

Abstract
Nepal is facing a large-scale labour migration—both internal and international—driven by economic and employment opportunities. There is sparse literature available at the national level which examines the link between migration and contraceptive use. This study aimed at identifying contraceptive use and the unmet need for family planning (FP) and exploring its correlates among the married women of reproductive age (MWRA) by their husbands' residence status, using data from Nepal Demographic Health Survey 2016–a nationally representative cross-sectional survey. A stratified two-stage cluster sampling in rural and a three-stage sampling in urban areas were used to select the sampling clusters, and data from 11,040 households were analyzed. Reported values were weighted by sample weights to provide national-level estimates. The adjusted odds ratio (aOR) was calculated using multiple logistic regressions using complex survey design, considering clusters, and stratification by ecological zones. All analyses were performed using Stata 15.0. Among the total MWRA, 53% were using a contraceptive method, whereas the proportion of contraceptive use among the cohabiting couple was 68%. The unmet need for contraceptive use was 10% among cohabiting couples and 50% among the noncohabiting couples. Contraceptive use was significantly low among the women reporting an induced abortion in the last five years and whose husbands were currently away. A strong negative association of spousal separation with contraceptive use was observed (aOR:0.14; p < 0.001) after controlling other covariates, whereas a positive association was observed with the unmet need (aOR:8.00; p < 0.001). Cohabiting couples had a significantly higher contraceptive use and lower unmet need compared with the couples living apart. Between 2006 and 2016, contraceptive use increased by 1% per year among cohabiting couples, although this increase is hugely attributable to the use of traditional methods, compared with modern methods. The labour migration being a significant and indispensable socioeconomic phenomenon for Nepal, it is necessary to monitor fertility patterns and contraceptive use by cohabitation status in order to ensure that the national family planning interventions are targeted to address the contraceptive and fertility needs of the migrant couples.
1. Background
Despite political instability, slow economic growth, and significant geographic and economic barriers to health care, Nepal has made considerable progress in improving reproductive health over the last two decades. Despite these gains, progress on universal access to reproductive health measured by the contraceptive prevalence rate (CPR) and unmet need for family planning remains unsatisfactory. Significant inequalities in use of and unmet need for contraceptives still exist by the place of residence, age-group, and migration status.
In Nepal, international migration and rural-to-urban migration within Nepal [migration may be seasonal, temporary, semipermanent, or permanent; its nature often depends on the reason for migration] are rapidly increasing [1]. A recent study in Nepal showed about a third of the households (30%) had at least one member of the family migrated. The proportion of migration was higher in the rural and disadvantaged regions of Nepal—the mid-western and far-western regions of the country compared with urban and relatively developed regions [2]. The Nepal Household Survey 2012 showed that almost half (47%) of households had at least one member migrating either inside or outside the country [3]. One in ten households (10%) had two migrants, 5% of the households had three migrants, and 7% had four or more migrants. The peak age for male migrants was within the age-groups 20–29 years. Among the male migrants, a majority fell in age-group 15–39 years, with the peak age group of 20–29 years, whereas a majority of female were in 15–29 years age-group [3]. The Nepal Household Survey 2012 also revealed that most of the migrants moved for employment reasons (59%), and this was true among both the group of migrants from urban (53%) and rural (60%) areas. Over a quarter (27%) of households had at least one migrant living overseas, with 6% of the households having at least two migrants and 2% having at least three international migrants (HHS 2012). Rural households (27%) were slightly more likely to have a migrant living overseas than the urban households (24%).
There is sparse literature examining the link between migration and contraceptive use and/or fertility. Using NDHS 2016 data, this study examines spousal separation and its effect on contraceptive use in Nepal [4]. Previous work on this topic using 2011 NDHS data [5] and the data from 40 rural districts [1] showed a significantly higher unmet need and lower use of modern contraceptives among couples living separately compared with cohabiting couples. Spousal separation was shown to play a crucial role in the decline of total fertility in the absence of a corresponding rise in the contraceptive uptake in Nepal [5], which is also supported by a recent mixed method study [2] that identified recently married couples delaying to plan for a baby due to spousal separation, usually husband. In this regard, regular monitoring of contraceptive use according to the changing migration trends and measuring the disaggregated fertility pattern/contraceptive use according to the cohabitation status can help policy makers and planners make an informed decision for family planning programming. This study was conducted to investigate a recent pattern in family planning use according to husband's residence status and study factors associated with the contraceptive use and unmet need for FP among cohabiting and noncohabiting women, to expand the evidence base and help policy makers make evidence based decisions.
2. Materials and Methods
Data for this study were drawn from Nepal Demographic Health Survey 2016 [4], a nationally representative survey conducted to provide up-to-date estimates on basic health and demographic indicators. A detailed methodology has been presented in the NDHS 2016 full report [4]. In brief, a stratified two-staged cluster sampling in rural and a three-staged sampling in urban areas were used in order to select the clusters. A total of 383 primary sampling units (PSUs) were selected using probability proportional to their size methods [6]. Subsequently, 30 households per cluster were selected with an equal probability systematic selection criterion. Interviews were completed for 11,040 households, yielding a response rate of 99%.
2.1. Variables
The dependent variable in this analysis was use of and unmet need for contraceptives among MWRA currently residing with husbands (cohabiting) and women whose husbands lived away (noncohabiting). Three major predictor variables were included in this analysis: individual factors (such as age, education, had an induced abortion in the last five years, and ever used emergency contraceptives), household-level variables (such as caste/ethnic group and wealth quintile), and community-level variables (such as urban/rural residence, provinces, and ecological zone).The method used to compute the wealth index is described in the NDHS 2016 report [3].
2.2. Statistical Analysis
All analyses were performed using Stata version 15 software. Reported values were weighted by sample weights to provide national estimates. Adjusted odds ratio (aOR) was calculated using multiple logistic regression, with all covariates (age, education, ecological zone, place of residence, provinces, wealth quintile, number of living children, caste/ethnicity, women who had induced abortion, and ever used emergency contraceptives) included simultaneously in the model using complex survey design, considering clusters, and stratification by ecological zones. p < 0.05 was considered to be statistically significant in this study. Because disaggregating family planning use and the unmet need for family planning by husband's residence status give a more realistic picture of family planning program performance at the population level, we present disaggregated results for the married women of reproductive age (MWRA) currently living with their husbands and women whose husbands lived away [1]. A sensitivity analysis was also carried for noncohabiting couples to identify the duration of separation (≤1 year vs > 1 year) that has more impact on use of and unmet need for family planning.
