

Abstract
Objective
To investigate the occurrence of olfactory and gustatory dysfunctions in patients with laboratory-confirmed COVID-19 infection.
Methods
Patients with laboratory-confirmed COVID-19 infection were recruited from 12 European hospitals. The following epidemiological and clinical outcomes have been studied: age, sex, ethnicity, comorbidities, and general and otolaryngological symptoms. Patients completed olfactory and gustatory questionnaires based on the smell and taste component of the National Health and Nutrition Examination Survey, and the short version of the Questionnaire of Olfactory Disorders-Negative Statements (sQOD-NS).
Results
A total of 417 mild-to-moderate COVID-19 patients completed the study (263 females). The most prevalent general symptoms consisted of cough, myalgia, and loss of appetite. Face pain and nasal obstruction were the most disease-related otolaryngological symptoms. 85.6% and 88.0% of patients reported olfactory and gustatory dysfunctions, respectively. There was a significant association between both disorders (p < 0.001). Olfactory dysfunction (OD) appeared before the other symptoms in 11.8% of cases. The sQO-NS scores were significantly lower in patients with anosmia compared with normosmic or hyposmic individuals (p = 0.001). Among the 18.2% of patients without nasal obstruction or rhinorrhea, 79.7% were hyposmic or anosmic. The early olfactory recovery rate was 44.0%. Females were significantly more affected by olfactory and gustatory dysfunctions than males (p = 0.001).
Conclusion
Olfactory and gustatory disorders are prevalent symptoms in European COVID-19 patients, who may not have nasal symptoms. The sudden anosmia or ageusia need to be recognized by the international scientific community as important symptoms of the COVID-19 infection.
Electronic supplementary material
The online version of this article (10.1007/s00405-020-05965-1) contains supplementary material, which is available to authorized users.
Keywords: Coronavirus, COVID, COVID-19, SARS-CoV-2, Anosmia, Smell, Hyposmia, Dysgeusia, Taste, Loss, Gustatory, Olfactory, Olfaction, Infection, ENT
Introduction
The coronavirus disease 2019 (COVID-19) is an ongoing viral pandemic that emerged from East Asia and quickly spread to the rest of the world [1]. This infection is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and is so far responsible for more than 15,000 deaths worldwide [2]. Human-to-human transmission is characterized by a troubling exponential rate, which has led to steep curves of onset in many areas [3]. According to the clinical studies from Asia, the most prevalent symptoms consist of fever, cough, dyspnea, sputum production, myalgia, arthralgia, headache, diarrhea, rhinorrhea, and sore throat [4, 5]. The spread of the COVID-19 infection in Europe has highlighted a new atypical presentation of the disease: patients with olfactory and gustatory dysfunctions. The occurrence of smell dysfunction in viral infections is not new in otolaryngology. Many viruses may lead to olfactory dysfunction (OD) through an inflammatory reaction of the nasal mucosa and the development of rhinorrhea; the most familiar agents being rhinovirus, parainfluenza Epstein–Barr virus, and some coronavirus [6, 7]. However, olfactory dysfunction linked to COVID-19 infection seems particular as it is not associated with rhinorrhea.
Over the past few weeks, some European otolaryngologists observed that many patients infected by SARS-CoV-2 presented with severe olfactory and gustatory dysfunctions without rhinorrhea or nasal obstruction. At baseline, no COVID-19 was suspected in some of these patients, because they had no fever, cough, or other systemic complaints. Faced with numerous reports from otolaryngologists all around Europe, the Young-Otolaryngologists of the International Federation of Oto-rhino-laryngological Societies (YO-IFOS) decided to conduct an international epidemiological study to characterize olfactory and gustatory disorders in infected patients.
The aim of this study is to investigate and characterize the occurrence of olfactory and gustatory disorders in patients with laboratory-confirmed COVID-19 infection.
Materials and methods
Three ethics committees approved the current study protocol (HAP2020-011; CHUSP20032020; EpiCURA-2020-2303). Patients were invited to participate and the informed consent was obtained.
Subjects and setting
The clinical data of patients with laboratory-confirmed COVID-19 infection have been collected from four Belgian Hospitals (CHU Saint-Pierre, Brussels; CHU Ambroise Paré, Mons; EpiCURA, Baudour; EpiCURA, Ath), and University of Mons (Belgium). In addition to these ones, many other patients, infected physicians and nurses have been voluntarily enrolled in the study from the following hospitals: Foch Hospital (Paris, France); Ambroise Paré Hospital (AP-HP, Paris), CHU Ambroise Paré (Mons, Belgium), Hospital Universitario Donostia (Donostia, Spain); Hospital Universitario Santiago de Compostela (Santiago de Compostela, Spain); Morgagni Pierantoni Hospital (Forli, Italy), Department of Neuroscience, Audiology Unit (Padova University, Treviso, Italy), and Medical Departments of the Università degli Studi della Campania ‘Luigi Vanvitelli’ (Naples, Italy).
