

Abstract
Acute gastroenteritis is one of the most common diseases in humans worldwide. Viruses are recognized as important causes of this disease, particularly in children. Since the Norwalk virus was identified as a cause of gastroenteritis, the number of viral agents associated with diarrheal disease in humans has steadily increased. Rotavirus is the most common cause of severe diarrhea in children under 5 years of age. Astrovirus, calicivirus and enteric adenovirus are also important etiologic agents of acute gastroenteritis. Other viruses, such as toroviruses, coronaviruses, picobirnaviruses and pestiviruses, are increasingly being identified as causative agents of diarrhea. In recent years, the availability of diagnostic tests, mainly immunoassays or molecular biology techniques, has increased our understanding of this group of viruses. The future development of a safe and highly effective vaccine against rotavirus could prevent, at least, cases of severe diarrhea and reduce mortality from this disease.
Keywords: Viral gastroenteritis, acute diarrhea, rotaviruses, enteric adenoviruses, astroviruses, human caliciviruses, coronaviruses, toroviruses, picobirnaviruses
Introduction
Acute gastroenteritis is one of the most common diseases in humans, and continues to be a significant cause of morbidity and mortality worldwide [1]. Children under 5 years of age are particularly prone, and it is calculated that, in this group, there are more than 700 million cases of acute diarrhea every year [2]. The mortality associated with gastroenteritis has been estimated to be 3–5 million cases per year, the majority of which occur in developing countries [3, 4, 5]. In the developed world, the impact of the illness is seen in its high morbidity and in the high incidence of hospitalization that this illness necessitates [6].
Historical background
Since the 1940s, viruses have been suspected of being important causes of gastroenteritis, as the etiology remained unknown in most cases [7, 8]. However, it was not until 1972 that Kapikian et al. first identified a virus (Norwalk virus) in feces after an outbreak of diarrhea [9] as a cause of gastroenteritis. One year later, Bishop et al. observed the presence of rotavirus in the duodenal mucosa of children with gastroenteritis [10], and in 1975, astroviruses [11] and enteric adenoviruses were identified in the feces of children with acute diarrhea [12].
Since then, the number of viruses associated with acute gastroenteritis has steadily increased. Thus, coronaviruses [13], picobirnaviruses [14, 15, 16], pestiviruses [17] and toroviruses [18], which produce diarrhea in animals, are emerging as causes of viral gastroenteritis in humans, according to several studies [19, 20, 21].
Description of the agents
Rotaviruses
Morphology
Rotaviruses are members of the Reoviridae family [22], and are characterized by their non‐enveloped icosahedral structure and 70‐nm diameter. When observed under an electron microscope, they have a ‘wheel’ shape [23, 24] (Figure 1a). The capsid consists of a double protein layer; the outer capsid is composed of the structural proteins VP7 and VP4, and the inner capsid mainly of VP6. The core is found inside the inner capsid, and encloses the rotavirus genome, composed of 11 segments of double‐stranded RNA. Given the segmented nature of the RNA genome, co‐infection of cells with two different strains of rotavirus may result in reassortant virus, with RNA segments from each of the progenitors [25].
Figure 1.
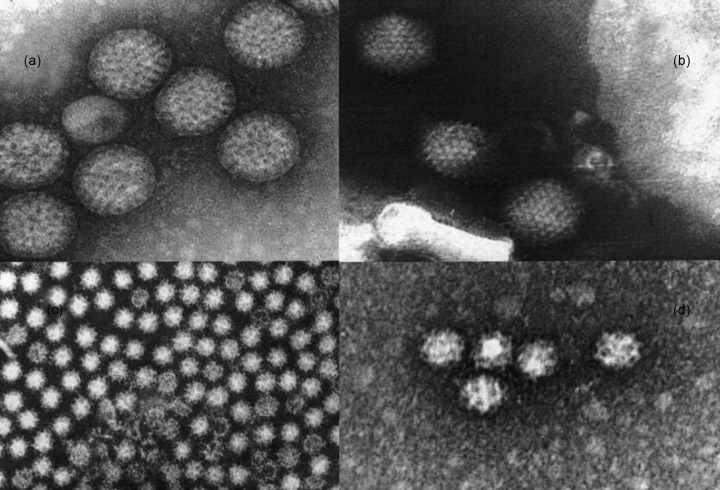
Electronmicrographs of: (a) human rotavirus; (b) enteric adenovirus; (c) human astrovirus with a diameter of 28 nm; (d) human calicivirus. Bar = 50 nm (Courtesy of Dr A. Sánchez‐Fauquier).
Each of the genomic segments encodes the structural VP proteins (VP1, VP2, VP3, VP4 (VP5 + VP8), VP6 and VP7) and the non‐structural NSP proteins (NSP1, NSP2, NSP3, NSP4 and NSP5) [23]. Table 1 shows the characteristics of these proteins. Of particular interest is NSP4, since it has enterotoxin‐like activity and can induce diarrhea in mice [26, 27].
Table 1.
Characteristics of structural and non‐structural rotavirus group A proteins
| Genome segment | Protein encoded | Viral particle localization | Function |
|---|---|---|---|
| 1 | VP1 | Core | RNA polymerase |
| 2 | VP2 | Core | RNA binding |
| 3 | VP3 | Core | Guanilyltransferase |
| 4 | VP4 | Outer capsid | Viral hemagglutinin, neutralization antigen, P serotypes |
| (VP5 + VP8 subunits) | Proteolytic cell cleavage | ||
| 5 | NSP1 | Non‐structural | RNA binding |
| 6 | VP6 | Inner capsid | Group and subgroup antigen |
| 7, 8, 9 | NSP3 | Non‐structural | RNA binding |
| 7, 8, 9 | VP7 | Outer capsid | Glycoprotein (G serotypes), neutralization antigen |
| 8 | NSP2 | Non‐structural | Viral replication |
| 10 | NSP4 | Non‐structural | Enterotoxin‐like activity, viral assembly |
| 11 | NSP5 | Non‐structural | RNA binding |
Classification
Rotaviruses are classified into groups, subgroups and serotypes according to the antigenic properties of the capsid proteins. Protein VP6 is the group reactivity determinant, with seven groups currently in existence, labeled A–G, and two subgroups, I and II [28]. Groups A, B and C are those which produce infection in humans. Classification into serotypes is based on the antigenic differences in the proteins of the outer capsid, VP7 and VP4. The first, a glycoprotein, determines the G‐type specificity, and the second, the P‐type specificity, owing to its protease sensitivity. At present, there are 15 G types [29], with G1, G2, G3 and G4 being the predominant ones throughout the world [6]. However, there have been reports of infections by unusual G types [30, 31, 32, 33, 34, 35], and recently there have been reports of the emergence of serotype G9 in several countries, such as Brazil [32], Malawi [35], the USA [36, 37], France [38], India [39], Argentina [40], the UK [41] and Australia [42].
Pathogenesis and immune response
Rotaviruses infect the mature enterocytes on the tips of small intestine villi and lead to villous epithelium atrophy and compensatory repopulation of the epithelium by immature secretor cells, with secondary hyperplasia of the crypts [43]. It has been proposed that cellular damage is secondary to villus ischemia [44]. The mechanism that induces the production of diarrhea is not well understood, although it appears to be mediated by the relative decrease of villous epithelium absorption in relation to the secretory capacity of the crypt cells [24]. There is also a loss of intestinal permeability to macromolecules such as lactose, secondary to a decrease in disaccharidase in the intestine. The enteric nervous system is stimulated by this virus, leading to the induction of intestinal water and electrolyte secretion [45].
The immunologic mechanisms responsible for protection against infection by rotavirus are still not well known. Several studies have shown that local intestinal immunity protects against successive severe episodes of diarrhea [46, 47, 48]. The presence of neutralizing antibodies directed towards the proteins VP4 or VP7 does not correlate with protection against this disease [49]. It has been reported that the first infection with rotavirus elicits a homotypic neutralizing antibody response, with heterotypic responses in subsequent infections [50]. It has recently been shown that protein NSP4 produces a cellular immunity‐mediated response [51].
Enteric adenoviruses
Morphology
Human adenoviruses belong to the Adenoviridae family and, within the genus, the majority of enteric adenoviruses reported to date belong to subgenus F [52, 53]. They are DNA viruses without an envelope, 70 nm in diameter, and with icosahedric symmetry (Figure 1). The protein capsid is composed of 252 capsomers—240 hexones and 12 pentones—and structures called fibers that protrude to the outside. The hexones contain proteins II, VI, VIII, and IX, which participate in the stability and assembly of the viral particle. The pentone proteins (III and IIIa) have the function of cellular penetration, and the fibers are hemagglutinins and are responsible for binding the virus to receptors (Figure 1b) [52, 53, 54]. There are at least eight proteins making up the core [55]; these maintain the integrity of the genome, and participate in enzymatic activity. The genome consists of a linear molecule of double‐stranded DNA that represents 15% of the viral mass [53].
Classification
The enteric serotypes that are most frequently associated with gastroenteritis caused by adenovirus are 40 and 41, which belong to subgenus F. More rarely, serotypes 31, 12 and 18 of subgenus A [53] and serotypes 1, 2, 5 and 6 of subgenus C [52, 56] have been involved in the etiology of acute diarrhea.
Pathogenesis and immune response
In the same way as in gastroenteritis produced by rotavirus, the lesions produced by serotypes 40 and 41 in the enterocytes lead to atrophy of the villi and compensatory hyperplasia in the crypts, with subsequent malabsorption and loss of fluids [44, 54]. After the infection, specific antibodies develop in most cases, and non‐neutralizing antibodies are useful for measuring the immune response. The specific type‐neutralizing antibodies can provide protection both in the current illness and in reinfections by the same serotype, although patients may continue to eliminate the virus in their feces for months after an effective humoral response [56].
Astroviruses
Morphology
In 1993, the Astroviridae family was established with a single genus, the astrovirus, which encompasses human and animal viruses [57, 58].
