10 cells/mm3; CSF is negative for bacterial culture, occurring usually in summer months. Viruses are most common causes. |
| • Encephalitis: an inflammation of the parenchymal tissue of the brain caused by an infection producing varying degrees of impaired consciousness. |
Meningitis occurs most commonly in the individual who bears the organisms as an asymptomatic carrier. Organisms enter the CNS through vulnerable sites in the blood-brain barrier (choroid plexus or cerebral microvasculature). The cell wall components of these organisms stimulate macrophage-equivalent brain cells (astrocytes, microglia). Once bacteria reach the CSF, they are likely to survive because humoral defences, including immunoglobulin, complement and opsonic activities, are virtually absent. Meningitis may also result from haematogenous dissemination or rarely by direct invasion from ear or sinus infection. Several cytokines, particularly IL-1 beta, IL-2, IL-4, IL-6 TNF-alpha and INF-gamma, increased the blood and CSF in almost all children with meningitis (Fig. 5.2).
Fig. 5.2.
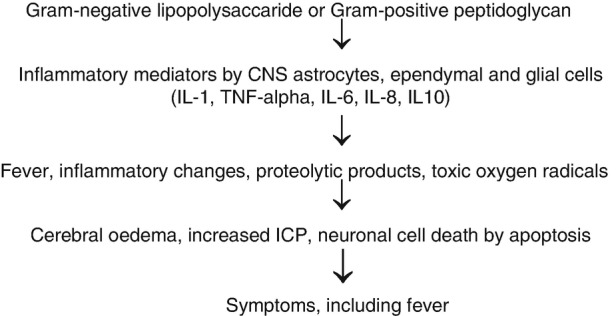
Pathogenesis of meningitis and fever
Meningitis accounts for an estimated 180,000 deaths every year worldwide. The widespread use of vaccines against Neisseria meningitidis, H. influenzae type B (Hib) and pneumococci have dramatically decreased the incidence of these forms of meningitis and their complications in well-immunized populations by approximately three quarters. This has led to an increase of the median age of patients with bacterial meningitis to nearly 40 years of age. In developing world with low immunization rates, however, these types of bacterial meningitis still occur.
Bacterial Meningitis
Neonatal meningitis is most common during the first week of life (early onset). Beyond the first week of life, it is termed late-onset. The susceptibility of neonates to meningitis, particularly premature infants, is mainly due to immaturity of cell- and antibody-mediated immune mechanisms. The neonate is infected by bacteria from the maternal genital tract, the risk being higher after membrane rupture.
A study of 274 neonates from England and Wales established an annual incidence of bacterial meningitis at 0.21/1000 births [18]. The overall case fatality rate was 6.6%. Group B streptococcus was the leading pathogen (about 50% of cases, Table 5.13). Currently, E. coli is the predominant bacteria isolated. In contrast to older children, the onset of neonatal meningitis is usually insidious. Infants present with:
Symptoms such as failure to feed, lethargy alternating with irritability, seizures, vomiting, thermal instability (fever or hypothermia), cyanosis, apnoea, jaundice and respiratory distress.
Signs such as an ill appearance, a tense or bulging fontanelle, pallor and reduced capillary refill time. Neck stiffness and head retraction are not parts of the symptomatology.
Table 5.13.
Causes of bacterial meningitis
| Neonate | |
| • Early-onset |
(Caused by vertical transmission) Group B streptococcus (GBS) Escherichia coli (E. coli) Listeria monocytogenes Coagulase-negative staphylococci H. influenzae |
| • Late-onset |
(Caused by nosocomial or community spread) Gram-negative enteric bacteria: E. coli, Klebsiella, Enterobacter, Salmonella, Proteus, Pseudomonas |
| Older children |
Neisseria meningitidis Streptococcus pneumoniae H. influenzae |
Complications include hydrocephalus, ventriculitis, neurodisability and seizures.
Meningitis in older children is mostly meningococcal (in combination with sepsis called meningococcal disease, MCD) or pneumococcal. Less common causes are E. coli, group B streptococci, staphylococci Listeria, Borrelia burgdorferi (Lyme disease), TB and fungi. Factors that increase the risk for bacterial meningitis include immunoglobulin deficiency (e.g. HIV infection), asplenia, neurosurgical procedures (e.g. ventriculoperitoneal shunt), penetrating head injury and cochlear implants (particularly for pneumococcal meningitis).
Meningitis has a variety of presentations:
In MCD, the nonspecific early symptoms (in the first 4–6 h) are fever, irritability and decreased appetite. This is followed (at a median time of 8 h) by early symptoms of sepsis: leg pain, abnormal skin colour and cold hands and feet. Classic meningitis symptoms appear later (13–22 h): purpuric rash, impaired consciousness and meningism.
Fever, vomiting, irritability or drowsiness, headache and photophobia.
Convulsive status epilepticus with fever.
Tuberculous meningitis compromises about 5–10% of extrapulmonary cases of TB. It often occurs within 6 months of the initial Tb infection following haematogenous dissemination or a rupture of a subependymal focus into subarachnoid space. Fever is the most common presenting symptom, and meningism (e.g. neck stiffness) is the most common finding at presentation. The incidence is highest in children aged 1–5 years. The three recognized stages are:
Conscious, with nonspecific symptoms (fever, night sweats, anorexia, weight loss, fatigue) and no neurological signs
Onset of neurological signs: headache, confusion, drowsiness, neck stiffness
Stupor, deepening coma, focal neurological signs
Relationship Between Meningitis and Fever
Fever in bacterial meningitis is:
The most common presenting symptom in children beyond the neonatal age owing to the presence of inflammatory mediators, particularly IL-1 and TNF in blood or within the CNS. In MCD, fever was the first symptom in children younger than 5 years and 94% developed fever at some point.
Uncommon in neonatal meningitis. It occurs in 30% of neonates with E. coli meningitis. Neonates have a reduced capacity to produce cytokines, which may explain their frequent afebrile presentation.
Usually very high in older children. Temperatures between 40 and 41 °C are common, with a mean degree of 39.2 °C. The degree of fever varies depending on the age of the patient and the causative organisms. The incidence of fever was 71% with meningococcal infection, 88% with staphylococcal infection and 90% with H. influenzae type B. Children with TB meningitis have the highest incidence of fever with 97% [19].
Absent in rare cases of severe infection. Hypothermia carries a bad prognosis.
May present as febrile seizures with meningitis as the underlying cause. These children are usually symptomatic (e.g. impaired consciousness) prior to the seizures. Features such as complex type of seizure (e.g. prolonged or focal) are suggestive of possible meningitis.
- An important sign when monitoring the effect of treatment in bacterial meningitis, i.e. normalization of fever, is very suggestive of a good response and improvement. Nonresponders may produce the following fever patterns:
- Persistent for 4–7 days
- Prolonged >7 days
- Secondary fever (fever reappearing after at least one afebrile day)
The following considerations should be made in persistent or prolonged fever:
-
The antibiotics or the doses used for meningitis therapy are inappropriate
(e.g. penicillin administered for staphylococcal meningitis).
The meningitis may be aseptic or TB meningitis.
There are complications listed in Table 5.14.
The child needs thorough re-evaluation to find out the cause of the fever.
Morbidity and mortality are higher than in those cases who have responded to treatment.
Table 5.14.
