

Abstract
Among the most relevant elements contributing to define the One World One Health programme we find epidemics. The reason is that in recent decades, infectious diseases such as HIV/SIDA, SARS and Influenza have shown that we need new approaches and concepts in order to understand how biological emergencies and health alerts deploy new scales of action. Especially relevant has been the case of A(H1N1) influenza. This reached the status of global threat virtually from its onset, triggering an international response with a diffusion, visibility and rapidity unparalleled in previous health alerts. This article maintains that this global condition cannot be explained solely by the epidemiologic characteristics of the disease, such as mortality rate, severe cases, propagation capacity, etc. Resorting to the approach proposed by the Actor-Network Theory (ANT), this paper suggests that the action of certain socio-technical operators was what built a heterogeneous network of ideas, concepts and materials that turned the A (H1N1) influenza into a global-scale phenomenon with unprecedented speed. Among these operators, the most important ones were: the speaking position, a discourse about threat, the protocols and guidelines that were used and, lastly, the maps that allowed a real-time monitoring of the influenza. The paper ends with the notion of panorama, as defined by Bruno Latour: a suggestion to describe the common denominator of the aforementioned operators, and a means to foresee the development of global scales for certain health alerts. The paper will conclude by proposing that this type of analysis would allow the One World One Health to understand with greater precision the dynamic of epidemics and thus make its principles of action much more specific as well as its definition of what global health should be.
Keywords: One World One Health, A (H1N1) influenza, Global scale, Socio-technical operators, Panorama, Actor-Network Theory
Highlights
-
•
We improve knowledge about the global condition of epidemics.
-
•
We offer a new way of viewing epidemics. These are conceptualized as sociotechnical objects.
-
•
We put forward a re-formulation of the One World One Health programme.
-
•
We show the use of qualitative methodologies for the sociotechnical analysis of epidemics.
1. Introduction
In recent years expressions such as One Health, Big Medicine, Global Health and One World One Health have acquired a certain degree of currency. They all refer to the necessity for a global well-being arising from the well-being of human beings, animals and the environment (Gibbs and Anderson, 2009, WHO et al., 2008). Among these expressions One World One Health seems to be prevailing over the rest. To a large degree this is due to the Manhattan Principles on One World One Health, which were announced on September 29, 2004 at a symposium organized by the Wildlife Conservation Society and hosted by The Rockefeller University (Wildlife Conservation Society, 2004).
At this meeting, on the basis of analysis of the recent outbreaks of West Nile Virus, Ebola Hemorrhagic Fever, SARS, Monkeypox, Mad Cow Disease and Avian Influenza, the twelve principles, which make up the One World One Health program, were set out. These principles urge world and civil society leaders, global health institutions and the scientific community to jointly respond to a situation characterized by: a) a general and global transformation of life on the planet due to factors such as climate change, pollution, loss of biodiversity and human population growth, b) increasingly common infectious disease threats to humans, domestic and wild animals and c) the ease and speed with which such threats can reach a global scale (Leboeuf, 2011, Sida Annual Health, 2009, WHO et al., 2008, World Bank/OIE, 2008). The Manhattan Principles, recognizing the link between human, domestic animal, and wildlife health, and the threat disease poses to people, their food supplies and economies, and the biodiversity essential to maintaining healthy environments and functioning ecosystems, put forward the imperious necessity of a Global Medicine – one without limits among species and one with a scope in different scales.
This program is based on two essential assumptions. Firstly, it is based directly on cases the majority of which can be categorized as Emerging Infectious diseases (EID) and more specifically, epidemics, with influenza being the most notable of these. And secondly, the risk of a rapid spread and global reach of these epidemics appears as the model of the main threat, which the One World One Health program should aim to prevent. These two assumptions are obvious from a perusal of the already existing literature on this approach (Alive, 2007, American Veterinary Medical Association, 2008, FAO, 2008, FAO et al., 2008).
Traditionally, the notion of epidemic is uncritically associated with a phenomenon of generalization, which is taken for granted and is directly tied to the biological–medical component related to any infectious vectors. Nonetheless, this global scale can be analyzed and understood from a different angle. Rather than regarding it as a biological effect, it can be described as a production, a scale that is built and requires a series of operators to elaborate it and make it effective. As some authors have pointed out, the high visibility of an epidemic is not always tied to biologic effects, as these are not noticeable, but to a retrospective historical and demographic analysis (Rosenberg, 1992, Ranger and Slack, 1992, Watts, 1997, Van Loon, 2005). In this way, the surprising rapidity with which the A (H1N1) influenza became a global phenomenon raises questions about the factors and the structures that made it possible.
Thus, the examination of how an epidemic acquires this global condition is fundamental to One World One Health for various reasons. In the first place, because epidemics are not only a biological or medical problem; along with these dimensions we find other problems, such as political, discursive, and technological ones. All these dimensions are entangled in a single totality with a homogeneous logic. Secondly, all these dimensions transform the social, political, technological, and medical aspects of our daily life. That is to say, an epidemic is something more than a medical threat: it is an event that completely transforms our immediate reality. Thus One World One Health amounts to something much greater than a medical program. Its relationship with epidemics and its proposals for action make it into something that aspires to participate in the immediate constitution of our reality.
This article will examine how epidemics achieve their global condition, looking beyond simply epidemiological data, and focusing on the A(H1N1) flu outbreak. It puts forward the view that the global condition of A(H1N1) influenza was not merely declared due to the medical features of the illness such as the virus's ability to mutate, its easy transmission or its death rates. Rather, we suggest that the global effect of H1N1 influenza should be sought in the activity of specific techno-social operators, which generated and brought together the necessary conditions for this global possibility. In order to prove the aforementioned hypotheses, first of all this paper will analyze the way in which medicine, and, more concretely, epidemiology, regards the global condition of an epidemic. Secondly, it will argue that the Actor-Network Theory (ANT) gives us instruments to conceptualize that condition in a different manner. Rather than tying it to the biological nature of the phenomenon, the concepts of operator and panorama allow the global scale to be defined as a production based on the articulation of a complex infrastructure, made of heterogeneous elements. Thirdly, it will describe the operators that had a specific role in the creation of an important global condition for the A(H1N1) influenza. Finally, it will resort to the notion of panorama, as proposed by Bruno Latour (2005), to describe the global status of certain biological phenomena in contemporary society. The paper will conclude by proposing that this type of analysis would allow One World One Health to develop a broad and socio-technical way of understanding the dynamic of epidemics and their consequences.
