

Abstract
Background
Vagus nerve stimulation (VNS) is a neuromodulatory treatment that is used as an adjunctive therapy for treating people with medically refractory epilepsy. VNS consists of chronic intermittent electrical stimulation of the vagus nerve, delivered by a programmable pulse generator. The majority of people given a diagnosis of epilepsy have a good prognosis, and their seizures will be controlled by treatment with a single antiepileptic drug (AED), but up to 20%‐30% of patients will develop drug‐resistant epilepsy, often requiring treatment with combinations of AEDs. The aim of this systematic review was to overview the current evidence for the efficacy and tolerability of vagus nerve stimulation when used as an adjunctive treatment for people with drug‐resistant partial epilepsy. This is an updated version of a Cochrane review published in Issue 7, 2010.
Objectives
To determine:
(1) The effects on seizures of VNS compared to controls e.g. high‐level stimulation compared to low‐level stimulation (presumed sub‐therapeutic dose); and (2) The adverse effect profile of VNS compared to controls e.g. high‐level stimulation compared to low‐level stimulation.
Search methods
We searched the Cochrane Epilepsy Group's Specialised Register (23 February 2015), the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 23 February 2015), MEDLINE (1946 to 23 February 2015), SCOPUS (1823 to 23 February 2015), ClinicalTrials.gov (23 February 2015) and ICTRP (23 February 2015). No language restrictions were imposed.
Selection criteria
The following study designs were eligible for inclusion: randomised, double‐blind, parallel or crossover studies, controlled trials of VNS as add‐on treatment comparing high and low stimulation paradigms (including three different stimulation paradigms ‐ duty cycle: rapid, mid and slow) and VNS stimulation versus no stimulation or a different intervention. Eligible participants were adults or children with drug‐resistant partial seizures not eligible for surgery or who failed surgery.
Data collection and analysis
Two review authors independently selected trials for inclusion and extracted data. The following outcomes were assessed: (a) 50% or greater reduction in total seizure frequency; (b) treatment withdrawal (any reason); (c) adverse effects; (d) quality of life; (e) cognition; (f) mood. Primary analyses were intention‐to‐treat. Sensitivity best and worst case analyses were also undertaken to account for missing outcome data. Pooled Risk Ratios (RR) with 95% confidence intervals (95% Cl) were estimated for the primary outcomes of seizure frequency and treatment withdrawal. For adverse effects, pooled RRs and 99% CI's were calculated.
Main results
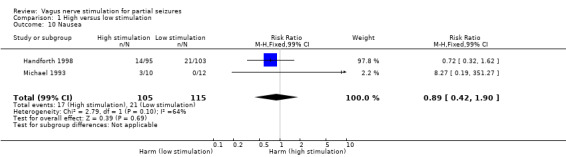
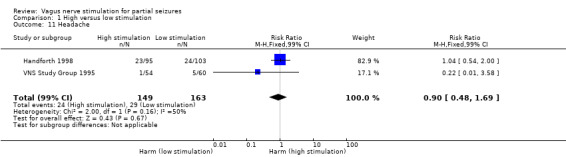
Five trials recruited a total of 439 participants and between them compared different types of VNS stimulation therapy. Baseline phase ranged from 4 to 12 weeks and double‐blind treatment phases from 12 to 20 weeks in the five trials. Overall, two studies were rated as having a low risk of bias and three had an unclear risk of bias due to lack of reported information around study design. Effective blinding of studies of VNS is difficult due to the frequency of stimulation‐related side effects such as voice alteration; this may limit the validity of the observed treatment effects. Four trials compared high frequency stimulation to low frequency stimulation and were included in quantitative syntheses (meta‐analyses).The overall risk ratio (95% CI) for 50% or greater reduction in seizure frequency across all studies was 1.73 (1.13 to 2.64) showing that high frequency VNS was over one and a half times more effective than low frequency VNS. For this outcome, we rated the evidence as being moderate in quality due to incomplete outcome data in one included study; however results did not vary substantially and remained statistically significant for both the best and worst case scenarios. The risk ratio (RR) for treatment withdrawal was 2.56 (0.51 to 12.71), however evidence for this outcome was rated as low quality due to imprecision of the result and incomplete outcome data in one included study. The RR of adverse effects were as follows: (a) voice alteration and hoarseness 2.17 (99% CI 1.49 to 3.17); (b) cough 1.09 (99% CI 0.74 to 1.62); (c) dyspnea 2.45 (99% CI 1.07 to 5.60); (d) pain 1.01 (99% CI 0.60 to 1.68); (e) paresthesia 0.78 (99% CI 0.39 to 1.53); (f) nausea 0.89 (99% CI 0.42 to 1.90); (g) headache 0.90 (99% CI 0.48 to 1.69); evidence of adverse effects was rated as moderate to low quality due to imprecision of the result and/or incomplete outcome data in one included study. No important heterogeneity between studies was found for any of the outcomes.
Authors' conclusions
VNS for partial seizures appears to be an effective and well tolerated treatment in 439 included participants from five trials. Results of the overall efficacy analysis show that VNS stimulation using the high stimulation paradigm was significantly better than low stimulation in reducing frequency of seizures. Results for the outcome "withdrawal of allocated treatment" suggest that VNS is well tolerated as withdrawals were rare. No significant difference was found in withdrawal rates between the high and low stimulation groups, however limited information was available from the evidence included in this review so important differences between high and low stimulation cannot be excluded . Adverse effects associated with implantation and stimulation were primarily hoarseness, cough, dyspnea, pain, paresthesia, nausea and headache, with hoarseness and dyspnea more likely to occur on high stimulation than low stimulation. However, the evidence on these outcomes is limited and of moderate to low quality. Further high quality research is needed to fully evaluate the efficacy and tolerability of VNS for drug resistant partial seizures.
Plain language summary
Vagus nerve stimulation for partial seizures
Epilepsy is a disorder where unexpected electrical discharges from the brain cause seizures. Most seizures can be controlled by a single antiepileptic drug but sometimes seizures do not respond to drugs. Some people require more than one antiepileptic medication to control their seizures, especially if these originate from one area of the brain (partial epilepsy), instead of involving the whole brain.
The vagus nerve stimulator (VNS) is a device that is useful as an additional treatment for epilepsy that does not respond well to drugs, and only affects one part of the brain. The device is connected to the vagus nerve in the neck, and sends mild electrical impulses to it. This is particularly important for treating people whose epilepsy does not respond well to drugs and who are not eligible for epilepsy surgery, or in whom surgery was not successful in reducing frequency of seizures. The aim of this systematic review was to look at the current evidence on how effective vagus nerve stimulation is in reducing frequency of epileptic seizures and any side effects associate with using the device.
Overall the five multi‐centre randomised controlled trials (RCTs) recruited a total of 439 participants and between them compared different types of VNS therapy. Overall there were three randomised controlled trials which compared high frequency stimulation to low frequency stimulation in participants aged 12‐60 years and another trial examined high frequency stimulation versus low frequency stimulation in children. Additionally, one trial examined three different stimulation frequencies.
The review of these trials found that vagus nerve stimulation is effective, when used with one or more antiepileptic drugs, to reduce the number of seizures for people whose epilepsy does not respond to drugs alone. Common side effects were voice alteration and hoarseness, pain, shortness of breath, cough, feeling sickly, tingling sensation, headache or infection at the site of the operation, with shortness of breath, voice alteration and hoarseness more common in people receiving high frequency stimulation compared to people receiving low level stimulation.
Out of the five included studies, two studies were rated individually as being of high quality and the other three studies were rated as being of unclear quality due to lack of reported information in the study paper about the methods of study design. The evidence for the effectiveness and side effects of VNS therapy was limited and imprecise from the small number of studies included in this review, so was rated as being of moderate to low quality. Further large, high quality studies are required to provide more information about the effectiveness and side effects of VNS therapy.
Summary of findings
Summary of findings for the main comparison. High versus low stimulation for partial seizures.
| High versus low stimulation for partial seizures | ||||||
| Patient or population: patients with partial seizures Settings: Outpatients Intervention: High versus low stimulation | ||||||
| Outcomes |
Illustrative comparative risks* (95% CI) For adverse effects (99% CI) |
Relative effect
(95% CI) For adverse effects (99% CI) |
No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Low stimulation (control) | High stimulation | |||||
| 50% reduction in seizure frequency (responders) | 144 per 1000 | 249 per 1000 (163 to 380) | RR 1.73 (1.13 to 2.64) | 373 (4 studies) | ⊕⊕⊕⊝ moderate1 | RR>1 indicates outcome is more likely on High Stimulation |
| Withdrawals | 10 per 1000 | 26 per 1000 (5 to 130) | RR 2.56 (0.51 to 12.71) | 375 (4 studies) | ⊕⊕⊝⊝ low1,2 | RR>1 indicates outcome is more likely on High Stimulation |
| Voice Alteration or Hoarseness | 251 per 1000 | 545 per 1000 (374 to 796) | RR 2.17 (1.49 to 3.17) | 330 (3 studies) | ⊕⊕⊕⊝ moderate1 | RR>1 indicates outcome is more likely on High Stimulation |
| Cough | 291 per 1000 | 317 per 1000 (215 to 471) | RR 1.09 (0.74 to 1.62) | 334 (3 studies) | ⊕⊕⊕⊝ moderate1 | RR>1 indicates outcome is more likely on High Stimulation |
| Dyspnea | 74 per 1000 | 181 per 1000 (79 to 414) | RR 2.45 (1.07 to 5.60) | 312 (2 studies) | ⊕⊕⊝⊝ low1,3 | RR>1 indicates outcome is more likely on High Stimulation |
| Pain | 239 per 1000 | 241 per 1000 (143 to 402) | RR 1.01 (0.60 to 1.68) | 312 (2 studies) | ⊕⊕⊕⊝ moderate1 | RR>1 indicates outcome is more likely on High Stimulation |
| Paresthesias | 172 per 1000 | 134 per 1000 (67 to 263) | RR 0.78 (0.39 to 1.53) | 312 (2 studies) | ⊕⊕⊕⊝ moderate1 | RR>1 indicates outcome is more likely on High Stimulation |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes.4 The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio. | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1 One study (VNS Study Group 1995) that contributed to this outcome was judged to be at high risk of bias, as it had incomplete outcome data, which could not be analysed by an intention to treat approach (see Characteristics of included studies for further information).
2Wide, imprecise confidence interval of the pooled effect estimate due to low withdrawal rates in the included studies.
3Wide, imprecise confidence interval of the pooled effect estimate due to low event rates in the included studies
4 Assumed Risk: The event rate in the low stimulation group multiplied by 1000. The event rate is the proportion of the total in which the event occurred.
Background
This review is an update of a previously published review in The Cochrane Database of Systematic Reviews (The Cochrane Library, Issue 7, 2010).