The following inclusion criteria have been considered: adult (> 18 years old); laboratory-confirmed COVID-19 infection (reverse transcription polymerase chain reaction, RT-PCR); native speaker patients, and patients clinically able to fulfill the questionnaire. The following exclusion criteria have been considered: patients with olfactory or gustatory dysfunctions before the epidemic; patients without a laboratory-confirmed COVID-19 infection diagnosis; patients who were in the intensive-care unit at the time of the study (due to their health status). Thus, we mainly included mild-to-moderate COVID-19 patients, defined as patients without need of intensive cares. Since we focused on the prevalence of olfactory and gustatory disorders, clinical presentation was not considered in as inclusion criteria.
Clinical outcomes
Clinical data have been prospectively collected during the ear, nose, and throat (ENT) consultation; in the patient’s room; or over the phone for house-bound patients or infected health professionals. The data were also collected through an online form for house-bound patients. The online questionnaire was created with Professional Survey Monkey (San Mateo, CA, USA), so that each participant could complete the survey only once.
The selection of the relevant epidemiological and clinical features composing the questionnaire was carried out by the COVID-19 Task Force of YO-IFOS, which includes otolaryngologists from North America, Europe, and Asia [8]. Experts analyzed the epidemiological publications of the current and the previous coronavirus infections, including SRAS-CoV-1 (2002); Middle-East respiratory syndrome-related coronavirus infection (MERS-CoV, 2012), and the COVID-19 infection. From the literature, ten experts (JRL, SS, MH, JHS, PL, TA, LD, FEA, CCH, and CMCE) developed the questionnaire, which consisted of four general questions (age, sex, ethnicity, and date of diagnosis); three general clinical questions (comorbidities, general, and ENT symptoms associated with COVID-19 infection); seven questions about olfactory function; four questions investigating gustatory function; and one question about the treatment of the COVID-19 infection. All patients were asked to complete the short version of the Questionnaire of Olfactory Disorders-Negative Statements (sQOD-NS) [9]. The questionnaire has been translated into Spanish, Italian, and English by two native speaker otolaryngologists for each language.
Olfactory and gustatory outcomes
The occurrence of anosmia or hyposmia has been identified in the questionnaire. The impact of olfactory dysfunction on the quality of life (QoL) of patients has been assessed through the validated sQOD-NS (Appendix 1) [9]. This is a seven-item patient-reported outcome questionnaire including social, eating, annoyance, and anxiety questions. Each item is rated on a scale of 0–3, with higher scores reflecting better olfactory-specific QoL. The total score ranges from 0 (severe impact on QoL) to 21 (no impact on QoL) [9]. The rest of the olfactory and gustatory questions were based on the smell and taste component of the National Health and Nutrition Examination Survey [10]. This population survey was implemented by the Centers for Disease Control and Prevention to continuously monitor the health of adult citizens in the United States through a nationally representative sample of 5000 persons yearly [10]. The questions have been chosen to characterize the variation, timing, and associated symptoms of both olfactory and gustatory dysfunctions, and, therefore, they suggest a potential etiology. Note that we assessed the mean recovery time of olfaction through four defined propositions: 1–4 days; 5–8 days; 9–14 days; and > 15 days.
Referring to the studies that have demonstrated that the viral load was significantly decreased after 14 days [11], we assessed the short-term olfaction non-recovery rate on patients exhibiting double criteria: an onset of the infection > 14 days before the assessment and the lack of general symptoms at the time of the evaluation.
Statistical methods
Statistical Package for the Social Sciences for Windows (SPSS version 22,0; IBM Corp, Armonk, NY, USA) was used to perform the statistical analyses. The potential associations between epidemiological, clinical and olfactory and gustatory outcomes have been assessed through cross-tab generation between two variables (binary or categorical variables) and Chi-square test. Incomplete responses were excluded from analysis. The differences in sQOD-NS scores between patients regarding the olfactory dysfunction were made through the Kruskal–Wallis test. A level of p < 0.05 was used to determine statistical significance.
