

Abstract
In the Spring of 2003, there was a huge interest in the global news media following the emergence of a new infectious disease: severe acute respiratory syndrome (SARS). This study examines how this novel disease threat was depicted in the UK newspapers, using social representations theory and in particular existing work on social representations of HIV/AIDS and Ebola to analyse the meanings of the epidemic. It investigates the way that SARS was presented as a dangerous threat to the UK public, whilst almost immediately the threat was said to be ‘contained’ using the mechanism of ‘othering’: SARS was said to be unlikely to personally affect the UK reader because the Chinese were so different to ‘us’; so ‘other’. In this sense, the SARS scare, despite the remarkable speed with which it was played out in the modern global news media, resonates with the meanings attributed to other epidemics of infectious diseases throughout history. Yet this study also highlights a number of differences in the social representations of SARS compared with earlier epidemics. In particular, this study examines the phenomena of ‘emerging and re-emerging infectious diseases’ over the past 30 or so years and suggests that these have impacted on the faith once widely held that Western biomedicine could ‘conquer’ infectious disease.
Keywords: SARS, Social representations, Newspapers, Infectious disease, UK
Introduction
Severe acute respiratory syndrome (SARS) first came to the attention of the World Health Organisation (WHO) at the end of February 2003 in Hanoi, Vietnam. The disease manifests as a fever, lasting 3–7 days, followed by a period of breathlessness and chest pain. Around 15% of patients affected required artificial ventilation and there was a relatively high death rate, in the order of 5%. By the third week in March, several hundred people were infected, with cases reported in Hong Kong, Singapore, Toronto, New Jersey, California and Bangkok (Zambon & Nicholson, 2003a).
The WHO then took the unusual step of issuing a worldwide alert. SARS was first reported in the UK newspapers on the 16 March 2003. This paper examines that reporting in the initial period following the ‘emergence’ of SARS. Social representations theory (SRT) is used to explore the meanings of this new disease. It also compares the way that SARS and other new infectious diseases are reported. In particular, it will compare the initial reporting of SARS with that of AIDS and Ebola.
Social representations theory
SRT holds that widely held shared ideas emerge spontaneously when a society is faced with a new phenomenon. These are a collective coping mechanism which help people by imposing order on a seemingly chaotic and unpredictable novelty. The mass media is the major source of these representations, and both cultivates and reflects them. Social representations are best studied when ‘new’ concerns arise for different groups, for example genetic engineering or modern biotechnology (see, for example, Wagner, Kronberger, & Seifert, 2002). A social representation consists of knowledge shared by members of a community about a given subject. It is disclosed by methodical study of the “common sense” knowledge of non-specialists on the subject. ‘Representations are embodied in communication and in individual minds, shared in a way similar to language’ (Bauer & Gaskell, 1999, p.167). These representations construct the world through images, terms, descriptions, examples, models and metaphors. Thus in this paper I do not attempt to measure what ‘the general public’ or even the ‘reading public’ think in the way that a ‘media effects’ approach would. Instead, here I will focus on the media representations.
Examining the reporting of new infectious diseases in the newspapers highlights wider contemporary public anxieties, in particular anxieties both about the apparent inability of technology (and biomedicine) to contain new threats and concerns about globalisation. Globalisation can mean many things: it is for many the worldwide spread of information, lifestyles, culture and technologies. But for many commentators, globalisation is primarily an economic force, implying that (nearly) all national economies are now networked with other economies around the world (Beck, 2000). One of the consequences of economic globalisation and the weakening of the nation state is greater mobility of people, both rich and poor. Another is a greater awareness of global ecological threats and the threat of global epidemics.
There are a number of different models of risk used in the social sciences: One is the Realist approach, where risk is seen as an objective hazard, threat or danger that exists ‘out there’ and can be measured independently of social or cultural forces, although risk may be distorted through social or cultural interpretations. The calculations the ‘expert’ provides about risk tend to be treated as if they were value-free, unbiased ‘objective’ facts (Lupton, 1999). Another model of risk is the Social Constructionist approach, which sees risk as an objective hazard, threat or danger but one that is inevitably mediated though social and cultural processes. This approach does not argue about the realities of the risk, but rather focuses on how they are politicised. Beck (1992) coined the term the Risk Society to characterise what he sees as this constant perception in late industrial or post-modern society of risk everywhere. But according to Joffe (1999), the ‘risk society’ does not necessarily leave people with a heightened state of anxiety. Rather people have defence mechanisms, namely their representations of risks, which function to control anxiety.
Contagion and containment
In 1972, Frank MacFarlane Burnet, the eminent Australian immunologist wrote:
On the basis of what has happened in the last thirty years, can we forecast any likely developments for the ‘70's? If for the present we retain a basic optimism and assume no major catastrophes occur and that any wars are kept at the ‘brush fire’ level, the most likely forecast about the future of infectious disease is that it will be very dull (MacFarlane Burnet & White, 1972, p. 263). (my italics)
With hindsight, MacFarlane Burnet's optimism was of course unfounded. Since 1973, over 20 new infectious diseases have been identified by the United States Centre for Disease control in Atlanta, including Ebola, AIDS, hepatitis C and vCJD (Satcher, 1995). SARS is just the latest to be added to this list. Some of these ‘emerging infectious diseases’ such as AIDS or Brazilian purpuric fever can be regarded as genuinely new. Others such as Hantaan viruses have been known in Asia for centuries but are now ‘emerging’ in other parts of the world. Hemorrhagic fevers such as Ebola have been recognised for a relatively long time. By ‘emerging’ what is more usually meant for a Western reader is ‘emerging from the poor’, in particular the poor in the developing world. The ‘emergence’ relates to modern communication and the media ‘Symbolically, if not epidemiologically, Ebola spread like wildfire—as a danger potentially without limit. It emerged’ (Farmer, 1999, p. 46).