Description of the condition
Epilepsy is a condition characterized by a tendency for recurrent seizures unprovoked by any known proximate insult. Epileptiform discharges involve either a localized area of the brain resulting in a partial seizure, or the entire brain resulting in a generalized seizure. The prevalence of epilepsy is estimated to be five to eight per 1000 population in developed countries, and in adults the most common type is partial epilepsy (Hauser 1975; Forsgren 2005). The majority of people given a diagnosis of epilepsy have a good prognosis, and their seizures will be controlled by treatment with a single antiepileptic drug (AED). However, 20% (reported in population‐based studies) to 30% (reported in clinical (non‐population‐based) series) will develop drug‐resistant epilepsy (Cockerell 1995; Kwan 2000), often requiring treatment with combinations of antiepileptic drugs (AEDs). These patients tend to have frequent, disabling seizures that limit their ability to work and participate in activities. Many of these patients also suffer from the chronic effects of long‐term, high‐dose AED polytherapy, while anxiety and depressive disorders are common in patients with epilepsy.The development of effective new therapies for the treatment of refractory seizures is therefore of considerable importance.
Description of the intervention
Vagus nerve stimulation (VNS) is a neuromodulatory treatment that is used as an adjunctive therapy for people with medically refractory epilepsy who are not eligible for epilepsy surgery or in whom surgery has failed. In this procedure, a pacemaker‐like device ‐ the Neuro‐cybernetic Prosthesis (NCP) ‐ is implanted under the skin of the chest. The stimulating electrodes of the NCP carry electrical signals from the generator to the left vagus nerve. By programming the device, the frequency, intensity, and duration of stimulation can be varied (the stimulation paradigm). In the initial trials, the vagus nerve was stimulated for 30 seconds, every five minutes (Sackeim 2001). During each 30‐second stimulation, the device delivered 500 microsecond pulses at 30 Hz frequency. For each individual, the intensity of the current was set at the highest that was tolerable, or to low intensity stimulation, depending on the allocated treatment group. Also, in an attempt to further abort seizures, patients could activate the device by placing a magnet over it when a seizure had occurred, or was about to occur. Participants enrolled into the initial randomised controlled trials of VNS had drug‐resistant partial epilepsy, and experienced a 24% to 28% median reduction in seizure frequency over a three month treatment period (Selway 1987).
How the intervention might work
Left VNS is a promising, relatively new treatment for epilepsy. In 1997, VNS was approved in the United States as an adjunctive treatment for medically refractory partial‐onset seizures in adults and adolescents. For some patients with partial‐onset seizures, the adverse effects of antiepileptic drugs (AEDs) are intolerable; for others, no single AED or combination of anticonvulsant agents is effective. Cerebral resective surgery is an alternative to pharmacotherapy in some cases, but many patients with partial‐onset seizures are not optimal candidates for intracranial surgery (Schachter 1998).
The mechanism of action of VNS is not fully understood, but can be reasonably assumed to involve brainstem nuclei. The nucleus of the solitary tract, the main terminus for vagal afferents, has direct or indirect projections to the locus coeruleus, raphe nuclei, reticular formation, and other brainstem nuclei. These nuclei have been shown to influence cerebral seizure susceptibility, hence vagal modulation of one or more of these nuclei could plausibly represent the mechanism for seizure suppression (Krahl 2012). In this context, the immunomodulatory function of the vagus nerve is of particular interest. Afferent signals can activate the so‐called cholinergic anti‐inflammatory pathway upon inflammation. Through this pathway, efferent vagus nerve fibres inhibit the release of pro‐inflammatory cytokines and in this way reduce inflammation. In recent years, inflammation has been strongly implicated in the development of seizures and epilepsy and therefore the activation of the anti‐inflammatory pathway by VNS could decrease the inflammatory response and thereby explain its clinical effects. In addition to anticonvulsive effects, VNS might have positive effects on behavior, mood and cognition (Vonck 2014).
Why it is important to do this review
In this review we summarise evidence from randomised controlled trials where the efficacy and tolerability of VNS for people with drug‐resistant partial epilepsy have been investigated in order to aid clinical decision making when considering VNS treatment within this population.The aim was to evaluate the effects of VNS on seizure frequency and its tolerability and safety when used as an add‐on treatment for people with medically refractory epilepsy.
Objectives
To determine:
(1) The effects on seizures of VNS compared to controls e.g. high‐level stimulation compared to low‐level stimulation (presumed sub‐therapeutic dose); and (2) The adverse effect profile of VNS compared to controls e.g. high‐level stimulation compared to low‐level stimulation.
Methods
Criteria for considering studies for this review
Types of studies
Trials had to meet all of the following criteria:
Randomised controlled trials;
Double blind trials;
Placebo controlled, active control (low stimulation) or other intervention control group; and
Parallel group or crossover studies.
Types of participants
Individuals of any age with partial epilepsy (i.e. experiencing simple partial, complex partial or secondarily generalized tonic‐clonic seizures) who have failed to respond to at least one AED, who were not eligible for surgery or in whom surgery had previously failed.
Types of interventions
VNS using high intensity (therapeutic) versus low intensity (presumed sub‐therapeutic) stimulation;
VNS stimulation versus different stimulation of VNS;
VNS stimulation versus no stimulation;
VNS stimulation versus different intervention.
Types of outcome measures
Primary outcomes
50% or greater reduction in seizure frequency The primary outcome is the proportion of participants with a 50% or greater reduction in seizure frequency in the treatment period compared to the pre‐randomisation baseline period.
Secondary outcomes
Treatment withdrawal The proportion of people having their allocated VNS paradigm stopped or altered during the course of the trial for whatever reason was used as a measure of "global effectiveness." Treatment is likely to be withdrawn due to adverse effects, lack of efficacy or a combination of both, and this is an outcome to which the individual makes a direct contribution.
Adverse effects We reported the incidence of adverse events in all VNS implanted patients and according to randomised group. We chose to investigate the following side effects which are most common and important:
Infection at implantation site.
Haemorrhage at implantation site.
Voice alteration or hoarseness.
Pain.
Dyspnea.
Cough.
Ataxia.
Dizziness.
Paresthesias.
Fatigue.
Nausea.
Somnolence.
Headache.
In addition, we reported the five most common adverse effects (if different from those stated above).
Quality of life
The difference between intervention and control group(s) means on quality of life measures used in the individual studies.
Cognition
The difference between intervention and control group(s) means on cognitive assessments used in the individual studies.
Mood
The difference between intervention and control group(s) means on mood assessments used in the individual studies.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Epilepsy Group's Specialized Register (23/02/2015) see Appendix 1. In addition we searched the following databases:
(a) The Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, 23 February 2015) using the strategy outlined in Appendix 2;
(b) MEDLINE (Ovid) (1946 to 23/02/2015) using the strategy outlined in Appendix 3;
(c) SCOPUS (1823 to 23/02/2015) see Appendix 4;
(d) ClinicalTrials.gov 23/02/2015, see Appendix 5; and
(e) WHO International Clinical Trials Registry Platform ICTRP 23/02/2015 see Appendix 6.
No language restrictions were imposed.
Searching other resources
We reviewed reference lists of included studies to search for additional reports of relevant studies.
Data collection and analysis
Selection of studies
For the update, two review authors (MP and AR) independently assessed trials for inclusion. Any disagreements were resolved by discussion with a third author (JW). Three reviewers (MP, AR and JW) extracted data and assessed the risk of bias; disagreements were again resolved by discussion.
Data extraction and management
The following data were extracted for each trial using a data extraction form:
(1) Methodological/trial design: (a) Method of randomisation. (b) Method of allocation concealment. (c) Method of double blinding. (d) Whether any participants had been excluded from reported analyses. (e) Duration of baseline period. (e) Duration of treatment period. (f ) Frequency of VNS tested. (g) Information on Sponsorship/Funding.
(2) Participant/demographic information: (a) Total number of participants allocated to each treatment group; (b) Age/sex; (c) Number with partial/generalized epilepsy; (d) Seizure types; (e) Seizure frequency during the baseline period; (f) Number of background drugs.
(3) Outcomes We recorded the number of participants experiencing each outcome (see Types of outcome measures) per randomised group and contacted authors of trials were for any missing information.
Assessment of risk of bias in included studies
MP and AR independently made an assessment of the risk of bias for each trial using the Cochrane 'Risk of bias' table as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Any disagreements were discussed and resolved. We rated all included studies as having a(n) low, high or unclear risk of bias on six domains applicable to randomised controlled trials: randomisation method, allocation concealment, blinding methods, incomplete outcome data, selective outcome reporting, and other sources of bias. We created summary of findings tables, employing the GRADE approach for assessing quality of evidence.
Measures of treatment effect
We analysed the primary outcome of seizure reduction as a binary outcome and presented it as a risk ratio. We also analysed secondary outcomes including adverse effects and treatment withdrawal as binary outcomes and presented risk ratios. We planned to analyse quality of life and cognition as continuous outcomes, presented using the standardised mean difference, but this was not possible due to limited information from single studies for cognition outcomes and heterogenous measurement scales for quality of life outcomes. Therefore these outcomes are discussed narratively.
Unit of analysis issues
We did not encounter any unit of analysis issues, as we did not find any crossover studies; we analysed all outcomes as risk ratios as planned or discussed them narratively.
Dealing with missing data
We sought missing data by contacting the study authors. We carried out intention‐to‐treat (ITT), best case and worst case analysis on the primary outcome to account for any missing data (see Data synthesis). All analyses are presented in the main report.
Assessment of heterogeneity
We assessed clinical heterogeneity by comparing the distribution of important individual participant factors among trials (for example age, seizure type, duration of epilepsy, number of AEDs taken at the time of randomisation) and trial factors (for example randomisation concealment, blinding, losses to follow‐up). We examined statistical heterogeneity using a Chi2 test and I2 statistic; providing no significant heterogeneity was present (P > 0.10), we employed a fixed‐effect model. In the event heterogeneity was found (> 50%), a random‐effects model analysis was planned.
Assessment of reporting biases
We requested protocols from study authors for all included studies to enable a comparison of outcomes of interest. If outcome reporting bias was suspected for any included study, we planned to further investigate using the ORBIT matrix system (Kirkham 2010). Examination of asymmetry funnel plots was planned to establish publication bias, but such an assessment was not possible due to the small number of studies included in the review.
Data synthesis
We employed a fixed‐effect model meta‐analysis to synthesise the data. Comparisons we expected to carry out included:
intervention group versus controls on seizure reduction;
intervention group versus controls on treatment withdrawal;
intervention group versus controls on adverse effects;
intervention group versus controls on quality of life;
intervention group versus controls on cognition;
intervention group versus controls on mood.
