

Abstract
Cardiology in China has shown significant changes in the last decade or so. Interventional cardiology, in particular, has shown remarkable advances, especially in the management of coronary artery disease, which, unfortunately, has shown a disconcerting increase in incidence in a country traditionally known for very low incidence of coronary artery disease. Important contributing factors include increasing affluence, westernization of dietary habit and lifestyle, and rampant cigarette smoking. At present, the Chinese population has an annual coronary mortality of one sixth of that reported in the West, an incidence of acute myocardial infarction of one tenth to one eighth, and a mortality of acute myocardial infarction of one eighth. The prevalence of coronary artery disease among the general Chinese population (3–7%) is roughly one quarter of that among the Caucasians in the West, but this will get worse for sure.
China still has a lot of catching up to do to reach full modernization. There is a price that every developing country must pay for modernization. However, let the price the Chinese pay not exceed the benefits derived from modernization. Can we achieve a utopian stage in the 21st century in which the modern Chinese retain their ancestral low rates of coronary artery disease while adapting the positive aspects of a modern western lifestyle?
Keywords: Cardiology, China, West
1. Introduction
I used to return to China to lecture, demonstrate, and exchange scientific and medical information every 1–2 years since 1972. I have previously reported my observations on several occasions [1], [2], [3], [4], [5], [6], [7], [8], [9], [10]. Due to increasing demand on my time by other countries around the world in the past decade, I have not been back to China as frequently in recent years. The last time I visited China before my latest visit in October 2002 was in 1996. So much changes have taken place that I felt it important to report a few of the more significant ones in modern China.
Incidentally, severe acute respiratory syndrome (SARS), the recent epidemic that spread through populous China then spread around the world and posed as a potential threat to China's stability, is said to have originated in the southern China province of Guangdong in the Fall of 2002. Despite the accusations that the Chinese authorities have been underreporting or covering up cases of SARS, I saw no evidence of such an occurrence during my visit in October 2002, which included Hong Kong, Guangzhou, Beijing, and Shanghai. It only came to surface early in 2003 when, according to a good colleague of mine in Guangzhou who apologized for not promptly responding to my correspondences, as he always did over the many years of our acquaintance, his hospital “had been kept busy with quite a few cases of atypical pneumonia since the Spring Festival,” another term for the Chinese New Year, which fell on February 1, 2003. Most cases of atypical pneumonia reported during that period were indeed cases of SARS. As a matter of fact, the Chinese term for SARS is still atypical pneumonia  . Personally, I do not believe for a moment that China was underreporting or covering up cases of SARS. China was simply caught offguard by the sudden appearance of this mysterious disease, which, on the surface, resembled common colds or ordinary flu. Because it occurred during the usual flu season, I could empathize with China's initial “what's the big deal?” attitude. To me, the most important outcome of this whole incident of SARS is that China's press and news media have now become completely transparent—a sign of Chinese “glasnost”. Of course, SARS is all history now (Fig. 1)
.
. Personally, I do not believe for a moment that China was underreporting or covering up cases of SARS. China was simply caught offguard by the sudden appearance of this mysterious disease, which, on the surface, resembled common colds or ordinary flu. Because it occurred during the usual flu season, I could empathize with China's initial “what's the big deal?” attitude. To me, the most important outcome of this whole incident of SARS is that China's press and news media have now become completely transparent—a sign of Chinese “glasnost”. Of course, SARS is all history now (Fig. 1)
.
Fig. 1.
Chinese stamp commemorating the conquest of SARS in China: “All Hearts United Against SARS” (courtesy of G.W. Yang and Dr. T.Y. Chen, both from China).
2. Coronary artery disease
As I pointed out in my earlier publications [11], [12], [13], coronary artery disease, which used to be extremely rare in old China [14], has increased considerably in prevalence in China in the past several decades. Coronary artery disease in China has climbed from the fifth most common form of heart disease in 1948–1957, to the second most common in 1958–1968 and 1969–1979, and to the most common in 1980–1989 (Table 1) , where it remains until this date.
Table 1.
Changing patterns of heart disease in China, 1948–1989
| Etiologic types | 1948–1957 (%) | 1958–1968 (%) | 1969–1979 (%) | 1980–1989 (%) |
|---|---|---|---|---|
| (Cardiac/total admissions | 10 | 16 | 21 | 24) |
| Coronary | 6 | 16 | 26 | 27 |
| Rheumatic | 50 | 44 | 30 | 24 |
| Hypertensive | 18 | 7 | 3 | 5 |
| Syphilitic | 9 | 3 | 1 | ≤1 |
| Pulmonary | 7 | 10 | 8 | 2 |
| Congenital | 2 | 12 | 17 | 13 |
| Myocarditis | 1 | 1 | 7 | 11 |
| Cardiomyopathy | ≤1 | ≤1 | 2 | 3 |
| Pericarditis | 2 | 2 | 2 | 2 |
| Thyroid | 2 | 1 | ≤1 | 1 |
| Mitral valve prolapse | – | – | – | ≤1 |
| Others | 2 | 3 | 3 | 10 |
Modified from Chen H. et al. Chin. Med. J. 1999;112:14–17.
This changing pattern of heart disease in China was also reflected in the changing etiologies of congestive heart failure in modern China. Whereas rheumatic heart disease used to be the most common cause of congestive heart failure in the 1980s, coronary artery disease took over in the 1990s and 2000 (Table 2) . Myocardial infarction, which was extremely rare in old China, has been the fifth leading cause of death in modern China [15]. I still recall that when I was a medical student, I saw only one case of acute myocardial infarction during my entire 5 years of schooling. It was such a rarity that the patient became the subject of Medical Grand Rounds, Cardiology Grand Rounds, ECG Conference, Radiology Conference, Physiology Seminar, Pharmacology Round Table, Journal Club, and Research Conference. I felt so sorry for that poor patient who had to be present in each of these didactic conferences.
Table 2.
Changing etiologies of congestive heart failure in modern China
| 1980 (%) | 1990 (%) | 2000 (%) | |
|---|---|---|---|
| Rheumatic heart disease | 46.8 | 24.2* | 8.9** |
| Coronary heart disease | 31.1 | 40.6 | 55.7 |
| Hypertensive cardiovascular disease | 8.5 | 10.3 | 13.9*** |
| Dilated cardiomyopathy | 6.0 | 6.9 | 7.5 |
| Others | 7.6 | 18.0 | 14.0 |
p<0.0001, as compared with 1980.
p<0.0001, as compared with 1990.
p=0.04.
At present, the Chinese population has an annual coronary mortality of one sixth of that reported in the West, an incidence of acute myocardial infarction of one tenth to one eighth, and a mortality of acute myocardial infarction of one eighth [16]. The prevalence of coronary artery disease among the general Chinese population (3–7%) is roughly one quarter of that among the Caucasians in the West [16]. But this will change for the worse in the years to come.
Part of the reason for this changing pattern is, of course, relative due to more accurate diagnosis, less people dying from malnutrition and infectious diseases, and more people living to an older age. But most of the increases are really due to the following contributing factors.
2.1. Changing dietary habit
Modern Chinese love the atherogenic fast food and devour them at an ever-faster rate. The huge success of the world's two of the best known fast-food giants, McDonald's (Fig. 2) and Kentucky Fried Chicken, also known as KFC (Fig. 3) , is the result of a change of Chinese lifestyles, which are becoming more geared to speed, convenience, and choice. Although most of the Chinese do not like the taste of either hamburgers (Chinese prefer pork to beef) or cheeseburgers (Chinese compare cheese to vomitus), they possess enough curiosity to try them. Furthermore, consumers in China are buying at McDonald's and KFC because they are fashionable in the West, not because they represent their own culture. If every Chinese tries just one fast-food item only once, these McDonald's and KFCs would have rung up US$1.3 billion sales in China. There are now over 800 KFCs [17] and over 430 McDonald's [18] in China. Every kid in China knows the name and can sing the song of McDonald's, although completely unaware of the frightening fact that a Big Mac contains 34 g of fat [19]. More than one third of adults in China and over half of adults in China's urban areas consume over 30% of their energy from fat [20].
