

Abstract
Objectives
1) To compare the 2-year completed suicide and reattempt rates in a preintervention group of Hong Kong Chinese suicide attempters (aged 65 years and older) who received standard care and a postintervention group enrolled in a regional elderly suicide prevention program (ESPP) that adopts a two-tiered multifaceted care management model and 2) to examine the trend of suicide rates in older adults aged 65 years and older in the pre- and postintervention periods.
Design
The first part is an observational cohort study with baseline, follow-up, and outcome data being identified from a clinical electronic registry. The second part examines changes in suicide rates from official mortality statistics.
Setting
A government-funded suicide intervention program serving catchment population (852,796 people aged 65 years and older) in Hong Kong, China.
Participants
Suicide attempters (aged 65 years and older) presenting to old-age psychiatric service in the pre- and postintervention phases.
Measurements
1) Two-year rates of completed suicide and suicide reattempt and 2) changes in population suicide rates in the pre- and postintervention periods.
Results
The 2-year completed suicide rate was 7.58% in the preintervention group (N = 66) and 1.99$% in the ESPP group (N = 351) χ2 = 6.192; p value: 0.028; df = 1). Reattempt rates were not different. At a population level, suicide rate dropped significantly only in women aged 85 years and older, relative to the preintervention period.
Conclusions
The ESPP was associated with a reduced rate of completed suicide in old-age suicide attempters and might have contributed to a fall of suicide rate in women aged 85 years and older.
Key Words: Suicide, old-age, intervention
Suicide is one of the most important public health issues. Suicidal behavior has multiple causes, expressed as proximal stressors or predisposing factors. Psychiatric illness is a major contributing factor and more than 90% of suicides have a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Axis I psychiatric illness.1,2 Although suicide prevention strategies usually adopt a multifaceted or multilayered approach with particular attention to mental health, systematic review of suicide prevention strategies fails to demonstrate consistently the efficacy of suicide prevention programs because of heterogeneity in study methodology and populations.3 Among different intervention strategies used, collaborative care approaches and physician education in depression recognition and treatment have been found to be effective in lowering suicide rates across diverse sociocultural settings.4, 5, 6, 7, 8, 9, 10
Older adults, being the fastest growing population segment worldwide, are at greater risk for suicide than any other age groups.11,12 The United Nations recently estimated that the population older than 60 years will reach 1 billion, with 70% residing in developing countries, by 2020.13 Suicide attempts in later life are often of greater determination and lethality.14,15 Those who attempt and complete suicide in later life are driven by the same spectrum of risk factors such as depression, ill health, and solitary living arrangements.16,17 Aftercare for suicide attempts, ranging from telecare, issuance of an emergency contact card, intensive psychosocial follow-up, and video education plus family therapy, have produced mixed results and often no difference between standard aftercare and intervention groups in the rate of reattempt and reemerging suicidal ideation.18, 19, 20, 21, 22, 23, 24
ELDERLY SUICIDE PREVENTION PROGRAM
Hong Kong is a small but densely populated city at south China. As of mid-2008, the population of Hong Kong was 6.98 million. The population sector aged 65 years and older has been rising from 6.4% in 1980 to 12.6% in 2008. The suicide rate among older adults (aged 65 years and older) in Hong Kong is 2–3 times higher than younger age groups.25 An “Elderly suicide prevention program” (ESPP) was launched in October 2002 to serve all areas in Hong Kong through seven regional services. This program is directly funded and managed by the Hospital Authority, the only government-funded health management organization in Hong Kong. The ESPP adopts a multifaceted model (treatment of depression, gatekeeper training, aftercare for suicide attempters, and care management) operating at two levels. The first tier is predominantly primary care, and the second tier is the old-age psychiatric service at tertiary care level.
A typical referral pathway and aftercare are as follows: a gatekeeper in the first tier (primary care physicians, social workers, frontline healthcare workers and volunteers in elderly service, and nonpsychiatric specialists in tertiary care) identifies an at-risk case (clinically depressed or having suicidal ideation/plans/attempts) and makes urgent referral. Each client will then be assigned a care manager (psychogeriatric nurse in the second tier) who arranges an urgent psychogeriatric appointment (with or without domestic visit) within 1 week. At the psychogeriatric clinic designated psychogeriatricians provide the ass-essment and follow-up care as clinically indicated. A care manager offers frequent phone contacts, regular home visits (usually biweekly or triweekly), and ad hoc home visits (in response to crisis) to monitor the client's mental and social situations, promote compliance with treatment, and provide psychoeducation in the first 6 months. The care manager liaises with other caregivers (both professional and nonprofessional) by phone contacts. ESPP clients are also given the emergency contacts of their care managers. A multidisciplinary team (consists of psychogeriatricians, care managers, and medical social workers ± occupational therapists) at tertiary care level holds regular case conferences to review the care plan and clinical progress.
This study primarily aims at examining the program effectiveness by comparing the 2-year suicide and reattempt rates of a subpopulation of ESPP clients, i.e., suicide attempters enrolled in ESPP from October 2002 to May 2007 and a preintervention historical cohort of elderly suicide attempters from 2001 to 2002. We also compare the sociodemographic and clinical characteristics of the ESPP cohort with the preintervention cohort with a view to eliciting plausible factors associated with the difference in 2-year suicide rates and reattempt rates.
As a secondary objective, we evaluate the possible effect of ESPP on elderly suicide rates at the population level by examining the trends of suicide rates in older adults in the pre- and postintervention periods in Hong Kong.
