

Abstract
Objectives:
The current study explored whether social support (SS) from family and peers, influences the relationship between depressed mood (DM) and substance use (SU). We hypothesized that SS would have a protective effect on DM, and moderate the association between DM and SU.
Participants and Methods:
Analyses focused on 703 individuals from the Carolina African American Twin Study on Aging (mean age =49.78 years, STD=14.52; 51% female). Participants reported on past year frequency of cigarettes and alcohol consumption, depressed mood, and stressful life events. Social support (SS) was assessed on two domains (i.e., emotional and instrumental), as well as for perceived quality and quantity of each type. Hypotheses were tested using ordinal logistic regression in Mplus while controlling for socioeconomic status, age, and gender.
Results:
Quality of emotional support was negatively associated with drinking. Smoking, but not drinking was associated with depressed mood. While individuals with high levels of depressed mood received more support, receiving better quality emotional support was associated with fewer mood and stress symptoms. Individuals who reported receiving better quality emotional support typically smoked fewer cigarettes.
Conclusion:
Quantity of emotional support was associated with higher levels of negative emotionality, whereas the opposite was found for quality of emotional support. Emotional support may indirectly influence smoking via depressed mood. Effecting the perceived quality of support appears to be the mechanism by which emotional support helps to reduce smoking in adult African Americans.
Keywords: Social Support, African American, Alcohol, Tobacco, Depressed Mood, Stress
1. Introduction
Alcohol and tobacco use have detrimental impacts on African American’s mental and physical health. African Americans have an increased risk of mortality associated with tobacco use (Thorpe et al., 2013) and alcohol problems compared to European Americans (Kerr et al., 2011). Unlike European Americans, rates of mortality among African Americans remain as high for late-onset smokers as early-onset smokers (Roberts et al., 2016). Additionally, general risk of developing a substance use disorder is higher among African Americans compared to European Americans despite European Americans displaying higher rates of tobacco smoking and alcohol use during adolescence. Interestingly, rates of initiation and use increase for African Americans around midlife according to recent findings from the National Epidemiologic Survey of Alcohol and Related Conditions-III (Vasilenko et al., 2017).
Alcohol and tobacco use have both been associated with depression and stress specifically in African Americans drinkers and smokers (Boardman et al., 2001; Chatters et al., 2015; Mulia et al., 2008). Older African Americans, in comparison to other ethnic groups, report higher levels of stress (Sheffler and Sachs-Ericsson, 2016), which is a known risk factor for the onset of drug use, other health disparities, and worse outcomes (Jackson et al., 2010). In a study of adult African Americans, daily smokers and daily drinkers were both 3 times more likely to show depressive symptomology in comparison to non-users of each substance (Epstein et al., 2009). Likewise, it has been shown that among African American’s, higher levels of psychosocial stress is associated with an 86% increase in risk for being a current smoker (as opposed to a non-smoker), and a 33% increase in risk for being a past smoker (as opposed to being a non-smoker) (Slopen et al., 2012).
Multiple hypotheses exist to explain the disparities between groups in the general population. The diathesis-stress model of addiction (Windle, 2010) focuses on the intersection of multiple factors, such as genetic, cognitive, social, and neighborhood characteristics, that conjointly influence the likelihood that a person will use and abuse a drug. The model asserts that the integrated effects of these factors may vary across individuals and over time. For example, despite lower levels of substance use among African Americans compared to their European American counterparts during adolescence and young adulthood, in combination with disproportionate differences in stress, depression, and other sociodemographic factors there exists the potential for these factors to greatly influences the likelihood of manifesting a substance use disorder for African Americans later in life.
A related explanation for disparities between groups in the general population is the self-medication hypothesis, which notes that individuals use substances as a means of reducing levels of stress or anxiety (Goeders, 2004; Jackson et al., 2010; Slopen et al., 2012) and that European Americans and African Americans may self-medicate to different extents. Individuals under stress may use tobacco or alcohol to soothe, distract from or avoid daily life stressors (Khantzian, 1997) that often precipitate a milieu of other psychological (Slopen et al., 2012) and physiological problems (Kim et al., 2012; Mulia et al., 2008; Rodriquez et al., 2017; Sheffler and Sachs-Ericsson, 2016).
Evidence suggests that social support (i.e., the perception and frequency of contact with friends, family, and other supportive network members (Chatters et al., 2015; Marshall and Rue, 2012) moderates alcohol and tobacco use (Romano et al., 1991; White et al., 2009), as well as the severity of negative emotionality (i.e. stress and depression; (Chatters et al., 2015; Sheffler and Sachs-Ericsson, 2016)). For instance, receiving support from family and church members is protective against depressive symptomology and severe psychological distress in African Americans (Archibald et al., 2013; Chatters et al., 2015). Sheffler and Sachs-Ericsson (2016) have recently shown that support from family and peers is associated with reduced stress and substance use in an older sample of community-dwelling African and European American adults. This body of evidence indicates that social support may mitigate the effects of stress on the development of depression (i.e., the buffering hypothesis (Cohen and Wills, 1985). Conversely, recent work by Chatters et al. (2015) found that a lack of social support from family and peers was associated with increases in both depressed mood and stress in older African Americans. Social support was operationalized as “emotional support” (i.e., “How often do the people in your church make you feel loved and cared for?”) and higher levels of this emotional social support were associated with lower levels of depressive symptomatology and severe psychological distress. Altogether, the evidence suggests that social support may be an important target for reducing negative emotionality and associated alcohol and tobacco use. What remains unclear is the pathways through which a person’s social context shapes their mood and substance use behavior.