Fig. 2.

The first McDonald's restaurant in China, located in Beijing.
Fig. 3.
The first KFC restaurant in China, located in Beijing, opposite the mausoleum where Mao Zedong was buried (visible in the left background).
As a consequence of the recent change in the dietary habits in China, the normal plasma cholesterol values in modern China have shown a steady increase. In 2003, the upper limit of normal was 6.0 mmol/l or 232 mg/dl, and the mean value was 5.06 mmol/l or 196 mg/dl [21]. These “normal” values, which were very similar to those reported recently from another study of 1211 retirees in Beijing [22] and the Chinese MONICA project involving 5 million Chinese from 16 provinces [23], were considerably higher than the normal values in China published in 1958 (155 mg/dl) [24], 1981 (191 mg/dl) [24], and 1997 (200 mg/dl) [25]. In a country known traditionally for its low plasma cholesterol values, low incidence of coronary artery disease, and lean body build, this upward adjustment of the so-called “normal” values in modern China represents an alarming trend that deserves special attention. This assumes an even greater significance in view of the recent report that blood cholesterol concentration is directly related to mortality from coronary artery disease even in those with—what was, by western standards—a “low” cholesterol concentration [26].
In addition to the recent fast-food onslaught, there is also a new craze in China for milk. China is starting to consume more milk, a basic change in the national diet that reflects an upward shift in the expanding Chinese middle class. In old China, milk was considered a luxury, costing more than water or tea. With the improvement of living standards, near doubling of milk production during the last 5 years [27], and the fitness craze sweeping across the country, Chinese are drinking more milk in record numbers—25% increase from 2001 to 2002 (Q.Y. Ge, personal communication, April 2, 2003). China's annual milk production has finally caught up with that of its grain alcohol [27]. So, instead of “Gan Bei” (“bottoms up”) with the traditional Mao-tai at most of the state banquets, Chinese hosts are now holding up glasses filled with milk. Unfortunately, while the older generations of Chinese have benefited from a diet high in vegetables and fruits and low in saturated fats, a move to too much milk undoubtedly would accelerate the development of atherosclerosis in modern China. Such changes in China's dietary intake will have a great influence on the coronary artery disease burden, as was supported by the recently reported Singapore experience in which the higher consumption of dietary saturated fat is associated with a higher serum cholesterol and higher coronary artery disease mortality in Singaporean Chinese compared with the Chinese in Hong Kong and mainland China [28].
2.2. Obesity
China used to be known for her slender people. I never saw a fat person in China until recent years (Fig. 4) . Now China is fighting obesity, especially childhood obesity, which is as high as 28% [29] as the rest of the world [30]. Excessive caloric intake from fast food [31]; insufficient exercise from increasing availability of, and increased reliance on, automobiles [13]; and the popularization of television result in weight gain. The effect of television viewing on pediatric obesity has recently been documented: each hourly increment of TV viewing is associated with a 1–2% increase in the prevalence of obesity in urban China [32].
Fig. 4.
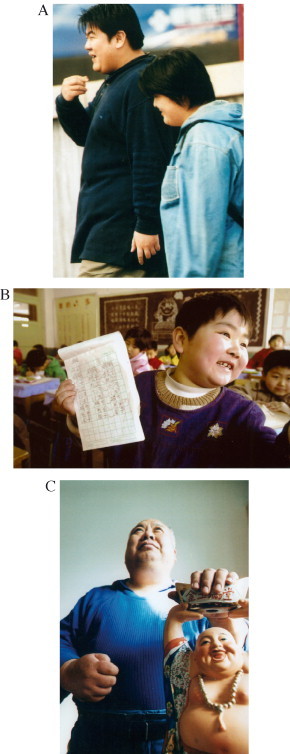
Obesity is prevalent in China among not only adults (A) but also children (B). Obese people in China are often compared to Buddha (C) and represent prosperity (courtesy of Beijing Review).
The prevalence of obesity continues its upward trend in China as the rest of the world. By the end of 2000, the obesity rate of male students in Beijing reached 15%, doubling that of 1990 and approaching that of developed countries [29]. Traditionally, a fat child in China meant a healthy child, one who was likely to survive the rigors of undernourishment and infections. This misconception still prevails today in many parts of China, which, unfortunately, is a participant in an international epidemic of childhood obesity [33], [34]. Fat children grow up to be fat adults. Overweight in China [body mass index (BMI) ≥25] has shown a progressive increase in both men and women over the past two decades (Table 3) [35]. It is estimated that overweight is present in 50–60% of northern Chinese and 20% of the total Chinese population [35]. Obesity (BMI≥30) is present in 10% of the population in northern China and 5% in southern China; the total number of obese people in China is now estimated to be 30–40 million [35].
Table 3.
Prevalence of overweight (BMI≥25) in China
Modified from Ref. [35].
p<0.05.
The Chinese have a lower baseline BMI to begin with (baseline value=21 [36]; mean=18.5–23.9 [37]), and it takes less increment to reach an obese level, so that a BMI of 24–27.9 is considered as overweight and ≥28 as obese [37]. It takes smaller increments to increase the risk of hypertension, coronary artery disease, and type II diabetes in the Chinese population [36], [38], [39]. China is in the midst of an obesity epidemic [40]. Obesity in China has reached such a serious stage that the Chinese government has started a national campaign against it [41]. Furthermore, the Chinese Medical Association just convened its first national symposium on the prevention and treatment of obesity on March 15, 2003 in Suzhou [42]. The recent report that obesity significantly raises cancer risk [43] will undoubtedly add impetus to China's war against obesity because of the Chinese's inordinate fear of cancer.
2.3. Cigarette smoking
China is the greatest producer and consumer of cigarettes in the world [44]. One of every three cigarettes manufactured in the world is consumed in China (Fig. 5) . Even more alarming is the prevalence of teenage smoking in China (Fig. 6) ; three of every five Chinese smokers begin smoking at the age of 15–20 years [45]. Although cigarette smoking is far less common among the Chinese women than men [46], women smoke almost as much as men in the Autonomous Region of Inner Mongolia. Cigarette smoking becomes the only pastime for both men and women who are housebound by the inclement weather in the winter in the Inner Mongolia grasslands (Fig. 7) . As the Chinese saying goes, “women uphold half of the sky”; therefore, women smoke as much as the men in Inner Mongolia [47].
Fig. 5.
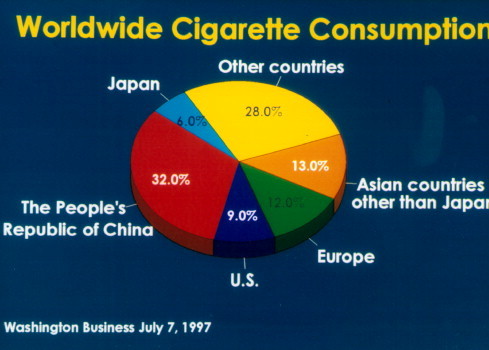
Worldwide cigarette consumption.
Fig. 6.