METHODS
Component 1—Two-Year Outcomes of Suicide Attempters Aged 65 Years and Older in the Pre-and Postintervention Groups
The first part compared the 2-year suicide rates and reattempt rates of the two cohorts of older adults (aged 65 years and older) with an index suicide attempt, presenting to psychogeriatric specialist care provided by the same healthcare administration (Hospital Authority of Hong Kong) in two consecutive time frames. There are two reasons for limiting the follow-up period to 2 years. First, the last subject in the intervention group was enrolled by the end of May 2007, and the data analysis of this study was performed at the end of May 2009. Hence, 2-year follow-up permits maximal inclusion of subjects in the intervention arm. The second reason being that completed suicides mostly likely occur in the first 1–2 years after an index attempt among older adults in Hong Kong, based on a 4.5-year naturalistic follow-up study on late-life suicide attempters presented to a district level hospital service in Hong Kong from 1990 to 1994.26
Subjects and Intervention
The intervention group was selected from 2,290 older adults (aged 65 years and older) enrolled in the ESPP from October 2002 to May 2007. As an early intervention program, the ESPP cohort includes a range of at-risk older adults without making an index suicide attempt at intake. ESPP clients without index suicide attempt were thus not included in our data analysis as our comparison subjects from the preintervention phase were all suicide attempters. From this cohort, there were 351 suicide attempters included as the intervention group. The intervention group received intensive care management as detailed in the introductory section. The intensive care management phase lasts for 6 months, but the aftercare component by psychogeriatrician is continued as clinically indicated.
The preintervention group was made up of a historical cohort from another study on late-life suicide.17 This group consisted of 66 suicide attempters aged 65 years and older who consecutively presented to a regional (namely the “New Territories East Cluster”[NTEC]) psychogeriatric consultation-liaison service and prospectively enrolled in a study during 2001–2002, shortly before the inception of ESPP. The NTECs regional mental health service serves a catchment area that hosts about one-fifth of the total population. In the preintervention period, all suicide attempters aged 65 years and older seeking help at publicly funded hospitals at NTEC were referred to psychogeriatric consultation-liaison services. With exception to NTEC, there was no database that systematically archived baseline clinical information of late-life suicide attempters presenting to other regional services in the preintervention phase. Suicide attempters presenting to other regional services during the preintervention phase were thus not included. Subjects in the preintervention group received standard psychogeriatric care (both outpatient and inpatient) after an index suicide attempt. In the preintervention phase, the standard psychogeriatric service was well equipped with multidisciplinary support from psychiatric inpatient/daycare facilities. The preintervention service was different from the ESPP in two aspects: 1) having no liaison with community gatekeepers and 2) lacking care management component and the multidisciplinary care planning and review meetings.
Measurements
Baseline variables include the following:
-
i
Sociodemographic profile (age, *sex, *marital status, *living arrangement, *financial support from social security system, and *educational level).
-
ii
Clinical variables (*current diagnosis of unipolar major depressive disorder by International Classification of Diseases, Tenth revision, [ICD-10] obtained by unstructured clinical interview, *score on Geriatric Depression Scale [GDS] at intake, with the local cutoff being г8).27, 28, 29
-
iii
Suicide behavior profile (method used for index attempt, *index attempt requiring hospitalization, and *history of suicide attempt not including the index attempt).
Variables on process indicators during the 2-year follow-up after an index attempt include the following:
-
i
Duration of psychogeriatric service contact.
-
ii
*Antidepressant prescription for 6 weeks or more after index attempt.
-
iii
Duration of antidepressant prescription.
-
iv
*Noncompliance with treatment defined as dropout from outpatient care for more than 3 months since index attempt or loss to follow-up since first contact.
The outcome variables are as follows:
-
i
*Completed suicide.
-
ii
*Repeat suicide attempt(s) defined as self-inflicted injury or poisoning under ICD-10 codes of intentional self-harm: X60–X84.
All dichotomous variables are denoted by asterisk (*).
Data Acquisition
For both groups, we retrieved the baseline and follow-up data on the clinical and sociodemographic variables from the computerized clinical database owned and managed by the Hospital Authority. Intention-to-treat principles were adopted throughout the process of data acquisition and data analysis. Hence, this study included subjects with history of noncompliance with treatment (defined as dropout from outpatient care for more than 3 months since index attempt or loss to follow-up since first contact). The key outcome status (completed suicide) was ascertained by searching the Hospital Authority's clinical database and verifying with the official data (Coroner's record).
Data Analysis
In the primary analyses, we compared the baseline variables, process indicators, and outcome variables of the ESPP and preintervention groups. Independent t-tests were used for continuous variables and χ2 statistics (or Fisher's exact test) for categorical variables. Subgroup analyses were then performed to compare the outcome variables in subjects selected by baseline variables and process indicators that were shown to be significantly different between the two groups in the primary analyses. As the two groups were not matched on baseline characteristics, Poisson regression models were fitted to test the independent effects of baseline variables, intervention group and “Group-by-baseline variable” interaction on completed suicide. All statistical tests were performed using SPSS 17.0.
Component 2—Analysis of Population Mortality Statistics
Measurements and Data Acquisition
In the second part of the study, the number of suicides in older adults (aged 65 years and older) from 1986 to 2007 were retrieved from the Hong Kong Government's mortality statistics (Census and Statistics Department) that were reliably derived from the Coroner's Court. The Coroner's Court is responsible for judicial enquiries into all suspected suicide deaths occurring in Hong Kong. Deaths with a final verdict of “undetermined cause” were excluded from analysis. Age-specific suicide rates were derived by dividing the number of deaths by mid-year population of the specific age group of concern (as determined by the Government's Census and Statistics Department) in the respective years, multiplied by 100,000.
Statistical Analysis
Poisson regressions were then applied to model and estimate the “Period” effect on suicide rates in the selected age group. We performed separate analyses on young-old (65–84 years) and old-old (85 years and older). Indicator variables were created for “Period” (one for each year 1986–2007). Separate models were fitted for men and women to estimate the incident risk ratios (IRRs) of suicide rate of each calendar period relative to the reference category (Period 2002). All statistical tests were performed using SPSS 17.0.
Ethical Approval
Ethical approval of the research protocol was obtained from local institutional review boards under different regional Clinical Research Ethics Committees (The Chinese University of Hong Kong [CUHK]/Clinical Research Ethics Committee [NTEC-CREC]; University of Hong Kong [HKU]/Hospital Authority [HA] Hong Kong West [HKW] Institutional Review Board [IRB]; Research Ethic Committee [REC]/Kowloon Central [KC-KE], KWC-CREC; and Hong Kong East Cluster Ethics Committee [HKEC-EC]).