The current study adds to the literature by examining the association between two types of social support (emotional and instrumental) and alcohol and tobacco use in older African Americans. Moreover, the effects of social support are examined in the context of stress, depression, and socioeconomic background. We hypothesized that social support would have a direct and protective effect on alcohol and tobacco use and negative emotionality. Likewise, higher levels of stress and depressed mood would be associated with elevated alcohol and tobacco use. Lastly, higher levels of social support would be associated with lower levels of negative emotionality, which would indirectly influence alcohol and tobacco use.
2. Methods
2.1. Sample
Data for the current study are from the Carolina African American Twin Study on Aging (CAATSA; (Whitfield, 2013; Whitfield et al., 2003)). Participants (N=703; ~51% female) ranged in age from 22 to 92 with a mean age of 50 years (standard deviation (SD) =14.62). The average level of education was 12.88 years (SD = 3.4), which translated into most participants having attended and completed high school. Participants were selected from regions in North Carolina identified to have the highest ethnic distribution; birth records were examined for African American twin births. Voter registration information, as well as white page advertisements, were also used to find all possible living twin pairs from the records. Individuals were then contacted through letters and phone calls. Demographic information is available in Table 1. Both the age of participants and the level of education matched the state of North Carolina’s records during the years the data was collected. Most (61.5%) participants endorsed a monthly earning of over $1,500.00 (minimum= Under $100 (0), maximum= Over $1500 (15)). Additional information on the study design can be found elsewhere (Whitfield, 2013).
Table 1.
Description of Substance Use, Negative Emotionality, Social Support, and Covariates
| Measure | N | Mean / % | SD | Min | Max |
|---|---|---|---|---|---|
| Smokers’ daily cigarette use | 160 | 1.96 | 1.07 | 0 | 5 |
| Drinkers’ alcohol use frequency | 452 | 1.71 | 1.57 | 0 | 5 |
| Depressed Mood | 697 | 6.12 | 5.54 | 0 | 30 |
| Perceived Stress | 693 | 11.76 | 6.05 | 0 | 35 |
| Life Events | 703 | 6.09 | 5.57 | 0 | 40 |
| Emotional Quality | 691 | 2.92 | 1.03 | 0 | 4 |
| Instrumental Quality | 689 | 2.95 | 0.99 | 0 | 4 |
| Emotional Quantity | 697 | 1.69 | 0.95 | 0 | 3 |
| Instrumental Quantity | 697 | 1.16 | 0.80 | 0 | 3 |
| Gender (Male=0, Female=1) | 703 | 60% | - | 0 | 1 |
| Age | 703 | 49.78 | 14.52 | 22 | 92 |
| Years of education | 703 | 12.88 | 4.15 | 1 | 31 |
| Work status (unemployed = 0, employed=1) | 696 | 67% | - | 0 | 1 |
| Gross income per month | 675 | 12.56 | 3.87 | 0 | 15 |
Note. SD = Standard Deviation, Min = Minimum, Max = Maximum
2.2. Frequency of Substance use
Data on alcohol and tobacco use were gathered using self-report questionnaires. Analyses on the frequency of tobacco use focused on participants who self-identified as current smokers (n = 160 [~23%]; see Table 1). Current smokers described the frequency of their cigarette consumption per day (over the past year) using the following scale: 0 (none), 1 (less than ½ a pack/day), 2 (½ a pack/day), 3 (one pack/day) 4, 1 ½ packs/day, 5 (2+ packs/day), where pack refers to a standard pack of cigarettes. Analyses on the frequency of past-year drinking focused on participants who self-identified as current drinkers (n = 452; [~64%]; see Table 1). Past year drinking was measured on the following scale: 0 (not in the past year), 1 (A few times a year), 2 (Once or twice a month), 3 (Once a week), 4 (Two or three times a week), and 5 (daily or almost daily). Participants who reported having never used alcohol or tobacco were excluded from analyses by assigning them a missing value on the consumption variables. Similarly, those who endorsed a past history of smoking were also excluded. Analyses focused on these ordered levels of exposure scores for tobacco and alcohol.
2.3. Mood
Assessments of depressed mood (DM) over the course of the past week were obtained using the 11–item version of the Center for Epidemiological Studies Depression (CES-D scale). The CES-D scale was designed to measure depressive symptomatology in the general population. Items of the scale are symptoms associated with the severity of clinical depression (Radloff, 1977). Examples of questions include, “During this past week… I felt lonely” and “During this past week… I felt that everything I did was an effort.” Each question used a 4-point Likert scale for responses ranging from 0 (rarely or never) to 3 (most of the time). Calculation of the total CES-D score required reverse scoring questions 5 and 8 and then summing responses across all questions. The reliability (i.e., Cronbach alpha [α]) of CED-D items for this study was 0.79.
