

Abstract
Intermittent outbreaks of infectious diseases have had profound and lasting effects on societies throughout history. Those events have powerfully shaped the economic, political, and social aspects of human civilization, with their effects often lasting for centuries. Epidemic outbreaks have defined some of the basic tenets of modern medicine, pushing the scientific community to develop principles of epidemiology, prevention, immunization, and antimicrobial treatments. This chapter outlines some of the most notable outbreaks that took place in human history and are relevant for a better understanding of the rest of the material. Starting with religious texts, which heavily reference plagues, this chapter establishes the fundamentals for our understanding of the scope, social, medical, and psychological impact that some pandemics effected on civilization, including the Black Death (a plague outbreak from the fourteenth century), the Spanish Flu of 1918, and the more recent outbreaks in the twenty-first century, including SARS, Ebola, and Zika.
Keywords: Pandemic outbreaks, History of pandemics, Plague, Spanish influenza, SARS, Ebola, Zika, Disease X
Very few phenomena throughout human history have shaped our societies and cultures the way outbreaks of infectious diseases have; yet, remarkably little attention has been given to these phenomena in behavioral social science and in branches of medicine that are, at least in part, founded in social studies (e.g., psychiatry).
This lack of attention is intriguing, as one of the greatest catastrophes ever, if not the greatest one in the entire history of humankind, was an outbreak of a pandemic [1]. In a long succession throughout history, pandemic outbreaks have decimated societies, determined outcomes of wars, wiped out entire populations, but also, paradoxically, cleared the way for innovations and advances in sciences (including medicine and public health), economy, and political systems [2]. Pandemic outbreaks, or plagues, as they are often referred to, have been closely examined through the lens of humanities in the realm of history, including the history of medicine [3]. In the era of modern humanities, however, fairly little attention has been given to ways plagues affected the individual and group psychology of afflicted societies. This includes the unexamined ways pandemic outbreaks might have shaped the specialty of psychiatry; psychoanalysis was gaining recognition as an established treatment within medical community at the time the last great pandemic was making global rounds a century ago.
There is a single word that can serve as a fitting point of departure for our brief journey through the history of pandemics – that word is the plague. Stemming from Doric Greek word plaga (strike, blow), the word plague is a polyseme, used interchangeably to describe a particular, virulent contagious febrile disease caused by Yersinia pestis, as a general term for any epidemic disease causing a high rate of mortality, or more widely, as a metaphor for any sudden outbreak of a disastrous evil or affliction [4]. This term in Greek can refer to any kind of sickness; in Latin, the terms are plaga and pestis (Fig. 2.1).
Figure 2.1.
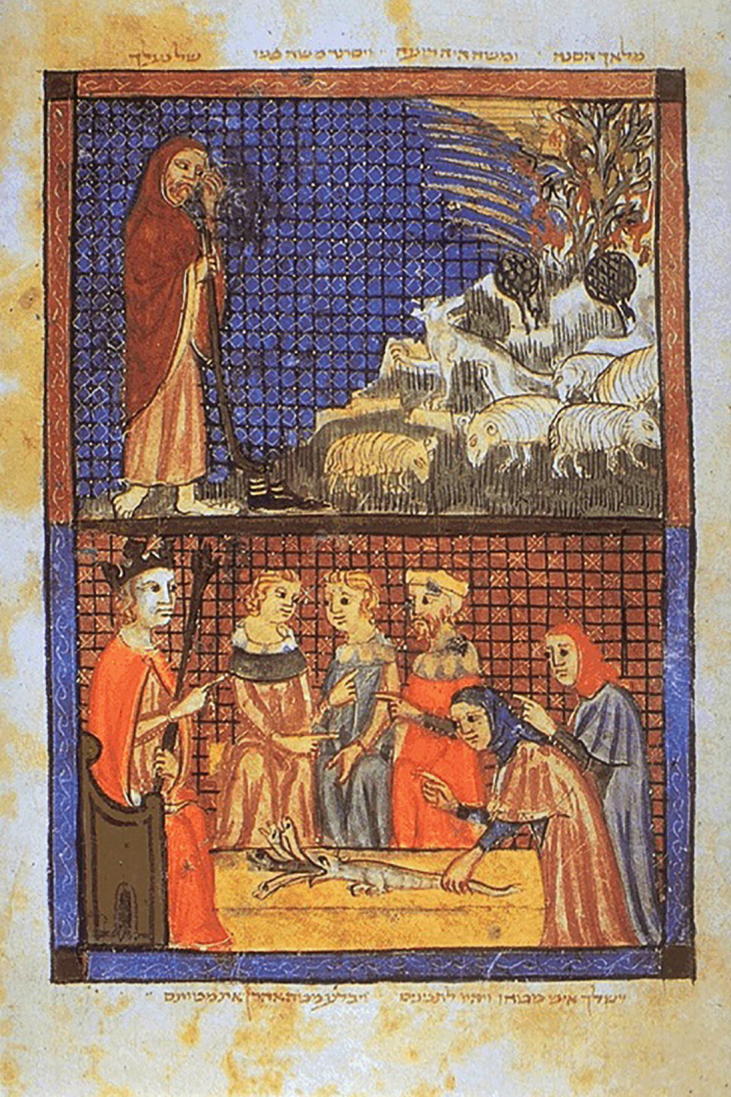
Plagues of Egypt depicted in Sarajevo Haggadah, Spain, cca. 1350, on display at National Museum of Bosnia-Herzegovina, Sarajevo
Perhaps the best-known examples of plagues ever recorded are those referred to in the religious scriptures that serve as foundations to Abrahamic religions, starting with the Old Testament. Book of Exodus, Chapters 7 through 11, mentions a series of ten plagues to strike the Egyptians before the Israelites, held in captivity by the Pharaoh, the ruler of Egypt, are finally released. Some of those loosely defined plagues are likely occurrences of elements, but at least a few of them are clearly of infectious nature. Lice, diseased livestock, boils, and possible deaths of firstborn likely describe a variety of infectious diseases, zoonoses, and parasitoses [5]. Similar plagues were described and referred to in Islamic tradition in Chapter 7 of the Qur’an (Surat Al-A’raf, v. 133) [6].
Throughout the Biblical context, pandemic outbreaks are the bookends of human existence, considered both a part of nascent human societies, and a part of the very ending of humanity. In the Apocalypse or The Book of Revelation, Chapter 16, seven bowls of God’s wrath will be poured on the Earth by angels, again some of the bowls containing plagues likely infectious in nature: “So the first angel went and poured out his bowl on the earth, and harmful and painful sores came upon the people who bore the mark of the beast” (Revelation 16:2).
Those events, regardless of factual evidence, deeply shaped human history, and continue to be commemorated in religious practices throughout the world. As we will see, the beliefs associated with those fundamental accounts have been rooted in societal responses to pandemics in Western societies and continue to shape public sentiment and perception of current and future outbreaks. Examined through the lens of Abrahamic spiritual context, serious infectious outbreaks can often be interpreted as a “Divine punishment for sins” (of the entire society or its outcast segments) or, in its eschatological iteration, as events heralding the “End of Days” (i.e., the end of the world).