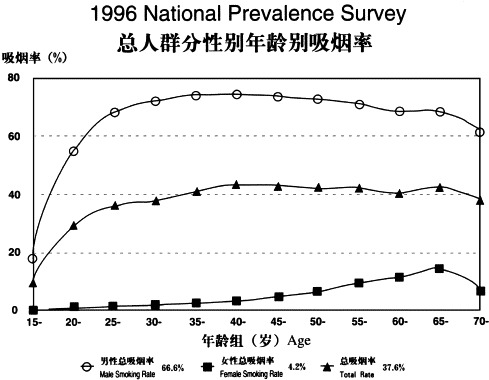
National survey in 1996 of the prevalence of smoking in China according to age, with the steepest rise in males between the ages of 15 and 20 years (courtesy of the Chinese Ministry of Health).
Fig. 7.

Woman smoker in Inner Mongolia, China.
Countries such as China, with its 300 million smokers, are being targeted by the tobacco industry as stricter control on tobacco began to bite in the United States. The young smokers in China not only like to smoke foreign brands of cigarettes but also name brands. Next to Coca Cola and Mickey Mouse, Marlboro is the third most well-known American name in China. Advertisements in the form of billboards are conspicuously shown in every major city in China (Fig. 8) . Despite health hazard warnings on the cigarette packs as required by the Ministry of Public Health and uncontroversial evidence that cigarette smoking is a major cause of death in China [48], a direct cause of coronary artery disease in China [49], and an indirect cause of coronary artery disease by causing hypertension [50] and diabetes [44], many Chinese continue to smoke, including medical professions.
Fig. 8.
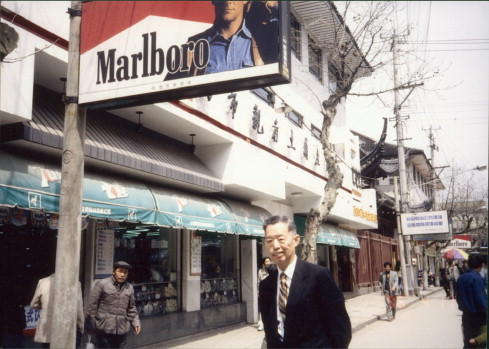
Large billboards advertising Marlboro cigarettes in China.
On each China visit, I always inquired why so many Chinese continue smoking despite the health hazards. They always pointed out to me that the late Chairman Mao Zedong smoked (Fig. 9) and the late Chairman Deng Xiaoping also smoked (Fig. 10) . Mao and Deng were China's two greatest leaders in the 20th century and are still revered throughout China. So I believe that example-setting is very important. Furthermore, despite the recent unanimous approval of the global antitobacco treaty by all 192 countries in the World Health Organization [51], of which China is a member, China is still not enforcing the ban, claiming that “individuals' rights should be respected.”
Fig. 9.

Mao Zedong smoking cigarette on an airplane.
Fig. 10.
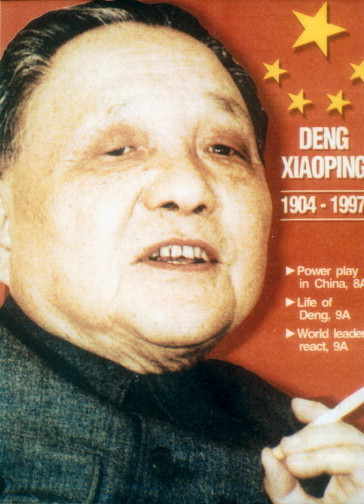
Deng Xiaoping, also an avid cigarette smoker.
3. Interventional cardiology
Since the introduction of selective cine coronary arteriography into China in 1973 [6], the field of interventional cardiology has been growing by leaps and bounds and is now an established discipline in China (Table 4) . Selective coronary arteriography is now routinely performed in every major medical center throughout China with a very respectable complication rate. As was recently reported from the Fu Wai Hospital and Cardiovascular Institute, Chinese Academy of Medical Sciences, Beijing [52], where I performed China's first selective cine coronary arteriogram in 1973 [6], in an analysis of 9196 cases from October 1987 to December 2000, death, myocardial infarction, stroke, serious arrhythmias, peripheral vascular complications, and allergic reactions to the contrast media were 0.02%, 0.01%, 0.01%, 0.29%, 0.26%, and 0.04%, respectively, as compared to 0.10%, 0.06%, 0.07%, 0.47%, 0.46%, and 0.23% in an analysis of 222,553 cases between 1984 and 1987 from the Registry of the Society for Cardiac Angiography and Interventions [53].
Table 4.
Major cardiac procedures performed in modern China
| 1973–1995 | Up to 2002 | |
|---|---|---|
| Coronary arteriography | 10,000 | 180,000a |
| PTCA | 2000 | 75,000a |
| CABG | 1000 | 20,000a |
| Heart transplantation | 7 | 150b |
| Coronary stenting | 30 | 73,300a |
| Brachytherapy | 0 | 200c |
| Percutaneous balloon mitral valvuloplasty | 5543 | 20,000c |
| Radiofrequency ablation, PSVT | 10,000a | 70,000a |
| Radiofrequency ablation, PVT | 40 | 3000c |
| Percutaneous transluminal septal myocardial ablation | 0 | 400d |
Prof. R.L. Gao, Cardiovascular Institute, Beijing Fu Wai Hospital.
Prof. Y.S. Wang, Renji Hospital, Shanghai Second Medical University.
Profs. Z.S. Wu and Z.G. Zhang, Beijing Institute for Heart, Lung, and Blood Vessel Diseases.
Drs. Z.Q. Li and W.W. Zhang, Liaoning Provincial Hospital.
Percutaneous transluminal coronary angioplasty (PTCA) was first performed in Xian, China, in 1984. Percutaneous coronary intervention (PCI) is growing rapidly in China (Fig. 11) at an annual rate of increment of around 40% [54], [55]. In 2001, 16,345 procedures were performed with a success rate of 97% [54], [55]. This, of course, is rather a small number as compared with the United States where, in 1999, 601,000 procedures were performed [56]. Similar to the trend in the western world, the Chinese cardiologists have also become more aggressive in the management of acute coronary syndromes. According to a recent report of a study, which is a part of the international multicenter registry, selective coronary arteriography was carried out in 35% of these patients, in half of whom (or 17%) PTCA was performed; thrombolytic therapy was carried out in only 3% of the patients and coronary artery bypass grafting (CABG) in 4% [57] Coronary stenting has also rapidly expanded in number; according to the Third National Coronary Intervention Registry, published at the end of 2002, over a 3-year period from 1999 to 2001, stents were implanted in 81% (43,304 of 53,695) of PCIs with a success rate of 99% [55].
Fig. 11.
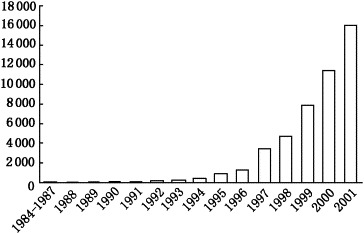
Rapid growth of PCIs in China from 1984 to 2001 (modified from Ref. [55]).
The number of PCIs has surpassed that of percutaneous balloon mitral valvuloplasty, which used to be the most frequently performed interventional cardiologic procedure in China [58], [59], [60]. This reversal in trend reflects the change in the etiologies of heart diseases in modern China over the past two decades, namely, an increase in coronary artery disease and a decline in rheumatic heart disease (Table 1).
Chinese cardiologists learn fast. Hypertrophic cardiomyopathy was an unfamiliar diagnosis in China until I introduced selective coronary arteriography in 1973 [6]; 3 of 11 patients catheterized because of exertional chest pain were found to have normal coronary arteriograms but hypertrophic obstructive cardiomyopathy with a significant systolic gradient across the left ventricular outflow tract and a typical angiographic appearance. This disease entity is encountered more and more often now in China. As a matter of fact, the interventional cardiologists in China have also become quite aggressive in treating these patients with the percutaneous technique of transluminal septal myocardial ablation with alcohol, with one center alone having performed such a procedure in 119 patients with excellent short- and long-term results [61]. According to the Chinese national registry, over 400 such procedures have been performed among 20 hospitals in China by the end of 2002. The Chinese cardiologists have also been actively engaged in laboratory investigations to determine whether it is the volume of the alcohol injected, or the rate of alcohol injection into the first septal perforator of the left anterior descending coronary artery during septal ablation that is important. It was concluded that the size of the iatrogenically induced myocardial infarct in piglets is directly related to the volume of intracoronary alcohol injection, rather than the rate of alcohol injection [62].