Results
A total of 417 patients completed the study. The mean age of patients was 36.9 ± 11.4 years (range 19–77). There were 263 females and 154 males. The following ethnicities composed the cohort: European (93.3%), South American (2.7%), Sub-Saharan African (2.2%), Black African (1.4%), Asian (0.2%), and North American (0.2%) (Table 1). The most prevalent comorbidities of patients were allergic rhinitis, asthma, high blood pressure, and hypothyroidism (Fig. 1). The mean time between the onset of the infection and the evaluation was 9.2 ± 6.2 days. At the time of the study, 34.5% of patients were in the acute phase of the infection, whereas the rest of the patients did not yet have general symptoms.
Table 1.
Demographic and epidemiological characteristics of patients
| Characteristics | Mean ± SD | Range |
|---|---|---|
| Age (years old) | 36.9 ± 11.4 | 19–77 |
| Characteristics | Number | Percentages |
|---|---|---|
| Gender | ||
| Male | 154 | 36.9 |
| Female | 263 | 63.1 |
| Ethnicity | ||
| European | 389 | 93.3 |
| Asian | 1 | 0.2 |
| Black African | 6 | 1.4 |
| Sub-Saharan African | 9 | 2.2 |
| North American | 1 | 0.2 |
| South American | 11 | 2.6 |
| Oceanian | 0 | 0.0 |
| Addictions | ||
| Non-smoker | 361 | 86.6 |
| Mild smoker (1–10 cigarettes daily) | 40 | 9.6 |
| Moderate smoker (11–20 cigarettes daily) | 16 | 3.8 |
| Heavy smoker (> 20 cigarettes daily) | 0 | 0.0 |
| Allergic patients | 85 | 20.4 |
SD standard deviation
Fig. 1.

Comorbidities of COVID-19 patients. The ordinate axis consists of percentages of patients with comorbidities in the cohort. Respiratory insufficiency consists of COPD, emphysema, fibrosis, or other chronic disease associated with a respiratory insufficiency. Neurological diseases include Parkinson disease, myasthenia, multiple sclerosis, and all degenerative diseases. COPD chronic obstructive pulmonary disease, CRS chronic rhinosinusitis, GERD gastroesophageal reflux disease
Clinical outcomes
The general symptoms of patients during the infection are described in Fig. 2. Cough, myalgia, loss of appetite, diarrhea, fever, headache, and asthenia were the most prevalent symptoms, accounting for more than 45% of patients. The otolaryngological symptoms most related to the infection are reported in Table 2.
Fig. 2.

General symptoms associated with COVID-19 infection. The ordinate axis consists of percentages of patients with such symptoms associated with the infection
Table 2.
Otolaryngological complaints associated with COVID-19 Infection
| Not related | Somewhat related | Highly related | |||
|---|---|---|---|---|---|
| (0) | (1) | (2) | (3) | (4) | |
| Nasal obstruction | 131 (31.49) | 91 (21.88) | 77 (18.51) | 67 (16.11) | 50 (12.02) |
| Rhinorrhea | 154 (37.11) | 122 (29.40) | 81 (19.52) | 40 (9.64) | 18 (4.34) |
| Postnasal drip | 203 (48.80) | 97 (23.32) | 61 (14.66) | 26 (6.25) | 29 (6.97) |
| Sore throat | 192 (46.15) | 96 (23.08) | 57 (13.70) | 38 (9.13) | 33 (7.93) |
| Face pain/heaviness | 198 (47.60) | 66 (15.87) | 59 (14.18) | 39 (9.38) | 54 (12.98) |
| Ear pain | 310 (74.52) | 45 (10.82) | 32 (7.69) | 16 (3.85) | 13 (3.13) |
| Dysphagia | 24 (22.64) | 40 (37.74) | 24 (22.64) | 11 (10.38) | 7 (6.60) |
| Dyspnea | 218 (52.40) | 83 (19.95) | 61 (14.66) | 35 (8.41) | 19 (4.57) |
Percentages are in brackets. Patients had to rate each of the following symptoms in terms of their relationship with your COVID-19 infection (scale: 0–4, where 0 = not related, 4 = highly related)
Olfactory outcomes
A total of 357 patients (85.6%) had olfactory dysfunction related to the infection. Among them, 284 (79.6%) patients were anosmic and 73 (20.4%) were hyposmic. Phantosmia and parosmia concerned 12.6% and 32.4% of patients during the disease course, respectively. The olfactory dysfunction appeared before (11.8%), after (65.4%) or at the same time as the appearance of general or ENT symptoms (22.8%). Note that 9.4% of patients did not remember the time of onset of olfactory dysfunction and, therefore, were not considered for the percentage evaluation.
Considering the 247 patients with a clinically resolved infection (absence of general and ENT symptoms), the olfactory dysfunction persisted after the resolution of other symptoms in 63.0% of cases. The mean time between the onset of the disease and the assessment of this group of patients was 9.77 ± 5.68 days.
