

Abstract
In healthcare settings microbial contaminated surfaces play an important role in indirect transmission of infection. Especially surfaces close to the patients’ environment may be touched at high frequencies, allowing transmission from animated sources to others via contaminated inanimate surfaces.
Therefore, the knowledge on the survival of bacteria, fungi, viruses and protozoa on surfaces, and hence, in a broader sense, in the human environment, is important for implementing tactics for prevention of Healthcare-acquired Infections (HAI). This chapter will elaborate the role of surfaces in the transmission of pathogens. Particular emphasis is laid on the current knowledge of the survival time and conditions favouring survival of the pathogens. Finally, mechanisms of transmission from inanimate surfaces to patients are highlighted.
Within the multi-barrier strategy of the prevention of HAI, environmental disinfection policies should be based on risk assessments for surfaces with different risks for cross contamination such as high- and low-touched surfaces with appropriate standards for adequate disinfection measures under consideration of the persistence and infectious dose of the pathogens. As a result, surface disinfection is indicated in the following situations:
Frequently touched surfaces adjacent to patients
Surfaces with assumed or visible contamination
Terminal disinfection in rooms or areas where infected or colonized patients with easily transferable nosocomial pathogens are cared for, and
in outbreak situations.
Furthermore, the knowledge of the persistence of pathogens will also support ensuring the biosafety in microbiological and biomedical laboratories, food-handling settings, and for hygienic behaviour in the everyday life to prevent transmission of infectious diseases.
Keywords: Persistence, Bacteria, Fungi, Viruses, Protozoa transmission mechanisms, Surface disinfection
Introduction
Microorganisms may be transmitted from animated sources to inanimate environmental sources, which may become secondary reservoirs if they meet the needs of transmitted pathogens to survive and to multiply. In healthcare settings, however, contaminated surfaces, which may not always be optimal for microbial survival and multiplication, still may play a role in the chain of infection, since surfaces close to the patients’ environment may be touched at high frequencies, allowing transmission from animated sources to others via contaminated inanimate surfaces.
Because of this, the knowledge on the survival of bacteria, fungi, viruses and protozoa on surfaces, and hence, in a broader sense, in the human environment, is important for planning and implementing tactics for prevention of Healthcare-acquired Infections (HAI). Furthermore, such knowledge will also assist ensuring the biosafety in microbiological and biomedical laboratories, food-handling settings, and for hygienic behaviour in the everyday life to prevent transmission of infectious diseases.
One example of microorganisms with relatively short ability of persisting in the environment is the severe acute respiratory syndrome (SARS) coronavirus (CoV), which became pandemic within months in China in 2002. This virus retains infectivity on different substrates up to 9 days, as compared to the influenza virus, which demonstrates a relatively long persistence in the environment up to 4 weeks [112]. Both viruses are airborne transmitted infectious agents, however, they may also be transmitted via hand-surface contacts, supporting the relevance of hand hygiene and personal protection against infection.
Because of a number of microorganisms’ ability to persist and survive for long-term periods on surfaces, particularly in healthcare settings, the usage of antimicrobially impregnated surfaces is increasingly discussed [82]. However, because of the required long contact times of microorganisms on antimicrobial surfaces [64, 65, 25, 45], such technologies may be useful for surfaces with low frequency of hand contacts.
The Role of Surfaces in the Transmission of Pathogenic Microorganisms Causing Healthcare-Acquired Infections (HAI)
In healthcare settings, bacteria, bacterial spores, viruses and yeasts are mainly transmitted from infected and/or colonized patients, but also from staff, and in some situations from visitors to the inanimate hospital environment, particularly to areas adjacent to patients and frequently touched surfaces by hands (“high-touch surfaces”). Potential pathogenic microbial flora of the respiratory tract and of the vestibulum nasi, such as methicillin- sensible (MSSA) or resistant Staphylococcus aureus (MRSA), is correlated with a higher risk of contamination of surrounding surfaces through direct or indirect contact with hands [81]. Intestinal infections caused i.e. by Clostridium difficile and Norovirus, or enteral colonization with nosocomial pathogens such as vancomycin-resistant enterococci (VRE) may also be associated with a risk of widespread environmental contamination [30]. Compared with the large number of published literature on environmental contamination with MRSA, VRE, and C. difficile, there are relatively few published studies on environmental contamination by Gram-negative bacteria [64, 65]. Aside of a possible publication bias in the past, one reason for this is the different ability of Gram-positive and Gram-negative bacteria to survive in the inanimate environment.
The level of microbial bio-burden on surface in healthcare settings is low compared to the numbers on patients’ skin or in faeces. However, even at low particle numbers there is a risk of transmission (Table 2.1). In immuno-compromised patients, the required numbers of microorganisms for causing infectious diseases is even lower, increasing the risk of HAI in these populations. Inanimate surfaces have been described as source for HAI-outbreaks. Hayden et al. [49] demonstrated that touching the environment contaminated with relatively low pathogen concentrations in a room occupied by a patient colonized with VRE is associated with approximately the same risk of VRE acquisition on hands as touching an affected patient directly. Evidence of the importance of environmental transmission is further provided by studies showing an increased risk of infection in patients admitted to the same rooms previously occupied by other infected/colonised cases. This has been shown for C. difficile [101], VRE and MRSA ([54, 55], and also own observations). Environmental Norovirus contamination has been repeatedly found to be correlated with continuing outbreaks [128], although the significance of this pathway has not been fully elucidated.
Table 2.1.
Infectious doses for selected pathogens
| Infectious dose | Organisms | Reference |
|---|---|---|
| (1)-10–100 viable particles | Norovirus, Rotavirus, EHEC, ETEC, C. difficile, Enterococci incl. VRE | Ward et al. [122], Paton and Paton [88], Pang et al. [85], Lawley et al. [68], Porter et al. [92], Yezli and Otter [130], Robine et al. [97] |
| ≥1 viable particle in water | Oocysts of cryptosporidia | Chappell et al. [17] |
| >105 viable particles | Salmonella enteritidis | Craven et al. [24] |
The importance of surface contamination is also shown by reduction in the rate of HAI when effective measures of environmental disinfection are implemented [50, 10, 26]. A recent observational study showed a significant reduction in C. difficile infection rates following the introduction of sporicidal wipes in an environmental cleaning regimen in an acute London trust [16]. However, not all studies have shown a direct link between surface disinfection and reduction in infection rates, probably because of the complex interactions and transmission routes in the clinical practice.
Yet, in summary it is undisputed that contaminated surfaces may contribute to the transmission of pathogens and may thus pose a critical element in the chain of transmission of microorganisms [41].
Persistence of Microorganisms on Inanimate Surfaces
The risk for transmission of HAI depends of the persistence of nosocomial pathogens on surfaces. The longer a microorganism may persist on a surface, the longer the contaminated surface may be a source of transmission and thus endanger a susceptible patient or healthcare worker of becoming the target of infection. In order to estimate the risk of cross contamination, Kramer et al. [64, 65] have published a systematic review on persistence of pathogens on surfaces. The following findings are based on this review; however, knowledge on persistence of microorganisms on inanimate surfaces is now expanded by additional findings published after 2005/2006.
Persistence of Bacteria
In most reports, persistence was studied on dry surfaces using artificial contamination of a standardized type of surface in a laboratory. Bacteria were prepared in broth, water or saline.
Most Gram-positive bacteria, such as Enterococcus spp. including VRE, S. aureus including MRSA, or Streptococcus pyogenes survive for months on dry surfaces (Table 2.2). In general, there is no observable difference in survival between multi-resistant and susceptible strains of S. aureus and Enterococcus spp. [78]. Only in one study [118] a difference of survival time between antibiotic resistant and susceptible bacteria was suggested, yet, the susceptible strains demonstrated only a non-significant shorter survival time on surfaces. The factors why the same bacteria may persist more or less on a surface (i.e. from hours to days as detailed in Table 2.2) will be discussed later in Sect. 2.3.5.
Table 2.2.