Frequent symposia on interventional cardiology are held regularly at both national and local levels to keep the cardiologists abreast of the latest developments in interventional cardiology. These meetings are usually supported by foreign pharmaceutical companies or/and device manufacturers, which also take care of the travel expenses of Chinese cardiologists going overseas to attend international cardiologic meetings. Unlike the United States where such practices are now forbidden, many Chinese cardiologists who otherwise would not be able to afford such international trips on their meager salaries1 are able to attend these cardiologic meetings in both Europe and North America. Upon returning to China from such meetings, they promptly report the highlights of such meetings in national or local medical journals in China. Such practices serve to educate the rest of the cardiologists in China who otherwise would not have an opportunity to keep abreast of the recent advances in cardiology due either to lack of financial means to go overseas, or to unfamiliarity with the English language.
4. Cardiovascular surgery
China's first CABG operation was performed in October 1974 at Beijing's Fu Wai Hospital where China's first selective coronary arteriogram was performed in June 1973 [6]. It was a single-vessel saphenous vein graft to the left anterior descending coronary artery in a 40-year-old male patient who survived for 8 years (Zhu Xiaodong, MD, Fu Wai Hospital, personal communication, August 1, 1997). Since then, over 20,000 CABGs have been carried out in China (Table 4) (i.e., less than 20 per million population in China as compared with 2000 per million population in the United States).
China's first heart transplantation was performed in 1978 in Shanghai's Ruijin Hospital, Shanghai Second Medical University where I am the Honorary Professor. The patient survived for 109 days. China has performed 150 heart transplantations by the end of 2002 (Table 4). One of the patients in Harbin, China, has survived for more than 10 years now following the heart transplantation.
As is the case with the rest of the world, the principal limiting factor in heart transplantation is scarcity of donors. The latter factor was further complicated in China by the traditional Buddhist teaching that a dead person must be buried with all the organs intact to ensure the spirit's happiness. There exist rumors that hearts and other organs from executed prisoners in China have been harvested as donor organs without the explicit consent of their family members. But I am unable to confirm such rumors. However, such practices provide a useful donor source in Taiwan where the condemned prisoners voluntarily initiated the process of organ donation [63].
5. Pulmonary embolism
Pulmonary embolism used to be thought of as rare in China [4]. But this is no longer the case. In a recent analysis of 37 documents of Chinese language case studies involving misdiagnoses of pulmonary embolism published from January 1980 to June 2001 and identified by searching the Chinese Biomedical Literature Database [64], 310 patients with misdiagnosed pulmonary embolism were identified. The five commonest misdiagnoses were coronary artery disease in 20%, pneumonia in 14%, primary pulmonary hypertension in 10%, cardiomyopathy in 7%, and pleurisy in 6% [64]. China is launching a campaign to increase awareness on this disease, as evidenced by several recent publications in major medical journals in China [64], [65], [66].
There are several explanations for underdiagnosing or misdiagnosing pulmonary embolism in China:
-
(1)
Traditional teaching by such authorities as Snapper (Fig. 12) , who was highly regarded in old China as one of the most astute diagnosticians, was that pulmonary embolism was rare in China. He did not even mention it in his book “Chinese Lessons to Western Medicine” [14].
-
(2)
Even as recent as 1970s, pulmonary embolism was thought to be rare in China [4] The rarity of pulmonary embolism was even more remarkable when one considered the widespread use of birth control pills among the Chinese women of child-bearing age [4]. Perhaps the use of acupuncture anesthesia [2], [7], [8], [9], which permitted early ambulation after major surgery, accounted for the low incidence of postoperative pulmonary embolism in China. Because acupuncture anesthesia is seldom employed in modern China, this protective factor is no longer operative.
-
(3)
More accurate in vivo diagnosis of pulmonary embolism is now possible because of improved diagnostic techniques.
Fig. 12.
Dr. I. Snapper, a highly regarded diagnostician from Holland, who served as chairman of the Department of Medicine of the Peking Union Medical College in the 1940s.
6. Publishing in cardiology
The publishing industry in China has shown an extraordinary growth in recent years. In 1978, China published 14,987 books; 20 years later, the number was 130,613—a little more than twice that of the United States [67]. Similarly, exponential growth took place for magazines (from 930 to 7999) and newspapers (from 186 to 1035) over the same period [67]. By comparison, the United States published 14,707 magazines in 1999 and 1489 newspapers in 1998 [67].
This publishing explosion was mirrored in medical publishing as well. Not only the quantity but also the quality of medical books showed a great deal of improvement within a relatively short period of time. Some textbooks in cardiology that were originally published as a single volume (Fig. 13A) had to be published in a two-volume set because of increased pages required to cover all the latest advances (Fig. 13B). Other books, such as the one on congestive heart failure, which originally appeared as monographs (Fig. 14A) , later were expanded to become textbooks (Fig. 14B). The Chinese medical doctors are thirsty for new knowledge; because attendance at national and international medical meetings was restricted by financial constraints, they have to rely mostly on books and journals for their postgraduate medical education.
Fig. 13.
(A) The first edition of The Textbook of Modern Cardiology was published as a single volume in 1994. (B) The second edition of The Textbook of Modern Cardiology was published as a two-volume set in 2002, being compared in size to Braunwald's Heart Disease, 6th edition.
Fig. 14.

(A) A monograph on Congestive Heart Failure, first published in 1990. (B) Congestive Heart Failure as a textbook published in 2003, being compared in size to Braunwald's Heart Disease.
China published some 700 medical journals in 1994 [68], 1085 in 1999 (Q. Wang, Shanghai Medical University, personal communication, May 9, 2003), and over 1200 in 2002 (Q. Wang, Shanghai Medical University, personal communication, May 9, 2003). Publishers include the Chinese Medical Association, which is a nongovernmental organization with many specialty societies, the Chinese Academy of Medical Sciences, the Chinese Academy of Traditional Chinese Medicine, various publishing houses, hospitals, and academic institutions. The major publisher of Chinese medical journals is the Chinese Medical Association, which published 46 journals in 1990, 56 journals in 1994, and 69 journals in 2003 (L.F. Cai, Chinese Medical Association, personal communication, May 2003).
Several monthly medical journals began to be published twice a month just as in the United States (e.g., the National Medical Journal of China). There were only seven specialty journals in cardiology in 1978, but in 1998, there were 25—a threefold increase in just two decades (Z.L. Xu, Institute of Medical Information, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, personal communication, May 13, 2003). Beginning in 2003, the Chinese Journal of Cardiology, which celebrated its 30th anniversary of publication in February 2003, increased its monthly pages from 64 to 80; beginning in 2004, it will be published twice a month (Y.M. Jiang, Chinese Journal of Cardiology, personal communication, May 14, 2003), just like Circulation and the Journal of the American College of Cardiology in the United States. Many print journals also appear online; there are currently 68 journals published by the Chinese Medical Association, most of which are also available on CD-ROM starting with 1996. Chinese editions of the Journal of American Medical Association and British Medical Journal have been in publication since February 1982 and May 1998, respectively.