Each comparison was to be stratified by type of control group, that is level of stimulation, and study characteristics to ensure the appropriate combination of study data. Our preferred estimator for all binary outcomes was the Mantel‐Haenzsel risk ratio (RR). For the outcomes 50% or greater reduction in seizure frequency and treatment withdrawal, we used 95% confidence intervals (Cls). For individual adverse effects we used 99% Cls to make an allowance for multiple testing. Our analyses included all participants in the treatment groups to which they had been allocated following transplantation. For the efficacy outcome (50% or greater reduction in seizure frequency) we undertook three analyses:
(1) Primary (ITT) analysis Participants not completing follow up or with inadequate seizure data were assumed non‐responders. To test the effect of this assumption, we undertook the following sensitivity analyses. Analysis by ITT was done where this was reported by the included studies.
(2) Worst case analysis Participants not completing follow up or with inadequate seizure data were assumed to be non‐responders in the high‐level stimulation group, and responders in the low‐level stimulation group.
(3) Best case analysis Participants not completing follow up or with inadequate seizure data were assumed responders in the high‐level stimulation group, and non‐responders in the low‐level stimulation group.
Subgroup analysis and investigation of heterogeneity
We performed a subgroup analysis for adverse effects. We intended to investigate heterogeneity using sensitivity analysis if deemed appropriate.
Sensitivity analysis
We also intended to carry out sensitivity analysis if peculiarities were found between study quality, characteristics of participants, interventions and outcomes.
Results
Description of studies
Results of the search
The search (carried out 19 September 2013) revealed 749 records identified from the databases outlined in Electronic searches. We screened the 486 records that remained after duplicates were removed for inclusion in the review. We excluded 438 at this point leaving 48 full‐text articles to be assessed for eligibility. Following this, we excluded 23 (see Figure 1 and Characteristics of excluded studies for reasons of exclusion). We included a total of five studies in the review, four of which were included in meta‐analyses (Handforth 1998; Klinkenberg 2012; Michael 1993; VNS Study Group 1995). DeGiorgio 2005 was not included in the meta‐analysis of high versus low stimulation, because this trial compared three different duty cycles paradigms; results of this trial are described narratively. We identified five ongoing studies and six abstracts for studies awaiting classification; authors of these studies were contacted for more information, providing their contact details were available.
1.
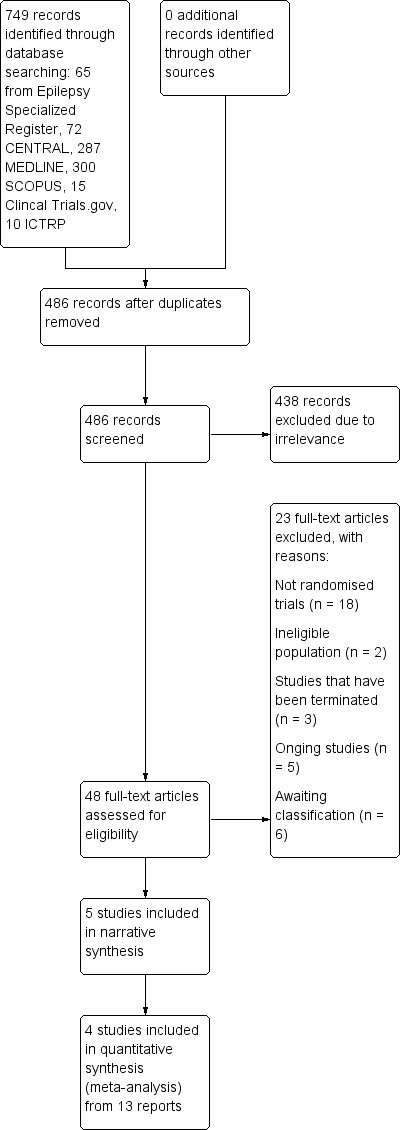
Study flow diagram (reflecting results of the search carried out on 19 September 2013).
A pre‐publication search carried out on 23 February 2015 identified 67 results; two studies have been identified as potentially relevant (Klinkenberg 2014 and NCT02089243 2014). These will be addressed in the next update.
Included studies
Overall, five randomised controlled trials which recruited a total of 439 participants were included in this review (DeGiorgio 2005; Handforth 1998; Klinkenberg 2012; Michael 1993; VNS Study Group 1995). Trial characteristics are summarised below. For further information on each trial please see Characteristics of included studies.
Three trials compared high stimulation to low stimulation in participants aged 12‐60 years (Handforth 1998, Michael 1993, VNS Study Group 1995) and another trial examined high stimulation versus low stimulation in children (Klinkenberg 2012). One trial examined three different stimulation paradigms (DeGiorgio 2005). In the majority of the trials, participants were eligible to take part in the double‐blind phase if they were found to experience a minimum of six partial seizures per month and were drug‐resistant.
One multi‐centre (USA) parallel trial (DeGiorgio 2005) randomised 64 subjects > 12 years of age to one of three treatment arms, corresponding to rapid, medium, and slow duty‐cycles: group A, seven seconds on and 18 seconds off (n = 19); group B, 30 seconds on and 30 seconds off (n = 19); group C, 30 seconds on and three minutes off (n = 23). The baseline period was four weeks in duration with a treatment period of three months.
Another multi‐centre (USA) parallel trial (Handforth 1998) included 198 subjects aged 13‐60 years and had two treatment arms: intervention, high stimulation (n = 95) and active control group, low stimulation (n = 103). This trial had a baseline period of 12‐16 weeks and a treatment period of 16 weeks. Dodrill 2000 and Amar 1998 are linked to this study.
A recent multi‐centre (Holland) parallel trial (Klinkenberg 2012) investigated children only and consisted of two treatment arms including high stimulation (n = 21) and low stimulation (n = 20). The baseline period was 12 weeks in duration followed by a treatment period of 20 weeks. After the blinded phase all participants underwent a non‐controlled follow‐up, in which they received high stimulation (add‐on phase). Aalbers 2012 is linked to this study.
One multi‐centre (USA and Europe) parallel trial (Michael 1993) had a pre‐randomisation period of 12 weeks and a treatment period of 14 weeks, where 22 adults were randomised to one of two treatment arms: high, therapeutic (n = 10) or low, sub‐therapeutic (n = 12). All patients completed the acute phase of the study and entered the extension phase.
A further multi‐centre (USA, Sweden and Germany) parallel trial (VNS Study Group 1995) randomised 114 patients to one of two treatment arms: high‐level stimulation (n = 54) and low‐level stimulation (n = 60). This trial had a baseline period of 12 weeks and a treatment period of 14 weeks. Patients exiting the study were offered indefinite extension treatment in an open trial. Ben‐Menachem 1994, Ben‐Menachem 1995, Elger 2000, Ramsay 1994, Holder 1992 and Lotvall 1994, are linked to this study.
Excluded studies
We excluded 23 studies for the following reasons: 18 studies were not randomised trials; two studies did not study an eligible population; three studies had been terminated (no results available). For further information on each trial please see Characteristics of excluded studies.
Risk of bias in included studies
See Figure 2 and Figure 3 for a summary of the risk of bias in each included study. Each study was allocated an overall rating for risk of bias: low, high, or unclear. See below for specific domain ratings.
2.
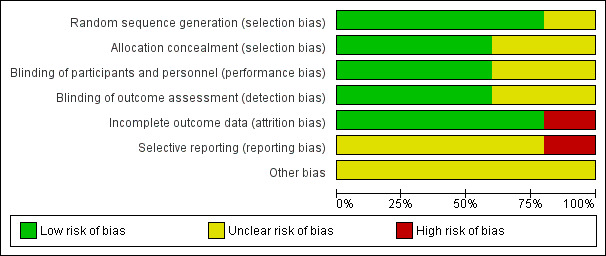
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
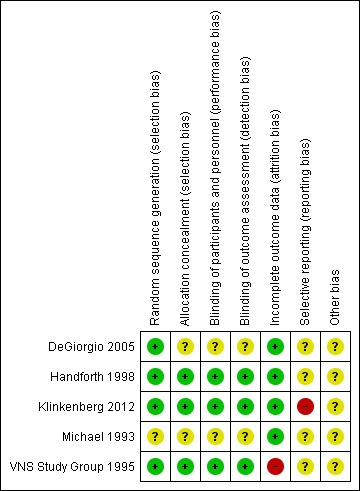
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
In three trials (Handforth 1998; Klinkenberg 2012; VNS Study Group 1995) we rated the method by which allocation was concealed as having a low risk of bias. Two trials did not provide clear methods and were rated as unclear on this domain (DeGiorgio 2005;Michael 1993). As for the domain of sequence generation, we rated four studies (DeGiorgio 2005; Handforth 1998; Klinkenberg 2012, VNS Study Group 1995) as having a low risk of bias due to using a computer‐generated randomisation schedule or random number tables/random permuted blocks. We rated one study (Michael 1993) as unclear due to a lack of details on the methods used.
In the DeGiorgio 2005 study, randomisation occurred in blocks of six (two for each group), with a unique predetermined randomisation schedule for each site. In the Handforth 1998 trial, randomisation schedule was generated by a statistical consultant. A consultant organisation served as central randomiser using this schedule. Randomisation for each study site was in groups of four participants. In order to randomise an individual, the unblinded programmer at that site telephoned the randomiser to obtain the randomised treatment assignment. The blinded interviewer at each site had no access to the randomiser, nor to the treatment assignment list, which was kept in a locked place by the site programmer. In Klinkenberg 2012 participants were allocated to a treatment condition by one trial nurse using a computer program. Finally, in the VNS Study Group 1995 report, randomisation tables were developed by an independent statistician. Assignments were made by a look‐up table in the software used to program the generator. Participants were randomised in blocks of four at each site. The investigators and sponsor were unaware of the assignments prior to randomisation.
Blinding
In all of the studies blinding was achieved by using identical implants within the different groups. We judged blinding of participants as unclear in two papers (DeGiorgio 2005; Michael 1993), as no details of the method of blinding were provided. We rated the other three studies (Handforth 1998;Klinkenberg 2012;VNS Study Group 1995) as having a low risk of bias on this particular domain, because to assure blinding, at each treatment‐phase visit the device was temporarily turned off while the participant was assessed by the blinded interviewer. An important issue in blinded trials on VNS is the difficulty of effectively blinding the patients given the frequency of stimulation‐related side effects such as voice alteration. This could limit the validity of the observed treatment effects.
Incomplete outcome data
We rated three studies (Handforth 1998; Klinkenberg 2012; Michael 1993) as having a low risk of bias for incomplete outcome data as low amounts of missing data were reported and either intention to treat analysis was employed or there were no concerns of missing data having an effect on the overall outcome estimate.We also rated the DeGiorgio 2005 study as unclear risk of bias as three participants out of 64 exited early from the study and an intention to treat analysis was not employed, however it is unclear if this approach as influenced the results of the study. We rated the VNS Study Group 1995 as having a high risk of bias because in this trial 57 patients were randomized to low stimulation, however three patients allocated to high stimulation had their stimulator programmed for low stimulation in error. These patients were analysed in the low stimulation group rather than the high stimulation group they were randomised to. This is not an intention to treat analysis.