3. Results
Among married women of reproductive age (MWRA), spousal separation was observed among 34% of the participants with a median duration of 11 months (data not shown). Among women whose husbands were currently living away, nearly half of them (49.3%) were separated for more than a year. More than one-third (36%) were separated for less than 6 months, and 14.7% were separated for 6–11 months. Spousal separation was more common among MWRA in rural areas (37%) than their urban counterparts (32%). The peak age for spousal separation was within the age-groups 20–29 years [20–24 (45%) and 25–29 (43%)]. The highest spousal separation was observed among those who reside in Province 4 (42%) and Province 2 (39%), among the third wealth quintile groups (40%) and among those who were Muslims and hill Dalits (39%) (Table 1). Higher spousal separation was observed among women reporting ever use of emergency contraception (39%) than those never had an emergency contraception (34%).
Table 1.
Background characteristics of married women by their cohabitation status with their husbands, 2016.
| Women's characteristic | Cohabitation status | Total MWRA | |||
|---|---|---|---|---|---|
| Cohabiting | Noncohabiting | ||||
| n | % | N | % | ||
| No. of living children | |||||
| None | 648 | 63.2 | 377 | 36.8 | 1025 |
| 1–2 | 3066 | 60.8 | 1978 | 39.2 | 5044 |
| 3–4 | 2148 | 72.4 | 817 | 27.6 | 2965 |
| 5+ | 659 | 78.4 | 181 | 21.6 | 840 |
|
| |||||
| Age-groups (years) | |||||
| 15–19 | 418 | 59.4 | 286 | 40.6 | 704 |
| 20–24 | 929 | 55.1 | 755 | 44.9 | 1684 |
| 25–29 | 1118 | 57.1 | 839 | 42.9 | 1957 |
| 30–34 | 1084 | 62.8 | 642 | 37.2 | 1726 |
| 35–39 | 1075 | 71.2 | 436 | 28.8 | 1510 |
| 40–44 | 1030 | 80.3 | 253 | 19.7 | 1283 |
| 45–49 | 868 | 85.9 | 143 | 14.1 | 1011 |
|
| |||||
| Level of educational | |||||
| No education | 2784 | 69.9 | 1200 | 30.1 | 3984 |
| Primary | 1182 | 63.8 | 670 | 36.2 | 1853 |
| Secondary | 1797 | 62.1 | 1094 | 37.9 | 2891 |
| Higher | 758 | 66.1 | 389 | 33.9 | 1147 |
|
| |||||
| Place of residence | |||||
| Urban | 4112 | 68.2 | 1919 | 31.8 | 6031 |
| Rural | 2409 | 62.7 | 1434 | 37.3 | 3844 |
|
| |||||
| Province | |||||
| Province 1 | 1118 | 67.5 | 537 | 32.5 | 1655 |
| Province 2 | 1329 | 61.3 | 839 | 38.7 | 2168 |
| Province 3 | 1446 | 75.3 | 473 | 24.7 | 1920 |
| Province 4 | 553 | 58.2 | 397 | 41.8 | 950 |
| Province 5 | 1150 | 65.8 | 599 | 34.2 | 1749 |
| Province 6 | 388 | 66.2 | 198 | 33.8 | 586 |
| Province 7 | 537 | 63.5 | 309 | 36.5 | 846 |
|
| |||||
| Ecological zone | |||||
| Mountain | 396 | 68.7 | 180 | 31.3 | 576 |
| Hill | 2791 | 67.3 | 1359 | 32.7 | 4150 |
| Terai | 3334 | 64.8 | 1814 | 35.2 | 5148 |
|
| |||||
| Wealth quintile | |||||
| Poorest | 1107 | 65.6 | 580 | 34.4 | 1687 |
| Poorer | 1235 | 63.5 | 711 | 36.5 | 1946 |
| Middle | 1263 | 60.5 | 825 | 39.5 | 2088 |
| Richer | 1359 | 64.5 | 749 | 35.5 | 2107 |
| Richest | 1557 | 76.1 | 490 | 23.9 | 2047 |
|
| |||||
| Caste/ethnicity | |||||
| Hill Brahmin | 769 | 69.1 | 343 | 30.9 | 1112 |
| Hill Chhetri | 1141 | 63.6 | 654 | 36.4 | 1794 |
| Terai Brahmin/Chhetri | 125 | 75.1 | 41 | 24.9 | 166 |
| Other Terai caste | 1057 | 66.3 | 536 | 33.7 | 1593 |
| Hill Dalit | 476 | 60.8 | 308 | 39.2 | 784 |
| Terai Dalit | 301 | 62.7 | 179 | 37.3 | 481 |
| Newar | 362 | 80.1 | 90 | 19.9 | 452 |
| Hill Janajati | 1283 | 64.2 | 717 | 35.8 | 2000 |
| Terai Janajati | 674 | 70.5 | 282 | 29.5 | 956 |
| Muslim | 306 | 60.7 | 198 | 39.3 | 504 |
| Others | 27 | 83.8 | 5 | 16.2 | 32 |
|
| |||||
| Had an induced abortion in the last five years | |||||
| No | 6199 | 66.0 | 3190 | 34.0 | 9389 |
| Yes | 322 | 66.3 | 164 | 33.7 | 486 |
|
| |||||
| Ever had emergency contraceptives | |||||
| No | 6435 | 66.1 | 3299 | 33.9 | 9734 |
| Yes | 86 | 61.0 | 55 | 39.0 | 141 |
| Total | 6522 | 66.0 | 3533 | 34.0 | 9875 |
Among all MWRA, 53% were using any contraceptives; of whom 81% were using modern methods rather than traditional ones (data not shown). This proportion of contraceptive use (any method) among cohabitating couples increased to 68% (Figure 1), whereas only 24% of women whose husbands lived away reported using any contraceptive methods (Table 2).
Figure 1.
