

Abstract
The number of children immigrating to the United States has increased steadily during the last decade. American families are adopting a significant portion of these children, more than 20,000. Recently immigrated children face many different health risks when compared to children born in the United States. They are subject to many infectious diseases no longer seen commonly in the United States such as malaria, tuberculosis, and HIV. They are more likely to have inadequate immunity to vaccine-preventable illnesses. Recent immigrants have a higher likelihood of having malnutrition and developmental delay. Finally, many will have suffered psychological trauma in either institutions or refugee camps. These children require specialized testing, care, and treatment in the pediatric office.
In 2002, 1,063,732 people immigrated to the United States. Of these, 186,328 were children younger than the age of 16 years.1 This population will face many unique health risks when compared with the general pediatric population in the United States. This article will discuss many of the infectious diseases commonly diagnosed among recently immigrated children. Special attention will be given to those children who are being adopted internationally by citizens of the United States. Finally, this article will touch on some of the more common psychosocial needs of children immigrating to the United States, as these issues often require long-term intervention by the pediatrician.
Epidemiology
Thirty-eight percent of immigrants to the United States originate from North or Central America. Mexico is the most common country of origin, comprising 20.6 percent of all immigrants to the United States. The next most common region of origin for persons immigrating to the United States is Asia, with 32.2 percent of all immigrants originating in Asia. Sixteen percent of the immigrants to the United States come from Europe.1 South America, Africa, and other regions each provides less than 10 percent of the immigrants. Prevalent infectious diseases vary by region as well as by country, and so the country from which a person immigrates will have implications for the infectious diseases for which they should be screened.
The number of children adopted internationally by American families has increased greatly during the last decade. In 1993, 7,377 children were adopted internationally, compared with 21,616 in 2003.2 Several factors account for the increase in international adoption. Domestically, parents placing children for adoption have more choices concerning who adopts their children, as well as increased access to information and contact with their biologic children. Some adoptive families are uncomfortable with this model. Also, awareness of the needs of children worldwide and a desire to provide a stable family for them have increased. Lastly, some misconception exists that children available for adoption from international settings are less likely to have been exposed to drugs or alcohol than are those available for domestic adoption. Of the children adopted in 2003, 32 percent were from China. The next most frequent country of origin was Russia, with 24 percent of the children originating from there.2 Other countries included Guatemala, South Korean, Ukraine, Kazakhstan, and India (Fig 1).
Figure 1.
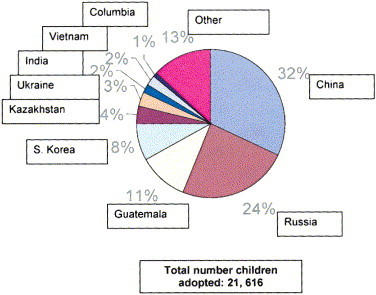
International adoptions by country, 2003. (Color version of figure is available online.)
The medical examination required before children can enter the United States varies depending on the type of visa held by the child. Those entering on a temporary visa, such as a tourist visa, have no medical requirements.3 If the child is entering on a permanent residency visa, all that is required is a physical examination for certain conditions, such as active tuberculosis, human immunodeficiency virus (HIV), syphilis, gonorrhea, or leprosy.3 If the child is younger than 15 years of age, no laboratory testing is required. With the exception of children being adopted by American families, all permanent residents are asked to show proof of appropriate immunizations. What is appropriate is based on U.S. standards, as well as what is available in the country of origin.3, 4 Internationally adopted children are given a waiver, as long as parents sign a declaration that they will have all immunizations updated within a month of the child’s arrival in the United States.4 Because little screening is required before a child enters the country, further testing falls to practitioners taking care of newly immigrated children in the United States.
Recent immigrants to the United States are at higher risk for bringing infectious diseases for many reasons. Their previous living situation may have put them at risk for exposure to various diseases. Refugee detention centers often have inadequate sanitation and water supplies. If the child is immigrating from crowded urban areas, these same issues may be present. Children being adopted from institutions often are exposed to many infectious diseases via constant contact with a large number of caregivers and other children. In each of these situations, available medical care may have been inadequate, allowing illnesses to progress to more serious complications. Many of the children have had diets inadequate in calories, protein, vitamins, and other micronutrients. This deficiency leaves them even more vulnerable to various infectious diseases and may impact their development as well.