Causes of persistent, prolonged and secondary fevers in meningitis
| Persistent |
| • Causative organisms S. pneumonia or H. influenzae, fungi |
| • Foci of the infection |
| • Nosocomial infection |
| • Subdural effusion |
| • Drug fever |
| • Phlebitis |
| Prolonged |
| • Subdural effusion |
| • Drug fever |
| • Arthritis |
| Secondary |
| • Causative organisms S. pneumonia or H. influenzae, fungi |
| • Nosocomial infection |
| • Subdural effusion |
| • Drug fever |
Animal models of meningitis have provided substantial information on the pathophysiology of fever in the disease. Fever on experimental meningitis in rabbits concluded that high body temperature had a direct inhibiting effect on the growth rate of bacteria in the CSF. On the other hand, the lower the temperature, the faster was the rate of bacterial growth. Thus fever is likely to be a host defence in this disease. Similar results are available in human studies. The reported overall case fatality rate in 100 children with meningococcal infection (55 had meningitis) did not indicate a poor prognosis, but all children with hypothermia died [19].
In a study of 476 children with meningitis, 90% of patients with S. pneumoniae and N. meningitidis became afebrile within 5 days of the antibiotic therapy, compared to 72% of those with H. influenzae meningitis. The rate of persistent fever, prolonged fever and secondary fever was 13, 13 and 16%, respectively [20]. Complications from meningitis have decreased following decreased incidence of meningitis due to the routine H. influenzae vaccination in 1992 and recently pneumococcal vaccine but still occur with other types of bacterial meningitis, including persistent and prolonged fever.
Laboratory findings include:
Characteristic CSF findings (Table 5.15) and identification of the pathogens in CSF and/or blood cultures and/or PCR. In TB meningitis, additional positive findings are microscopy for acid-fast bacilli from CSF, gastric aspirate, sputum (ZN stain), tuberculin test >5 or 10 induration, history of TB contact and radiological evidence in the CNS of tuberculoma and/or other changes, such as hydrocephalus.
A polymorphonuclear leukocytosis and high CRP in the blood.
High procalcitonin (PCT) level (>0.5 ng/mL). PCT is a precursor of calcitonin, which is more valuable than CRP and IL-6 in early differentiating bacterial from viral meningitis. PCT is also higher in severe compared to mild disease.
Other abnormalities: Inappropriate secretion of ADH with hyponatraemia, water retention, increased intracranial pressure, DIC (manifesting as thrombocytopenia, increased fibrin degradation products and prolonged prothrombin, PT, and partial thromboplastin time, PTT).
Table 5.15.
Usual CSF findings in normal and in various central nervous system (CNS) infections
| Normal | Cell-mm3 | protein Mg/dl | CSF/serum glucose ratio % |
|---|---|---|---|
| Normal | 0–5 (lymphocytes) | 20–40 | >50 |
| Bacterial meningitis | 100 to 1000 (PMN) | 100–500 | <0.5 |
| Tuberculosis | 30–600 (lymphocytes)a | >100 up to 3 g | <0.5 |
| Viral meningitis | 100–2000 (lymphocytes)a | Normal to 200 | Normal |
| Encephalitis | Normal to few hundreds | 50–100 | Normal |
| Abscess | 10–100 (PMN/lymphocytes | 30–200 | Normal |
PMN polymorphonuclear cells
aPMN predominate initially with lymphocytes predominating after 48 h
Complications include seizures, neurodisability, paralysis of the cranial nerves, subdural collection, blindness, hydrocephalus, cerebral herniation and deafness.
Therapy consists of prompt IV administration of antibiotics. Neonates are treated with cefotaxime, penicillin (or ampicillin) and gentamicin for a duration of 2 (GBS and Listeria) or 3 weeks (Gram-negative bacteria). Older children are treated with third-generation cephalosporin cefotaxime or ceftriaxone. Treatment of TB meningitis is shown in Table 5.16. Dexamethasone has been advocated for the treatment of bacterial meningitis. Early dexamethasone has been shown to reduce the duration of fever, levels of cytokine concentration and the incidence of hearing impairment. It is mainly beneficial for H. influenzae and S. pneumoniae meningitis if it is given with or before antibiotics.
Table 5.16.
Treatment recommended for children with tuberculosis
| Drugs | Daily dose mg |
Maximal daily mg/kg/day |
Major side-effects |
|---|---|---|---|
| INH | 10 | 300 | Peripheral neuropathy |
| Rifampicin | 10–20 | 600 | Hepatitis |
| Pyrazinamide | 25–35 | 2 g | Hepatotoxicity |
| Ethambutol | 15–20 | 2 g | Optic neuritis |
| Streptomycin | 40 | 1 g | Ototoxicity |
Intravenous fluid should be restricted to minimize the effect of inappropriate ADH effect and the cerebral oedema. Monitoring the electrolytes and body weight is important for the management of the fluid and electrolyte balance.
The presence of coma, shock, seizures and hypothermia are associated with poor prognosis. Children with TB meningitis usually make full recovery if they are fully conscious at presentation, while those in coma have high rate of neurodisability and deaths. The younger the child, the worse the prognosis.
Viral Meningitis
The true incidence of viral meningitis is unknown mainly because CSF with aseptic meningitis is often not examined for viruses. The incidence of proven viral meningitis is 0.05/1000 live births. As there has been substantial reduction in bacterial meningitis following routine vaccination, most childhood meningitis in developed countries is now caused by viruses. The most frequent aetiological agents remain non-polio enteroviruses (echovirus and coxsackievirus). Mumps meningitis, which used to be the most common form of viral meningitis prior to the combined measles, mumps and rubella (MMR) vaccination in 1988, has declined dramatically. Symptoms are similar to those of bacterial meningitis, but they are usually mild and the children appear generally well. This infection affects mainly older children.
Fever varies usually between 38.5 and 39.5 °C, rarely higher. Fever along with drowsiness and irritability are the major presenting symptoms. The incidence of fever is around 70%.
Of the various cytokines capable of inducing fever, INF-gamma produced in the intrathecal space appears to be associated with the pathogenesis of viral meningitis and the production of fever. CSF INF-gamma levels correlate well with the severity of febrile episodes.
Laboratory findings include clear or rarely opalescent CSF. CRP and WBC are usually normal. Procalcitonin is a useful marker to differentiate bacterial and aseptic meningitis.
Diagnosis requires isolation of the specific virus from the CSF and/or a fourfold rise in antibody titre to the virus. Rapid identification of the virus by immunofluorescent examination of the CSF is possible for many viruses. The prognosis is very good.
Acute Viral Encephalitis
This is an illness with an acute onset and rapid progression caused commonly by herpes simplex virus (HSV). Other viruses include varicella, cytomegalovirus, EB-virus, coxsackievirus, echovirus, poliovirus, mumps, measles and adenovirus. The annual incidence is 8.8/100000 children younger than 16 years of age [21].
Clinical features vary depending on the nature of the causative virus, the age of the patient and the severity of the infection. Commonly the disease begins with an acute onset of fever, headache and vomiting. Evidence of meningeal irritation and stiff neck is often lacking. Encephalitis is suggested by drowsiness, paralysis, coma, seizure (febrile seizure), ataxia, tremor, mental confusion or hyperexcitability. Ataxia is common, particularly following varicella encephalitis.