Published data on survival of nosocomial and community acquired pathogens on various inanimate surfaces
| Organism | Range of survival (environment) | Reference |
|---|---|---|
| Acinetobacter spp. | 3 days to 1 year (in-vitro) | Wagenvoort and Joosten [117], Espinal et al. [36]a |
| 36 days within biofilm vs. 15 days for non-biofilm-forming strains | ||
| Bordetella pertussis | 3 to >10 days; in pernasal swabs: >4 days | Hunter [57], Walther and Ewald [121]a |
| Campylobacter jejuni | >6 days, in water >60 days | González and Hänninen [44]a |
| Clostridium difficile spores | 5 months | Weber et al. [123]a |
| C. difficile, vegetative form | 15 min (dry surface) | |
| 6 h (moist surface) | ||
| Chlamydia pneumoniae | ≤96 h | Fukumoto et al. [40], Haider et al. [51], Matsuo et al. [70]a |
| C. trachomatis | <1 week | |
| Chlamydia psittaci | 15 days to months (environment) | Wendel [125]a |
| Corynebacterium diphtheriae | 7 days to 6 months | Walther and Ewald [121]a |
| Corynebacterium pseudotuberculosis | 1–8 days, up to several weeks (environment) | Yeruham et al. [129]a, Dorella et al. [31] |
| Enterococcus spp. including VRE | 5 days up to 30 months | Robine et al. [97], Wagenvoort et al. [116]a |
| Escherichia coli | 1.5 h to 16 months | Guan and Holley [46], Erickson et al. [35], Chauret [19]a, Duffitt et al. [33] |
| E. coli O157:H7 | 27 days on spinach leaves, 179 days in soil, 98 days in water | |
| Haemophilus influenzae | 12 days | a |
| Helicobacter pylori | ≤90 min; in water: 2–30 days | West et al. [124], Percival and Thomas [89]a |
| Klebsiella spp. | 2 h to >30 months, ≤144 h in detergent solution | Beadle and Verran [6]a |
| Listeria spp. | 1 day–months, 141 days in water | Budzińska et al. [13]a |
| Mycobacterium bovis | >2 months | a |
| Mycobacterium tuberculosis | 1 day up to 4 months | Walther and Ewald [121]a |
| Neisseria gonorrhoeae | 1–3 days | a |
| Neisseria meningitidis | 72 h | Tzeng et al. [110]a |
| Parachlamydia acanthamoebae | <4 weeks, in presence of blood <7 weeks | Fukumoto et al. [40]a |
| Proteus vulgaris | 1–2 days | a |
| Pseudomonas aeruginosa | 6 h up to 16 months; on dry floor: 5 weeks; in aerosol: few hours | Clifton et al. [21]a |
| Salmonella typhi | 6 h up to 4 weeks | a |
| Salmonella typhimurium | 10 days up to 4.2 years | a |
| Salmonella spp. | 1 day | a |
| non typhoid Salmonella spp. | 336 days | Morita et al. [76]a |
| Salmonella enteritidis (broiler farms) | 1 year | Davies and Wray [27]a |
| Salmonella enteritica sv. Tennessie | 30 days (dried in desiccated milk powder) | Aviles et al. [1]a |
| Serratia marcescens | 3 days up to 2 months; on dry floor: 5 weeks | a |
| Shigella spp. | 2 days up to 5 months | Ghosh and Sehgal [42]a |
| 3–11 days in water | ||
| Staphylococcus aureus including MRSA and MSSA | 7 days up to 1 year (in-vitro) | Oie and Kamiya [81], Wagenvoort and Penders [118], Huang et al. [54, 55], Noyce et al. [80], Tolba et al. [108], Petti et al. [90]a |
| 9–12 days (plastic surfaces) | ||
| 72 h (stainless steel) | ||
| 6 h (copper) | ||
| ≤28 days (dry mops) | ||
| ≤14 days (in water) | ||
| Streptococcus pneumoniae | 1 day up to 30 month | Walsh and Camilli [120]a |
| Streptococcus pyogenes | 3 days up to 6.5 months | Wagenvoort et al. [119]a |
| Vibrio cholerae | 1–7 days | a |
| Yersinia enterocolitica | Up to 64 weeks (in water) | Guan and Holley [46]a |
| Yersinia pestis | Up to 5 days | Rose et al. [98]a |
Many Gram-negative species, such as Acinetobacter spp., Escherichia coli, Klebsiella spp., Pseudomonas aeruginosa, Serratia marcescens, or Shigella spp. can survive on inanimate surfaces even for months (Table 2.2). These species are found among the most frequent isolates from patients with HAI [64, 65]. However, a few others Gram-negative bacteria, such as Bordetella pertussis, Haemophilus influenzae, Proteus vulgaris, or Vibrio cholera persist only for days (Table 2.2).
Mycobacteria, including Mycobacterium tuberculosis, and spore-forming bacteria, such as C. difficile, can survive for many months on surfaces (Table 2.2).
Because paper still is omnipresent in healthcare settings worldwide today, Hübner et al. [56] have analysed the persistence of various Gram-positive and Gram-negative bacteria including E. coli, S. aureus, P. aeruginosa, and Enterococcus hirae on office paper after contamination with standardised inocula of bacterial suspensions in the range of 2.8 × 107 cfu/mL. Opposite to E. coli, all other organisms were more stabile at room conditions and were reduced on paper only by 3 log10 after 7 days, whereas E. coli was reduced by 5 log10 within 24 h. Furthermore, the transmissibility of bacteria from hands to paper and back could be demonstrated for all bacteria strains. Similar investigations showed that paper money notes could harbour and transmit pathogens [62, 111, 115].
Persistence of Viruses
In order to estimate the persistence of viruses on inanimate surfaces, usually cell culture media are prepared [64, 65]. Most viruses from the respiratory tract such as Corona-, Coxsackie-, or Influenza virus, SARS, or rhinovirus can persist on surfaces only for a few days [18]. Herpes viruses such as Cytomegalie virus or Herpes simplex virus type 1 and 2 have been shown to persist from only a few hours up to 7 days.
Viruses from the gastrointestinal tract, such as Astrovirus, Hepatitis A virus, Polio- and Rotavirus persist significantly longer for approximately 2 months. Blood-borne viruses, such as Hepatitis B virus or Human Immunodeficiency virus can persist for more than 1 week (Table 2.3).
Table 2.3.
Survival of clinically relevant viruses on dry inanimate surfaces
| Organisms | Range of survival (environment) | Reference |
|---|---|---|
| Adenovirus | <6 h up to 3 months (type dependent), ≤301 days (in water) | Hara et al. [48], Rigotto et al. [95]a |
| Astrovirus | 7–90 days | a |
| Avian metapneumonovirus | ~48 h up to 6 days | Tiwari et al. [107]a |
| SARS Coronavirus | <5 min up to 24 h (on paper) | Lai et al. [66], Rabenau et al. [93], Guionie et al. [47] |
| 5–28 days (at room temp.) | ||
| 28 days (at 4 °C) | ||
| Coxsackievirus | 7–10 days, up to >2 weeks | Wong et al. [127]a |
| Cytomegalovirus | 1–8 h | Faix [37], Stowell et al. [102]a |
| Echovirus | Up to 7 days | a |
| Hepatitis A virus | 2 h up to 60 days | a |
| Hepatitis B virus | ≥1 week | a |
| Human immunodeficiency virus | Up to 7 days, 7 days (in peritoneal dialysis effluent), 48 h (on peritoneal dialysis exchange and tubing), 4–8 weeks (on glass cover slides) | Van Bueren et al. [113], Farzadegan et al. [38]a |
| Herpes simplex virus, Type 1 & 2 | <2 h up to 8 weeks | Larson and Bryson [67], Bardell [2], Rabenau et al. [93]a |
| Influenza virus | 1–28 days (strain dependent) | Edward and Derrick [34], Walther and Ewald [121], Tiwari et al. [107]a, Thomas et al. [106] |
| 1–3 days (on banknotes), up to 8 days (admixed in mucous) | ||
| Marburg virus (strain Popp) | 4–5 days | Belanov et al. [7]a |
| Para-influenza virus | 10 h | Brady et al. [11]a |
| Norovirus, Feline calici virus (FCV), Murine norovirus (MNV) | 8 h up to 7 days, MNV > 40 days (in diapers and gauze) | Cannon et al. [14], Lee et al. [69]a |
| Papillomavirus 16 | ≤7 days | Hsueh [53]a |
| Papovavirus | 8 days | a |
| Parvovirus | >1 year | a |
| Poliovirus type 1 | 4 h to <8 days | a |
| Poliovirus type 2 | 1 day up to 8 weeks | a |
| Pseudorabies virus | ≥7 days, <1 h (in aerosol infectivity decreases by 50 % per hour) | Schoenbaum et al. [100] |
| Respiratory syncytial virus | up to 6 h | a |
| Rhinovirus | 2 h up to 7 days | a |
| Rotavirus | 30 min, 6–60 days | Keswick et al. [61]a |
| Vacciniavirus | 3 weeks up to >20 weeks | a |
Persistence of Fungi
Candida albicans, the most important nosocomial yeast, can survive up to 4 months on surfaces. Persistence of other yeasts was described to be similar (Torulopsis glabrata: 5 months) or shorter (Candida parapsilosis: 14 days) (Table 2.4). The survival of fungi in the environment, however, is strongly influenced by physical factors in nature, such as temperature and relative humidity (see Sect. 2.3.5). Moulds are ubiquitous in nature, thermo-tolerant, and can survive in house dust for long time. Indoor airborne mould measurements underline the survival for several months [4, 5].