Astrovirus has been reported as small round viruses of 28 nm with an appearance like that of a five‐ or six‐pointed star by direct visualization with electron microscopy. The name stems from the Greek astron, meaning star [11]. However, it has recently been verified that this virus has a different morphology, with an icosahedric appearance, a diameter of 41 nm, and well defined spikes. When these viruses are subjected to a high pH, they transform and present the typical morphology of the initially described star [59] (Figure 1c).
The genome of human astroviruses is composed of single‐stranded, positive‐sense RNA which contains three ‘open reading frames’ (ORFs). ORF1a and ORF1b encode viral protease and polymerase, respectively. ORF2 encodes protein capsid precursor and is found at the 3′‐terminus of the genome [57, 60].
The protein structure of astrovirus is not well known at present. However, it seems that the precursor of the capsid proteins, an 87‐kDa polyprotein, gives rise to the structural capsid proteins VP32, VP29, and VP26 [61].
Trials with monoclonal antibodies against human astrovirus suggest that VP26 and/or VP29 may be important in the neutralization, heterotypic immunity and binding of the virus to the target cells [61, 62]. These proteins, especially VP26, seem to be responsible for the antigenic variation observed among the different serotypes [61].
Classification
Astroviruses are classified into serotypes based on the reactivity of the capsid proteins with polyclonal sera and monoclonal antibodies [57, 63]. To date, there have been reports of four neutralizing monoclonal antibodies, developed by Sanchez‐Fauquier et al. against serotype 2 human astrovirus [61] and by Bass and Upadhyayula against serotype 1 astrovirus [62]. They all react with the VP26 capsid protein, involved in the neutralization of human astroviruses.
Astroviruses can also be classified into genotypes on the basis of the nucleotide sequence of a 348‐bp region of the ORF2, and there is a good correlation with the serotypes [64]. There are seven established genotypes, which correspond with seven serotypes. The existence of an eighth genotype has been suggested, due to the sequence of a putative serotype 8 [65]. Serotype 1 is predominant in most studies, followed by 2, 3, 4 and 5. Serotypes 6, 7 and 8 are rarely detected [63, 65, 66, 67, 68, 69].
Pathogenesis and immune response
The pathogenesis of the disease induced by astrovirus has not yet been established, although it has been suggested that viral replication occurs in intestinal tissue [57, 70]. Studies in adult volunteers have not clarified the pathogenic mechanisms [71, 72]. In animal studies, atrophy of the intestinal villi is observed, as well as inflammatory infiltrates in the lamina propria [73], leading to osmotic diarrhea.
Symptomatic astrovirus infection occurs mainly in small children and the elderly, which suggests a reduction in antibodies in recent years, but the determinants of immunity are not well known [57]. Studies in adult volunteers indicate that people with detectable levels of antibodies do not develop the illness [71].
Human caliciviruses
Morphology
Human caliciviruses are members of the Caliciviridae family, and two genera have been described, the Norwalk‐like viruses (NLVs) and Sapporo‐like viruses (SLVs) [74]. The virions are composed of a single structural capsid protein, with icosahedric symmetry [75]. This protein, composed of 180 molecules, folds into 90 dimers, which form a continuous shell with protrusions in the shape of an arch (Figure 1d). A key characteristic is the existence of 32 cup‐shaped depressions, situated on the axes of the icosahedron, from whose Latin designation, calyx, the virus derives its name [76].
The genome of the NLVs consists of positive‐sense, single‐stranded RNA organized into three ORFs. ORF1 encodes the non‐structural proteins, such as RNA‐dependent RNA polymerase and helicase [77], ORF2 encodes the structural protein of the capsid, and ORF3 encodes for a small protein whose function is unknown [76]. The genome of the SLVs differs from the NLV genome in that the ORF1 encodes the non‐structural proteins as well as the structural protein of the capsid [78, 79]. ORF2 encodes a small protein of unknown function, and the significance of ORF3 is still uncertain.
Classification
The human caliciviruses genera (NLVs and SLVs) can be further divided into genetic clusters. The NLVs include Norwalk virus (the type species), Desert Storm virus, Southampton virus, Snow Mountain agent, Hawaii virus, Toronto virus, Bristol virus, and Jena virus. The SLVs includes Sapporo virus (the type species), Parkville virus, and London virus [80, 81].
Pathogenesis and immune response
In studies carried out on volunteers, infection by calicivirus was observed to produce an expansion of the villi of the proximal small intestine. The epithelial cells remain intact, and there is shortening of the microvilli [82, 83]. The mechanism by which diarrhea is produced is unknown, although it has been suggested that the delay in gastric emptying observed in Norwalk virus gastroenteritis may play a role [84].
Infection by the Norwalk virus induces a specific IgG, IgA and IgM serum antibody response, even if there has been previous exposure [83]. Two weeks after infection by the Norwalk virus, an increase in jejunal synthesis has been demonstrated for IgA [85], and most patients are resistant to reinfection for 4–6 months [83]. Nevertheless, a lack of long‐term protection has been observed.
Other gastroenteritis‐producing viruses
Torovirus
Torovirus is a genus within the Coronaviridae family. Torovirus was detected for the first time in the feces of patients with gastroenteritis in 1984 [18]. These viruses have an envelope of 100–140 nm, with a capsid of helicoidal symmetry and a single‐stranded RNA genome of positive sense [86]. They are associated with persistent and acute diarrhea in children, and may represent an important cause of nosocomial diarrhea [19, 87].
Coronavirus
Included in the Coronaviridae family, these viruses are between 60 and 220 nm, with helicoidal symmetry and a spiculated envelope that gives them the appearance of a crown. The genome is composed of positive monocatenary RNA [88, 89]. Coronavirus was linked with diarrhea in humans for the first time in 1975, but studies have not yet been able to establish a definite etiologic role [90].
Picobirnaviruses
These are small viruses, without an envelope, 30–40 nm in diameter, with a capsid of icosahedric symmetry, and a genome made up of two or three segments of bicatenary RNA. They were identified for the first time by Pereira et al. in 1988 [91]. Since then, they have been found in a wide variety of animal species [14] and in both children and adults with diarrhea, including immunodepressed patients [92, 93, 94, 95, 96]. In a recent publication, however, this virus was not found in HIV‐infected children with diarrhea [97].
Clinical aspects
Viral diarrhea in children
Rotavirus is the main cause of severe diarrhea in children under 5 years of age, and causes more than 130 million episodes per year throughout the world, and between 600 000 and 870 000 deaths [98, 99], the vast majority of which are in developing countries [100, 101, 102]. Several European studies point to rotavirus as the agent responsible for 20–60% of cases of gastroenteritis requiring hospitalization [103, 104, 105, 106, 107, 108]. In Australia, similar figures have been reported [109], and in the USA it has been estimated that one in every 73 children will have been hospitalized because of diarrhea due to rotavirus A during the first 5 years of life [110].
As far as ‘non‐group A’ rotavirus is concerned, group B rotavirus has been identified in epidemic outbreaks of severe diarrhea in adults in Southeast Asia since 1982 [111], and in symptomatic infections in children. Outbreaks of diarrhea due to group C rotavirus have been identified in Asia [112], Brazil [113], and Europe [114, 115], and outbreaks of sporadic gastroenteritis caused by this virus in children have been observed in the USA [116], Japan [117], and the UK [118], with frequencies ranging from 1% to 6.8%.
Enteric adenoviruses present variable incidences of infection. In industrialized countries, the incidence varies from 1% to 8% [119, 120, 121, 122, 123, 124], whereas in developing countries, figures of 2–31% have been published [125, 126, 127, 128].
In the initial studies of astrovirus by electron microscopy carried out in several countries, the virus was detected in about 1% of cases [129, 130, 131]. At present, thanks to the development of enzyme immunoassay (EIA) techniques, which use monoclonal antibodies [132], incidences of 2–13% have been detected in children seenat hospitals [65, 67, 127, 133, 134, 135, 136, 137, 138]. In the community, astrovirus is responsible for 4–10% of cases of gastroenteritis [66, 69, 119, 139, 140], and has become the leading cause of this illness [141].
Human calicivirus was first identified as a cause of outbreaks of non‐bacterial diarrhea, initially using electronmicroscopic techniques [9, 142]. In recent studies, with the application of new assays such as EIA and reverse transcription–polymerase chain reaction (RT‐PCR), our knowledge of the epidemiology of human calicivirus has changed, especially for Norwalk‐type virus [76]. Thus, these viruses are recognized as the main agents responsible for outbreaks of non‐bacterial diarrhea, and new estimates suggest that they represent the most common cause of illness with a food origin [143, 144, 145, 146, 147]. Similarly, recent studies investigating calicivirus in sporadic cases of gastroenteritis in children have found that Norwalk‐type viruses comprise the second cause of viral gastroenteritis after rotavirus [119, 148, 149, 150].
From the clinical point of view, acute viral gastroenteritis cannot be distinguished from that caused by bacteria, and in general it is a self‐limiting process of diarrhea and vomiting, with a duration of 1–7 days, which may sometimes become prolonged or persistent [69, 121, 122, 151, 152].
The most common age of presentation of sporadic viral gastroenteritis is 6–24 months [7, 139, 153, 154, 155]. During the neonatal period, infection by rotavirus is mostly asymptomatic, possibly due to maternal protective factors and intestinal immaturity. Another factor could be the attenuated nature of certain strains, frequently detected in neonates with symptomatic and asymptomatic infections [153, 155, 156]. During the first 2 years of life, repeated rotavirus infections occur, 50% of which are asymptomatic [157, 158, 159]. Several studies have also shown the asymptomatic elimination in feces of adenovirus and astrovirus, and it is calculated that about 50% of infections by calicivirus are asymptomatic [122, 133, 139, 141, 150, 154].
The severity of the infection, together with the need for hospitalization, is greater with gastroenteritis caused by group A rotavirus than with that associated with adenovirus [121, 160, 161], astrovirus [139, 140, 162] or calicivirus [119, 149, 150].