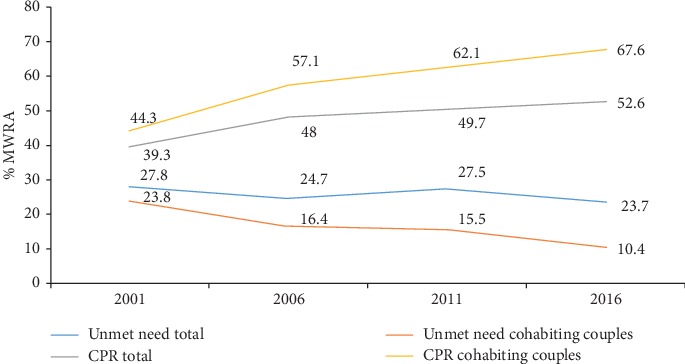
Trend of CPR (any method) and unmet need among total MWRA and the MWRA cohabiting with their husbands (NDHS 2001 to 2016).
Table 2.
Use of any method of FP (%) and its difference by cohabitation status among married women, 2016.
| Women's characteristic | Cohabiting | Noncohabiting | Difference | ||
|---|---|---|---|---|---|
| Any method | (N) | Any method | (N) | ||
| Living children | |||||
| None | 21.4 | 648 | 5.1 | 377 | 16.3 |
| 1–2 | 69.9 | 3066 | 18.8 | 1978 | 51.1 |
| 3–4 | 78.1 | 2148 | 40.3 | 817 | 37.8 |
| 5+ | 68.2 | 659 | 37.0 | 181 | 31.2 |
|
| |||||
| Age-groups (years) | |||||
| 15–19 | 33.4 | 418 | 8.2 | 286 | 25.2 |
| 20–24 | 50.1 | 929 | 9.8 | 755 | 40.3 |
| 25–29 | 65.6 | 1118 | 19.5 | 839 | 46.1 |
| 30–34 | 76.2 | 1084 | 28.9 | 642 | 47.3 |
| 35–39 | 79.9 | 1075 | 40.4 | 436 | 39.5 |
| 40–44 | 77 | 1030 | 38.5 | 253 | 38.5 |
| 45–49 | 68.2 | 868 | 48.0 | 143 | 20.2 |
|
| |||||
| Highest educational level | |||||
| No education | 69.5 | 2784 | 32.1 | 1200 | 37.4 |
| Primary | 66.3 | 1182 | 22.3 | 670 | 44 |
| Secondary | 64.5 | 1797 | 17.8 | 1094 | 46.7 |
| Higher | 69.9 | 758 | 15.0 | 389 | 54.9 |
|
| |||||
| Place of residence | |||||
| Urban | 69.6 | 4112 | 23.1 | 1919 | 46.5 |
| Rural | 64.2 | 2409 | 24.0 | 1434 | 40.2 |
|
| |||||
| Province | |||||
| Province 1 | 72.9 | 1118 | 18.2 | 537 | 54.7 |
| Province 2 | 59.8 | 1329 | 28.5 | 839 | 31.3 |
| Province 3 | 70.7 | 1446 | 30.0 | 473 | 40.7 |
| Province 4 | 72.1 | 553 | 15.6 | 397 | 56.5 |
| Province 5 | 63.4 | 1150 | 18.4 | 599 | 45.0 |
| Province 6 | 65.5 | 388 | 23.0 | 198 | 42.5 |
| Province 7 | 73.5 | 537 | 29.2 | 309 | 44.3 |
|
| |||||
| Ecological zone | |||||
| Mountain | 68.9 | 396 | 23.1 | 180 | 45.8 |
| Hill | 70.2 | 2791 | 20.5 | 1359 | 49.7 |
| Terai | 65.3 | 3334 | 25.8 | 1814 | 39.5 |
|
| |||||
| Wealth index | |||||
| Poorest | 63.5 | 1107 | 21.6 | 580 | 41.9 |
| Poorer | 70 | 1235 | 24.6 | 711 | 45.4 |
| Middle | 66.3 | 1263 | 24.0 | 825 | 42.3 |
| Richer | 64.6 | 1359 | 23.8 | 749 | 40.8 |
| Richest | 72.3 | 1557 | 22.5 | 490 | 49.8 |
|
| |||||
| Ethnicity∗ | |||||
| Hill Brahmin | 76.6 | 769 | 17.7 | 343 | 58.9 |
| Hill Chhetri | 70.1 | 1141 | 19.0 | 654 | 51.1 |
| Terai Brahmin/Chhetri | 70.8 | 125 | 20.4 | 41 | 50.4 |
| Other Terai caste | 61 | 1057 | 30.8 | 536 | 30.2 |
| Hill Dalit | 69.2 | 476 | 22.5 | 308 | 46.7 |
| Terai Dalit | 51.5 | 301 | 26.4 | 179 | 25.1 |
| Newar | 67.6 | 362 | 32.1 | 90 | 35.5 |
| Hill Janajati | 69.7 | 1283 | 19.5 | 717 | 50.2 |
| Terai Janajati | 77.6 | 674 | 38.6 | 282 | 39 |
| Muslim | 39.2 | 306 | 14.8 | 198 | 24.4 |
|
| |||||
| Had an induced abortion in the last five years | |||||
| No | 67.4 | 6199 | 24.0 | 3190 | 43.4 |
| Yes | 72.5 | 322 | 12.5 | 164 | 60 |
|
| |||||
| Ever had emergency contraceptives | |||||
| No | 67.6 | 6435 | 23.5 | 3299 | 44.1 |
| Yes | 67.6 | 86 | 24.6 | 55 | 43 |
|
| |||||
| Total | 67.6 | 6521 | 23.5 | 2354 | 44.1 |
∗Missing = 32.
The use of contraceptives among women currently residing with husbands and women whose husbands lived away was most common for the age range 35–49 years, the age range when women are most likely to want to stop (rather than delay or space) childbearing. By provinces, among the women currently residing with husbands and women whose husbands lived away, the highest use of contraceptive methods was observed among those residing in Province 7 (74% and 29%, respectively).
The largest gap in contraceptive use (any method) by husband's cohabitation status was observed among those with a higher level of education (55%), those residing in Province 4 (57%) followed by Province 1 (55%), hill Brahmins (59%), and who had and induced abortion in the last five years (60%) (Table 2).