2. According to epidemiology, when does an epidemic turn global?
The first cases of the A (H1N1) influenza that were confirmed in the laboratory were diagnosed in California (US), on April 17, 2009. The same country was then affected by the first confirmed death attributed to the above-mentioned outbreak (CDC, 2009). From this date on, the epidemic of A (H1N1) has been surrounded by a vigorous debate, which has been documented and fueled by the media (Yang et al., 2009). The reasons for this debate are not to be found in the strictly medical or biological aspects of the outbreak. In this respect, it might be useful to recall a few facts. First of all, the influenza was classified as new not because it is a type A outbreak, or a H1N1 subtype – the well-known pandemic of influenza of 1918 was a type A/H1N1, and since the seventies this type of virus has been detected in seasonal outbreaks; it was because a different strain was found, the so-called S-OIV. This is the real novelty of this epidemic, which, to be precise, should be called A/H1N1 virus influenza and S-OIV strain (Webby and Webster, 2003, Zimmer, 2009). Secondly, from its onset until September 15, 2009 it has caused the deaths of 137 people in Europe, and almost 4.000 worldwide, but the number of deaths in Europe is between 40,000 and 220,000 every year. Furthermore, unlike in other outbreaks, the population most at risk is not aged between 50 and 70, but between 25 and 49.
As a matter of fact, the reasons for the controversy are to be found elsewhere. Immediately after its onset, the new epidemic became a worldwide exceptional situation. It is worth mentioning that the US declared a “State of National Health Emergency” with only 20 infected people in the whole country, and although they had not yet reported deaths attributable to the new virus. Similarly, on April 29, 2009, only 12 days after the first two confirmed cases, Margaret Chan, the General Director of the WHO, increased the level of pandemic alert, declaring Phase 5 and calling on WHO member states to activate the emergency plans to respond to an influenza pandemic. A month later, on June 11, 2009, the WHO raised the pandemic alert to Phase 6. This was the official declaration of the first pandemic of the 21st century caused by the A/H1N1 S-OIV virus. From its onset, the new A influenza had entailed the emergence of an exceptional situation in our everyday life. First of all, due to its global condition and, secondly, due to the rapidity with which it acquired that condition (Cohen, 2010, Ebrahim et al., 2009).
Until 2009, the WHO considered an epidemic as global when three criteria were met: infection due to an infectious agent, simultaneity in different countries, and a significant mortality in relation to the proportion of the infected population. From that year on, the WHO reduced the weight of mortality in the definition (Parliamentary Assembly, 2010) and stated that, in order to declare a pandemic:
-
a)
A new virus should appear, that has not been described yet, hence, with no existing immune population to it.
-
b)
This virus should be able to produce severe cases of illness.
-
c)
This virus should be able to spread effectively from person to person.
Moreover, the entity described phases for global application that serve as guide both for countries in preparing for a pandemic as well as for the declaration of a pandemic by the WHO (Fig. 1 ).
Fig. 1.
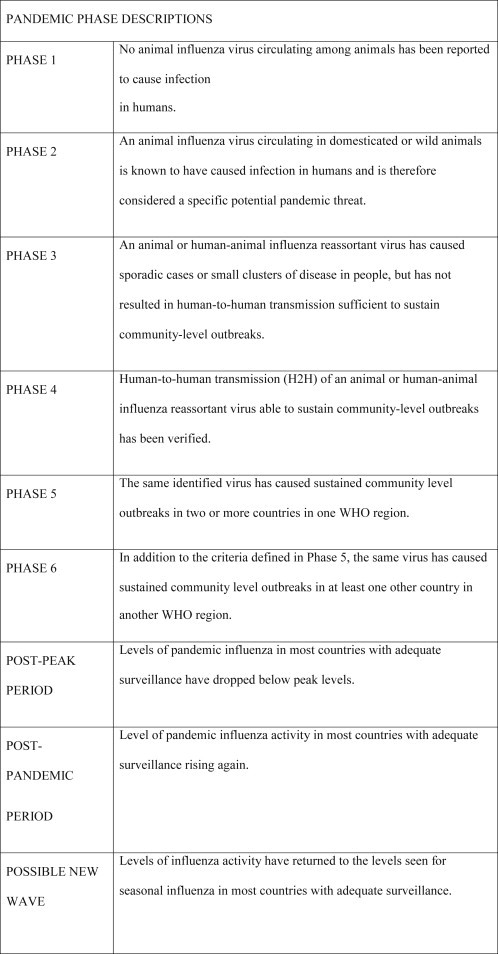
Pandemic phase descriptions, WHO, 2009b: 11.
From the biomedical definitions it follows that the H1N1 influenza acquires its global condition (pandemic) when an antigenic strain develops its complexity as a consequence of genetic exchange between human, avian and swine strains (Domínguez et al., 2011). Among other features, it was considered as distinctive of this flu its enhanced transmission capacity in comparison with the seasonal flu; the greater number of severe and lethal cases among the young, geographical variations in its impact, the presence of activity outside the cold season and the occurrence of more than one wave. Nevertheless, it is possible to analyze the global condition of H1N1 in a different and more interesting way thanks to Actor-Network Theory.