Once arriving in the United States, many immigrants and refugees may face barriers in accessing medical care. These barriers can include language barriers, financial barriers, and fear or misunderstanding of the medical system in the United States. They may have limited access within medical settings to trained translators. The use of friends or relatives can compromise confidentiality and, hence, the accuracy of information gathered. Immigrants may prefer to access ethnic medical practitioners familiar to them rather than seek traditional Western medical treatment. These practitioners may use traditional medications or herbs that contain heavy metals or strychnine. Alternatively, if family members have brought antibiotics or other agents that are available over the counter in other countries, their diseases may be treated with inadequate doses.
Dietary traditions may pose another risk. For instance, nonpasteurized milk or cheeses from India or Mexico may pose a health risk in some immigrant populations. Traditional clay cooking pots have been found to contain high levels of lead, leading to poisoning.5 Religious practices such as tattooing or circumcision may expose the child to infectious diseases, as well as other complications, when performed by nonmedical practitioners.
Different populations have different cultural concepts regarding the cause of illness. Hence, what may be considered as illness by Western practitioners may not be perceived as illness by the parents. One famous example is that of the Hmong culture, which attributes many illnesses to an imbalance in the universe that must be corrected to restore health. Failure to recognize this barrier leads many U.S. practitioners to determine the family is noncompliant or ignorant.4 These delays can further the risk a child faces for developing serious complications from infectious diseases and other illnesses.
Common infectious diseases
Intestinal parasites
One of the most common infectious diseases diagnosed in children recently arrived to the United States is some type of intestinal parasite. Among children adopted internationally, 15 to 35 percent have some pathogen identified on routine testing.6 Giardia lamblia was diagnosed in 87 (19%) of 461 children screened in one study.7 Those born in eastern European countries such as Russia were at higher risk for being infected with G. lamblia. Other common pathogens included Ascaris lumbricoides and Blastocystis hominis.
Both G. lamblia and B. hominis can be treated with metronidazole 35 to 50 mg/kg/d divided 3 times per day for 10 days. Nitazoxanide also has been approved for the treatment of G. lamblia in immunocompetent children older than 12 months of age. Although initial treatment guidelines are for nitazoxanide 100 mg/dose twice daily for 3 days, most practitioners have found that a longer course is necessary for eradication (up to 6 days).
Tuberculosis
Fifty-three percent (7,845) of new tuberculosis infections diagnosed in the United States are among foreign-born patients.8 Of these, approximately 1,400 are in children younger than 15 years of age. Tuberculosis screening is recommended for all children immigrating to the United States. This screening will consist of tuberculin skin testing and chest radiograph if needed. Tuberculosis is discussed in more detail in another article of this issue.
Hepatitis B
Worldwide, 2 billion people are infected with hepatitis B; 350 million have chronic infections.9 These infections are concentrated in the developing world: sub-Sahara Africa, Asia, and the Pacific. Those infected as children are more likely to develop chronic hepatitis: as many as 90 percent of those infected in the first year of life and 30 to 50 percent of those infected between 1 and 4 years of life. Of these children, one-quarter are at risk of developing liver cirrhosis or cancer.
Hepatitis B is a bloodborne pathogen and can be transmitted from mother to child during pregnancy or delivery, by unsafe use of needles or transfusion, and by sexual contact. For children, the most common route of transmission is from mother to child. Hepatitis B can be prevented by vaccination; however, the vaccine is not available in many parts of the world.
All children newly immigrated to the United States should be screened for hepatitis B infection. Studies have shown anywhere from 1 to 15 percent of children adopted internationally are positive for hepatitis B surface antigen.6 Screening consists of obtaining hepatitis B surface antigen, surface antibody, and core antigen. If the child has adequate immunization records, one can include a quantitative test for hepatitis B surface antibody to confirm immunity. Children should be rescreened 6 months after their arrival in the United States to ensure that they were not exposed to hepatitis B just before leaving their country of origin and that initial test results were falsely negative.
Hepatitis C
The World Health Organization (WHO) estimates that 200 million people, or 3 percent of the world’s population, are infected with hepatitis C (HCV). Like HIV or hepatitis B virus, HCV is transmitted from mother to child during pregnancy and delivery, through sexual contact, and via blood products or improperly used needles. Of those who are exposed to HCV, approximately 40 percent recover fully, whereas the remainder become chronic carriers. Of the carriers, 20 percent will develop cirrhosis of the liver. Transmission from mother to child takes place in approximately 5 percent of those exposed to HCV in utero. This number increases if the mother is coinfected with HIV.