Overall, unmet need of contraceptive use was 24% among any MWRA and 10% among those currently residing with husbands (Figure 1), whereas the unmet need was 50% among those women whose husbands were away. The largest crude difference in unmet need by husband's cohabitation status was observed among couples who had 1–2 living children (45%) compared with other categories (no children, 3–4 children, 5, and more). By age categories, the difference in unmet need by husband's cohabitation was almost similar among age categories covering 15–34 years (39–42%). Those with higher educational status, primary (42%), secondary (47%), and higher education (43%), had large differences in unmet need than those with no education (28%). Province 1 (48%) and Province 4 (50%) had higher difference in unmet need by husband's cohabitation status. Similarly, hills region (45%) had a higher difference in unmet need than the mountain (40%) and Terai regions (35%) of Nepal. By ethnicity, hill Brahmin (48%), hill Chhetri (46%), and hill Janajati (48%) showed the largest crude difference in unmet need than other caste/ethnicities. Women who had an abortion in the last five years had much higher difference in the unmet need for FP (51%) by husbands' cohabitation status than women reporting no abortion in the last five years (39%) (Table 3).
Table 3.
Unmet need for FP(%) and its difference by cohabitation status among married women in Nepal, 2016.
| Women's characteristic | Cohabiting | Noncohabiting | Difference | ||
|---|---|---|---|---|---|
| Any method | Total (N) | Any method | Total (N) | ||
| Living children | |||||
| None | 9.7 | 648 | 36.9 | 377 | 27.2 |
| 1–2 | 11.1 | 3066 | 56.3 | 1978 | 45.2 |
| 3–4 | 9.4 | 2148 | 41.5 | 817 | 32.1 |
| 5+ | 11.4 | 659 | 38.9 | 181 | 27.5 |
|
| |||||
| Age-groups (years) | |||||
| 15–19 | 18.4 | 418 | 59.0 | 286 | 40.6 |
| 20–24 | 13.8 | 929 | 55.6 | 755 | 41.8 |
| 25–29 | 13.3 | 1118 | 52.4 | 839 | 39.1 |
| 30–34 | 9.0 | 1084 | 50.9 | 642 | 41.9 |
| 35–39 | 7.1 | 1075 | 41.8 | 436 | 34.7 |
| 40–44 | 7.6 | 1030 | 37.9 | 253 | 30.3 |
| 45–49 | 8.6 | 868 | 20.6 | 143 | 12.0 |
|
| |||||
| Highest educational level | |||||
| No education | 9.4 | 2784 | 37.8 | 1200 | 28.4 |
| Primary | 11.1 | 1182 | 53.5 | 670 | 42.4 |
| Secondary | 12.4 | 1797 | 59.4 | 1094 | 47.0 |
| Higher | 8.7 | 758 | 51.5 | 389 | 42.8 |
|
| |||||
| Place of residence | |||||
| Urban | 9.8 | 4112 | 50.4 | 1919 | 40.6 |
| Rural | 11.5 | 2409 | 48.5 | 1434 | 37.0 |
|
| |||||
| Province | |||||
| Province 1 | 9.4 | 1118 | 57.2 | 537 | 47.8 |
| Province 2 | 10.2 | 1329 | 37.0 | 839 | 26.8 |
| Province 3 | 9.9 | 1446 | 50.2 | 473 | 40.3 |
| Province 4 | 9.2 | 553 | 59.0 | 397 | 49.8 |
| Province 5 | 13.8 | 1150 | 54.9 | 599 | 41.1 |
| Province 6 | 12.9 | 388 | 50.8 | 198 | 37.9 |
| Province 7 | 7.0 | 537 | 46.1 | 309 | 39.1 |
|
| |||||
| Ecological zone | |||||
| Mountain | 10.3 | 396 | 50.1 | 180 | 39.8 |
| Hill | 10.7 | 2791 | 56.1 | 1359 | 45.4 |
| Terai | 10.2 | 3334 | 44.7 | 1814 | 34.5 |
|
| |||||
| Wealth index | |||||
| Poorest | 14.0 | 1107 | 51.8 | 580 | 37.8 |
| Poorer | 8.8 | 1235 | 49.8 | 711 | 41.0 |
| Middle | 9.3 | 1263 | 47.1 | 825 | 37.8 |
| Richer | 10.6 | 1359 | 47.7 | 749 | 37.1 |
| Richest | 9.9 | 1557 | 53.9 | 490 | 44.0 |
|
| |||||
| Ethnicity | |||||
| Hill Brahmin | 7.2 | 769 | 55.6 | 343 | 48.4 |
| Hill Chhetri | 10.2 | 1141 | 56.3 | 654 | 46.1 |
| Terai Brahmin/Chhetri | 8.9 | 125 | 40.4 | 41 | 31.5 |
| Other Terai caste | 11.4 | 1057 | 36.6 | 536 | 25.2 |
| Hill Dalit | 15.3 | 476 | 56.7 | 308 | 41.4 |
| Terai Dalit | 13.3 | 301 | 35.3 | 179 | 22.0 |
| Newar | 11.8 | 362 | 52.7 | 90 | 40.9 |
| Hill Janajati | 10.2 | 1283 | 58.4 | 717 | 48.2 |
| Terai Janajati | 5.2 | 674 | 37.7 | 282 | 32.5 |
| Muslim | 17.3 | 306 | 40.9 | 198 | 23.6 |
|
| |||||
| Had an abortion in the last five years | |||||
| Yes | 16.9 | 322 | 67.4 | 164 | 50.5 |
| No | 10.1 | 6199 | 48.7 | 3190 | 38.6 |
|
| |||||
| Ever had emergency contraceptives | |||||
| Yes | 18.1 | 86 | 60.8 | 55 | 42.7 |
| No | 10.3 | 6435 | 49.4 | 3299 | 39.1 |
| Total | 10.4 | 6521 | 49.6 | 2354 | 39.2 |
∗Missing = 32.