2.4. Stress and life events
Perceived stress (PS) was assessed using the Perceived Stress Scale (PSS) (Cohen et al., 1983). The PSS consists of 14 items on feelings experienced within the last month. Examples included, “In the last month, how often have you been upset because of something that happened unexpectedly?” and “In the last month, how often have you been able to control irritations in your life?” Each question was assessed on a 5-point scale ranging from 0 (never) to 4 (very often). Total scores were derived by reverse scoring responses to items 4, 5, 7, and 8. A measure of total perceived stress was obtained by summing across all of the items. As such, higher scores are indicative of a higher level of perceived stress. Analyses focused on nine of the questions in the 10-item version (Taylor, 2015). Specifically, the question, “In the last month, how often have you felt that you were unable to control the important things in your life?” was removed to achieve acceptable internal consistency (α=0.78).
An additional measure of stress was obtained using the number of positive and negative potentially stressful life events (LE) that participants reported experiencing in the past year. Examples of events included marriage, divorce, retirement, changes in living arrangements, acquiring an illness, and illness or death of close friends or family members. The number of life events was assessed using a 26-item questionnaire. For each item endorsed, participants rated its importance using the following scale: “of little importance”, “somewhat important” or “very important”. Since it was commonly observed that, if an event occurred it was rated as being of high importance, only the number of events experienced was used for the purpose of this analysis. This was done so as not to conflate event importance with event occurrence.
2.5. Social Support (SS)
Levels of social support in the past year were assessed using a self-report questionnaire that allowed for an examination of the importance of two subjective features: quality (i.e., the perceived level of satisfaction with the quality of support received) and quantity (i.e., the perceived amount of support received). Questionnaire items focused on the perceived quality and quantity of instrumental and emotional forms of social support (ISS and ESS, respectively), where ISS was defined as instances when family and friends performed actions, such as giving one a ride, looking after one’s home; or buying one food. ESS was defined as instances in which the participant was able to confide in loved ones about problems and worries. Quality of ISS and ESS was measured with a five-point Likert scale of 1 (not satisfied at all) to 5 (extremely satisfied). For the quantity of ISS, participants provided the frequency of three activities: (1) receiving a ride, (2) getting help around the home, or (3) receiving a monetary loan. For the quantity of ESS, participants provided the frequency of two activities: (1) receiving advice or (2) discussing issues with family and/or peers. Quantity of ISS and ESS were based on participant averages across the respective activities.
2.6. Covariates
Several covariates were included to minimize the possibility of confounding due to other factors known to be associated with levels of substance misuse (Compton et al., 2007; Sacco et al., 2014; Vasilenko et al., 2017), stress (Sacco et al., 2014; Woodward et al., 2012), and depressed mood (Fernandez et al., 1998; Pickett et al., 2013). Covariates included age, gender, and three measures socioeconomic status (education level (which was mean-centered), gross household income per month, and current employment status).
2.7. Statistical Analysis
Data were prepared and described using SPSS (version 24) (IBM_Corporation, 2016). Ordinal logistic regression analyses were conducted using Mplus (Version 8) (Muthén and Muthén, 2017). Analyses focused on the primary study hypotheses. Specifically, we examined the association between alcohol and tobacco consumption with each measure of social support, both before and after adjusting for the effects of the covariates (i.e., age, gender, and SES). Similarly, we examined the effect of social support on DM, PS, and LE, as well as the association between each measure of negative emotionality with alcohol and tobacco use. Incrementally complex models were used to assess the effects of covariates as confounders. Lastly, interaction and mediation models were used to determine whether any significant main effects of negative emotionality on drug use were moderated by social support, or whether the effects of social support were mediated by DM, PS, or LE. All models were tested while controlling for non-independence in the data since individuals were nested within families.
3. Results
3.1. Sample Description
The average level of smoking in the sample corresponded to roughly a half a pack a day. The mean level of frequency of drinking was roughly “once or twice a month”. The observed mean level of depressed mood in the sample was below the established clinical threshold for the 11-item CES-D-10 (M=6.12, SD=5.54). Lastly, the sample mean for the observed level of stress was low (M=11.76, SD=6.05).
Table 2 shows the association between covariates and substance use outcomes. Age was the only covariate that was significantly associated with cigarette smoking, suggesting that older individuals consumed more cigarettes per day. On the contrary, alcohol consumption was negatively associated with age and income but was positively associated with current work status; though it should be noted that individuals with higher incomes consumed less frequently. Females also consumed alcohol less frequently.
Table 2.
Effect of Covariates on Alcohol and Tobacco Use
| Average # of cigarettes smoked per day |
Alcohol frequency |
|
|---|---|---|
| Covariates | β | β |
| SES: Education | −0.02 (0.08) | 0.12 (0.07) |
| SES: Gross income | 0.01 (0.12) | −0.14 (0.06)* |
| SES: Work status (0=not working, 1=working) | −0.05 (0.11) | 0.19 (0.06)** |
| Age | 0.23 (0.09)* | −0.21 (0.05)** |
| Gender (0=Male, 1=Female) | −0.01 (0.09) | −0.19 (0.05)** |
Note. SES =socioeconomic status composed of mean-centered education, gross income per month, and work status (0=not working, 1=working). SES estimates presented here are the partial effects of each measure on outcome controlling for the other 2 forms of SES. Mean-centered age. Gender assessed with 0=Male, and 1=Female. SE = Standard Error.
p≤0.05,
p≤0.01.