Throughout known, predominantly Western history, there have been recorded processions of pandemics that each shaped our history and our society, inclusive of shaping the very basic principles of modern health sciences. What follows is an outline of major pandemic outbreaks throughout recorded history extending into the twenty-first century.
The Athenian Plague of 430 B.C.
The Athenian plague is a historically documented event that occurred in 430–26 B.C. during the Peloponnesian War, fought between city-states of Athens and Sparta. The historic account of the Athenian plague is provided by Thucydides, who survived the plague himself and described it in his History of the Peloponnesian War [7]. The Athenian plague originated in Ethiopia, and from there, it spread throughout Egypt and Greece. Initial symptoms of the plague included headaches, conjunctivitis, a rash covering the body, and fever. The victims would then cough up blood, and suffer from extremely painful stomach cramping, followed by vomiting and attacks of “ineffectual retching” [7]. Infected individuals would generally die by the seventh or eighth day. Those who survived this stage might suffer from partial paralysis, amnesia, or blindness for the rest of their lives. Doctors and other caregivers frequently caught the disease, and died with those whom they had been attempting to heal. The despair caused by the plague within the city led the people to be indifferent to the laws of men and gods, and many cast themselves into self-indulgence [8]. Because of wartime overcrowding in the city of Athens, the plague spread quickly, killing tens of thousands, including Pericles, Athens’ beloved leader. With the fall of civic duty and religion, superstition reigned, especially in the recollection of old oracles [7].
The plague of Athens affected a majority of the inhabitants of the overcrowded city-state and claimed lives of more than 25% of the population [9]. The cause of the Athenian plague of 430 B.C. has not been clearly determined, but many diseases, including bubonic plague, have been ruled out as possibilities [10]. While typhoid fever figures prominently as a probable culprit, a recent theory, postulated by Olson and some other epidemiologists and classicists, considers the cause of the Athenian plague to be Ebola virus hemorrhagic fever [11].
The Antonine Plague
While Hippocrates is thought to have been a contemporary of the plague of Athens, even possibly treating the afflicted as a young physician, he had not left known accounts of the outbreak [12]. It was another outbreak that occurred a couple of centuries later that was documented and recorded by contemporary physicians of the time. The outbreak was known as the Antonine Plague of 165–180 AD and the physician documenting it was Galen; this outbreak is also known as the Plague of Galen [13].
The Antonine plague occurred in the Roman Empire during the reign of Marcus Aurelius (161–180 A.D.) and its cause is thought to be smallpox [14]. It was brought into the Empire by soldiers returning from Seleucia, and before it abated, it had affected Asia Minor, Egypt, Greece, and Italy. Unlike the plague of Athens, which affected a geographically limited region, the Antonine plague spread across the vast territory of the entire Roman Empire, because the Empire was an economically and politically integrated, cohesive society occupying wide swaths of the territory [15]. The plague destroyed as much as one-third of the population in some areas, and decimated the Roman army, claiming the life of Marcus Aurelius himself [13].
The impact of the plague on the Roman Empire was severe, weakening its military and economic supremacy. The Antonine plague affected ancient Roman traditions, leading to a renewal of spirituality and religiousness, creating the conditions for spreading of new religions, including Christianity. The Antonine Plague may well have created the conditions for the decline of the Roman Empire and, afterwards, for its fall in the West in the fifth century AD [13].
The Justinian Plague
The Justinian plague was a “real plague” pandemic (i.e., caused by Yersinia Pestis) that originated in mid-sixth century AD either in Ethiopia, moving through Egypt, or in the Central Asian steppes, where it then traveled along the caravan trading routes. From one of these two locations, the pestilence quickly spread throughout the Roman world and beyond. Like most pandemics, the Justinian plague generally followed trading routes providing an “exchange of infections as well as of goods,” and therefore, was especially brutal to coastal cities. Military movement at the time also contributed to spreading the disease from Asia Minor to Africa and Italy, and further to Western Europe. Described in detail by Procopius, John of Ephesus, and Evagrius, the Justinian epidemic is the earliest clearly documented example of the actual (bubonic) plague outbreak [16].
During the plague, many victims experienced hallucinations prior to the outbreak of illness. The first symptoms of the plague followed closely behind; they included fever and fatigue. Soon afterwards, buboes appeared in the groin area or armpits, or occasionally beside the ears. From this point, the disease progressed rapidly; infected individuals usually died within days. Infected individuals would enter a delirious, lethargic state, and would not wish to eat or drink. Following this stage, the victims would be “seized by madness,” causing great difficulties to those who attempted to care for them [17]. Many people died painfully when their buboes gangrened; others died vomiting blood. There were also cases, however, in which the buboes grew to great size, and then ruptured and suppurated. In such cases, the patient would usually recover, having to live with withered thighs and tongues, classic aftereffects of the plague. Doctors, noticing this trend and not knowing how else to fight the disease, sometimes lanced the buboes of those infected to discover that carbuncles had formed. Those individuals who did survive infection usually had to live with ‘‘withered thighs and tongues’’, the stigmata of survivors. Emperor Justinian contracted the plague himself, but did not succumb [18].
Within a short time, all gravesites were beyond capacity, and the living resorted to throwing the bodies of victims out into the streets or piling them along the seashore to rot. The empire addressed this problem by digging huge pits and collecting the corpses there. Although those pits reportedly held 70,000 corpses each, they soon overflowed [17]. Bodies were then placed inside the towers in the walls, causing a stench pervading the entire city.
Streets were deserted, and all trade was abandoned. Staple foods became scarce and people died of starvation as well as of the disease itself [17]. The Byzantine Empire was a sophisticated society in its time and many of the advanced public policies and institutions that existed at that time were also greatly affected. As the tax base shrank and the economic output decreased, the Empire forced the survivors to shoulder the tax burden [19]. Byzantine army suffered in particular, being unable to fill its ranks and carry out military campaigns, and ultimately failing to retake Rome for the Empire. After the initial outbreak in 541, repetitions of the plague established permanent cycles of infection. By 600, it is possible that the population of the Empire had been reduced by 40%. In the city of Constantinople itself, it is possible that this figure exceeded 50 % [17].
At this point in history, Christian tradition enters the realm of interpreting and understanding the events of this nature [20]. Drawing on the eschatological narrative of the Book of Revelations, plague and other misfortunes are seen and explained as a “punishment for sins,” or retribution for the induction of “God’s wrath” [21]. This interpretation of the plague will reappear during the Black Death and play a much more central role throughout affected societies in Europe. Meanwhile, as the well-established Byzantine Empire experienced major challenges and weakening of its physical, economic, and cultural infrastructure during this outbreak, the nomadic Arab tribes, moving through sparsely populated areas and practicing a form of protective isolation, were setting a stage for the rapid expansion of Islam [22, 23].