Emergence is rarely a purely virological event without identifiable causative co-factors. Even where microbes have evolved, humans have usually played a large role in enhancing pathogenicity. The underlying factors which are responsible for the emergence of new infectious diseases are: agricultural or economic development; anomalies or change in climate; human demographic changes caused by migration, war, rural urbanisation and human behaviour (such as changing sexual mores and intra-venous drug use); travel and commerce; technology and industry (modern food production methods and hospital acquired infections for example); microbial adaptation and change (antibiotic resistant bacteria for example); or a breakdown in public health measures (Morse, 1995). Not surprisingly, these underlying factors tend to be the highlighted when these diseases are reported in the newspapers.
HIV/AIDS and Ebola
AIDS has been a news story now for over 20 years but here I will focus on news coverage in the very early days of the epidemic. In the US and the UK, there was remarkably little coverage of the new disease on its first appearance. Coverage in the mainstream US press was ‘virtually non-existent’ for the first 2 years following the identification of the new disease (Allen, 2002, p. 122). Only in May 1983, when an editorial in The Journal of the American Medical Association raised the proposition that HIV might be transmissible to the entire population through ‘routine close contact’ did the US news media pick up the story in earnest.
Media editors on both sides of the Atlantic refused to see how a story about homosexuals and drug users could interest their audiences. For them it failed the test of newsworthiness that other diseases such as Legionnaires or Toxic Shock Syndrome passed because editors felt the latter threatened people like them, whereas AIDS did not. This angle was taken as common-sense in newsrooms. In the early days of the epidemic, both in the US and the UK, the dominant representation of AIDS was that of a ‘gay plague’.
Perhaps the most insidious dimension of the plague metaphor was the way in which it contributed to the normalization of an ideological dichotomy between alien, less than human ‘others’, on the one hand, and everyone else, on the other, during the initial stages of the moral panic. In the case of news reporting, the underlying imperatives of this ‘us’ versus ‘them’ dichotomy began to cohere as a form of prejudice from the outset. (Allen, 2002, p. 128)
Overwhelmingly in the case of AIDS (at least in the early days of the epidemic), gay men bore the brunt of the blame for the epidemic, although later ‘foreigners’ and other marginal groups in or outside the ‘general population’: in particular prostitutes and drug addicts were blamed (Sacks, 1996). Different groups blamed ‘other people’ (people not like us) for AIDS, the common factor being the shifting of the blame to the ‘other’, people outside of one's own community (Park, 1993; Treichler, 1988; Joffe, 1999; Farmer, 1999; Goodwin et al., 2003).
The reporting of Ebola
In his review of how newspapers cover emerging diseases, Ungar (1998) writes that the pattern that usually follows in newspaper reporting is that initially the ‘emerging’ disease is characterised as a frightening threat. What he calls the mutation-contagion package is composed of the following core ideas: that microbes are on the rampage and that we are experiencing a ‘wave of new assailants’; that microbes are cleverer than us and are evolving to ‘outwit us’; that microbes and environment are conjoined in an ecological parable, and that population growth, environmental degradation and factors such as antibiotic overuse are responsible for this unfolding catastrophe; that microbes know no boundaries (through globalisation and travel); and that we are waiting for the next plague (apocalyptic prophesy). This package is clearly constructed around a frightening core with few instances of reassurance. However frightening this may be, the sense of threat is still somehow hypothetical. The diseases themselves and the likelihood that readers will be personally affected (at least for now) remain abstract and distant as the threat tends to arise in geographically distant or marginal populations. At the same time, the threats are offset by the promise of ‘medical progress’, which presents a stream of ‘amazing new discoveries’. Soon after the initial reporting however, the tone of newspaper coverage tends to shift to what Ungar (1998) calls the containment package, which aims to defuse the potential panic that emerges early in the coverage. This containment package is “erected on the metaphor of ‘otherness’” (Ungar, 1998, p. 49).
Ebola first appeared in Africa in 1976, but generated little news interest in the Western press. Yet by the time it reappeared in Zaire in 1995/96, the climate had changed and ‘emerging infectious diseases’ were clearly much higher on the news agenda. Ungar (1998) uses his framework for reporting of other infectious diseases to examine the newspaper coverage of the 1995 Ebola outbreak in Canadian, the US and the British newspapers. He argues that the coverage embodies many of the most terrifying aspects of the mutation-contagion package: Ebola comes from elsewhere, fits the ecological parable, and is always paired with ‘killer’ or ‘deadly’, and is almost always accompanied by descriptions of liquefying organs and profuse bleeding. What characterised the Ebola coverage was that it could be the harbinger of a wider pandemic and attendant panic. ‘Ebola, as the embodiment of the mutation-contagion package, represents a monster virus on a potential rampage’ (Ungar, 1998, p. 47).
But after just a few days, what Ungar (1998) calls the containment package appears and the focus of the threat moves from the virus itself to Africa's hospitals. The ‘appalling sanitary conditions’ of many African hospitals are contrasted with the exemplary protective methods of the Western experts. A few days later, there is a further shift in the tone of the newspaper coverage, as attention is given to Western health teams, who, as opposed to the chaos in Zaire, are ‘disease detectives’. By now Ebola is treated not as a rampaging virus, but as a disease that is difficult to catch. In particular, the ‘stepping off a plane scenario’ (where a person can travel across the world whilst carrying the infection) is undermined, often in the very newspapers who days before espoused it, as journalists begin to report that people with Ebola are not infectious until ill, and then unlikely to be allowed to catch a plane.
Joffe and Haarhoff's (2002) analysis of the newspaper coverage of the same Ebola outbreak found that all articles about Ebola in the UK mentioned Africa; almost half linked this to monkeys; another half linked this to the lack of appropriate medical facilities there to deal with it. Beyond this, other factors implicated in the spread of Ebola are poverty, pollution, forest environment and tribal rituals. By symbolising Ebola as essential to Africa as a whole, it implies that such disasters are ‘incontrovertibly African’ (disaster ridden), and by implication that the West is superior. In terms of whether Ebola is a threat, the newspapers evoke fear by highlighting how terrifying and horrific it is (providing vivid descriptions of liquefying bodies); and by comparisons with AIDS. Alongside the fear theme, the articles are pervaded by an emphasis on how Ebola can be brought under control by isolation, quarantine and surveillance (by Westerners), at the same time rarely alluding to the role played by Africans, who are portrayed as passive and voiceless. The way that reassurance is provided is through the notion that Africa and the Africans are so different to ‘us’ (so ‘other’) that the disease will be contained, and will in reality provide nothing more that a hypothetical threat.