It may be of interest to note how frequently different foreign medical journals are being cited as references in articles that appeared in the Chinese Journal of Cardiology. A perusal of the list published recently in the Chinese Journal of Cardiology showed that, in 2000–2001, Circulation was on top of the list, followed by the Journal of the American College of Cardiology, American Journal of Cardiology, New England Journal of Medicine, Lancet, etc. (Table 5) [69]. The top five journals represented nearly one third of the citations. This list is somewhat reminiscent of the omnipotent Science Citation Index impact factors of these journals. According to the Chinese Scientific and Technological Journal Citation Reports 2001, which was published in 2002, impact factor and total citation frequency for the Chinese Journal of Cardiology ranked 9th and 21st, respectively, among 2000 Chinese scientific and technological journals (Y.M. Jiang, Chinese Journal of Cardiology, personal communication, June 17, 2003).
Table 5.
Foreign cardiologic journals cited in the Chinese Journal of Cardiology, 2000–2001
| (1) Circulation | 396 |
| (2) Journal of the American College of Cardiology | 183 |
| (3) American Journal of Cardiology | 163 |
| (4) New England Journal of Medicine | 95 |
| (5) Lancet | 89 |
| (6) American Heart Journal | 74 |
| (7) Circulation Research | 60 |
| (8) Hypertension | 55 |
| (9) European Heart Journal | 44 |
| (10) Journal of the American Medical Association | 43 |
| (11) Journal of Clinical Investigation | 42 |
| (12) Arteriosclerosis, Thrombosis, and Vascular Biology | 40 |
| (13) Journal of Hypertension | 38 |
| (14) Pacing and Clinical Electrophysiology | 35 |
| (15) Annals of Thoracic Surgery | 34 |
| (16) Cardiovascular Research | 33 |
| (17) Journal of Biological Chemistry | 32 |
| (18) Journal of Thoracic and Cardiovascular Surgery | 31 |
| (19) Atherosclerosis | 29 |
| (20) Heart (British Heart Journal) | 27 |
| (21) American Journal of Physiology | 27 |
| (22) Journal of Molecular and Cellular Cardiology | 26 |
| (23) Journal of Cardiovascular Electrophysiology | 23 |
| (24) Thrombosis and Haemostasis | 21 |
| (25) Nature | 20 |
| (26) Proceedings of the National Academy of Sciences | 20 |
| (27) Chest | 19 |
| (28) Diabetes | 19 |
| (29) International Journal of Cardiology | 18 |
Adapted from Ref. [69].
A word about international access to the Chinese medical literature through MEDLINE: Users doing author searches may have difficulties with common Chinese surnames, especially if only one given name initial is used [70]. The difficulty may be further compounded by the fact that Chinese authors customarily spell their last names first and first names last [71], [72], [73], [74], [75], [76].
7. Research in cardiology
China, in both basic research and clinical investigation in cardiology, has made significant improvements and advances over the years in the following several broad areas.
7.1. Participation in NIH Visiting Program
According to Lenfant [Director, National Heart, Lung, and Blood Institute, National Institutes of Health (NIH), personal communication, May 7, 2003], during the brief period of a little more than a decade from FY 1989 to FY 2002, the number of Chinese participants in the NIH Visiting Program increased by more than 270% from 142 to 531. For FY 2002, China led the list (531), followed by Japan (518), Korea (339), India (243), and other countries, whereas Japan (342) led the list for FY 1989, followed by Italy (144), China (142), and United States (98, permanent residents). China was also on top of the list for FY 2001 with 509 participants, followed by Japan (498), Korea (298), India (217), and other countries. The growth in the number of participants from China reflects an increased interest in biomedical collaboration between US and Chinese scientists.
7.2. Presentation at the American Heart Association annual meetings
Over a 10-year period from 1992 to 2002, the number of abstracts submitted from China increased from 34 to 85, and the number accepted for presentation showed a parallel increase from three to eight (Table 6) . A similar trend was noticed for the American College of Cardiology Annual Scientific Meetings. Such increases in contributions of our Chinese colleagues to these national heart meetings are quite impressive.
Table 6.
American Heart Association scientific sessions abstracts submitted and accepted from China, 1992–2002
| 1992 | 1993 | 1994 | 1995 | 1996 | 1997 | 1998 | 1999 | 2000 | 2001 | 2002 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Submitted | 34 | 23 | 14 | 37 | 10 | 25 | 14 | 60 | 56 | 67 | 85 |
| Accepted | 3 | 1 | 2 | 1 | 1 | 3 | 3 | 2 | 6 | 8 | 8 |
Courtesy of American Heart Association, May 20, 2003.
7.3. Clinical trials
China is a huge country with its 1.3 billion population; one of every five persons on Earth lives in China. China's unique environment, therefore, constitutes a tremendous opportunity for intervention trials. Ethnic, demographic, and cultural diversities make it easier to conduct major epidemiologic studies in China. Because the Chinese population is more compliant than the western population, high participation rates are certain. Because the Chinese population is more stable than the western population, follow-up is easier and more complete. Finally, the studies are much cheaper to carry out, “practically nothing compared to what a similar trial will cost in the United States,” as noted by fraumeni of NIH according to Mervis [77].
Besides participating in many international trials, China also conducts several national trials on her own [e.g., Tissue plasminogen activator/Urokinase Comparisons in China (TUCC)] [78]. Some of these trials carry rather cute acronyms [e.g., CAST (Chinese Active Stroke Trial), CAT (Chinese Angiotensin-converting enzyme inhibitor in acute myocardial infarction Trial), CATHAY (Chinese ATHerosclerosis study in the Aged and Young), and STONE (Shanghai Trial Of Nifedipine in the Elderly)], similar to the fascination with the creation of attractive trial acronyms by the western investigators [79], [80], [81], [82], [83].
7.4. Statistical methods in medical journals published in China
The use of statistical methods in Chinese medical journals has been improving [84]. According to Wang and Zhang [84], the percentages of original articles reporting clinical trials, prospective studies, or basic science research increased from 18% in 1985 to 31% in 1995 (p<0.001), of articles using statistical methods increased from 40% in 1985 to 60% in 1995 (p<0.001), and of those articles using appropriate statistical methods increased from 22% to 46% (p<0.001).
In both 1985 and 1995, the most commonly used statistical methods in the Chinese medical journals were t tests and contingency tables [84]. According to Wang and Zhang [84], the most common errors the Chinese authors committed were presentations of p values without specifying the test used, use of multiple t tests instead of analysis of variance, and use of unpaired t tests when paired tests were required.
7.5. Genetic research and genomics
Medical genetic research in China started in the late 1950s [85]. Molecular genetic research started in China in the 1990s [85]. As the Human Genome Project was initiated in the 1990s, China also launched a national Human Genome Project as part of its contribution to international efforts to sequence the human genome [86].
China's contribution in the Human Genome Project could be significant. According to one official from the National Science Foundation of China, “the Chinese account for over one fifth of the world's population, and the country has 56 ethnic groups. As a result, no databank of human genetic information can be said to be complete without a detailed study of the Chinese human genome” [86]. The project will have important practical implications, as the Chinese, with their powerful sequencing capacity and capability in the genome project, are expected to contribute vital information that may lead to the early diagnosis and treatment of more than 5000 hereditary diseases [86].
In 1998, China's scientific leaders overcame skepticism from some members of the Human Genome Project to become the only developing country to take a role in sequencing the human genome by contributing 1% of the published sequence—an achievement that is of huge symbolic importance [87]. Chinese researchers are now setting up programs in everything from stem cell research, through large-scale efforts to determine protein structures, to population studies to hunt for human disease genes [87]. There is even talk of trying to clone the endangered giant panda [87].
Recently, China presented her new edition of a genetic map illustrating the no. 3 human chromosome, as part of the Human Genome Project [88]. The new completed map—considered 99.99% accurate—would help improve medical diagnosis and also aid the discovery of new drugs and new treatments [88].