RESULTS
Component 1—Two-Year Outcomes of Suicide Attempters Aged 65 Years and Older in Pre- and Postintervention Groups
Table 1 shows the comparisons of the preintervention group (N = 66) and the ESPP cohort (N = 351) on baseline variables, process indicators, and outcome variables.
TABLE 1.
Comparison of Baseline Variables, Process Indicators, and Outcome Variables
| Preintervention Group (N = 66) | ESPP Group (N = 351) | Test Statistics | p | |
|---|---|---|---|---|
| Baseline variables | ||||
| Age (SD) | 75.48 (6.907) | 76.87 (8.039) | t = −1.308a | 0.192 |
| Sex (%) | ||||
| Male | 24 (36.4) | 150 (42.7) | χ2 = 0.927b | 0.336 |
| Female | 42 (63.6) | 201 (57.3) | ||
| Marital status (%) | ||||
| Married | 24 (36.4) | 155 (44.2) | χ2 =1.653b | 0.199 |
| Unmarried | 42 (63.6) | 190 (54.1) | ||
| Missing data | 0 (0) | 6 (1.7) | ||
| Living alone (%) | ||||
| Yes | 15 (22.7) | 31 (8.8) | χ2 = 10.929b | 0.001 |
| No | 51 (77.3) | 320 (91.2) | ||
| Financial support from social security system (%) | ||||
| Yes | 27 (40.9) | 120 (34.2) | χ2 =1.099b | 0.294 |
| No | 39 (59.1) | 231 (65.8) | ||
| Educational level (%) | ||||
| Primary or below | 58 (87.9) | 299 (85.2) | χ2 = 0.225b | 0.636 |
| Secondary or above | 8 (12.1) | 50 (14.2) | ||
| Missing data | 0 (0) | 2 (0.6) | ||
| Current diagnosis of depressive disorder (ICD-10) (%) | ||||
| Yes | 45 (68.2) | 170 (48.4) | χ2 =8.675b | 0.003 |
| No | 21 (31.8) | 181 (51.6) | ||
| Score on Geriatric Depression Scale (%) | ||||
| Below cutoff (<8) | 14 (21.2) | 132 (37.6) | χ2 =6.563b | 0.010 |
| At or above cutoff (≥8) | 52 (78.8) | 219 (62.4) | ||
| History of suicide attempt (excluding index attempt) (%) | ||||
| Yes | 24 (36.4) | 70 (19.9) | χ2 =8.579b | 0.003 |
| No | 42 (63.6) | 281 (80.1) | ||
| Method of index suicide attempt (%) | ||||
| Drug overdose + ingestion of nondrugs | 26 (39.4) | 99 (28.2) | χ2 =4.500c | 0.343 |
| Jumping from heights | 14 (21.2) | 71 (20.2) | ||
| Hanging | 7 (10.6) | 48 (13.7) | ||
| Stabbing/wrist laceration | 5 (7.6) | 47 (13.4) | ||
| Others | 14 (21.2) | 86 (24.5) | ||
| Index attempt requiring hospitalization (%) | ||||
| Yes | 46 (69.7) | 228 (65) | χ2 = 0.554b | 0.457 |
| No | 20 (30.3) | 123 (35) | ||
| Process indicators | ||||
| Duration of psychogeriatric service contact/months (SD) | 19.55 (7.181) | 18.67 (8.065) | t = 0.734d | 0.464 |
| Antidepressant prescriptions after index attempt (= 6 weeks) (%) | ||||
| Yes | 46 (69.7) | 276 (78.6) | χ2 =2.521b | 0.112 |
| No | 20 (30.3) | 75 (21.4) | ||
| Duration of antidepressant prescriptions/months (SD) | 14.06 (10.861) | 15.37 (10.227) | t = −0.918e | 0.359 |
| History of noncompliance with treatment (%) | ||||
| Yes | 22 (33.3) | 62 (17.7) | χ2 =8.480b | 0.004 |
| No | 44 (66.7) | 289 (82.3) | ||
| Outcome variables | ||||
| Repeat suicide attempt (%) | 7 (10.61) | 35 (9.97) | χ2 = 0.025b | 0.875 |
| Completed suicide (%) | 5 (7.58) | 7 (1.99) | χ2 =6.192b | 0.028f |
Notes: SD: standard deviation.
t test with df = 415.
χ2 test with df = 1.
χ2 test with df = 4.
t test with df = 352.
t test with df = 407.
Fisher's exact test.
In terms of the baseline variables, there were significantly more people living alone but more having GDS г8 (at or above the local cutoff score) in the preintervention group. The percentage that had an ICD-10 diagnosis of depressive disorder and a prior suicide attempt (not including the index attempt) was also significantly higher in the preintervention group. The two groups were not significantly different on other baseline variables. As for the process indicators, older adults in the preintervention group had a higher frequency of service dropout during the 2-year follow-up period. Two-year suicide rate was 7.58% (number of suicide deaths = 5) in the preintervention group and 1.99% (number of suicide deaths = 7) in the ESPP cohort (χ2 = 6.192; p value = 0.028, df = 1). The 2-year reattempt rates were not significantly different from each other between the two groups.
Table 2 presents the results of subgroup analyses examining differences in the two main outcomes (completed suicide and repeat suicide attempts) between the ESPP and preintervention groups. Significantly higher rates of completed suicide were observed in the preintervention group among subjects with an apparent low-risk profile, i.e., GDS below cutoff score at intake or those with history of treatment compliance. For the relatively high-risk group who required hospitalization for index attempt, the 2-year rate of completed suicide was significantly higher in the preintervention group. Trend toward higher suicide rates in the preintervention group was seen in subjects selected by male gender. On the other hand, the subgroup analyses showed no significant differences in the frequency of repeat suicide attempts between the two groups.