The Black Death
“The Plague” was a global outbreak of bubonic plague that originated in China in 1334, arrived in Europe in 1347, following the Silk Road. Within 50 years of its reign, by 1400, [24] it reduced the global population from 450 million to below 350 million, possibly below 300 million, with the pandemic killing as many as 150 million. Some estimates claim that the Black Death claimed up to 60% of lives in Europe at that time [25].
Starting in China, it spread through central Asia and northern India following the established trading route known as the Silk Road. The plague reached Europe in Sicily in 1347. Within 5 years, it had spread to the virtually entire continent, moving onto Russia and the Middle East. In its first wave, it claimed 25 million lives [24].
The course and symptoms of the bubonic plague were dramatic and terrifying. Boccaccio, one of the many artistic contemporaries of the plague, described it as follows:
In men and women alike it first betrayed itself by the emergence of certain tumours in the groin or armpits, some of which grew as large as a common apple, others as an egg...From the two said parts of the body this deadly gavocciolo soon began to propagate and spread itself in all directions indifferently; after which the form of the malady began to change, black spots or livid making their appearance in many cases on the arm or the thigh or elsewhere, now few and large, now minute and numerous. As the gavocciolo had been and still was an infallible token of approaching death, such also were these spots on whomsoever they showed themselves [26].
Indeed, the mortality of untreated bubonic plague is close to 70%, usually within 8 days, while the mortality of untreated pneumonic plague approaches 95%. Treated with antibiotics, mortality drops to around 11% [27].
At the time, scientific authorities were at a loss regarding the cause of the affliction. The first official report blamed an alignment of three planets from 1345 for causing a “great pestilence in the air” [28]. It was followed by a more generally accepted miasma theory, an interpretation that blamed bad air. It was not until the late XIX century that the Black Death was understood for what it was – a massive Yersinia Pestis pandemic [29].
This strain of Yersinia tends to infect and overflow the guts of oriental rat fleas (Xenopsylla cheopis) forcing them to regurgitate concentrated bacteria into the host while feeding. Such infected hosts then transmit the disease further and can infect humans – bubonic plague [30]. Humans can transmit the disease by droplets, leading to pneumonic plague.
The mortality of the Black Death varied between regions, sometimes skipping sparsely populated rural areas, but then exacting its toll from the densely populated urban areas, where population perished in excess of 50, sometimes 60% [31].
In the vacuum of a reasonable explanation for a catastrophe of such proportions, people turned to religion, invoking patron saints, the Virgin Mary, or joining the processions of flagellants whipping themselves with nail embedded scourges and incanting hymns and prayers as they passed from town to town [32]. The general interpretation in predominantly Catholic Europe, as in the case of Justinian plague, centered on the divine “punishment for sins.” It then sought to identify those individuals and groups who were the “gravest sinners against God,” frequently singling out minorities or women. Jews in Europe were commonly targeted, accused of “poisoning the wells” and entire communities persecuted and killed. Non-Catholic Christians (e.g., Cathars) were also blamed as “heretics” and experienced a similar fate [33]. In other, non-Christian parts of the world affected by the plague, a similar sentiment prevailed. In Cairo, the sultan put in place a law prohibiting women from making public appearances as they may tempt men into sin [34].
For bewildered and terrified societies, the only remedies were inhalation of aromatic vapors from flowers or camphor. Soon, there was a shortage of doctors which led to a proliferation of quacks selling useless cures and amulets and other adornments that claimed to offer magical protection [35].
Entire neighborhoods, sometimes entire towns, were wiped out or settlements abandoned. Crops could not be harvested, traveling and trade became curtailed, and food and manufactured goods became short. The plague broke down the normal divisions between the upper and lower classes and led to the emergence of a new middle class. The shortage of labor in the long run encouraged innovation of labor-saving technologies, leading to higher productivity [2].
The effects of such a large-scale shared experience on the population of Europe influenced all forms of art throughout the period, as evidenced by works by renowned artists, such as Chaucer, Boccaccio, or Petrarch. The deep, lingering wake of the plague is evidenced in the rise of Danse Macabre (Dance of the death) in visual arts and religious scripts [36], its horrors perhaps most chillingly depicted by paintings titled the Triumph of Death (Fig. 2.2) [37].
Figure 2.2.
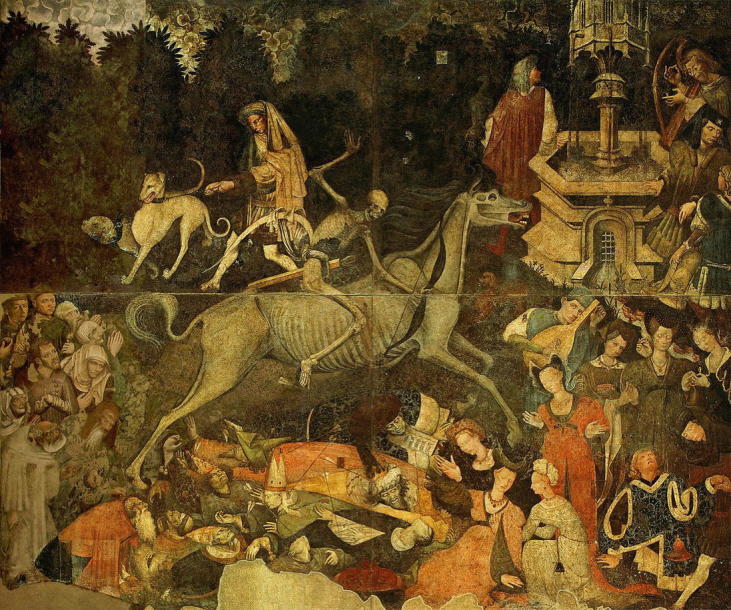
The Triumph of Death (Trionfo Della Morte), fresco, author unknown, cca. 1446, on display at Palazzo Abatellis, Palermo, Italy
The plague made several encore rounds through Europe in the following centuries, occasionally decimating towns and entire societies, but never with the same intensity as the Black Death [2].
The Plague Doctor
With the breakdown of societal structure and its infrastructures, many professions, notably that of medical doctors, were severely affected. Many towns throughout Europe lost their providers to plague or to fear thereof. In order to address this shortage in times of austere need, many municipalities contracted young doctors from whatever ranks were available to perform the duty of the plague doctor (medico della peste) [38]. Venice was among the first city-states to establish dedicated practitioners to deal with the issue of plague in 1348. Their principal task, besides taking care of people with the plague, was to record in public records the deaths due to the plague [39]. In certain European cities like Florence and Perugia, plague doctors were the only ones allowed to perform autopsies to help determine the cause of death and managed to learn a lot about human anatomy. Among the most notable plague doctors of their time were Nostradamus, Paracelsus, and Ambrois Pare [40]. The character of the plague doctor was immortalized by a later invention (from the seventeenth century) of a plague doctor costume by Charles De l’Orme (Fig. 2.3) [41].