Fever is common in viral encephalitis irrespective of the causative agent. It was present in 30% patients with mumps encephalitis, in 85% with coxsackievirus B encephalitis and in 90% of patients (A third had a fever greater than 39 °C) with herpes encephalitis [22]. Fever, lethargy and headaches may last 4–5 days before other symptoms (such as behavioural abnormalities) occur.
Laboratory diagnosis of herpes encephalitis mainly depends on PCR (polymerase chain reaction) detection from the CSF, which is highly sensitive and specific. EEG commonly shows paroxysmal focal abnormalities (such as slow complexes every 2–3 s) over the involved temporal areas. A CT scan of the head may show characteristic low-density lesions in these areas, in addition to diffuse brain oedema. An MRI is a superior investigation for showing lesions in the temporal areas, uni- or bilateral.
Therapy with acyclovir should be initiated to all cases with suspected encephalitis while awaiting laboratory confirmation.
Subacute sclerosing panencephalitis (SPPE) is a progressive inflammatory disease of the CNS caused by persistent, aberrant measles virus infection, characterized by progressive loss of intellectual function, with behaviour and learning difficulty, often associated with abnormal myoclonic movements. High anti-measles antibody titres in serum and CSF confirm the diagnosis. The mean interval between measles and the onset of SPPE is about 10 years. The MMR vaccine has resulted in virtual elimination of SSPE. Fever is not part of SPPE.
Brain Abscess
Brain abscess is uncommon in children. It may occur as a complication of otitis media, mastoiditis, sinusitis or meningitis or ventriculoperitoneal shunt infection, following trauma or surgery to the skull or as a result of haematogenous dissemination in children with acyanotic congenital heart disease.
Fever was the most common clinical finding in a study [23]of 101 children with brain abscess, occurring in 80% of the children, followed by vomiting, headache, seizure, focal neurological abnormalities and lethargy. Papilloedema and meningeal signs were also common. Overall mortality was 30%. High fever, age less than 1 year, multiple brain foci and the presence of meningism or coma have a poorer prognosis.
The most frequently encountered pathogens are S. aureus, streptococci and Gram-negative aerobic bacilli.
Laboratory findings in the CSF reveal that the CSF culture is usually negative unless there is rupture of the abscess into ventricles. A CT scan shows the characteristic finding of a ring-enhancing lesion.
Therapy consists of antimicrobial treatment (third-generation cephalosporin, vancomycin and metronidazole) with or without surgical excision or aspiration.
Osteomyelitis and Septic Arthritis (See Also Chap. 10.1007/978-3-319-92336-9_12: Differential Diagnosis: Arthritis)
Infection of the bone may occur as a complication of septicaemia or due to local trauma (e.g. wound, abrasion). Acute haematogenous osteomyelitis involves most commonly the rapidly growing metaphysis of the long bones. The femur and tibia are most commonly affected bones. Septic arthritis is usually haematogenously acquired or the result of an extension from an osteomyelitic lesion. The knee is most commonly involved. Staphylococcal aureus is the most frequent bacteria causing the infection (accounts for 90%), followed by Kingella kingae, S. pneumonia, S. pyogenes and P. aeruginosa as less common causes. Children with sickle-cell anaemia and other haemoglobulinopathy are at high risk of osteomyelitis caused by non-typhi salmonella.
This infection presents:
In neonates with irritability and tenderness when the affected area is touched. There is limited movement of the affected extremities (Pseudoparalysis). Fever is either mild or absent.
In older children with high fever, refusal to walk, bone pain and limping (if the lower extremities are affected). Examination reveals localized pain, tenderness, warmth and erythema of the affected area.
The diagnosis is based on the following criteria:
The isolation of bacterial pathogens or positive PCR from blood (positive in 30–60%), bone or joint. Needle aspiration of the soft tissue or incision and drainage of the bone may yield the organism. In septic arthritis, joint fluid aspiration usually reveals purulent exudates with >50,000 leukocytes/mm3, Gram-positive cocci and a positive culture. Leukocytosis and elevated CRP are usually present. CRP is a very reliable parameter to assess the effectiveness of the treatment and recovery.
Radiological findings (soft tissue swelling, bone rarefaction, periosteal elevation, bone necrosis) may not appear during the first 2 weeks of the infection. A nuclear bone scan (showing increased uptake of the isotope) is a valuable adjunct to the diagnosis and is often positive before the appearance of the lesion in the X-ray.
Fever is the most common presenting symptom of bone infection, occurring in 90% on admission with a mean temperature of 39.1 °C [24]. The majority of those who were afebrile on admission became febrile during the ensuing 48 h after admission. Normalization of fever is not usually achieved during the first week despite antibiotic treatment. High fever usually continues for 4–5 days after the treatment. Therefore the presence of persistent and high during treatment does not necessarily signify failure of antibiotic treatment.
Initial antibiotics are likely to include IV ceftriaxone with clindamycin, flucloxacillin or fucidin for 3–6 weeks.
Viral Exanthems
Viral exanthems are common causes of febrile illness in children. More than 50 viral agents are known to cause a rash. Historically, exanthems were numbered in the order in which they were differentiated from other exanthems. Thus the first was measles; second, scarlet fever; third, rubella; forth, so-called Filatov-Dukes disease (no longer recognized as an entity); fifth, erythema infectiosum; and sixth, exanthema subitum. As more exanthems were described, numerical assignment became impractical.
Measles
The first written record of measles is credited to Razes, a Persian physician of the tenth century; before that measles was thought to be a mild form of smallpox. Sydenham in the seventeenth century drew an accurate clinical picture of the disease, including recognition of its complications. When the USA was swept by measles during the seventeenth and eighteenth centuries, the infection was still believed to be a sequel to smallpox. Measles virus was cultivated in 1938.
Prior to the present vaccine, the attack rate of measles worldwide was close to 100% and measles was an important cause of mortality. Measles vaccine resulted in about 80% decease in measles deaths, preventing an estimated 20.3 million deaths between 2000 and 2015 [25]. In developing countries without immunization, measles affects virtually all children by the age of 4 years, the highest incidence being in the second half of the second year. Mortality in the past has ranged between 15 and 25%. More recently this mortality has decreased progressively in developing countries. The single most important factor affecting mortality is poor nutritional status, leading to deficiencies in cell-mediated immunity and often death due to giant-cell pneumonia, diarrhoea or inclusion body encephalitis.
Measles is caused by paramyxovirus, which spreads by droplets from person to person. The incubation period is about 11 days. The spreads of the virus occur through the following steps:
Virus entry to the epithelium of the conjunctiva and upper respiratory tract.
Viral antigens activate macrophages and T cells to produce pro-inflammatory cytokines TNF, IL-1β, IL-6 and IL-17. The IFN production is inhibited.
High affinity IL-2 receptors rise before the onset of the rash and remain elevated for several weeks.
Following its spread by day 5 to the mononuclear phagocytes of the liver and spleen, the virus continues its spread by day 8 via the blood to its target tissue (eye, lung and gut epithelial cells). During these stages, viral spread is limited by natural killer cells and cytotoxic T cells. B cells are primed to produce antibody.
Complications occur in about 30% and include pneumonia (viral or bacterial), otitis media, gastroenteritis, laryngitis, encephalitis, bronchiectasis, reactivation of tuberculosis and SSPE.