Selective reporting
None of the protocols for the included studies were available, therefore we could not compare a priori methods and outcomes to the published reports. Because of this, we rated all but one study (Klinkenberg 2012) as having an unclear risk of bias. It should be noted, however, that based on the information contained in the publications, there was no suspicion of reporting bias. In Klinkenberg 2012, the secondary outcome of IQ which was described in the methods section was not reported in the results, thus we assessed this study as having a high risk of reporting bias..
Other potential sources of bias
All studies were sponsored by Cyberonics, Inc, Webster (TX), the manufacturers of the device, and were therefore rated as having an unclear risk of bias on this domain.
Effects of interventions
See: Table 1
1) High versus Low Vagus Nerve Stimulation
50% or greater reduction in seizure frequency
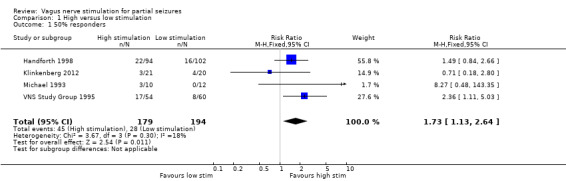
Data from 4 studies contributed to this outcome.
(a) Intention‐to‐treat analysis:
Results of a Chi2 test showed no significant heterogeneity between trial for a response to VNS (Chi2 = 3.67, df = 3, P = 0.30, I2=18%). The overall risk ratio (RR) for a response to high stimulation compared to low stimulation using the fixed‐effect model is 1.73 (95% Cl 1.13 to 2.64, P = 0.01), showing that patients receiving high stimulation are more likely to show a 50% or greater reduction in seizure frequency (See Analysis 1.1.).
1.1. Analysis.
Comparison 1 High versus low stimulation, Outcome 1 50% responders.
(b) Best and worst case scenarios:
No significant heterogeneity was found for these outcomes (worst case: Chi2 = 4.94, df = 3, P = 0.18; best case: Chi2 = 2.13, df = 3, P = 0.55); I2= 0% and 39% respectively. The overall worst case RR (95%) for a response to VNS is 1.61 (95% CI 1.07 to 2.43, P = 0.02) and best case is 1.91 (95% CI 1.27 to 2.89, P = 0.002). For all three analyses, results suggest a statistically significant treatment effect for high stimulation (See Analysis 1.2 and Analysis 1.3)..
1.2. Analysis.
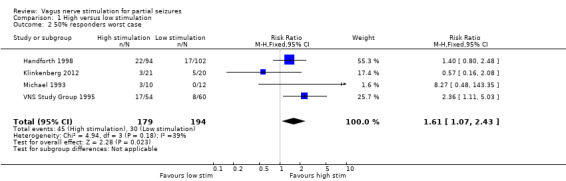
Comparison 1 High versus low stimulation, Outcome 2 50% responders worst case.
1.3. Analysis.
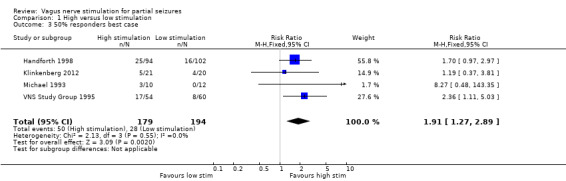
Comparison 1 High versus low stimulation, Outcome 3 50% responders best case.
Treatment withdrawal
Data from four studies contributed to this outcome. Five participants withdrew from high level stimulation and three participants withdrew from low level stimulation in Handforth 1998 and Klinkenberg 2012 combined, while no participant withdrew from either stimulation paradigm in Michael 1993 and VNS Study Group 1995. A Chi2 test revealed no significant statistical heterogeneity (Chi2 = 0.11, df = 1, P = 0.74). The overall risk ratio (RR) for withdrawal for any reason is 2.56 (95% CI 0.51 to 12.71). We found no significant difference in withdrawal between high and low level stimulation P = 0.2 (See Analysis 1.4).
1.4. Analysis.
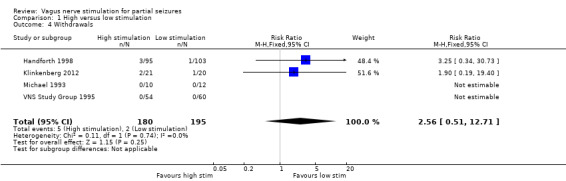
Comparison 1 High versus low stimulation, Outcome 4 Withdrawals.
Adverse effects
The risk ratios (RR) of adverse effects were as follows:
(a) Voice alteration and hoarseness: 2.17 (99% CI 1.49 to 3.17, P = 0.23, I2 = 32%) from three studies recruiting 334 participants; 159 to high level stimulation and 175 to low level stimulation (Handforth 1998; Michael 1993; VNS Study Group 1995). 87 participants reported this adverse effect in the high level stimulation group and 44 in the low level stimulation group (see Analysis 1.5).
1.5. Analysis.
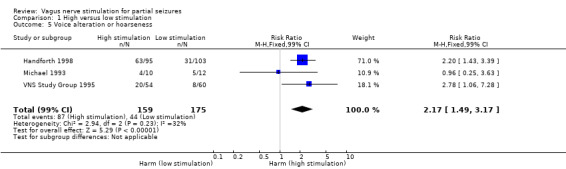
Comparison 1 High versus low stimulation, Outcome 5 Voice alteration or hoarseness.
(b) Cough: 1.09 (99% CI 0.74 to 1.62, P = 0.54, I2 = 0%) from three studies recruiting 334 participants; 159 to high level stimulation and 175 to low level stimulation (Handforth 1998; Michael 1993; VNS Study Group 1995); 51 participants reported this adverse effect in the high level stimulation group and 51 in the low level stimulation group (see Analysis 1.6).
1.6. Analysis.
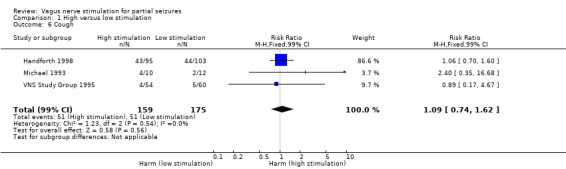
Comparison 1 High versus low stimulation, Outcome 6 Cough.
(c) Dyspnea: 2.45 (99% CI 1.07 to 5.60, P = 0.77, I2 = 0%) from two studies recruiting 312 participants; 149 to high level stimulation and 163 to low level stimulation (Handforth 1998; VNS Study Group 1995); 27 participants reported this adverse effect in the high level stimulation group and 12 in the low level stimulation group (see Analysis 1.7).
1.7. Analysis.
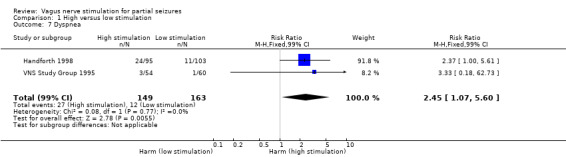
Comparison 1 High versus low stimulation, Outcome 7 Dyspnea.
(d) Pain: 1.01 (99% CI 0.60 to 1.68, P = 0.57, I2 = 0%) from two studies recruiting 312 participants; 149 to high level stimulation and 163 to low level stimulation (Handforth 1998; VNS Study Group 1995); 36 participants reported this adverse effect in the high level stimulation group and 39 in the low level stimulation group (see Analysis 1.8).
1.8. Analysis.
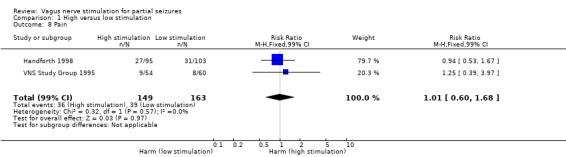
Comparison 1 High versus low stimulation, Outcome 8 Pain.
(e) Paresthesia 0.78 (99% CI 0.39 to 1.53, P = 0.36, I2 = 0%) from two studies recruiting 312 participants; 149 to high level stimulation and 163 to low level stimulation (Handforth 1998; VNS Study Group 1995); 20 participants reported this adverse effect in the high level stimulation group and 28 in the low level stimulation group (see Analysis 1.9).
1.9. Analysis.
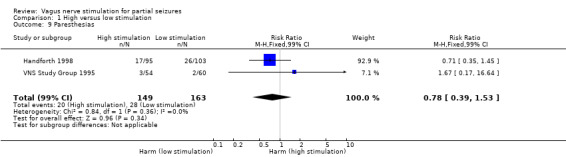
Comparison 1 High versus low stimulation, Outcome 9 Paresthesias.
(f) Nausea: 0.89 (99% CI 0.42 to 1.90, P = 0.10, I2 = 64%) from two studies recruiting 312 participants; 149 to high level stimulation and 163 to low level stimulation (Handforth 1998; Michael 1993); 17 participants reported this adverse effect in the high level stimulation group and 21 in the low level stimulation group (see Analysis 1.10).
1.10. Analysis.
Comparison 1 High versus low stimulation, Outcome 10 Nausea.
(g) Headache: 0.90 (99% CI 0.48 to 1.69, P = 0.16, I2 = 50%) from two studies recruiting 220 participants; 105 to high level stimulation and 115 to low level stimulation (Handforth 1998; VNS Study Group 1995); 24 participants reported this adverse effect in the high level stimulation group and 29 in the low level stimulation group (see Analysis 1.11)
1.11. Analysis.
Comparison 1 High versus low stimulation, Outcome 11 Headache.
One out of 198 participants in Handforth 1998 and two out of 41 participants in Klinkenberg 2012, experienced an infection after implantation and were not randomised. Overall, this shows that voice alteration and hoarseness, and dyspnea are significant adverse effects of high stimulation. Haemorrhage at implantation site, ataxia, dizziness, fatigue and somnolence were not reported in any included studies.
Quality of life (QOL)
Data from two studies are reported narratively; the Dodrill 2000 paper as part of Handforth 1998 and the Holder 1992 paper as part of VNS Study Group 1995 contributed to this outcome.
On the Quality of Life in Epilepsy‐31 (QOLIE‐31), there was no statistically significant differences of interaction effects between high versus low VNS frequency. On the Short Form (36) Health Survey(SF‐36), there was a statistically significant difference between groups on the domains of Physical Function and Social Function, but no difference for all other domains. There were no statistically significant differences between groups on the Medical Outcomes Study (MOS) and Health‐Related Hardiness Scale (H‐RHS). On the Washington Psychosocial Seizure Inventory (WPSI), only financial status was reported to be significantly different between groups (Handforth 1998).