The strategy of othering is a direct counterpoint to the theme of globalisation… Whereas globalisation is predicated on a levelling of nations and individuals, othering aims to reverse the rites of inclusion and protect the social order by erecting barriers of exclusion. (Ungar, 1998, p. 52)
The discussion of the ‘othering’ in the context of AIDS and Ebola connects with Said's (1978) account of Orientalism, in which he argues that the construction of identity involves establishing opposites and what he labels ‘others’, ‘whose actuality is always subject to the continuous interpretation and re-interpretation of their differences from ‘us’’ (Said, 1978, p. 332). His central point is to contest the idea that there are geographical spaces with indigenous, radically “different” inhabitants who can be defined on the basis of some religion, culture or racial essence. Orientalism is a collective notion identifying “us” Europeans against “those” non-Europeans, and advocating that European identity is superior to all the non-European peoples and cultures. The resulting portrait of “us” and “them” is reductive and ‘invidiously ideological’; where the West is portrayed as:
rational, developed, humane, superior and the Orient, which is aberrant, undeveloped, inferior…the Orient is at bottom something either to be feared (the Yellow peril, the Mongol hordes, the brown dominions) or to be controlled (by pacification, research and development, outright occupation wherever possible). (Said, 1978, pp. 300–301)
Method
SARS was first reported in the UK newspaper on Sunday 16 March 2003. In the weeks that followed there were an increasing number of newspaper articles (up to a peak of 182 on 25 April), although interest tailed off after a point (see Fig 1 ).
Fig 1.
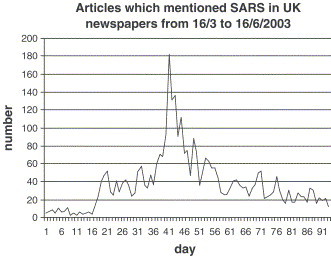
Source: Lexis-Nexis professional.
This research considered the first 4 weeks following 16 March 2003, so as to examine how the initial responses to this new threat were articulated. The sample was all the articles which mentioned SARS in the Sunday UK national newspapers only. The Sunday national newspapers in the UK (Independent on Sunday, Mail on Sunday, News of the World, Observer, People, Sunday Express, Sunday Mirror, Sunday Telegraph and Sunday Times) represent a broad spectrum of political viewpoints from left to right, as well as a spectrum of ‘highbrow’ to ‘lowbrow’ viewpoints (broadsheet to tabloid). Many of the articles that appeared in the daily newspapers on SARS were short descriptive pieces on how many new cases of SARS had been reported, or how a particular case in the UK had been confirmed or ruled out as having in fact been SARS. By contrast, the Sunday newspapers contained many longer articles on SARS, which were often more analytical and frequently more lurid. The final reason for the choice of Sunday newspapers was that by sampling every 7 days, it was possible to get a ‘feel’ for how the coverage had shifted focus over the course of the preceding week.
The full-text of all the articles about SARS in the UK national Sunday newspapers for the five Sundays following the first reports of SARS (16 March–13 April 2003 inclusive) were downloaded from the Lexis-Nexis news service on the Internet (74 articles: four on 16 March, 11 on 23 March, 6 on 30 March, 29 on 6 April and 24 on 13 April). Research has shown that the UK medical journalists rely almost exclusively on the British Medical Journal and The Lancet as the source of their stories (Bartlett, Sterne, & Egger, 2002; Entwistle, 1995). Therefore, all the articles and editorials on SARS from the British Medical Journal and The Lancet for the same 4-week period following the announcement of SARS were also downloaded as full-text from the journals’ Internet sites (16 articles).
All the documents were then analysed using ATLAS/ti 4.2 qualitative research software, with an initial coding frame based on Joffe and Haarhoff's (2002) and Ungar's (1998) work on Ebola, although new themes emerged and were included as the analysis proceeded. See Table 1 for the full coding frame and occurrences.
Table 1.
Codes and occurrences
| Code | Week 1 | Week 2 | Week 3 | Week 4 |
|---|---|---|---|---|
| Black humour | 11 | 0 | 5 | 3 |
| Difficult to catch | 2 | 0 | 1 | 2 |
| Earlier epidemics | 0 | 0 | 16 | 1 |
| Effect on economy | 0 | 7 | 21 | 12 |
| Environmental degradation | 1 | 1 | 0 | 0 |
| Geographically distant | 6 | 0 | 2 | 0 |
| Globalisation | 2 | 3 | 5 | 2 |
| Graphic description | 2 | 0 | 0 | 0 |
| Insanitary conditions | 14 | 1 | 6 | 2 |
| Killer/deadly | 1 | 4 | 7 | 3 |
| Local corruption | 1 | 8 | 4 | 0 |
| Local customs | 0 | 1 | 6 | 0 |
| Marginal populations | 0 | 0 | 0 | 0 |
| Medical miracles | 2 | 0 | 6 | 0 |
| Microbes evolving | 6 | 4 | 9 | 3 |
| New microbial threat | 2 | 3 | 15 | 4 |
| Next plague | 5 | 0 | 1 | 0 |
| Passive locals | 0 | 0 | 1 | 0 |
| Patient zero | 5 | 3 | 6 | 6 |
| Population growth | 0 | 1 | 0 | 0 |
| Poverty | 0 | 0 | 1 | 0 |
| Travel | 6 | 7 | 17 | 4 |
| War | 0 | 0 | 9 | 4 |
| Western doctors | 6 | 8 | 19 | 3 |
The spike in Fig. 1 occurred on Friday 25 April when 182 articles in the UK national newspapers mentioned SARS. Several news items appeared that day, although the cumulative total of news stories around SARS had been building all week: Dr. Liam Fox, the UK shadow health secretary, accused the Government of being “feeble, complacent and irresponsible” and called for SARS to be made a notifiable disease. A WHO official announced that travel restrictions to some areas affected by SARS would possibly be eased over the forthcoming few weeks; The Organisation for Economic Co-operation and Development (OECD) said SARS could lead to “severe macroeconomic consequences” for Hong Kong and East Asia; and The World Bank announced it was cutting its forecasts for economic growth in East Asia because of the virus; Finally the tabloids carried the story that television soap opera star Todd Carty had been admitted to hospital with ‘mysterious SARS-like symptoms’.