In the field of cardiology, China has made much progress in research work for gene therapy of hypertension [89], myocardial infarction [90], and congestive heart failure [91]. On the long list of organs that should be sequenced, the Beijing Genomics Institute has already started investigations into proteomics and drug discovery, including a project to isolate the active compounds in the herbs used in traditional Chinese medicine [92]. There are many Chinese herbs that are widely used in this country, especially for treatment of coronary artery disease and congestive heart failure. Unfortunately, they tend to interact unfavorably with commonly prescribed western cardiac drugs, including warfarin [93], [94], [95], [96], [97], [98], digoxin [98], [99], [100], [101], and hypoglycemic agents [102]. Therefore, the isolation of the active compounds in these herbs will facilitate the understanding of the pharmacodynamics of these herbs and thus avoid their inadvertent adverse interactions with the western medications.
8. Conclusion
Cardiology in China has shown significant changes in the last decade or so. Interventional cardiology, in particular, has shown remarkable advances, especially in managing coronary artery disease, which, unfortunately, has shown a disconcerting increase in incidence in a country traditionally known for its very low incidence of coronary artery disease. Important contributing factors include increasing affluence, westernization of dietary habit and lifestyle, and rampant cigarette smoking .
Footnotes
Despite frequent gifts from their grateful patients, which may range from a chicken from a farmer to a Mercedes Benz automobile from a well-to-do businessman.
References
- 1.Cheng T.O. Changes in China. N Engl. J. Med. 1972;287:259. doi: 10.1056/NEJM197208032870527. [DOI] [PubMed] [Google Scholar]
- 2.Cheng T.O. Acupuncture anesthesia. Science. 1973;179:521. doi: 10.1126/science.179.4073.521. [DOI] [PubMed] [Google Scholar]
- 3.Cheng T.O. A view of modern Chinese medicine. Observations by a Shanghai-born physician during his recent visit after 22 years of absence. Ann. Intern. Med. 1973;78:285–290. doi: 10.7326/0003-4819-78-2-285. [DOI] [PubMed] [Google Scholar]
- 4.Cheng T.O. Medicine in modern China. J. Am. Geriatr. Soc. 1973;21:289–313. doi: 10.1111/j.1532-5415.1973.tb01227.x. [DOI] [PubMed] [Google Scholar]
- 5.Cheng T.O. Cardiovascular diseases. In: Quinn J., editor. China medicine as we saw it. The Fogarty International Center; Bethesda: 1974. pp. 261–288. [Google Scholar]
- 6.Cheng T.O., Paul D. White lecture—Cardiology in People's Republic of China. In: Russek H.I., editor. New horizons in cardiovascular practice. University Park Press; Baltimore: 1975. pp. 1–27. [Google Scholar]
- 7.Cheng T.O. Acupuncture anesthesia for open heart surgery. Am. J. Cardiol. 1975;36:411. doi: 10.1016/0002-9149(75)90502-0. [DOI] [PubMed] [Google Scholar]
- 8.Cheng T.O. Cardiology in People's Republic of China in 1977. Chest. 1978;74:209–211. doi: 10.1378/chest.74.2.209. [DOI] [PubMed] [Google Scholar]
- 9.Cheng T.O. Cardiology in China revisited. Am. J. Cardiol. 1978;42:700–702. [Google Scholar]
- 10.Cheng T.O. Barefoot doctors. Postgrad. Med. 1981;70(5):41. [Google Scholar]
- 11.Cheng T.O. Cardiovascular disease in China. Nat. Med. 1998;4:1209–1210. doi: 10.1038/3169. [DOI] [PubMed] [Google Scholar]
- 12.Cheng T.O. Coronary heart disease in China. Hosp. Med. 1999;60:456. [PubMed] [Google Scholar]
- 13.Cheng T.O. Price of modernization of China. Circulation. 2001;103:e132. doi: 10.1161/01.cir.103.25.e131. [DOI] [PubMed] [Google Scholar]
- 14.Snapper I. Chinese lessons to western medicine. Interscience; New York: 1941. p. 160. [Google Scholar]
- 15.Phillips M.R., Li X., Zhang Y. Suicide rates in China 1995–99. Lancet. 2002;359:835–840. doi: 10.1016/S0140-6736(02)07954-0. [DOI] [PubMed] [Google Scholar]
- 16.Sung J.J.Y., Wong L.K.S., Li P.K.T., Sanderson J., Kwok T.C.Y. Principles and practice of clinical medicine in Asia. Treating the Asian patient. Lippincott, Williams and Wilkins; Philadelphia: 2002. p. 35. [Google Scholar]
- 17.McGregor R. China swallows fast food at an ever more rapid rate. Financial Times. 2003:12. [January 20] [Google Scholar]
- 18.Winslow R. Risk of having heart disease soars in China. Wall Str. J. 2002:B1. [April 25] [Google Scholar]
- 19.Leung S. Experts differ on healthiness of ‘fast’ salad. Wall Str. J. 2003:B1. [May 8] [Google Scholar]
- 20.Du S., Lu B., Zhai F., Popkin B.M. A new stage of the nutrition transition in China. Public Health Nutr. 2002;5(1A):169–174. doi: 10.1079/PHN2001290. [DOI] [PubMed] [Google Scholar]
- 21.Wang X., Fan Z., Huang J., Su S., Yu Q., Zhao J. Extensive association analysis between polymorphisms of PON gene cluster with coronary heart disease in Chinese Han population. Arterioscler. Thromb. Vasc. Biol. 2003;23:328–334. doi: 10.1161/01.atv.0000051702.38086.c1. [DOI] [PubMed] [Google Scholar]
- 22.Li J., Chen M., Wang S., Deng J., Zeng P., Hou L. A long-term follow-up study of serum lipids and coronary heart disease in the elderly. Chin. J. Cardiol. 2002;30:647–650. [PubMed] [Google Scholar]
- 23.Zhao D. Epidemiologic study of blood lipids in the Chinese population. Chin. J. Cardiol. 2003;31:74–78. [Google Scholar]
- 24.Cheng T.O. The international textbook of cardiology. Pergamon; New York: 1987. p. 12. [Google Scholar]
- 25.Chen G.W., Cheng T.O. The textbook of modern cardiology. 2nd ed. Hunan Science and Technology Press; China: 2002. p. 1546. [Google Scholar]
- 26.Chen Z., Peto R., Collins R., MacMahon S., Lu J., Li W. Serum cholesterol concentration and coronary heart disease in population with low cholesterol concentrations. BMJ. 1991;303:276–282. doi: 10.1136/bmj.303.6797.276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chen K. New craze seizes China's consumers: a glass of milk. Wall Str. J. 2003:A1. [February 28] [Google Scholar]
- 28.Dwyer T., Emmanuel S.C., Janus E.D., Wu Z., Hynes K.L., Zhang C. The emergence of coronary heart disease in populations of Chinese descent. Atherosclerosis. 2003;67:303–310. doi: 10.1016/s0021-9150(03)00008-x. [DOI] [PubMed] [Google Scholar]
- 29.Luo Z. Obesity: a warning to Chinese children. Beijing Rev. 2002;45(26):14–16. [Google Scholar]