In VNS Study Group 1995, Quality of Life was evaluated according to 'patient,' 'investigator' and 'companion' Global Rating Scales; an evaluation of the patient's condition at each follow up visit compared to baseline measured on a Visual Analogue Scale. Quality of life was significantly improved compared to baseline according to all three Global Rating Scales (patient, investigator and companion) in both the high stimulation and low stimulation groups compared to the low stimulation group (p<0.001 for both groups for all three scales), but no significant difference between stimulation groups was observed in Quality of Life.
In addition, results from these two studies showed that the patients who had at least 50% seizure reduction exhibited signs of slight improvement in QOL variables compared to those patients who did not demonstrate this degree of seizure reduction. Overall, a small number of favourable QOL effects were associated with levels of VNS stimulation that are now typically used clinically.
Cognition
Data from one study (Dodrill 2000 paper as part of Handforth 1998) contributed to this outcome. No statistically significant differences in interaction effects were reported between high versus low frequency VNS on all four measures used: Wonderlic Personnel Test, Digit Cancellation, Stroop Test, Symbol Digit Modalities.
Mood
Data from one study (Elger 2000 paper as part of VNS Study Group 1995) contributed to this outcome. Mood was measured according to the Montgomery–Åsberg Depression Rating Scale (MADRS) at baseline 3 months and 6 months. A MADRS Total score of between 10 and 20 (maximum score 20) indicated mild depressive mood disorder. At baseline, three out of five patients in the low stimulation group and four out of six patients in the high stimulation group had MADRS scores greater than 10, at three months, two out of five patients in the low stimulation group and two out of six patients in the high stimulation group had MADRS scores greater than 10 and at six months, one out of five patients in the low stimulation group and one out of six patients in the high stimulation group had MADRS scores greater than 10. Overall, four out of five patients in the low stimulation group and five out of six patients in the high stimulation group showed decreases in MADRS scores over the study, but no statistically difference in was present between high and low stimulation groups (Mann‐Whitney's test; P < 0.10).
2) Rapid versus Mild versus Slow duty cycle VNS
50% or greater reduction in seizure frequency
Data from just one study (DeGiorgio 2005) contributed to this comparison. The reduction in seizure frequency was 22% for rapid cycle (P = 0.0078), 26% for medium cycle (P = 0.0270), and 29% for slow cycle (P = 0.0004). For all three groups combined, the reduction in seizure frequency was 40%. Between group comparisons revealed no statistically significant differences in seizure frequency (Kruskal Wallis test, p value is not reported). The >50% responder rate was the same for all three groups (six participants in each group achieved 50% or greater reduction in seizure frequency).
Treatment withdrawal
Throughout the study period only three patients withdrew and the reasons for this were: one developed a device infection, one was lost to follow‐up, and one could not tolerate stimulation (rapid cycle). The randomisation assignments of the first two patients are unknown, presumably as this was deemed by the study authors to be irrelevant to the conclusion.
Adverse effects
The percentage of adverse effects in all three groups combined were as follows: post‐operative pain at the generator 21.3%, throat pain and pharyngitis 9.8%, cough 9.8%, voice alteration 4.9%, vocal cord paralysis 1.6%, abdominal pain and diarrhoea 1.6%. Cough and voice alteration were more common among rapid cycle stimulation (26%, versus 5% medium cycle and 9% for slow cycle). Other adverse effects were not sub‐divided into treatment groups.
Discussion
Summary of main results
Five randomised controlled trials which recruited 439 participants were included in this review. All trials were sponsored by Cyberonics, Inc., Webster, TX, USA. In four trials, participants were randomised to high or low VNS and in the remaining trial participants were randomised to duty cycles of rapid, mild or slow VNS.
Results of the overall efficacy analysis show that people receiving high VNS stimulation were 1.73 (95% Cl 1.13 to 2.64) times more likely to have reduced seizures compared to those receiving low stimulation. This effect did not vary substantially and remained statistically significant for both the best and worst case scenarios, accounting for missing outcome data in one study. Results from one study contributed to the comparison of three different duty cycles paradigms (rapid versus mild versus slow), showing no statistically significant differences in seizure frequency. All included studies were of short duration, so no conclusions can be drawn about long term efficacy of VNS.
Results for treatment withdrawal rates of high and low stimulation groups were similar; there was little difference between the numbers of people who dropped out of the high stimulation group (n = 5) compared to the low stimulation group (n = 2). However, due to imprecision of the pooled result (RR 2.56 [95% Cl 0.51 to 12.71]), important differences in withdrawal rates between the stimulation paradigms cannot be ruled out based on current evidence. The most common adverse events were voice alteration and hoarseness, cough, dyspnea, pain, paresthesias, nausea, and headache. For these adverse effects, voice alteration/hoarseness and dyspnea were over twice as likely to occur in people receiving high stimulation. However, there is some uncertainty and imprecision in reported differences in adverse events between groups; there are often wide confidence intervals, making it difficult to draw conclusions. Only three out of sixty‐four subjects exited early in the study comparing rapid versus mild versus slow stimulation (DeGiorgio 2005): one developed a device infection, requiring removal, one could not tolerate stimulation (high stimulation group), and one was lost to follow‐up. This total percentage withdrawal rate of 4.7% suggests that the treatment is well tolerated.
Results from two studies (Handforth 1998; VNS Study Group 1995)contributed to QOL outcome and showed that a small number of favourable QOL effects were associated with VNS stimulation, but no statistically significant differences between high and low level stimulation groups. Data from one study contributed to cognition outcome (Handforth 1998); no statistically significant differences were reported between high versus low frequency VNS on all four measures used. Data from one study contributed to mood outcome (VNS Study Group 1995); the majority of patients showed an improvement in mood on the MADRS scale compared to baseline but no statistically significant differences were reported between high versus low frequency VNS.
Overall completeness and applicability of evidence
Currently there are only five studies which look at VNS for partial seizures, with less than 500 participants in total. The addition of further evidence from future studies may change the results and conclusions of this review.
This review focuses on the use of VNS in drug‐resistant partial seizures. The results cannot be extrapolated to other patient groups like those with generalised epilepsy. The results of this review indicate that VNS is an effective add‐on treatment for drug‐resistant seizures, but we cannot state how VNS compares to other antiepileptic treatments. This is especially true for VNS because it was tested in an active control situation whereas antiepileptic drugs are tested against placebo. Head‐to‐head trials are needed to assess the relative efficacy and tolerability of antiepileptic treatments.
Quality of the evidence
Out of the five included studies, two studies (Handforth 1998; VNS Study Group 1995) were rated individually as having a low risk of bias and the other three studies were rated as having an unclear risk of bias (DeGiorgio 2005; Klinkenberg 2012; Michael 1993), due to lack of methodological detail concerning study design. The GRADE approach was employed to rate the level of evidence per outcome and this is presented in a summary of findings table (see Table 1). For the main outcome of 50% reduction in seizure frequency, the quality of evidence was rated as moderate due to incomplete outcome data from one study contributing to the analysis (VNS Study Group 1995), however results of best case and worst case scenario analysis to account for missing outcome data showed similar results (see Effects of interventions). Tolerability outcomes (withdrawal and adverse effects) were judged as moderate to low quality due to the imprecision of pooled results and incomplete outcome data from one study contributing to the analysis (VNS Study Group 1995).
In three trials, adequate methods of allocation concealment and randomisation were described (Handforth 1998; Klinkenberg 2012; VNS Study Group 1995). In two papers, no details on the methods of blinding of participants and outcome assessors were reported (DeGiorgio 2005; Michael 1993). The issue of blinding in these studies is somewhat more complex than in typical randomised controlled trials of antiepileptic drugs where a placebo tablet can be administered. The different stimulation paradigms raise the possibility that investigators and participants may not have been adequately blinded to the treatment groups because individuals in the control group may been able to detect that the stimulations were very infrequent; this is likely to be an issue in all trials involving a VNS device.
All protocols for the trials were requested from authors, but no protocols were provided to assist in fully assessing the risk of selective outcome reporting, so this remains unclear in most included studies.
Potential biases in the review process
Although all protocols were requested, the time frame in which the majority of the studies were conducted made retrieval of all of these difficult. This could lead to potential bias through omitted information to which we did not have access.
Agreements and disagreements with other studies or reviews
The studies included in this review were essentially active control trials, thus results may be difficult to compare against other meta‐analyses of antiepileptic drugs that were compared against placebo. The magnitude of the risk ratio for high VNS treatment compared to control would tend to be reduced by any anti‐seizure effect of the low stimulation. A higher risk ratio may have been found if high VNS treatment was compared against no stimulation, but the investigators decided that with a low level of stimulation that was thought to be ineffective, participants were less likely to guess which treatment they were receiving.
Another recent review on VNS (Morris 2013) supports the conclusions made in this review with regard to a positive outcome through use of VNS. This review also describes an association between VNS and mood in adult patients, and includes children‐specific analyses.
Authors' conclusions
Implications for practice.
VNS appears to be an effective treatment for people with drug‐resistant partial epilepsy, as an add‐on treatment. Results of the overall efficacy analysis show that VNS stimulation using the high stimulation paradigm was significantly better than low stimulation in reducing seizure frequency by 50%. High and low stimulation VNS are both well tolerated and withdrawals are rare, however limited information regarding withdrawal from treatment was available from the evidence included in this review so important differences between high and low stimulation cannot be excluded. Adverse effects associated with implantation and stimulation were primarily hoarseness, cough, dyspnea, pain, paresthesia, nausea and headache, with voice alteration and dyspnea more likely to occur on high level stimulation than low level stimulation according to current evidence. The adverse effect profile was substantially different from the adverse effect profile associated with antiepileptic drugs, making VNS a potential alternative for patients with difficulty tolerating antiepileptic drug adverse effects.
Implications for research.
Identifying the adverse effect profile of VNS was rather complex because treatment involves both implantation of the device and intermittent stimulation, each with slightly different adverse effects. In addition, these studies were essentially active control trials.
Further research is needed to determine the:
mode of action of VNS;
long term effects of VNS;
details of effective stimulation paradigms/protocols;
effectiveness of VNS compared to antiepileptic drugs currently available.
Feedback
Query regarding analysis 01.01, 21 May 2006
Summary
The following comment was made on 21 May 2006 regarding Analysis 01.01. Comparison 01 High stimulation versus low stimulation, Outcome 01 50% responders. The two groups in the VNS Study Group consists of 54 people and 60 people and NOT 2 x 57 people. This mistake is shown in many of the analyses.
Reply
Whilst there may be a discrepancy between the data presented in this review and the original published report by the VNS Study Group, the authors have not made a mistake in the preparation of this review.