The viruses that produce gastroenteritis represent an important cause of nosocomial infection in pediatric admission units. Between 20% and 50% of cases of gastroenteritis caused by rotavirus in hospitals are considered to be of nosocomial origin [6, 163, 164], and nosocomial diarrhea has been described in 2–6% of children admitted [165, 166]. Nosocomial infections by adenovirus and astrovirus also represent an important problem, as several studies have shown [69, 136, 167, 168]. There are fewer data on the incidence of nosocomial infection due to calicivirus, although in the studies published it is calculated to be high, following group A rotavirus in frequency [130, 167, 169, 170, 171]. The prevalence and transmission of nosocomial infection are accounted for by the many asymptomatic patients who eliminate the virus in feces [57, 172, 173] and the environmental contamination that accompanies the relative resistance of these viruses to normal disinfectants [174, 175].
Viral gastroenteritis in adults
Calicivirus is the main agent of viral gastroenteritis in adults, and generally produces epidemic outbreaks [143, 176, 177]. The cause of sporadic acute non‐bacterial gastroenteritis has not been well studied in adults, although a viral origin is presumed, due to the similarity of the illness with the epidemics produced by calicivirus [176]. The detection of calicivirus antigen in the feces of patients with sporadic gastroenteritis has been infrequent, although a high seroprevalence of antibodies against calicivirus has been found in young adults [178, 179].
We do not know the frequency of sporadic gastroenteritis caused by rotavirus in adults either, as this is generally secondary to disease in a child, and it also occurs as travelers' diarrhea [180], with some cases of severe diarrhea and death in the elderly [181].
Epidemic outbreaks of diarrhea in adults caused by infrequent serotypes of astrovirus have been reported [129, 182], and more sensitive techniques such as RT‐PCR are likely to reveal a greater prevalence of sporadic gastroenteritis in adults.
Viral gastroenteritis in the immunocompromised patient
The main viral causes of severe gastroenteritis in immunosuppressed patients are cytomegalovirus (CMV) and Epstein–Barr virus (EBV), which mainly affect patients with AIDS and transplant recipients [176, 183, 184]. CMV is a frequent pathogen in diarrhea associated with AIDS with CD4 counts below 100 cells/mm3[185, 186], although the introduction of antiretroviral therapy has drastically reduced its frequency in this group of patients [176]. Other viruses that produce HIV‐associated gastroenteritis include astrovirus, picobirnavirus, calicivirus and adenovirus [92, 93]. There is evidence of gastroenteritis due to astrovirus and adenovirus in both child and adult bone marrow transplant recipients [187, 188]. Similarly, torovirus has been associated with diarrhea in immunocompromised children [19].
Detection of gastroenteritis‐producing viruses
Detection of gastroenteritis‐producing viruses has traditionally been based on techniques of direct visualization using electron microscopy, which, although it is still useful, is limited to reference laboratories [6, 23, 76, 189, 190].
Cell culture of these viruses is not considered to be useful for diagnostic purposes, as it is technically cumbersome and slow. Propagation in cellular media of calicivirus, human torovirus or coronavirus has not yet been achieved [76, 189].
The progressive incorporation of more sensitive techniques for antigen detection in feces based on immunoassay techniques, as well as the development of molecular biology techniques, has improved the diagnosis of this virus and contributed to an appreciation of its clinical importance.
Antigen detection techniques
In recent years, a wide variety of techniques for the detection of antigen in fecal samples have been developed. These are based on EIA, agglutination with latex particles (LA) and, more recently, immunochromatography (ICG), all of which are available commercially for group A rotavirus, adenovirus and astrovirus [6, 189].
EIA has proven to be more sensitive than direct visualization by electron microscopy [191, 192], and also has a high specificity in the detection of group A rotavirus, especially when monoclonal antibodies are used [193, 194]. The LA technique has lower sensitivity than EIA [6, 194]. ICG showed high sensitivity and results comparable to those achieved with EIA, and is rapid and technically very simple [195, 196].
Group C rotavirus can be detected in fecal samples by means of recently described immunoanalysis techniques, which use different antigens and monoclonal antibodies [116, 118, 197] and are more sensitive than electron microscopy.
In the case of adenoviruses, many of these techniques detect group common antigen, and several studies have shown that between 45% and 93% of the samples positive for the group correspond to enteric serotypes 40 and 41 [121, 122, 198, 199].
At present, EIA techniques are available for the detection of astroviruses, due to the development of monoclonal antibodies against this virus [62, 132, 168, 200]. Some have recently been marketed, with good sensitivity and specificity compared with electron microscopy and RT‐PCR [67, 201].
Recently, EIA methods have been developed with monoclonal and polyclonal antibodies for the detection of human calicivirus. These methods have promise, although their use currently seems to be limited to research laboratories [76, 202].
Molecular biology techniques
PCR techniques have been developed for many of the viruses that produce gastroenteritis, although they are not used routinely. These techniques are more sensitive than immunoassay methods. They are useful for the confirmation of the results of other techniques, and for the study of samples such as cerebrospinal fluid or serum, and environmental samples [203, 204, 205, 206, 207, 208].
In the case of human calicivirus, RT‐PCR is the most sensitive and widely used technique at present for the detection of these viruses [209, 210, 211, 212].
Molecular techniques are also used to genotype these viruses [24, 31, 63, 64]. RT‐PCR techniques have been developed to genotype group A rotavirus with type‐specific primers for genotypes G and P [213, 214].
Prevention of disease
Treatment of viral gastroenteritis is symptomatic, and its aim is to prevent or treat the dehydration secondary to the disease. For this, it is important to start liquid intake early, in order to correct the water deficit and combat the losses due to vomiting and diarrhea [215].
Interruption of transmission of the infection is extremely important, especially in hospitals and centers which care for small children. Therefore, it is necessary to reinforce hygiene measures and clean all surfaces with suitable disinfectants [105, 165, 174].
Studies with vaccines against group A rotavirus began in 1982. The first vaccine developed was the tetravalent human–rhesus reassortant vaccine, which induces protection against the four main rotavirus serotypes, G1–G4. Efficacy studies showed a reduction in the appearance of severe gastroenteritis caused by rotavirus of between 69% and 91% in vaccinated children [216], and the vaccine was approved in the USA in 1998 [217]. However, the detection of an increase in the risk of intussusception after vaccination led to its suspension [218, 219]. At present, plasmidic DNA and antigenic vaccines, which code for specific viral proteins, are being investigated [220].
The wide variety found among circulating genotypes and serotypes of group A rotavirus in studies from around the world leads us to examine the need to cover more serotypes in the development of new vaccines [34, 35, 40, 42, 221, 222, 223].
References
- 1. Glass RI, Kilgore PE. Etiology of acute viral gastroenteritis In: Gracey M, Walker JA, eds. Diarrheal disease. Nestlé Nutrition Workshop Series. Philadelphia: Lippincott‐Raven, 1997: 39–54. [Google Scholar]
- 2. Snyder JD, Merson MH. The magnitude of the global problem of acute diarrhoeal disease: a review of active surveillance data. Bull WHO 1982; 60: 605–31. [PMC free article] [PubMed] [Google Scholar]
- 3. Bern C, Glass RI. Impact of diarrhoeal disease worldwide In: Kapikian AZ, ed. Viral infection of gastrointestinal tract. New York: Marcel Dekker, 1994: 1–26. [Google Scholar]
- 4. Guerrant RI, Hughes JM, Lima NL, Crane J. Diarrhea in developed and developing countries: magnitude, special settings, and etiologies. Rev Infect Dis 1990; 12(suppl 1): S41–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Warren KS. Tropical medicine or tropical health. The Health Clark lectures 1988. Rev Infect Dis 1990; 12: 142–56. [DOI] [PubMed] [Google Scholar]
- 6. Christensen ML. Rotaviruses In: Murray PR, Baron EJ, Pfaller MA, Tenover FC, Yolken RH, eds. Manual of clinical microbiology. Washington: ASM Press, 1999: 999–1004. [Google Scholar]