- 30.Popkin B.M., Doak C.M. The obesity epidemic is a worldwide phenomenon. Nutr. Rev. 1998;56:106–114. doi: 10.1111/j.1753-4887.1998.tb01722.x. [DOI] [PubMed] [Google Scholar]
- 31.Cheng T.O. Fast food and obesity in China. J. Am. Coll. Cardiol. 2003;42:773. doi: 10.1016/s0735-1097(03)00792-7. [DOI] [PubMed] [Google Scholar]
- 32.Ma G.S., Li Y.P., Hu X.Q., Ma W.J., Wu J. Effect of television viewing on pediatric obesity. Biomed. Environ. Sci. 2002;15:291–297. [PubMed] [Google Scholar]
- 33.Torpy J.M., Lynm C., Glass R.M. JAMA patient page. Obesity. JAMA. 2003;289:1880. doi: 10.1001/jama.289.14.1880. [DOI] [PubMed] [Google Scholar]
- 34.Yanovski J.A., Yanovski S.Z. Treatment of pediatric and adolescent obesity. JAMA. 2003;289:1851–1853. doi: 10.1001/jama.289.14.1851. [DOI] [PubMed] [Google Scholar]
- 35.Shi H., Zhu Z. Program of National Congress on Prevention and Treatment of Obesity, Suzhou, China. 2003. Advances in research on hypertension and obesity; pp. 36–41. [Google Scholar]
- 36.Li G., Chen X., Jang Y., Wang J., Xing X., Yang W. Obesity, coronary heart disease risk factors and diabetes in Chinese: an approach to the criteria of obesity in the Chinese population. Obes. Rev. 2002;3:167–172. doi: 10.1046/j.1467-789x.2002.00067.x. [DOI] [PubMed] [Google Scholar]
- 37.Chinese Medical Association Subsection of Cardiovascular Disease, Chinese Journal of Cardiology Editorial Board Highlights of the Second National Conference on Dyslipidemia. Chin. J. Cardiol. 2002;30:643–646. [Google Scholar]
- 38.Jia W.P., Xiang K.S., Chen L., Lu J.X., Wu Y.M. Epidemiological study on obesity and its comorbidities in urban Chinese older than 20 years of age in Shanghai, China. Obes. Rev. 2002;3:157–165. doi: 10.1046/j.1467-789x.2002.00071.x. [DOI] [PubMed] [Google Scholar]
- 39.Zhou B., Wu Y., Yang J., Li Y., Zhang H., Zhao L. Overweight is an independent risk factor for cardiovascular disease in Chinese populations. Obes. Rev. 2002;3:147–156. doi: 10.1046/j.1467-789x.2002.00068.x. [DOI] [PubMed] [Google Scholar]
- 40.Cheng T.O. An obesity epidemic in modern China. Am. J. Cardiol. 2001;88:721–722. doi: 10.1016/s0002-9149(01)01867-7. [DOI] [PubMed] [Google Scholar]
- 41.Zhai F., Fu D., Du S., Ge K., Chen C., Popkin B.M. What is China doing in policy-making to push back the negative aspects of the nutrition transition? Public Health Nutr. 2002;5(1A):269–273. doi: 10.1079/phn2001303. [DOI] [PubMed] [Google Scholar]
- 42.National Conference on Prevention and Treatment of Obesity to be held in Suzhou. Nat. Med. J. China. 2002;82:1631. [Google Scholar]
- 43.Calle E.E., Rodriguez C., Walker-Thurmond K., Thun M.J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of US adults. N. Engl. J. Med. 2003;348:1625–1638. doi: 10.1056/NEJMoa021423. [DOI] [PubMed] [Google Scholar]
- 44.Cheng T.O. Smoking and diabetes in Chinese men. Postgrad. Med. J. 2001;77:551. doi: 10.1136/pmj.77.910.551a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Cheng T.O. Teenage smoking in China. J. Adolesc. 1999;22:607–620. doi: 10.1006/jado.1999.0256. [DOI] [PubMed] [Google Scholar]
- 46.Cheng T.O. Smoking and health. Can. Med. Assoc. J. 1991;144:630–631. [Google Scholar]
- 47.Cheng T.O. Do photographs lie? Smoking in China. Gerontologist. 1992;32:274. doi: 10.1093/geront/32.2.274a. [DOI] [PubMed] [Google Scholar]
- 48.Lam T.H., He Y., Li L.S., He S.F., Liang B.Q. Mortality attributable to cigarette smoking in China. JAMA. 1997;278:1505–1508. [PubMed] [Google Scholar]
- 49.He Y., Lam T.H. A review on studies of smoking and coronary heart disease in China and Hong Kong. Chin. Med. J. 1999;112:3–8. [PubMed] [Google Scholar]
- 50.Luo L., Luan R.S., Yuan P. Meta-analysis of risk factors on hypertension in China. Chin. J. Epidemiol. 2003;24:50–53. [PubMed] [Google Scholar]
- 51.WHA approves historic tobacco accord. Lancet. 2003;361:1793. doi: 10.1016/S0140-6736(03)13448-4. [DOI] [PubMed] [Google Scholar]
- 52.Yu M., Gao R., Chen J., Yang Y., Qin X., Qiao S. Complications in selective coronary arteriography: analysis of 9196 cases. Nat. Med. J. China. 2003;83:91–95. [PubMed] [Google Scholar]
- 53.Johnson L.W., Lozner E.C., Johnson S., Krone R., Pichard A.D., Vetrovec G.W. Coronary arteriography 1984–1987: a report of the Registry of the Society for Cardiac Angiography and Interventions: I. Results and complications. Catheter. Cardiovasc. Diagn. 1989;17:5–10. doi: 10.1002/ccd.1810170103. [DOI] [PubMed] [Google Scholar]
- 54.Gao R. Furthering the healthy development of percutaneous coronary interventions in China. Chin. J. Cardiol. 2002;30:705–706. [Google Scholar]
- 55.Section of Interventional Cardiology, Chinese Society of Cardiology, Editorial Office of Chinese Journal of Cardiology: A data analysis of the Third National Coronary Intervention Registry Chin. J. Cardiol. 2002;30:719–723. [Google Scholar]
- 56.Fleisher L.A., Barash P.G. Treatment of coronary artery disease in the year 2003. J. Cardiothorac. Vasc. Anesth. 2003;17:258–259. doi: 10.1053/jcan.2003.99. [DOI] [PubMed] [Google Scholar]
- 57.Tan H.Q., Liang Y., Zhu J., Liu L.S. Clinical characteristics of acute ischemic syndrome in China. Chin. Med. J. 2002;115:1123–1126. [PubMed] [Google Scholar]
- 58.Chen C., Cheng T.O., for the Multicenter Study Group Percutaneous balloon mitral valvuloplasty using Inoue technique: a multicenter study of 4832 patients in China. Am. Heart J. 1995;129:1197–1204. doi: 10.1016/0002-8703(95)90404-2. [DOI] [PubMed] [Google Scholar]
- 59.Cheng T.O., Holmes D.R., Jr. Percutaneous balloon mitral valvuloplasty by the Inoue balloon technique: the procedure of choice for treatment of mitral stenosis. Am. J. Cardiol. 1998;81:624–628. doi: 10.1016/s0002-9149(97)00978-8. [DOI] [PubMed] [Google Scholar]
- 60.Cheng T.O., Chen C.R. Late results of percutaneous balloon mitral valvuloplasty: the Chinese experience. Circulation. 2000;102:e18. doi: 10.1161/01.cir.102.2.e18. [DOI] [PubMed] [Google Scholar]
- 61.Li Z.Q., Cheng T.O., Zhang W.W., Qiao S.B., Zhao L.Y., Jin Y.Z., Guan R.M., Li L. Percutaneous transluminal septal myocardial ablation for hypertrophic obstructive cardiomyopathy. The Chinese experience in 119 patients from a single center. Int. J. Cardiol. 2004;93:197–202. doi: 10.1016/j.ijcard.2003.03.005. [DOI] [PubMed] [Google Scholar]