TABLE 2.
Subgroup Analyses—Differences in 2-Year Rates of Completed Suicide Between the Preintervention Group and ESPP Group Selected by Baseline Variables and Process Indicators
| Preintervention Group | ESPP Group | Test Statistics | p | |
|---|---|---|---|---|
| Baseline variables | ||||
| Male | (N = 24) 3 (12.5%) | (N = 150) 4 (2.67%) | χ2 = 5.181a | 0.056b |
| Female | (N = 42) 2 (4.76%) | (N = 201) 3 (1.49%) | χ2 = 1.843a | 0.207 |
| Living alone | (N = 15) 1 (6.67%) | (N = 31) 2 (6.45%) | χ2 = 0.001a | 1.000b |
| History of suicide attempt | (N = 24) 1 (4.17%) | (N = 70) 2 (2.86%) | χ2 = 0.099a | 1.000b |
| Current diagnosis of depressive disorder (ICD-10) | (N = 45) 3 (6.67%) | (N = 170) 4 (2.35%) | χ2 = 2.102a | 0.161b |
| Index attempt requiring hospitalization | (N = 46) 5 (10.87%) | (N = 228) 6 (2.63%) | χ2 = 6.741a | 0.023b |
| Score on Geriatric Depression Scale below cutoff (<8) | (N = 14) 3 (21.43%) | (N = 132) 3 (2.27%) | χ2 = 11.786a | 0.012b |
| Score on Geriatric Depression Scale at or above cutoff (≥8) | (N = 52) 2 (3.85%) | (N = 219) 4 (1.83%) | χ2 = 0.792a | 0.325b |
| Process indicators | ||||
| History of noncompliance with treatment | (N = 22) 2 (9.09%) | (N = 62) 4 (6.45%) | χ2 = 0.171a | 0.650b |
| Compliance with treatment | (N = 44) 3 (6.82%) | (N = 289) 3 (1.04%) | χ2 = 7.211a | 0.032b |
χ2 test with df = 1.
Fisher's exact test.
Table 3 presents six Poisson regression models testing the independent effects of intervention group and the respective baseline variables on completed suicide. For each model, an interaction term (group-by-baseline variable) was fitted to test whether it made significant contribution to the outcome prediction. The respective interaction terms were removed from the final models because the relative risks failed to reach significance level. In the final models, only “group” remained as significant outcome predictor. All Poisson regression models demonstrated a significant reduction in relative risk for completed suicide in the ESPP group relative to the preintervention group.
TABLE 3.
Poisson Regressions—Independent Effects of Intervention Group, Baseline Variable, and “Group-by-Baseline Variable” Interaction on Outcome (Completed Suicide)
| Independent Variables (Group and Gender) | p | RR (95% CI) ESPP/Preintervention Group | p | RR (95% CI) Female/Male | p | RR (95% CI) Group × Gender (Interaction) |
|---|---|---|---|---|---|---|
| Model 1 | ||||||
| Asymptotic model: with interaction term | 0.043a | 0.213 (0.048–0.953) | 0.290a | 0.381 (0.064 – 2.280) | 0.747a | 1.469 (0.143–15.143) |
| Asymptotic model: removing interaction term | 0.018a | 0.251 (0.079–0.792) | 0.206a | 0.476 (0.151 – 1.504) | ||
| Independent Variables (Group and Living Arrangement) | ESPP/Preintervention Group | Living Alone: Yes/No | Group × Living Alone (Interaction) | |||
| Model 2 | ||||||
| Asymptotic model: with interaction term | 0.016a | 0.199 (0.053–0.742) | 0.884a | 0.850 (0.095–7.605) | 0.258a | 4.858 (0.315–75.001) |
| Asymptotic model: removing interaction term | 0.044a | 0.297 (0.091–0.969) | 0.309a | 2.011 (0.524–7.721) | ||
| Independent Variables (Group and GDS Below Cutoff) | ESPP/Preintervention Group | GDS < 8: Yes/No | Group × GDS <8 (Interaction) | |||
| Model 3 | ||||||
| Asymptotic model: with interaction term | 0.390a | 0.475 (0.087–2.593) | 0.060a | 5.571 (0.931–33–343) | 0.208a | 0.223 (0.022–2.302) |
| Asymptotic model: removing interaction term | 0.013a | 0.225 (0.070–0.726) | 0.154a | 2.317 (0.731–7.346) | ||
| Independent Variables (Group and History of Suicide Attempt) | ESPP/Preintervention Group | History of Suicide Attempt: Yes/No | Group × History of Suicide Attempt (Interaction) | |||
| Model 4 | ||||||
| Asymptotic model: with interaction term | 0.012a | 0.187 (0.050–0.696) | 0.460a | 0.438 (0.049–3–914) | 0.352a | 3.670 (0.238–56.667) |
| Asymptotic model: removing interaction term | 0.023a | 0.259 (0.081–0832) | 0.887a | 0.908 (0.241–3–428) | ||
| Independent Variables (Group and ICD-10 Depressive Disorder) | ESPP/Preintervention Group | Current Diagnosis of Depressive Disorder (ICD-10): Yes/No | Group × Current Diagnosis of Depressive Disorder (ICD-10) (Interaction) | |||
| Model 5 | ||||||
| Asymptotic model: with interaction term | 0.055a | 0.174 (0.029–1.042) | 0.696a | 0.700 (0.117–4.189) | 0.552a | 2.028 (0.197–20.903) |
| Asymptotic model: removing interaction term | 0.027a | 0.267 (0.083–0.860) | 0.905a | 1.074 (0.333–3–460) | ||
| Independent Variables (Group and Index Attempt Requiring Hospitalization) | ESPP/Preintervention Group | Index Attempt Requiring Hospitalization: Yes/No | Group × Index Attempt Requiring Hospitalization (Interaction) | |||
| Model 6 | ||||||
| Asymptotic model: with interaction termb | — | — | — | — | — | — |
| Asymptotic model: removing interaction term | 0.029a | 0.278 (0.088–0.875) | 0.105a | 5.449 (0.703–42.245) | ||
Notes: RR: relative risk (e.g., RR of ESPP/preintervention group = risk for completed suicide when exposed to ESPP group relative to exposure to preintervention group); group: intervention group (ESPP versus preintervention group); CI: confidence interval.
p values are from Poisson regression with df = 1.