Results
Table 1 shows the numbers of occurrence of quotes under a particular code for that week.
In the very first reports of SARS on 16 March, all the articles referred to the new illness as a ‘killer bug’ or to a ‘mysterious’ ‘lethal’ ‘deadly pneumonia virus’. This new ‘threat’ was described as ‘moving at the speed of a jet’ and people affected were not responding to traditional treatments. Combined with adjectives like ‘untreatable’ were some graphic descriptions of how the “victims’ lungs swell and they suffocate”.
In the British Medical Journal of the 22 March, there was already speculation as to the origins of the virus which was thought to be an influenza virus or the Hong Kong Avian Flu. In The Lancet of the same day, whilst focusing on the Western Authorities which were investigating the illness, they also said that ‘a WHO team is working closely with the Chinese authorities’. Both journals mentioned that chlamydia was also found by the Chinese authorities in the lung tissue of many of the early cases. The Lancet also mentioned that bioterrorism had not been ruled out as a possible cause.
Within 7 days of the first reports, speculation began in the newspapers about both the origin of SARS and the outcome of the unfolding epidemic. There was speculation that the ‘bug’ (usually referred to by the second week as a virus) had ‘mutated’ from horses or pigs. This was usually combined with explanations of how AIDS had jumped species from monkeys. In particular, there were descriptions of life in “rural China, where people routinely live in insanitary, cramped conditions in close proximity to poultry and other animals” (McDonald & Rogers, 2003).
At this early point there were several stories about how this could be ‘the next plague’. One byline from The Sunday Telegraph of 23 March sums this theme up: ‘The next pandemic is now ready for take-off. The devastating effects of a mystery pathogen have given rise to fears of a modern-day Black Death. Doctors say it is not a question of if such a virus will emerge but when—and, …millions of air travellers could spread it around the globe’. Other epidemics with death tolls in the millions were frequently cited: such as Spanish flu and AIDS.
Also frequently mentioned, even at this early stage, were how Western doctors and authorities were moving quickly and using their expertise to contain the threat or how British scientists were working ‘flat out’ to process samples sent by worried doctors who acted with ‘military precision’. Apart from Hong Kong scientists and authorities, Chinese authorities were only mentioned insofar as Western scientists were ‘helping the Chinese communicable disease surveillance network in its attempts to track the infection’.
By the second week there were also beginning to be reports of SARS's own ‘patient zero’. [In the early days of AIDS, epidemiologists established that at least 40 of the first 248 gay men diagnosed with AIDS in the US had sexual links with a Canadian air steward, Gaetan Dugas, who was controversially dubbed patient zero (Shilts, 1987). The term is used in the newspapers in the context of SARS without any explanation of its origins.] One particularly lurid piece, told of how ‘As he shuffled through the lobby of the Hotel Metropole, the elderly professor was feeling feverish and faint. At the lift, he steadied himself for a moment in the open doorway before his body convulsed in a series of wracking coughs that sprayed fine droplets of saliva onto the walls and the people waiting inside.’ (Fraser, 2003)
On the 29 March, the British Medical Journal editorial set the tone for much of the newspaper coverage that weekend. ‘Sudden acute respiratory syndrome—May be a rehearsal for the next influenza pandemic’
Plagues are as certain as death and taxes. The optimism of the 1960s and 1970s has given way to a mature realism that the relationship between human beings and microbes is neither completely predictable nor biased in favour of humans… The speed of travel favours intercontinental spread of disease. The rapid dissemination of sudden acute respiratory syndrome around the world should be considered a rehearsal for the next pandemic of influenza, as it shows what will happen with a new human virus spread by the respiratory route, with no vaccines and antivirals in limited supply. However, the speed of communication in the virtual world is an advantage to the microbial detective. The tried and trusted forensic approaches of the classical virologist, the electron microscope and the tissue culture plate, become powerful investigative tools when the images of a suspect can be shared immediately between laboratories thousands of miles apart. (Zambon & Nicholson, 2003b, p. 669)
Here we see two of the elements which were to be central to newspaper coverage throughout this period: this could the next plague, but followed immediately by the reassurance that Western scientific biomedicine can successfully contain it. The British Medical Journal and The Lancet contained long descriptions of which laboratories and which experts were investigating SARS. Another theme which emerged in both medical journals and the newspapers was the ‘scepticism’ about the official Chinese figures for the disease.
By the third Sunday (30 March), there was a marked shift in the coverage of SARS in the newspapers. Three strands of the story dominate: one about local (Chinese) corruption and inefficiency, and another about Western doctors, and finally about the effect that SARS was beginning to have on the local and international economy. The first strand followed the admission by Chinese officials that the original estimates of numbers were too low. ‘Traditional Chinese reticence’ was widely criticised. Chinese officials were widely reported to have ‘covered up existence of killer pneumonia’. By contrast, Western ‘health experts’ were said to be critical of ‘the secretiveness’ of Chinese authorities, and that it had ‘delayed efforts to combat the disease’. Unidentified Chinese journalists were also widely reported as saying that the Chinese authorities thought that news of the outbreak would ‘spoil the city's image’ and that rumours of the illness would lead to panic.