Figure 2.3.

Doctor Beak (Doctor Schnabel), copper engraving by Paulus Fürst, cca. 1656, from Die Karikatur und Satire in der Medizin: Medico-Kunsthistorische Studie von Professor Dr. Eugen Holländer, 2nd edn (Stuttgart:Ferdinand Enke, 1921), fig. 79 (p. 171)
Quarantine
Drawing from experiences from ancient cultures that had dealt with contagious diseases, medieval societies observed the connection between the passage of time and the eruption of symptoms, noting that, after a period of observation, individuals who had not developed symptoms of the illness would likely not be affected and, more importantly, would not spread the disease upon entering the city. To that end, they started instituting mandatory isolation. The first known quarantine was enacted in Ragusa (City-state of Dubrovnik) in 1377, where all arrivals had to spend 30 days on a nearby island of Lokrum before entering the city. This period of 30 days (trentine) was later extended to 40 days (quarenta giorni or quarantine) [42]. The institution of quarantine was one of the rarely effective measures that took place during the Black Death and its use quickly spread throughout Europe. Quarantine remains in effect in the present time as a highly regulated, nationally and internationally governed public health measure available to combat contagions [43].
“Spanish Flu” Pandemic 1918–1920
The Spanish flu pandemic in the first decades of the twentieth century was the first true global pandemic and the first one that occurred in the setting of modern medicine, with specialties such as infectious diseases and epidemiology studying the nature of the illness and the course of the pandemic as it unfolded. It is also, as of this time, the last true global pandemic with devastating consequences for societies across the globe [44]. It was caused by the H1N1 strain of the influenza virus, [45] a strain that had an encore outbreak in the early years of the twenty-first century.
Despite advances in epidemiology and public health, both at the time and in subsequent decades, the true origin of Spanish flu remains unknown, despite its name. As possible sources of origin, cited are the USA, China, Spain, France, or Austria. These uncertainties are perpetuated by the circumstances of the Spanish flu – it took place in the middle of World War I, with significant censorships in place, and with fairly advanced modes of transportation, including intercontinental travel [44].
Within months, the deadly H1N1 strain of influenza virus had spread to every corner of the world. In addition to Europe, where massive military movements and overcrowding contributed to massive spread, this virus devastated the USA, Asia, Africa, and the Pacific Islands. The mortality rate of Spanish flu ranged between 10% and 20%. With over a quarter of the global population contracting that flu at some point, the death toll was immense – well over 50 million, possibly 100 million dead. It killed more individuals in a year than the Black Death had killed in a century [46].
This pandemic, unusually, tended to mortally affect mostly young and previously healthy individuals. This is likely due to its triggering a cytokine storm, which overwhelms and demolishes the immune system. By August of 1918, the virus had mutated to a much more virulent and deadlier form, returning to kill many of those who avoided it during the first wave [47].
Spanish flu had an immense influence on our civilization. Some authors (Price) even point out that it may have tipped the outcome of World War I, as it affected armies of Germany and the Austrian–Hungarian Empire earlier and more virulently than their Allied opponents (Fig. 2.4) [48].
Figure 2.4.

American Expeditionary Force, victims of Spanish flu in France, 1918. Uncredited U.S. Army photographer – U.S. Army Medical Corps photo via National Museum of Health & Medicine website at U.S. Army Camp Hospital No. 45, Aix-Les-Bains, France, Influenza Ward No. 1
Many notable politicians, artists, and scientists were either affected by the flu or succumbed to it. Many survived and went on to have distinguished careers in arts and politics (e.g., Walt Disney, Greta Garbo, Raymond Chandler, Franz Kafka, Edward Munch, Franklin Delano Roosevelt, and Woodrow Wilson). Many did not; this pandemic counted as its victims, among others, outstanding painters like Gustav Klimt and Egon Schiele [49], and acclaimed poets like Guillaume Apollinaire. It also claimed the life of Sigmund Freud’s fifth child – Sophie Halberstadt-Freud.
This pandemic was also the first one where the long-lingering effects could be observed and quantified. A study of US census data from 1960 to 1980 found that the children born to women exposed to the pandemic had more physical ailments and a lower lifetime income than those born a few months earlier or later. A 2006 study in the Journal of Political Economy found that “cohorts in utero during the pandemic displayed reduced educational attainment, increased rates of physical disability, lower income, lower socioeconomic status, and higher transfer payments compared with other birth cohorts” [50].
Despite its immense effect on the global civilization, Spanish flu started to fade quickly from the public and scientific attention, establishing a precedent for the future pandemics, and leading some historians (Crosby) to call it the “forgotten pandemic” [51]. One of the explanations for this treatment of the pandemic may lie in the fact that it peaked and waned rapidly, over a period of 9 months before it even could get adequate media coverage. Another reason may be in the fact that the pandemic was overshadowed by more significant historical events, such as the culmination and the ending of World War I. A third explanation may be that this is how societies deal with such rapidly spreading pandemics – at first with great interest, horror, and panic, and then, as soon as they start to subside, with dispassionate disinterest.
HIV Pandemic
HIV/AIDS is a slowly progressing global pandemic cascading through decades of time, different continents, and different populations, bringing new challenges with every new iteration and for every new group it affected. It started in the early 1980s in the USA, causing significant public concern as HIV at the time inevitably progressed to AIDS and ultimately, to death. The initial expansion of HIV was marked by its spread predominantly among the gay population and by high mortality, leading to marked social isolation and stigma.
HIV affects about 40 million people globally (prevalence rate: 0.79%) and has killed almost the same number of people since 1981 [52]. It causes about one million deaths a year worldwide (down from nearly two million in 2005) [53]. While it represents a global public health phenomenon, the HIV epidemic is particularly alarming in some Sub-Saharan African countries (Botswana, Lesotho, and Swaziland), where the prevalence tops 25% [54]. In the USA, about 1.2 million people live with HIV and about 12,000 die every year (down from over 40,000 per year in the late 1990s). HIV in the USA disproportionately affects gay population, transgendered women, and African-Americans [55].
Being a fairly slowly spreading pandemic, HIV has received formidable public health attention, both by national and by international administrations and pharmaceuticals. Advances in treatment (protease inhibitors and anti-retrovirals) have turned HIV into a chronic condition that can be managed by medications. It is a rare infectious disease that has managed to attract the focus of mental health which, in turn, resulted in a solid volume of works on mental health and HIV [56]. By studying the mental health of HIV, we can begin to understand some of the challenges generally associated with infectious diseases. We know, for example, that the lifetime prevalence rate for depression in HIV individuals is, at 22%, more than twice the prevalence rate in general population [57].