Fever in measles: Clinically, the infection progresses through the following steps:
The pre-exanthem stage expresses like a common cold, with abrupt high fever, sneezing, dry cough and conjunctivitis. The temperature increases gradually to reach a level ranging from 39 to 40.5 °C that lasts 4 to 7 days. About 24 h prior to the appearance of exanthem, Koplik’s spots can be detected in about 80% of cases as tiny (about 1 mm) whitish spots in the buccal mucosa opposite the lower morals.
The exanthem appears at the peak of symptoms with a temperature of about 39.5 °C. The rash appears first behind the ears and spreads to the face, neck, trunk and extremities. The rash begins to clear on the third day. During the exanthem period, the fever usually peaks on the second or third day and then falls by lysis over a 24-h period. Fever which persists after the third day may signify bacterial complication. There are signs of pharyngitis, cervical lymphadenopathy and occasionally a mild splenomegaly. Shortly after the rash appears, the child becomes anergic, with suppression of the delayed hypersensitivity to skin test antigens and reduced lymphoproliferation and lymphokine production in response to mitogenic stimuli. The infectivity decreases considerably with the onset of the rash.
Laboratory findings: Blood counts often show leucopenia and lymphopenia. Suppression of immune function is manifested in vivo by the loss of response to tuberculin skin test. The diagnosis of measles can be confirmed by measles complement fixation or haemagglutination antibody test. Blood or saliva can be utilized to demonstrate measles-specific IgA.
Therapy: Paracetamol or ibuprofen may be administered to reduce fever and pain Aspirin should be avoided because of Reye’s syndrome. Gamma globulin (0.25 mg/kg) within 5 days of exposure to measles virus prevents the disease. Treatment is symptomatic. Oral vitamin A (400,000 U) can decrease mortality in children in developing countries.
Varicella
Varicella zoster virus is a member of the herpesvirus family. The eruption is often the first sign of the onset of varicella, particularly in young children. Older children and adults may have prodromal symptoms preceding the characteristic eruption by 1–2 days, which include fever usually in the range of 38–38.5 °C (temperature up to 40.5 °C may rarely occur during the first 3 days), malaise, headache and abdominal pain. The characteristic eruption of macules and papules appears first on the back and then on the rest of the trunk, spreading within hours to the face and scalp. The lesions progress from macules to papules to vesicles and begin crusting within 8–10 h. Characteristically, these lesions are found simultaneously.
When maternal varicella develops within 4 days of delivery, neonates develop severe varicella within 5–10 days postpartum. The disease is associated with a mortality of around 20% due to disseminated chickenpox, usually with severe pneumonitis. When maternal varicella develops 10–20 days before delivery, transfer of maternal antibodies causes a more benign illness.
Varicella is usually a benign disease. Complications include pneumonia in about 1% (affecting primarily adults and newborn) with a chest X-ray showing nodular infiltrates, secondary staphylococcal skin infection, thrombocytopenic purpura, cerebellar ataxia and encephalitis. Secondary bacterial infection from staphylococci and streptococci can be fatal and needs urgent treatment. Varicella is severe and may be fatal in patients with impaired cellular immunity, such as those receiving cytotoxic drugs. Children with hypogammaglobulinaemia recover normally from varicella.
Therapy: The majority of patients require no special treatment. Aspirin should not be administered because of the risk of Reye’s syndrome. Itching can be relieved by simple soothing lotions such as calamine and oral antihistamine. Patients with severe varicella or with complication should receive acyclovir. This antiviral drug promotes the cutaneous healing and reduces the duration of fever. A vaccine is now available and is increasingly being used to prevent this disease. Vaccination is associated with increased risk of febrile seizures (FS), and the use of antipyretics prophylactically prior to vaccination does not prevent FS.
Rubella
Rubella virus may cause inapparent or severe infection. The infection is usually mild, and children usually present with sore throat, rash, lymphadenopathy and low-grade fever (rarely exceeding 39 °C) for several days. Fever may persist for 1–2, rarely 3 days. In older children, particularly in females after puberty, the infection is more severe and prolonged. There are usually painful and visibly enlarged lymph nodes, involving postauricular, occipital and posterior cervical nodes, with polyarthralgia or arthritis.
The infection with rubella virus is particularly important to paediatricians because of possible foetal-maternal transmission. Congenital infection (rubella syndrome) is highest in the early weeks of pregnancy, manifesting as eye disease (cataract, retinopathy, glaucoma), sensorineural deafness, heart lesions (patent ductus arteriosus, pulmonary artery stenosis, aortic stenosis, coarctation of the aorta or ventricular septal defect), neurological abnormalities or thrombocytopenic purpura. Prevention of maternal rubella used to be through routine immunization of all girls of 11–14 years of age and women of child-bearing age, but the use of the MMR has been more successful in reducing rubella syndrome by preventing transmission of the virus from children to pregnant mothers. Rubella, as measles, could be eliminated worldwide if comprehensive vaccination was achieved.
Erythema Infectiosum (EI)
EI or the fifth disease is an acute benign, communicable disease with a characteristic eruption that usually affects children aged 5–15 years. The infection is caused by parvovirus B19, which also can cause a transient aplastic crisis in patients with haemolytic anaemia, bone marrow failure, anaemia and hydrops during pregnancy and arthritis similar to rheumatoid arthritis.
Fever in EI: During 5–10-day incubation, children may be asymptomatic or have mild influenza-like symptoms with fevers. The eruption is generally the first and only diagnostic clinical manifestation of the disease, occurring in 100% of cases. It starts on the face with a “slapped cheeks” appearance, with nasal sparing, resembling scarlet fever. The rash spreads to the trunk and extremities in 1–4 days after the onset of the facial rash. The rash is erythematous maculopapular and tends to assume a reticular or lacy pattern, which last for 4–6 days. Fever is observed in about 23% of cases. Common associated clinical findings are pruritis, arthralgia/or arthritis (mainly in adults) and headache. Encephalitis is a very rare complication.
Exanthema Subitum (ES)
ES is a common self-limiting illness caused by human herpes virus 6 (HHV-6) that was identified in 1988. HHV-7 can also cause ES. The virus is a major cause of febrile illness with viraemia and a high temperature (mean 39.7 °C). Sometimes the virus can cause febrile seizures, an inapparent infection without fever or a rash without fever or fever without any focus. HHV-6 is implicated in drug-induced hypersensitivity syndrome, multiple sclerosis, chronic lymphocytic thyroiditis and chronic fatigue syndrome.
ES is the most common febrile exanthem in children under the age of 3 years causing up to 20% of all febrile illnesses. Approximately 30% of children develop this disease eventually. Ninety percent of all cases occur in children aged 6–24 months. HHV-6 stimulates the secretion of pro-inflammatory cytokines including IL-1β, IL-15, TNF-ɑ and interferon.
Before the onset, children may have a short period of irritability and malaise. Onset of fever is abrupt (sometimes triggering a febrile seizure) and characteristically continuous (or less commonly intermittent), often as high as 40–41 °C. The fever persists for 3–4 days in about 75% and for 5–6 days in the remaining 25%. There is usually no focus to explain the presence of fever except often a mild pharyngitis, suboccipital or posterior cervical lymphadenopathy. The temperature usually drops by crisis over a period of a few hours, coinciding with the appearance of the rash (Fig. 5.3). The rash appears predominately on the neck and trunk, lasting 24–36 h. Characteristically, the child becomes well and afebrile when the rash erupts.
Fig. 5.3.