3. Actor-Network Theory and epidemics
Actor-Network Theory (ANT) constitutes an ideal framework to analyze the creation of a global scale for the H1N1 epidemic. Its founders define this theory as a simple toolbox to explain social transformation. The main principles of this approach can be summarized in the following points. First, ANT is a collection of explanations about social reality in which the analyst looks and defines relations and not essences, fixed entities or taken-for-granted categories. Second, these explanations do not respect either the mainstream academic frontiers (sociological, psychological or historical, given the questions are mixed) or methodological frontiers. Another frontier it breaches is that of mainstream social sciences dualisms: social versus natural, molar versus micro or agency versus structure (Krarup and Blok, 2011). Third, ANT accounts are based on conventional ethnographies, discursive analyses, interviewers, etc. Fourth, ANT talks about social reality in terms of practices. Finally, in these practices the activity of human beings is as important as the action of materiality. In fact, ANT is very well known in social sciences thanks to the role and relevance that materiality has in its explanation (Latour, 1999, Latour, 2005, Law, 2004, Law and Mol, 1995, Law and Mol, 2001, Law and Mol, 2002).
The point we want to highlight here is the non-distinction between global and local put forward by ANT (Latour, 2005, 2013). This suggests that the global is not different to the local. In this theory, macro no longer describes a wider or a larger site in which the micro would be embedded but rather another equally local, equally micro place. The macro is neither above nor below the interactions, but added to them as another of their connections, feeding them and feeding off them. There is no other known way to achieve changes in a relative scale. For each of the macro places, the same type of questions can be raised. The answer provided by fieldwork will bring attention back to a local site and re-describe it as some disheveled arrays of connections.
Global is a site articulated or produced in the same way that the local is shaped. There are specific operators (an idea, image, action or object) that open and set out the global condition. Furthermore this condition is attached to a phenomenon. In this sense, the macro effects of an event or the macro political features of a phenomenon are built up from a complex network of localized technical practices and devices (Barry, 2001, Latour, 2005). As Latour says, “you will soon realize that, in spite of so much ‘globaloney’, globalization circulates along minuscule rails” (Latour, 2005: 190).
Some authors have approached the phenomenon of epidemics from this perspective. In some cases they have shown how the material action of the protocols allows the interconnection of political decisions with biological facts, building their own definition of the epidemic phenomenon (Schillmeier, 2008). Some others have maintained that within an epidemic there are different spaces related to the virus and when it organizes into a structure, it produce the homogeneous and global space that is then defined as an epidemic (Van Loon, 2005). Finally, some authors have insisted on the social globalization entailed by all epidemics. That is, they have shown how an epidemic represents an ideal chance for information, objects, practices and capital to interweave in one seamless fabric (Wagner-Egger et al., 2011). All these contributions have been relevant in order to understand epidemics in a broad sociotechnical way. In this sense, the insights provided by the ANT allow us to go into such an analysis in greater depth. Specifically, they provide the tools to describe in detail the operators, which are the starting point for building the global scale of an epidemic, and how to deal with it. In the next section we will clarify the relevance of operators in Actor-Network Theory and in our proposal for a new understanding of pandemics.
4. Empirical work and data collection
This article is based on work carried out in the years 2010, 2011 and 2012. The methodological approach was completely qualitative in nature. This type of methodology focuses on the study of meanings and relationships in specific contexts on the basis of observational, descriptive and interpretational work (Silverman, 1985, Willig and Stainton-Rogers, 2008). This methodology is suitable for the present study precisely because it seeks to clarify relationships and meanings.
More specifically, what was carried out was an intensive case study of the A(H1N1) flu epidemic. The case study consists of an intensive collecting of relevant data and material in order to answer a question or analyze a social situation. Thus this type of method combines interviews, both with individuals and groups, participant observations and the gathering of audiovisual and written material, etc (George, 2005, Yin, 2009). We regard this type of methodology as suitable given the complexity and profundity required to describe all the non-medical and non-biological elements involved in the constituting of an epidemic on a global scale.
The following information gathering activities were carried out: a) in depth interviews with ten medical experts who work in Barcelona, Spain, b) visits to some infectious disease treatment centers, c) the collecting of press and specialized publications relating to the case which interested us, with special attention being paid to WHO publications and d) the action protocols of the Spanish monitoring system and those used by the WHO, the Centre for Disease Control and Prevention in the United States and its equivalent in the European Union were all collected. The guiding themes for the interviews were: 1. How the monitoring and alert system works, 2. Definition of the A(H1N1) flu epidemic, 3. Actions carried out by people, experts and politicians and 4. Opinions regarding media treatment of the matter and the response of lay citizens.
Our data analysis is based on a critical discourse analysis approach (Wodack and Meyer, 2009) since it assumes that the narratives coming from the managers, experts, corporate documents, and the graphical arena can all be seen as texts (Fairclough and Wodak, 1997). Critical discourse analysis allowed us to explore how these texts may be drawing and constructing (favored) versions of reality, relations and topological positions. Following this approach, the verbal interactions, the data, claims and images from the documentation and brochures, the instructions from the protocols etc., were all treated and analyzed as structures of text (Van Dijk, 1993).
4.1. Socio-technical operators in the H1N1 influenza
As Michel Serres (2007) and Bruno Latour (2005) have pointed out, an operator is any element (material or not, human or not) allowing, under certain conditions, the connection between different actors, which results in a network, a situation or a new reality. The notion is massively present in the philosophy of Michel Serres and is called mediator in Actor-Network Theory. An operator or mediator points to the existence of an event or action that creates a relation. This itself, and not its reference to a possible cause or consequent effect, is the element relevant in the explanation of the phenomenon studied. For Actor-Network Theory, mediators establish sets of relations that constitute the essense of every social object and their description is the real work of social thought.
The present study identifies four operators that had a fundamental role in the fast global constitution of the A(H1N1) influenza: a) who is speaking and from where, b) the way things are said (crisis discourse and global response), c) action protocols and guides in different scales, and d) the illness tracking maps.
4.1.1. Speaking position
Since the appearance of the first A(H1N1) influenza cases, the WHO was the body that emerged as the scientific expert reference point for tracking the epidemic, discussing its impact and suggesting action pathways to different countries. The WHO was able to play this role due to the infrastructure that it had developed for more than half a century, which in the last few years has been optimized to respond to the growing worldwide concern about the pandemic potential of some infectious diseases like influenza. A key element of this infrastructure is the WHO's Global Influenza Surveillance and Response System (GISRS), founded in 1952. At present this is made up of an extensive global network of laboratories, national influenza centers and collaborating centers, established in more than 100 countries. In addition to monitoring the evolution of the influenza virus, this system acts as a mechanism of global alert in the event of outbreaks with a pandemic potential. The virological information provided by the GISRS centers is entered into a specific system called FluNet, which processes the information and shows it by means of graphics, tables or maps, available to the public on the WHO website. Most of these maps circulated on the Internet and the media during the A(H1N1) influenza to show the evolution of the disease.
