

Abstract
In China, national regulations and standards for health care waste management were implemented in 2003. To investigate the current status of health care waste management at different levels of health care facilities (HCF) after the implementation of these regulations, one tertiary hospital, one secondary hospital, and four primary health care centers from Binzhou District were visited and 145 medical staff members and 24 cleaning personnel were interviewed.
Generated medical waste totaled 1.22, 0.77, and 1.17 kg/bed/day in tertiary, secondary, and primary HCF, respectively. The amount of medical waste generated in primary health care centers was much higher than that in secondary hospitals, which may be attributed to general waste being mixed with medical waste. This study found that the level of the HCF, responsibility for medical waste management in departments and wards, educational background and training experience can be factors that determine medical staff members’ knowledge of health care waste management policy. Regular training programs and sufficient provision of protective measures are urgently needed to improve occupational safety for cleaning personnel. Financing and administrative monitoring by local authorities is needed to improve handling practices and the implementation of off-site centralized disposal in primary health care centers.
1. Introduction
Health care waste management is a crucial public health and environmental issue. According to a survey of the World Health Organization (WHO) on health care waste management in 22 developing countries, the proportion of health care facilities (HCF) with inappropriate waste disposal methods was between 18% and 64% (WHO, 2005). To improve health care waste management, several previous studies in developing countries indicated the importance of a national regulatory framework (Askarian et al., 2004, Massrouje, 2001, Phengxay et al., 2005, Shinee et al., 2008), a sound internal management system and training program for related personnel (Abdulla et al., 2008, Da Silva et al., 2005, Mohee, 2005, Danchaivijitr et al., 2005), estimation of health care waste generated (Bdour et al., 2007, Tsakona et al., 2007) and appropriate techniques for disposal (Diaz et al., 2005, Lee et al., 2004, Rogers and Brent, 2006) . The WHO provided HCF with comprehensive guidelines on safe, efficient, and environmentally sound methods of health care waste handling and disposal (Prüss et al., 1999).
In China, health care waste management is in need of improvement. A previous study found that in the northwestern Gansu Province of China, approximately 80% of all medical waste was mixed with general waste (Wu et al., 2005). Experts working in five of China’s northwestern provinces also reported the same problems (Kobayashi et al., 2002). Since an outbreak of severe acute respiratory syndrome (SARS) in early 2003, the government has been aware that health care waste management could be crucial to emerging disease preparedness and infection control. The State Council adopted Regulations on Medical Waste Management in June 2003 (MoH of China, 2003), which are the country’s first regulations on medical waste management. Later, a series of regulations and standards consisting of classification, treatment procedures, occupational safety, and internal policies and administration were promulgated.
The WHO guidelines indicated the necessity for review of the national program to manage health care waste after their implementation. However, no studies investigated the implementation of national regulations at different levels of HCF in China after 2003. The objectives of this case study were: to explore the current status of health care waste management in terms of handling practices, occupational safety, and internal policies and administration; to assess the amount of health care waste generated from tertiary, secondary, and primary HCF; to examine medical staff members’ knowledge of health care waste management policy; and to understand cleaning personnel’s self-practices and protective measures regarding occupational safety in Binzhou District, Shandong Province, China.
2. Methods
This study was a case study in Binzhou District, Shandong Province performed from December 2006 to January 2007. Binzhou District is one of 17 administrative districts including one city (urban area) and six countries (mostly rural areas). In 2005, the district’s per capita GDP was 18,031 RMB (approximately 2,200 US dollars) and its population was 3,712,500. There are a total of 142 HCF in Binzhou District. This study only focused on general hospitals and health care centers because they covered most types of health care services, produced a variety of health care wastes, and could be compared using the same standards. Traditional Chinese medicine hospitals and specialist hospitals (maternal and child, cancer, injury, infectious disease, rehabilitation, etc.) were excluded. This case study involved visits to a total of six HCF: one tertiary hospital, one secondary hospital, and four primary health care centers. In that HCF, 145 medical staff members (randomly selected from a total of 1636 individuals) and all 24 cleaning personnel were interviewed.