Table 2.4.
Survival of clinically relevant fungi on dry inanimate surfaces
| Organisms | Range of survival (environment) | Reference |
|---|---|---|
| Aspergillus spp. | >30 days | Neely and Orloff [79]a |
| Candida albicans | 1 up to 120 days, 24 weeks (in soil-water mixture) | Neely and Orloff [79], Théraud et al. [105]a |
| Candida parapsilosis | >30 days | Neely and Orloff [79]a |
| Candida krusei | 11 days | |
| Cryptococcus spp. | 24 weeks (in soil-water mixture) | Théraud et al. [105]a |
| Fusarium spp. | >30 days | Neely and Orloff [79]a |
| Mucor spp. | >30 days | |
| Paecilomyces spp. | 11 days | |
| Torulopsis glabrata | 102–150 days | Kane et al. [59] |
Persistence of Other Pathogenic Microorganisms
Cryptosporidium spp. can induce water-born infection. Their oocysts can survive for months in surface water [96, 20, 75, 15], and up to 120 days in soil [60].
Acanthamoeba are one of the most common protozoa in soil, and frequently found in fresh water and other environmental habitats. An important habitat and vector for infection are hydrogel contact lenses, resulting in contact lens associated keratitis caused by acanthamoeba and fusarium [87], particularly since the contact lenses’ moist condition supports survival protozoa.
Factors Influencing the Survival of Microorganisms in the Environment
Relative Humidity (RH)
Generally, viruses with lipid envelops, such as most respiratory viruses including Influenza virus, Para-Influenza virus, Corona virus, Respiratory syncytial virus, Herpes simplex virus, Measles virus, Rubella virus, and Varicella zoster virus will tend to survive longer at lower relative humidity (20–30 % RH) [103]. However, Cytomegalie virus makes an exception, as it was more likely isolated from moist surfaces [102].
Conversely to enveloped viruses, non-lipid enveloped viruses such as Adenovirus, Enterovirus, and Rhinoviruses tend to survive longer at higher relative humidity (70–90 % RH) [103]. For Rotavirus and Poliovirus conflicting results were reported [64, 65].
S. aureus can persist longer at low humidity [74]. However, for Enterococcus faecalis the survival kinetic is decreased at 25 % RH compared to 0 % RH [97].
The survival of aerosolized Gram-negative bacteria including Pseudomonas spp., Enterobacter spp. and Klebsiella spp. improved at higher relative humidity and low temperature [103]. Studies on airborne Gram-negative bacteria such as S. marcescens, E. coli, Salmonella pullorum, Salmonella derby, and Proteus vulgaris showed decreased survival at intermediate (approx. 50–70 % RH) to high (approx. 70–90 % RH) relative humidity. For some airborne Gram-positive bacteria, such as Staphylococcus epidermidis, Streptococcus haemolyticus, Bacillus subtilis, and Streptococcus pneumoniae, their survival rate also decreased at intermediate relative humidity ranging at 50–70 % RH [103]. Gram-positive cocci were most prevalent in indoor air, followed by Gram-positive rods (e.g. Bacillus spp. and Actinomycetes spp.), Gram-negative rods and Gram-negative cocci [103]. The reason for this bacterial behaviour is the design of bacterial cell wall, which allows Gram-positive organisms to tolerate dry conditions better than Gram-negative organisms. Because of a lipid double-layer structure with a thin peptidoglycan (Murein) layer consisting of alternating residues of β-(1,4) N-acetylglucosamine and N-acetylmuramic acid, the later are not so well protected against physical stress and need higher RH in order to survive.
Temperature
The viral genome (viral DNA or RNA) is sensitive to the surrounding temperature. Indeed, temperature is an important factor influencing the survival of a number of viruses. Higher temperatures impact viral proteins and enzymes, as well as the viral genome. In general, DNA viruses are more stable than RNA viruses; yet, high temperature also will affect DNA integrity.
For most viruses, such as Astrovirus, Adenovirus, Poliovirus, Herpes simplex virus, and Hepatitis A virus, low temperature is associated with a longer persistence [64, 65]. Constant temperatures >24 °C appear universally to decrease airborne bacterial survival [103].
Biofilm
Biofilm is the predominate form of life for microorganisms in a nutrient-sufficient ecosystem. Adhesion triggers the expression of a sigma factor that depresses a large number of genes so that bacteria within the biofilm are at least 500 times more tolerable against antimicrobial agents [23] as well as against physical cold plasma [71, 72]. The reason for the unspecific increased tolerance is the production of extracellular substances like polysaccharides, proteins and DNA after attachment to surfaces. A precondition for biofilm formation is the presence of certain amounts of humidity. The biofilm matrix restrains water and nutrients and protects the microorganisms against environmental influences [28, 39]. Because of that, once formed biofilms are an important factor of persistence of microorganisms on surfaces in nature as well as in industrial or medical areas [22, 29, 12]. The persistence on inanimate surfaces is prolonged and depends of the environmental conditions, especially the humidity. Also on hospital surfaces biofilms were demonstrated on a number of objects and surfaces, such as sterile supply buckets, opaque plastic doors, venetian blind cords, and sink rubbers, and it was possible to cultivate viable bacteria. Currently, there is not enough research to elucidate whether presence or absence of biofilm affect the risk of transmission or possibility for cross-transmission. However, multi-drug resistant bacteria may not only be protected within biofilms, which may be the mechanism why they persist within the hospital environment [114], but may also exchange virulence factors among their own species or to other species present in biofilms as well [29, 43, 109].
Other Factors
A number of other factors may influence the survival of microorganisms on surfaces. Clearly, the material character of a surface itself may play in important role. However, inconsistent results are reported for the influence of type of materials on microbial survival. Some authors described that the type of material did not affect the persistence of Echovirus, Adenovirus, Para-Influenza virus, Rotavirus, Respiratory syncytial virus, Poliovirus, or Norovirus. Other investigators found that persistence was favoured on non-porous surfaces for Influenza virus on formica and gloves for Respiratory syncytial virus, and on hand pieces of telephones for Feline calicivirus [64, 65]. Other factors for a longer persistence of viruses include the presence of faecal suspension and a higher bio-inoculum [66, 64, 65]. Interestingly and by nature, Urease activity enhances the survival of Haemophilus influenzae at a reduced pH [77].
Limitations on the Knowledge of Microbial Survival on Inanimate Surfaces
Laboratory studies to determine the survival and persistence do not reflect the clinical situation, in which surfaces can be simultaneously contaminated with various nosocomial pathogens, different types of bodily and other fluids, secretions, and antimicrobial residues, i.e. from the last surfaces disinfection. However, little dispute exists that beside the hands of healthcare workers surfaces in the close vicinity of patients may play a key role for the transfer of nosocomial pathogens.
Mechanisms of Transmission from Inanimate Surfaces to Susceptible Patients and Consequences Thereof
The main route of transmission of HAI is via transiently contaminated hands of healthcare workers, but contaminated surfaces may serve as important vectors for cross transmission after hand contact as well (Fig. 2.1).
Fig. 2.1.