Another important element of the WHO surveillance infrastructure is the Global Outbreak Alert & Response Network (GOARN), founded in 2000 as a mechanism of cooperation and communication between institutions and networks, which aims to identify and deal with epidemic outbreaks of international importance. GOARN was fundamental for the WHO to acquire a leading role in reporting and verifying epidemic outbreaks, and negotiating the measures to prevent and control threats with the affected state and the neighboring countries (Davies, 2009).
By means of the International Health Regulations (IHR) of 2005, the Member States committed to improving a number of public health conditions, and gave the WHO a mandate to detect, verify, and act in case of health emergencies that are of concern for international public health:
Under the IHR (2005) a number of reporting requirements oblige States Parties to promptly inform WHO of cases or events involving a wide range of diseases and public health risks including ‘all cases of human influenza caused by a new virus subtype’ (Briand, 2011, p.2)
In this way, the IHR has become the framework for the WHO to guide the development of national pandemic preparedness plans, elaborated by the majority of the Member States when they had to face the A(H1N1) influenza crisis.
During the A(H1N1) influenza crisis the WHO activated its real-time epidemic control and monitoring surveillance system, which began providing information to the rest of the world. This system is a clear example of the connections between different scales, as it articulates research laboratories, epidemiological surveillance protocols, sovereign states, legislations, people, etc. And most importantly, a connection was established with the media, which gave visibility to the H1N1 Influenza to much of the world population. With the information collected through the surveillance system and the advice of the Emergency Committee, the Director of the WHO progressively declared the pandemic phases – established according to a scale from 1 to 6 – while the disease was spreading across the world. This system of scales generated controversy between experts, because it created confusion between those phases and a scale of danger.
The office's Health President, Marc Van Ranst, pointed out an existing confusion between alert levels and degrees of threat. The proposed levels between 1 and 6 do not necessarily mean that for every phase increase the virus is more dangerous, but it rather expresses its territorial expansion. The WHO had two reactions to this controversy: 1) Blocking – in the midst of the crisis – access to the information generated by its real time monitoring system regarding the infected and deceased in each country, which was previously available to everyone on its website (one of the corner stones of the WHO's infectious alerts system), and stop publishing its epidemic evolution world maps, and 2) A meeting of the Committee of Experts that advises the WHO was convened, in which the phase 6 of the protocol was reassessed.
That previously created infrastructure allowed the WHO to be the agency that set the terms, virtually from the beginning, of the debate on the A(H1N1) influenza as an exclusive responsibility of international organizations. Also the subsequent controversy reinforces this idea. As a consequence, local research groups and national experts lost any chance to express their opinions through the media, subordinating themselves to the WHO announcements.
4.1.2. A discourse about threat
The global condition of H1N1 influenza is not only explained by the action of certain agents like the WHO, but rather the way in which the threat is defined and communicated becomes an operator in itself. Thus, we observed that long before the outbreak of H1N1 appeared, the WHO already had begun to elaborate a discourse in which the influenza epidemics were conceptualized as a public health risk of “international importance.” Since the emergence of avian influenza (H5N1) in humans in 1997 and especially since the severe acute respiratory syndrome (SARS) outbreak in 2003, the WHO has been warning about the risk of an influenza pandemic with serious consequences at a world level.
This previous stage to A(H1N1) influenza, which we will denominate “preparatory,” was characterized by the development of strategies, plans and protocols for facing a possible pandemic. A set of connections that were activated, updated or transformed during the development of H1N1influenza was established.
In terms of connections, the one established between animals and human beings was one of the most important (Schillmeier, 2008). In its discourse, the WHO warned that the main pandemic threat would come from the influenza virus circulating among animals, which, in annealing or genetically mutating, could infect human beings. Thus, whilst circulating between these two worlds the virus might blur the boundaries between species, breaking down this classic dichotomy.
Wild birds form a reservoir for a large number of other influenza viruses and influenza viruses are found in other animal species as well. Any one of these other viruses, which normally do not infect people, could transform itself into a pandemic virus (WHO, 2009b, p. 14)
The start of H1N1 influenza was strongly marked by this animal–human connection, as it is an animal sourced virus that combines genes from swine, avian and human influenza virus. Actually, in their initial press releases the WHO named the disease “swine flu”, a name that was reproduced by the media and for which it was known worldwide (WHO, 2009a).
As this disease was arriving from the animal world, humans would not have the necessary immunity and this would cause many serious cases and deaths, as well as a rapid global spread.
Modeling research using today's global population has projected that at a minimum, between 2 and 7.4 million people might die in the next pandemic. More deaths are certainly possible, but until the pandemic strain emerges and we are able to determine its lethality and attack rate, it will be difficult to predict its impact worldwide (WHO, 2005:5)
Therefore, in this preparatory stage another connection operates, of a temporary kind, which connects the level of future threat (death and rapid expansion) with the present measures. The risks are placed on a dimension operating in the present through the future, as it is the promise of a negative event that may occur which leads to action, generally preventive, in the present. The mobilization achieved against a risk would grow in proportion to the content of its future threat (Beck, 1992).
The reference case used for this threat was the avian flu (H5N1) because it was considered the pandemic virus with the greatest potential. One of the features highlighted was the high rate of serious illness and deaths caused. The underlying threat was the possibility of a virus – as deadly as the former – reaching a high level of spread, hence threatening the whole world.
Every time the H5N1 virus spreads to new regions, you increase the probability and also the opportunity for the virus to mutate. With each human infection, the probability for the virus to mutate increases. This virus is very treacherous (WHO, 2005, p.4).
If the threat was so comprehensive, an answer in keep with the circumstances was required to establish another connection between the level of threat and the need for global protection.