Relative risk and p value could not be calculated as Hessian matrix singularity was caused by parameter.
Component 2—Analysis of Population Mortality Statistics
Figure 1 shows the graphical presentation of suicide rates in older adults aged 85 years and older from 1986 to 2007. Age-specific IRRs for suicide mortality by year of death for male and female were shown in Table 4 , with 2002 being the year of reference. Among women aged 85 years and older, the IRRs for suicide mortality in 1986–2001 (with exceptions to 1995, 1999, and 2000) were significantly higher by approximately 2–4-fold than the reference year, whereas IRRs in 2003–2007 were not significantly different from 2002. Hence, a steady trough level was not seen in women aged 85 years and older until 2002 onward. On the other hand, we found no consistently significant downward trend of suicide rates in men aged 85 years and older during 1986–2007.
Figure 1.
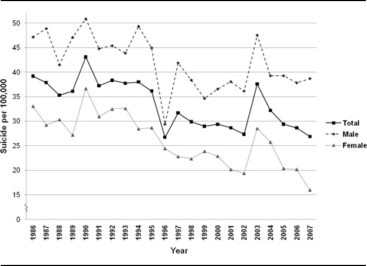
Suicide Rates in Old-Olds (85 Years and Older) in Hong Kong (1986–2007)
TABLE 4.
Poisson Regression—Incident Risk Ratios for Suicide Mortality by Year of Death (1986–2007) in Old-Olds (Aged 85 Years and Older) With 2002 Being the Year of Reference
| Women |
Men |
|||
|---|---|---|---|---|
| Year | IRR | p,a2*1 Sided | IRR | p,a2*1 Sided |
| 1986 | 4.6154 | 0.0001 | 1.8542 | 0.2057 |
| 1987 | 3.3152 | 0.0009 | 1.3520 | 0.5626 |
| 1988 | 2.7766 | 0.0056 | 1.9229 | 0.1401 |
| 1989 | 2.7993 | 0.0047 | 0.8778 | 0.8182 |
| 1990 | 2.7872 | 0.0049 | 1.8669 | 0.1440 |
| 1991 | 2.7391 | 0.0062 | 2.2210 | 0.0477 |
| 1992 | 3.7573 | 0.0001 | 1.2771 | 0.5972 |
| 1993 | 2.2621 | 0.0288 | 0.8055 | 0.6780 |
| 1994 | 2.9254 | 0.0022 | 0.5881 | 0.3491 |
| 1995 | 1.9803 | 0.0673 | 1.5940 | 0.2360 |
| 1996 | 2.1853 | 0.0299 | 0.8346 | 0.6962 |
| 1997 | 2.2693 | 0.0202 | 1.1984 | 0.6534 |
| 1998 | 2.3915 | 0.0120 | 1.7557 | 0.1240 |
| 1999 | 1.0960 | 0.8230 | 0.5186 | 0.2075 |
| 2000 | 1.3864 | 0.3886 | 1.2077 | 0.6241 |
| 2001 | 1.9964 | 0.0447 | 0.2318 | 0.0216 |
| 2003 | 1.0774 | 0.8441 | 0.9593 | 0.9124 |
| 2004 | 1.2823 | 0.4897 | 1.5906 | 0.1644 |
| 2005 | 1.1296 | 0.7379 | 1.0606 | 0.8689 |
| 2006 | 1.1501 | 0.6946 | 1.1689 | 0.6480 |
| 2007 | 0.5323 | 0.1338 | 1.2825 | 0.4530 |
p values are from Wald χ2 tests with df = 1.
Figure 2 shows the graphical presentation of suicide rates in adults aged 65–84 years from 1986 to 2007. Age-specific IRRs for suicide mortality by year of death for male and female are shown in Table 5 , with 2002 being the year of reference. For women in this age group, IRRs were significantly higher than the reference year by 41%–90% in 1986–1995. The IRRs in 1996–2001 did not deviate significantly from 2002, indicating a steady trough level was reached in 1996– 2002. The IRR in 2003 was significantly higher than the reference year by 47% and then returned to trough level comparable with the reference year (2002) in 2004–2007. As for men aged 65–84 years, IRRs in most of the years during 1986–2007 were not significantly higher than the reference year with exceptions to 1987, 1989, 1990, 1994, and 2003, suggesting that suicide rates in men aged 65 years and older did not follow any statistically meaningful downward trend.
Figure 2.
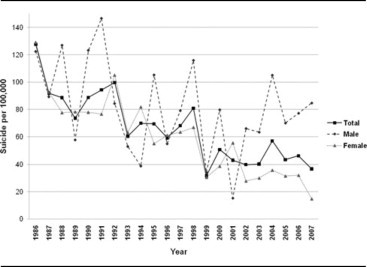
Suicide Rates in Young-Olds (65–85 Years) in Hong Kong (1986–2007)
TABLE 5.