The second major strand of the story concerned the death from SARS of Dr. Carlo Urbani, the Italian communicable diseases doctor who worked in Thailand for the WHO. The WHO issued a press statement praising Dr. Urbani, crediting him as being ‘the first World Health Organization (WHO) officer to identify the outbreak of this new disease’ (WHO, 2003a). However, the newspapers credited him with being ‘the first person’ to identify the disease.
The third strand that emerged by the end of March was the effect on the economy and on daily life, particularly in Hong Kong. There were descriptions of deserted shopping malls, cinemas and restaurants; cancelled concerts, sporting fixtures and other public events; people wearing face masks in the street; banks and businesses closed. There was news of screening air travellers but as yet there was little mention of the effect of SARS on the travel industry.
There were further descriptions of the poor hygiene standards of the Chinese, and a new aspect started to be mentioned: spitting.
This is a common habit in southern China, where most people cough and sneeze without covering their faces. Pools of saliva are frequent sights in restaurants, trains and buses.
Epidemiologists say such practices, combined with overcrowding and pollution, plus a history of viral outbreaks jumping from pigs and poultry to humans, make Guangdong province one of the world's most dangerous breeding grounds for infectious viruses. (Sheriden, 2003)
Here we see the seeds of a number of themes which were to grow in importance over the next few weeks: spitting, pollution, dirt, living close to animals and previous epidemics.
The British Medical Journal and The Lancet of the 5 April were focussed on the search for the cause for SARS and how Hong Kong scientists had discovered the coronavirus responsible, findings which were corroborated by other Western scientists. Another aspect of the story given wide coverage in both journals was the ‘slowness’ of the Chinese authorities in reporting the initial outbreak to the WHO. The medical journals also reported the effect on the economy of Hong Kong.
By Sunday 6 April, the interest in SARS in the newspapers had increased greatly from the previous week. The main theme that occurs by this point was the effect that SARS was having on the economy, particularly the Hong Kong economy, where major banks such as Morgan Stanley and Goldman Sachs were warning that the epidemic could tip the whole of Asia, and subsequently the world into a ‘global slowdown’. Staff of Western companies in China and Hong Kong were ordered to stay home. The other sector of the economy affected was the commercial airlines and tour operators. British Airways was one of several airlines to announce that it was cutting flights to and from Hong Kong, reflecting decreased demand. Predictions were made that SARS could be the final straw for several airlines that were already in a weakened financial state following the war in Iraq.
After the effect on the economy, by this point the most frequently occurring theme was the role of Western doctors and authorities in controlling the epidemic and searching for its cause and cure (disease detectives). Scientists were mentioned (by name) in Winnipeg, Atlanta and London, often reporting that they were on the ‘verge of a breakthrough’ or that ‘a test is only days away’ (medical miracles). Because these are British newspapers, it is perhaps not surprising that they focused particularly on Dr. Maria Zambon's work at the Collingdale laboratory in North London:
“It is like a detective game, only on an extraordinary international scale”, she explained
In a week which has seen the number of cases leap fivefold, her efforts could not be more crucial. Dark lines under her eyes attest to the fact that Zambon, mother of a young son, has spent the last three weeks analysing data and looking at samples late into the night. (Revill & Aglionby, 2003)
Virologist Professor John Oxford of the University of London was widely quoted as saying that he did not think that SARS would constitute a major epidemic, as it was geographically distant, difficult to catch and tended to adversely affect those whose immune systems were already compromised by the secondary effects of poverty. However, his reassurances were often followed by death tallies from other past epidemics, and estimates that apart from the 2409 cases by then confirmed, as many as another 24,000 could be spreading the virus. (A few weeks later, after the time frame of this project, there were predictions that SARS could kill millions.)
Another feature at this point in the reporting was the way that earlier epidemics are recounted, e.g. ‘the fatal flu virus of 1918’. The themes of microbes mutating, evolving, of new microbial threats and how ‘we are waiting for the next big one’, were by this point well established. A frequently recurring theme was that SARS could mutate into a more infectious and potentially more lethal form. China in particular was said to be the source of so many of these epidemics because of its insanitary conditions and its reliance on fowl farming, where influenza viruses are said to originate (although scientists were not sure at this point that SARS was either a zoonose or an influenza virus). Bubonic plague, cholera, smallpox, etc. were all described, with their death counts. Ebola and AIDS were also described, thus contextualising SARS as a threat on a similar scale. Scientific theories as to what actually causes SARS were widely reported, though not with any great clarity. Also reported were theories as to how SARS was being spread: airborne, by droplet or by the sewerage system.
Chinese Communist party officials were blamed for covering up the scale of the epidemic. Their complaints that the response to SARS in Hong Kong was ‘hysterical’ were taken as further evidence that they were dangerously underplaying the seriousness of the epidemic. In contrast to the descriptions of deserted Hong Kong, the city of Guangzhou, the capital of Guangdong and the putative source of the epidemic, was described as carrying on business as normal. Again Chinese conditions were blamed squarely for the emergence of this virus which was assumed to have jumped species because of Chinese hygiene, fondness for exotic foods and farming methods. The following is a typical example (from a broadsheet, The Sunday Times):
Just a six miles north of the city lies old China, which has yet to be sanitised by steel and concrete. The main market for live animals is like a scene from a virologist's nightmare: slaughtered carcasses of dogs, pigs and cows are steamed and skinned by teams of bare-handed workers.
Blood, skin and offal are stamped into the mud, mingling with the droppings of ducks and chickens confined by the thousand in cages. As one trader boasts: “We Cantonese like our food so fresh we prefer to buy it alive.”
Experts believe the proximity of animals and humans in unsanitary conditions explains why viruses here often “jump the species barrier”, usually from poultry, which have weak immune systems, to pigs and thence to people.