In the VNS study group trial, 57 patients were randomized to high stimulation and 57 were randomized to low stimulation. However, three patients allocated to high stimulation had their stimulator programmed for low stimulation in error. For the paper published in Neurology, these three patients were analysed in the low stimulation group rather than in the group to which they had been allocated. The authors of this Cochrane review preferred to use the more conservative intention to treat analysis in which patients are analysed in the treatment group which they were allocated.
Reply made by Dr Tony Marson (Co‐ordinating Editor ‐ Cochrane Epilepsy Group) on behalf of the review authors (06 August 2008).
Update 2014: Following re‐review of the data extracted from the VNS study Group manuscripts, the majority of the data used in the analyses in this review is presented for the High Stimulation Group of 54 people and the Low Stimulation Group of 60 people; in other words, groups according to the treatment received rather than treatment allocated. In the analysis of the previous version of the review, the event rates reported for the groups of 54 and 60 patients respectively were used in analysis but with group totals assigned as 57 participants per group as an intention to treat analysis.
However, following consideration for this update, given that separate data for the three participants randomised to high stimulation but received low stimulation is not presented, assuming event rates in the treatment received groups would be in same as in the treatment allocated groups may not necessarily be correct. For this reason, the authors of the updated review have presented results in terms of the treatment received groups. They acknowledge that this is not an intention to treat approach and have reflected this in the risk of bias table for the VNS Study Group 1995 study.
Contributors
Comment made by Dr Jesper Erdal.
What's new
| Date | Event | Description |
|---|---|---|
| 23 February 2015 | New search has been performed | The searches were updated on 23rd February 2015. |
| 23 February 2015 | New citation required but conclusions have not changed | Three new studies have been included (identified from a search carried out in September 2013); however the conclusions remain unchanged. A pre‐publication search carried out on 23rd February 2015 identified two potentially relevant studies (Klinkenberg 2014; NCT02089243 2014). These will be addressed at the next update. |
History
Protocol first published: Issue 1, 2001 Review first published: Issue 1, 2002
| Date | Event | Description |
|---|---|---|
| 7 August 2009 | Amended | Copyedits made at editorial base. |
| 24 October 2008 | Amended | Search strategy amended to comply with RevMan 5. |
| 11 August 2008 | Feedback has been incorporated | A response has now been made to the feedback originally left on 21 May 2006. |
| 31 July 2008 | Amended | Converted to new review format. |
| 19 July 2007 | New search has been performed | Searches updated 6 July 2007; no new studies identified. |
Acknowledgements
The review authors acknowledge Dr. Michael D. Privitera, Dr. Timothy T.E. Welty, Dr. David D.M. Ficker and Dr. Jeffrey Welge for the contributions that they made to the previous review. We thank Anat Fisher and Jun Xia for helping to translate articles (from Hebrew and Chinese respectively).
This project was supported by the National Institute for Health Research, via Cochrane Programme Grant funding to the Epilepsy Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Appendices
Appendix 1. Epilepsy Specialized Register
#1 MeSH DESCRIPTOR Vagus Nerve Explode All
#2 (vagus or vagal) NEAR2 stimul*
#3 (#1 OR #2)
Appendix 2. CENTRAL search strategy
#1 MeSH descriptor: [Vagus Nerve] explode all trees
#2 (vagus or vagal) near/2 stimul*
#3 #1 or #2
#4 (epilep* or seizure* or convuls*):ti,ab,kw (Word variations have been searched)
#5 MeSH descriptor: [Epilepsy] explode all trees
#6 MeSH descriptor: [Seizures] explode all trees
#7 (#4 or #5 or #6) in Trials
#8 #3 and #7
Appendix 3. MEDLINE search strategy
1. exp Vagus Nerve/
2. ((vagus or vagal) adj3 stimul$).tw.
3. 1 or 2
4. exp Epilepsy/
5. exp Seizures/
6. (epilep$ or seizure$ or convuls$).tw.
7. 4 or 5 or 6
8. exp Pre‐Eclampsia/ or exp Eclampsia/
9. 7 not 8
10. (validation studies or clinical trial or clinical trial phase i or clinical trial phase ii or clinical trial phase iii or clinical trial phase iv or comparative study or evaluation studies or multicenter study).pt.
11. ((observation$ or cohort or case$ or cross?section$ or "cross section$" or "time‐series" or "time series" or "before and after" or "before‐and‐after" or retrospective) adj2 (study or trial or method)).mp.
12. (randomized controlled trial or controlled clinical trial).pt. or (randomi?ed or placebo or randomly).ab.
13. clinical trials as topic.sh.
14. trial.ti.
15. 10 or 11 or 12 or 13 or 14
16. exp animals/ not humans.sh.
17. 15 not 16
18. 17 not case reports.pt.
19. 3 and 9 and 18
Appendix 4. SCOPUS Search Strategy
(TITLE‐ABS‐KEY((vagus or vagal) PRE/2 stimul*)) AND ((TITLE‐ABS‐KEY(epilep* OR "infantile spasm" OR seizure OR convuls* OR (syndrome W/2 (aicardi OR angelman OR doose OR dravet OR janz OR jeavons OR "landau kleffner" OR "lennox gastaut" OR ohtahara OR panayiotopoulos OR rasmussen OR rett OR "sturge weber" OR tassinari OR "unverricht lundborg" OR west)) OR "ring chromosome 20" OR "R20" OR "myoclonic encephalopathy" OR "pyridoxine dependency") AND NOT (TITLE(*eclampsia) OR INDEXTERMS(*eclampsia))) OR (TITLE‐ABS‐KEY(lafora* W/4 (disease OR epilep*)) AND NOT (TITLE(dog OR canine) OR INDEXTERMS(dog OR canine)))) AND ((TITLE((randomiz* OR randomis* OR controlled OR placebo OR blind* OR unblind* OR "parallel group" OR crossover OR "cross over" OR cluster OR "head to head") PRE/2 (trial OR method OR procedure OR study)) OR ABS((randomiz* OR randomis* OR controlled OR placebo OR blind* OR unblind* OR "parallel group" OR crossover OR "cross over" OR cluster OR "head to head") PRE/2 (trial OR method OR procedure OR study))) OR (TITLE((validation OR clinical OR cohort OR comparative OR controlled OR evaluation OR multicenter OR observation* OR "case control" OR "case series" OR "cross section*" OR "time series" OR "before and after" OR prospective OR retrospective) PRE/2 (trial OR method OR procedure OR study)) OR ABS((validation OR clinical OR cohort OR comparative OR controlled OR evaluation OR multicenter OR observation* OR "case control" OR "case series" OR "cross section*" OR "time series" OR "before and after" OR prospective OR retrospective) PRE/2 (trial OR method OR procedure OR study))))
Appendix 5. ClinicalTrials.gov Search Strategy
vagus nerve stimulation AND epilepsy
Appendix 6. WHO International Clinical Trials Registry Platform (ICTRP) Search Strategy
http://apps.who.int/trialsearch/
vagus nerve stimulation AND epilepsy
Data and analyses
Comparison 1. High versus low stimulation.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 50% responders | 4 | 373 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.73 [1.13, 2.64] |
| 2 50% responders worst case | 4 | 373 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.61 [1.07, 2.43] |
| 3 50% responders best case | 4 | 373 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.91 [1.27, 2.89] |
| 4 Withdrawals | 4 | 375 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.56 [0.51, 12.71] |
| 5 Voice alteration or hoarseness | 3 | 334 | Risk Ratio (M‐H, Fixed, 99% CI) | 2.17 [1.49, 3.17] |
| 6 Cough | 3 | 334 | Risk Ratio (M‐H, Fixed, 99% CI) | 1.09 [0.74, 1.62] |
| 7 Dyspnea | 2 | 312 | Risk Ratio (M‐H, Fixed, 99% CI) | 2.45 [1.07, 5.60] |
| 8 Pain | 2 | 312 | Risk Ratio (M‐H, Fixed, 99% CI) | 1.01 [0.60, 1.68] |
| 9 Paresthesias | 2 | 312 | Risk Ratio (M‐H, Fixed, 99% CI) | 0.78 [0.39, 1.53] |
| 10 Nausea | 2 | 220 | Risk Ratio (M‐H, Fixed, 99% CI) | 0.89 [0.42, 1.90] |
| 11 Headache | 2 | 312 | Risk Ratio (M‐H, Fixed, 99% CI) | 0.90 [0.48, 1.69] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
DeGiorgio 2005.
| Methods | Randomised, prospective, active‐control study. Pre‐randomisation baseline period: 4 weeks. Duration of treatment: 3 months. This period included Month 1 ‐ Month 2 ‐ Month 3 time‐points. |
|
| Participants | A multi‐centre trial (USA). 64 people randomised. Group A (rapid cycle): 19 participants; mean output current at completion of study 0.87 mA. Group B (med cycle): 19 participants; mean output current at completion of study 0.80 mA. Group C (low cycle): 23 participants; mean output current at completion of study 0.93 mA. |
|
| Interventions | Randomised comparison of three distinct duty‐cycles: on/off time 7 s/18 s, duty‐cycle 28%, frequency 20 Hz, pulse width 500 sec (rapid cycle ‐ Group A); on/off time 30 s/30 s, duty‐cycle 50%, frequency 20 Hz, pulse width 250 sec (mild cycle ‐ Group B); and on/off time 30 s/3min, duty‐cycle 14%, frequency 30 Hz, pulse width 500 sec (slow cycle ‐ Group C) in treatment of refractory partial seizures. All patients had an identical implantation of the vagus nerve stimulation device (NeuroCybernetic Prosthesis, Cyberonics). |
|
| Outcomes | Primary outcome: Seizure frequency (50% and 75% reduction of seizures). Secondary outcomes: a) Dropouts. b) Adverse events. |
|
| Notes | Supported by a grant from Cyberonics, Inc., Webster, TX. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation occurred in blocks of six (2 for each group), with a unique predetermined randomisation schedule for each site. |
| Allocation concealment (selection bias) | Unclear risk | No details of concealment of allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Identical implants used, but no details of method of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No information provided. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3 out 64 participants exited early.One developed a device infection so the device had to be removed, one could not tolerate rapid cycle stimulation so was converted to a standard duty cycle and removed from the study and one participant was lost to follow up. No intention‐to‐treat analysis was performed. |
| Selective reporting (reporting bias) | Unclear risk | Protocol unavailable, but appears all expected and pre‐specified outcomes are reported. |
| Other bias | Unclear risk | The study appeared to be free of other sources of bias. |
Handforth 1998.