The outbreak of H1N1 triggered the promise of a threat that would affect all of humanity and, therefore, the WHO focused risk management in protecting the health of the international population. At this stage, that we shall call “risk management”, the WHO activated the protocols in which the body had been working together with its 194 states members. Since the beginning of H1N1, the Director-General of WHO, Margaret Chan, stressed international preparedness.
All countries should immediately activate their pandemic preparedness plans. Countries should remain on high alert for unusual outbreaks of influenza-like illness and severe pneumonia (Chan, 2009).
Hence, thanks to the connections of the preparatory stage, the onset of the first case of H1N1 influenza was characterized as a global threat that could affect all humanity, thereby requiring a global response. This demanded the activation of protocols designed for this purpose, which is the third operator we will analyze.
4.1.3. Protocols and action guidelines
The plans and other action protocols mentioned in the WHO's statements created a connection between actors who were not necessarily linked in the past. In this sense, these plans would not be simple intermediary objects, but rather by their “action” they also became part of the network of actors who give continuity to the action and change its meaning.
The WHO developed its protocols based on a strategy they called, “of the whole society,” understanding that to safeguard the health of the population the agency should trespass across its own institutional boundaries, even the health sector, and should involve governments, civil society organizations, businesses, communities, families and individuals. Hence, preparedness and response should extend not only internationally but also had to include the different levels of each country.
This change to a higher phase of alert is a signal to governments, to ministries of health and other ministries, to the pharmaceutical industry and the business community that certain actions should now be undertaken with increased urgency, and at an accelerated pace (Chan, 2009).
The protocols prepared and used by the WHO during the H1N1 influenza outbreak exemplify this philosophy, one that articulates the action of the different scales and agents who constitute the social fabric. For example, in the International Health Regulations, written in the 1960s but updated in 2005, its presentation and definition states:
The purpose and scope of the IHR (2005) are “to prevent, protect against, control and provide a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade.” The IHR (2005) contain a range of innovations, including: (a) a scope not limited to any specific disease or manner of transmission, but covering “illness or medical condition, irrespective of origin or source, that presents or could present significant harm to humans”; (b) State Party obligations to develop certain minimum core public health capacities; (c) obligations on States Parties to notify WHO of events that may constitute a public health emergency of international concern according to defined criteria; (d) provisions authorizing WHO to take into consideration unofficial reports of public health events and to obtain verification from States Parties concerning such events; (e) procedures for the determination by the Director-General of a “public health emergency of international concern” and issuance of corresponding temporary recommendations, after taking into account the views of an Emergency Committee; (f) protection of the human rights of persons and travellers; and (g) the establishment of National IHR Focal Points and WHO IHR Contact Points for urgent communications between States Parties and WHO” (WHO, 2008 p.1).
This protocol has a broad spectrum of general application intended to be useful for any disease or biological emergency. The IHR places WHO in a supervision position over state health agencies and obliges states to coordinate through the WHO. Also, it gives the body the authority to protect general public health, as well as the transportation and movement of people. This general and global nature of the protocol becomes evident once again if one examines the Whole-of-Society Pandemic Readiness, a guide developed by WHO within the so-called “Global Influenza Programme.” One of the most interesting aspects of this document is that from its title on it insists on its general and global nature, whilst clearly depicts the articulation of different scales and social actors.
The IHR emphasizes the relationship between people who move, states, health agencies, health rights and the WHO. Meanwhile, the Whole-of-Society Pandemic Readiness Society (WHO, 2009c) expands and incorporates a multitude of actors and dimensions of our social life. Thus, it is a guide that reviews health aspects, but also elements such as ethical issues, relationships between institutions and organizations outside the health sector, institutional and individual behaviors, movement activities between countries, etc. The guide depicts a global situation in extension, i.e., in the number of actors and agencies involved in its implementation and use, and in intent, because it outlines activities and behaviors for those actors.
Finally, some similarities can be detected if local protocols are discussed, as they are usually developed following WHO guidelines. An example is the one used in Spain to deal with such emergencies, the protocol Plan Nacional de Preparación y Respuesta ante una Pandemia de Gripe (Ministry of Health of Spain, 2005). This document, after the necessary sections devoted to health claims, details the actions of the government and its relationship with the health sector and how other sectors -apart from health-should act. These include the various social communities, families and individuals.
Therefore, in addition to the discourse of “crisis and global response”, made to refer to the H1N1 influenza pandemic, we find protocols that address it as a global phenomenon. These documents show the involvement of different levels (WHO, states, health agencies, communities, families and citizens), offer tips and tools to articulate them in a certain way and structure them pointing towards the supervisory structure of WHO. Therefore, when the phenomenon of H1N1 was faced, it was already caught in this global network of levels that gave the issue a dispersed dimension spread throughout the social fabric and with a global character.
4.1.4. Real-time tracking maps
As noted above, from the outset, the WHO was able to track H1N1 in a way that was presented as novel:
For the first time in history, we can track the evolution of a pandemic in real-time. (Chan, 2009)
The information generated was made available to institutions, media and general public through diverse formats (Fig. 2, Fig. 3 ):
Fig. 2.
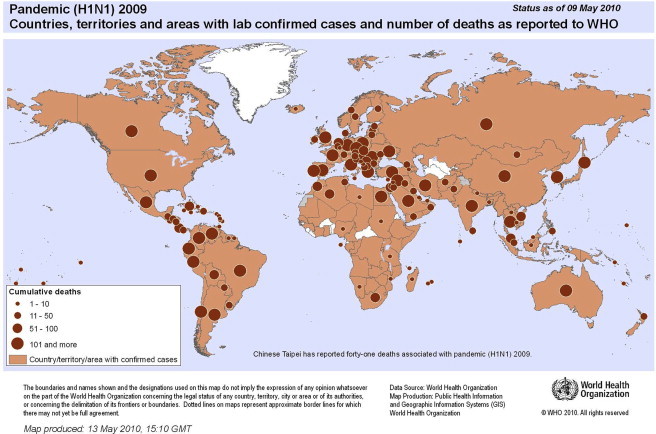
World Health Organization, Programm Influenza, FluNet. http://gamapserver.who.int/mapLibrary/app/searchResults.aspx. Downloaded October/8/2010.