Poisson Regression—Incident Risk Ratios for Suicide Mortality by Year of Death (1986–2007) in Young-Olds (Aged 65–84 Years) With 2002 Being the Year of Reference
| Women |
Men |
|||
|---|---|---|---|---|
| Year | IRR | p,a 2*1 Sided | IRR | p,a2 *1 Sided |
| 1986 | 1.7093 | 0.0012 | 1.3048 | 0.0624 |
| 1987 | 1.5105 | 0.0147 | 1.3524 | 0.0303 |
| 1988 | 1.5676 | 0.0070 | 1.1481 | 0.3389 |
| 1989 | 1.4050 | 0.0460 | 1.3029 | 0.0546 |
| 1990 | 1.8958 | 0.0001 | 1.4071 | 0.0105 |
| 1991 | 1.5996 | 0.0038 | 1.2389 | 0.1164 |
| 1992 | 1.6785 | 0.0012 | 1.2559 | 0.0903 |
| 1993 | 1.6858 | 0.0009 | 1.2138 | 0.1487 |
| 1994 | 1.4701 | 0.0167 | 1.3653 | 0.0152 |
| 1995 | 1.4806 | 0.0138 | 1.2439 | 0.0924 |
| 1996 | 1.2625 | 0.1514 | 0.8125 | 0.1446 |
| 1997 | 1.1774 | 0.3207 | 1.1591 | 0.2490 |
| 1998 | 1.1539 | 0.3841 | 1.0619 | 0.6432 |
| 1999 | 1.2330 | 0.1934 | 0.9582 | 0.7468 |
| 2000 | 1.1812 | 0.3039 | 1.0115 | 0.9297 |
| 2001 | 1.0407 | 0.8100 | 1.0530 | 0.6850 |
| 2003 | 1.4735 | 0.0108 | 1.3154 | 0.0218 |
| 2004 | 1.3302 | 0.0649 | 1.0865 | 0.5035 |
| 2005 | 1.0517 | 0.7562 | 1.0862 | 0.5037 |
| 2006 | 1.0419 | 0.8004 | 1.0465 | 0.7147 |
| 2007 | 0.8234 | 0.2579 | 1.0708 | 0.5781 |
p values are from Wald χ2 tests with df = 1.
DISCUSSION
Limitations
Our results should be interpreted considering the following methodological limitations. For instance, use of historical cohort does not permit adequate control for particular baseline characteristics as in randomized controlled trials. In a publicly funded suicide intervention program that is intended for all in the city, it is impossible to have a contemporary control group receiving “care as usual.” Under the “one-country, two-systems” administrative schema in China, socially compatible cities for comparison are virtually nonexistent. In this study, more often older people in the preintervention cohort were di-agnosed to have ICD-10 depressive disorder, living alone, and had history of previous suicide attempt, all well-known risk factors for suicide. Also, all pre-intervention subjects were referred from the inpatient consultation-liaison service, whereas some subjects in the intervention groups were referred from community gatekeepers. These uncontrolled baseline factors might account partly for the difference in the 2-year suicide rates. However, we found the “groupby-baseline variable” interactions were insignificant in Poisson regression models, whereas only intervention group remained significant predictor for completed suicide. The degrees of underreporting of suicide reattempt in the 2-year follow-up period for both groups were also uncertain, because it remained inevitable in both pre- and postintervention phases that suicide attempts not requiring any clinical attention at the publicly funded healthcare system were more likely to be missed. On the other hand, underreporting of completed suicide was less likely as the “caseness” was ascertained by standard judicial procedure.
Effectiveness of ESPP in Preventing Completed Suicide or Repeat Attempt in Late-Life Suicide Attempters
The 2-year suicide mortality (but not reattempt rate) in the ESPP group was significantly lower than a preintervention cohort. The lack of significant “group-by-baseline variable” interaction in the subgroup analyses suggested that the difference in suicide mortality was unlikely due to the uncontrolled baseline characteristics. The observation leads us to ask the following: 1) What is/are the specific factor(s) or service component(s) that account for the reduced rate of completed suicide in the ESPP group? and 2) Beyond the high-risk population, does the current evidence support that the ESPP is effective at the population level?
Specific Service Component(s) that Account for Decreased Rate of Completed Suicide in the ESPP Group
The active components of ESPP are combinations of treatment of depression, gatekeeper training, and aftercare for suicide attempters using a community-oriented psychiatric care management model. A number of ecological studies have demonstrated the association of increased antidepressant use with fewer completed suicides based on national registry and population statistics.30,31 Such association was selectively observed in older adults in an Australian study in which the association was in the opposite direction for adolescents.32 In this study, it was shown that the rate of antidepressant prescription in the ESPP group was comparable with the preintervention group, but the service dropout rate was significantly higher in the preintervention group. Care management might have provided continuity of care and reliable timely delivery of effective treatment components.
Higher prevalence of previous suicide attempt might confound the association between higher rate of completed suicide and the preintervention group. However, this observation might indirectly support that ESPP is more accessible and assertive than the standard psychogeriatric service. The assertive nature of the ESPP might have offered early intervention for at-risk older people well before they decompensate to a perisuicidal state. It is also interesting to note that higher suicide rate among older people with an apparently low-risk profile, i.e., scoring below cutoff on the GDS, and being compliant with treatment in the preintervention phase. This possibly means that ESPP is more receptive to the needs of these apparently low-risk older people.
Potential Implications for Suicide Prevention in Later Life at the Population Level
We could not demonstrate a clear-cut reduction of elderly suicide rates in the postintervention phase as our society has been taking graduated steps to develop elderly health and social welfare service infrastructure before implementing the ESPP. Also, the lack of reliable local prevalence data on depressive disorder in this age group precludes the estimation of the percentage of depressed older adults reached by this program.
A significant fall in suicide rates at the population level among women aged 65–84 years was seen in the preintervention phase against the background that suicide rate was on a steep rise in people younger than 65 years.33,34 The unusual peaks of suicide rates among older adults in 2003 and 2004 should be interpreted in the context of the severe acute respiratory syndrome (SARS) epidemic, which caused suspension of regular mental health services from April to June in 2003. We have reported that excess elderly suicides in April 2003 coincided with the peak of incident SARS cases.34 Hence, the temporary suspension of healthcare services and the concurrent upsurge in elderly suicide rates lend support to the reversibility of the effect of the standard old-age psychiatric services. It was speculated that the aftermath effects of SARS such as mass pessimism and fear of the epidemic returning were carried through 2004, accounting for the relatively high suicide rates in older adults that year.35
Our Poisson regression analysis showed that a steady trough level of suicide rates among old-old women (aged 85 years and older) was not reached until 2002. This observation suggests that ESPP (in place since 2002) may offer added benefit to the old-old adults who would not seek help from the standard psychogeriatric service. We speculate that the gatekeeper training component of the ESPP has resulted in better recognition of depressive illness and enhanced access of the service to the at-risk old-old women. Our study showed that 20% of ESPP clients were aged 85 years and older, compared with 10% of the preintervention cohort.