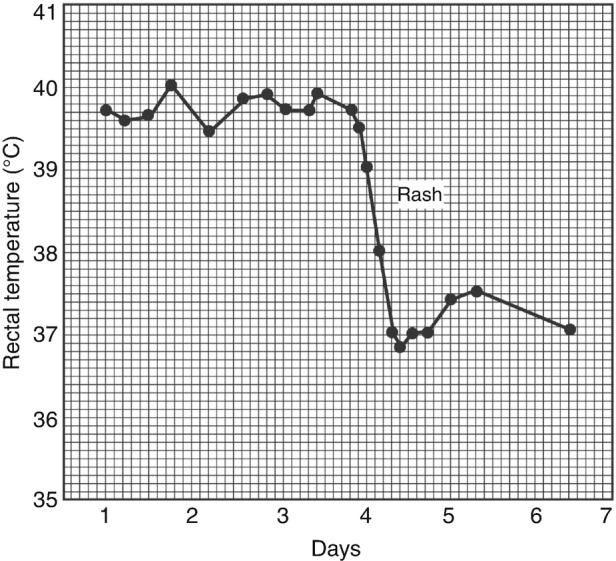
Continuous fever pattern seen in erythema subitum, with a drop in temperature by crisis
When fever is intermittent, the temperature is normal or slightly elevated in the morning, only to rise to 40–40.5 °C by early evening. Fever may fall by lysis over a period of 24–36 h.
Laboratory findings commonly show leukocytosis of 12,000–20,000 with a slight increase in neutrophils.
Tropical Diseases
Tuberculosis
Tuberculosis is a major cause of morbidity and mortality throughout the world. Although reported cases have declined, particularly in developed countries, about one million children still develop TB each year, and about 210,000 die because of its complications [26]. Children acquire the infection from adults who have active disease and are expectorating tubercle bacilli. Children themselves are non-contagious. Therefore every effort should be made to identify the adult source for eradicating the source.
Neonatal TB occurs through transmission of infection from mother to infant via the placenta or amniotic fluid. Neonates present with feeding difficulty, failure to thrive, jaundice, respiratory distress or hepatosplenomegaly. Fever is usually absent. Chest X-ray shows bronchopneumonia. The disease often runs a fulminant course with rapid multiplication of tubercle bacilli and minimal giant cell formation.
Older children often experience typical reactivation tuberculosis with classical symptoms of low-grade fever (38–38.5 °C), night sweats and cough. Radiologically, a parenchymal lesion is usually not visible, but hilar adenitis is prominent and may cause compression of the adjacent soft bronchus, causing wheezing and non-productive cough. With increased compression, or following perforation of an infected lymph node into the bronchus, segmental atelectasis may ensue. Other presentations are erythema nodosum, phlyctenular conjunctivitis (as a result of hypersensitivity reaction) or TB pneumonia, which resembles radiologically bacterial pneumonia with high fever, cough and dyspnoea. Haematogenous disseminated TB may cause miliary TB in children <3 years and within 2–6 months of infection. The illness can be either acute or more often indolent and prolonged with spiking fever found in about 75% of cases. Associated symptoms include anorexia, weight loss, night sweats and dyspnoea. Ophthalmoscopy may detect typical choroidal tubercles in the retina.
Extrapulmonary manifestations account for about 30% of cases, of which two thirds present with lymphadenitis of cervical lymphadenitis, followed by TB meningitis.
The diagnosis of TB is established by:
History of contact with an infectious case.
Symptoms: persistent, unremitting cough, persistent fever and fatigue, night sweating, chest pain and weight loss.
Identification of the mycobacteria (positive in about 30–40% of cases), from sputum, early morning gastric fluid, pleural fluid, CSF or other tissues or by PCR. Acid-fast smear is positive in 10–20%.
X-ray findings, often in the form of “unresolved pneumonia”, with enlarged mediastinal lymphadenopathy.
Positive tuberculin test, performed by using 5 tuberculin units of purified protein derivative (PPD). A positive reaction is 5 mm or more induration present after 48–72 h.
Detection of Mycobacterium tuberculosis-specific antigens (IFN-γ release assays).
Fever in TB may occur in the following situations:
In pulmonary TB, disseminated TB, e.g. miliary TB, and in extrapulmonary TB. Children with combined intrapulmonary and extrapulmonary TB have a higher peak and a longer duration of fever than those with intrapulmonary TB alone.
As a persistent fever without focus for several weeks and sometimes for several months presenting as pyrexia of unknown origin (PUO).
In HIV as a coinfection, often present as unresolving pneumonia. This carries a high mortality despite adequate anti-TB and HIV therapy.
In hypersensitivity to antituberculous drugs (usually appearing between the third and fifth day of treatment). This should be considered in any patient with persistent fever after initiation of therapy. Such a drug reaction should be suspected if the fever becomes higher than it was prior to therapy and when other manifestations of hypersensitivity such as rash or eosinophilia appear.
Drugs used for treatment of TB are shown in the Table 5.16. A 6-month regimen for drug-susceptible TB with isoniazid (INH) and rifampicin and pyrazinamide for the first 2 months followed by INH and rifampicin for the remaining 4 months is recommended. This regimen cures 99% of cases. If drug resistance is possible, initial treatment should include ethambutol, streptomycin, amikacin or ciprofloxacin. Shorter regimes using four drugs in the initial phase are increasingly being adopted. After commencing anti-TB therapy, fever usually subsides within 1 week and occasionally within 2 weeks of commencing medications. Adverse reactions to drugs include hepatotoxicity (due to INH and rifampicin) and fever mainly linked to pyrazinamide.
Malaria
Malaria is caused by a protozoan of the genus Plasmodium transmitted by Anopheles mosquitoes. The four species that commonly infect man are P. malariae (benign quartan malaria), P. vivax, P. ovale (benign tertian malaria) and P. falciparum (malignant tertian malaria). Whereas P. vivax invades mostly the youngest erythroblast and P. malariae invades primarily the older erythrocytes in both no more than 1–2% of erythrocytes are infected at a time. Plasmodium falciparum, on the other hand, invades all ages of erythrocytes indiscriminately, resulting in a very high infection rate and death. The number of malaria cases and deaths has decreased globally since 2000. In 2013 there were 584,000 deaths and 198 million malaria cases. Over 50% of childhood deaths in many parts of Africa are attributed to malaria [27].
Patients with P. falciparum infection have elevated tumour necrosis factor-alpha (TNF-α), soluble interleuin-2 (IL-2) receptors and natural killer cell activity but a decrease in the CD4:CD8 lymphocyte ratio. The level of TNF correlates with the severity and mortality rate in patients with this infection. Changes in the TNF also correlate with the rise and fall in temperature during P. vivax paroxysms.
Infected children present with fever, lethargy headache, cough anorexia, nausea, vomiting, diarrhoea, abdominal pain and dehydration. Physical examination reveals splenomegaly (detected in almost 100%) and commonly hepatomegaly. Nephrotic syndrome may occur with P. malariae infection. The presenting clinical signs of cerebral malaria are severe headache, irritability, delirium, coma, hyperpyrexia, convulsion and meningism.
Relationship between malaria and fever: There is a strong positive correlation between malaria and fever. Malaria is a major cause of fever, occurring in virtually 100% of cases. Out of 11,480 febrile children younger than 5 years of age from Nairobi, Kenya, 22% had malaria [28]. Classical periodicity of fever may not occur in children during the first few years of life, rather intermittent, continuous or remittent patterns may all occur. In endemic areas, malaria is often diagnosed and empirically treated based on the presence of fever alone.