By caste/ethnicity, the lowest use of contraceptive methods was observed among Muslims currently residing with husbands (32%), whereas the highest use was observed among hill Janajati (70%) (Table 2). Among the women whose husbands were away, the less likelihood of using contraceptives was observed among those who had an induced abortion in the last five years (13%) compared with those women who did not have any induced abortion (24%). In the adjusted model, age, number of living children, education, province, caste/ethnicity, and use of induced abortion in the last five years were associated with contraceptive use among those women whose husbands away (Table 4). No difference was found on the impact of the duration of separation (≤1 year vs > 1 year) on use of and unmet need for FP.
Table 4.
Factors associated with CPR (any method) and unmet need among cohabiting and noncohabiting women in Nepal, 2016.
| Women's characteristic | CPR (any method) | Unmet need | ||
|---|---|---|---|---|
| Cohabiting | Noncohabiting | Cohabiting | Noncohabiting | |
| Adjusted odds ratio∗ | aOR∗ | aOR∗ | aOR∗ | |
| Living children | ||||
| None | 1 | 1 | 1 | 1 |
| 1–2 | 7.03 (5.59–8.84) | 2.97 (1.74–5.06) | 1.95 (1.35–2.81) | 3.64 (2.73–4.85) |
| 3–4 | 12.90 (9.89–16.82) | 6.10 (3.41–10.91) | 2.26 (1.41–3.63) | 3.82 (2.73–5.34) |
| 5+ | 9.66 (6.92–13.49) | 4.25 (2.16–8.36) | 2.82 (1.60–4.98) | 5.39 (3.33–8.73) |
|
| ||||
| Age-groups (years) | ||||
| 15–19 | 1 | 1 | 1 | 1 |
| 20–24 | 0.97 (0.69–1.35) | 1.01 (0.56–1.83) | 0.60 (0.41–0.90) | 0.50 (0.36–0.70) |
| 25–29 | 1.24 (0.86–1.77) | 1.93 (1.10–3.38) | 0.53 (0.34–0.83) | 0.35 (0.25–0.51) |
| 30–34 | 1.83 (1.27–2.64) | 3.18 (1.73–5.86) | 0.32 (0.21–0.50) | 0.29 (0.20–0.43) |
| 35–39 | 2.21 (1.49–3.28) | 5.64 (3.03–10.50) | 0.25 (0.16–0.39) | 0.21 (0.14–0.31) |
| 40–44 | 1.84 (1.19–2.85) | 5.50 (2.87–10.53) | 0.26 (0.15–0.45) | 0.15 (0.09–0.25) |
| 45–49 | 1.00 (0.67–1.49) | 7.30 (3.47–15.34) | 0.31 (0.18–0.53) | 0.07 (0.04–0.13) |
|
| ||||
| Level of education | ||||
| No education | 1 | 1 | 1 | 1 |
| Primary | 0.92 (0.76–1.12) | 1.16 (0.86–1.57) | 1.05 (0.81–1.38) | 1.23 (0,95–1.59) |
| Secondary | 1.06 (0.86–1.32) | 1.43 (1.07–1.89) | 1.26 (0.97–1.64) | 1.32 (1.03–1.67) |
| Higher | 1.44 (1.02–2.02) | 1.45 (0.93–2.28) | 0.91 (0.59–1.39) | 0.97 (0.68–1.37) |
|
| ||||
| Place of residence | ||||
| Urban | 1 | 1 | 1 | 1 |
| Rural | 0.92 (0.77–1.08) | 1.10 (0.87–1.40) | 1.06 (0.85–1.31) | 1.04 (0.87–1.25) |
|
| ||||
| Province | ||||
| Province 1 | 1 | 1 | 1 | 1 |
| Province 2 | 0.69 (0.50–0.96) | 1.14 (0.69–1.91) | 0.90 (0.59–1.38) | 0.83 (0.57–1.21) |
| Province 3 | 0.76 (0.57–1.01) | 2.51 (1.42–4.44) | 1.07 (0.76–1.51) | 0.65 (0.42–1.03) |
| Province 4 | 0.77 (0.58–1.01) | 1.01 (0.62–1.63) | 0.92 (0.62–1.36) | 0.86 (0.60–1.22) |
| Province 5 | 0.63 (0.47–0.84) | 0.92 (0.58–1.45) | 1.49 (1.05–2.09) | 0.97 (0.70–1.33) |
| Province 6 | 0.77 (0.58–1.03) | 2.13 (1.25–3.61) | 1.13 (0.76–1.68) | 0.61 (0.41–0.91) |
| Province 7 | 0.81 (0.63–1.06) | 2.12 (1.38–3.25) | 0.77 (0.51–1.16) | 0.58 (0.41–0.83) |
|
| ||||
| Ecological zone | ||||
| Mountain | 1 | 1 | 1 | 1 |
| Hill | 0.95 (0.70–1.30) | 0.78 (0.44–1.37) | 1.12 (0.75–1.67) | 1.24 (0.77–2.00) |
| Terai | 0.97 (0.67–1.39) | 0.95 (0.48–1.88) | 1.08 (0.67–1.74) | 1.18 (0.70–2.00) |
|
| ||||
| Wealth quintile | ||||
| Poorest | 1 | 1 | 1 | 1 |
| Poorer | 1.66 (1.35–2.05) | 1.20 (0.82–1.76) | 0.61 (0.46–0.82) | 1.15 (0.84–1.57) |
| Middle | 1.73 (1.35–2.23) | 1.09 (0.72–1.65) | 0.63 (0.45–0.88) | 1.18 (0.87–1.61) |
| Richer | 1.54 (1.20–1.97) | 1.06 (0.65–1.74) | 0.69 (0.49–0.97) | 1.12 (0.81–1.57) |
| Richest | 1.91 (1.43–2.56) | 0.98 (0.52–1.85) | 0.71 (0.50–1.01) | 1.41 (0.88–2.25) |
|
| ||||
| Caste/ethnicity | ||||
| Hill Brahmin | 1 | 1 | 1 | 1 |
| Hill Chhetri | 0.85 (0.64–1.14) | 1.07 (0.69–1.66) | 1.20 (0.82–1.75) | 1.05 (0.75–1.46) |
| Terai Brahmin/Chhetri | 0.77 (0.43–1.37) | 1.57 (0.57–4.31) | 1.35 (0.69–2.64) | 0.46 (0.23–0.90) |
| Other Terai caste | 0.52 (0.34–0.79) | 3.17 (1.85–5.43) | 1.54 (0.93–2.57) | 0.33 (0.21–0.52) |
| Hill Dalit | 0.96 (0.71–1.30) | 1.59 (1.01–2.49) | 1.79 (1.15–2.78) | 0.98 (0.67–1.43) |
| Terai Dalit | 0.41 (0.24–0.70) | 2.12 (1.07–4.19) | 1.95 (1.11–3.43) | 0.37 (0.22–0.61) |
| Newar | 0.73 (0.43–1.22) | 2.61 (1.00–6.84) | 1.87 (1.03–3.41) | 0.75 (0.36–1.58) |
| Hill Janajati | 0.94 (0.72–1.23) | 1.45 (0.94–2.24) | 1.21 (0.81–1.82) | 1.00 (0.75–1.35) |
| Terai Janajati | 1.27 (0.87–1.86) | 4.32 (2.55–7.31) | 0.69 (0.40–1.19) | 0.39 (0.25–0.60) |
| Muslim | 0.20 (0.13–0.31) | 1.01 (0.50–2.02) | 2.57 (1.45–4.53) | 0.41 (0.25–0.67) |
|
| ||||
| Had an abortion in the last five years | ||||
| No | 1 | 1 | 1 | 1 |
| Yes | 1.08 (0.74–1.56) | 0.42 (0.26–0.68) | 1.62 (1.06–2.47) | 1.65 (1.14–2.39) |
|
| ||||
| Ever had emergency contraceptives | ||||
| No | 1 | 1 | 1 | 1 |
| Yes | 0.79 (0.41–1.50) | 1.59 (0.57–4.39) | 2.02 (0.91–4.49) | 1.28 (0.56–2.91) |
∗All the variables presented are included in the model.