Fig. 3.

HealthMap, a team of researchers, epidemiologists and software developers at Boston Children's Hospital founded in 2006, is an established global leader in utilizing online informal sources for disease outbreak monitoring and real-time surveillance of emerging public health tretas. http://healthmap.org. Reproduced with screenshot October/13/2009.
These images (the source of these maps is the World Health Organization) are revelatory of what the H1N1 influenza crisis was. For the first time in the history of public health emergencies the process was tracked beyond the surveillance system and maps were developed under the principles of the alarm system. The images are maps of the planet, which were developed almost in real time, showing the levels of infection in each country and its progression over time. Some even seemed to indicate the direction and force vector of contagion. This material is important because it creates several effects:
-
a)
It gives visibility to the disease from a geographical perspective rather than from biological or medical devices. It also places the influenza in a global context that spans the whole planet thus presenting it as a problem that affects everyone and all countries.
-
b)
It generates a sense of homogeneity in the development and characteristics of the disease, i.e., it seems that what happens in the U.S. has the same features as what happens in Spain. Therefore, it creates the impression that the phenomenon is comparable and equivalent in all places.
-
c)
It generates the feeling that you can view, track and trace the phenomenon. Namely, it cannot hide in any corner of the planet.
-
d)
Finally, it generates the feeling that the problem can be handled. This is possible because the map offers at first glance the possible origin of pandemics, its evolution, countries infected, actors involved, the speed of the infection and so on. Having all this information in a single map, on paper or in a computer, shapes the feeling of certainty and control.
Both the protocols and these tracking maps produced uniformity and comparability, which are critical issues in this type of phenomenon. In the words of Barry (2001), uniformity and comparability that produces various socio-technical operators create a plane in which objects, people and actions become absolutely comparable, suffer and produce the same effects, acquire the same properties and are susceptible to the same type of intervention.
4.1.5. The global condition and the panoramas
Speaking position, the discourse about threat, protocols and guidelines for action at various scales and disease tracking maps are four operators that generated a kind of socio-technical infrastructure that gave the H1N1 influenza global status. All these items generated a material and symbolic network, which framed H1N1 influenza in a certain way whilst establishing its global condition.
However, in the last phase of the disease this global feature encountered a crisis. The number of people affected by A(H1N1) influenza could not stand comparison with other diseases or outbreaks that did not have the same features. Therefore, a strong challenge to the criteria used by the WHO to declare a pandemic emerged. Actors from different backgrounds and points of the globe and media of different countries, medical journals and supranational organizations – like the Council of Europe – produced allegations ranging from unjustified alarm generation to alleged conflicts of interests, with some WHO advisers related to the pharmaceutical industry. Faced with these challenges, the WHO argued that its actions were not intended to benefit the pharmaceutical industry and that their declaration of a pandemic was based solely on scientific criteria, in this case, virological and epidemiological causes. Indeed, we consider that the WHO acted following expert and specialized parameters. In fact, what happens is that, as suggested by several authors (Latour, 1999, Ong and Collier, 2005), such parameters currently include the global condition in the way they define and act upon certain phenomena.
As a matter of fact, the common denominator that all operators share, as described in this article, is that they are what Latour (2005) called “panoramas.” He reminds us that panoramas, as the etymology of the word suggests, see everything. But they also see nothing since they simply show an image painted (or projected) on some sort of material. What is so powerful in panoramas is that they nicely solve the question of staging the totality, of ordering the ups and downs, of nesting ‘micro’, ‘meso’, and ‘macro’ into one another:
They design a picture which has no gap in it, giving the spectator the powerful impression of being fully immersed in the real world without any artificial mediations or costly flows of information leading from or to the outside (Latour, 2005, p.145).
The panoramas are coherent and complete accounts. They provide the occasion to see the story as a whole. They provide totalizing views. They offer a foretaste for the one world to be lived in. They frame and order. And in that sense, they mobilize resources and define realities. Two good examples of panoramas very usual in our daily life could be the mapamundis we offer to children in order to learn geography or books containing the entire history of human civilization.
The WHO is a huge panorama that aims to dictate the biological condition and the health standards of the whole of humanity. The discourse of the threat and the global response is another panorama that collects a state of global emergency. The protocols are small panoramas, which articulate in the same sense and direction all levels of society. And probably, the maps are the most archetypal panoramas, as they pretend to represent, through a picture, the planet and its relation to A (H1N1). Besides, the four panoramas related provide or shape a new one. Bigger and broader, it is, in fact, the global phenomenon known as A(H1N1). That is, the panoramas described are like a matrioska or Russian doll: inside each one there is a smaller one and so on.
This particular influenza outbreak was characterized by reaching, in record time, the definition of a global phenomenon. As we tried to show, this was not based on biological or epidemiological elements, rather, it was articulated from the activity of certain socio-technical operators who imprinted this condition because they themselves had adopted a panorama form.
The future will likely see similar situations in which this accelerated global condition is also deployed, formed by operators acting in the form of panoramas. This is for a simple reason: our scientific knowledge and expertise is deeply linked to these panoramas, their production and management. In that vein we have confirmed two things. First, the A(H1N1) influenza was a kind of flash point that showed how many medical phenomena act in – and thanks to – the generation of panoramas and therefore are quickly installed on a global scale that articulates and stands in for local elements or practices. In fact panoramas are just that: local products. Second, the A (H1N1) outbreak transformed our daily lives in a definitive way because we have come to think, speak, understand, and so on, many health phenomena on this global scale.