To determine the general status of health care waste management at every HCF, in-depth interviews were conducted with waste management officers or infection control officers. A semi-structured questionnaire was designed based on national regulations for health care waste management and the WHO’s rapid assessment tool (2004). It included handling practices in separation, collection, transport, storage, and final disposal of waste; occupational education and safety for related personnel; and internal policies and administration. Additionally, there was an open-ended question on the final page of the questionnaire asking officers to discuss issues regarding health care waste management in detail in order to identify detailed issues related to current health care waste management in HCF. Observation of departments/wards, storage locations, handling practices, equipment, and records of the handling process was also undertaken in order to verify the interview data.
To assess amounts of health care waste generated in health care centers and in tertiary and secondary hospitals, the weight of health care waste was measured just before cleaning personnel visited departments and wards to collect the waste. In primary health care centers, weight was measured in the storage location (or a temporary storage room) just before final disposal because of lack of management of collection and on-site transport at those facilities. Measurements were made daily for one week. Responding staff members (doctors or nurses) in departments/wards and primary health care centers were asked to fill out a sheet that included the daily number of patients, number of beds, and amounts of health care waste during the study period. Based on those data, the generation rate (kg/bed/day) and the daily amount of health care waste generated from each level of HCF were calculated.
To examine medical staff members’ knowledge of health care waste management policy, questions and answers were designed through discussions with experts from the study site because no similar study has been conducted in China. Those questions included six items: categories of health care waste (including infectious, sharps, pathological, chemical, pharmaceutical, and radioactive wastes), bio-hazard markings, related national regulations, internal policies, storage location in the HCF, and use of a consignment note system (a set of sheets recording the amount of waste, its content, and the complete handling process). The questionnaire also asked about training experience. An open-ended portion was included at the end of each question to encourage the participants to explain their knowledge of the question in as much detail as possible in order to accurately score the answer based on master answers designed in advance and to comprehensively ascertain their level of understanding.
A semi-structured questionnaire for cleaning personnel included items on their self-protective practices, attitudes towards self-protective practices, training experience, protective measures, and guidance provided by the HCF.
Quantitative data were analyzed with SPSS version 13.0 statistical software. Descriptive analysis and a non-parametric test were used on quantitative data. The K.J. Method, a direct qualitative analysis method designed by the Japanese ethnologist Kawakita (1975), was applied to qualitative data. All issues regarding health care waste management in HCF that were brought up in interviews with officers were listed, and then a card was made for each issue mentioned and these were grouped with similar ideas. Then, the groups were arranged into a relationship model with a logical order.
The ethical committees for research of the University of Tokyo and Shandong University approved this study and ethical permission was obtained from each HCF. All participants were informed about the study procedures and the investigation was conducted after their informed consent was obtained.
3. Results
Regarding the current status of health care waste management, results of interviews with waste management officers or infection control officers and observations are summarised in Table 1 .
Table 1.