- 62.Li Z.Q., Cheng T.O., Liu L., Jin Y.Z., Zhang M., Guan R.M. Experimental study of relationship between intracoronary alcohol injection and the size of resultant myocardial infarct. Int. J. Cardiol. 2003;91:93–96. doi: 10.1016/s0167-5273(02)00592-2. [DOI] [PubMed] [Google Scholar]
- 63.Hsieh H., Yu T.J., Yang W.C., Chu S.S., Lai M.K. The gift of life from prisoners sentenced to death: preliminary report. Transplant. Proc. 1992;24:1335–1336. [PubMed] [Google Scholar]
- 64.Jia W., Li F., Cui T., Wang H. An investigation on the misdiagnosis of pulmonary embolism in China. Chin. J. Cardiol. 2002;30:406–409. [Google Scholar]
- 65.Zhai Z., Wang C. Nomenclature and definition of pulmonary thromboembolism. Nat. Med. J. China. 2002;82:1574–1575. [Google Scholar]
- 66.Guidelines to the diagnosis and treatment of pulmonary thromboembolism. Chin. Tuberculosis Respir. J. 2001;24:259–264. [Google Scholar]
- 67.Holden J.L. The role of the media in a market economy (report by R.L. Keatley). China Policy Series No. 19. National Committee on United States–China Relations; New York, NY: 2003. Preface. [February] [Google Scholar]
- 68.Smith R. Chinese medical journals; getting in touch. Chinese editors and medical journals have much to offer. BMJ. 1994;309:74. doi: 10.1136/bmj.309.6947.74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Zhang H., Wang F., Li C. A preliminary study of reference citations of foreign journals in articles published in the Chinese Journal of Cardiology. Chin. J. Cardiol. 2002;30:615. [Google Scholar]
- 70.Moriearty P.L., Chen S.B. International access to the Chinese medical literature through MEDLINE. Chin. Med. J. 1993;106:243–249. [PubMed] [Google Scholar]
- 71.Cheng T.O. The Chinese last name. J. Thorac. Cardiovasc. Surg. 1988;96:832. [Google Scholar]
- 72.Cheng T.O. What's in a name—the Chinese name? Angiology. 1989;40:324. [Google Scholar]
- 73.Cheng T.O. Word order: oriental or occidental? Texas Heart Inst. J. 1989;16:121. [PMC free article] [PubMed] [Google Scholar]
- 74.Cheng T.O. Chinese name. Prehosp. Disaster Med. 1993;8:268–269. [Google Scholar]
- 75.Cheng T.O. Use of surnames to identify individuals of Chinese ancestry. Am. J. Epidemiol. 1994;140:76. doi: 10.1093/oxfordjournals.aje.a116910. [DOI] [PubMed] [Google Scholar]
- 76.Cheng T.O. Chinese last name comes first. Int J. Cardiol. 1995;49:94. doi: 10.1016/0167-5273(95)02280-a. [DOI] [PubMed] [Google Scholar]
- 77.Mervis J. China's unique environment favors large intervention trials. Science. 1995;270:1149–1151. doi: 10.1126/science.270.5239.1149. [DOI] [PubMed] [Google Scholar]
- 78.Ross A.M., Gao R., Coyne K.S., Chen J., Yao K., Yang Y. A randomized trial confirming the efficacy of reduced dose recombinant tissue plasminogen activator in a Chinese myocardial infarction population and demonstrating superiority to usual dose urokinase: the TUCC trial. Am. Heart J. 2001;142:244–247. doi: 10.1067/mhj.2001.116963. [DOI] [PubMed] [Google Scholar]
- 79.Cheng T.O. Acronyms of clinical trials in cardiology—1994. Am. J. Cardiol. 1994;74:79–94. doi: 10.1016/0002-9149(94)90500-2. [DOI] [PubMed] [Google Scholar]
- 80.Cheng T.O. Acronymophilia: the exponential growth of the use of acronyms should be resisted. BMJ. 1994;309:683–684. doi: 10.1136/bmj.309.6956.683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Cheng T.O. Acronymania, acronymophilia and acronymophobia. Br. J. Cardiol. 1998;5:624–625. [Google Scholar]
- 82.Cheng T.O. Acronyms of clinical trials in cardiology—1998. Am. Heart J. 1999;137:726–765. doi: 10.1016/s0002-8703(99)70230-9. [DOI] [PubMed] [Google Scholar]
- 83.Cheng T.O., Julian D. Acronyms of cardiologic trials—2002. Int. J. Cardiol. 2003;91:261–351. doi: 10.1016/s0167-5273(03)00158-x. [DOI] [PubMed] [Google Scholar]
- 84.Wang Q., Zhang B. Research design and statistical methods in Chinese medical journals. JAMA. 1998;280:283–285. doi: 10.1001/jama.280.3.283. [DOI] [PubMed] [Google Scholar]
- 85.Xia J., Tang D., Xia K., Tan S. The achievements of medical genetic research in China during the past 50 years. Chin. Med. J. 1999;112:956–958. [PubMed] [Google Scholar]
- 86.Li Y.Q. China launches genome project. Nature. 1993;365:200. doi: 10.1038/365200a0. [DOI] [PubMed] [Google Scholar]
- 87.Cyranoski D. A great leap forward. Nature. 2001;410:10–12. doi: 10.1038/35065246. [DOI] [PubMed] [Google Scholar]
- 88.Genetic map. Beijing Rev. 2001;44(32):4. [Google Scholar]
- 89.Chen G.W., Cheng T.O. The textbook of modern cardiology. 2nd ed. Hunan Science and Technology Press; China: 2002. pp. 1527–1530. [Google Scholar]
- 90.Peng S., Peng J., Gong W. Relationship between apolipoprotein E gene polymorphism and myocardial infarction or its action on clinical courses. Int. J. Cardiovasc. Med. 2003;5:26–28. [Google Scholar]
- 91.Zhang Z., Cheng T.O., Zhang Y. A textbook on congestive heart failure. Beijing, China: Science and Technology Publishers, 2003, pp. 3–48, 572–585, 972–973.
- 92.Normile D. From standing start to sequencing superpower. Science. 2002;296:36–39. doi: 10.1126/science.296.5565.36. [DOI] [PubMed] [Google Scholar]
- 93.Cheng T.O. Warfarin danshen interaction. Ann. Thorac. Surg. 1999;67:894. [PubMed] [Google Scholar]
- 94.Cheng T.O. Warning about a medicinal herb. Hosp. Pract. 1999;34(10):23. [PubMed] [Google Scholar]
- 95.Cheng T.O. Herbal remedies. Am. Fam. Phys. 1999;60:1661. [PubMed] [Google Scholar]
- 96.Cheng T.O. Interaction of herbal medicine with coumadin. J. Emerg. Med. 2000;18:122. doi: 10.1016/s0736-4679(99)00170-5. [DOI] [PubMed] [Google Scholar]
- 97.Cheng T.O. Ginseng–warfarin interaction. Am. Coll. Cardiol. Curr. J. Rev. 2000;9(1):84. [Google Scholar]
- 98.Cheng T.O. Comment: drug–herb interaction. Ann. Pharmacother. 2001;35:124. doi: 10.1177/106002800103500101. [DOI] [PubMed] [Google Scholar]
- 99.Cheng T.O. Herbal interactions with cardiac drugs. Arch. Intern. Med. 2000;160:870–871. doi: 10.1001/archinte.160.6.870. [DOI] [PubMed] [Google Scholar]
- 100.Cheng T.O. St. John's Wort interaction with digoxin. Arch. Intern. Med. 2000;160:2548. doi: 10.1001/archinte.160.16.2548. [DOI] [PubMed] [Google Scholar]
- 101.Cheng T.O. Interaction of herbal drugs with digoxin. J. Am. Coll. Cardiol. 2002;40:838–839. doi: 10.1016/s0735-1097(02)02022-3. [DOI] [PubMed] [Google Scholar]
- 102.Cheng T.O. Panax (Ginseng) is not a panacea. Arch. Intern. Med. 2000;160:3329. doi: 10.1001/archinte.160.21.3329. [DOI] [PubMed] [Google Scholar]