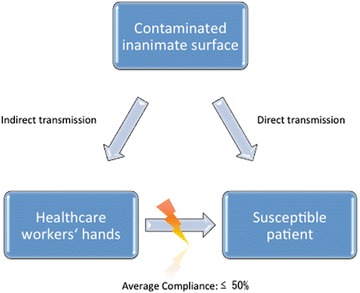
Transmission routes for nosocomial pathogens
A single hand contact with a contaminated surface results in a variable degree of pathogen transfer. Transmission from surfaces to hands was most successful with E. coli, Salmonella spp., S. aureus (all 100 %), C. albicans (90 %), Rhinovirus (61 %), Hepatitis A virus (22–33 %), and Rotavirus (16 %) [64, 65]. Other transfer rates were calculated for Echovirus, Poliovirus, and Rotavirus with 50 % transmissibility, and for Salmonella enteritidis, Shigella spp., and E. coli O157:H7 with 33 % [104]. Contaminated hands can transfer viruses to 5 more surfaces or 14 other subjects. Contaminated hands can also be the source of re-contamination of the surface, as demonstrated with Hepatitis A virus [64, 65].
Because of this, it is critical to note that healthcare workers’ compliance with hand hygiene varies between 13 % and 94 % with a median of less than 50 % [91]. Moreover hand hygiene is performed less frequently after contact with the environment than with the patient [94]. Both facts underline the necessity to perform additional surface decontamination procedures to interrupt the transmission of nosocomial pathogens. Due to the overwhelming evidence of low compliance of hand disinfection, the risk from contaminated surfaces cannot be overlooked and must not be down played by hospital administrations.
During outbreaks, the role of the patients’ environment is particularly evident, as suggested by observed evidence for Acinetobacter baumannii, C. difficile, MRSA, P. aeruginosa, VRE, Adenovirus, SARS virus, Rotavirus, and Norovirus [64, 65, 54, 55, 99, 9, 123, 83, 58]. The role of contaminated surfaces is also underlined by the observation that after environmental disinfection, significant decrease of transmissions and HAI have been shown, i.e. for C. difficile [73, 126], for VRE [50], for MRSA [32], for multidrug-resistant A. baumanii [84], for S. marcescens [3], and for other multidrug-resistant Gram-negative rods [86].
If performed correctly, also the burden of microbial airborne transmission can be significantly decreased by surface disinfection. This again may have an impact on healthcare organisations, resulting in i.e. higher clean room class of drug manufacturing areas [8] by elimination of critical bacterial and fungal contamination [63]. As consequence for the successful interruption of cross contamination and infections a multi-barrier approach is required with the key points of hand hygiene and surface disinfection, appropriate used of antisepsis, barrier nursing, and safe reprocessing of contaminated medical devices. Within such multi-barrier strategy, environmental disinfection policies should be based on risk assessments for surfaces with different risks for cross contamination such as high- and low-touched surfaces with appropriate standards for adequate disinfection measures. Generally, surface disinfection is indicated in the following situations:
Frequently touched surfaces adjacent to patients
Surfaces with assumed or visible contamination
Terminal disinfection in rooms or areas where infected or colonized patients with easily transferable nosocomial pathogens are cared for, and
in outbreak situations.
The purpose of preventive or targeted disinfection on inanimate surfaces is the killing or irreversible inactivation of pathogens to an extent which prevents subsequent infection transmission [41]. In order to ensure the success of environmental disinfection, education, training [52], and targeted microbiological control are important measures and have been shown to improve both, cleaning performance and infection prevention [50]. Increasingly, novel technologies are introduced, which may be used additionally to cleaning. Such technologies may include antimicrobial surfaces on basis of different antimicrobial compounds and are provided for hospital door handles, alarm knobs, curtains, and other objects with high frequencies of hand contact. However, such technologies must be used appropriately and as an adjunct measure to meaningful cleaning and disinfection processes.
Contributor Information
Axel Kramer, Email: kramer@uni-greifswald.de
Ojan Assadian, Email: ojan.assadian@meduniwien.ac.at.
References
- 1.Aviles B, Klotz C, Eifert J, Williams R, Ponder M. Biofilms promote survival and virulence of Salmonella enterica sv. Tennessee during prolonged dry storage and after passage through an in vitro digestion system. Int J Food Microbiol. 2013;162:252–259. doi: 10.1016/j.ijfoodmicro.2013.01.026. [DOI] [PubMed] [Google Scholar]
- 2.Bardell D. Survival of herpes simplex virus type 1 on some frequently touched objects in the home and public buildings. Microbios. 1990;63:145–150. [PubMed] [Google Scholar]
- 3.Bates CJ, Pearse R. Use of hydrogen peroxide vapour for environmental control during a Serratia outbreak in a neonatal intensive care unit. J Hosp Infect. 2005;61:364–366. doi: 10.1016/j.jhin.2005.05.003. [DOI] [PubMed] [Google Scholar]
- 4.Baudisch C, Assadian O, Kramer A. Concentration of the genera Aspergillus, Eurotium and Penicillium in 63-μm house dust fraction as a method to predict hidden moisture damage in homes. BMC Public Health. 2009;9:247. doi: 10.1186/1471-2458-9-247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Baudisch C, Assadian O, Kramer A. Evaluation of errors and limits of the 63-μm house-dust-fraction method, a surrogate to predict hidden moisture damage. BMC Res Notes. 2009;2:218. doi: 10.1186/1756-0500-2-218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Beadle IR, Verran J. The survival and growth of an environmental Klebsiella isolate in detergent solutions. J Appl Microbiol. 1999;87:764–769. doi: 10.1046/j.1365-2672.1999.00923.x. [DOI] [PubMed] [Google Scholar]
- 7.Belanov EF, Muntyanov VP, Kryuk VD, Sokolov AV, Bormotov NI, P’yankov OV. Survival of marburg virus on contaminated surfaces and in aerosol. Russian Progr Virol. 1996;1:47–50. [PubMed] [Google Scholar]
- 8.Below H, Ryll S, Empen K, Dornquast T, Felix S, Rosenau H, Kramer S, Kramer A (2010) Impact of surface disinfection and sterile draping of furniture on room air quality in a cardiac procedure room with a ventilation and air-conditioning system (extrusion airflow, cleanroom class 1b (DIN 1946-4). GMS Krankenhaushyg Interdiszip 2:Doc10 (20100921) [DOI] [PMC free article] [PubMed]
- 9.Boyce JM, Havill NL, Otter JA, Adams NM. Widespread environmental contamination associated with patients with diarrhea and methicillin-resistant Staphylococcus aureus colonization of the gastrointestinal tract. Infect Control Hosp Epidemiol. 2007;28:1142–1147. doi: 10.1086/520737. [DOI] [PubMed] [Google Scholar]
- 10.Boyce JM, Havill NL, Otter JA, McDonald LC, Adams NM, Cooper T, Thompson A, Wiggs L, Killgore G, Tauman A, Noble-Wang J. Impact of hydrogen peroxide vapor room decontamination on Clostridium difficile environmental contamination and transmission in a healthcare setting. Infect Control Hosp Epidemiol. 2008;29:723–729. doi: 10.1086/589906. [DOI] [PubMed] [Google Scholar]
- 11.Brady MT, Evans J, Cuartas J. Survival and disinfection of parainfluenza viruses on environmental surfaces. Am J Infect Control. 1990;18:18–23. doi: 10.1016/0196-6553(90)90206-8. [DOI] [PubMed] [Google Scholar]