The gender difference in trend of suicide rates at the population level among older adults is intriguing. The social reforms and the availability of psychogeriatric service may have had an effect on reducing suicide risk preferentially in women. Earlier studies conducted in Gotland, Sweden, and Padua, Italy, showed that the effect of community-based suicide prevention for older people was specific to women.7,36 Recent studies of community-based interventions in rural Japan also observed that older women were more receptive to suicide prevention programming.37 The latest service statistics of the ESPP shows that more than half of the clients are women, indicating that at risk older men remain elusive to a two-tieredassertive care management model enhanced with gatekeeper training component. Future service provision should incorporate effective means to reach the high-risk older men. These measures might include strengthening the gate-keeping mechanisms in different sectors (non-goverment organizations [NGOs], social welfare sector, and primary care). Future studies should address the help-seeking behavior and barriers to healthcare among older men in our community, which in turn might inform innovative ways to engage this elusive risk group.
CONCLUSIONS
The ESPPs two-tiered multifaceted care management model was associated with a reduced rate of completed suicide in a high-risk group of old-age suicide attempters. This model might have contributed to better treatment compliance than standard care, which in turn resulted in better clinical outcome. Ecological data also suggest that the ESPP may be more effective in reaching the needs of old-old women (85 years and older) than standard psychogeriatric care probably by way of gatekeeper training and enhanced access to service.
Footnotes
The authors thank all the psychogeriatricians and case managers of the ESPP for their dedication to patient care and upkeeping the clinical database for all these years since the inception of the ESPP. The authors also thank Mr. Tony Leung for his advice on statistical analysis and Miss. Catherine Li and Miss Corine Wong for retrieving and cleaning the dataset.
References
- 1.Barraclough B, Bunch J, Nelson B. A hundred cases of suicide: clinical aspects. Br J Psychiatry. 1974;125:355–373. doi: 10.1192/bjp.125.4.355. [DOI] [PubMed] [Google Scholar]
- 2.Cavanagh JT, Carson AJ, Sharpe M. Psychological autopsy studies of suicide: a systematic review. Psychol Med. 2003;33:395–405. doi: 10.1017/s0033291702006943. [DOI] [PubMed] [Google Scholar]
- 3.Mann JJ, Apter A, Bertolote J. Suicide prevention strategies: a systematic review. JAMA. 2005;294:2064–2074. doi: 10.1001/jama.294.16.2064. [DOI] [PubMed] [Google Scholar]
- 4.Bruce ML, Ten Have TR, Reynolds CF., III Reducing suicidal ideation and depressive symptoms in depressed symptoms in depressed older primary care patients: a randomized controlled trial. JAMA. 2004;291:1081–1091. doi: 10.1001/jama.291.9.1081. [DOI] [PubMed] [Google Scholar]
- 5.Asarnow JR, Jaycox LH, Duan N. Effectiveness of a quality improvement intervention for adolescent depression in primary care clinics: a randomized controlled trial. JAMA. 2005;293:311–319. doi: 10.1001/jama.293.3.311. [DOI] [PubMed] [Google Scholar]
- 6.Pfaff JJ, Acres JG, McKelvey RS. Training general practitioners to recognize and respond to psychological distress and suicidal ideation in young people. Med J Aust. 2001;174:222–226. doi: 10.5694/j.1326-5377.2001.tb143241.x. [DOI] [PubMed] [Google Scholar]
- 7.Rutz W, von Knorring L, Wlinder J. Frequency of suicide on Gotland after systematic postgraduate education of general practitioners. Acta Psychiatr Scand. 1989;80:151–154. doi: 10.1111/j.1600-0447.1989.tb01318.x. [DOI] [PubMed] [Google Scholar]
- 8.Rutz W. Preventing suicide and premature death by education and treatment. J Affect Disord. 2001;62:123–129. doi: 10.1016/s0165-0327(00)00356-6. [DOI] [PubMed] [Google Scholar]
- 9.Szanto K, Kalmar S, Hendin H. A suicide prevention program in a region with a very high suicide rate. Arch Gen Psychiatry. 2007;64:914–920. doi: 10.1001/archpsyc.64.8.914. [DOI] [PubMed] [Google Scholar]
- 10.Takahashi K, Naito H, Morita M. Suicide prevention for the elderly in Matsunoyama Town, Higashikubiki County, Niigata Prefecture: psychiatric care for elderly depression in the community (in Japanese) Seishin Shinkeigaku Zasshi. 1998;100:469–485. [PubMed] [Google Scholar]
- 11.Stevens JA, Hasbrouck LM, Durant TM. Surveillance for injuries and violence among older adults. MMWR CDC Surveill Summ. 1999;48:27–50. [PubMed] [Google Scholar]
- 12.World Health Organization . Figures and Facts About Suicide. Mental and Behavioral Disorders. Department of Mental Health, World Health Organization; Geneva, Switzerland: 1999. [Google Scholar]
- 13.United Nations Population Division/DESA . World Population to Exceed 9 Billion by 2050: Developing Countries to Add 2.3 Billion Inhabitants With 1.1 Billion Aged Over 60 Years and 1.2 Billion of Working Age. [Press release] United Nations Population Division/DESA; New York: March 11, 2009. [Google Scholar]
- 14.Conwell Y. Suicide in later life: a review and recommendations for prevention. Suicide Life Threat Behav. 2001;(31 suppl):32–47. doi: 10.1521/suli.31.1.5.32.24221. [DOI] [PubMed] [Google Scholar]