In the multivariate model, maternal age, number of living children, education, province, wealth quintile, and caste/ethnicity were associated with contraceptive use among those currently residing with husbands (Table 4). The higher likelihood of contraceptive use was observed among those currently residing with husbands with higher education than the participants with no education (aOR:1.44; 95% CI: 1.02–2.02). Significantly lower contraceptive use was observed among women reporting an induced abortion in the last five years and whose husbands were currently away (aOR:0.42; 95% CI: 0.26–0.68). Reporting of ever use of emergency contraception was not significantly associated with the lower use of contraceptives (any method) both among cohabiting and noncohabiting couples.
Similarly, maternal age, number of living children, province, wealth quintile, caste/ethnicity, and use of induced abortion services in the last five years were associated with unmet need among women currently residing with husbands (Table 4). An inverse relationship of age with the unmet need was observed. Similarly, age, number of living children, education, province, caste/ethnicity, and use of induced abortion services in the last five years were associated with unmet need among women whose husbands were away (Table 4). A strong negative association of spousal separation with contraceptive use was observed (aOR:0.14; p < 0.001) after controlling other covariates, whereas a positive association was observed with unmet need (aOR:8.00; p < 0.001) (data not shown in table).
4. Discussion
Our aim in this study was to study the effect of spousal separation on use of and unmet need for contraceptives in Nepal. The analysis revealed that although family planning use (any method) has slightly increased or leveled off with the any MWRA group, there is an increment of 11% (from 57% in 2006 to 68% in 2016)—with an approximate rise of 1% annually among the cohabiting couples. The overall CPR is 53% among any MWRA, while this rate is much higher at 68% among the cohabiting couples as shown by the NDHS 2016 [4]. Likewise, unmet need for family planning among any MWRA is 24%, whereas this is only 10% among the cohabiting couples. This shows that although overall unmet need remained almost constant between 2006 and 2016, it has decreased by 6% among the cohabiting couples. These findings clearly suggest that presenting aggregate information (without disaggregating the rates with status of cohabitation) on contraceptive use and unmet need can be misinterpreted, which can ultimately affect the appropriate use of scarce resources and prioritization of the family planning program within the neediest population subgroups of the entire MWRA age range. On the other hand, increasing share of the traditional method among the cohabiting couples (4.7% in 2006 to 13.8% in 2016) [4, 5] is another factor to be considered to examine whether this has indeed affected the fertility structure and has not led to increasing unintended pregnancies.
Nepal's labour-related out-migration is male dominated, even though the number of female migrants has seen a rise in recent years. In 2013/2014 alone, of 521,878 total labour migrants, a majority was males (94.5%) [7]. Additionally, a significant number of men and women work in India, who are more likely to be undocumented because of open border policy between India and Nepal [8]. Approximately 8% of Nepalese were out of the country as shown by the 2011 household census, and majority of the out-migrants were of reproductive age [9].
There is a complex and dynamic relationship between migration and fertility. Much of the literature discusses the “fertility-depressing effect” of spousal separation for a short term [10–13]. The fertility depression effect is described as having a reduced fertility rate. Some argue that the fertility-depressing effect is expected to be higher (or more visible) in areas of high fertility and low contraceptive use [13] and also depends on the duration of separation and postpartum amenorrhea [14]. While others argue that migration can result in increased fertility because of higher coital frequency after return from migration [15]. A study from Mozambique revealed that wives of successful migrants were more likely to use modern contraceptives than wives of nonmigrants or less successful migrants [13], thus validating the principle of selective hypothesis [14]. The selective hypothesis proposes that migrants are self-selective groups who consciously control marriage and prefer fewer children [16]. Furthermore, the use of contraceptives when husband is away may depend on service accessibility, sociocultural factors, and women's autonomy. One recent study from Nepal documents that young couples are delaying plan to have a child due to strong socioeconomic pressure [2]. The study explored young couples becoming more conscious to not to bear a child before having themselves economically empowered—which in most cases was to migrate to industrial/developed countries for job opportunities due to increasing unemployment rates at the home country. Increasing aspirations to provide quality education to their kids, the cost of health care, and responsibility to take care of old family members back home has pushed today's youths to migrate out of the country—with Gulf countries becoming the top destination. It appears that migration to countries other than India (which used to be the top destination before) have delayed childbearing because of relatively longer spousal separation. On the other hand, rising general literacy and exposure due to migration must have created an immense pressure on young couples to limit their family size as they become more aware and sensitive about their future and resources needed to plan a family well. With a recent trend of female migration, the study also identified that recently married couples who had unintended pregnancy even opted for abortion, besides economic pressure, which to some extent could have been eased by the legalized and accessible abortion services in Nepal [17]. Furthermore, breakdown of the traditional family structure with a move towards nuclear family might have been another factor behind why couples today plan for a less number of children. With a joint family structure, it is natural that couples have always grandparents and other family members to take responsibility for raising a child. However, recently, this is becoming a less common phenomenon in Nepal. Considering all of these sociocultural factors, we add into the argument that the fertility structure should be seen as a complex and dynamic indicator. Analysis of the impact of spousal separation is the beginning of it, thus moving further from simply concluding the fertility structure as an outcome of a nation's contraceptive prevalence rate.