Among children referred for international adoption, the number exposed to HCV has risen dramatically. The prevalence ranges from 1 to 5 percent10 in Commonwealth of Independent States (CIS) countries, where many international adoptees originate. In our clinic, a review of 200 adoption referral charts revealed that 24 children showed evidence of exposure to hepatitis C before being adopted. Of these, none was found to be infected on arrival to the United States. However, one child with no previous record of testing was found to be infected with HCV on arrival to the United States. All children recently immigrated to the United States should be screened for hepatitis C on arrival and again at 6 months.
Malaria
Between 300 and 400 million people become infected with malaria each year, leading to more than 1 million deaths. These deaths occur primarily in children younger than the age of 5 years and located in Africa. Treatment of malaria is becoming increasingly difficult. When evaluating a child newly immigrated to the United States, one should have a high index of suspicion for malaria. This illness is discussed in more detail in another article of this issue.
HIV
In 2002, 3.2 million children (<15 years old) were estimated to be living with HIV/acquired immunodeficiency syndrome (AIDS). Most HIV-infected children live in sub-Saharan Africa. The diagnosis and treatment of HIV/AIDS is covered in another section of this issue. Among 7,299 children adopted internationally since 1990, 12 children have been found to be infected with HIV. Only two children were known to be infected before their arrival in the United States. These children came from Russia, Cambodia, Romania, Panama, and Vietnam.11 All children, regardless of age, who are arriving in the United States should be screened for HIV using an enzyme-linked immunosorbent assay (ELISA) test. If this test is positive, more specific testing can be ordered depending on the child’s age. Using polymerase chain reaction technology as a screening tool in those children younger than 18 months of age is not advised as there is a risk of obtaining a false-negative result in those infected with a non-B subtype.
Measles
Although measles can be prevented by vaccination, worldwide, 30 to 40 million cases still occur each year, with 745,000 deaths.12 Fatalities are more common in developing countries, particularly where vitamin A deficiency is a common occurrence. Measles also is the most common preventable cause of blindness worldwide. The WHO is working to increase the number of children vaccinated against measles worldwide. However, because many children immigrating to the United States are coming from orphanages and/or refugee camps, they often are undervaccinated.
In the last 4 years, two measles outbreaks have occurred among children being adopted from China. The first, which occurred in February of 2001, initially was identified in a 10-month-old infant presenting to Texas Children’s Hospital, Houston, Texas, with measles-like symptoms developing immediately after the child entered the United States. Measles was confirmed serologically and contact investigation was begun. In all, 14 measles cases were identified, 10 in children adopted internationally, three in caregivers, and one in a sibling.13 Again in April 2004, another outbreak was noted among children adopted from Hunan Province, China. Six cases were confirmed serologically in this group.14 Lastly, one child adopted from Vietnam has been reported to develop SSPE after being adopted.15 Hence, when evaluating children recently adopted from international settings or recently immigrated, one should screen for vaccine-preventable illnesses such as measles. Often, interviewing families briefly before their clinic appointment is wise. If one suspects measles, varicella, or other communicable illnesses, families should not be allowed to wait in a clinic waiting area, which increases the risk of exposing other children, but should be placed immediately in an examination room for assessment.
Severe acute respiratory syndrome (SARS)
The first SARS outbreak, which occurred in 2002 to 2003, consisted of 8,098 probable cases in 29 countries. The illness spread between countries in part because of international travel. The case fatality was 9.6 percent.16 Since this initial outbreak occurred, researchers have predicted that SARS would continue to be a seasonal epidemic illness. However, 2004 brought only a few scattered cases of SARS, primarily in China. Several cases were associated with exposure during research activities with the virus.16
The virus that causes SARS is a coronavirus (CoV) and is spread via respiratory droplets. Individuals are most contagious on the 10th day postexposure. The elderly and chronically ill are at highest risk for the development of severe complications. Diagnosing SARS requires clinical, laboratory, and epidemiological criteria. Clinical criteria for diagnosing SARS are divided into three categories: early, mild/moderate, or severe disease (Table 1). Laboratory confirmation requires the detection of antibody to SARS-CoV. Cell culture also can be used. An RNA polymerase chain reaction test has been developed to detect SARS-CoV, but at this time it is not accepted for definitive diagnoses. Lastly, the epidemiologic criteria are as follows: those who have traveled to an at-risk area in the last 10 days, or have had close contact with a known case, or have had close contact with someone who traveled to an at-risk area in the last 10 days. Taken together, these criteria can establish a probable or confirmed case of SARS. Patients recently immigrated from areas where a risk for SARS exists should be screened clinically with these criteria in mind.