- 7. Kapikian AZ. Overview of viral gastroenteritis. Arch Virol Suppl 1996; 12: 7–19. [DOI] [PubMed] [Google Scholar]
- 8. Parashar UD, Bresee JS, Gentsch JR, Glass RI. Rotavirus. Emerg Infect Dis 1998; 4: 561–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kapikian AZ, Wyatt RG, Dolin R, Thornhill TS, Kalica AR, Chanock RM. Visualization by immune electron microscopy of a 27 nm particle associated with acute infectious non‐bacterial gastroenteritis. J Virol 1972; 10: 1075–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Bishop RF, Davidson GP, Holmes IH, Ruck BJ. Virus particles in epithelial cells of duodenal mucosa from children with acute non bacterial gastroenteritis. Lancet 1973; 2: 1281–3. [DOI] [PubMed] [Google Scholar]
- 11. Madeley CR, Cosgrove BP. 28 nm particles in faeces in infantile gastroenteritis. Lancet 1975; 2: 451–2. [DOI] [PubMed] [Google Scholar]
- 12. Flewett TH, Bryden AS, Davies H, Morris CA. Epidemic viral enteritis in a long‐stay children's ward. Lancet 1975; 1: 4–5. [DOI] [PubMed] [Google Scholar]
- 13. Caul EOK, Paver K, Clarke SKR. Coronavirus particles in faeces from patients with gastroenteritis. Lancet 1975; i: 1192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Chandra R. Picobirnavirus, a novel group of undescribed viruses of mammals and birds: a minireview. Acta Virol 1997; 41: 59–62. [PubMed] [Google Scholar]
- 15. Grohmann GS, Glass RI, Pereira HG, Monroe SS, Hightower AW, Bryan RT. Enteric virus and diarrhea in HIV infected patients. N Engl J Med 1993; 329: 14–20. [DOI] [PubMed] [Google Scholar]
- 16. Ludert JE, Liprandi F. Identification of viruses with bi‐ and trisegmented double‐stranded RNA genome in faeces of children with gastroenteritis. Res Virol 1993; 144: 219–24. [DOI] [PubMed] [Google Scholar]
- 17. Yolken RH, Dubovi E, Leister F, Reid R, Almeido‐Hill J, Santosham M. Infantile gastroenteritis associated with excretion of pestiviruses antigens. Lancet 1989; i: 517–20. [DOI] [PubMed] [Google Scholar]
- 18. Beards GM, Brown WG, Green J, Flewett TH. An enveloped virus in stools of children and adults with gastroenteritis that resembles de Breda virus of calves. J Med Virol 1986; 20: 67–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Jamieson F, Wang EI, Bain C et al. Human torovirus: a new nosocomial gastrointestinal pathogen. J Infect Dis 1998; 178: 1263–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Kapikian AZ. Viral gastroenteritis In: Evans AS, Kaslow RA, eds. Viral infections of humans: epidemiology and control. New York: Plenum Medical Book Company, 1997: 285–343. [Google Scholar]
- 21. Kilgore PE, Glass RI. Gastrointestinal syndromes In: Richman DD, Whitley RJ, Hayden FG, eds. Clinical virology. New York: Churchill Livingstone, 1997: 55–67. [Google Scholar]
- 22. Matthews REF. The classification and nomenclature of viruses: summary of results of meetings of the International Committee on Taxonomy of Viruses in The Hague. Intervirology 1979; 11: 133–5. [DOI] [PubMed] [Google Scholar]
- 23. Kapikian AZ, Chanock RM. Rotaviruses In: Fields BN, Knipe DM, Howley PM, eds. Virology, 3rd edn Philadelphia: Lippincott‐Raven Press, 1996: 1657–708. [Google Scholar]
- 24. Offit PA, Clark HF. Rotavirus In: Mandell GL, Bennet JE, Dolin R, eds. Principles and practice of infectious diseases. New York: Churchill Livingstone, 1995: 1448–55. [Google Scholar]
- 25. Desselberger U. Genome rearrangements of rotaviruses. Arch Virol Suppl 1996; 12: 37–51. [DOI] [PubMed] [Google Scholar]
- 26. Ball JM, Tian P, Zeng CQY, Morris AP, Estes MK. Age‐dependent diarrhea induced by a rotaviral nonstructural glycoprotein. Science 1996; 272: 101–4. [DOI] [PubMed] [Google Scholar]
- 27. Kirkwood CD, Palombo EA. Genetic characterization of the rotavirus nonstructural protein, NSP4. Virology 1997; 236: 258–65. [DOI] [PubMed] [Google Scholar]
- 28. Estes MK, Cohen J. Rotavirus gene structure and function. Microbiol Rev 1989; 53: 410–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Rao CD, Gowda K, Reddy BS. Sequence analysis of VP4 and VP7 genes of nontypeable strains identifies a new pair of outer capsid proteins representing novel P and G genotypes in bovine rotaviruses. Virology 2000; 276: 104–13. [DOI] [PubMed] [Google Scholar]
- 30. Beards G, Xu L, Ballard A, Desselberger U, McCrae MA. A serotype 10 human rotavirus. J Clin Microbiol 1992; 30: 1432–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Gouvea V, Santos N. Rotavirus serotype G5: an emerging cause of epidemic childhood diarrhea. Vaccine 1999; 17: 1291–2. [DOI] [PubMed] [Google Scholar]
- 32. Santos N, Lima RCC, Pereira CFA, Gouvea V. Detection of rotavirus types G8 and G10 among Brazilian children with diarrhea. J Clin Microbiol 1998; 36: 2727–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Steele AD, Parker SP, Peenze I, Pager CT, Taylor MB, Cubitt WD. Comparative studies of human rotavirus serotype G8 strains recovered in South Africa and the United Kingdom. J Gen Virol 1999; 80: 3029–34. [DOI] [PubMed] [Google Scholar]
- 34. Adah MI, Wade A, Taniguchi K. Molecular epidemiology of rotaviruses in Nigeria. Detection of unusual strains with G2 P[6] and G8P[1] specificities. J Clin Microbiol 2001; 39: 369–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Cunliffe NA, Gondwe JS, Graham SM et al. Rotavirus strain diversity in Blantyre, Malawi, from 1997 to 1999. J Clin Microbiol 2001; 39: 836–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Griffin DD, Kirkwood CD, Parashar UD et al. Surveillance of rotavirus strains in the United States: identification of unusual strains. J Clin Microbiol 2000; 38: 2784–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Ramachandran M, Gentsch JR, Parashar UD et al. Detection and characterization of novel rotavirus strains in the United States. J Clin Microbiol 1998; 36: 3223–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Bon F, Fromatin C, Aho S, Pothier P, Kohli E. G and P genotyping of rotavirus strains circulating in France over a three year period: detection of G9 and P6 strains at low frequencies. J Clin Microbiol 2000; 38: 1681–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Unicomb LE, Podder G, Gentsch JR et al. Evidence of high‐freqency genomic reassortment of group A rotavirus strains in Bangladesh: emergence of type G9 in 1995. J Clin Microbiol 1999; 37: 1885–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Bok K, Palacios G, Sijvarger K, Matson D, Gómez J. Emergence pf G9 P[6] human rotaviruses in Argentina: phylogenetic relationships among G9 strains. J Clin Microbiol 2001; 39: 4020–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Iturriza‐Gomara M, Cubitt D, Steele D et al. Characterization of rotavirus G9 strain isolated in the UK between 1995 and 1998. J Med Virol 2000; 61: 510–17. [DOI] [PubMed] [Google Scholar]
- 42. Palombo EA, Masendycz PJ, Bugg HC, Bogdanovic‐Sakran N, Barnes GL, Bishop RF. Emergence of serotype G9 human rotavirus in Australia. J Clin Microbiol 2000; 38: 1305–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Salim AF, Phillips AD, Walker‐Smith JA, Farthing MJG. Sequential changes in small intestinal structure and function during rotavirus infection in neonatal rats. Gut 1995; 36: 231–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Farthing MJG. Acute diarrhea: pathophysiology In: Gracey M, Walker‐Smith JA, eds. Diarrheal disease. Nestlé Nutrition Workshop Series. Philadelphia: Lippincott‐Raven, 1997: 55–73. [Google Scholar]
- 45. Lundgren O, Peregrin AT, Persson K, Kordasti S, Uhnoo I, Svensson L. Role of the enteric nervous system in the fluid and electrolyte secretion of rotavirus diarrhea. Science 2000; 287: 491–5. [DOI] [PubMed] [Google Scholar]
- 46. Bishop RF, Bugg HC, Masendycz PJ, Lund JS, Gorrell RJ, Barnes GL. Serum, fecal, and breast milk rotavirus antibodies as indices of infection in mother–infant pairs. J Infect Dis 1996; 174(suppl 1): S22–9. [DOI] [PubMed] [Google Scholar]
- 47. Colomina J, Raga J, Gil MT, Buesa J. Virus‐specific serum and fecal antibodies response in children with acute rotavirus gastroenteritis. Enferm Infecc Microbiol Clin 1998; 16: 55–60. [PubMed] [Google Scholar]
- 48. Burns WB, Siadat‐Pajouh M, Krishnamey AA, Greenberg HB. Protective effect of rotavirus VP6 specific IgA monoclonal antibodies that lack conventional neutralizing activity. Science 1996; 272: 104–7. [DOI] [PubMed] [Google Scholar]
- 49. Ward RL. Mechanisms of protection against rotavirus in humans and mice. J Infect Dis 1996; 174(suppl 1): S51–8. [DOI] [PubMed] [Google Scholar]
- 50. Gorrell RJ, Bishop RF. Homotypic and heterotypic serum neutralizing antibody response to rotavirus proteins following natural primary infection and reinfection in children. J Med Virol 1999; 57: 204–11. [PubMed] [Google Scholar]
- 51. Johansen K, Hinkula J, Espinoza F et al. Humoral and cell‐mediated immune responses in humans to the NSP4 enterotoxin of rotavirus. J Med Virol 1999; 59: 369–77. [PubMed] [Google Scholar]