Handling practices, occupational safety, internal policies and administration in HCF
| Tertiary n = 1 | Secondary n=1 | Primary n = 4 | |
|---|---|---|---|
| Handling practices | |||
| Separation | 1/1 | 1/1 | 2/4 |
| Special containers with bio-hazard markings | 1/1 | 1/1 | 4/4 |
| Special tools for collection and transport | 1/1 | 1/1 | 1/4 |
| Special route for collection and transport | 1/1 | 1/1 | 0/4 |
| Special time for collection and transport | 1/1 | 1/1 | 4/4 |
| Establishment of a storage location | 1/1 | 1/1 | 3/4 |
| Sealed containers in storage location | 1/1 | 1/1 | 3/4 |
| Protective measures in storage location | 1/1 | 1/1 | 1/4 |
| Complete records of handling procedures | 1/1 | 1/1 | 0/4 |
| Consignment note system | 1/1 | 1/1 | 0/4 |
| Final disposal | Off-site | Off-site | On-site |
| Occupational safety | |||
| Training for related personnel | 1/1 | 1/1 | 4/4 |
| Health checks and vaccination for all personnel | 1/1 | 0/1 | 0/4 |
| Provision of protective equipment | 1/1 | 1/1 | 1/4 |
| Internal policies and administration | |||
| Internal plan | 1/1 | 1/1 | 4/4 |
| Handling manuals | 0/1 | 0/1 | 0/4 |
| Management sector | 1/1 | 1/1 | 4/4 |
| Waste management team | 1/1 | 1/1 | 3/4 |
| Regular supervision of the health agency | 1/1 | 1/1 | 4/4 |
| Regular supervision of the hospital director | 1/1 | 1/1 | 3/4 |
3.1. Handling practices and final disposal of health care waste
Secondary and tertiary hospitals separated different categories of health care waste right after production, used special containers with bio-hazard markings and special tools for collection and transport, and arranged special routes and times for collection and transport. In terms of storage, all secondary and tertiary hospitals established a storage location, used sealed containers, and provided various protective measures against rats, theft, and emergencies such as spillage and leakage. Conversely, some primary health care centers had domestic waste mixed in with health care waste in the separation and collection process and lacked containers and tools for handling. Only one primary health care center had a storage location with complete protective measures.
Tertiary and secondary hospitals contracted with a regional centralized disposal facility for final disposal. Conversely, primary health care centers did not implement centralized disposal. Rather, all surveyed primary HCF used a small-scale incinerator for on-site burning. Moreover, in primary HCF, health care waste was often observed to be mixed with domestic waste or discarded in the back or nearby.
In Shandong Province, the regional centralized disposal facility was run by Ke–Lin Solid Waste Disposal Co. Ltd., a private company authorized by the local Environment Bureau and operated since April 2006. The company collected and transported health care waste generated by HCF and finally disposed of it by large-scale incineration, disinfection, and placement in a landfill. The standard disposal fee was 2 RMB/bed/day (approximately 0.26 US dollars/bed/day). Payment for the disposal varied among HCF; some charged patients a user fee while others bore the full cost themselves.
3.2. Occupational education and safety aspects
All HCF had a training program for personnel involved in health care waste treatment, although the components differed among HCF: primary health care centers provided only a simple orientation for new employees while the training program in tertiary and secondary hospitals was much more varied, including orientation for new employees, regular training, and special lectures. Health checks and vaccinations in secondary and primary HCF and provision of protective measures in primary health care centers were found to be deficient.
3.3. Internal policies and administration of health care waste management
Following national regulations, all secondary and tertiary hospitals formulated an internal plan for health care waste management and organized a health care waste management team involving related professionals such as hospital directors, infection control officers, directors of departments and wards, senior nurses, and medical technicians. Supervision by the local government and the hospital director regularly occurred in most HCF surveyed. That said, no HCF had waste handling manuals with detailed guidelines for related personnel.
3.4. Assessment of health care waste generated
The total amount of health care waste generated each day was 1064.27, 123.33, and 41.09 kg per tertiary, secondary, and primary HCF, respectively. Based on the total amounts of waste generated and the number of beds, the average health care waste generation was 1.22, 0.77, and 1.17 kg/bed/day, in tertiary, secondary, and primary HCF, respectively (Table 2 ).
Table 2.