A large difference in contraceptive use (any method) by husband's cohabitation status among women from well-off groups (higher education and higher wealth quintiles) than those with less education and lower wealth quintile suggests these groups have a higher tendency to refrain from using contraceptives when their husbands are away. Thapa et al. (2014) found that improvements in knowledge and awareness of legalization of abortion, circumstances in which abortion is allowed, and places to obtain services were largely limited among women with higher education and higher wealth quintile [17]. It was estimated that 137,000 legal and over 186,000 illegal abortions were conducted in 2014 in Nepal [18] and figure continue to rise annually [19]. Given the easy availability of surgical and medical abortion in Nepal, educated and wealthy women could have misused abortion service as a means of family planning. Even though the current analysis did not show any association of the ever use of emergency contraceptives with the current use of contraceptives (any method) or unmet need for family planning both among cohabiting and noncohabiting women, over-the-counter availability of emergency contraceptives (ECPs) has proved to be popular among young and educated women in Nepal [20]. ECP use is often under-reported in household surveys such as DHS [20]. Hence, for many noncohabiting women, abortion services and emergency contraceptives could have been the means for meeting fertility regulation needs in Nepal.
This study also found the significantly lower contraceptive use and higher unmet need for family planning among those who had had an induced abortion in the last five years and whose husbands were currently away. A study among women who received surgical abortion in Kathmandu showed that one in five women who had an abortion left the facility without using the family planning method [21]. Almost one-third of the abortion users had a repeat abortion. Regular provision of a range of contraceptives and availability of effective counseling are lacking in many health facilities and clinics in Nepal [21]. Women whose husbands are away experience societal and familial pressure not to use contraceptives. When unplanned pregnancy occurs—either due to husband's unplanned arrival or due to extramarital relationship—abortion becomes the ultimate resort to end unintended pregnancy, which often results in repeated abortions.
Results from multivariate logistic regression showed that age, number of living children, education, province, wealth quintile, and caste/ethnicity were associated with contraceptive use. Increasing age and the higher number of living children were associated with higher chances of using family planning methods. The relative strength of association of increasing age (after 30 years) with the use of modern contraceptives compared with those aged 15–19 years was lower among cohabiting couples than couples living separately. Lindstorm and Giorguli argue that migration has an impact on timing of the first birth and subsequent birth patterns [11]. Cohabiting young couples (15–19 years) may be more likely to delay childbearing by using contraceptives than young couples who separate after marriage. Young couples who live separately might face familial/societal pressure to have children before they separate; however, this needs further investigation.
A significant association was observed between higher levels of education (primary, secondary, and higher) and use of modern methods among cohabiting couples. Given that access to education has increased over time, age-group needs to be taken into account when looking at the relationship between education and use of contraceptives. Additionally, NDHS 2016 found that women with higher education and cohabiting couples were more likely to use traditional methods than those with lower education and couples living separately [4].
4.1. Policy Implications
Nepal's case is unique in terms of reduction in total fertility from 4.1 in 2001 to 2.3 in 2016—a reduction of 2 children per women within 15 years' period. The overall status of CPR and unmet need do not fully explain this transition without examining the disaggregated data on contraceptive use and unmet need for family planning by cohabitation status. A further analysis of the NDHS 2011 data revealed that spousal separation played a major role in the reduction of TFR from 3.1 births per women in 2006 to 2.6 per women in 2011 [5].Therefore, it is important to present information on contraceptives use by disaggregating with respect to spousal separation. Furthermore, regular monitoring of family planning indicators according to spousal separation is necessary as the migration trends change. Such a monitoring can help program managers see a real effect of family planning-related interventions and help allocate scarce resources appropriately. Although slightly different from the focus of this study, the growing evidence of the lower birth rate and infertility among migrant couples [22] warrants a major policy reform to manage labour-related migration trend from Nepal to maintain a desired population structure.
4.2. Implications for Program
The family planning needs differ significantly between cohabiting and noncohabiting couples. One cannot deny the occurrence of sexual activity among separately living couples [23]. Additionally, spouses need adequate planning in situations where the husband's return is unannounced [1]; therefore, family planning interventions should cater the need of spouse of migrant labours through educational messages such as related to the fertility period, and provision of family planning services. In addition, program should also cater to the needs of specific subgroups such as temporarily separated couples who will be reunited later and couples from different caste/ethnic groups where family planning uptake is very low (Muslims and Terai Dalits) [5].
4.3. Future Research Recommendations
We know very little about the family planning needs of migrant population and their spouses. The DHS surveys do not adequately capture fertility desire, unmet need for family planning, and current use of family planning among this population [23]. It is not clear whether spouses of migrants have a lower need for family planning services due to lower coital frequency, whether their complex family planning needs are not being met, or whether emergency contraception or abortion is turning out as a means of family planning. Hence, in-depth qualitative studies are needed to further understand fertility desires, facilitators, and barriers for contraceptive use among spouses of labour migrants in Nepal.
5. Conclusion
This study confirms earlier findings by Ban et al. 2012 [1] and Khanal 2013 [5] that spousal separation remains a significant explanatory factor in the use of and unmet need for contraception in Nepal. Among noncohabiting couples, CPR (any method) was at 24%, which is 44 percentage points lower than among the cohabiting couples who had a CPR of 68%. The unmet need for family planning was 50% among noncohabiting couples, while it was 10% among cohabiting couples. This study found that use of family planning methods has increased at a rate of almost 1% per year (between 2006 and 2016) among cohabiting couples, although the overall use of family planning methods seems to have leveled off or slightly increased among total MWRA in Nepal. The labour migration being a significant and indispensable socioeconomic phenomenon for Nepal, it is necessary to monitor fertility patterns and contraceptive use by cohabitation status in order to ensure that the national family planning interventions are targeted to address the contraceptive and fertility needs of the migrant couples.