Table 1.
Clinical Criteria for Severe Acute Respiratory Syndrome (SARS)
| Stage | Criteria |
|---|---|
| Early | Two or more: fever (may be subjective), chills, rigors, myalgia, headache, diarrhea, sore throat, rhinorrhea |
| Mild-moderate | Temperature >38°C and cough, shortness of breath, or difficulty breathing |
| Severe | Pneumonia or acute respiratory distress syndrome (ARDS) or autopsy findings of either |
Medical evaluation
History
All children recently immigrated to the United States, whether with their biologic families or when adopted by an American family, should have complete history and physical and laboratory examinations performed on their arrival in the United States. In addition to past medical history, as much as can be ascertained, an important factor to determine is in what countries a newly arrived immigrant has been living. Immigrants often have lived as refugees or temporarily in various countries before coming to the United States, which may change their risk for acquisition of various infectious diseases. Many immigrants may experience a change in their economic status. Some immigrants, such as refugees from refugee camps or internationally adopted children, will experience an increase in their economic fortunes. Others, such as those immigrating to escape political pressure, may experience a decrease in their economic earning power. Such changes will affect their health status as well as their ability to access health care. Lastly, any change in caregivers should be noted. Children often are the last members of a family to immigrate and, hence, their parents may not be the most recent caregiver. If such is the case, attempts should be made to obtain a medical history for the interim period (between when the parents left the country of origin and when the child did).
With children being adopted internationally, the amount of past medical history available will vary. The accuracy of information provided varies as well. If parents are adopting from Russia, they may receive some medical information before meeting the child. If they are adopting from Ukraine, no information will be available before adoption, but some will be accessible at adoption. For Guatemala, brief reports of physician visits are available, but scant maternal history. South Korea often provides extensive medical records before adoption. A review of medical records from Eastern Europe found the following diagnoses: 68 percent with anemia, 41 percent with rickets, 11 percent with hip dysplasia, and 2 percent with prenatal exposure to alcohol.7 Of all the diagnoses made on medical forms, 6 to 24 percent were confirmed on arrival to the United States.17 Hence, all medical records should be reviewed with some amount of skepticism.
Immunizations
Few children immigrating to the United States will have received all of the immunizations currently recommended by the American Academy of Pediatrics (AAP), in part because many vaccines are not readily available in the developing world (ie, varicella or Prevnar). One study reviewed the records of 504 internationally adopted children and found that only 178 had immunization records before being adopted.18 Of these only 14 (9%) were up to date for all vaccines, according to the recommendations by AAP. Children from China were twice as likely to have incomplete records.18
When a child presents with a vaccine record, it should be evaluated first for acceptability. A record is consider acceptable if it includes the date of administration for each vaccine, if the interval between doses is adequate (for most vaccines at least one month), and if the child was the appropriate age when vaccinated. Records have been evaluated that showed vaccines given before the child’s date of birth—obviously rendering the entire record invalid! In other cases, vaccines may have been given when the child was younger than is recommended in the United States (ie, measles vaccine often is given when children are 9 months of age in endemic areas, as opposed to waiting until they are 1 year of age). In such cases, the particular vaccine may need to be repeated. If the record is thought to be acceptable and the child is older than 1 year of age, titers to confirm vaccination can be drawn. Care should be taken so that the appropriate tests are completed. For example, to confirm vaccination with hepatitis B, one must check a quantitative serum level, not just a qualitative value as seen with most acute hepatitis panels. If a child is younger than 1 year of age, vaccines should be repeated regardless of the records obtained. Titers measure the presence of antibodies, and maternal antibodies may cloud the issue in those younger than one year of age. The only caveat to repeating all vaccinations is that a child should not receive more than seven doses of diphtheria/tetanus before reaching 7 years of age.