| Methods | Randomised, prospective, double blind, active‐control study. Pre‐randomisation baseline period: 12‐16 weeks. Duration of treatment: 16 weeks. This period included 2‐12‐16 week time‐points. |
|
| Participants | A multi‐centre trial (USA). 198 people randomised. High stimulation group: 95 participants; mean age 32.1 years; 51.6% male and 48.4% female; mean seizures/day 1.59; mean duration of epilepsy 22.1 years. Low stimulation group: 103 participants; mean age 34.2 years; 42.7% male and 57.3% female; mean seizures/day 0.97; mean duration of epilepsy 23.7 years. |
|
| Interventions | Comparison of high (on/off cycles of 30 seconds every 5 minutes, each "on" period consisting of 500 µs duration pulses at 30 Hz frequency) and low stimulation (on/off cycles of 30 seconds every 3 hours, each "on" cycle of 130 µs duration pulse at 1 Hz frequency) in treatment of refractory partial seizures. All patients had an identical implantation of the vagus nerve stimulation device (NeuroCybernetic Prosthesis, Cyberonics). |
|
| Outcomes | Primary outcome: Seizure frequency (50% reduction of seizures). Secondary outcomes: a) Dropouts. b) Adverse events. c) Cognitive impact (reported in Dodrill 2000 paper). d) Quality‐of‐life (QOL) impact (reported in Dodrill 2000 paper). |
|
| Notes |
DODRILL 2000 Epilepsy and Behavior and AMAR A.P. 1998 Neurosurgery are linked to this study. Supported by a grant from Cyberonics, Inc., Webster, TX. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation schedule was generated by a statistical consultant before study initiation. |
| Allocation concealment (selection bias) | Low risk | Telephone communication to obtain randomised treatment assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Study personnel and participants are blinded. Identical implants used. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The study data were analysed by a blinded interviewer. Identical implants used. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4 patient withdrawals, but the reasons for exclusion are reported. |
| Selective reporting (reporting bias) | Unclear risk | All outcomes stated in methods section of paper were reported in the results. There was no protocol available to check to priori outcomes. |
| Other bias | Unclear risk | All studies are sponsored by Cyberonics, the manufactures of the device. |
Klinkenberg 2012.
| Methods | Randomised, double‐blinded add‐on, active‐control study in children with refractory partial seizures. Pre‐randomisation baseline period: 12 weeks. Duration of treatment phase: 20 weeks. |
|
| Participants | A multi‐centre trial (Holland). 41 people randomised. High‐output stimulation group: 21 participants; mean age at onset 2:10 (y:mo); median age at onset 1:2 (y:mo); mean age at implantation 10:11 (y:mo); 11/10 male/female; median seizures/day 2.1; Localisation related 90% (symptomatic 71%, cryptogenic (19%); Generalized 10% (Idiopathic 0, symptomatic 10%). Low‐ouput stimulation group: 20 participants; mean age at onset 1:8 (y:mo); median age at onset 1:2 (y:mo); mean age at implantation 11:6 (y:mo);12/8 male/female; median seizures/day 0.9; Localisation related 80% (symptomatic 50%, cryptogenic (30%); Generalized 20% (Idiopathic 10%, symptomatic 10%). A small sample (6 patients) had generalised epilepsy (2 idiopathic and 2 symptomatic). |
|
| Interventions | Comparison of high (output current 0.25 mA, duty‐cycle on/off 30 s/5 min, frequency 30 Hz, pulse width 0.5 ms) and low (output current 0.25 mA, duty‐cycle on/off 14 s/60 min, frequency 1 Hz, pulse width 0.1 ms) stimulation frequency in treatment of refractory partial seizures. In the treatment group the current was increased stepwise at 2 week intervals to the maximally tolerated output current (maximum 1.75 mA). All patients had an identical implantation of the vagus nerve stimulation device (NeuroCybernetic Prosthesis, Cyberonics). |
|
| Outcomes | Primary outcomes: Seizure frequency (50% reduction of seizures). Secondary outcomes: a) Dropouts. b) Adverse events. c) Intelligence quotient (IQ), assessment described in the methods section of the study. |
|
| Notes |
AALBERS 2012 NeuroImmunoModulation is linked to this study. Supported by Cyberonics, Inc., Webster, TX. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated randomisation method used. |
| Allocation concealment (selection bias) | Low risk | Participants were allocated to a treatment condition by one trial nurse using a computer program. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Neurologist, participants and parents are blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigators are blinded. Identical implants used. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3 patient withdrawals, but the reasons for exclusion are reported. |
| Selective reporting (reporting bias) | High risk | The secondary outcome of IQ described in the methods was not reported in the results. There was no protocol available to check to priori outcomes. |
| Other bias | Unclear risk | All studies are sponsored by Cyberonics, the manufacturer of the device |
Michael 1993.
| Methods | Randomised, controlled, double blind, active‐control study of patients with refractory partial seizures. Pre‐randomisation baseline period: 12 weeks. Duration of treatment: 14 weeks. Efficacy was determined at the end of the acute phase. At the end of the 14 week double‐blind phase patients entered an extension phase in which low stimulation patients were switched to high stimulation. |
|
| Participants | A multi‐centre trial (USA). 22 people randomised. High stimulation group: 10 participants. Low stimulation group: 12 participants. Mean age 32 years (range 15‐56); seizure frequency 2 per day; mean duration of epilepsy 19 years (range 5‐32). |
|
| Interventions | Comparison of high (output current 1.0‐3.0 mA, on/off time 30 s/5 min, frequency 30 Hz, pulse width 500 µs) and low (output current 0.25‐0.5 mA, on/off time 30 s/60‐90 min, frequency 1 Hz, pulse width 130 µs) stimulation in treatment of refractory partial seizures. All patients had an identical implantation of the vagus nerve stimulation device (NeuroCybernetic Prosthesis, Cyberonics). |
|
| Outcomes | Primary outcome: Seizure frequency (mean seizure frequency percent reduction).
Secondary outcomes: a) Dropouts. b) Adverse events. |
|
| Notes | Supported by Cyberonics, Inc., Webster, TX. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation not specified. |
| Allocation concealment (selection bias) | Unclear risk | No information provided. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No details provided. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | No details provided. Identical implants used. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants were included in the analysis. |
| Selective reporting (reporting bias) | Unclear risk | Protocol unavailable, but appears all expected and pre‐specified outcomes are reported. |
| Other bias | Unclear risk | All studies are sponsored by Cyberonics, the manufacturer of the device. |
VNS Study Group 1995.
| Methods | Randomised, prospective, double‐blind, active‐control study. Pre‐randomisation baseline period: 12 weeks. Duration of treatment: 14 weeks. Efficacy was determined at the 12 week. At the end of the 14 week double‐blind phase patients entered an extension phase in an open trial. |
|
| Participants | A multi‐centre trial (USA, Canada, Sweden and Germany). 114 people randomised. High stimulation group: 54 participants; mean age 33.1 years; 61% male and 39% female; mean seizures/day 1.49; median seizures/day 0.73; mean duration of epilepsy 23.1 years; simple partial seizures 24 participants; complex partial seizures 50 participants; secondarily generalised seizures 38 participants. Low stimulation group: 60 participants; mean age 33.5 years; 63% male and 37% female; mean seizures/day 1.71; median seizures/day 0.82; mean duration of epilepsy 20.0 years; simple partial seizures 25 participants; complex partial seizures 58 participants; secondarily generalised seizures 33 participant. |
|
| Interventions | Comparison of high (output current 0.25‐3.0 mA, on/off time 30‐90 s/5‐10 min, frequency 20‐50 Hz, pulse width 500 µs) and low (output current 0.25‐1.75 mA, on/off time 30 s/60‐180 min, frequency 1‐2 Hz, pulse width 130 µs) stimulation in treatment of refractory partial seizures. All patients had an identical implantation of the vagus nerve stimulation device (NeuroCybernetic Prosthesis, Cyberonics). |
|
| Outcomes | Primary outcome: Seizure frequency (50% and 75% reduction of seizures). Secondary outcomes: a) Dropouts. b) Adverse events. c) Quality of life (reported in Holder 1992 paper). d) Mood changes (reported in Elger 2000 paper). |
|
| Notes |
BEN‐MENACHEM 1994 Epilepsy Research, BEN‐MENACHEM 1995 Epilepsy Research, ELGER 2000 Epilepsy Research, RAMSAY 1994 Epilepsia, HOLDER 1992 PACE and LOTVALL 1994 Epilepsy Research, are linked to this study. Supported by a grant from Cyberonics, Inc., Webster, TX. I did not contact study authors because the study is quite old. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation tables were developed by an independent statistician with assignments based on the patient's identification code. |
| Allocation concealment (selection bias) | Low risk | Assignments were made automatically by a look‐up table in the PC software used to program the generator. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants are blinded and one investigator for each site was unblinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The interviewer remained blinded to treatment group. Identical implants used. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 57 participants were randomised to low stimulation. 3 participants allocated to high stimulation had their stimulator programmed for low stimulation in error. These patients were analysed in the low stimulation group according to the treatment they received rather than the treatment they were randomised to . This is not an intention to treat analysis. |
| Selective reporting (reporting bias) | Unclear risk | All outcomes stated in methods section of paper were reported in the results. There was no protocol available to check to priori outcomes. |
| Other bias | Unclear risk | All studies are sponsored by Cyberonics, the manufacturer of the device. |
VNS = Vagus Nerve Stimulation
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Clarke 1997 | Not an RCT. |
| Cukiert 2013 | Ineligible population (patients with Lennox‐Gastaut Syndrome). |
| DeGiorgio 2000 | Not an RCT. |
| Garcia‐Navarrete 2013 | Not an RCT. |
| George 1994 | Not an RCT. |
| Hornig 1997 | Not an RCT. |
| Marras 2013 | Not an RCT. |
| Marrosu 2003 | Not an RCT. |
| Marrosu 2005 | Not an RCT. |
| Morris 1999 | Not randomised controlled trial. |
| Muller 2010 | Ineligible population (patients with Lennox‐Gastaut Syndrome). |
| NCT00215215 2005 | This study has been terminated and no data was available. |
| NCT01118455 2004 | This study has been terminated and no data was available (insufficient enrolment). |
| NCT01178437 2009 | This study has been terminated and no data was available. |
| Ronkainem 2006 | Not an RCT. |
| Rossignol 2009 | Not an RCT. |
| Salinsky 1996 | Not an RCT. |
| Scherrrmann 2001 | Not an RCT. |
| Shimizu 1995 | Not an RCT. |
| Sirven 2000 | Not an RCT. |
| Uthman 1993 | Not an RCT. |
| Wang 2004 | Not an RCT. |
| Wang 2009 | Not an RCT. |
Characteristics of studies awaiting assessment [ordered by study ID]
Boon 2001.
| Methods | No details. |
| Participants | No details. |
| Interventions | No details. |
| Outcomes | No details. |
| Notes |
Gates 2005.