Amount of medical waste generated by HCF
| HCF | Medical waste generated per day (kg) | Number of beds | Rate of medical waste generation (kg/bed/day) |
|---|---|---|---|
| Tertiary | 1064.27 | 870 | 1.22 |
| Secondary | 123.33 | 160 | 0.77 |
| Primary | 41.09 | 35 | 1.17 |
3.5. Medical staff members’ knowledge of health care waste management
Questions about medical staff members’ knowledge of health care waste management policy included six items and each was allotted one point for a correct answer. Then, the scores were calculated and compared among different groups of medical staff members. The total score for knowledge ranged from 0 to 6. According to a histogram and the Kolmogorov–Smirnov test, the score did not follow a normal distribution, so the median of the score was compared by non-parametric tests instead of the average by a t-test. Table 3 shows that medical staff members from secondary and tertiary HCF (p < 0.001, by a Kruskal Wallis test), senior nurses (p < 0.001, by a Kruskal Wallis test), health care waste management staff members in departments or wards (p = 0.001, by a Mann–Whitney U test), those with a junior college education or above (p = 0.001, by a Mann–Whitney U test), and those receiving regular training (p < 0.001, by a Mann–Whitney U test) tended to have a better understanding of health care waste management policy.
Table 3.
Medical staff members’ knowledge of medical waste management policy
| Knowledge items (score range: 0 ∼ 6) | (1) Categories of medical waste;(2) bio-hazard markings;(3) national regulations;(4) internal policies;(5) storage location;(6) consignment note system | ||
|---|---|---|---|
| Frequency | Median (IQR: 25%–75%) | p | |
| Level | <0.001a | ||
| Tertiary | 76 | 6 (4.25–6.00) | |
| Secondary | 38 | 5 (4.00–6.00) | |
| Primary | 31 | 1 (1.00–2.00) | |
| Profession | <0.001a | ||
| Senior nurse | 18 | 6 (5.75–6.00) | |
| Nurse | 38 | 5 (4.75–6.00) | |
| Doctor | 70 | 4 (2.00–6.00) | |
| Other | 19 | 3 (1.00–6.00) | |
| Responsibility for medical waste management | 0.001b | ||
| Yes | 13 | 6 (6.00–6.00) | |
| No | 132 | 5 (3.00–6.00) | |
| Education | |||
| Junior college graduate and above | 108 | 5 (4.00–6.00) | 0.001b |
| High school or less | 37 | 3 (1.00–5.50) | |
| Training | <0.001b | ||
| Yes | 117 | 5 (4.00–6.00) | |
| No | 28 | 2 (1.00–3.75) | |
| Total | 145 | 5 (3.00–6.00) | |
By Kruskal Wallis test.
By Mann–Whitney U test.
3.6. Cleaning personnel’s self-protective practices and protective measures
Most of the 24 cleaning personnel interviewed were irregularly employed as part-time or short-term workers and had a low level of education. As shown in Table 4 , 29.2% did not receive training before starting work and 8.3% did not receive protective equipment provided by the HCF. As many as 79.2% did not receive any vaccinations before work and 62.5% did not receive regular health checks in the workplace; 33.3% were not aware of the hazardousness of the work.
Table 4.
Cleaning personnel’s protective measures and occupational safety
| N = 24 | Percentage (%) | ||
|---|---|---|---|
| Education | |||
| Primary school or below | 15 | 62.5 | |
| Junior high school | 9 | 37.5 | |
| High school or above | 0 | 0.0 | |
| Experience with a sharps injury | |||
| Yes | 8 | 33.3 | |
| No | 16 | 66.7 | |
| Wear a mask | |||
| Yes | 22 | 91.7 | |
| No | 2 | 8.3 | |
| Wear gloves | |||
| Yes | 24 | 100 | |
| No | 0 | 0.0 | |
| Provided protective materials by HCF | |||
| Yes | 22 | 91.7 | |
| No | 2 | 8.3 | |
| Training before work | |||
| Yes | 17 | 70.8 | |
| No | 7 | 29.2 | |
| Vaccination | |||
| Yes | 5 | 20.8 | |
| No | 19 | 79.2 | |
| Health checks in the workplace | |||
| Yes | 9 | 37.5 | |
| No | 15 | 62.5 | |
| Hazardous work | |||
| Yes, I think so. | 16 | 66.7 | |
| No, not especially. | 8 | 33.3 | |
3.7. Issues regarding management systems in HCF as brought up in interviews
Besides quantitative data, results of interviews of officers with open-ended questions were summarized into a relationship model (Fig. 1 ). In tertiary and secondary hospitals, officers mentioned the positive effect of national regulations on the establishment of a management system. They felt that financial investment in internal storage locations, equipment, occupational education, and final disposal had increased, contributing to the improvement of management. In contrast, officers from primary health care facilities said such investment was beyond the affordability of their institutions and remained an obstacle to the improvement of management. Most participants also mentioned compliance with national regulations as a priority for the future.