Correlations among measures of social support ranged from 0.11 to 0.58. The largest association was between quality of emotional support and quality of instrumental support (r=0.58 [SE=0.04]). The association between quantity of emotional and quantity of instrumental support was moderate (r=0.35 [SE=0.04]). Correlations between quality of support and quantity of support were modest both within (i.e., emotional support: rQuality:Quantity = 0.23 [SE=0.04]; instrumental support: rQuality:Quantity = 0.16 [SE=0.04]) and across support types (rQuality-emotional:Quantity-instrumental = 0.11 [SE=0.04]; rQuality-instrumental:Quantity-emotional = 0.15 [SE=0.04]).”
3.2. The effect of SS on alcohol and tobacco use
Analysis of the effect of each measure of social support suggested main effects on alcohol, but not tobacco use (Table 3). Specifically, findings before (model-1) and after (model-2) adjusting for covariates indicated that more social support, in general, was associated with less alcohol consumption. The exception to this was quantity of instrumental support, which was not associated with frequency of alcohol use in either model. Protective effects of quality support on drinking were observed to be limited in model-3, which was adjusted for all covariates and all other forms of social support to account for any potential confounding (i.e., due to other covariates) in the observed association between quality of support and drinking.
Table 3.
Effects of Social Support on Alcohol and Tobacco Use
| Outcome | Predictors | Model-1 |
Model-2 |
Model-3 |
|---|---|---|---|---|
| β (SE) | β (SE) | β (SE) | ||
| Tobacco | Emotional Quality | −0.02 (0.09) | <−0.01 (0.09) | 0.04 (0.12) |
| Emotional Quantity | −0.06 (0.09) | <−0.01 (0.10) | 0.02 (0.11) | |
| Instrumental Quality | −0.01 (0.10) | −0.03 (0.10) | −0.06 (0.13) | |
| Instrumental Quantity | 0.02 (0.10) | −0.01 (0.10) | <0.01 (0.12) | |
| Alcohol | Emotional Quality | −0.08 (0.05)† | −0.09 (0.04)* | −0.02 (0.06) |
| Emotional Quantity | −0.11 (0.05)* | −0.08 (0.05)† | −0.09 (0.06) | |
| Instrumental Quality | −0.12 (0.05)* | −0.11 (0.05)* | −0.09 (0.06) | |
| Instrumental Quantity | −0.03 (0.05) | −0.02 (0.05) | 0.01 (0.06) | |
Note. Table showing the standardized regression coefficient from models predicting variation in alcohol and tobacco use with each type of social support. Model-1 includes no covariates. Model-2 controls for the effects of age, gender, and SES (education, income, work status). Model-3 additionally accounts for the joint effect of all forms of social support.
p<0.05,
p<0.01,
p<0.10.
3.3. The effect of SS on DM, PS, and LE
The effects of social support varied across measures of negative emotionality (Table 4). Both quantity and quality of ESS were significantly associated with depressed mood and perceived stress, but ISS was not. Quality of ESS was associated with fewer DM and PS symptoms, while quantity of ESS was associated with more DM and PS symptoms. Overall, this suggests that quality of social support may be a protective mechanism whereas quantity of social support reflects an increased need.
Table 4.
Association between Four Types of Social Support and Negative Emotionality
| Predictor | Depressed Mood |
Perceived Stress |
Life Events |
|---|---|---|---|
| β (SE) | β (SE) | β (SE) | |
| Emotional Quality | −0.22 (0.05)*** | −0.28 (0.04)*** | −0.03 (0.06) |
| Emotional Quantity | 0.15 (0.04)*** | 0.22 (0.04)*** | 0.13 (0.04)** |
| Instrumental Quality | −0.01 (0.05) | −0.05 (0.05) | <0.01 (0.05) |
| Instrumental Quantity | 0.04 (0.04) | 0.07 (0.04) | 0.05 (0.04) |
Note. Table showing the conditional effect of each form of social support on measures of negative emotionality while controlling for covariates. SE = Standard Error.
p<0.05,
p<0.01,
p<0.001.
3.4. The effect of DM, PS, and LE on alcohol and tobacco use
The relative predictive importance of DM, PS, and LE varied by substance (Table 5). Higher levels of depressed mood were positively associated with tobacco usage, such that individuals who smoked more cigarettes per day had above average depressed mood; PS and LE were not associated with smoking. Notably, mood effects on smoking were not confounded with covariates or social support. Neither DM, PS, nor LE were associated with alcohol consumption. Given the associations between ISS and ESS with substance use and negative emotionality, we further examined whether there could be indirect or moderating effects of social support between DM and substance use. As such, we explored whether the observed effect of DM on tobacco consumption was moderated by social support (see Table 6); no significant interactions between depression and any of the social support variables were observed. Our examination of the total and indirect effects revealed that quality of emotional support and quantity of emotional support significantly predicted depression severity, over and above the effects of instrumental support and covariates (see Figure 1). Moreover, quantity and quality of emotional support had significant indirect effects on cigarette smoking via their effects on depression (Total indirect for: quantity of emotional support - β = 0.03 (SE=0.01), p<.05; quality of emotional support - β = −0.05 (SE=0.02),p<.05).
Table 5.