The short-term olfaction recovery rate, which was assessed in 59 clinically cured patients, was 44.0%. The different recovery times of the olfactory function of patients who reported a recovery of the olfactory function are available in Fig. 3. In total, 72.6% of these patients recovered olfactory function within the first 8 days following the resolution of the disease. Among the patients who reported anosmia, then, excluding hyposmic patients, the olfactory function recovered throughout the 8 first days following the resolution of the disease in 67.8% of cases (Fig. 3).
Fig. 3.

Pattern of recovery time for patients with olfactory dysfunction. The ordinate axis consists of percentages of patients. The patients with hyposmia or anosmia had the following recovery times a 1–4 days (33.0%), 5–8 days (39.6%), 9–14 days (24.2%), and more than 15 days (3.3%). The patients with anosmia had the following recovery times b 1–4 days (20.3%), 5–8 days (47.5%), 9–14 days (28.8%), and more than 15 days (3.4%)
In the present study, 76 patients did not suffer from nasal obstruction or rhinorrhea (18.2%). Among them, 20.3% did not report olfactory dysfunction, whereas 66.2% and 13.5% suffered from anosmia and hyposmia, respectively.
The impact of olfactory dysfunction on patient QoL is reported in Table 3. Anosmic patients at the time of the evaluation had a significant lower sQOD-NS score compared with hyposmic and normosmic individuals (p = 0.001; Kruskal–Wallis).
Table 3.
Short version of questionnaire of olfactory disorders-negative statements of patient
| Short version QOD-NS items | Anosmia | Hyposmia | No LS |
|---|---|---|---|
| Changes in my sense of smell isolate me socially | 1.68 ± 0.91* | 2.34 ± 0.75 | 2.53 ± 0.65 |
| The problems with my sense of smell have a negative impact on my daily social activities | 1.37 ± 0.93* | 2.11 ± 0.84 | 2.56 ± 0.69 |
| The problems with my sense of smell make me more irritable | 1.46 ± 0.92* | 2.21 ± 0.82 | 2.64 ± 0.59 |
| Because of the problems with my sense of smell, I eat out less | 1.30 ± 1.09* | 2.12 ± 0.99 | 2.31 ± 1.04 |
| Because of the problems with my sense of smell, I eat less than before (loss of appetite) | 1.00 ± 0.88* | 1.59 ± 0.97 | 2.36 ± 0.90 |
| Because of the problems with my sense of smell, I have to make more effort to relax | 1.67 ± 0.88* | 2.91 ± 0.79 | 2.61 ± 0.60 |
| I’m afraid I’ll never be able to get used to the problems with my sense of smell. | 0.73 ± 0.86* | 1.90 ± 1.06 | 2.06 ± 1.19 |
| Short version QOD-NOS total score | 9.15 ± 4.60* | 14.44 ± 4.59 | 13.60 ± 8.17 |
sQOD-NS is a seven-item patient-reported outcome questionnaire including social, eating, annoyance, and anxiety questions. Each item is rated on a scale of 0–3, with higher scores reflecting better olfactory-specific QOL. The total score ranges from 0 (severe impact on QoL) to 21 (no impact on QoL) [9]. The item and total scores of sQOD-NS significantly differ between patients with anosmia at the time of the assessment, and those with hyposmia or without olfactory dysfunction (*p = 0.001)
LS loss of smell, sQOD-NS Short version of Questionnaire of Olfactory Disorders-Negative Statements
Gustatory outcomes
A total of 342 patients (88.8%) reported gustatory disorders, which was characterized by impairment of the following four taste modalities: salty, sweet, bitter, and sour. Note that 32 patients did not remember if they had gustatory dysfunction and, therefore, they were not considered for the assessment of the gustatory disorder prevalence. The gustatory dysfunction consisted of reduced/discontinued or distorted ability to taste flavors in 78.9% and 21.1% of patients, respectively.
Among the 43 patients without gustatory dysfunction, 19 (44.2%) have no olfactory dysfunction, whereas 16 (37.2%) and 4 (9.3%) patients had anosmia or hyposmia.
The olfactory and gustatory disorders were constant and unchanged over the days in 72.8% of patients, whereas they fluctuated in 23.4% of patients. Among the patients who reported gustatory and olfactory disorders, 3.8% revealed that these disorders occurred during their rhinorrhea or nasal obstruction episodes.
Among the cured patients who had residual olfactory and/or gustatory dysfunction, 53.9% had isolated olfactory dysfunction, 22.5% had isolated gustatory dysfunction, and 23.6% had both olfactory and gustatory dysfunctions.