We understand how depression in HIV individuals shows association with substance abuse and that issues of stigma, guilt, and shame affect the outlook for HIV patients, including their own adherence to life-saving treatments [58]. We know about medical treatments of depression in HIV and we have studies in psychotherapy for patients with HIV. Some of those approaches can be very useful in treating patients in the context of a pandemic. Given the contrast between the chronicity of the HIV and the acuity of a potential pandemic, most of those approaches cannot be simply translated from mental health approach to HIV and used for patients in a rapidly advancing outbreak or a pandemic.
Smallpox Outbreak in Former Yugoslavia (1972)
Smallpox was a highly contagious disease for which Edward Jenner developed the world’s first vaccine in 1798. Caused by the Variola virus, it was a highly contagious disease with prominent skin eruptions (pustules) and mortality of about 30%. It may have been responsible for hundreds of millions of fatalities in the twentieth century alone. Due to the well-coordinated global effort starting in 1967 under the leadership of Donald Henderson, smallpox was eradicated within a decade of undertaking the eradication on a global scale [59].
The smallpox outbreak in the former Yugoslavia in 1972 was a far cry from even an epidemic, let alone a pandemic, but it illustrated the challenges associated with a rapidly spreading, highly contagious illness in a modern world. It started with a pilgrim returning from the Middle East, who developed fever and skin eruptions. Since a case of smallpox had not been seen in the region for over 30 years, physicians failed to correctly diagnose the illness and nine healthcare providers ended among 38 cases infected by the index case and first fatality [60].
Socialist Yugoslavia at the time declared martial law and introduced mandatory revaccination. Entire villages and neighborhoods were cordoned off (cordon sanitaire is a measure of putting entire geographic regions in quarantine). About 10,000 individuals who may have come into contact with the infected were placed in an actual quarantine. Borders were closed, and all non-essential travel was suspended. Within 2 weeks, the entire population of Yugoslavia was revaccinated (about 18 million people at the time). During the outbreak, 175 cases were identified, with 35 fatalities. Due to prompt and massive response, however, the disease was eradicated and the society returned to normal within 2 months [60]. This event has proven to be a useful model for working out scenarios (“Dark Winter”) [61] for responses to an outbreak of a highly contagious disease, both as a natural occurrence [62] and as an act of bioterrorism [63].
SARS
Severe Acute Respiratory Syndrome (SARS) was the first outbreak in the twenty-first century that managed to get public attention. Caused by the SARS Corona virus (SARS-CoV), it started in China and affected fewer than 10,000 individuals, mainly in China and Hong Kong, but also in other countries, including 251 cases in Canada (Toronto) [64].
The severity of respiratory symptoms and mortality rate of about 10% caused a global public health concern. Due to the vigilance of public health systems worldwide, the outbreak was contained by mid-2003 [65]. This outbreak was among the first acute outbreaks that had mental health aspects studied in the process and in the aftermath, in various part of the world and in different societies, yielding valuable data on effects of an acute infectious outbreak on affected individuals, families, and the entire communities, including the mental health issues facing healthcare providers [66]. Some of the valuable insights into the mental health of patients in isolation, survivors of the severe illness, or psychological sequelae of working with such patients were researched during the SARS outbreak.
“Swine Flu” or H1N1/09 Pandemic
The 2009 H1N1 pandemic was a reprise of the “Spanish flu” pandemic from 1918, but with far less devastating consequences. Suspected as a re-assortment of bird, swine, and human flu viruses, it was colloquially known as the “swine flu” [67]. It started in Mexico in April of 2009 and reached pandemic proportions within weeks [68]. It began to taper off toward the end of the year and by May of 2010, it was declared over.
It infected over 10% of the global population (lower than expected), with a death toll estimated varying from 20,000 to over 500,000 [69]. Although its death rate was ultimately lower than the regular influenza death rates, at the time it was perceived as very threatening because it disproportionately affected previously healthy young adults, often quickly leading to severe respiratory compromise. A possible explanation for this phenomenon (in addition to the “cytokine storm” applicable to the 1918 H1N1 outbreak) is attributed to older adults having immunity due to a similar H1N1 outbreak in the 1970s [70].
This pandemic also resulted in some valuable data studying and analyzing the mental health aspects of the outbreak. It was among the first outbreaks where policy reports included mental health as an aspect of preparedness and mitigation policy efforts. This outbreak of H1N1 was notable for dissonance between the public sentiment about the outbreak and the public health steps recommended and undertaken by WHO and national health institutions. General public sentiment was that of alarm caused by WHO releases and warnings, but it quickly turned to discontent and mistrust when the initial grim outlook of the outbreak failed to materialize [71]. Health agencies were accused of creating panic (“panicdemic”) and peddling unproven vaccines to boost the pharmaceutical companies (in 2009, some extra $1,5 billion worth of H1N1 vaccines were purchased and administered in the USA) [72].
This outbreak illustrated how difficult it may be to gauge and manage public expectations and public sentiments in the effort to mobilize a response. It also demonstrated how distilling descriptions of the impact of a complex public health threat like a pandemic into a single term like “mild,” “moderate,” or “severe” can potentially be misleading and, ultimately, of little use in public health approach [73].
Ebola Outbreak (2014–2016)
Ebola virus, endemic to Central and West Africa, with fruit bats serving as a likely reservoir, appeared in an outbreak in a remote village in Guinea in December 2013. Spreading mostly within families, it reached Sierra Leone and Liberia, where it managed to generate considerable outbreaks over the following months, with over 28,000 cases and over 11,000 fatalities. A very small number of cases were registered in Nigeria and Mali, but those outbreaks were quickly contained [74]. Ebola outbreak, which happened to be the largest outbreak of Ebola infection to date, gained global notoriety after a passenger from Liberia fell ill and died in Texas in September of 2014, infecting two nurses caring for him, and leading to a significant public concern over a possible Ebola outbreak in the USA [75]. This led to a significant public health and military effort to address the outbreak and help contain it on site (Operation United Assistance) [76, 77].
ZIKA (2015–2016)
Zika virus was a little known, dormant virus found in rhesus monkeys in Uganda. Prior to 2014, the only known outbreak among humans was recorded in Micronesia in 2007. The virus was then identified in Brazil in 2015, after an outbreak of a mild illness causing a flat pinkish rash, bloodshot eyes, fever, joint pain and headaches, resembling dengue. It is a mosquito-borne disease (Aedes Aegypti), but it can be sexually transmitted. Despite its mild course, which initially made it unremarkable form the public health perspective, infection with Zika can cause Guillain-Barre syndrome in its wake in adults and, more tragically, cause severe microcephalia in unborn children of infected mothers (a risk of about 1%) [78].
In Brazil, in 2015, for example, there were 2400 birth defects and 29 infant deaths due to suspected Zika infection [79]. Zika outbreak is an illustrative case of the context of global transmission; it was transferred from Micronesia, across the Pacific, to Brazil, whence it continued to spread [78]. It is also a case of a modern media pandemic; it featured prominently in the social media. In early 2016, Zika was being mentioned 50 times a minute in Twitter posts. Social media were used to disseminate information, to educate, or to communicate concerns [80].