Main Effects of Negative Emotionality on Alcohol and Tobacco Use
| Outcome | Predictors | Model-1 |
Model-2 |
Model-3 |
|---|---|---|---|---|
| β (SE) | β (SE) | β (SE) | ||
| Tobacco | Depressed Mood | 0.19 (0.08)* | 0.22 (0.09)* | 0.25 (0.10)* |
| Perceived Stress | 0.06 (0.09) | 0.07 (0.10) | 0.06 (0.11) | |
| Life Events | 0.08 (0.09) | 0.08 (0.09) | 0.10 (0.10) | |
| Alcohol | Depressed Mood | 0.03 (0.05) | 0.01 (0.05) | 0.00 (0.05) |
| Perceived Stress | −0.01 (0.05) | −0.01 (0.05) | −0.03 (0.06) | |
| Life Events | −0.01 (0.01) | −0.04 (0.05) | −0.02 (0.05) | |
Note. Table showing the standardized regression coefficient from models predicting variation of frequency of alcohol and tobacco use across the three mood variables. Model-1 includes no covariates. Model-2 controls for the effects of age, gender, and SES. Model-3 builds upon model-2 by also controlling for all four social support variables. Note. SE = Standard Error.
p≤0.05,
p<0.01.
Table 6.
Interaction effects of depression and social support on tobacco consumption
| Predictors | β | S.E. | p |
|---|---|---|---|
| Depressed Mood | 0.34 | 0.24 | 0.17 |
| Emotional Quality | −0.07 | 0.25 | 0.80 |
| Emotional Quantity | 0.17 | 0.19 | 0.36 |
| Instrumental Quality | 0.00 | 0.23 | 0.99 |
| Instrumental Quantity | −0.09 | 0.21 | 0.68 |
| Int 1: Quality ESS x CES-D | 0.44 | 0.40 | 0.26 |
| Int 2: Quantity ESS x CES-D | −0.40 | 0.31 | 0.20 |
| Int 3: Quality ISS x CES-D | −0.34 | 0.44 | 0.43 |
| Int 4: Quantity ISS x CES-D | 0.17 | 0.35 | 0.63 |
| Age | 0.23 | 0.11 | 0.03 |
| Gender | −0.09 | 0.11 | 0.46 |
| Years of education | 0.11 | 0.11 | 0.33 |
| Gross income per month | −0.03 | 0.12 | 0.84 |
| Work status | 0.07 | 0.12 | 0.54 |
Note. Table showing the results of the multivariate ordinal logistic regression model of smoking including age, gender, and SES as covariates (not shown). Abbreviations ESS - Emotional Social Support, Int1 thru 5 - interaction variable, ISS - Instrumental Social Support. Notations. S.E. - standard error, p – p-value,
p≤0.05.
Figure 1:
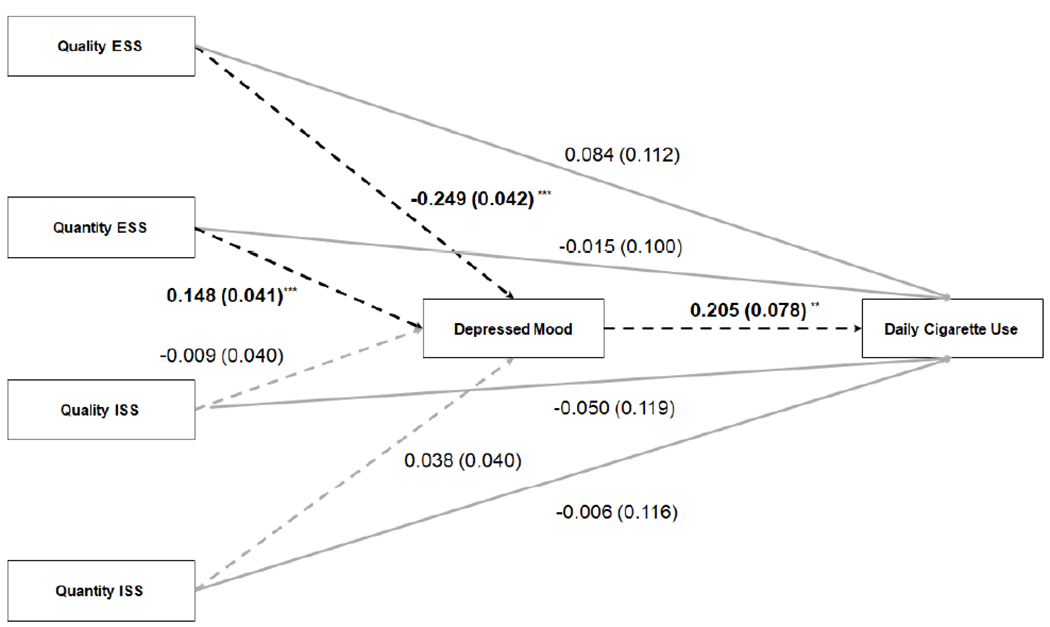
Illustration of multivariate path model of the total and indirect effects of social support (SS) and depressed mood on daily cigarette use among African Americans; covariates not shown. Notation: *p<0.05, **p<0.01, ***p<0.001 indicate standardized loadings that were significantly different from zero. Solid arrows indicate direct effects on cigarette consumption. Dashed arrows indicate indirect pathway from social support to cigarette consumption. Grayed out lines are non-significant. Following path tracing rules, the product of the standardized indirect path plus the square of the direct path equals the total effects of each form of SS on cigarette consumption. Abbreviations: ESS – Emotional Social Support, ISS – Instrumental Social Support.