Olfactory and gustatory outcome associations
There was no significant association between comorbidities and the development of olfactory or gustatory dysfunctions. Olfactory dysfunction was not significantly associated with rhinorrhea or nasal obstruction. There was a significant positive association between olfactory and gustatory dysfunctions (p < 0.001). The statistical analysis identified a significant association between the fever and the anosmia (p = 0.014). The females would be proportionally more affected by hyposmia or anosmia compared with males (p < 0.001). Similar results were found for gustatory dysfunction (p = 0.001, Mann–Whitney U test).
Treatments of COVID-19 patients
The following general treatments have been considered for patients with the COVID-19 infection: paracetamol (62.4%); non-steroidal anti-inflammatory drugs (9.8%); nasal saline irrigations (9.6%); Chloroquine (7.9%); mucolytics (5.0%); and oral corticosteroids (1.4%, with concomitant antibiotics) (Fig. 4). The treatments that have been most used for olfactory dysfunction were nasal saline irrigations (16.7%); nasal corticosteroids (8.1%), oral corticosteroids (2.5%), and others (2.5%, e.g., vitamins, non-corticoid decongestants, and trace elements) (Fig. 4). Gustatory dysfunction was treated in 1.4% of patients: four patients received treatment, consisting of l-carnitine or trace elements and vitamins. Telemedicine has been used in 42.6% of patients for prescribing the treatment.
Fig. 4.
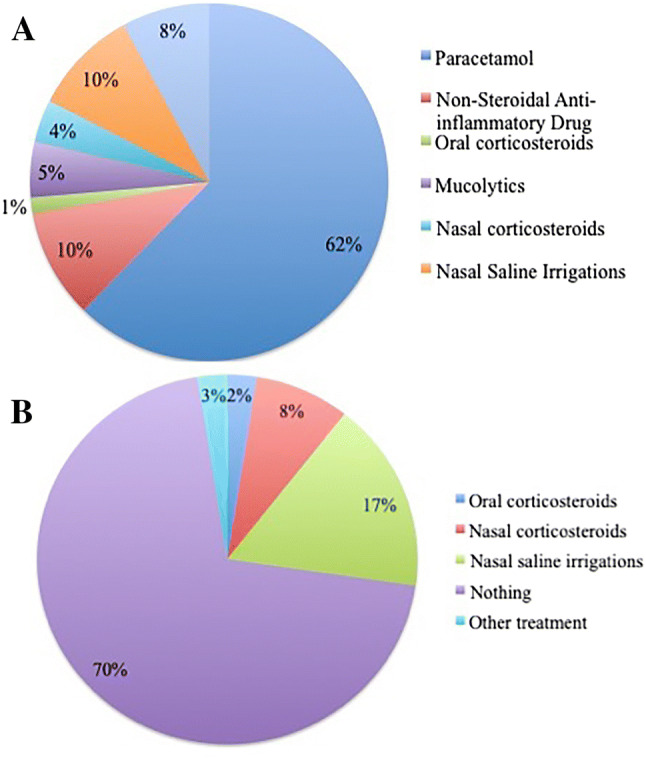
Therapeutic strategies for COVID-19 infection (a) and olfactory dysfunction (b)
Discussion
Over the past few weeks, an increasing number of otolaryngologists reported sudden anosmia or hyposmia as concurrent symptoms of COVID-19 infection. In these patients, the diagnosis of COVID-19 could be missed, because these symptoms were not known to be specific. As a result, the patients were not isolated and the spread of the virus continued. In this context, the COVID-19 Task Force of the YO-IFOS has conducted this study to investigate the prevalence and the short-term evolution of both olfactory and gustatory disorders.
Based on the National Health and Nutrition Examination Survey questions, our results support that olfactory and gustatory dysfunctions are both prevalent in patients with mild-to-moderate COVID-19 infection. Thus, 85.6% of patients reported olfactory dysfunction; 79.6% of them having anosmia. Interestingly, many profiles of patients have been identified. First, our data showed that 79.7% of patients without nasal obstruction or rhinorrhea reported hyposmia or anosmia, supporting the role of otolaryngologists as the first-line physicians for some COVID-19 patients. Second, the olfactory dysfunction may appear before, during, or after the general symptoms, with the occurrence of fever being associated with the olfactory dysfunction. There have been few studies on the occurrence of olfactory and gustatory dysfunctions in Asia, since only one study reported hyposmia as a symptom of the COVID-19 infection [12]. In the study of Mao et al., patients with peripheral nervous system symptoms attributed to COVID-19 infection, the most common the most common complaints were hypogeusia (5.6%) and hyposmia (5.1%) [12]. According to the data of the present study, the prevalence of olfactory and gustatory dysfunction is substantially higher in European COVID-19 patients. In addition to the high prevalence, physicians must keep in mind that olfactory disorder may appear before the rest of the complaints in 11.8% of cases, yielding the symptoms important for the early detection of the disease.