5. Conclusions: One World One Health revisited
Our study has three important conclusions for the One World One Health programme. First, it has shown that the global condition, which an epidemic may reach, is not solely determined by biological or medical elements. Many other factors are involved, among them institutional actors, scientific representation materials and the action of laboratories and monitoring systems etc. When we refer to a phenomenon, which has a global scale, we are not describing a situation present in every corner of the planet. On the contrary, we are referring to the constitution of a heterogeneous network of entities, which has the capacity to cause generalizable and homogenized effects. For this reason the first conclusion that should be drawn by One World One Health is that epidemics are much more than health problems. Our article suggests conceptualizing epidemics as a socio-technical phenomenon, which means that the analysis should simultaneously include – in their entirety – dimensions related to medicine, politics, science, technology, public opinion, etc. In the case of A(H1N1) influenza, it has been shown how its global condition can be explained on the basis of the action and articulation of different operators that has nothing to do with the biological component of the problem.
Secondly, our work has shown that these operators have given A(H1N1) its global status in a very short time, and their observation shows that they all share a common denominator: they produce panoramas. These in turn have the ability to represent and contain totality in a simple, manageable locality. As suggested by Latour (2005), the production of panoramas has been a privilege of science, and they have articulated themselves in special spaces, such as laboratories. The A(H1N1) influenza outbreak shows that certain institutions, such as the WHO, generate and use panoramas. They produce and articulate them within their activity in order to represent certain phenomena, and they end up establishing them in our everyday life, presenting them as assumptions, or truths that are difficult to question. From this fact there immediately arises a second conclusion for the One World One Health focus; the Manhattan Principles, the studies and statistical models that support it and the general demands made on the international community may themselves operate as panoramas and articulate themselves on specific occasions with other elements to contribute to producing a global condition in certain phenomena related to health. Thus the One World One Health should be capable of reflecting on and analyzing the type of networks, which involve all the demands and materials of various sorts that are being generated. In fact, all of this can be summarized in the necessity for an internal ethical reflection that would examine the consequences of the simple existence and activities of the movement itself. That is, the One World One Health movement should start to regard itself as a new way of understanding our daily life and our relation with our planet.
The Manhattan Principles make it very clear that One World One Health is a health project focused on eliminating the risks that arise from the relationship between man and animals (Wildlife Conservation Society, 2004). However, as we have seen in the case of A(H1N1), in the same way that epidemics are something more than a biological phenomenon the One World One Health is also much more than a medical phenomenon. Its search for global welfare is a proposal that is social in nature and its activities are techno-scientific and governmental in nature. The analysis of all these dimensions in the future will demand a real coming together of social and medical science.
References
- Alive . 2007. Guidelines for a Comprehensive Approach for the Rapid Assessment of Avian and Human Influenza in Sub-saharan Africa.http://www.aliveonline.org/data/files/alive-ra-guidelines-final.pdf Available at: [Google Scholar]
- American Veterinary Medical Association . 2008. One Health: a New Professional Imperative.http://www.avma.org/onehealth Final Report of the One Health Initiative Task Force. Available at: [Google Scholar]
- Barry A. The Athlone Press; London: 2001. Political Machines: Governing a Technological Society. [Google Scholar]
- Beck U. Sage; London: 1992. Risk Society, towards a New Modernity. [Google Scholar]
- Briand S. WHO; 2011. Challenges of Global Surveillance during an Influenza Pandemic.http://www.who.int/entity/influenza/surveillance_monitoring/Challenges_global_surveillance.pdf Available from: (accessed 05.08.12) [DOI] [PMC free article] [PubMed] [Google Scholar]
- CDC Swine influenza A(H1N1) infection in two children-Southern California, March–April 2009. MMWR. 2009;58:400–402. [PubMed] [Google Scholar]
- Chan Margaret. WHO; 2009, April 29. Influenza A (H1N1)http://www.who.int/mediacentre/news/statements/2009/h1n1_20090429/en/index.htm Available from: (accessed 05.08.12) [Google Scholar]
- Cohen J. Out of Mexico? Scientists ponder swine flu's origins. Science. 2010;324(May):700–703. doi: 10.1126/science.324_700. [DOI] [PubMed] [Google Scholar]
- Davies S. Real Instituto El Cano; 2009. Preparing for Pandemics through Surveillance.http://www.realinstitutoelcano.org/wps/portal/rielcano_in/Content?WCM_GLOBAL_CONTEXT=/wps/wcm/connect/elcano/Elcano_in/Zonas_in/ARI9-2009 ARI N°9. Available from: (accessed 05.08.12) [Google Scholar]
- Domínguez Factores de riesgo de hospitalización por gripe (H1N1) 2009 y efectividad de intervenciones farmacológicas y no farmacológicas en su prevención. Estudio de casos y controles. RevEsp Salud Pública. 2011;85:3–15. doi: 10.1590/S1135-57272011000100002. [DOI] [PubMed] [Google Scholar]
- Ebrahim S. Pandemic H1N1 and the 2009. Science. 2009;326:938–940. doi: 10.1126/science.1183210. [DOI] [PubMed] [Google Scholar]
- Fairclough N., Wodak R. Critical discourse analysis. In: Van Dijk T., editor. vol. 2. Sage; London: 1997. (Discourse as social interaction: a multidisciplinary introduction). [Google Scholar]
- FAO . 2008. FAO Report Exercise on Highly Pathogenic Avian Influenza.http://www.fao.org/docrep/010/a1145e/a1145e00.htm Available at: [Google Scholar]
- FAO and OIE, in collaboration with WHO (2008). The Global Strategy for Prevention and Control of H5N1 Highly Pathogenic Avian Influenza. Available at: http://www.fao.org/docrep/010/a1145e/a1145e00.htm.