- 12.Bryers JD. Medical biofilms. Biotechnol Bioeng. 2008;100:1–18. doi: 10.1002/bit.21838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Budzińska K, Wronsky G, Szejniuk B. Survival time of bacteria Listeria monocytogenes in water environment and sewage. Pol J Environ Stud. 2012;21:31–37. [Google Scholar]
- 14.Cannon JL, Papafragkou E, Park GW, Osborne J, Jaykus LA, Vinjé J. Surrogates for the study of norovirus stability and inactivation in the environment: a comparison of murine norovirus and feline calicivirus. J Food Prot. 2006;69:2761–2765. doi: 10.4315/0362-028x-69.11.2761. [DOI] [PubMed] [Google Scholar]
- 15.Carey CM, Lee H, Trevors JT. Biology, persistence and detection of Cryptosporidium parvum and Cryptosporidium hominis oocyst. Water Res. 2004;38:818–862. doi: 10.1016/j.watres.2003.10.012. [DOI] [PubMed] [Google Scholar]
- 16.Carter Y, Barry D. Tackling C. difficile with environmental cleaning. Nurs Times. 2011;107:22–25. [PubMed] [Google Scholar]
- 17.Chappell CL, Okhuysen PC, Sterling CR, Wang C, Jakubowski W, DuPont HL. Infectivity of Cryptosporidium parvum in healthy adults with pre-existing anti-C. parvum serum immunoglobulin G. Am J Trop Med Hyg. 1999;60:157–164. doi: 10.4269/ajtmh.1999.60.157. [DOI] [PubMed] [Google Scholar]
- 18.Casanova LM, Jeon S, Rutala WA, Weber DJ, Sobsey MD. Effects of air temperature and relative humidity on coronavirus survival on surfaces. Appl Environ Microbiol. 2010;76:2712–2717. doi: 10.1128/AEM.02291-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chauret C. Survival and control of Escherichia coli O157:H7 in foods, beverages, soil and water. Virulence. 2011;2:593–601. doi: 10.4161/viru.2.6.18423. [DOI] [PubMed] [Google Scholar]
- 20.Chauret C, Chen P, Springthorpe S, Sattar S (1995) Effect of environmental stressors on the survival of Cryposporidium oocysts. In: Proceedings of the American water works association water quality technology conference, New Orleans, Nov 1995, American Water Works Association, Denver
- 21.Clifton IJ, Fletcher LA, Beggs CB, Denton M, Peckham DG. A laminar flow model of aerosol survival of epidemic and non-epidemic strains of Pseudomonas aeruginosa isolated from people with cystic fibrosis. BMC Microbiol. 2008;8:105. doi: 10.1186/1471-2180-8-105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Costerton JW, Lewandowski Z, DeBeer D, Caldwell D, Korber D, James G. Biofilms, the customized microniche. J Bacteriol. 1994;176:2137–2142. doi: 10.1128/jb.176.8.2137-2142.1994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lappin-Scott HM. Microbial biofilms. Annu Rev Microbiol. 1995;49:711–745. doi: 10.1146/annurev.mi.49.100195.003431. [DOI] [PubMed] [Google Scholar]
- 24.Craven PC, Mackel DC, Baine WB, Barker WH, Gangarosa EJ, Goldfield M, Rosenfeld H, Altman R, Lachapelle G, Davies JW, Swanson RC. International outbreak of Salmonella eastbourne infection traced to contaminated chocolate. Lancet. 1975;1:788–793. doi: 10.1016/s0140-6736(75)92446-0. [DOI] [PubMed] [Google Scholar]
- 25.Daeschlein G, Assadian O, Arnold A, Haase H, Kramer A, Jünger M. Bacterial burden of worn therapeutic silver textiles for neurodermitis patients and evaluation of efficacy of washing. Skin Pharmacol Physiol. 2010;23:86–90. doi: 10.1159/000265679. [DOI] [PubMed] [Google Scholar]
- 26.Dancer SJ, White LF, Lamb J, Girvan EK, Robertson C. Measuring the effect of enhanced cleaning in a UK hospital: a prospective cross-over study. BMC Med. 2009;7:28. doi: 10.1186/1741-7015-7-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Davies RH, Wray C. Persistence of Salmonella enteritidis in poultry units and poultry food. Br Poult Sci. 1996;37:589–596. doi: 10.1080/00071669608417889. [DOI] [PubMed] [Google Scholar]
- 28.Donlan RM. Role of biofilms in antimicrobial resistance. ASAIO J. 2000;46:S47–S52. doi: 10.1097/00002480-200011000-00037. [DOI] [PubMed] [Google Scholar]
- 29.Donlan RM. Biofilms: microbial life on surfaces. Emerg Infect Dis. 2002;8:881–890. doi: 10.3201/eid0809.020063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Donskey CJ. The role of the intestinal tract as a reservoir and source for transmission of nosocomial pathogens. Clin Infect Dis. 2004;39:219–226. doi: 10.1086/422002. [DOI] [PubMed] [Google Scholar]
- 31.Dorella FA, Pacheco LGC, Oliveira SC, Miyoshi A, Azevedo V. Corynebacterium pseudotuberculosis: microbiology, biochemical properties, pathogenesis and molecular studies of virulence. Vet Res. 2006;37:201–218. doi: 10.1051/vetres:2005056. [DOI] [PubMed] [Google Scholar]
- 32.Dryden M, Parnaby R, Dailly S, Lewis T, Davis-Blues K, Otter JA, Kearns AM. Hydrogen peroxide vapour decontamination in the control of a polyclonal methicillin-resistant Staphylococcus aureus outbreak on a surgical ward. J Hosp Infect. 2008;68:190–192. doi: 10.1016/j.jhin.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 33.Duffitt AD, Reber RT, Andrew Whipple A, Chauret C (2011) Gene expression during survival of Escherichia coli O157:H7 in soil and water. Int J Microbiol 2011, Article ID 340506. 10.1155/2011/340506 [DOI] [PMC free article] [PubMed]
- 34.Edward FF, Derrick G. Resistance of influenza virus to drying and its demonstration on dust. Lancet. 1941;241:664–666. [Google Scholar]
- 35.Erickson MC, Webb C, Diaz-Perez JC, Phatak S, Sivoy JJ, Davey L, Payton AS, Liao J, Ma L, Doyle MP. Surface and internalized Escherichia coli O157:H7 on field-grown spinach and lettuce treated with spray-contaminated irrigation water. J Food Prot. 2010;73:1023–1029. doi: 10.4315/0362-028x-73.6.1023. [DOI] [PubMed] [Google Scholar]
- 36.Espinal P, Marti S, Vila J. Effect of biofilm formation on the survival of Acinetobacter baumannii on dry surfaces. J Hosp Infect. 2012;80:56–60. doi: 10.1016/j.jhin.2011.08.013. [DOI] [PubMed] [Google Scholar]
- 37.Faix RG. Survival of cytomegalovirus on environmental surfaces. Clin Lab Observ. 1985;106:649–652. doi: 10.1016/s0022-3476(85)80096-2. [DOI] [PubMed] [Google Scholar]
- 38.Farzadegan H, Ford D, Malan M, Masters B, Scheel PJ. HIV-1 survival kinetics in peritoneal dialysis effluent. Kidney Int. 1996;50(5):1659–1662. doi: 10.1038/ki.1996.482. [DOI] [PubMed] [Google Scholar]
- 39.Flemming HC, Wingender J. The biofilm matrix. Nat Rev. 2010;8(9):623–633. doi: 10.1038/nrmicro2415. [DOI] [PubMed] [Google Scholar]
- 40.Fukumoto T, Matsuo J, Hayashi M, Oguri S, Nakamura S, Mizutani Y, Yao T, Akizawa K, Suzuki H, Shimizu C, Matsuno K, Yamaguchi H. Impact of free-living amoebae on presence of Parachlamydia acanthamoebae in the hospital environment and its survival in-vitro without requirement for amoebae. J Clin Microbiol. 2010;48:3360–3365. doi: 10.1128/JCM.00366-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Gebel J, Exner M, French G, Chartier Y, Christiansen B, Gemein S, Goroncy-Bermes P, Hartemann P, Heudorf U, Kramer A, Maillard JY, Oltmanns P, Rotter M, Sonntag HG (2013) The role of surface disinfection in infection prevention. GMS Hyg Infect Control 8:Doc10 (20130429) [DOI] [PMC free article] [PubMed]
- 42.Ghosh AR, Sehgal SC. Survivability of Shigella dysenteriae type 1 & S. flexneri 2a in laboratory conditions simulating aquatic environment. Indian J Med Res. 2001;114:199–206. [PubMed] [Google Scholar]
- 43.Gillings MR, Holley MP, Stokes HW. Evidence for dynamic exchange of qac gene cassettes between class 1 integrons and other integrons in freshwater biofilms. FEMS Microbiol Lett. 2009;269:282–288. doi: 10.1111/j.1574-6968.2009.01646.x. [DOI] [PubMed] [Google Scholar]