One of the most important questions from the otolaryngologists concerned the recovery of olfactory and gustatory functions. Although our results are still preliminary, it seems that, at least, 25.5% of patients recovered both olfactory and gustatory functions throughout the 2 weeks after the resolution of general symptoms. Considering the time to get a significant reduction of the viral load [10], we have estimated that 56% of patients have persistent olfactory dysfunction over the days following the resolution of the COVID-19 general clinical manifestations. In the same vein, some patients seemed to recover olfaction, but not taste, and vice versa. Naturally, there are short-term observations and it is reasonable to think that a large number of these patients will recover the olfactory or gustatory functions over the weeks following the disease resolution. To summarize, the present study clearly supports the recent declarations of many physicians from South Korea, Iran, Germany, Italy, Spain, France, Belgium, UK, and US that olfactory and gustatory functions may be impaired in COVID-19 patients.
The pathophysiological mechanisms leading to the olfactory and gustatory dysfunctions in the COVID-19 infection are still unknown. Coronavirus has already been identified as a family of viruses that may be associated with anosmia [6]. In 2007, Suzuki et al. demonstrated that coronavirus may be detected in the nasal discharge of patients with olfactory dysfunction. Moreover, they observed that some patients with normal acoustic rhinometry did not recover their olfaction, suggesting that nasal inflammation and related obstruction were not the only etiological factors underlying the olfactory dysfunction in viral infection.
The ability of human coronavirus to invade the olfactory bulb and, therefore, the central nervous system, is most likely a future research path for improving the knowledge about the clinical presentation of patients. From a biomolecular standpoint, viruses could infect peripheral neurons, using the cell machinery of active transport to access the central nervous system [13]. Thus, for the SARS-CoV receptor (human angiotensin-converting enzyme 2), it has been demonstrated on transgenic mice that SARS-CoV may enter the brain through the olfactory bulb, leading to rapid transneuronal spread [14]. Interestingly, authors demonstrated that the virus antigen was first detected 60–66 h post-infection and was most abundant in the olfactory bulb. Regions of the cortex (piriform and infralimbic cortices), basal ganglia (ventral pallidum and lateral preoptic regions), and midbrain (dorsal raphe) were also strongly infected after the virus had spread [14]; these regions are connected with the olfactory bulb. The rapid spread of SARS-CoV in the brain was also associated with significant neuronal death. In humans, autopsy samples from eight patients with SARS revealed the presence of SARS-CoV in brain samples by immunohistochemistry, electron microscopy, and real-time RT-PCR [15]. It is currently suspected that the neuroinvasive potential of SARS-CoV2 plays a key role in the respiratory failure of COVID-19 patients [16]. Medical imaging and neuropathology will certainly play an important rule to detect abnormalities in olfactory bulb, cranial nerves, and brain of COVID-19 patients.
The otolaryngological symptoms in our European cohort were particularly prevalent compared with the Asian cohorts. In their clinical series of 99 patients, Chen et al. reported four patients with rhinorrhea (4%) [17]. Then, Guan et al. reported a prevalence of nasal obstruction in 5% of patients in a cohort of 1099 patients [18]. The lack of otolaryngological complaints in Asian papers, e.g., nasal obstruction, rhinorrhea, and olfactory and gustatory dysfunctions, raises many questions. Either they did not assess the ENT complaints, or the Chinese patients had a few ENT complaints. The second hypothesis may be likely regarding previous studies. Benvenuto et al. have recently compared the complete genomes of 15 virus sequences from patients treated in different regions of China with other coronaviruses [19]. Interestingly, they observed mutations of surface proteins (spike-S-protein and nucleocapsid-N-protein), conferring stability to the viral particle. Such mutations could be clinically relevant, because the viral spike protein is responsible for virus entry into the cell, whereas the N-protein plays a pivotal role in the virus transcription and assembly efficiency. Previously, Chan et al. determined five virus sequences from patients traveling in Wuhan at the end of December 2019. This study reported identities, but less than 68%, with the SARS-related coronaviruses in specific domains. Particularly, the external subdomain region of receptor-binding domain of the S-protein only presents 39% identity, and Chan et al. propose that it might affect the choice of human receptor and, therefore, the biological behaviour of this virus [20]. The affinity of some viruses for some tissues and individuals constitutes another area to investigate and explain the potential clinical differences between patients from different world regions. Recent studies suggested that the angiotensin converting enzyme 2 (ACE2), which is the receptor of SARS-CoV-2, could be specific to certain populations. Li et al. demonstrated that some ACE2 variants could reduce the association between human ACE2 and SARS-CoV S-protein [21]. In other words, the expression level of ACE2 in different tissues might be critical for the susceptibility, symptoms, and outcomes of COVID-19 infection [21]. Moreover, the comparison of the 15 expression quantitative trait loci (eQTLs) variants of the ACE2 gene suggested that there will be a lot of ACE2 polymorphisms and ACE2 expression levels between Asian and European populations [22]. According to these studies, it is conceivable that the diversity of ACE2 expression pattern in Asian and European populations could be an important track that needs further investigation.