- 52. Baum SG. Adenovirus In: Mandell GL, Bennet JE, Dolin R, eds. Principles and practice of infectious diseases. New York: Churchill Livingstone, 2000: 1624–30. [Google Scholar]
- 53. Brown M, Grydsuk JD, Fortsas E, Petric M. Structural features unique to enteric adenoviruses. Arch Virol Suppl 1996; 12: 301–7. [DOI] [PubMed] [Google Scholar]
- 54. Wadell G, Allard A, Hierholzer JC. Adenoviruses In: Murray PR, Baron EJ, Pfaller MA, Tenover FC, Yolken RH, eds. Manual of clinical microbiology. Washington: ASM Press, 1999: 970–82. [Google Scholar]
- 55. Shenk T. Adenoviridae: the viruses and their replication In: Fields BN, Knipe DM, Howley PM, eds. Virology, 3rd edn Philadelphia: Lippincott‐Raven, 1996: 2111–48. [Google Scholar]
- 56. Horwitz MS. Adenoviruses In: Fields BN, Knipe DM, Howley PM, eds. Virology, 3rd edn Philadelphia: Lippincott‐Raven, 1996: 2149–71. [Google Scholar]
- 57. Matsui SM, Greenberg HB. Astroviruses In: Fields BN, Knipe DM, Howley PM, eds. Virology, 3rd edn Philadelphia: Lippincott‐Raven, 1996: 811–24. [Google Scholar]
- 58. Monroe SS, Jiang B, Stine SE, Koopmans M, Glass RI. Subgenomic RNA sequence of human astrovirus supports classification of Astroviridae as a new family of RNA viruses. J Virol 1993; 67: 3611–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Risco C, Carrascosa JL, Pedregosa AM, Humphrey CD, Sánchez‐Fauquier A. Ultrastructure of human astrovirus serotype 2. J Gen Virol 1995; 76: 2075–80. [DOI] [PubMed] [Google Scholar]
- 60. Carter MJ, Willcocks MM. The molecular biology of astroviruses. Arch Virol Suppl 1996; 12: 277–85. [DOI] [PubMed] [Google Scholar]
- 61. Sanchez‐Fauquier A, Carrascosa AL, Carrrascosa JL et al. Characterization of a human astrovirus serotype 2 structural protein (VP26) that contains an epitope involved in virus neutralization. Virology 1994; 201: 312–20. [DOI] [PubMed] [Google Scholar]
- 62. Bass DM, Upadhyayula U. Characterization of human serotype 1 astrovirus‐neutralizing epitopes. J Virol 1997; 71: 8666–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Lee TW, Kurtz JB. Prevalence of human astrovirus serotypes in the Oxford region 1976–92, with evidence for two new serotypes. Epidemiol Infect 1994; 112: 187–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Noel JS, Lee TW, Kurtz JB, Glass RI, Monroe SS. Typing of human astroviruses from clinical isolates by enzyme immunoassay and nucleotide sequencing. J Clin Microbiol 1995; 33: 797–801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Mustafa H, Palombo EA, Bishop RF. Epidemiology of astrovirus infection in young children hospitalized with acute gastroenteritis in Melbourne, Australia, over a period of four consecutive years, 1995 to 1998. J Clin Microbiol 2000; 38: 1058–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Gaggero A, O'Ryan M, Noel JS et al. Prevalence of astrovirus infection among Chilean children with acute gastroenteritis. J Clin Microbiol 1998; 36: 3691–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. McIver CJ, Palombo EA, Doultree JC, Mustafa H, Marshall JA, Rawlinson WD. Detection of astrovirus gastroenteritis in children. J Virol Method 2000; 84: 99–105. [DOI] [PubMed] [Google Scholar]
- 68. Palombo EA, Bishop RF. Annual incidence, serotype distribution, and genetic diversity of human astrovirus isolates from hospitalized children in Melbourne, Australia. J Clin Microbiol 1996; 34: 1750–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Unicomb LE, Banu NN, Azim T et al. Astrovirus infection in association with acute, persistent and nosocomial diarrhea in Bangladesh. Pediatr Infect Dis J 1998; 17: 611–14. [DOI] [PubMed] [Google Scholar]
- 70. Phillips AD, Rice SJ, Walker‐Smith JA. Astrovirus within human small intestinal mucosa. Gut 1982; 23: 923–4. [Google Scholar]
- 71. Kurtz JB, Lee TW, Craig JW, Reed SE. Astrovirus infection in volunteers. J Med Virol 1979; 3: 221–30. [DOI] [PubMed] [Google Scholar]
- 72. Midthun K, Greenberg HB, Kurtz JB, Gary GW, Lin FC, Kapikian AZ. Characterization and seroepidemiology of a type 5 astrovirus associated with an outbreak of gastroenteritis in Marin County, California. J Clin Microbiol 1993; 31: 955–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Treanor JJ, Dolin R. Astroviruses, toroviruses, and picobirnaviruses In: Mandell GL, Bennet JE, Dolin R, eds. Principles and practice of infectious diseases. New York: Churchill Livingstone, 2000: 1956–8. [Google Scholar]
- 74. Berke T, Golding B, Jiang X et al. Phylogenetic analysis of caliciviruses. J Med Virol 1997; 52: 419–24. [DOI] [PubMed] [Google Scholar]
- 75. Prasad BVV, Hardy ME, Dokland T, Bella J, Rossmann MG, Estes MK. X‐ray crystallographic structure of the Norwalk virus capsid. Science 1999; 286: 287–90. [DOI] [PubMed] [Google Scholar]
- 76. Atmar RL, Estes MK. Diagnosis of noncultivatable gastroenteritis viruses, the human calicivirus. Clin Microbiol Rev 2001; 14: 15–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Seah E, Marshall JA, Wright PJ. Open reading frame 1 of Norwalk‐like virus Camberwell: completion of sequence and expression in mammalian cells. J Virol 1999; 73: 10531–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Liu BL, Clarke NI, Caul EO, Lambden PR. Human enteric caliciviruses have a unique genome structure and are distinct from the Norwalk‐like viruses. Arch Virol 1995; 140: 1345–56. [DOI] [PubMed] [Google Scholar]
- 79. Liu BL, Clarke NI, Caul EO, Lambden PR. The genomic 5′‐terminus of Manchester calicivirus. Virus Genes 1995; 15: 25–8. [DOI] [PubMed] [Google Scholar]
- 80. Green KY, Ando T, Balayan MS et al. Taxonomy of caliciviruses. J Infect Dis 2000; 181(suppl 2): S322–30. [DOI] [PubMed] [Google Scholar]
- 81. Ando T, Noel JS, Frankhauser RL. Genetic classification of Norwalk‐like viruses. J Infect Dis 2000; 181(suppl 2): S336–48. [DOI] [PubMed] [Google Scholar]
- 82. Schreiber DS, Blacklow NR, Trier JS. The small intestinal lesion induced by Hawaii agent acute infectious nonbacterial gastroenteritis. J Infect Dis 1974; 129: 705–8. [DOI] [PubMed] [Google Scholar]
- 83. Treanor JJ, Dolin R. Norwalk virus and other caliciviruses In: Mandell GL, Bennet JE, Dolin R, eds. Principles and practice of infectious diseases. New York: Churchill Livingstone, 2000: 1949–56. [Google Scholar]
- 84. Meeroff JC, Schreiber DS, Trier JS, Blacklow NR. Abnormal gastric motor function in viral gastroenteritis. Ann Intern Med 1980; 92: 370–3. [DOI] [PubMed] [Google Scholar]
- 85. Agus S, Falchuk ZM, Sessoms CS et al. Increased jejunal IgA synthesis in vitro during acute infectious non bacterial gastroenteritis. Am J Dig Dis 1974; 19: 127–31. [DOI] [PubMed] [Google Scholar]
- 86. Horzinek MC. Molecular evolution of corona and toroviruses. Adv Exp Med Biol 1999; 473: 6172. [DOI] [PubMed] [Google Scholar]
- 87. Koopmans M, Goosen ESM, Lima AAM et al. Association of torovirus with acute and persistent diarrhea in children. Pediatr Infect Dis J 1997; 16: 504–7. [DOI] [PubMed] [Google Scholar]
- 88. McIntosh K. Coronaviruses In: Mandell GL, Bennett JE, Dolin R, eds. Principles and practice of infectious diseases. Philadelphia: Churchill Livingstone, 2000: 1767–70. [Google Scholar]
- 89. Holmes KV, Lai MMC. Coronaviridae: the viruses and their replication In: Fields BN, Kipe DM, Howley PM, eds. Virology. Philadelphia: Lippincott‐Raven, 1996: 1075–93. [Google Scholar]
- 90. Glass RI. Other viral agents of gastroenteritis In: Blaser MJ, Smith PD, Raudin JI, Greenberg HB, Guerrant RL, eds. Infections of the gastrointestinal tract. New York: Raven Press, 1995: 1055–64. [Google Scholar]
- 91. Pereira HG, Flewett TH, Candeias JAN, Barth OM. A virus with a bisegmented double‐stranded RNA genome in rat intestines. J Gen Virol 1988; 69: 2749–54. [DOI] [PubMed] [Google Scholar]
- 92. Grohmann GS, Glass RI, Pereira HG et al. Enteric viruses and diarrhea in HIV infected patients. N Engl J Med 1993; 329: 1420. [DOI] [PubMed] [Google Scholar]
- 93. Giordano MO, Martinez LC, Rinaldi D et al. Diarrhea and enteric emerging viruses in HIV infected patients. AIDS Res Hum Retroviruses 1999; 15: 1427–32. [DOI] [PubMed] [Google Scholar]
- 94. Gonzalez GG, Pujol FH, Liprandi F, Deibis L, Ludert JE. Prevalence of enteric viruses in human immunodeficiency virus seropositive patients in Venezuela. J Med Virol 1998; 55: 288–92. [DOI] [PubMed] [Google Scholar]
- 95. Gallimore CL, Appleton H, Lewis D, Green J, Brown DW. Detection and characterization of bisegmented double stranded RNA viruses (picobirnaviruses) in human fecal specimens. J Med Virol 1995; 45: 135–40. [DOI] [PubMed] [Google Scholar]
- 96. Cascio A, Bosco M, Giammanco A, Ferraro D, Arista S. Identification of picobirnavirus from feces of Italian children suffering from acute diarrhea. Eur J Epidemiol 1996; 12: 545–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Liste MB, Natera I, Suarez JA, Pujol FH, Liprandi F, Ludert JE. Enteric virus infection and diarrhea in healthy and human immunodeficiency virus infected children. J Clin Microbiol 2000; 38: 2873–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Glass RI, Gentsch J, Smith JC. Rotavirus vaccines: success by reassortment. Science 1994; 265: 1389–91. [DOI] [PubMed] [Google Scholar]