A child with fever caused by malaria may present with:
A typical tertian paroxysm (P. vivax and P. ovale) in a nonimmune child with shivering and rigor (usually in the afternoon or evening), lasting 1–2 h. The skin is cold and pale. The next stage is marked by high fever, up to 41 °C, lasting 2–4 h. The skin is dry and warm and the patient feels hot and has usually headache. The last 2–4 h are characterized by a drop in body temperature to normal with sweating. In tertian infection, the paroxysm recurs at 48 h intervals (Figs. 5.3 and 5.4), while in quartan infection the paroxysm recurs at 72 h intervals (Fig. 5.4). Early in the infection with P. falciparum the fever may be irregular or continuous. A significant correlation exists between heavy parasitaemia of 2% or greater and high-grade temperature.
Febrile seizure (FS). Malaria is the most common cause of FS worldwide.
Blackwater fever, a state of acute intravascular haemolysis accompanied by haemoglobulinuria, as a complication of P. falciparum.
Human parvovirus B19 infection, adding to the severity of anaemia. The virus is highly erythrotropic, infecting erythroid progenitor cells.
Complication of malaria, e.g. pneumonia or anaemia.
PUO, with fever as the only sign of malaria without anaemia or splenomegaly.
Recurrent fever months after treatment of falciparum malaria due to relapse.
Fig. 5.4.
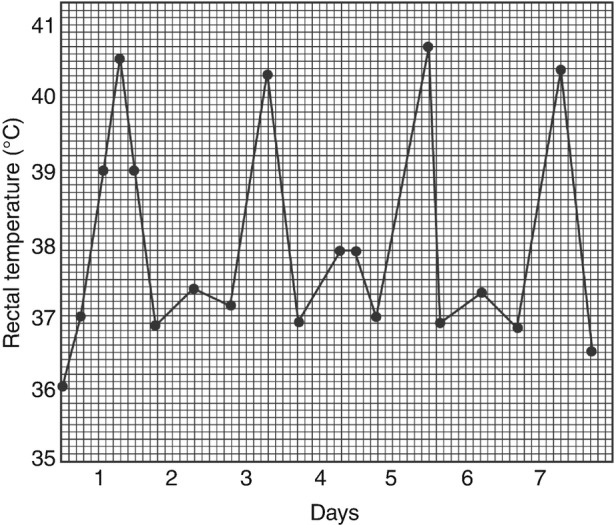
Febrile cycle seen in tertian malaria caused by Plasmodium vivax infection
Diagnosis is easy when children present with typical paroxysms of fever. Definite diagnosis is made by a Giemsa-stained blood smear (thick smear increases the yield). A rapid diagnostic tests (RDTs) can be obtained by utilizing ribosomal ribonucleic acid (rRNA) of the parasite. Laboratory findings include anaemia (Hb: 5–11 g/dL), leukopenia, thrombocytopenia, hyponatraemia and hypoglycaemia.
Therapy: Hospitalization for any child with suspected or confirmed malaria is always indicated to assess severity and extent of severity. Paracetamol is commonly used for fever management. Paracetamol has been reported to prolong parasitaemia although the evidence for that was found to be insufficient. Chemoprophylaxis and therapy are shown in the Table 5.17. Chloroquine remains the treatment for choice for benign malarias while quinine is given for falciparum malaria. Children receiving iron therapy may be at increased risk of fever associated with severe parasitaemia (see the section of anaemia Chap. 10.1007/978-3-319-92336-9_6).
Table 5.17.
Drugs used for prophylaxis and therapy of malariaa
| Dose | Adverse reaction | |
|---|---|---|
| Prophylaxis | ||
| Chloroquine | 5 mg base/kg/weekly | Retinal damage |
| Fansidar | 125–750 mg (according to the age) | Severe mucocutaneous reaction |
| Therapy | ||
| Chloroquine | 10 mg/kg; followed by 5 mg/kg in 6 h, then 5 mg/kg twice daily for 2 days | Gastrointestinal upset, visual disturbance, rash |
| Quinine | 25 mg/kg/day three times for 10–14 days | Tinnitus |
| Primaquine | 0.3 mg base/kg once daily for 14 days | Methaemoglobulinaemia, haemolytic anaemia (in G6PD) |
aTreatment of malaria varies considerably around the world and advice about antimalarial drugs will depend upon the location and expert advice
Brucellosis
Brucellosis is primarily a zoonotic infection caused by small, nonmotile, Gram-negative coccobacilli of the genus Brucella. There are four important species pathogenic to humans: B. melitensis (Malta fever, found primarily in goats and sheep), B. abortus (abortus fever, in cattle), B. suis (swine) and B. canis (dogs). The infection is transmitted to humans through direct contact with infected animals or their products and through consumption of infected milk, milk products or meat. More than half a million cases per year occur worldwide.
The clinical features of brucellosis depend largely upon the infected species of organism. Infection with B. melitensis produces more severe symptoms and signs than other species. Fever is usually present with nonspecific symptoms of migratory arthralgia, myalgia, anorexia and sweats at night. Hepatosplenomegaly and cervical adenopathy are common findings.
Fever manifests in almost every patient (90–100% of cases) as:
Undulant fever rising insidiously over the course of 1–3 weeks with temperature rising to reach 39–40 °C then falling like a wave (Fig. 5.5) to remain normal for 10 days before rising again.
A remittent pattern, suddenly with chills, rising to a peak of 40.5 °C in the afternoon and falling to a normal level at night.
Pyrexia of unknown origin (PUO), particularly in endemic areas.
Fig. 5.5.

Febrile cycle seen in quartan malaria caused by Plasmodium malariae infection
Complications include spondylitis, osteomyelitis, granulomatous reaction of the eye, meningitis or meningoencephalitis. Brucella endocarditis is rare and may be responsible for the majority of death due to the disease.
Laboratory findings include anaemia, leucopenia, lymphopenia and raised liver enzymes. The diagnosis is established by positive culture of brucella organisms from blood or bone marrow aspirate or positive serological tests (agglutination titre of >1:80), IgM by ELISA or PCR.
Therapy: The best option is a combination of doxycycline and rifampicin for 3 weeks with or without gentamicin. Rifampicin has also been used successfully in combination with streptomycin in the treatment of Brucella endocarditis.
Lyme Disease
Borreliosis includes both relapsing fever and Lyme disease (LD). LD is a multisystem inflammatory disease caused by the spirochete Borrelia burgdorferi. It is transmitted by the deer tick (Ixodes dammini). LD is the most common vector-borne illness in the USA. B. burgdorferi is a potent inducer of IL-1 from peripheral blood mononuclear cells. Lyme disease has been divided into three stages:
The first one consists of a flu-like illness with a characteristic annular skin rash (Erythema migrans), which develops at the site of the tick bite in approximately in two thirds of patients. Antibiotics at this stage may prevent subsequent stages.
The second stage follows 2–12 weeks after the tick bite and is characterized by disseminated infection causing aseptic meningitis and cranial neuritis (most commonly presenting as facial palsy) and carditis (most commonly presenting as atrioventricular block or myocarditis).
The third stage is characterized by oligoarticular arthritis and acrodermatitis chronica atrophicans from 6 weeks to 2 years after the tick bite in 50–80% of patients.