Fig. 1.
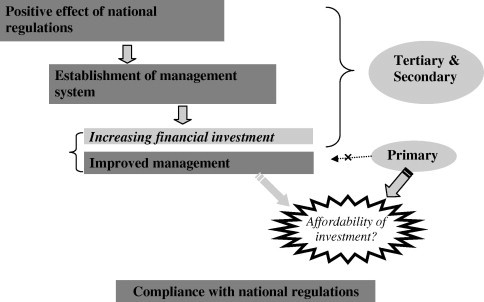
Summary of issues regarding management systems at HCF as brought up in interviews.
4. Discussion
This study found that the implementation of a management system based on national regulations differed among HCF visited: tertiary and secondary hospitals fully complied with national regulations; in contrast, primary health care centers had a number of problems such as poor waste separation, lack of equipment, unsanitary storage locations, deficient protective measures, and unsafe on-site disposal. According to interviews, the implementation of the management system was accompanied by increasing financial investment in internal storage locations, equipment, occupational education, and final disposal that were beyond the affordability of most primary health care centers. With health system reform based on a market economy, governmental subsidies to HCF have decreased, causing severely limited financial resources in primary health care centers (Liu et al., 1995). This may explain the poor performance of primary health care centers and suggests that local authorities should financially subsidise primary health care centers.
Moreover, primary health care centers still dispose of health care waste by incineration on-site. When the operating temperature is below 800 °C, the incinerator can produce dioxins, furans, or other toxic pollutants (WHO, 2005). Incinerators were operated by poorly trained workers. Operations did not comply with standards related to environmental protection. Health care waste was often observed to be inappropriately discarded or mixed with domestic waste, creating a high potential risk to public health and the environment. Results confirmed the advantage of off-site disposal in terms of administrative monitoring and supervision: tertiary and secondary hospitals implementing off-site centralized disposal had completed consignment notes with which the local environment agency was able to monitor the management system and handling processes; conversely, primary health care centers disposed of health care waste on-site and had no records. This could be attributed to lax monitoring of these health care centers by local authorities.
The WHO directed that the selection of disposal methods should be based on local circumstances (Prüss et al., 1999). The advantages of centralized regional disposal facilities are greater cost-effectiveness for larger units, easier disposal on a regional basis and supervision and monitoring by the government, and better assurance of more environment-friendly operations. However, Prüss et al. (1999) also pointed out that on-site disposal is particularly appropriate in areas where HCF is situated far from each other and the road system is poor. For cost-effectiveness, a previous study in South Africa recommended, based on trial and experience, that rural primary HCF use on-site small-scale incinerators for disposal (Rogers and Brent, 2006). Appropriate methods of disposal in primary health care centers remain a subject for further study.
The amount of health care waste generated in the HCF surveyed was generally consistent with the range of the data from previous studies in developing countries, including 0.57 kg/bed/day in Brazil (Da Silva et al., 2005), 1.6 kg/bed/day in India (Patil and Shekdar, 2001), 1.25 kg/bed/day in Iran (Askarian et al., 2004), 0.5–2.2 kg/bed/day in Jordan (Abdulla et al., 2008), and 0.47 kg/bed/day in Mauritius (Mohee, 2005). The amount of health care waste generated in high-level HCF was highest in tertiary hospitals, which can be mainly attributed to the various types and ranges of health care services provided (Bdour et al., 2007). The amount of such waste was much higher in primary health care centers (1.17 kg/bed/day) than in secondary hospitals, which coincides with a previous study in Laos PDR (Phengxay et al., 2005). The current study found that this larger amount can be attributed to domestic waste being mixed with health care waste in the separation and collection process. In this study, specialist hospitals and traditional Chinese medicine hospitals were excluded because of the different types of health care services, thus resulting in a differing content of health care waste which may have prohibited comparison. In future, a similar study will be conducted at such hospitals.