- 99. Glass RI, Bresee JS, Parashar UD, Holman RC, Gentsch JR. First rotavirus vaccines licensed: is there really a need? Acta Paediatr Suppl 1999; 88: 2–8. [DOI] [PubMed] [Google Scholar]
- 100. Cama RI, Parashar UD, Taylor DN et al. Enteropathogens and other factors associated with severe disease in children with acute watery diarrhea in Lima, Peru. J Infect Dis 1999; 179: 1139–44. [DOI] [PubMed] [Google Scholar]
- 101. Cunliffe NA, Kilgore PE, Bresee JS et al. Epidemiology of rotavirus diarrhea in Africa: a review to assess the need for rotavirus immunization. Bull WHO 1998; 76: 525–37. [PMC free article] [PubMed] [Google Scholar]
- 102. Unicomb LE, Kilgore PE, Faruque ASG et al. Anticipating rotavirus vaccines: hospital‐based surveillance for rotavirus diarrhea and estimates of disease burden in Bangladesh. Pediatr Infect Dis J 1997; 16: 947–51. [DOI] [PubMed] [Google Scholar]
- 103. Caprioli A, Pezzella C, Morelli R et al. Enteropathogens associated with childhood diarrhea in Italy. Pediatr Infect Dis J 1996; 15: 876–83. [DOI] [PubMed] [Google Scholar]
- 104. Johansen K, Bennet R, Bondesson K et al. Incidence and estimates of the disease burden of rotavirus in Sweden. Acta Paediatr Suppl 1999; 88: 20–3. [DOI] [PubMed] [Google Scholar]
- 105. Matson DO, Estes MK. Impact of rotavirus infection at a large pediatric hospital. J Infect Dis 1990; 162: 598–604. [DOI] [PubMed] [Google Scholar]
- 106. Mrukowicz JZ, Krobicka B, Duplaga M et al. Epidemiology and impact of rotavirus diarrhoea in Poland. Acta Paediatr Suppl 1999; 88: 53–60. [DOI] [PubMed] [Google Scholar]
- 107. Ruuska T, Vesikari T. A prospective study of acute diarrhoea in Finnish children from birth to 2½ years of age. Acta Paediatr Scand 1991; 80: 500–7. [DOI] [PubMed] [Google Scholar]
- 108. Szücs G, Uj M, Mihály I, Deák J. Burden of human rotavirus‐associated hospitalizations in three geographic regions of Hungary. Acta Paediatr Suppl 1999; 88: 61–5. [DOI] [PubMed] [Google Scholar]
- 109. Barnes GL, Uren U, Stevens KB, Bishop RF. Etiology of acute gastroenteritis in hospitalized children in Melbourne, Australia, from April 1980 to March 1993. J Clin Microbiol 1998; 36: 133–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Glass RI, Kilgore PE, Holman RC et al. The epidemiology of rotavirus diarrhea in the United States: surveillance and estimates of disease burden. J Infect Dis 1996; 174(suppl 1): S5–11. [DOI] [PubMed] [Google Scholar]
- 111. Fang ZY, Ye Q, Ho MS et al. Investigation of an outbreak of adult diarrhea rotavirus in China. J Infect Dis 1989; 160: 948–53. [DOI] [PubMed] [Google Scholar]
- 112. Otsu R. A mass outbreak of gastroenteritis associated with group C rotaviral infection in schoolchildren. Comp Immunol Microbiol Infect Dis 1998; 21: 75–80. [DOI] [PubMed] [Google Scholar]
- 113. Souza DF, Kisielius JJ, Ueda M et al. An outbreak of group C rotavirus gastroenteritis among adults living in Valentim Gentil, Sao Paulo state, Brazil. J Diarrhoeal Dis Res 1998; 16: 59–65. [PubMed] [Google Scholar]
- 114. Bonsdorf CHV, Svensson L. Human serogroup C rotavirus in Finland. Scand J Infect Dis 1988; 20: 475–8. [DOI] [PubMed] [Google Scholar]
- 115. Caul EO, Ashley CR, Darville JM, Bridger JC. Group C rotavirus associated with fatal enteritis in a family outbreak. J Med Virol 1990; 30: 201–5. [DOI] [PubMed] [Google Scholar]
- 116. Jiang B, Dennehy PH, Spangenberger S, Gentsch JR, Glass RI. First detection of group C rotavirus in fecal specimens of children with diarrhea in the United States. J Infect Dis 1995; 172: 45–50. [DOI] [PubMed] [Google Scholar]
- 117. Kuzuya M, Fujii R, Hamano M et al. Survey of human group C rotaviruses in Japan during the winter of 1992 to 1993. J Clin Microbiol 1998; 36: 6–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. James VLA, Lambden PR, Caul EO, Clarke IN. Enzyme‐linked immunosorbent assay based on recombinant human group C rotavirus inner capsid protein (VP6) to detect human group C rotaviruses in fecal samples. J Clin Microbiol 1998; 36: 3178–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119. Bon F, Fascia P, Dauvergne M et al. Prevalence of group A rotavirus, human calicivirus, astrovirus, and adenovirus type 40 and 41 infections among children with acute gastroenteritis in Dijon, France. J Clin Microbiol 1999; 37: 3055–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120. De Jong JC, Bijlsma K, Wermenbol AG et al. Detection, typing, and subtyping of enteric adenoviruses 40 and 41 from fecal samples and observation of changing incidences of infections with these types and subtypes. J Clin Microbiol 1993; 31: 1562–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121. Grinwood K, Carzino R, Narnes GL, Bishop RF. Patients with enteric adenovirus gastroenteritis admitted to an Australian pediatric teaching hospital from 1981 to 1992. J Clin Microbiol 1995; 33: 131–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122. Kotloff KL, Losonsky GA, Morris JG, Wasserman SS, Singh‐Naz N, Levine MM. Enteric adenovirus infection and childhood diarrhea: an epidemiologic study in three clinical settings. Pediatrics 1989; 84: 219–25. [PubMed] [Google Scholar]
- 123. Shinozaki T, Araki K, Fujita Y, Kobayashi M, Tajima T, Abe T. Epidemiology of enteric adenoviruses 40 and 41 in acute gastroenteritis in infants and young children in the Tokyo area. Scand J Infect Dis 1991; 23: 543–7. [DOI] [PubMed] [Google Scholar]
- 124. Wood DJ, Longhurst D, Killough RI, David TJ. One‐year prospective cross‐sectional study to assess the importance of group F adenovirus infections in children under 2 years admitted to hospital. J Med Virol 1988; 26: 429–35. [DOI] [PubMed] [Google Scholar]
- 125. Cruz JR, Cáceres P, Cano F, Flores J, Bartlett A, Torún B. Adenovirus types 40 and 41 and rotaviruses associated with diarrhea in children from Guatemala. J Clin Microbiol 1990; 28: 1780–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Kim K‐H, Yang J‐M, Joo S‐I, Cho Y‐G, Glass RI, Cho Y‐J. Importance of rotavirus and adenovirus types 40 and 41 in acute gastroenteritis in Korean children. J Clin Microbiol 1990; 28: 2279–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127. Qiao H, Nilsson M, Abreu ER et al. Viral diarrhea in children in Beijing, China. J Med Virol 1999; 57: 390–6. [PubMed] [Google Scholar]
- 128. Stewien KE, Mos EN, Yanaguita RM et al. Viral, bacterial and parasitic pathogens associated with severe diarrhoea in the city of Sao Paulo, Brazil. J Diarrhoeal Dis Res 1993; 11: 148–52. [PubMed] [Google Scholar]
- 129. Glass RI, Noel J, Mitchell D et al. The changing epidemiology of astrovirus‐associated gastroenteritis: a review. Arch Virol Suppl 1996; 12: 287–300. [DOI] [PubMed] [Google Scholar]
- 130. Lew JF, Glass RI, Petric M et al. Six year retrospective surveillance of gastroenteritis viruses identified at ten electron microscopy centers in the United States and Canada. Pediatr Infect Dis J 1990; 9: 709–14. [DOI] [PubMed] [Google Scholar]
- 131. Monroe SS, Glass RI, Noah N et al. Electronmicroscopic reporting of gastrointestinal viruses in the United Kingdom. J Med Virol 1991; 33: 193–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Herrmann JE, Nowak NA, Perron‐Henry DM, Hudson RW, Cubitt WD, Blacklow NR. Diagnosis of astrovirus gastroenteritis by antigen detection with monoclonal antibodies. J Infect Dis 1990; 161: 226–9. [DOI] [PubMed] [Google Scholar]
- 133. Cruz JR, Bartlett AV, Herrmann JE, Cáceres P, Blacklow NR, Cano F. Astrovirus‐associated diarrhea among Guatemalan ambulatory rural children. J Clin Microbiol 1992; 30: 1140–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Gómez López A, Díez R, Coperias JL, Ladrón de Guevara C. Astrovirus infection in children with gastroenteritis. Enferm Infecc Microbiol Clin 2001; 19: 199–201. [DOI] [PubMed] [Google Scholar]
- 135. López L, Castillo FJ, Fernández MA et al. Astrovirus infection among children with gastroenteritis in the city of Zaragoza, Spain. Eur J Clin Microbiol Infect Dis 2000; 19: 545–7. [DOI] [PubMed] [Google Scholar]
- 136. Kotloff KL, Herrmann JE, Blacklow NR et al. The frequency of astrovirus as a cause of diarrhea in Baltimore children. Pediatr Infect Dis J 1992; 11: 587–9. [PubMed] [Google Scholar]
- 137. Lew JF, Moe CL, Monroe SS et al. Astrovirus and adenovirus associated with diarrhea in children in day care settings. J Infect Dis 1991; 164: 673–8. [DOI] [PubMed] [Google Scholar]
- 138. Guix S, Caballero S, Villena C et al. Molecular epidemiology of astrovirus infection in Barcelona, Spain. J Clin Microbiol 2002; 40: 133–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139. Guerrero ML, Noel JS, Mitchell DK et al. A prospective study of astrovirus diarrhea of infancy in Mexico city. Pediatr Infect Dis J 1998; 17: 723–7. [DOI] [PubMed] [Google Scholar]