Moreover, regarding our results, future studies have to explore the potential gender differences in the development of anosmia. The highest susceptibility of females to develop olfactory and gustatory dysfunctions would be related to the gender-related differences in the inflammatory reaction process [23].
The present study has several limitations. First, our patients did not benefit from specific examinations for olfactory and gustatory functions, including psychophysical tests or electrophysiological methods [24, 25]. The use of objective approaches makes sense for investigating both gustatory and olfactory functions in COVID-19 patients, and to avoid the confusion related to the retro-olfaction. These approaches would provide many responses for patients who may recover olfaction, but not taste, and vice versa. Second, our patient sample consisted of young and mild-to-moderate COVID-19 patients with little comorbidities. They may be not representative of the infected population. However, it seems ethically difficult to investigate olfaction and gustatory function in patients in life-threatening condition, such as patients in intensive-care units. Note that in this study, the majority of included patients were identified from hospital laboratory results. However, many infected physicians completed the study, and, therefore, it remains possible that many infected physicians participated to the study, because they suffered from olfactory dysfunction, although the authors have been particularly vigilant to this potential bias. Third, the lack of consistent follow-up of our patients limits us from inquiring into the recovery time of olfactory and gustatory functions, and, therefore, the rate of permanent anosmia or ageusia. Fourth, it seems difficult to identify the potential negative impact of nasal and oral corticosteroids on the clinical course of the disease; these treatments are usually used for anosmia or in common nasal complaints. In the absence of such data, the precautionary principle may prevail and, according to the guidelines of the French Society of Otolaryngology, patients must avoid corticosteroids for the treatment of the COVID-19 infection. All of these weaknesses should be considered in future studies to investigate and characterize the olfactory and gustatory functions in COVID-19 patients.
Conclusion
Since the disease is new and the virus is most likely associated with different mutations and clinical patterns, as of yet, there remain more questions than answers. This study is the first to identify both olfactory and gustatory dysfunctions as significant symptoms in the clinical presentation of the European COVID-19 infection. Based on our results, it seems that infected patients may just present olfactory and gustatory dysfunctions without other significant complaints. The sudden anosmia or ageusia need to be recognized by the international scientific community as important symptoms of the COVID-19 infection. Future epidemiological, clinical, and basic science studies must elucidate the mechanisms underlying the development of these symptoms in such a specific world population.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgements
C. Omer, S. Amsellem, and C. Debuschere US MD Native Speakers for the proofreading. The University of Mons head and staff; and the following researchers and professors: A. Legrand, A.E. Decleves, A. Nachtergeal, P. Duez, B. Harmegnies, L. Tafforeau, and their collaborators.
Compliance with ethical standards
Conflict of interest
The authors have no conflicts of interest.
Research involving human participants and/or animals
Three ethics committees approved the current study protocol (HAP2020-011; CHUSP20032020; EpiCURA-2020-2303).
Informed consent
Patients were invited to participate and the informed consent was obtained.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Jerome R. Lechien and Carlos M. Chiesa-Estomba have equally contributed to this work and should be regarded as joint first authors.
Tareck Ayad and Sven Saussez have equally contributed to this work and should be regarded as joint senior authors.