Add the Chinese peasant habits of frequent spitting, coughing and sneezing without covering the face, and all the ingredients for an epidemic are in place. (Sheriden & Rogers, 2003)
Another similarly lurid example (from another broadsheet, The Independent on Sunday) reads:
…in the narrow streets of the old town by Shamian Island on the Pearl river, a clue can be found to the source of the virus. You can buy live scorpions by the jar here. Women using chopsticks deftly lift them one by one from red, round plastic tubs containing a seething mass of the creatures. There are puppies and kittens in tiny cages, tanks of fish, terrapins and tortoises of all sizes, five mice in a row, turning their wheels and a family of sleepy rabbits. Half-gallon jars of five- snake wine, the skins of the reptiles gleaming in the amber liquid, stand next to bottles of black ant wine and cock testis wine, revered for their health-giving properties.
The Chinese fondness for animals and birds, and the proximity in which they live to them, provides ideal conditions for viruses to jump to humans. Reports last week suggested that the first cases of Sars in Guangzhou were seen among bird vendors and chefs. Bi Shengli, a virologist from the Chinese Centre for Disease Control, said: “Guangdong people like eating exotic animals and I don’t find it a healthy practice.”
It is not the only dubious tradition. As I watched a man buying scorpions, the woman serving him hawked a gob of sputum from her throat, lurched to her feet and spat expertly behind my heel. Spitting is as natural as sneezing here–bubbles of phlegm pepper the streets–and could be spreading the virus. Of such simple habits are global epidemics made. (Laurance, 2003)
By this point, the themes of difference, of dirt and ‘our’ disgust at the way ‘they’ live and what ‘they’ eat begin to from into a coherent package. The (British) reader is led to place the responsibility for SARS at the feet of the Chinese and at the same time is reassured that ‘it couldn’t happen here’ because ‘we’ don’t live like that.
In the fifth week following the WHO announcement (13 April), the themes from the previous week have become embedded. The most frequent references were to effects on the economy, which by this stage was more usually taken to mean the ‘global’ economy. The microbes are evolving theme was combined with the patient zero theme to promote the speculative theory that so-called ‘super-carriers’ of infection who were without symptoms themselves were responsible for an unexplained cluster of cases in a Hong Kong residential tower block. Other ‘experts’ were reported to believe the cause was the sewerage system, or rats, cockroaches, or other insects ‘numerous in Hong Kong's tropical weather’. Some human interest is added by stories of boarding school children either being kept in the UK, or quarantined on their return from countries affected by SARS. Also reported was news that Prince Harry's school, Eton, had banned pupils returning from the Far East.
Before leaving the results of the newspaper reporting, which were on the whole largely similar in tone, I want to highlight one exception. Of the articles sampled over those four Sundays, one piece, by David Aaronovich, from The Observer of the 6 April questioned the appropriateness of the current panic over SARS. In it, he writes:
EVER SINCE WE settled down in cities and communities, we have been open to the possibility of communicable disease. And, in our folk history, most of this arises in the East, a treacherous result of trade and modernity. The Black Death is supposed to have originated variously in the Gobi desert, in Manchuria, or (best of all) ‘in the depths of Asia’, reaching Dorset in August 1348. The cholera pandemic that swept across England in 1832 was supposed to have entered on a ship from Hamburg, but to have started in Bengal. Latterly Africa has been fixed upon as an alternative starting place for terrible diseases. Teeming Asia or the Heart of Darkness—take your pick of which most frightens you.
This fear of epidemics and pandemics is interesting. In psychological terms it is a way of externalising evil and badness; the nastiness is placed outside us. (Aaronovitch, 2003)
Although he does not use the term, Aaronovitch's (2003) article is the only one from the sample which highlights the social representational aspect of SARS.
Discussion
The first interesting feature of the SARS phenomenon is the speed at which this whole episode unfolds, from first reporting, to panic, to a rather embarrassed silence—all in 3 months. We might contrast this to the response to AIDS in the early 1980s when the news media both in the UK and the US largely ignored the story for many months (years even) until it became clear that white heterosexual people (people like “us”) were at risk. The early Ebola outbreak in 1976 also got little attention in the news media. Yet SARS evoked a worldwide response almost immediately. This is no doubt partly due to the recent experience of AIDS, which alerts us all to the possibility of an obscure new disease becoming a pandemic which could kill tens of millions of people.
Another interesting result which fits with earlier studies is the dynamic between posing the threat and almost immediately de-emphasising it. Ungar (1998) noted in his analysis that the threat of contagion is almost immediately followed by the reassurance of containment. This pattern is clearly replicated in the case of SARS reporting. The first descriptions always talk of the new threat being a ‘killer’ or ‘deadly’, and early on speculation follows on how the epidemic will play itself out. The predictions were dire: this could be the ‘next plague’, the ‘big one we’ve been waiting for’ and so on. But the melioration comes almost immediately when it is acknowledged that this probably is not ‘the big one’ but rather can be seen as a rehearsal for it. The threat, the risk, is postponed, but at the same time kept fresh in our minds.
The SARS epidemic occurred at roughly at the same time as the US and the UK were invading Iraq. (The White House announced that the war had begun on the 20 March 2003.) Possibly the media attention on the war in Iraq kept SARS out of the newspapers to a certain extent. Although there was some speculation at the outset that SARS may be connected to bioterrorism, this was discounted early on. Mentions of the war in the newspapers in connection with SARS were usually simply to say that the war, in combination with SARS, was damaging the economy, in particular the commercial airlines. But the general sense of gloom and pessimism emanating from the ongoing so-called “war on terror” does perhaps pervade the reporting of SARS, albeit in a subtle way.
For example, the millennialism and sense of impending apocalypse is greeted with something approaching warmth, as if ‘we’ deserve it for ‘interfering with nature’. Earlier epidemics are invoked, together with their death tolls: the Black Death, Spanish Flu and AIDS. For example, in the context of SARS the Spanish Flu epidemic of 1918 which killed around 40 million people was widely recalled; as opposed to, for example, the West Nile Virus outbreak in the New York in 1999 where there were (only) 62 cases and seven deaths (with 4156 US cases and 284 deaths since then) (PHLS, 2003). Or another more relevant example which was infrequently cited in the coverage of SARS is the case of vCJD. There have been 137 cases vCJD of which 132 have died (up to 2003), but again this is very much lower than the figures that some were predicting at the height of that particular media scare (The UK CJD Surveillance Unit, 2003). This use of earlier epidemics to illustrate the devastating potential of SARS was one of the features of the SARS reporting which is not present in the analyses of Joffe and Haarhoff (2002) and Ungar's (1998) work on Ebola (and which warranted a new code to be added to the coding frame here).