Its presence in social media, perhaps for the first time in history, allowed social researchers to study the public sentiment, also known as the emotional epidemiology (Ofri), in real time [81]. While both public health institutions and the general public voiced their concern with the outbreak, scientists and officials sought to provide educational aspect, while concerned public was trying to have their emotional concerns addressed. It is indicative that 4 out of 5 posts on Zika on social media were accurate; yet, those that were “trending” and gaining popularity were posts with inaccurate content (now colloquially referred to as the “fake news”) [82]. This is a phenomenon that requires significant attention in preparing for future outbreaks because it may hold a key not only to preparedness, but also to execution of public health plans that may involve quarantine and immunization.
Since 2016, Zika has continued to spread throughout South America, Central America, the Caribbean, and several states within the USA. It remains a significant public health concern, as there is no vaccine and the only reliable way to avoid the risk for the offspring is to avoid areas where Zika was identified or to postpone pregnancy should travel to or living in affected areas be unavoidable [78].
Disease X
Disease X is not, as of yet, an actual disease caused by a known agent, but a speculated source of the next pandemic that could have devastating effects on humanity. Knowing the scope of deleterious effects a pandemic outbreak can have on humankind, in the wake of the Ebola outbreak, the World Health Organization (WHO) decided to dedicate formidable resources to identifying, studying, and combating possible future outbreaks. It does so in the form of an R&D Blueprint, though devising its global strategy and preparedness plan that allows the rapid activation of R&D activities during epidemics [83].
R&D Blueprint maintains and updates a list of so-called identified priority diseases. This list is updated at regular intervals and, as of 2018, it includes diseases such as Ebola and Marburg virus diseases, Lassa fever, Middle East respiratory syndrome coronavirus (MERS-CoV) and Severe Acute Respiratory Syndrome (SARS), Nipah and henipa virus diseases, Zika, and others [84]. For each disease identified, an R&D roadmap is created, followed by target product profiles (i.e., immunizations, treatment, and regulatory framework). Those efforts are important to help us combat a dangerous outbreak of any of the abovementioned diseases, but also to fend off Disease X. Since Disease X is a hypothetical entity, brought by a yet unknown pathogen that could cause a serious international pandemic, the R&D Blueprint explicitly seeks to enable cross-cutting R&D preparedness that is also relevant for both existing culprits and the unknown future “Disease X” as much as possible.
WHO utilizes this R&D Blueprint vehicle to assemble and deploy a broad global coalition of experts who regularly contribute to the Blueprint and who come from several medical, scientific, and regulatory backgrounds. Its advisory group, at the time, does not include mental health specialists [85].
Contributor Information
Damir Huremović, Phone: +116462697431, Email: damirh@gmail.com.
Damir Huremović, Email: dhuremov@northwell.edu.
References
- 1.Benedictow OJ. The black death: the greatest catastrophe ever. Hist Today. 2005;55(3):42–49. [Google Scholar]
- 2.Scheidel W. The great leveler: violence and the history of inequality from the stone age to the twenty-first century. Chapter 10: the black death. Princeton: Princeton University Press; 2017. pp. 291–313. [Google Scholar]
- 3.DeWitte SN. Mortality risk and survival in the aftermath of the medieval black death. PLoS One. 2014;9(5):e96513. doi: 10.1371/journal.pone.0096513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Plague. Merriam-Webster.com. Merriam-Webster, n.d. Web. 2018 Nov 10.
- 5.Marr JS, Malloy CD. An epidemiologic analysis of the ten plagues of Egypt. Caduceus. 1996;12(1):7–24. [PubMed] [Google Scholar]
- 6.The Noble Qur’an Surah 7, v. 133. https://quran.com/7/133.
- 7.Thucydides, history of the Peloponnesian War, Book 2, Chapter VII. p. 89–100., trans. Crawley R. Digireads.com Publishing; 2017 Sept. ISBN-10: 1420956418.
- 8.Page DL. Thucydides’ description of the great plague. Class Q. 1953;47(3):97–119. doi: 10.1017/S0009838800003050. [DOI] [Google Scholar]
- 9.Littman RJ. The plague of Athens: epidemiology and paleopathology. Mt Sinai J Med. 2009;76(5):456–467. doi: 10.1002/msj.20137. [DOI] [PubMed] [Google Scholar]
- 10.Langmuir AD, Worthen TD, Solomon J, Ray CG, Petersen E. The Thucydides syndrome: a new hypothesis for the cause of the plague of Athens. N Engl J Med. 1985;313:1027–1030. doi: 10.1056/NEJM198510173131618. [DOI] [PubMed] [Google Scholar]
- 11.Olson PE, Hames CS, Benenson AS, Genovese EN. The Thucydides syndrome: Ebola Déjà vu? (or Ebola Reemergent?) Emerg Infect Dis. 1996;2(2):155–156. doi: 10.3201/eid0202.960220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yapijakis C. Hippocrates of Kos, the father of clinical medicine, and Asclepiades of Bithynia, the father of molecular medicine. Review. In Vivo. 2009;23(4):507–514. [PubMed] [Google Scholar]
- 13.Sabbatani S, Fiorino S. The Antonine plague and the decline of the Roman empire. Infez Med. 2009;17(4):261–275. [PubMed] [Google Scholar]
- 14.Fears JR. The plague under Marcus Aurelius and the decline and fall of the Roman empire. Infect Dis Clin N Am. 2004;18(1):65–77. doi: 10.1016/S0891-5520(03)00089-8. [DOI] [PubMed] [Google Scholar]
- 15.Sáez A. The Antonine plague: a global pestilence in the II century d.C. Rev Chil Infectol. 2016;33(2):218–221. doi: 10.4067/S0716-10182016000200011. [DOI] [PubMed] [Google Scholar]
- 16.Horgan J. Justinian’s Plague (541–542 CE). Ancient history encyclopedia; 2014 Dec 26. Retrieved from https://www.ancient.eu/article/782/
- 17.Procopius, history of the wars. 7 Vols., trans. Dewing HB, Loeb Library of the Greek and Roman Classics; 1914. Cambridge, MA: Harvard University Press. Vol. I, p. 451–73.
- 18.Rosen W. Justinian’s flea: Plague, empire, and the birth of Europe. New York: Viking Adult, Hardcover; 2007.