Macrophages and B cells produce both pro-inflammatory and anti-inflammatory cytokines, particularly IL-1 and IL-6. Interleukin-1 and IL-1 receptor antagonist, both produced by monocytes and macrophages, may influence the course of arthritis. High concentration of IL-1 receptor antagonist and low concentration of IL-1 may indicate rapid resolution of arthritis, whereas the reverse pattern of cytokine concentration may indicate recovery.
Fever is often an early sign of the disease, appearing within 18 h of the bite. It occurs with other flu-like manifestations. Fever is usually intermittent and low-grade and has been reported in about 50% of children. Fever, however, can be as high as 40 °C and persistent, which can cause pyrexia of unknown origin (PUO). Approximately 1:80 patients present with PUO defined as fever that lasts at least a week during which fever is present in most days and the diagnosis is not clear after 1 week of intense investigation (Chap. 10.1007/978-3-319-92336-9_1). There is no pattern of fever in LD but it can be recurrent.
Diagnosis of LD depends on characteristic clinical features, in particular the appearance of erythema migrans. PCR may detect B. burgdorferi. Specific IgM antibodies against B. burgdorferi appear 3–4 weeks after the infection and peak after 6–8 weeks. Specific IgG antibodies usually become detectable in the second month of the illness. Both IgM and IgG can be detected by ELISA test.
Therapy: Uncomplicated cases of LD are treated with oral penicillin or amoxicillin divided into three doses for 21 days. For children older than 12 years, doxycycline twice daily for 21 days or tetracycline for the same duration is effective. For arthritis, antibiotic therapy should continue for 4 weeks and often includes a third-generation cephalosporin. For meningitis, penicillin G/cephalosporin is given IV for 2–3 weeks.
Leptospirosis
Leptospirosis is a zoonosis, which is probably the most common zoonosis worldwide. It is caused by spirochaetal bacteria of the genus Leptospira. Human infections occur through contact with water (e.g. flood water) or soil contaminated with infected animal’s urine. The incubation period is usually between 6 and 12 days. The common presentation is characteristically biphasic:
The primary phase manifests as an influenza-like illness lasting 5–7 days with abrupt onset of chills and fever 39.5–40.5 °C lasting 3–7 days. This phase reflects the presence of leptospiraemia (the septicaemic phase). Fever lasts longer than 5 days in two thirds of cases.
In the second phase, lasting 4–30 days (the immune phase), specific antibodies begin to appear and fever starts to subside. Leptospira are excreted in the urine. Fever is not prominent in this phase but may occur as a result of aseptic meningitis mediated by antigen-antibody reaction.
A small proportion of patients develop a severe and potentially fatal form (Weil’s disease), and patients present with jaundice, haemorrhage, anaemia and multi-organ failure (e.g. acute renal failure). Cases with PUO may occur in about 10% of cases.
Concentrations of various cytokines, such as IL-1β, IL-2, IL-8, IL-10 and TNF-ɑ, are significantly higher in severe and fatal cases compared to those in mild cases.
Laboratory findings include leukocytosis, hyperbilirubinaemia and intravascular haemolysis. Leptospira may be cultured from the blood (dark field microscopy), urine and CSF. IgM-Elisa test and PCR confirm the diagnosis.
Doxycycline and penicillin are the treatment of choice. Initiation of antibiotic therapy may precipitate a febrile inflammatory reaction known as Jarisch-Herxheimer reaction, which was originally described in patients treated for syphilis.
Leishmaniasis
Of the three clinical forms of leishmaniasis, cutaneous, mucocutaneous and visceral, only the latter form is associated with febrile episodes. The infection is defined as a person from an endemic area with fever for more than 2 weeks and splenomegaly and confirmed by either rapid diagnostic test (based on rk39 antigen) or bone marrow or splenic aspirate. The disease is transmitted to humans by a bite of infected sand fly Phlebotomus. It is the second most fatal parasitic disease after malaria. Coinfection with HIV is not uncommon.
The visceral form (also known as kala-azar, black fever) is caused by the protozoan Leishmania donovani. The infection produces the following clinical course:
Following the invasion of the blood stream, the organisms settle in the reticuloendothelial system and viscera, where they multiply within the cell’s cytoplasm despite being engulfed by mononuclear cells. Eventually, the mononuclear cells rupture and release many organisms, which are subsequently engulfed by other phagocytic cells.
A few months after the initial bite, the patients develop symptoms manifested by varying degree and patterns of fever (see below), emaciation, massive hepatosplenomegaly, lymphadenopathy, profound weakness and pancytopenia. The weakness is mainly caused by anaemia and chronic infection. The pancytopenia is caused by a combination of invading the bone marrow by Leishmania, hypersplenism and autoimmune process. Thrombocytopenia may be severe enough to produce bleeding. Leukopenia causes secondary bacterial infections, such as pneumonia.
Death occurs within 1–2 years in 80–90% of untreated patients.
All infected children have fever (Table 5.18), which manifests in protean patterns:
In young children, it increases gradually to a peak within 2 weeks from the onset (40–41.1 °C), becoming then intermittent (temperature returning to a normal level within the same day) or continuous (fever fluctuates by less than 1 °C) and resolving usually by lysis.
In older children, with more chronic presentation, fever may be continuous initially but is usually low grade.
Classically fever is double quotidian (two spikes within 24-h or a 12-h cycle).
PUO may occur with a duration between 1 and 18 months, with a median duration of fever of 4–5 weeks.
Table 5.18.
symptoms and signs of kala-azar in 100 children, admitted to Baghdad’s University Hospital
| Clinical findings % | |
|---|---|
| Fever | 100 |
| Splenomegaly | 96 |
| Hepatomegaly | 91 |
| Abdominal distention | 89 |
| Respiratory distress | 50 |
| Diarrhoea | 13 |
| Jaundice | 3 |
| Associated septicaemia | 2 |
| Haemorrhage | 1 |
Pathogenesis and fever are related to the interaction of T-helper cells and various cytokines. INF-gamma, IL-6 and IL-4 are involved during active disease. Dysfunctions of macrophages and T cells lead to severe immunosuppression.
Treatment is presently with miltefosine, orally 2.5 mg/kg/day for 4 weeks. Pentavalent antimony compounds and liposomal amphotericin B are also used. Defervescence usually occurs after a median of 6 days of treatment.
Fever and Malnutrition
It has been estimated that 10.6 million children are still dying yearly, mostly due to pneumonia, diarrhoea, neonatal causes and malaria in sub-Saharan Africa. Malnutrition was an underlying cause in over 50% of the deaths. These children are particularly susceptible to measles and tuberculosis.
Protein-calorie malnutrition (PCM) has been divided into severe (kwashiorkor, marasmus and intermediate cases), moderate severe (nutritional, dwarfing or stunting and wasting) and early (clinically detectable only by anthropometric measurement). In developing countries, the severe form of malnutrition is common as a result of several factors, including severe dietary imbalance. Marasmus results from deficiency of all nutrients, whereas kwashiorkor is due primarily to protein deficiency. In developed countries, PCM may result from debilitating chronic diseases.
Patients with PCM are susceptible to infection and fever for a variety of reasons:
Delayed mononuclear cell release from the bone marrow.
Impaired T-cell-mediated immunity, deficiency in circulating levels of the complement system and interferon.
Reduced secretary IgA (while B-cells and circulating immunoglobulins are normal).