- 44.González M, Hänninen ML. Effect of temperature and antimicrobial resistance on survival of Campylobacter jejuni in well water: application of the Weibull model. J Appl Microbiol. 2012;113:284–293. doi: 10.1111/j.1365-2672.2012.05342.x. [DOI] [PubMed] [Google Scholar]
- 45.Groß R, Hübner N, Assadian O, Jibson B, Kramer A, Working Section for Clinical Antiseptic of the German Society for Hospital Hygiene (2010) Pilot study on the microbial contamination of conventional vs. silver-impregnated uniforms worn by ambulance personnel during one week of emergency medical service. GMS Krankenhaushyg Interdiszip 5:Doc09 (20100921) [DOI] [PMC free article] [PubMed]
- 46.Guan TTY, Holley RA. Hog manure management, the environment and human health. New York: Kluwer; 2003. [Google Scholar]
- 47.Guionie O, Courtillon C, Allee C, Maurel S, Queguiner M, Eterradossi N. An experimental study of the survival of turkey coronavirus at room temperature and +4C. Avian Pathol. 2013;42:248–252. doi: 10.1080/03079457.2013.779364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hara J, Okamoto S, Minekawa Y, Yamazaki K, Kase T. Survival and disinfection of adenovirus type 19 and enterovirus 70 in ophthalmic practice. Jpn J Ophthalmol. 1990;34:421–427. [PubMed] [Google Scholar]
- 49.Hayden MK, Blom DW, Lyle EA, Moore CG, Weinstein RA. Risk of hand or glove contamination after contact with patients colonized with vancomycin-resistant enterococcus or the colonized patients’ environment. Infect Control Hosp Epidemiol. 2008;29:149–154. doi: 10.1086/524331. [DOI] [PubMed] [Google Scholar]
- 50.Hayden MK, Bonten MJ, Blom DW, Lyle EA, van de Vijver DA, Weinstein RA. Reduction in acquisition of vancomycin-resistant enterococcus after enforcement of routine environmental cleaning measures. Clin Infect Dis. 2006;42:1552–1560. doi: 10.1086/503845. [DOI] [PubMed] [Google Scholar]
- 51.Haider S, Wagner M, Schmid MC, Sixt BS, Christian JG, Häcker G, Pichler P, Mechtler K, Müller A, Baranyi C, Toenshoff ER, Montanaro J, Horn M. Raman microspectroscope reveals long-term extracellular activity of chlamydiae. Mol Microbiol. 2010;77:687–700. doi: 10.1111/j.1365-2958.2010.07241.x. [DOI] [PubMed] [Google Scholar]
- 52.Hota B, Blom DW, Lyle EA, Weinstein RA, Hayden MK. Interventional evaluation of environmental contamination by vancomycin-resistant enterococci: failure of personnel, product, or procedure? J Hosp Infect. 2009;71:123–131. doi: 10.1016/j.jhin.2008.10.030. [DOI] [PubMed] [Google Scholar]
- 53.Hsueh PR. Human papillomavirus, genital warts, and vaccines. J Microbiol Immunol Infect. 2009;42:101–106. [PubMed] [Google Scholar]
- 54.Huang R, Mehta S, Weed D, Price CS. Methicillin-resistant Staphylococcus aureus survival on hospital fomites. Infect Control Hosp Epidemiol. 2006;27:1267–1269. doi: 10.1086/507965. [DOI] [PubMed] [Google Scholar]
- 55.Huang SS, Datta R, Platt R. Risk of acquiring antibiotic-resistant bacteria from prior room occupants. Arch Intern Med. 2006;166:945–951. doi: 10.1001/archinte.166.18.1945. [DOI] [PubMed] [Google Scholar]
- 56.Hübner NO, Hübner C, Kramer A, Assadian O. Survival of bacterial pathogens on paper and bacterial retrieval from paper to hands: preliminary results. Am J Nurs. 2011;111:30–34. doi: 10.1097/01.NAJ.0000408181.37017.82. [DOI] [PubMed] [Google Scholar]
- 57.Hunter PR. Survival of Bordetella pertussis in transport media. J Clin Pathol. 1986;39:119–120. doi: 10.1136/jcp.39.1.119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Jury LA, Sitzlar B, Kundrapu S, Cadnum JL, Summers KM, Muganda CP, Deshpande A, Sethi AK, Donskey CJ. Outpatient healthcare settings and transmission of Clostridium difficile. PLoS One. 2013;8:e70175. doi: 10.1371/journal.pone.0070175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Kane J, Summerbell R, Sigler L, Krajden S, Land G. Laboratory handbook of dermatophytes. A clinical guide and laboratory manual of dermatophytes and other filamentous fungi from skin, hair, and nails. Belmont: Star; 1997. [Google Scholar]
- 60.Kato S, Jenkins M, Fogarty E, Bowman D. Cryptosporidium parvum oocyst inactivation in field soil and its relation to soil characteristics: analysis using geographic information systems. Sci Total Environ. 2004;321:47–58. doi: 10.1016/j.scitotenv.2003.08.027. [DOI] [PubMed] [Google Scholar]
- 61.Keswick BH, Pickering LK, DuPont HL, Woodward WE. Survival and detection of surfaces in day care centers. Appl Environ Microbiol. 1983;46:813–816. doi: 10.1128/aem.46.4.813-816.1983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Khin Nwe Oo, Phyu Phyu Win, Aung Myo Han, Aye T. Contamination of currency notes with enteric bacterial pathogens. J Diarrhoeal Dis Res. 1989;7:92–94. [PubMed] [Google Scholar]
- 63.Kramer A, Assadian O, Ryll S, Selleng K, Below H (2013) Immediate infection control measures and preventive monitoring after excessive water damage in an aseptic working area of a blood donation service centre. Indoor Built Environ. 29 Oct 2013, doi: 10.1177/1420326X13508144
- 64.Kramer A, Guggenbichler P, Heldt P, Jünger M, Ladwig A, Thierbach H, Weber U, Daeschlein G. Hygienic relevance and risk assessment of antimicrobial-impregnated textiles. Curr Probl Dermatol. 2006;33:78–109. doi: 10.1159/000093938. [DOI] [PubMed] [Google Scholar]
- 65.Kramer A, Schwebke I, Kampf G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis. 2006;6:130–137. doi: 10.1186/1471-2334-6-130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Lai MYY, Cheng PKC, Lim WWL. Survival of severe acute respiratory syndrome coronavirus. Clin Infect Dis. 2005;41:e67–e71. doi: 10.1086/433186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Larson T, Bryson YJ. Fomites and herpes simplex virus. J Infect Dis. 1985;151:7467. doi: 10.1093/infdis/151.4.746. [DOI] [PubMed] [Google Scholar]
- 68.Lawley TD, Clare S, Deakin LJ, Goulding D, Yen JL, Raisen C, Brandt C, Lovell J, Cooke F, Clark TG, Dougan G. Use of purified Clostridium difficile spores to facilitate evaluation of health care disinfection regimens. Appl Environ Microbiol. 2010;76:6895–6900. doi: 10.1128/AEM.00718-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Lee J, Zoh K, Ko G. Inactivation and UV disinfection of murine norovirus with TiO2 under various environmental conditions. Appl Environ Microbiol. 2008;74:2111–2117. doi: 10.1128/AEM.02442-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Matsuo J, Kobayashi M, Nakamura S, Mizutani Y, Yao T, Hirai I, Yamamoto Y, Yamaguchi H. Stability of Chlamydophila pneumoniae in a harsh environment without a requirement for acanthamoebae. Microbiol Immunol. 2010;54:63–73. doi: 10.1111/j.1348-0421.2009.00182.x. [DOI] [PubMed] [Google Scholar]
- 71.Matthes R, Koban I, Bender C, Masur K, Kindel E, Weltmann KD, Kocher T, Kramer A, Hübner NO. Antimicrobial efficacy of an atmospheric pressure plasma jet against biofilms of Pseudomonas aeruginosa and Staphylococcus epidermidis. Plasma Process Polym. 2013;10:161–166. [Google Scholar]