References
- 1.Guan WJ, Ni ZY, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020 doi: 10.1056/NEJMoa2002032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ramanathan K, Antognini D, Combes A, Paden M, Zakhary B, Ogino M, MacLaren G, Brodie D, Shekar K. Planning and provision of ECMO services for severe ARDS during the COVID-19 pandemic and other outbreaks of emerging infectious diseases. Lancet Respir Med. 2020 doi: 10.1016/s2213-2600(20)30121-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wu YC, Chen CS, Chan YJ. Overview of the novel coronavirus (2019-nCoV): the pathogen of severe specific contagious pneumonia (SSCP) J Chin Med Assoc. 2020 doi: 10.1097/JCMA.0000000000000270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Young BE, Ong SWX, Kalimuddin S, et al. Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA. 2020 doi: 10.1001/jama.2020.3204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wan S, Xiang Y, Fang W, Zheng Y, et al. Clinical features and treatment of COVID-19 patients in Northeast Chongqing. J Med Virol. 2020 doi: 10.1002/jmv.25783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Suzuki M, Saito K, Min WP, Vladau C, Toida K, Itoh H, Murakami S. Identification of viruses in patients with postviral olfactory dysfunction. Laryngoscope. 2007;117(2):272–277. doi: 10.1097/01.mlg.0000249922.37381.1e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.van Riel D, Verdijk R, Kuiken T. The olfactory nerve: a shortcut for influenza and other viral diseases into the central nervous system. J Pathol. 2015;235(2):277–287. doi: 10.1002/path.4461. [DOI] [PubMed] [Google Scholar]
- 8.Ayad T, Stephenson K, Smit D, et al. Young Otolaryngologists of International Federation of Oto-rhino-laryngological Societies (YO-IFOS) committees. Eur Ann Otorhinolaryngol Head Neck Dis. 2018;135(5S):S61–S65. doi: 10.1016/j.anorl.2018.08.004. [DOI] [PubMed] [Google Scholar]
- 9.Mattos JL, Edwards C, Schlosser RJ, Hyer M, Mace JC, Smith TL, Soler ZM. A brief version of the questionnaire of olfactory disorders in patients with chronic rhinosinusitis. Int Forum Allergy Rhinol. 2019;9(10):1144–1150. doi: 10.1002/alr.22392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bhattacharyya N, Kepnes LJ. Contemporary assessment of the prevalence of smell and taste problems in adults. Laryngoscope. 2015;125(5):1102–1106. doi: 10.1002/lary.24999. [DOI] [PubMed] [Google Scholar]
- 11.Zou L, Ruan F, Huang M, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382(12):1177–1179. doi: 10.1056/NEJMc2001737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mao L, Wang M, Chen S, et al. Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: a retrospective case series study. MedRXiv. 2020 doi: 10.1101/2020.02.22.20026500. [DOI] [Google Scholar]
- 13.Koyuncu OO, Hogue IB, Enquist LW. Virus infections in the nervous system. Cell Host Microbe. 2013;13(4):379–393. doi: 10.1016/j.chom.2013.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Netland J, Meyerholz DK, Moore S, Cassell M, Perlman S. Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J Virol. 2008;82(15):7264–7275. doi: 10.1128/JVI.00737-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gu J, Gong E, Zhang B, et al. Multiple organ infection and the pathogenesis of SARS. J Exp Med. 2005;202(3):415–424. doi: 10.1084/jem.20050828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Li YC, Bai WZ, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol. 2020 doi: 10.1002/jmv.25728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi: 10.1016/S0140-6736(20)30211-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Guan W, Ni Z, Hu Y, Liang W, Ou C, He J et al (2020) Clinical characteristics of 2019 novel coronavirus infection in China. Medrxiv
- 19.Benvenuto D, Giovanetti M, Ciccozzi A, Spoto S, Angeletti S, Ciccozzi M. The 2019-new coronavirus epidemic: evidence for virus evolution. J Med Virol. 2020;92(4):455–459. doi: 10.1002/jmv.25688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):514–523. doi: 10.1016/S0140-6736(20)30154-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Li W, Zhang C, Sui J, Kuhn JH, et al. Receptor and viral determinants of SARS-coronavirus adaptation to human ACE2. EMBO J. 2005;24(8):1634–1643. doi: 10.1038/sj.emboj.7600640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cao Y, Li L, Feng Z, Wan S, Huang P, Sun X, Wen F, Huang X, Ning G, Wang W. Comparative genetic analysis of the novel coronavirus (2019-nCoV/SARS-CoV-2) receptor ACE2 in different populations. Cell Discov. 2020;6:11. doi: 10.1038/s41421-020-0147-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lefèvre N, Corazza F, Valsamis J, Delbaere A, De Maertelaer V, Duchateau J, Casimir G. The number of X chromosomes influences inflammatory cytokine production following toll-like receptor stimulation. Front Immunol. 2019;10:1052. doi: 10.3389/fimmu.2019.01052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hummel T, Whitcroft KL, Andrews P, et al. Position paper on olfactory dysfunction. Rhinol Suppl. 2017;54(26):1–30. doi: 10.4193/Rhino16.248. [DOI] [PubMed] [Google Scholar]
- 25.Gudziol H, Guntinas-Lichius O. Electrophysiologic assessment of olfactory and gustatory function. Handb Clin Neurol. 2019;164:247–262. doi: 10.1016/B978-0-444-63855-7.00016-2. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.