Joffe (1999) points out that the link between a new disease and previous ones is made by this anchoring mechanism, which integrates the understanding of a new phenomenon by configuring it in terms of past epidemics (e.g. AIDS was initially configured in terms of earlier epidemics which had been linked to foreigners, out groups and perverse practices). Why then are some past events and not others chosen to anchor the new phenomenon? According to Joffe (1999), the motivation is primarily to do with identity protection, which refers simultaneously to the protection of the in-group and self-identity (and to building its cohesion by negatively distinguishing the ‘other’ from it). Anchors are devices that the group finds comfortable, familiar and acceptable. At the same time, the chosen representation maintains the status of certain groups in society.
In making a comparison of the SARS coverage with that of Ebola, what is also worth noting is what themes featured in the coverage of Ebola but not in the case of SARS. There were very few graphic descriptions of the disease, as there had been with Ebola; and there only a handful of occurrences (n<5) throughout the whole 4 weeks newspaper sample of any of the following codes: poverty, population growth, environmental degradation; marginal populations, difficult to catch; geographically distant. The depictions of locals as passive, that had been a feature of the Ebola coverage also received no mention in the SARS coverage. However, this is because the only mention of the (mainland) Chinese themselves in the newspapers is to describe their officials as corrupt, secretive, incompetent, chaotic or mendacious. The Chinese people themselves are not depicted as passive (as were the Africans in the Ebola reporting), but they are invisible: for example, Dr. Urbani became for the newspapers the first person to identify SARS, rather than the first WHO official. Yet the newspaper allegations of a Chinese cover-up reveal that Chinese doctors were aware of this new disease before Dr. Urbani reported it. The Chinese themselves are rarely quoted and their opinions rarely sought. The only time they are depicted is when vivid descriptions of the filth, sputum, live animals for food and so on which are clearly meant to invoke disgust at the way ‘they’ live. Interestingly, Hong Kong, which has only recently ceased to be a British colony, is regarded as Western from the point of view of the UK newspapers; it is only the mainland Chinese authorities and people that are treated as ‘other’.
Another feature of the reporting of SARS which was absent in coverage of Ebola was the effect on the economy (Ebola did not have any direct effect on the economy outside of the local area). The final difference between the SARS and Ebola coverage is that in the SARS case there are individuals who are targeted for blame: the ‘patient zeros’. Two people in particular are mentioned: one is the Professor in Hong Kong, and the other the index patient in Hanoi, who was the source of the cluster that alerted and ultimately killed Dr. Urbani.
But despite all these differences, there were many similarities between the coverage of SARS and Ebola. In particular, the way the readers’ fears are aroused and then almost simultaneously dampened through ‘othering’. The descriptions of the effect on daily life, particularly in Hong Kong: the deserted shopping malls, cinemas and restaurants; empty public transport; events where crowds would gather cancelled; the surgical face masks; all evoke either zombie or post-apocalypse horror-film imagery. Yet at the same time, we are told that ‘it couldn’t happen here’ because the Chinese are so different to ‘us’. As Africa and Africans were portrayed as disaster ridden in the case of Ebola, so China and the Chinese are portrayed as an inevitable breeding ground for new infections. Whether it be African local customs in the case of Ebola or Chinese ones with SARS, all confirm the African/Chinese as ‘other’ (and by implication inferior to ‘us’). And with both Ebola and SARS, the only hope of containment is provided by the promise of (Western) biomedicine.
Conclusion
Up to 11 July 2003, there were a cumulative number of 8437 confirmed cases of SARS worldwide of which 813 people died, with four cases and no deaths in the UK. The last case of this epidemic was reported in China on the 25 June 2003. On 14 July, the WHO stopped publishing a daily table of the cumulative number of reported probable cases of SARS (WHO, 2003b) (although there may of course be a recurrence of SARS in the future). SARS undoubtedly presented a serious risk to human health in the realist sense, insofar as it was contagious to people in very close contact to an affected person (family members and health care staff in particular), but very much less infectious to people in ordinary social contact with someone with the illness. It was an illness which killed around 5% of those affected, but mostly those with other underlying health problems, but which was very much less dangerous to those in the West who were well-nourished and in otherwise good health.
Modern biomedicine has delivered many remarkable successes in terms of infectious diseases over the past century. These successes are in part due to vaccination programmes, leading to the global eradication of smallpox, and dramatic reductions in the Western world in the incidence of, for example, diphtheria, polio, measles, whooping cough and mumps. Biomedicine has also produced major advances in drug therapy such as antibiotics leading to dramatic reductions in incidence of tuberculosis or syphilis for example (although incidence of both diseases is beginning to rise again in the West). Until the 1970s, there was a widespread notion within and outside of the medical profession that biomedicine could one day ‘conquer’ infectious disease. SARS is the latest in a growing list of newly emerging infectious diseases that have been reported over the last 30 or so years. In the light of the phenomenon of emerging and re-emerging infectious diseases, very few people still share that optimism.
Most epidemics throughout history have been global in the sense that they were not contained within national boundaries, travelling across land and sea if not by air. The spread of SARS was facilitated by the modern availability of air travel and by migration attendant on economic globalisation affecting the Far East. And ultimately the SARS epidemic was contained through surveillance and scientific investigation of its cause co-ordinated on a global scale.
But beyond the realist global epidemic of (the disease) SARS lies the globalisation of the phenomenon of the SARS panic, where the saturation and speed of the world news media's coverage leads to the (supposed) risk posed by SARS being socially constructed on a global scale. And yet despite the modernity of the medium, the message is almost comfortingly familiar: The social representation of SARS resonates with representations of infectious diseases throughout history: we lay the blame for the new threat on those outside one's own community, the ‘other’.