- 72.Matthes R, Bender C, Schlüter R, Koban I, Bussiahn R, Reuter S, Lademann J, Weltmann K, Kramer A, Kaufmann GF. Antimicrobial efficacy of two surface barrier discharges with air plasma against in vitro biofilms. PLoS One. 2013;8:e70462. doi: 10.1371/journal.pone.0070462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Mayfield JL, Leet T, Miller J, Mundy LM. Environmental control to reduce transmission of Clostridium difficile. Clin Infect Dis. 2000;31:995–1000. doi: 10.1086/318149. [DOI] [PubMed] [Google Scholar]
- 74.McDade JJ, Hall LB. Survival of Staphylococcus aureus in the environment. II. Effect of elevated temperature on surface-exposed staphylococci. Am J Hyg. 1964;80:184–191. doi: 10.1093/oxfordjournals.aje.a120467. [DOI] [PubMed] [Google Scholar]
- 75.Medema GJ, Bahar M, Schets FM. Survival of Cryptosporidium parvum, Escherichia coli, faecal enterococci and Clostridium perfringens in river water: influence of temperature and autochthonous microorganism. Water Sci Technol. 1997;35:249–252. [Google Scholar]
- 76.Morita Y, Komoda E, Ono K, Kumagai S. Survival of biofilm-forming Salmonella on stainless steel bolt threads under dry conditions. J Food Hyg Soc Jpn. 2011;52:299–303. doi: 10.3358/shokueishi.52.299. [DOI] [PubMed] [Google Scholar]
- 77.Murphy TF, Brauer AL. Expression of urease by Haemophilus influenzae during human respiratory tract infection and role in survival in an acid environment. BMC Microbiol. 2011;11:183. doi: 10.1186/1471-2180-11-183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Neely AN, Maley MP. Survival of enterococci and staphylococci on hospital fabric and plastic. J Clin Microbiol. 2000;38:724–726. doi: 10.1128/jcm.38.2.724-726.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Neely AN, Orloff MM. Survival of some medically important fungi on hospital fabrics and plastics. J Clin Microbiol. 2001;39:3360–3361. doi: 10.1128/JCM.39.9.3360-3361.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Noyce JO, Michels H, Keevil CW. Potential use of copper surfaces to reduce survival of epidemic meticillin-resistant Staphylococcus aureus in the healthcare environment. J Hosp Infect. 2006;63:289–297. doi: 10.1016/j.jhin.2005.12.008. [DOI] [PubMed] [Google Scholar]
- 81.Oie S, Kamiya A. Survival of methicillin-resistant Staphylococcus aureus (MRSA) on naturally contaminated dry mops. J Hosp Infect. 1996;34:145–149. doi: 10.1016/s0195-6701(96)90140-1. [DOI] [PubMed] [Google Scholar]
- 82.Ojeil M, Jermann C, Holah J, Denyer SP, Maillard JY (2013) Evaluation of new in vitro efficacy test for antimicrobial surface activity reflecting UK hospital conditions. J Hosp Infect 85:274–281. doi:pii: S0195-6701(13)00313-7 [DOI] [PubMed]
- 83.Otter JA, Yezli S, French GL. The role played by contaminated surfaces in the transmission of nosocomial pathogens. Infect Control Hosp Epidemiol. 2011;32:687–699. doi: 10.1086/660363. [DOI] [PubMed] [Google Scholar]
- 84.Otter JA, Yezli S, Schouten MA, van Zanten AR, Houmes-Zielman G, Nohlmans-Paulssen MK. Hydrogen peroxide vapor decontamination of an intensive care unit to remove environmental reservoirs of multidrug-resistant gram-negative rods during an outbreak. Am J Infect Control. 2010;38:754–756. doi: 10.1016/j.ajic.2010.03.010. [DOI] [PubMed] [Google Scholar]
- 85.Pang XL, Joensun J, Vesikar T. Human calici-virus-associated sporadic gastroenteritis in Finnish children less than two years of age followed prospectively during a rotavirus vaccine trial. J Pediatr Infect Dis. 1999;18:420–426. doi: 10.1097/00006454-199905000-00005. [DOI] [PubMed] [Google Scholar]
- 86.Passaretti CL, Otter JA, Reich NG, Myers J, Shepard J, Ross T, Carroll KC, Lipsett P, Perl TM. An evaluation of environmental decontamination with hydrogen peroxide vapor for reducing the risk of patient acquisition of multidrug-resistant organisms. Clin Infect Dis. 2013;56:27–35. doi: 10.1093/cid/cis839. [DOI] [PubMed] [Google Scholar]
- 87.Patel A, Hammersmith K. Contact lens-related microbial keratitis: recent outbreaks. Curr Opin Ophthalmol. 2008;19:302–306. doi: 10.1097/ICU.0b013e3283045e74. [DOI] [PubMed] [Google Scholar]
- 88.Paton JC, Paton AW. Pathogenesis and diagnosis of Shiga toxin-producing Escherichia coli infections. Clin Microbiol Rev. 1998;11:450–479. doi: 10.1128/cmr.11.3.450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Percival SL, Thomas JG. Transmission of Helicobacter pylori and the role of water and biofilms. J Water Health. 2009;7:469–477. doi: 10.2166/wh.2009.070. [DOI] [PubMed] [Google Scholar]
- 90.Petti S, De Giusti M, Moroni C, Polimeni A. Long-term survival curve of methicillin-resistant Staphylococcus aureus on clinical contact surfaces in natural-like conditions. Am J Infect Control. 2012;40:1010–1012. doi: 10.1016/j.ajic.2011.11.020. [DOI] [PubMed] [Google Scholar]
- 91.Pittet D. Improving compliance with hand hygiene in hospitals. Infect Control Hosp Epidemiol. 2000;21:381–386. doi: 10.1086/501777. [DOI] [PubMed] [Google Scholar]
- 92.Porter CK, Riddle MS, Tribble DR, Louis Bougeois A, McKenzie R, Isidean SD, Sebeny P, Savarino SJ. A systematic review of experimental infections with enterotoxigenic Escherichia coli (ETEC) Vaccine. 2011;29:5869–5885. doi: 10.1016/j.vaccine.2011.05.021. [DOI] [PubMed] [Google Scholar]
- 93.Rabenau HF, Cinatl J, Morgenstern B, Bauer G, Preiser W, Doerr HW. Stability and inactivation of SARS coronavirus. Med Microbiol Immunol. 2005;194:1–6. doi: 10.1007/s00430-004-0219-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Randle J, Arthur A, Vaughan N. Twenty-four-hour observational study of hospital hand hygiene compliance. J Hosp Infect. 2010;76:252–255. doi: 10.1016/j.jhin.2010.06.027. [DOI] [PubMed] [Google Scholar]
- 95.Rigotto C, Hanley K, Rochelle PA, De Leon R, Barardi CR, Yates MV. Survival of adenovirus types 2 and 41 in surface and ground waters measured by a plaque assay. Environ Sci Technol. 2011;45:4145–4150. doi: 10.1021/es103922r. [DOI] [PubMed] [Google Scholar]
- 96.Robertson LJ, Campbell AT, Smith HV. Survival of Cryptosoridium parvum oocysts under various environmental pressures. Appl Environ Microbiol. 1992;58:3494–3500. doi: 10.1128/aem.58.11.3494-3500.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Robine E, Derangere D, Robin D. Survival of a Pseudomonas fluorescens and Enterococcus faecalis aerosol on inert surfaces. Int J Food Microbiol. 2000;55:229–234. doi: 10.1016/s0168-1605(00)00188-4. [DOI] [PubMed] [Google Scholar]
- 98.Rose LJ, Donlan R, Banerjee SN, Arduino SM. Survival of Yersinia pestis on environmental surfaces. Appl Environ Microbiol. 2003;69:2166–2171. doi: 10.1128/AEM.69.4.2166-2171.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Rutala WA, Peacock JE, Gergen MF, Sobsey MD, Weber DJ. Efficacy of hospital germicides against adenovirus 8, a common cause of epidemic keratoconjunctivitis in health care facilities. Antimicrob Agents Chemother. 2006;50:1419–1424. doi: 10.1128/AAC.50.4.1419-1424.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Schoenbaum MA, Zimmerman JJ, Beran GW, Murphy DP. Survival of pseudorabies virus in aerosol. Am J Vet Res. 1990;51:331–333. [PubMed] [Google Scholar]
- 101.Shaughnessy MK, Micielli RL, DePestel DD, Arndt J, Strachan CL, Welch KB, Chenoweth CE. Evaluation of hospital room assignment and acquisition of Clostridium difficile infection. Infect Control Hosp Epidemiol. 2011;32:201–206. doi: 10.1086/658669. [DOI] [PubMed] [Google Scholar]