The results of medical staff members’ knowledge of health care waste management policy suggested that the level of the HCF, professionals involved, responsibility for health care waste management, and training experience can be associated factors. Better understanding of health care waste management policy of medical staff members at tertiary and secondary hospitals can be attributed to the greater variety of training programs at those facilities. The results also confirmed that medical staff members involved in the management of medical activities, such as senior nurses and members dealing with health care waste management in departments and wards, had a better understanding of related knowledge because they had the opportunity to acquire adequate information and knowledge (Lymer et al., 2004). Results confirmed the effects of training programs in terms of providing knowledge of health care waste management policy. To further improve training programs in HCF, a waste handling manual with detailed guidelines should be distributed to all those involved in health care waste management, as pointed out by Danchaivijitr et al. (2005).
This study also revealed a deficiency in occupational safety among cleaning personnel, to whom sufficient attention was not paid in comparison to staff employees at the HCF surveyed. Regular training programs and adequate protective measures such as immunization, health checks, and equipment should be provided not only to regular employees but also to cleaning personnel since they are often exposed to a relatively high risk of accidents and infections (Danchaivijitr et al., 2005).
5. Conclusion and policy recommendations
In China, a health care waste management system based on a national regulatory framework has been established at the tertiary and secondary hospitals surveyed. Poor management was found at primary health care centers. Financing and administrative monitoring by local authorities is urgently needed to improve handling practices and implement off-site centralized disposal. In terms of occupational education and safety, HCF should provide sufficient training programs and protective measures to all relevant personnel, including non-staff members such as cleaning personnel. Training programs in primary health care centers should be varied to meet the needs of personnel and to improve their understanding of the management system.
Acknowledgements
This is a Japan–China cooperative study supported by a grant from the Ministry of Environment of Japan and the Ministry of Health of China and involved researchers from the University of Tokyo, Japan and Shandong University, China. The authors wish to thank the directors of the Dongying District Health Bureau, Weifang District Health Bureau, and Binzhou District Health Bureau and all officers and staff members at the study sites for their keen cooperation and assistance with this study.
References
- Abdulla F., Qdais Abu H., Rabi A. Site investigation on medical waste management practices in northern Jordan. Waste Management. 2008;28:450–458. doi: 10.1016/j.wasman.2007.02.035. [DOI] [PubMed] [Google Scholar]
- Askarian M., Vakili M., Kabir G. Results of hospital waste survey in private hospitals in Fars province, Iran. Waste Management. 2004;24:347–352. doi: 10.1016/j.wasman.2003.09.008. [DOI] [PubMed] [Google Scholar]
- Bdour A., Altrabsheh B., Hadadin N., Al-Shareif M. Assessment of medical waste management practices: a case study of the northern part of Jordan. Waste Management. 2007;27:746–759. doi: 10.1016/j.wasman.2006.03.004. [DOI] [PubMed] [Google Scholar]
- Da Silva C., Hoppe A., Ravanello M., Mello N. Medical wastes management in the south of Brazil. Waste Management. 2005;25:600–605. doi: 10.1016/j.wasman.2004.03.002. [DOI] [PubMed] [Google Scholar]
- Danchaivijitr S., Santiprasitkul S., Pumsuwan V., Tiersuwan S., Naksawas K. Problems in the management of medical waste in Thailand. Journal of Medical Association of Thailand. 2005;88(Suppl. 10):140–144. [PubMed] [Google Scholar]
- Diaz L., Savage G., Eggerth L. Alternatives for the treatment and disposal of healthcare wastes in developing countries. Waste Management. 2005;25:626–637. doi: 10.1016/j.wasman.2005.01.005. [DOI] [PubMed] [Google Scholar]
- Kawakita J. Kawakita Research Institute; Tokyo, Japan: 1975. The KJ Method: A Scientific Approach to Problem Solving. Technical Report. [Google Scholar]
- Kobayashi, M., Murakami, H., Kinomoto, M., 2002. Chugoku ni okeru iryouhaikibutushori no genjou to torikumi [current state of and efforts at medical waste treatment in China]. Iryouhaikibutukenkyu [Journal of the Japan Medical Wastes Research Association] 14, 95–99 (in Japanese).