- 19.Smith CA. Plague in the ancient world: a study from Thucydides to Justinian; 1997. www.loyno.edu/~history/journal/1996-7/Smith.html
- 20.Evagrius Scholasticus, Ecclesiastical history (AD431–594), trans. Walford E; 1846. Book 4. Chapter 29. http://www.tertullian.org/fathers/evagrius_4_book4.htm#12
- 21.Evans JAS. The attitude of the secular historians of the age of Justinian towards the classical past. Traditio. 1976;32:164–165. doi: 10.1017/S0362152900005572. [DOI] [Google Scholar]
- 22.Sabbatani S, Manfredi R, Fiorino S. The Justinian plague (part one) Infez Med. 2012;20(2):125–139. [PubMed] [Google Scholar]
- 23.Sabbatani S, Manfredi R, Fiorino S. The Justinian plague (part two). Influence of the epidemic on the rise of the Islamic empire. Infez Med. 2012;20(3):217–232. [PubMed] [Google Scholar]
- 24.The Editors of Encyclopaedia Britannica. Black death, Encyclopædia Britannica; 2018 Sept 4. https://www.britannica.com/event/Black-Death. Accessed Oct 2018.
- 25.DeWitte SN. Mortality risk and survival in the aftermath of the medieval black death. PLoS One. 2014;9(5):e96513. doi: 10.1371/journal.pone.0096513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Boccaccio, Decameron., trans. Rigg M. London: David Campbell; 1921. Vol. 1, p. 5–11.
- 27.Centers for Disease Control (CDC). 2015 Sept 24. FAQ: Plague. https://www.cdc.gov/plague/faq/index.html. Retrieved October 2018
- 28.Horrox R. Black death. Manchester University Press; 1994. p. 159. ISBN 978-0-7190-3498-5.
- 29.Halliday S. Death and miasma in Victorian London: an obstinate belief. BMJ. 2001;323:1469. doi: 10.1136/bmj.323.7327.1469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Eisen RJ, Gage KL. Adaptive strategies of Yersinia pestis to persist during inter-epizootic and epizootic periods. Vet Res. 2008;40(2):1. doi: 10.1051/vetres:2008039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Benedictow OJ. The black death 1346–1353: the complete history. Woodbridge: Boydell Press; 2012. p. 380. [Google Scholar]
- 32.Bennett JM, Hollister CW. Medieval Europe: A short history. New York: McGraw-Hill; 2006. p. 326. [Google Scholar]
- 33.Gottfried RS. Black death. Simon and Schuster; 2010. p. 74. ISBN 978-1-4391-1846-7.
- 34.Byrne JP. The black death. Westport: Greenwood Press; 2004. p. 108. [Google Scholar]
- 35.Hajar R. The air of history (part II) medicine in the middle ages. Heart Views. 2012;13(4):158–162. doi: 10.4103/1995-705X.105744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Oosterwijk S, Knoell S. Mixed metaphors. The Danse macabre in medieval and early modern Europe. Newcastle upon Tyne: Cambridge Scholars Publishing; 2011. [Google Scholar]
- 37.Volser I. The theme of death in Italian art: The Triumph of Death [Doctoral dissertation]. McGill University; 2001.
- 38.Byrne JP. Daily life during the black death. Greenwood Publishing Group; 2006. p. 168–70. ISBN 0-313-33297-5.
- 39.Wray SK. Communities and crisis: Bologna during the black death. Brill; 2009. p. 172–3. ISBN 978-90-04-17634-8.
- 40.Hogue J. Nostradamus: the new revelations. Barnes & Noble Books; 1995. p. 1884. ISBN 1-56619-948-4.
- 41.Boeckl CM. Images of plague and pestilence: iconography and iconology. Kirksville: Truman State University Press; 2000. p. 15. [Google Scholar]
- 42.Sehdev PS. The origin of quarantine. Clin Infect Dis. 2002;35(9):1071–1072. doi: 10.1086/344062. [DOI] [PubMed] [Google Scholar]
- 43.Tognotti E. Lessons from the history of quarantine, from plague to influenza A. Emerging Infectious Diseases. 2013. 10.3201/eid1902. [DOI] [PMC free article] [PubMed]
- 44.CDC: Remembering the 1918 influenza pandemic. https://www.cdc.gov/features/1918-flu-pandemic/index.html. Accessed Oct 2018.
- 45.Antonovics J, Hood ME, Baker CH. Molecular virology: was the 1918 flu avian in origin? Nature. 2006;440(7088):E9. doi: 10.1038/nature04824. [DOI] [PubMed] [Google Scholar]
- 46.Flecknoe D, Charles Wakefield B, Simmons A. Plagues & wars: the ‘Spanish flu’ pandemic as a lesson from history. Med Confl Surviv. 2018;34(2):61–68. doi: 10.1080/13623699.2018.1472892. [DOI] [PubMed] [Google Scholar]
- 47.Simonsen L, Clarke MJ, Schonberger LB, Arden NH, Cox NJ, Fukuda K. Pandemic versus epidemic influenza mortality: a pattern of changing age distribution. J Infect Dis. 1998;178(1):53–60. doi: 10.1086/515616. [DOI] [PubMed] [Google Scholar]
- 48.Price-Smith AT. Contagion and chaos. Cambridge, MA: MIT Press; 2008. [Google Scholar]
- 49.Whitford F. Expressionist portraits. Abbeville Press; 1987. p. 46. ISBN 0-89659-780-6.
- 50.Almond D. Is the 1918 influenza pandemic over? Long-term effects of in utero influenza exposure in the Post-1940 U.S. population. J Polit Econ. 2006;114(4):672–712. doi: 10.1086/507154. [DOI] [Google Scholar]
- 51.Crosby AW. America’s forgotten pandemic: the influenza of 1918. 2. Cambridge: Cambridge University Press; 2003. [Google Scholar]
- 52.Cohen MS, Hellmann N, Levy JA, DeCock K, Lange J. The spread, treatment, and prevention of HIV-1: evolution of a global pandemic. J Clin Invest. 2008;118(4):1244–1254. doi: 10.1172/JCI34706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Wang H, Wolock TM, Carter A, Nguyen G, Kyu H, Gakidou E, Hay SI, Mills EJ, Trickey A. Estimates of global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2015: the global burden of disease study 2015. Lancet HIV. 2016;3(8):e361–e387. doi: 10.1016/s2352-3018(16)30087-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.UNAIDS Data. 2018. http://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf
- 55.Today’s HIV/AIDS epidemic factsheet. https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/todaysepidemic-508.pdf. Centers for Disease Control and Prevention. U.S. Government. Accessed Oct 2018.
- 56.Academy of consultation-Liaison psychiatry, HIV Psychiatry Bibliography. https://www.clpsychiatry.org/member-resources/clinical-monographs/hiv-biblio/. Accessed Oct 2018.