- 102.Stowell JD, Forlin-Passoni D, Din E, Radford K, Brown D, White A, Bate SL, Dollard SC, Bialek SR, Cannon MJ, Schmid DS. Cytomegalovirus survival on common environmental surfaces: opportunities for viral transmission. J Infect Dis. 2012;205:211–214. doi: 10.1093/infdis/jir722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Tang JW. The effect of environmental parameters on the survival of airborne infectious agents. Interface. 2009;6(Suppl 6):S737–S774. doi: 10.1098/rsif.2009.0227.focus. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Tanner BD. Reduction in infection risk through treatment of microbially contaminated surfaces with a novel, portable, saturated steam vapor disinfection system. Am J Infect Control. 2009;37:20–27. doi: 10.1016/j.ajic.2008.03.008. [DOI] [PubMed] [Google Scholar]
- 105.Théraud M, Gangneux JP, Preney L, Guiguen C. Comparative survival of clinical and environmental isolates of Candida albicans and Cryptococcus neoformans in natural and experimental conditions. J Mycol Med. 2003;2:93–97. [Google Scholar]
- 106.Thomas Y, Vogel G, Wunderli W, Suter P, Witschi M, Koch D, Tapparel C, Kaiser L. Survival of influenza virus on banknotes. Appl Environ Microbiol. 2008;74:3002–3007. doi: 10.1128/AEM.00076-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Tiwari A, Patnayak DP, Chander Y, Parsad M, Goyal SM. Survival of two avian respiratory viruses on porous and nonporous surfaces. Avian Dis. 2006;50:284–287. doi: 10.1637/7453-101205R.1. [DOI] [PubMed] [Google Scholar]
- 108.Tolba O, Loughrey A, Goldsmith CE, Millar BC, Rooney PJ, Moore JE. Survival of epidemic strains of healthcare (HA-MRSA) and community-associated (CA-MRSA) methicillin resistant Staphylococcus aureus (MRSA) in river-, sea- and swimming pool water. Int J Hyg Environ Health. 2008;211:398–402. doi: 10.1016/j.ijheh.2007.06.003. [DOI] [PubMed] [Google Scholar]
- 109.Tribble GD, Rigney TW, Dao DH, Wong CT, Kerr JE, Taylor BE, Pacha S, Kaplan HB (2012) Natural competence is a major mechanism for horizontal DNA transfer in the oral pathogen Porphyromonas gingivalis. MBio 3:pii: e00231-11 [DOI] [PMC free article] [PubMed]
- 110.Tzeng YL, Martin LE, Stephens DS. Environmental survival of Neisseria meningitidis. Epidemiol Infect. 2013;10:1–4. doi: 10.1017/S095026881300085X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Uneke CJ, Ogbu O. Potential for parasite and bacteria transmission by paper currency in Nigeria. J Environ Health. 2007;69:54–60. [PubMed] [Google Scholar]
- 112.Valtierra HN. Stability of viral pathogens in the laboratory environment. Appl Biosaf. 2008;13:21–26. [Google Scholar]
- 113.Van Bueren J, Simpson RA, Jacobs P, Cookson BD. Survival of human immunodeficiency virus in suspension and dried onto surfaces. J Clin Microbiol. 1994;32:571–574. doi: 10.1128/jcm.32.2.571-574.1994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Vickery K, Deva A, Jacombs A, Allan J, Valente P, Gosbell IB. Presence of biofilm containing viable multiresistant organisms despite terminal cleaning on clinical surfaces in an intensive care unit. J Hosp Infect. 2012;80:52–55. doi: 10.1016/j.jhin.2011.07.007. [DOI] [PubMed] [Google Scholar]
- 115.Vriesekoop F, Russell C, Alvarez-Mayorga B, Aidoo K, Yuan Q, Scannell A, Beumer RR, Jiang X, Barro N, Otokunefor K, Smith-Arnold C, Heap A, Chen J, Iturriage MH, Hazeleger W, DeSlandes J, Kinley B, Wilson K, Menz G. Dirty money: an investigation into the hygiene status of some of the world’s currencies as obtained from food outlets. Foodborne Pathog Dis. 2010;7:1497–1502. doi: 10.1089/fpd.2010.0606. [DOI] [PubMed] [Google Scholar]
- 116.Wagenvoort HT, De Brauwer EIGB, Penders RJR, Willems RJ, Top J, Bonten MJ. Environmental survival of vancomycin-resistant Enterococcus faecium. J Hosp Infect. 2011;77:274–283. doi: 10.1016/j.jhin.2010.11.008. [DOI] [PubMed] [Google Scholar]
- 117.Wagenvoort JHT, Joosten EJAJ. An outbreak of Acinetobacter baumannii which mimics MRSA in its environmental longevity. J Hosp Infect. 2002;52:226–229. doi: 10.1053/jhin.2001.1294. [DOI] [PubMed] [Google Scholar]
- 118.Wagenvoort JH, Penders RJ. Long-term in-vitro survival of an epidemic MRSA phage-group III-29 strain. J Hosp Infect. 1997;35(4):322–325. doi: 10.1016/s0195-6701(97)90229-2. [DOI] [PubMed] [Google Scholar]
- 119.Wagenvoort JH, Penders RJ, Davies BI, Lutticken R. Similar environmental survival patterns of Streptococcus pyogenes strains of different epidemiologic backgrounds and clinical severity. Eur J Clin Microbiol Infect Dis. 2005;24:65–67. doi: 10.1007/s10096-004-1256-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Walsh RL, Camilli A. Streptococcus pneumoniae is desiccation tolerant and infectious upon rehydration. MBio. 2011;2:e00092-11. doi: 10.1128/mBio.00092-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Walther BA, Ewald PW. Pathogen survival in the external environment and the evolution of virulence. Biol Rev Camb Philos Soc. 2004;79:849–869. doi: 10.1017/S1464793104006475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Ward RL, Bernstein DI, Young EC, Sherwood JR, Knowlton DR, Schiff GM. Human rotavirus studies in volunteers: determination of infectious dose and serological response to infection. J Infect Dis. 1986;154:871–880. doi: 10.1093/infdis/154.5.871. [DOI] [PubMed] [Google Scholar]
- 123.Weber DJ, Rutala WA, Miller MB, Huslage K, Sickbert-Bennett E. Role of hospital surfaces in the transmission of emerging health care-associated pathogens: norovirus, Clostridium difficile, and Acinetobacter species. Am J Infect Control. 2010;38(Suppl 1):S25–S33. doi: 10.1016/j.ajic.2010.04.196. [DOI] [PubMed] [Google Scholar]
- 124.West AP, Millar MR, Tomkins DS. Effect of physical environment on survival of Helicobacter pylori. J Clin Pathol. 1992;45:228–231. doi: 10.1136/jcp.45.3.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Wendel KA. Diseases due to other category B bacterial pathogens II: psittacosis, Q fever and typhus. In: Bronze MS, Greenfield RA, editors. Biodefense: principles and pathogens. Norfolk: Horizon Bioscience; 2005. pp. 493–498. [Google Scholar]
- 126.Wilcox MH, Fawley WN, Wigglesworth N, Parnell P, Verity P, Freeman J. Comparison of the effect of detergent versus hypochlorite cleaning on environmental contamination and incidence of Clostridium difficile infection. J Hosp Infect. 2003;54:109–114. doi: 10.1016/s0195-6701(02)00400-0. [DOI] [PubMed] [Google Scholar]
- 127.Wong SS, Yip CC, Lau SK, Yuen KY. Human enterovirus 71 and hand, foot and mouth disease. Epidemiol Infect. 2010;138:1071–1089. doi: 10.1017/S0950268809991555. [DOI] [PubMed] [Google Scholar]
- 128.Wu HM, Fornek M, Schwab KJ, Chapin AR, Gibson K, Schwab E, Spencer C, Henning K. A norovirus outbreak at a long-term–care facility: the role of environmental surface contamination. Infect Control Hosp Epidemiol. 2005;26:802–810. doi: 10.1086/502497. [DOI] [PubMed] [Google Scholar]
- 129.Yeruham I, Friedman S, Perl S, Elad D, Berkovich Y, Kalgard Y. A herd level analysis of a Corynebacterium pseudotuberculosis outbreak in a dairy cattle herd. Vet Dermatol. 2004;15(5):315–320. doi: 10.1111/j.1365-3164.2004.00388.x. [DOI] [PubMed] [Google Scholar]
- 130.Yezli S, Otter JA. Minimum infective dose of the major human respiratory and enteric viruses transmitted through food and the environment. Food Environ Microbiol. 2011;3:1–30. doi: 10.1007/s12560-011-9056-7. [DOI] [PMC free article] [PubMed] [Google Scholar]