Acknowledgments
The authors would like to acknowledge the DHS Programme for providing the data sets.
Data Availability
The data used in this study are available at https://www.dhsprogram.com.
Ethical Approval
The 2016 Nepal Demographic and Health Survey protocol received ethical approval from the Nepal Health Research (NHRC)–Ethical Review Board and ICF Institutional Review Board.
Disclosure
All the views expressed in this article are entirely the personal opinion of the authors, and this does not necessarily reflect the views of agencies to which they are affiliated.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- 1.Ban B., Karki S., Shrestha A., Hodgins S. Spousal separation and interpretation of contraceptive use and unmet need in rural Nepal. International Perspectives on Sexual and Reproductive Health. 2012;38(01):043–047. doi: 10.1363/3804312. [DOI] [PubMed] [Google Scholar]
- 2.Thapa N., Paudel M., Guragain A. M., et al. Status of Migration and Socio-Reproductive Impacts on Migrants and Their Families Left behind in Nepal. Kathmandu, Nepal: Migration and Development; 2019. [Google Scholar]
- 3.Mehata S., Baral S., Chand P., Singh D., Poudel P., Barnett S. Nepal Household Survey 2012. Kathmandu, Nepal: 2013. [Google Scholar]
- 4.Ministry of Health and Population (MoHP) Nepal, New ERA, and ICF International Inc. Nepal Demographic and Health Survey 2016. Kathmandu, Nepal: Ministry of Health and Population; 2017. [Google Scholar]
- 5.Khanal M. N. Impact of Male Migration on Contraceptive Use, Unmet Need, and Fertility in Nepal: Further Analysis of the 2011 Nepal Demographic and Health Survey. Kathmandu, Nepal: Ministry of Health and Population; 2013. [Google Scholar]
- 6.Karandikar S., Coles L., Jayawant S., Kemp A. M. The neurodevelopmental outcome in infants who have sustained a subdural haemorrhage from non-accidental head injury. Child Abuse Review. 2004;13(3):178–187. doi: 10.1002/car.850. [DOI] [Google Scholar]
- 7.Ministry of Labour and Employment Government of Nepal. Labour Migration for Employment, A Status Report for Nepal: 2013/14. Kathmandu, Nepal: 2014. [Google Scholar]
- 8.Gartaula H. N., Niehof A. Migration to and from the terai: shifting movements and motives. The South Asianist. 2013;2(2):28–50. [Google Scholar]
- 9.Central Bureau of Statistics Nepal. National Population and Housing Census, 2011. 2012. [Google Scholar]
- 10.Clifford D. Spousal separation, selectivity and contextual effects: exploring the relationship between international labour migration and fertility in post-Soviet Tajikistan. Demographic Research. 2009;21:945–975. doi: 10.4054/demres.2009.21.32. [DOI] [Google Scholar]
- 11.Lindstrom D. P., Giorguli Saucedo S. The interrelationship of fertility, family maintenance and Mexico-U.S. Migration. Demographic Research. 2007;17:821–858. doi: 10.4054/demres.2007.17.28. [DOI] [Google Scholar]
- 12.Lindstrom D. P., Saucedo S. G. The short- and long-term effects of U.S. migration experience on Mexican women’s fertility. Social Forces. 2002;80(4):1341–1368. doi: 10.1353/sof.2002.0030. [DOI] [Google Scholar]
- 13.Agadjanian V., Yabiku S. T., Cau B. Men’s migration and women’s fertility in rural Mozambique. Demography. 2011;48(3):1029–1048. doi: 10.1007/s13524-011-0039-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Millman S. R., Potter R. G. The fertility impact of spousal separation. Studies in Family Planning. 1984;15(3):121–126. doi: 10.2307/1965462. [DOI] [PubMed] [Google Scholar]
- 15.Omondi D., Ochola C. Migration and fertility relationship: a case study of Kenya. African Population Studies. 2003;18(1):97–113. [Google Scholar]
- 16.Jingyue Z. The influence of migration on Chinese Korean Women’s Fertility Behavior. Studies in Asian Social Science. 2016;3(1):10–20. doi: 10.5430/sass.v3n1p10. [DOI] [Google Scholar]
- 17.Thapa S., Sharma S. K., Khatiwada N. Women’s knowledge of abortion law and availability of services in Nepal. Journal of Biosocial Science. 2014;46(2):266–277. doi: 10.1017/s0021932013000461. [DOI] [PubMed] [Google Scholar]
- 18.Puri M., Singh S., Sundaram A., Hussain R., Tamang A., Crowell M. Abortion incidence and unintended pregnancy in Nepal. International Perspectives on Sexual and Reproductive Health. 2016;42(4):p. 197. doi: 10.1363/42e2116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ministry of Health Nepal. Annual Report, Department of Health Services 2074/2075 (2017/2018) Kathmandu, Nepal: Ministry of Health; 2019. [Google Scholar]
- 20.Thapa S. A new wave in the quiet revolution in contraceptive use in Nepal: the rise of emergency contraception. Reproductive Health. 2016;13(1):p. 49. doi: 10.1186/s12978-016-0155-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Thapa S., Neupane S. Risk factors for repeat abortion in Nepal. International Journal of Gynecology & Obstetrics. 2013;120(1):32–36. doi: 10.1016/j.ijgo.2012.07.016. [DOI] [PubMed] [Google Scholar]
- 22.Khan N. N. Seasonal migration induced spousal separation and infertility: growing evidences demand significance in developing countries. International Journal of Perceptions in Public Health. 2017;1(4):215–217. [Google Scholar]
- 23.Khan R., MacQuarrie K., Nahar Q., Sultana M. The men are away: pregnancy risk and family planning needs among women with a migrant husband in Barisal, Bangladesh. 2016;(98) doi: 10.1080/26410397.2022.2097044. DHS Further Analysis Reports. [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used in this study are available at https://www.dhsprogram.com.