- George A. MIT Press; Cambridge: 2005. Case Studies and Theory Development in the Social Sciences. [Google Scholar]
- Gibbs E.P., Anderson T. One World-One Health and the global challenge of epidemic disease of viral aetiology. Veterinaria Ital. 2009;45(1):35–44. [PubMed] [Google Scholar]
- Krarup T., Blok A. Unfolding the social: quasi-actants, virtual theory, and the new empiricism of Bruno Latour. Sociol. Rev. 2011;59(1):42–63. [Google Scholar]
- Latour B. Oxford University Press; New York: 2005. Reassembling the Social. [Google Scholar]
- Latour B. Harvard University Press; London: 1999. Pandora's Hope. [Google Scholar]
- Latour B. Harvard University Press; Cambridge: 2013. An Inquiry into Modes of Existence. [Google Scholar]
- Law J. Routledge; London: 2004. After Method, Mess in Social Science Research. [Google Scholar]
- Law J., Mol A. Notes on materiality and sociality. Sociol. Rev. 1995;43:274–294. [Google Scholar]
- Law J., Mol A. Situating technoscience: an inquiry into spatialites. Soc. Space. 2001;19:609–621. [Google Scholar]
- Law John, Mol Annemarie. Duke University Press; Durham, NC: 2002. Complexities: Social Studies of Knowledge Practices. [Google Scholar]
- Leboeuf A. IFRI; Paris: 2011. Making Sense of One Health Cooperating at the Human–Animal–Ecosystem Health Interface. Health and Environment Reports n°7. [Google Scholar]
- Ministry of Health of Spain . MSC; 2005. Plan Nacional de Preparación y Respuesta ante una Pandemia de Gripe.http://www.msc.es/ciudadanos/enfLesiones/enfTransmisibles/docs/PlanGripeEspanol.pdf Available from: (accessed 05.08.12) [Google Scholar]
- Ong A., Collier S., editors. Global Assemblages: Technology, Politics, and Ethics as Anthropological Problems. Blackwell; Malden MA: 2005. [Google Scholar]
- Parliamentary Assembly . Council of Europe; 2010. The Handling of the H1N1 Pandemic: More Transparency Needed.http://www.assembly.coe.int/ASP/Doc/XrefViewPDF.asp?FileID=12463&Language=EN Doc 12283. Available from: (accessed 05.08.12) [Google Scholar]
- Ranger T., Slack P., editors. Epidemics and Ideas. Essays on the Historical Perception of Pestilence. Cambridge University Press; New York: 1992. [Google Scholar]
- Rosenberg Charles. Cambridge University Press; New York: 1992. Explaining Epidemics and Other Studies in the History of Medicine. [Google Scholar]
- Schillmeier M. Globalizing risks. The cosmo-politics of SARS and its impact on globalizing sociology. Mobilities. 2008;3(2):179–199. [Google Scholar]
- Serres M. The Johns Hopkins University Press; Baltimore: 2007. The Parasite. [Google Scholar]
- Sida Annual Health . Faculty of Veterinary Medicine and Animal Science; Stockholm: 2009. Synopsis of an Open Seminar on One World One Health. [Google Scholar]
- Silverman D. Gower; Aldershot: 1985. Qualitative Methodology and Sociology: Describing the Social World. [Google Scholar]
- Van Dijk T. Principles of critical discourse analysis. Discourse Soc. 1993;4(2):249–283. [Google Scholar]
- Van Loon J. Epidemics space. Crit. Public Health. 2005;15(1):39–52. [Google Scholar]
- Wagner-Egger P. Lay perceptions of collectives at the outbreak of the H1N1 epidemic: heroes, villains and victims. Public Underst. Sci. 2011;20(1):442–445. doi: 10.1177/0963662510393605. [DOI] [PubMed] [Google Scholar]
- Watts S. Yale University Press; New Haven and London: 1997. Epidemics and History. Disease, Power and Imperialism. [Google Scholar]
- Webby R., Webster R. Are we ready for pandemic influenza? Science. 2003;302(November):1519–1522. doi: 10.1126/science.1090350. [DOI] [PubMed] [Google Scholar]
- Wildlife Conservation Society . The Rockefeller University; New York, NY: 2004. Conference Summary. One World One Health: Building Interdisciplinary Bridges to Health and Globalized World. [Google Scholar]
- Willig C., Stainton-Rogers W. Sage; London: 2008. The Sage Handbook of Qualitative Research in Psychology. [Google Scholar]
- World Bank/OIE . 2008. Prevention and Control of Animal Diseases Worldwide.http://www.oie.int/eng/OIEWB_Conference_1007/en_Global_Animal_Health_Initiative.htm (Economic Studies). Available at: [Google Scholar]
- Wodack R., Meyer M. Sage; London: 2009. Methods of Critical Discourse Analysis. [Google Scholar]
- World Health Organization . WHO; 2005. Handbook for Journalists: Influenza Pandemic.http://www.who.int/csr/don/Handbook_influenza_pandemic_dec05.pdf Available from: (accessed 05.08.12) [Google Scholar]
- World Health Organization (WHO) WHO Website; 2008. Contributing to One World, One Health. A Strategic Framework for Reducing Risks of Infectious Diseases at the Animal–Human–Ecosystems Interface. Consultation Document (un-influenza.org/files/OWOH_14Oct08.pd) [Google Scholar]
- World Health Organization . WHO; 2008. International Health Regulations (2005)http://whqlibdoc.who.int/publications/2008/9789241580410_eng.pdf Available from: (accessed 05.08.12) [Google Scholar]
- World Health Organization . WHO; May 7, 2009. Joint FAO/WHO/OIE Statement on Influenza A(H1N1) and the Safety of Pork.http://www.who.int/mediacentre/news/statements/2009/h1n1_20090430/en/index.html Available from: (accessed 05.08.12) [Google Scholar]
- World Health Organization . WHO; 2009. Pandemic Influenza Preparedness and Response.http://whqlibdoc.who.int/publications/2009/9789241547680_eng.pdf Available from: (accessed 05.08.12) [PubMed] [Google Scholar]
- World Health Organization . WHO; 2009. Whole of Society Pandemic Readiness.http://www.who.int/influenza/preparedness/pandemic/2009-0808_wos_pandemic_readiness_final.pdf Available from: (accessed 05.08.09) [Google Scholar]
- Yin R. Sage; London: 2009. Case Study Research: Design and Methods. [Google Scholar]
- Yang The transmissibility and control of pandemic influenza A (H1N1) virus. Science. 2009;326(October):729–733. doi: 10.1126/science.1177373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimmer Sam. Historical perspective: emergence of influenza A (H1N1) viruses. N. Engl. J. Med. 2009;16(July):279. doi: 10.1056/NEJMra0904322. [DOI] [PubMed] [Google Scholar]