- 140. Pang XL, Vesikari T. Human‐astrovirus associated gastroenteritis in children under 2 years of age followed prospectively during a rotavirus vaccine trial. Acta Paediatr 1999; 88: 532–6. [DOI] [PubMed] [Google Scholar]
- 141. Maldonado Y, Cantwell M, Old M et al. Population‐based prevalence of symptomatic and asymptomatic astrovirus infection in rural Mayan infants. J Infect Dis 1998; 178: 334–9. [DOI] [PubMed] [Google Scholar]
- 142. Kapikian AZ, Estes MK, Chanock RM. Norwalk group of viruses In: Fields BN, Knipe DM, Howley PM, eds. Virology, 3rd edn Philadelphia: Lippincott‐Raven, 1996: 783–810. [Google Scholar]
- 143. Frankhauser RL, Noel JS, Monroe SS, Ando TA, Glass RI. Molecular epidemiology of Norwalk‐like viruses in outbreaks of gastroenteritis in the United States. J Infect Dis 1998; 178: 1571–8. [DOI] [PubMed] [Google Scholar]
- 144. Koopmans M, Vinjé J, De Wit M, Leenen I, Poel W, Duynhoven Y. Molecular epidemiology of human enteric caliciviruses in The Netherlands. J Infect Dis 2000; 181(suppl 2): S262–9. [DOI] [PubMed] [Google Scholar]
- 145. Mead PS, Slutzker L, Dietz V et al. Food‐related illness and death in the United States. Emerg Infect Dis 1999; 5: 607–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146. Nakata S, Honma S, Numata K‐K et al. Members of the family Caliciviridae (Norwalk virus and Sapporo virus) are the most prevalent cause of gastroenteritis outbreaks among infants in Japan. J Infect Dis 2000; 181: 2029–32. [DOI] [PubMed] [Google Scholar]
- 147. Vinjé J. The incidence and genetic variability of small round structured viruses in outbreaks of gastroenteritis in the Netherlands. J Infect Dis 1997; 176: 1374–8. [DOI] [PubMed] [Google Scholar]
- 148. Lew JF, Valdesuso J, Vesikari T et al. Detection of Norwalk virus or Norwalk‐like virus infections in Finnish infants and young children. J Infect Dis 1994; 169: 1364–7. [DOI] [PubMed] [Google Scholar]
- 149. Pang X‐L, Honma S, Nakata S, Vesikari T. Human caliciviruses in acute gastroenteritis of young children in the community. J Infect Dis 2000; 181(suppl 2): S288–94. [DOI] [PubMed] [Google Scholar]
- 150. Pang X‐L, Joensuu J, Vesikari T. Human calicivirus‐associated sporadic gastroenteritis in Finnish children less than two years of age followed prospectively during a rotavirus vaccine trial. Pediatr Infect Dis J 1999; 18: 420–6. [DOI] [PubMed] [Google Scholar]
- 151. Blacklow NR, Greenberg HB. Viral gastroenteritis. N Engl J Med 1991; 325: 252–64. [DOI] [PubMed] [Google Scholar]
- 152. Krajden M, Brown M, Petrasek A, Middleton PJ. Clinical features of adenovirus enteritis: a review of 127 cases. Pediatr Infect Dis 1990; 9: 636–41. [PubMed] [Google Scholar]
- 153. Bishop RF. Natural history of human rotavirus infection. Arch Virol Suppl 1996; 12: 119–28. [DOI] [PubMed] [Google Scholar]
- 154. Cohen MB, Laney DW. Infectious diarrhea In: Wyllie R, Hyams JS, eds. Pediatric gastrointestinal disease: pathophysiology, diagnosis, management. Philadelphia: WB Saunders, 1999: 348–70. [Google Scholar]
- 155. Haffejee IE. The epidemiology of rotavirus infection: a global perspective. J Pediatr Gastroenterol Nutr 1995; 20: 275–86. [DOI] [PubMed] [Google Scholar]
- 156. Das BK, Gentsch JR, Cicirello HG et al. Characterization of rotavirus strains from newborns in New Delhi, India. J Clin Microbiol 1994; 32: 1820–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157. Espinoza F, Paniagua M, Hallander H, Svensson L, Strannegard O. Rotavirus infections in young Nicaraguan children. Pediatr Infect Dis J 1997; 16: 564–71. [DOI] [PubMed] [Google Scholar]
- 158. Ruuska T, Vesikari T. Rotavirus disease in Finnish children: use of numerical scores for clinical severity of diarrhoeal episodes. Scand J Infect Dis 1990; 22: 259–67. [DOI] [PubMed] [Google Scholar]
- 159. Velazquez FR, Matson DO, Calva JJ et al. Rotavirus infection in infants as protection against subsequent infections. N Engl J Med 1996; 335: 1022–8. [DOI] [PubMed] [Google Scholar]
- 160. Jarecki‐Khan K, Tzipori SR, Unicomb LE. Enteric adenovirus infection among infants with diarrhea in rural Bangladesh. J Clin Microbiol 1993; 31: 484–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161. Reina J, Hervás J, Ros MJ. Differential clinical characteristics among pediatric patients with gastroenteritis caused by rotavirus and adenovirus. Enferm Infecc Microbiol Clin 1994; 12: 378–84. [PubMed] [Google Scholar]
- 162. Herrmann JE, Taylor PD, Echeverría P, Blacklow NR. Astroviruses as a cause of gastroenteritis in children. N Engl J Med 1991; 324: 1757–60. [DOI] [PubMed] [Google Scholar]
- 163. Cone R, Mohan K, Thouless M, Corey L. Nosocomial transmission of rotavirus infection. Pediatr Infect Dis J 1988; 7: 103–9. [DOI] [PubMed] [Google Scholar]
- 164. Mesa F, Lajo A, Alonso F, Borque C, Segurado E, Ladrón de Guevara C. Rotavirus infection: clinical characteristics and time of elimination of rotavirus antigen in the feces. Enferm Infecc Microbiol Clin 1996; 14: 106–10. [PubMed] [Google Scholar]
- 165. Bennet R, Hedlund KO, Ehrnst A, Eriksson M. Nosocomial gastroenteritis in two infant wards over 26 months. Acta Paediatr 1995; 84: 667–71. [DOI] [PubMed] [Google Scholar]
- 166. Rodriguez Cervilla J, Peñalver MD, Curros MC, Pavón P, Alonso C, Fraga JM. Rotavirus: clinical and epidemiological study in hospitalized children under two years of age. An Esp Pediatr 1996; 45: 499–504. [PubMed] [Google Scholar]
- 167. Ford‐Jones EL, Mindorff CM, Gold R, Petric M. The incidence of viral‐associated diarrhea after admission to a pediatric hospital. Am J Epidemiol 1990; 131: 711–18. [DOI] [PubMed] [Google Scholar]
- 168. Shastri S, Doane AM, Gonzales J, Upadhyayula U, Bass DM. Prevalence of astroviruses in a children's hospital. J Clin Microbiol 1998; 36: 2571–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169. Lew JF, Petric M, Kapikian AZ, Jiang X, Estes MK, Green KY. Identification of minireovirus as a Norwalk‐like virus in pediatric patients with gastroenteritis. J Virol 1994; 68: 3391–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170. Struve J, Bennet R, Ehrnst A et al. Nosocomial calicivirus gastroenteritis in a pediatric hospital. Pediatr Infect Dis J 1994; 13: 882–5. [DOI] [PubMed] [Google Scholar]
- 171. Caceres VM, Kim DK, Bresee JS et al. A viral gastroenteritis outbreak associated with person‐to‐person spread among hospital staff. Infect Control Hosp Epidemiol 1998; 19: 162–7. [DOI] [PubMed] [Google Scholar]
- 172. Dennehy PH, Tente WE, Fisher DJ, Veloudis BA, Peter G. Lack of impact of rapid identification of rotavirus‐infected patients on nosocomial rotavirus infections. Pediatr Infect Dis J 1989; 8: 290–6. [PubMed] [Google Scholar]
- 173. Matson D, Estes MK, Tananka T, Bartlett AV, Pickering LK. Asymptomatic human calicivirus infection in a day care center. Pediatr Infect Dis J 1990; 9: 190–6. [DOI] [PubMed] [Google Scholar]
- 174. Ojeh CK, Cusak TM, Yolken RH. Evaluation of the effects of disinfectants on rotavirus RNA and infectivity by the polymerase chain reaction and cell‐culture methods. Mol Cell Prob 1995; 9: 341–6. [DOI] [PubMed] [Google Scholar]
- 175. Sattar SA, Jacobsen H, Rahman H, Cusack M, Rubino JR. Interruption of rotavirus spread through chemical disinfection. Infect Control Hosp Epidemiol 1994; 15: 751–6. [DOI] [PubMed] [Google Scholar]
- 176. Goodgame RW. Viral causes of diarrhea. Gastroenterol Clin North Am 2001; 30: 779–95. [DOI] [PubMed] [Google Scholar]
- 177. Hardy M. Norwalk and Norwalk‐like viruses in epidemic gastroenteritis. Clin Lab Med 1999; 19: 675–90. [PubMed] [Google Scholar]
- 178. Nakata S, Honma S, Numata K et al. Prevalence of human calicivirus infection in Kenya as determined by enzyme immunoassay for three genogroups of the virus. J Clin Microbiol 1998; 36: 3160–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179. Pelosi E, Lambden P, Caul E et al. The seroepidemiology of genogroup I and genogroup II Norwalk‐like virus in Italy. J Med Virol 1999; 58: 93–9. [PubMed] [Google Scholar]
- 180. Hardy D. Epidemiology of rotaviral infection in adults. Rev Infect Dis 1987; 9: 461–9. [DOI] [PubMed] [Google Scholar]
- 181. Halvorsrud J, Orstavik I. An epidemic of rotavirus‐associated gastroenteritis in a nursing home for the elderly. J Infect Dis 1980; 12: 161–4. [DOI] [PubMed] [Google Scholar]
- 182. Belliot G, Laveran H, Monroe S. Outbreaks of gastroenteritis in military recruits associated with serotype 3 astrovirus infection. J Med Virol 1997; 51: 101–6. [DOI] [PubMed] [Google Scholar]
- 183. Yuen K, Woo P, Liang R et al. Clinical significance of alimentary tract microbes in bone marrow transplant recipients. Diagn Microbiol Infect Dis 1998; 30: 75–81. [DOI] [PubMed] [Google Scholar]