- Lee B., Ellenbecker M., Moure-Ersaso R. Alternatives for treatment and disposal cost reduction of regulated medical wastes. Waste Management. 2004;24:143–151. doi: 10.1016/j.wasman.2003.10.008. [DOI] [PubMed] [Google Scholar]
- Liu Y., Hsiao WC., Li Q. Transformation of China’s rural health care financing. Social Science and Medicine. 1995;41:1085–1093. doi: 10.1016/0277-9536(95)00428-a. [DOI] [PubMed] [Google Scholar]
- Lymer B., Richt B., Isaksson T. Blood exposure: factors promoting health care workers’ compliance with guidelines in connection with risk. Journal of Clinical Nursing. 2004;13:547–554. doi: 10.1111/j.1365-2702.2004.00897.x. [DOI] [PubMed] [Google Scholar]
- Massrouje H. Medical waste and health workers in Gaza governorates. Eastern Mediterranean Health Journal. 2001;7:1017–1024. [PubMed] [Google Scholar]
- Ministry of Health China, 2003. Management guideline for medical waste management in health care facilities.
- Mohee R. Medical wastes characterisation in healthcare institutions in Mauritius. Waste Management. 2005;25:575–581. doi: 10.1016/j.wasman.2004.10.003. [DOI] [PubMed] [Google Scholar]
- Patil A.D., Shekdar A.V. Health-care waste management in India. Journal of Environmental Management. 2001;63:211–220. doi: 10.1006/jema.2001.0453. [DOI] [PubMed] [Google Scholar]
- Phengxay S., Okumura J., Kuroiwa C. Health-care waste management in Lao PDR: a case study. Waste Management and Research. 2005;23:571–581. doi: 10.1177/0734242X05059802. [DOI] [PubMed] [Google Scholar]
- Prüss A., Giroult E., Rushbrook P. World Health Organisation; Geneva: 1999. Safe Management of Wastes from Health-Care Activities. [Google Scholar]
- Rogers D., Brent A. Small-scale medical waste incinerators–experiences and trials in South Africa. Waste Management. 2006;26:1229–1236. doi: 10.1016/j.wasman.2005.08.007. [DOI] [PubMed] [Google Scholar]
- Shinee E., Gombojav E., Nishimura A. Healthcare waste management in the capital city of Mongolia. Waste Management. 2008;28:435–441. doi: 10.1016/j.wasman.2006.12.022. [DOI] [PubMed] [Google Scholar]
- Tsakona M., Anagnostopoulou E., Gidarakos E. Hospital waste management and toxicity evaluation: a case study. Waste Management. 2007;27:912–920. doi: 10.1016/j.wasman.2006.04.019. [DOI] [PubMed] [Google Scholar]
- World Health Organisation Safe healthcare waste management–Policy paper by the World Health Organisation. Waste Management. 2005;25:568–569. [Google Scholar]
- Wu S., Sun N., Zhou F., Liu Y. Present conditions and countermeasures of medical waste management in China. Environmental Protection. 2005;316:36–38. in Chinese. [Google Scholar]