4. Discussion
4.1. Summary and Explanation of Results
The current study builds upon the existing literature by providing new evidence to support the role of social support in alcohol and tobacco use in African American adults, albeit via different mechanisms. We found that social support was directly related to frequency of alcohol consumption, but indirectly related to tobacco smoking. Our results are in line with the buffering hypothesis, whereby social support impacts tobacco consumption indirectly by ameliorating the severity of depressed mood. Throughout all analyses, both ISS and ESS were associated with negative emotionality. Better quality ISS and ESS were associated with less negative emotionality, capturing the protective effects of social support. Higher quantities of ISS and ESS were associated with more negative emotionality respectively, suggesting that individuals who are experiencing more stress and depression may need more social support.
Consistent with previous observations of the complex interrelationship between negative emotionality and substance use, we found that higher levels of depressed mood were associated with more frequent cigarette smoking. The strong association observed between smoking and negative emotionality is in line with both the self-medication and the diathesis-stress model. As African American individuals age, the continued experience of stress may lead to both a lower threshold for substance use problems, as well as increased substance use to cope with those stressors. Experiences of race-related stress or discrimination contribute to overall reported stress and, potentially, contribute to worse outcomes for African Americans. Although the current study does not examine race-related stress, previous studies have found that African Americans experienced higher race-related stress than other ethnic minority groups, that race-related stress was a significantly more powerful risk factor than stressful life events for negative emotionality, and that institutional racism-related stress was a significant predictor of psychological health in older African Americans (Utsey et al., 2002a; Utsey et al., 2008; Utsey et al., 2002b). The impact of race-related stress on depressed mood is a mechanism unique to African Americans by which risk may be conferred.
Contrary to prior findings using a broad measure of peer and family support (Romano et al., 1991), none of the forms of social support were directly associated with tobacco consumption. This may be due to differences in measures of social support and samples between studies. For instance, Romano, et al., (1991) examined one item regarding emotional support and the likelihood of turning to one’s network for instrumental support in a sample of African Americans in two major cities, which was significantly associated with tobacco use among women. In the present study, quality of ESS and ISS have a significant protective effect on both depressed mood and perceived stress. Quality of social support has previously been shown to differentially alleviate negative emotionality depending on race/ethnicity, such that satisfaction with social support was associated with lower psychological distress among European Americans but not African Americans (Morin and Midlarsky, 2016). The difference in our findings could also result from the wide age distribution in this sample.
Maladaptive coping with negative emotionality has been associated with the initiation and maintenance of tobacco use (Carmody et al., 2007). The current findings make an important contribution to the literature and can inform the development of interventions aimed at reducing tobacco-related health disparities. Despite the lack of a direct effect of ISS and ESS on alcohol and tobacco consumption, both were protective against higher reported perception of stress. Notably, the pattern of effects indicated that higher quality and not quantity of support was the mechanism by which SS may be protective against stress (Benca-Bachman et al., in press). Similar to the findings of Web Hooper et al. (Webb Hooper et al., 2013), we found the role of social support in reducing smoking to operate indirectly through a mediating mechanism, in this instance by quality of ESS reducing depressed mood. While these results are still in need of further replication, they suggest that enhancing supportive social interactions specific to the emotional needs of smokers may be an effective means to reduce smoking in African Americans. Due to the positive association between increased depression symptoms and daily cigarette use, higher quality ESS may decrease depressed mood and, in turn, decrease tobacco use triggered by maladaptive coping.
4.2. Limitations
There are several important considerations for interpreting these data. First, the current study uses self-report questions about substance use, which may be biased upward for case-control differences. However, given that CAATSA’s sampling pool was large and focused on a community sample, these effects are expected to be limited. Second, gender differences may play a role in the observed effects, although, larger sample sizes are needed to robustly estimate these effects; we report point estimates that control for gender as a way of minimizing any bias in our estimates. Third, given that this study utilized cross-sectional data, we could not determine whether thresholds were changing over time, as might be expected if the diathesis-stress model holds true. Pursuant to this issue, we also did not have information on why participants chose to use substances (i.e., whether it was it to self-medicate or due to other motivating factors) and whether the associations observed represent causal effects of social support; future studies are needed in prospective samples to infer causal effects. Fourth, our interpretations are limited to the frequency of smoking and drinking. Given the relatively low frequency of drinking, the heaviness of drinking among the sample was not explored. Lastly, it is unknown whether these findings generalize to additional forms and sources of social support.
4.3. Future Directions
This study could be improved through an increase in the overall sample size to better understand gender differences and the effects of other substances, such as marijuana, which has lower rates of use (Lloyd and Striley, 2018) compared to alcohol and tobacco. Additionally, the effects of social support (both ESS and ISS) on substance use and negative emotionality may change depending on the source of social support, and therefore support sources should be examined. Previous literature has noted the potential beneficial effects of church-based social support systems (Chatters et al., 2015), particularly for African American populations that historically have utilized religious and spiritual support in times of distress. Religious social support may be key to the differing effect of social support on negative emotionality among older African Americans populations in comparison to European Americans (Debnam et al., 2012). Likewise, interventions that incorporate social support from friends/peers have been shown to reduce drinking amongst heavy drinkers (Mavandadi et al., 2015). A recent finding suggests that family/friends can be trained to promote and effect smoking cessation (Aschbrenner et al., 2018) though it remains unclear if these trends generalize to African Americans.