- 184. Pirsch J. Cytomegalovirus infection and posttransplant lymphoproliferative disease in renal transplant. Results of the US multicenter FK 506 Kidney Transplant Study Group. Transplantation 1999; 68: 1203–5. [DOI] [PubMed] [Google Scholar]
- 185. Bini E, Cohen J. Diagnostic yield and cost‐effectiveness of endoscopy in chronic human immunodeficiency virus related diarrhea. Gastrointest Endosc 1998; 48: 354–61. [DOI] [PubMed] [Google Scholar]
- 186. Weber R, Ledergerber B, Zbinden R et al. Enteric infections and diarrhea in human immunodeficiency virus‐infected persons: prospective community‐based cohort study. Arch Intern Med 1999; 159: 1473–80. [DOI] [PubMed] [Google Scholar]
- 187. Hale G, Heslop H, Krance R et al. Adenovirus infection after pediatric bone marrow transplantation. Bone Marrow Transplant 1999; 23: 277–82. [DOI] [PubMed] [Google Scholar]
- 188. Cox G, Matsui S, LO R et al. Etiology and outcome of diarrhea after bone marrow transplantation. Gastroenterology 1994; 107: 1398–407. [DOI] [PubMed] [Google Scholar]
- 189. Petric M. Caliciviruses, astroviruses and other diarrheic viruses In: Murray PR, Baron EJ, Pfaller MA, Tenover FC, Yolken RH, eds. Manual of clinical microbiology. Washington: ASM Press, 1999: 1005–13. [Google Scholar]
- 190. Sherlock CH, Brandt CJ, Middleton PJ, Smith JA. Laboratory diagnosis of viral infections producing enteritis In: Smith JA, ed. Cumitech 26. Washington DC: American Society for Microbiology, 1989:. 1–12. [Google Scholar]
- 191. Dennehy PH, Gauntlett DR, Spangenberger SE. Choice of reference assay for the detection of rotaviruses in fecal specimens: electron microscopy versus enzyme inmunoassay. J Clin Microbiol 1990; 28: 1280–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192. Singh‐Naz N, Rodriguez WJ, Kidd AH, Brandt CD. Monoclonal antibody enzyme linked immunosorbent assay for specific identification and typing of subgroup F adenoviruses. J Clin Microbiol 1988; 26: 297–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 193. Dennehy PH, Gaultlett DR, Tente WE. Comparison of nine commercial inmunoassays for detection of rotaviruses in fecal specimens. J Clin Microbiol 1988; 26: 1630–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194. Thomas EE, Puterman ML, Kawano E, Curran M. Evaluation of seven immunoassays for detection of rotavirus in pediatric stool samples. J Clin Microbiol 1988; 26: 1189–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 195. Dennehy PH, Hartin M, Nelson SM, Reising SF. Evaluation of the InmunoCards TAT rotavirus assay for detection of group A rotavirus in fecal specimens. J Clin Microbiol 1999; 37: 1977–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 196. Wilhelmi I, Colomina J, Martín‐Rodrigo D, Román E, Sánchez‐Fauquier A. New immunochromatographic method for rapid detection of rotaviruses in stool samples compared with standard enzyme immunoassay and latex agglutination techniques. Eur J Clin Microbiol Infect Dis 2000; 20: 741–3. [DOI] [PubMed] [Google Scholar]
- 197. Fujii R, Kuzuya M, Hamano M, Yamada M, Yamazaki S. Detection of human group C rotaviruses by an enzyme‐linked immunosorbent assay using monoclonal antibodies. J Clin Microbiol 1992; 30: 1307–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198. Moore PL, Steele AD, Alexander JJ. Relevance of commercial diagnostic tests to detection of enteric adenovirus infections in South Africa. J Clin Microbiol 2000; 38: 1661–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199. Noel J, Mansoor A, Thaker U, Herrmann J, Perron‐Henry D, Cubitt WD. Identification of adenoviruses in faeces from patients with diarrhoea at the hospitals for sick children, London, 1989–1992. J Med Virol 1994; 43: 84–90. [DOI] [PubMed] [Google Scholar]
- 200. Moe CL, Allen JR, Monroe SS et al. Detection of astrovirus in pediatric stool samples by immunoassay and RNA probe. J Clin Microbiol 1991; 29: 2390–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 201. Putzker M, Sauer H, Kirchner G, Keksel O, Malic A. Community acquired diarrhea—the incidence of astrovirus infections in Germany. Clin Lab 2000; 46: 269–73. [PubMed] [Google Scholar]
- 202. Jiang X, Wilton N, Zhong WM et al. Diagnosis of human caliciviruses by use of enzyme immunoassays. J Infect Dis 2000; 181(suppl 2): S349–59. [DOI] [PubMed] [Google Scholar]
- 203. Buesa J, Colomina J, Raga J, Villanueva A, Prat J. Evaluation of reverse transcription and polymerase chain reaction (RT/PCR) for the detection of rotaviruses: applications of the assay. Res Virol 1996; 157: 353–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 204. Cubitt WD, Mitchell DK, Carter MJ, Willcocks MM, Holzel H. Application of electronmicroscopy, enzyme immunoassay, and RT‐PCR to monitor an outbreak of astrovirus type 1 in a pediatric bone marrow transplant unit. J Med Virol 1999; 57: 313–21. [DOI] [PubMed] [Google Scholar]
- 205. Mustafa H, Palombo EA, Bishop RF. Improved sensitivity of astrovirus‐specific RT‐PCR following culture of stool samples in CaCO‐2 cells. J Clin Virol 1998; 11: 103–7. [DOI] [PubMed] [Google Scholar]
- 206. Pang XL, Joensuu J, Hoshino Y, Kapikian AZ, Vesikari T. Rotaviruses detected by reverse transcription polymerase chain reaction in acute gastroenteritis during a trial of rhesus–human reassortant rotavirus tetravalent vaccine: implications for vaccine efficacy analysis. J Clin Virol 1999; 13: 9–6. [DOI] [PubMed] [Google Scholar]
- 207. Allard A, Albinsson B, Wadell G. Detection of adenoviruses in stools from healthy persons and patients with diarrhea by two‐step polymerase chain reaction. J Med Virol 1992; 37: 149–57. [DOI] [PubMed] [Google Scholar]
- 208. Mitchell DK, Monroe SS, Jiang X, Matson DO, Glass RI, Pickering LK. Virologic features of an astrovirus diarrhea outbreak in a day care center revealed by reverse transcriptase–polymerase chain reaction. J Infect Dis 1995; 172: 1437–44. [DOI] [PubMed] [Google Scholar]
- 209. Jiang X, Matson DO, Cubitt WD, Estes MK. Genetic and antigenic diversity of human caliciviruses (HuCVs) using RT‐PVR and new EIAs. Arch Virol Suppl 1996; 12: 251–62. [DOI] [PubMed] [Google Scholar]
- 210. Le Guyader F, Estes MK, Hardy ME et al. Evaluation of a degenerate primer for the PCR detection of human caliciviruses. Arch Virol 1996; 141: 2225–35. [DOI] [PubMed] [Google Scholar]
- 211. Vinjé J, Koopmans MPG. Molecular detection and epidemiology of small round structured viruses in outbreaks of gastroenteritis in The Netherlands. J Infect Dis 1996; 174: 610–15. [DOI] [PubMed] [Google Scholar]
- 212. Vinjé J, Deijl H, Reina H et al. Molecular detection and epidemiology of Sapporo‐like viruses. J Clin Microbiol 2000; 38: 530–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 213. Gentsch JR, Woods PA, Ramachandran M et al. Review of G and P typing results from a global collection of rotavirus strains: implications for vaccine development. J Infect Dis 1996; 174(suppl 1): S30–6. [DOI] [PubMed] [Google Scholar]
- 214. Gentsch JR, Glass RI, Woods P et al. Identification of group A rotavirus genes 4 types by polymerase chain reaction. J Clin Microbiol 1992; 30: 1365–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 215. ESPGAN Working Group on Acute Diarrhoea. Recommendations for feeding in childhood gastroenteritis. J Pediatr Gastroenterol Nutr 1997; 24: 619–20. [DOI] [PubMed] [Google Scholar]
- 216. Joensuu J, Koskenniemi E, Vesikari T. Prolonged efficacy of rhesus–human reassortant rotavirus vaccine. Pediatr Infect Dis 1998; 17: 427–9. [DOI] [PubMed] [Google Scholar]
- 217. Centers for Disease Control and Prevention. Rotavirus vaccine for the prevention of rotavirus gastroenteritis among children. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1999; 48: 1–23. [PubMed] [Google Scholar]
- 218. Advisory Committee on Immunization Practices (ACIP). Centers for Disease Control and Prevention. Withdrawal of rotavirus vaccine recommendation. MMWR 1999; 48: 1007. 10577495 [Google Scholar]
- 219. Centers for Disease Control and Prevention. Intussusception among recipients of rotavirus vaccine—United States, 1998–1999. MMWR 1999; 48: 577–81. [PubMed] [Google Scholar]
- 220. Bresee JS, Glass RI, Ivanoff B, Gentsch JR. Current status and future priorities for rotavirus vaccine development, evaluation and implementation in developing countries. Vaccine 1999; 17: 2207–22. [DOI] [PubMed] [Google Scholar]
- 221. Wilhelmi I, Mier C, Román E, Colomina J, Prat J, Sánchez‐Fauquier A. Molecular epidemiology of rotavirus in Spanish children. Enferm Infecc Microbiol Clin 1999; 17: 509–14. [PubMed] [Google Scholar]
- 222. Jain V, Das BK, Bhan MK, Glass RI, Gentsch JR. Great diversity of group A rotavirus strains and high prevalence of mixed rotavirus infection in India. J Clin Microbiol 2001; 39: 3524–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 223. Das S, Sen A, Uma G et al. Genomic diversity of group A rotavirus strains infecting humans in eastern India. J Clin Microbiol 2002; 40: 146–9. [DOI] [PMC free article] [PubMed] [Google Scholar]