- 15.Lawrence D, Almeida OP, Hulse GK. Suicide and attempted suicide among older adults in Western Australia. Psychol Med. 2000;30:813–821. doi: 10.1017/s0033291799002391. [DOI] [PubMed] [Google Scholar]
- 16.De Leo D, Scocco P. Treatment and prevention of suicidal behaviour in the elderly. In: Hawton K, Van Heeringen C, editors. The International Handbook of Suicide and Attempted Suicide. Wiley; New York: 2000. pp. 556–570. [Google Scholar]
- 17.Tsoh J, Chiu HF, Duberstein PR. Attempted suicide in elderly Chinese persons: a multi-group, controlled study. Am J Geriatr Psychiatry. 2005;13:562–571. doi: 10.1176/appi.ajgp.13.7.562. [DOI] [PubMed] [Google Scholar]
- 18.Cedereke M, Monti K, Ojehagen A. Telephone contact with patients in the year after a suicide attempt: does it affect treatment attendance and outcome? A randomized controlled study. Eur Psychiatry. 2002;17:82–91. doi: 10.1016/s0924-9338(02)00632-6. [DOI] [PubMed] [Google Scholar]
- 19.Allard R, Marshall M, Plante MC. Intensive follow-up does not decrease the risk of repeat suicide attempts. Suicide Life Threat Behav. 1992;22:303–314. [PubMed] [Google Scholar]
- 20.Motto JA, Bostrom AG. A randomized controlled trial of postcrisis suicide prevention. Psychiatr Serv. 2001;52:828–833. doi: 10.1176/appi.ps.52.6.828. [DOI] [PubMed] [Google Scholar]
- 21.Morgan HG, Jones EM, Owen JH. Secondary prevention of nonfatal deliberate self-harm. The green card study. Br J Psychiatry. 1993;163:111–112. doi: 10.1192/bjp.163.1.111. [DOI] [PubMed] [Google Scholar]
- 22.Dieserud G, Loeb M, Ekeberg O. Suicidal behavior in the municipality of Baerum, Norway: a 12-year prospective study of parasuicide and suicide. Suicide Life Threat Behav. 2000;30:61–73. [PubMed] [Google Scholar]
- 23.Aoun S. Deliberate self-harm in rural Western Australia: results of an intervention study. Aust N Z J Ment Health Nurs. 1999;8:65–73. doi: 10.1046/j.1440-0979.1999.00133.x. [DOI] [PubMed] [Google Scholar]
- 24.Carter GL, Clover K, Whyte IM. Postcards from the EDge project: randomised controlled trial of an intervention using postcards to reduce repetition of hospital treated deliberate self poisoning. BMJ. 2005;331 doi: 10.1136/bmj.38579.455266.E0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chiu HF, Yip PS, Chi I. Elderly suicide in Hong Kong–a case-controlled psychological autopsy study. Acta Psychiatr Scand. 2004;109:299–305. doi: 10.1046/j.1600-0447.2003.00263.x. [DOI] [PubMed] [Google Scholar]
- 26.Chiu HF, Lam LC, Pang AH. Attempted suicide by Chinese elderly in Hong Kong. Gen Hosp Psychiatry. 1996;18:444–447. doi: 10.1016/s0163-8343(96)00063-1. [DOI] [PubMed] [Google Scholar]
- 27.Yesavage JA, Brink TL, Rose TL. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982–1983;17:37–49. doi: 10.1016/0022-3956(82)90033-4. [DOI] [PubMed] [Google Scholar]
- 28.Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): Recent Evidence and Development of a Shorter Version. Clinical Gerontology: A Guide to Assessment and Intervention. The Haworth Press; New York: 1986. pp. 165–173. [Google Scholar]
- 29.Lee HC, Chiu HF, Wing YK. Chinese elderly and the GDS short form. A preliminary study. Clin Gerontol. 1993;14:37–41. [Google Scholar]
- 30.Henriksson S, Isacsson G. Increased antidepressant use and fewer suicides in Jämtland county, Sweden, after a primary care educational programme on the treatment of depression. Acta Psychiatr Scand. 2006;114:159–167. doi: 10.1111/j.1600-0447.2006.00822.x. [DOI] [PubMed] [Google Scholar]
- 31.Bramness JG, Walby FA, Tverdal A. The sales of antidepressants and suicide rates in Norway and its counties 1980–2004. J Affect Disord. 2007;102:1–9. doi: 10.1016/j.jad.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 32.Hall WD, Mant A, Mitchell PB. Association between antidepressant prescribing and suicide in Australia, 1991–2000: trend analysis. BMJ. 2003;326 doi: 10.1136/bmj.326.7397.1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Census and Statistics, the Government of the Hong Kong Special Administrative Region Hong Kong Statistics: Population and Vital Events, by Age Group and Sex. Available at: http:www.censtatd.gov.hk/hong_kong_statistics/statistical_tables/index.jsp=subjectID=1&tableID=002 Accessed July 22, 2009.
- 34.Chan SM, Chiu FK, Lam CW. Elderly suicide and the 2003 SARS epidemic in Hong Kong. Int J Geriatr Psychiatry. 2006;21:113–118. doi: 10.1002/gps.1432. [DOI] [PubMed] [Google Scholar]
- 35.Cheung YT, Chau PH, Yip PS. A revisit on older adults suicide and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int J Geriatr Psychiatry. 2008;23:1231–1238. doi: 10.1002/gps.2056. [DOI] [PubMed] [Google Scholar]
- 36.De Leo D, Dello Buono M, Dwyer J. Suicide among the elderly: the long-term impact of a telephone support and assessment intervention in northern Italy. Br J Psychiatry. 2002;181:226–229. doi: 10.1192/bjp.181.3.226. [DOI] [PubMed] [Google Scholar]
- 37.Oyama H, Watanabe N, Ono Y. Community-based suicide prevention through group activity for the elderly successfully reduced the high suicide rate for females. Psychiatry Clin Neurosci. 2005;59:337–344. doi: 10.1111/j.1440-1819.2005.01379.x. [DOI] [PubMed] [Google Scholar]