Acknowledgements
I would like to thank Jon Turney, Brian Balmer and Helene Joffe as well as my two anonymous reviewers for their invaluable comments on earlier drafts of this paper.
References
- Aaronovitch, D. (2003). Fever pitch: Once it was the chicken virus, then Ebola, now it's Sars. We worry too much. The Observer, April 6.
- Allen S. Open University Press; Buckingham: 2002. Media, risk and science. [Google Scholar]
- Bartlett C., Sterne J., Egger M. What is newsworthy? Longitudinal study of the reporting of medical research in two British newspapers. British Medical Journal. 2002;325:81–84. doi: 10.1136/bmj.325.7355.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bauer M., Gaskell G. Towards a paradigm for research on social representations. Journal for the Theory of Social Behaviour. 1999;29:163–186. [Google Scholar]
- Beck U. Sage; London: 1992. The risk society—towards a new modernity. [Google Scholar]
- Beck U. Polity Press; Cambridge: 2000. What is globalization? [Google Scholar]
- Entwistle V. Reporting research in medical journals and newspapers. British Medical Journal. 1995;310:920. doi: 10.1136/bmj.310.6984.920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farmer P. University of California Press; Berkeley and Los Angeles: 1999. Infections and inequalities—the modern plagues. [Google Scholar]
- Fraser, L. (2003). The next pandemic is now ready for take off. The Sunday Telegraph, March 23.
- Goodwin R., Kozlova A., Kwiatkowska A., Anh Nguyen Luu L., Nizharadze G., Realo A., Kulvet A., Rammer A. Social representations of HIV/AIDS in Central and Eastern Europe. Social Science & Medicine. 2003;56:1373–1384. doi: 10.1016/s0277-9536(02)00135-1. [DOI] [PubMed] [Google Scholar]
- Joffe H. Cambridge University Press; Cambridge: 1999. Risk and the other. [Google Scholar]
- Joffe H., Haarhoff G. Representations of far-flung illnesses: The case of Ebola in Britain. Social Science & Medicine. 2002;54:955–969. doi: 10.1016/s0277-9536(01)00068-5. [DOI] [PubMed] [Google Scholar]
- Laurance, J. (2003). Focus: Something in the food. The Independent on Sunday, April 6.
- Lupton D. Routledge; London and New York: 1999. Risk. [Google Scholar]
- MacFarlane Burnet, White D. 4th ed. Cambridge University Press; London: 1972. The natural history of infectious disease. [Google Scholar]
- McDonald, D., & Rogers, L. (2003). Scientists probe killer pneumonia link to animals. The Sunday Times, March 23.
- Morse S.S. Factors in the emergence of infectious diseases. Emerging Infectious Diseases. 1995;1:7–15. doi: 10.3201/eid0101.950102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park K. Kimberley Bergalis, AIDS and the plague metaphor. In: Garber M., Matlock J., Walkowitz R., editors. Media spectacles. Routledge; New York and London: 1993. pp. 232–254. [Google Scholar]
- Public Health Laboratory Service (PHLS). (2003). West Nile virus questions and answers. UK Government, from the World Wide Web: http://www.phls.co.uk/topics_az/west_nile/WNV_QA_July2003.pdf.
- Revill, J., & Aglionby, J. (2003). Mystery virus: Race to beat the bug. The Observer, April 6.
- Sacks V. Women and AIDS: An analysis of media misrepresentations. Social Science & Medicine. 1996;42:59–73. doi: 10.1016/0277-9536(95)00079-8. [DOI] [PubMed] [Google Scholar]
- Said E. Penguin Books; London: 1978. Orientalism. [Google Scholar]
- Satcher D. Emerging infections: Getting ahead of the curve. Emerging Infectious Diseases. 1995;1:1–6. doi: 10.3201/eid0101.950101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheriden, M. (2003). China covered up existence of killer pneumonia. The Sunday Times, March 30.
- Sheriden, M., & Rogers, L. (2003). It may only be a cousin of the common cold, but it has already killed 87 people and infected 2400. Will the Sars virus cause a global epidemic? The Sunday Times, April 6.
- Shilts R. Penguin Books; New York: 1987. And the band played on—politics, people and the AIDS epidemic. [Google Scholar]
- The UK Creutzfeldt-Jakob Disease Surveillance Unit. (2003). CJD statistics. University of Edinburgh from the World Wide Web: http://www.cjd.ed.ac.uk/figures.htm.
- Treichler P. AIDS: An epidemic of signification. In: Bersani L., Crimp D., editors. AIDS: Cultural analysis, cultural activism. MIT Press; Cambridge, MA: 1988. [Google Scholar]
- Ungar S. Hot crises and media reassurance. British Journal of Sociology. 1998;49:36–56. [Google Scholar]
- Wagner W., Kronberger N., Seifert F. Collective symbolic coping with new technology: Knowledge, images and public discourse. British Journal of Social Psychology. 2002;41:323–343. doi: 10.1348/014466602760344241. [DOI] [PubMed] [Google Scholar]
- World Health Organisation. (2003a). Dr. Carlo Urbani of the World Health Organization dies of SARS. World Health Organisation Media Centre from the World Wide Web: http://www.who.int/mediacentre/notes/2003/np6/en/.
- World Health Organisation. (2003b). Cumulative number of reported probable cases of SARS from 1 Nov 2002 to 11 July 2003. World Health Organisation from the World Wide Web: http://www.who.int/csr/sars/country/2003_07_11/en/.
- Zambon M., Nicholson K.G. Sudden acute respiratory syndrome. British Medical Journal. 2003;326:669. doi: 10.1136/bmj.326.7391.669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zambon M., Nicholson K.G. Sudden acute respiratory syndrome may be a rehearsal for the next influenza pandemic. British Medical Journal. 2003;326:669–670. doi: 10.1136/bmj.326.7391.669. [DOI] [PMC free article] [PubMed] [Google Scholar]