4.4. Conclusions
These results point to the importance of studying specific aspects of social support simultaneously. In particular, different aspects of the same type of social support, quality and quantity, are differentially related to negative emotionality. We found the quantity of both ISS and ESS are indicative of higher levels of negative emotionality. Perceived quality of support appears to be the mechanism by which social support helps to reduce related tobacco use. In summary, these findings confirm that depressed mood is a notable intervention target for reducing tobacco use in African Americans. Similarly, the type and quality of social support are indirect mechanisms to effect reduced tobacco consumption. However, further inquiry is required to assess the potential moderating effects of ISS and ESS, albeit with larger samples.
Highlights.
Emotional, not instrumental, social support is directly associated with reduced daily drinking.
In African Americans, higher levels of depressed mood are associated with heavier daily smoking.
The protective effects of social support on daily smoking is mediated by negative emotionality.
Acknowledgments
Role of funding sources: This work was supported by the National Institute of Health’s National Institute on Aging grant (R01AG013662 [Whitfield] and K02AG059140 [Thorpe]), the National Institute on Minority Health and Health Disparities (NIMHD U54MD000214 [Thorpe]), and the National Institute on Drug Abuse (DP1DA042103; Palmer).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of interest: The authors have no conflicts to declare.
REFERENCES
- Archibald PC, Dobson Sydnor K, Daniels K, Bronner Y, 2013. Explaining African-Americans’ depressive symptoms: a stress-distress and coping perspective. J Health Psychol 18(3), 321–331. [DOI] [PubMed] [Google Scholar]
- Aschbrenner KA, Patten CA, Brunette MF, 2018. Feasibility of a support person intervention to promote smoking cessation treatment use among smokers with mental illness. Transl Behav Med 8(5), 785–792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benca-Bachman CE, Najera D, Whitfield K, Taylor JJ, Thorpe RJ, Palmer R, in press Quality and Quantity of Social Support Show Differential Associations with Stress and Depression in African Americans. . American Journal of Geriatric Psychiatry. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boardman JD, Finch BK, Ellison CG, Williams DR, Jackson JS, 2001. Neighborhood disadvantage, stress, and drug use among adults. J Health Soc Behav 42(2), 151–165. [PubMed] [Google Scholar]
- Carmody TP, Vieten C, Astin JA, 2007. Negative affect, emotional acceptance, and smoking cessation. J Psychoactive Drugs 39(4), 499–508. [DOI] [PubMed] [Google Scholar]
- Chatters LM, Taylor RJ, Woodward AT, Nicklett EJ, 2015. Social support from church and family members and depressive symptoms among older African Americans. Am J Geriatr Psychiatry 23(6), 559–567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S, Kamarck T, Mermelstein R, 1983. A global measure of perceived stress. J Health Soc Behav 24(4), 385–396. [PubMed] [Google Scholar]
- Cohen S, Wills TA, 1985. Stress, social support, and the buffering hypothesis. Psychol Bull 98(2), 310–357. [PubMed] [Google Scholar]
- Compton WM, Thomas YF, Stinson FS, Grant BF, 2007. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States: results from the national epidemiologic survey on alcohol and related conditions. Archives of general psychiatry 64(5), 566–576. [DOI] [PubMed] [Google Scholar]
- Debnam K, Holt CL, Clark EM, Roth DL, Southward P, 2012. Relationship between religious social support and general social support with health behaviors in a national sample of African Americans. J Behav Med 35(2), 179–189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epstein JF, Induni M, Wilson T, 2009. Patterns of clinically significant symptoms of depression among heavy users of alcohol and cigarettes. Prev Chronic Dis 6(1), A09. [PMC free article] [PubMed] [Google Scholar]
- Fernandez ME, Mutran EJ, Reitzes DC, Sudha S, 1998. Ethnicity, gender, and depressive symptoms in older workers. Gerontologist 38(1), 71–79. [DOI] [PubMed] [Google Scholar]
- Goeders NE, 2004. Stress, Motivation, and Drug Addiction. Current directions in psychological science 13(1), 33–35. [Google Scholar]
- IBM_Corporation, 2016. SPSS Statistics for Windows, Version 24.0. IBM Corp, Armonk, NY. [Google Scholar]
- Jackson JS, Knight KM, Rafferty JA, 2010. Race and unhealthy behaviors: chronic stress, the HPA axis, and physical and mental health disparities over the life course. Am J Public Health 100(5), 933–939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerr WC, Greenfield TK, Bond J, Ye Y, Rehm J, 2011. Racial and ethnic differences in all-cause mortality risk according to alcohol consumption patterns in the national alcohol surveys. Am J Epidemiol 174(7), 769–778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khantzian EJ, 1997. The self-medication hypothesis of substance use disorders: a reconsideration and recent applications. Harv Rev Psychiatry 4(5), 231–244. [DOI] [PubMed] [Google Scholar]
- Kim G, Bryant AN, Parmelee P, 2012. Racial/ethnic differences in serious psychological distress among older adults in California. Int J Geriatr Psychiatry 27(10), 1070–1077. [DOI] [PubMed] [Google Scholar]