Growth and developmental assessment
Several studies have shown that children residing in institutions will have growth delays. Researchers have estimated that for every 4 months spent in an institution, children will be 1 month delayed in all of their growth parameters (weight, height, and head circumference).19 Growth delays are present for several reasons. Children from developing nations, especially from refugee camps or institutions, often have suffered from malnutrition, leading to failure to thrive. Moreover, children may experience growth failure secondary to psychological trauma. Children who are not nurtured often will grow poorly. For children being adopted internationally, fetal alcohol syndrome or other congenital illnesses often can be an additional cause of failure to thrive. For infants, one expects that their head circumference will be preserved better than will be the other growth parameters. If it is not, one must look closely for other signs of developmental delay.
Developmental delay also is found very commonly in recently immigrated children. At least half of international adoptees have some form of developmental delay. A survey of 452 girls adopted from China found that 75 percent had some type of developmental delay and 44 percent had global developmental delay.20 All of these children were evaluated within 3 months of arriving in the United States. Many children will overcome their delays and by 1 year after adoption will have “caught up” with their peers. However, some will exhibit delays or isolated deficiencies for their entire lives.
Because of the overwhelming number of children with developmental delays, hearing and vision screening is recommended for all recent immigrants. Many children will have exaggerated speech delays; hence, any hearing loss should be excluded as a possible cause.
Some growth delay also may be attributable to inaccurate birth records. Often, both for children adopted internationally and for refugees or other immigrants, birth dates may be incorrect. Hence, a child may exhibit growth or developmental mismatching with their given date of birth. Most experts recommend observing the child for at least a year in the improved nutritional and stimulated environment. After that time, formal developmental assessment and radiographic bone age may help determine a child’s “true” age. Children should be placed in school according to their developmental level, with less regard for chronological age.
Laboratory examinations
Several laboratory examinations are recommended for newly immigrated children (Table 2). Screening for all of the infectious diseases discussed is recommended. Moreover, children should be rescreened for HIV, hepatitis B and C, and tuberculosis 6 months after arrival in the United States. Exposure to any of these diseases just before coming to the United States may be missed on the initial screening. Children also should be screened for syphilis. When reviewing medical records of children adopted internationally, 30 percent had a maternal history of syphilis and 0.3 to 1.6 percent showed signs of infection.7 In addition, screening for lead poisoning is recommended. Increased lead levels have been seen in children from various parts of the world. In Massachusetts, 693 recently immigrated children younger than the age of 7 years were evaluated for serum lead levels. Of these, 11.3 percent had elevated serum lead levels, twice as many as the U.S.-born controls.21 This disparity remained on follow-up, possibly because of continued exposure in older U.S. housing. Thyroid function testing often is recommended. Many children come with no medical history and growth failure. One should rule out other treatable causes for growth failure and not assume all failure is due solely to nutritional shortages. If a child’s family history is unknown, one may consider performing glucose-6-phosphate dehydrogenase assay and/or hemoglobin electrophoresis, depending on the country of origin.
Table 2.
Recommended Laboratory Examinations
| HIV |
| Hepatitis B/C |
| Syphilis |
| Tuberculin skin test |
| Intestinal parasites |
| Comprehensive metabolic panel |
| Complete blood count |
| Lead |
| Thyroid function tests |
Other issues
Often the most acute issues faced by recently immigrated children are infectious diseases. Over the course of time, these issues resolve and other problems arise. Many children have come from environments that leave a psychological mark on them. Those coming from war-torn areas or refugee camps may exhibit symptoms of posttraumatic stress disorder. Children who have spent their early months or years in an institution often have difficulties with attachment to caregivers or with the integration of sensory input. Many have been exposed to alcohol in utero and will have long-term mental and psychological consequences. These issues often are the ones that complicate a child’s adjustment to his or her new environment and require a physician’s assistance in finding appropriate resources.
Conclusion
Children recently immigrated to the United States come from a variety of backgrounds. Cultural differences can become a barrier to obtaining medical care. These children are at high risk for having many infectious diseases. Screening for these diseases, as well as having a high index of suspicion for unusual infectious agents, is important for establishing a proper diagnosis. Children adopted internationally are a rapidly growing group of children immigrating from overseas. Many of their issues are the same as those of other immigrants, but some are unique. Their caregivers may know very little about their past medical history. In addition, the growth and developmental effects of institutionalization can differ from those of other immigrants. Finally, all recently immigrated children are at risk for having adverse psychological effects resulting from their experiences before immigration, as well as from the difficulty of making the transition to a new culture. All of these issues render this population an interesting part of any pediatric practice.