Impaired acute-phase response.
Fever in a malnourished child is usually the result of infection. Respiratory infections, e.g. pneumonia, TB and intestinal infection, are most common. In severe malnutrition, fever may be absent, and instead hypothermia may occur in response to infection signifying a poor prognosis for survival.
Malnourished children who are febrile are at increased risk of paracetamol-induced hepatotoxicity. Reduction in calorie or protein intake in association with multiple doses of paracetamol may have profound effects on sulphate and glucuronide. The combination of malnutrition and HIV is particularly devastating.
References
Acute Upper Airway Obstruction
- 1.Davis HW, Carter JC, Galvis AG, et al. Acute upper airway obstruction: croup and epiglottitis. Pediatr Clin N Am. 1981;28:859–880. doi: 10.1016/S0031-3955(16)34073-1. [DOI] [PubMed] [Google Scholar]
Bronchiolitis & Asthma
- 2.El-Radhi AS, Barry W, Patel S. Association of fever and severe clinical course in bronchiolitis. Arch Dis Child. 1999;81:231–234. doi: 10.1136/adc.81.3.231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.El-Radhi AS Patel S. The clinical course of childhood asthma in association with fever (unpublished). [DOI] [PubMed]
- 4.El-Radhi AS, Hogg CL, Bungre JK, et al. Effect of oral glucocorticoid treatment on serum inflammatory markers in acute asthma. Arch Dis Child. 2000;83:158–162. doi: 10.1136/adc.83.2.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pneumonia
- 5.McCarthy PL, Tomasso L, Dolan TF. Predicting fever response of children with pneumonia treated with antibiotics. Clin Pediatr. 1980;19:753–760. doi: 10.1177/000992288001901108. [DOI] [PubMed] [Google Scholar]
Gastroenteritis
- 6.Kosek M, Bern C, Guerrant RL. The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000. Bull World Health Organ. 2003;81(3):197–204. [PMC free article] [PubMed] [Google Scholar]
- 7.El-Radhi AS, Rostila T, Vesikari T. Association of high fever and short bacterial excretion after salmonellosis. Arch Dis Child. 1992;67:531–532. doi: 10.1136/adc.67.4.531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ryan CA, Hargrett –BNT, Blake PA. Salmonella typhi infections in the united States1975-1984: increasing role of foreign travel. Rev Infect Dis. 1989;11(1):1–8. doi: 10.1093/clinids/11.1.1. [DOI] [PubMed] [Google Scholar]
- 9.El-Radhi AS, Newcombe T, Ghalli A. Effect of pyrexia on Shigella and salmonella gastroenteritis (unpublished).
- 10.Thoren A, Wolde-Mariam T, Stintzing G, et al. Antibiotics in the treatment of gastroenteritis caused by enteropathogenic Escherichia coli. J Infect Dis. 1980;141:27–31. doi: 10.1093/infdis/141.1.27. [DOI] [PubMed] [Google Scholar]
- 11.Mohammed HF, Hassan MK, Bakir SS. Campylobacter jejuni gastroenteritis in children in Basrah, Iraq. Med J Basrah Univ. 2004;22(1&2):1–5. [Google Scholar]
- 12.Marks MI, Pai CH, Lafleur L, et al. Yersinia enterocolitica: a prospective study of clinical, bacteriologic, and epidemiologic features. J Pediatr. 1980;96:26–31. doi: 10.1016/S0022-3476(80)80318-0. [DOI] [PubMed] [Google Scholar]
- 13.Cook SM, Glass RI, Le Baron CW. Global seasonality of Rota virus infection. Bull World Health Organ. 1990;68:171–177. [PMC free article] [PubMed] [Google Scholar]
- 14.Ruuska T, Vesikari T. Rotavirus disease in Finnish children: use of numerical scores for clinical severity of diarrhoeal episodes. Scand J Infect Dis. 1990;22:259–267. doi: 10.3109/00365549009027046. [DOI] [PubMed] [Google Scholar]
- 15.Brandt CD, Rodriguez WJ, Arrobio JO, et al. Adenovirus and pediatric gastroenteritis. J Infect Dis. 1985;151:437–443. doi: 10.1093/infdis/151.3.437. [DOI] [PubMed] [Google Scholar]
- 16.Grajden M, Brown M, Petrasek A, et al. Clinical features of adenovirus gastroenteritis: a review of 127 cases. Pediatr Infect Dis J. 1990;9:636–641. [PubMed] [Google Scholar]
HIV
- 17.Ruiz-Contreras J, De Jose MI, Ciria L, Mellado MJ, Ramos JT, Clemente J, et al. Fever of unknown origin in HIV infected children. Int Conf AIDS 1998; 12: 44. (abstract no. 12165).
Infection of the CNS
- 18.Holt DE, Halket S, Jde L, et al. Neonatal meningitis in England and Wales: 10 years on. Arch Dis Child Fetal Neonatal Ed. 2001;84:F85–F89. doi: 10.1136/fn.84.2.F85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wong VK, Hitchcock W, Mason WH. Meningococcal infection in children: a review of 100 cases. Pediatr Infect Dis J. 1989;8:224–227. doi: 10.1097/00006454-198909000-00015. [DOI] [PubMed] [Google Scholar]
- 20.Lin TY, Nelson JD, McCracken GH. Fever during treatment for bacterial meningitis. Pediatr Infect Dis. 1984;3:319–322. doi: 10.1097/00006454-198407000-00009. [DOI] [PubMed] [Google Scholar]
- 21.Rantala H, Uhari N. Occurrence of childhood encephalitis: a population-based study. Pediatr Infect Dis. 1989;8:426–430. doi: 10.1097/00006454-198907000-00004. [DOI] [PubMed] [Google Scholar]
- 22.Koskiniemi M, Vaheri A. Acute encephalitis of viral origin. Scand J Infect Dis. 1982;14:181–187. doi: 10.3109/inf.1982.14.issue-3.05. [DOI] [PubMed] [Google Scholar]
- 23.Saez-Liorens XJ, Umana MA, Odio CM, et al. Brian abscess in infants and children. Pediatr Infect Dis. 1989;8:449–458. doi: 10.1097/00006454-198907000-00009. [DOI] [PubMed] [Google Scholar]
Osteomyelitis
- 24.Ceroni D, Requsci M, Pazos J, et al. Acute bone and joint infection in children: how much attention should be paid to persistent fever during IV antibiotic therapy. Rev Chir Orthop Reparatrice Appar Mot. 2003;89:250–256. [PubMed] [Google Scholar]
Viral Exanthems
Tropical Diseases
- 26.Lamb GS, Starke JR. Tuberculosis in infants and children. Microbiol Spectr. 2017;5 (2). 10.1128/microbiolspec.TNM17-0037-2016. [DOI] [PMC free article] [PubMed]
- 27.Hoffman SL, Vetemans J, Richie TL, et al. The march toward malaria vaccines. Am J Prev Med. 2015;49(6 Suppl 4):S319–S333. doi: 10.1016/j.amepre.2015.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Njuguna HN, Montgomery JM, Cosmas L, et al. Malaria parasitaemia among febrile patients seeking clinical care at an outpatient health facility in an urban informal settlement area in Nairobi, Kenya. Am J Trop Med Hyg. 2016;94(1):122–112. doi: 10.4269/ajtmh.15-0293. [DOI] [PMC free article] [PubMed] [Google Scholar]