- 57.Ciesla JA, Roberts JE. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry. 2001;158(5):725–730. doi: 10.1176/appi.ajp.158.5.725. [DOI] [PubMed] [Google Scholar]
- 58.Safren SA, Bedoya CA, O’Cleirigh C, Biello KB, Pinkston MM, Stein MD, Traeger L, Kojic E, Robbins GK, Lerner JA, Herman DS, Mimiaga MJ, Mayer KH. Cognitive behavioural therapy for adherence and depression in patients with HIV: a three-arm randomised controlled trial. Lancet HIV. 2016;3(11):e529–e538. doi: 10.1016/S2352-3018(16)30053-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Tarantola D. DA Henderson, Smallpox Eradicator. Am J Public Health. 2016;106(11):1895. doi: 10.2105/AJPH.2016.303477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Ilic M, Ilic I. The last major outbreak of smallpox (Yugoslavia, 1972): the importance of historical reminders. Travel Med Infect Dis. 2017;17:69–70. doi: 10.1016/j.tmaid.2017.05.010. [DOI] [PubMed] [Google Scholar]
- 61.O’Toole T, Mair M, Inglesby TV. Shining light on “dark winter”. Clin Infect Dis. 2002;34(7):972–983. doi: 10.1086/339909. [DOI] [PubMed] [Google Scholar]
- 62.Glasser JW, Foster SO, Millar JD, Lane JM. Evaluating public health responses to reintroduced smallpox via dynamic, socially structured, and spatially distributed metapopulation models. Clin Infect Dis. 2008;46(Suppl 3):S182–S194. doi: 10.1086/524382. [DOI] [PubMed] [Google Scholar]
- 63.Nishiura H, Brockmann SO, Eichner M. Extracting key information from historical data to quantify the transmission dynamics of smallpox. Theor Biol Med Model. 2008;5:20. doi: 10.1186/1742-4682-5-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Smith RD. Responding to global infectious disease outbreaks: lessons from SARS on the role of risk perception, communication and management. Soc Sci Med. 2006;63(12):3113–3123. doi: 10.1016/j.socscimed.2006.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.World Health Organization (WHO). Summary of probable SARS cases with onset of illness from 1 November 2002 to 31 July 2003. http://www.who.int/csr/sars/country/table2004_04_21/en/. Accessed Oct 2018.
- 66.Maunder RG. Was SARS a mental health catastrophe? Gen Hosp Psychiatry. 2009;31(4):316–317. doi: 10.1016/j.genhosppsych.2009.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Trifonov V, Khiabanian H, Rabadan R. Geographic dependence, surveillance, and origins of the 2009 influenza A (H1N1) virus. N Engl J Med. 361(2):115–9. 10.1056/NEJMp0904572. PMID 19474418. [DOI] [PubMed]
- 68.McNeil Jr DG. In new theory, swine flu started in Asia, not Mexico. The New York Times. 2009 June 23. Accessed Oct 2018.
- 69.Dawood FS, Iuliano AD, Reed C, et al. Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: a modelling study. Lancet Infect Dis. 2012;12(9):687–695. doi: 10.1016/S1473-3099(12)70121-4. [DOI] [PubMed] [Google Scholar]
- 70.Nguyen-Van-Tam JS, Openshaw PJM, Hashim A, et al. Risk factors for hospitalisation and poor outcome with pandemic A/H1N1 influenza: United Kingdom first wave (May–September 2009) Thorax. 2010;65(7):645–651. doi: 10.1136/thx.2010.135210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Garske T, Legrand J, Donnelly CA, Ward H, Cauchemez S, Fraser C, et al. Assessing the severity of the novel influenza A/H1N1 pandemic. BMJ. 2009;339:b2840. doi: 10.1136/bmj.b2840. [DOI] [PubMed] [Google Scholar]
- 72.Drugmakers, Doctors rake in billions battling H1N1 Flu By Dalia Fahmy. ABC News. 2009 Oct 14. https://abcnews.go.com/Business/big-business-swine-flu/story?id=8820642. Accessed Oct 2018.
- 73.Leung GM, Nicoll A. Reflections on pandemic (H1N1) 2009 and the international response. PLoS Med. 2010;7(10):e1000346. doi: 10.1371/journal.pmed.1000346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Kalra S, Kelkar D, Galwankar SC, Papadimos TJ, Stawicki SP, Arquilla B, Hoey BA, Sharpe RP, Sabol D, Jahre JA. The emergence of ebola as a global health security threat: from ‘lessons learned’ to coordinated multilateral containment efforts. J Global Infect Dis. 2014;6(4):164–177. doi: 10.4103/0974-777X.145247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Bell BP, Damon IK, Jernigan DB, et al. Overview, control strategies, and lessons learned in the CDC response to the 2014–2016 Ebola epidemic. Morb Mortal Wkly Rep. 2016;65(3):4–11. doi: 10.15585/mmwr.su6503a2. [DOI] [PubMed] [Google Scholar]
- 76.CDC: 2014–2016 Ebola outbreak in West Africa. https://www.cdc.gov/vhf/ebola/history/2014-2016-outbreak/. Accessed Oct 2018.
- 77.Zoroya G. Military Ebola mission in Liberia coming to an end. 2015 Feb 4. https://www.militarytimes.com/2015/02/04/military-ebola-mission-in-liberia-coming-to-an-end/MilitaryTimes.Gannett. Accessed Oct 2018.
- 78.Kindhauser MK, Allen T, Frank V, Santhanaa RS, Dye C. Zika: the origin and spread of a mosquito-borne virus. Bull World Health Organ. 2016; 10.2471/BLT.16.171082. [DOI] [PMC free article] [PubMed]
- 79.MFPM A, Souza WV, TVB A, Braga MC, Miranda Filho DB, RAA X, de Melo Filho DA, CAA B, Valongueiro S, APL M, Brandão-Filho SP, CMT M. The microcephaly epidemic and Zika virus: building knowledge in epidemiology. Cad Saude Publica. 2018;34(10):e00069018. doi: 10.1590/0102-311X00069018. [DOI] [PubMed] [Google Scholar]
- 80.Wood MJ. Propagating and debunking conspiracy theories on twitter during the 2015-2016 Zika virus outbreak. Cyberpsychol Behav Soc Netw. 2018;21(8):485–490. doi: 10.1089/cyber.2017.0669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Ofri D. The emotional epidemiology of H1N1 influenza vaccination. N Engl J Med. 2009;361(27):2594–2595. doi: 10.1056/NEJMp0911047. [DOI] [PubMed] [Google Scholar]
- 82.Sommariva S, Vamos C, Mantzarlis A, Đào LU-L, Tyson DM. Spreading the (fake) news: exploring health messages on social media and the implications for health professionals using a case study. Am J Health Educ. 2018;49(4):246–255. doi: 10.1080/19325037.2018.1473178. [DOI] [Google Scholar]
- 83.WHO: R&D Blueprint, about the R&D Blueprint. https://www.who.int/blueprint/about/en/. Accessed Oct 2018.
- 84.WHO: R&D Blueprint, list of Blueprint priority diseases. https://www.who.int/blueprint/priority-diseases/en/. Accessed Oct 2018. [DOI] [PubMed]
- 85.WHO: R&D Blueprint, scientific advisory group members. https://www.who.int/blueprint/about/sag-members/en/. Accessed Oct 2018.