References
- 1.United States Department of Homeland Security. 2002. Yearbook of Immigration Statistics Available at http://uscis.gov/graphics/shared/aboutus/statistics/IMM02yrbk/IMM2002list.htm; Internet; accessed January 11, 2005. [Google Scholar]
- 2.United States Department of State. Orphan Visa Statistics. Available at http://travel.state.gov/family/adoption_resources_02.html; Internet; accessed January 11, 2005.
- 3.Centers for Disease Control and Prevention. Immigration medical examination requirements. Available at http://www.cdc.gov/ncidod/dq/dsforms/; Internet; accessed January 11, 2005.
- 4.Jenista J.A. The immigrant, refugee, or internationally adopted child. Pediatr Rev. 2001;22:419–429. doi: 10.1542/pir.22-12-419. [DOI] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention. Lead Poisoning. http://www.cdc.gov/nceh/publications/Factbook2000/Default/htm; Internet; accessed January 11, 2005.
- 6.Pickering . 2000 Red Book: Report of the Committee on Infectious Diseases. 25th ed. American Academy of Pediatrics; Elk Grove Village, IL: 2000. LK Medical Evaluation in Internationally Adopted Children. [Google Scholar]
- 7.Saiman L., Aronson J., Zhou J. Prevalence of infectious diseases among internationally adopted children. Pediatrics. 2001;108:608–612. doi: 10.1542/peds.108.3.608. [DOI] [PubMed] [Google Scholar]
- 8.Centers for Disease Control Trends in Tuberculosis—United States, 1998–2003. MMWR. 2004;53:209–232. [PubMed] [Google Scholar]
- 9.World Health Organization. Fact sheet on hepatitis B. Available at www.who.int/mediacentre/factsheets/fs204/en; Internet; accessed January 11, 2005.
- 10.World Health Organization Fact sheet on hepatitis C. Available at: www.who.int/mediacentre/factsheets/fs164/en; Internet; accessed January 11, 2005.
- 11.Aronson, J HIV among internationally adopted children. Available at: http://www.orphandoctor.com/medical/general/hiv_infection.html; Internet; accessed January 11, 2005.
- 12.World Health Organization. Fact sheet on measles. Available at www.who.int/topics/measles/en; accessed January 11, 2005.
- 13.Centers for Disease Control and Prevention Measles outbreak among internationally adopted children arriving in the United States—February-March 2001. MMWR. 2002;51:1115–1116. [PubMed] [Google Scholar]
- 14.Centers for Disease Control and Prevention Update: multistate investigation of measles among adoptees from China—April 16, 2004. MMWR. 2004;53:1. [PubMed] [Google Scholar]
- 15.Bonthius D.J., Stanek N., Grose C. Subacute sclerosing panencephalitis, a measles complication, in an internationally adopted child. Emerging Infect Dis. 2000;6:377–381. doi: 10.3201/eid0604.000409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.World Health Organization. Cumulative number of SARS cases November 1 2002-July 31 2003. Available at http://www.who.int/csr/sars/country/en/; accessed January 11, 2005.
- 17.Aronson J. Medical evaluation and infectious considerations on arrival. Pediatr Ann. 2000;29:218–233. doi: 10.3928/0090-4481-20000401-07. [DOI] [PubMed] [Google Scholar]
- 18.Schulte J.M., Maloney S., Aronson J. Evaluating acceptability and completeness of overseas immunization records of internationally adopted children. Pediatrics. 2002;109:122. doi: 10.1542/peds.109.2.e22. [DOI] [PubMed] [Google Scholar]
- 19.Johnson D.E. Long-term medical issues in international adoptees. Pediatr Ann. 2000;29:234–241. doi: 10.3928/0090-4481-20000401-09. [DOI] [PubMed] [Google Scholar]
- 20.Miller L.C., Hendrie N.W. Health of children adopted from China. Pediatrics. 2000;105:e76. doi: 10.1542/peds.105.6.e76. [DOI] [PubMed] [Google Scholar]
- 21.Geltman P.L., Brown M.J., Cochran J. Lead poisoning among refugee children resettled in Massachusetts, 1995 to 1999. Pediatrics. 2001;108:158–162. doi: 10.1542/peds.108.1.158. [DOI] [PubMed] [Google Scholar]