- Lloyd SL, Striley CW, 2018. Marijuana Use Among Adults 50 Years or Older in the 21st Century. Gerontol Geriatr Med 4, 2333721418781668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall GL, Rue TC, 2012. Perceived discrimination and social networks among older African Americans and Caribbean blacks. Fam Community Health 35(4), 300–311. [DOI] [PubMed] [Google Scholar]
- Mavandadi S, Helstrom A, Sayers S, Oslin D, 2015. The Moderating Role of Perceived Social Support on Alcohol Treatment Outcomes. J Stud Alcohol Drugs 76(5), 818–822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morin RT, Midlarsky E, 2016. Social Support, Mastery, and Psychological Distress in Black and White Older Adults. Int J Aging Hum Dev 82(2-3), 209–228. [DOI] [PubMed] [Google Scholar]
- Mulia N, Ye Y, Zemore SE, Greenfield TK, 2008. Social disadvantage, stress, and alcohol use among black, Hispanic, and white Americans: findings from the 2005 U.S. National Alcohol Survey. J Stud Alcohol Drugs 69(6), 824–833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO, 2017. Mplus User’s Guide. Eighth Edition Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Pickett YR, Bazelais KN, Bruce ML, 2013. Late-life depression in older African Americans: a comprehensive review of epidemiological and clinical data. Int J Geriatr Psychiatry 28(9), 903–913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff LS, 1977. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement 1(3), 385–401. [Google Scholar]
- Roberts ME, Colby SM, Lu B, Ferketich AK, 2016. Understanding Tobacco Use Onset Among African Americans. Nicotine Tob Res 18 Suppl 1, S49–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodriquez EJ, Gregorich SE, Livaudais-Toman J, Perez-Stable EJ, 2017. Coping With Chronic Stress by Unhealthy Behaviors: A Re-Evaluation Among Older Adults by Race/Ethnicity. J Aging Health 29(5), 805–825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romano PS, Bloom J, Syme SL, 1991. Smoking, social support, and hassles in an urban African-American community. Am J Public Health 81(11), 1415–1422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sacco P, Bucholz KK, Harrington D, 2014. Gender differences in stressful life events, social support, perceived stress, and alcohol use among older adults: results from a National Survey. Subst Use Misuse 49(4), 456–465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheffler J, Sachs-Ericsson N, 2016. Racial Differences in the Effect of Stress on Health and the Moderating Role of Perceived Social Support. J Aging Health 28(8), 1362–1381. [DOI] [PubMed] [Google Scholar]
- Slopen N, Dutra LM, Williams DR, Mujahid MS, Lewis TT, Bennett GG, Ryff CD, Albert MA, 2012. Psychosocial stressors and cigarette smoking among African American adults in midlife. Nicotine Tob Res 14(10), 1161–1169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor JM, 2015. Psychometric analysis of the Ten-Item Perceived Stress Scale. Psychological assessment 27(1), 90–101. [DOI] [PubMed] [Google Scholar]
- Thorpe RJ Jr., Wilson-Frederick SM, Bowie JV, Coa K, Clay OJ, LaVeist TA, Whitfield KE, 2013. Health behaviors and all-cause mortality in African American men. Am J Mens Health 7(4 Suppl), 8S–18S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Utsey SO, Chae MH, Brown CF, Kelly D, 2002a. Effect of ethnic group membership on ethnic identity, race-related stress, and quality of life. Cultur Divers Ethnic Minor Psychol 8(4), 366–377. [DOI] [PubMed] [Google Scholar]
- Utsey SO, Giesbrecht N, Hook J, Stanard PM, 2008. Cultural, sociofamilial, and psychological resources that inhibit psychological distress in African Americans exposed to stressful life events and race-related stress. Journal of Counseling Psychology 55(1), 49–62. [Google Scholar]
- Utsey SO, Payne YA, Jackson ES, Jones AM, 2002b. Race-related stress, quality of life indicators, and life satisfaction among elderly African Americans. Cultur Divers Ethnic Minor Psychol 8(3), 224–233. [DOI] [PubMed] [Google Scholar]
- Vasilenko SA, Evans-Polce RJ, Lanza ST, 2017. Age trends in rates of substance use disorders across ages 18-90: Differences by gender and race/ethnicity. Drug and alcohol dependence 180, 260–264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Webb Hooper M, Baker EA, McNutt MD, 2013. Associations between coping, affect, and social support among low-income African American smokers. Addict Behav 38(11), 2736–2740. [DOI] [PubMed] [Google Scholar]
- White AM, Philogene GS, Fine L, Sinha S, 2009. Social support and self-reported health status of older adults in the United States. Am J Public Health 99(10), 1872–1878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitfield KE, 2013. A registry of adult African American twins: the Carolina African American Twin Study of Aging. Twin research and human genetics : the official journal of the International Society for Twin Studies 16(1), 476–480. [DOI] [PubMed] [Google Scholar]
- Whitfield KE, Brandon DT, Wiggins S, Vogler G, McClearn G, 2003. Does intact pair status matter in the study of African American twins? The Carolina African American Twin Study of Aging. Exp Aging Res 29(4), 407–423. [DOI] [PubMed] [Google Scholar]
- Windle M, 2010. A Multilevel Developmental Contextual Approach To Substance Use and Addiction. Biosocieties 5, 124–136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woodward AT, Taylor RJ, Bullard KM, Aranda MP, Lincoln KD, Chatters LM, 2012. Prevalence of lifetime DSM-IV affective disorders among older African Americans, Black Caribbeans, Latinos, Asians and non-Hispanic White people. Int J Geriatr Psychiatry 27(8), 816–827. [DOI] [PMC free article] [PubMed] [Google Scholar]