| Methods | Randomised, double‐blind study to evaluate the effects of two parameter settings (low and high) on seizure control. |
| Participants | The study population consisted of 13 patients with a diagnosis of refractory seizures that are treated with adjunctive VNS Therapy. The two groups were a high stimulation setting (HSS, n=5) group and a low stimulation setting (LSS, n=8) group comparison. |
| Interventions | VNS therapy. |
| Outcomes | Efficacy was evaluated as reduction in seizure frequency. The mean pre‐activation seizure frequencies/60‐days for the LSS and HSS‐groups were 16.0 and 43.6 respectively. For the LLS group, the 30‐, 90‐, and 180‐day post‐activation mean seizure frequencies were 9.1, 9.1 and 20.4 respectively. For the HSS group, the 30‐, 90‐, and 180‐day post‐activation mean seizure frequencies were 17.0, 35.6 and 68.0 respectively. |
| Notes |
Klinkenberg 2014.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes |
Landy 1993.
| Methods | Randomised controlled study of patients that received either high or low current stimulation. |
| Participants | The study population consisted of 9 patients with complex partial seizures that are treated with adjunctive VNS Therapy. |
| Interventions | VNS therapy. |
| Outcomes | Efficacy was evaluated as reduction in seizure frequency. The high‐current stimulation group showed a median reduction in seizure frequency of 27.7% compared to the preimplantation baseline, while the low‐current stimulation group showed a median increase of 6.3%. |
| Notes |
Leach 2001.
| Methods | Randomized, blinded, crossover study comparing the effect of three different stimulus settings (off, standard, and rapid stimulation). Each treatment phase lasted 6 months and seizure frequency was monitored. |
| Participants | 21 patients with refractory epilepsy were randomised and were treated with adjunctive VNS Therapy. Median age was 25 years; median duration of epilepsy was 21 years. |
| Interventions | VNS therapy. |
| Outcomes | Efficacy was evaluated as reduction in seizure frequency. Median reduction in GTC seizures during standard and rapid stimulation was 31 and 24% respectively. Median reduction in complex partial seizures was 0 during rapid stimulation and 50% during standard stimulation and 50% during rapid stimulation. 3 patients were withdrawn from the study because of adverse events; 1 patient withdrew because of worsening seizures; 2 withdrew consent and there were an additional 2 protocol violations. |
| Notes |
Ney 1998.
| Methods | Randomised controlled study of patients in the treatment arm stimulated with levels that were thought to be therapeutic, whereas those in the placebo arm received VNS at levels that were thought to be sub‐therapeutic. |
| Participants | The study population consisted of patients with refractory epilepsy. |
| Interventions | VNS therapy: comparison of high (therapeutic) and low (sub‐therapeutic) stimulation frequency. |
| Outcomes | Efficacy was evaluated as reduction in seizure frequency. There was a 28% reduction in seizure frequency in the treatment arm and a 15% reduction in the placebo arm after 3 months of treatment. |
| Notes |
Scherrmann 2001.
| Methods | Study 2: a prospective randomised controlled trial to compare efficacy of standard stimulation and rapid cycle. |
| Participants | The study population consists of patients with drug‐resistant epilepsy. |
| Interventions | VNS therapy: to compare efficacy of standard stimulation and rapid cycle. |
| Outcomes | Efficacy was evaluated as >50% seizure frequency reduction. Patients treated with standard parameters showed a responder rate of 25%, whereas patients under rapid‐cycle conditions showed a responder rate of 39%. |
| Notes |
Characteristics of ongoing studies [ordered by study ID]
DRKS00003689 2012.
| Trial name or title | A randomised, controlled, double‐blind, two‐arm clinical trial to assess safety and efficacy of transcutaneous vagus nerve stimulation in patients with drug‐resistant epilepsy. |
| Methods | Randomized controlled trial, parallel, double‐blind,active control. |
| Participants | The study population will consist of patients with drug‐resistant epilepsy. |
| Interventions | Add‐on therapy with high‐level t‐VNS in comparison with low‐level t‐VNS. |
| Outcomes | 1) Seizure frequency. 2) Safety. 3) Quality of life. |
| Starting date | April 2012 |
| Contact information | Nadine Wolf, Henkestr. 91, 91052 Erlangen ‐ Germany nadine.wolf@cerbomed.com: Birgit Klee birgit_klee@medpharmtec.de |
| Notes |
NCT00782249 2005.
| Trial name or title | Trial comparing different stimulation paradigms in patients treated with vagus nerve stimulation for refractory epilepsy. |
| Methods | Prospective randomised trial. |
| Participants | The study population consist of patients with refractory epilepsy. |
| Interventions | Comparison of three different paradigms in patients treated with VNS therapy. |
| Outcomes | 1) Seizure frequency. 2) Side effects. 3) Quality of life. |
| Starting date | October 2005 |
| Contact information | Veerle De Herdt, MD veerle.deherdt@ugent.be |
| Notes |
NCT01281293 2011.
| Trial name or title | Vagus Nerve Stimulation Clinical Outcomes Measured Prospectively in Patients Stimulated. |
| Methods | Long Term, Prospective, Observational, Multi‐site Outcome Study to Follow the Clinical Course and Seizure Reduction of Patients With Refractory Seizures Who Are Being Treated With Adjunctive VNS Therapy. |
| Participants | The study population consist of patients with a diagnosis of refractory seizures that are treated with adjunctive VNS Therapy. |
| Interventions | VNS therapy. |
| Outcomes | 1) Efficacy. 2) Safety and tolerability. |
| Starting date | January 2011 |
| Contact information | Mark Bunker, PharmD mark.bunker@cyberonics.com |
| Notes |
NCT01378611 2006.
| Trial name or title | Does VNS interact with the serotonergic and immune system in children with intractable epilepsy? |
| Methods | Clinical randomised controlled observer blinded add‐on design. |
| Participants | The study population consist of children (age 4‐18 years) with intractable epilepsy and not eligible for resective surgery. |
| Interventions | VNS therapy. |
| Outcomes | Seizure frequency. |
| Starting date | March 2006 |
| Contact information | No details. |
| Notes |
NCT01910129 2013.
| Trial name or title | Neurostimulation to the vagus nerve for the reduction in frequency of seizures associated with epilepsy. |
| Methods | A randomised, multicenter, double‐blind, parallel, crossover study. |
| Participants | The study population consist of subjects 18 or older with seizures associated with epilepsy. |
| Interventions | VNS therapy. |
| Outcomes | 1) Frequency, severity and duration of seizure activity. 2) Type and frequency of adverse events. |
| Starting date | July 2013 |
| Contact information | Professor Roy Beran, Australia 0294114991 |
| Notes |
NCT02089243 2014.
| Trial name or title | |
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Starting date | |
| Contact information | |
| Notes |
Differences between protocol and review
This update changed the inclusion criteria slightly to include active controlled trials.
Contributions of authors
Mariangela Panebianco was primarily responsible for the writing of this update and completed data extraction and risk of bias assessments. Alexandra Rigby assessed studies for eligibility, extracted data and assessed risk of bias, and Jennifer Weston provided training, updated the methods, and double checked data extraction and risk of bias. Anthony G. Marson provided guidance and manuscript feedback during the update process.
Sources of support
Internal sources
No sources of support supplied
External sources
-
National Institute for Health Research, UK.
This review presents independent research commissioned by the National Institute for Health Research (NIHR). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Declarations of interest
Nothing to declare.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
DeGiorgio 2005 {published data only}
- DeGiorgio C, Heck C, Bunch S, Britton J, Green P, Lancman M, et al. Vagus nerve stimulation for epilepsy: randomized comparison of three stimulation paradigms. Neurology 2005;65(2):317‐9. [DOI] [PubMed] [Google Scholar]
Handforth 1998 {published data only}
- Amar AP, Heck C, Levi M, Smith T, DeGiorgio CM, Oviedo S, et al. An institutional experience with cervical vagus nerve trunk stimulation for medically refractory epilepsy: rationale, technique and outcome. Neurosurgery 1998;43(6):1265‐76. [DOI] [PubMed] [Google Scholar]
- Dodrill CB, Morris GL. Effects of vagal nerve stimulation on cognition and quality of life in epilepsy. Epilepsy & Behavior 2000;2(1):46‐53. [DOI] [PubMed] [Google Scholar]
- Handforth A, DeGiorgio CM, Schachter SC, Uthman BM, Naritoku DK, Tecoma ES, et al. Vagus nerve stimulation therapy for partial‐onset seizures: a randomized active‐control trial. Neurology 1998;51(1):48‐55. [DOI] [PubMed] [Google Scholar]
Klinkenberg 2012 {published data only}
- Aalbers MW, Klinkenberg S, Rijkers K, Verschuure P, Kessels A, Aldenkamp A, et al. The effects of vagus nerve stimulation on pro‐ and anti‐inflammatory cytokines in children with refractory epilepsy: an exploratory study. Neuroimmunomodulation 2012;19(6):352‐8. [DOI] [PubMed] [Google Scholar]
- Klinkenberg S, Aalbers MW, Vles JSH, Cornips EMJ, Rijkers K, Leenen L, et al. Vagus nerve stimulation in children with intractable epilepsy: a randomized controlled trial. Development Medicine & Child Neurology 2012;54(9):855‐61. [DOI] [PubMed] [Google Scholar]
Michael 1993 {published data only}
- Michael JE, Wegener K, Barners DW. Vagus nerve stimulation for intractable seizures: one year follow‐up. Journal of Neuroscience Nursing 1993;25(6):362‐6. [DOI] [PubMed] [Google Scholar]
VNS Study Group 1995 {published data only}
- Ben‐Menachem E, Hamberger A, Hedner T, Hammond EJ, Uthman BM, Slater J, et al. Effects of vagus nerve stimulation on amino acids and other metabolites in the CSF of patients with partial seizures. Epilepsy Research 1995;20(3):221‐7. [DOI] [PubMed] [Google Scholar]
- Ben‐Menachem E, Manon‐Espaillat R, Ristanovic R, Wilder BJ, Stefan H, Mirza W, et al. Vagus nerve stimulation for treatment of partial seizures: 1. A controlled study of effect on seizures. Epilepsia 1994;35(3):616‐26. [DOI] [PubMed] [Google Scholar]
- Elger G, Hoppe C, Falkai P, Rush AJ, Elger CE. Vagus nerve stimulation is associated with mood improvements in epilepsy patients. Epilepsy Research 2000;42(2‐3):203‐10. [DOI] [PubMed] [Google Scholar]
- Holder LK, Wernicke JF, Tarver WB. Treatment of refractory partial seizures: preliminary results of a controlled study. Pacing & Clinical Electrophysiology 1992;15(10 Pt 2):1557‐71. [DOI] [PubMed] [Google Scholar]
- Lotvall J, Lunde H, Augustinson LE, Hedner T, Svedmyr N, Ben‐Menachem E. Airway effects of direct left‐sided cervical vagal stimulation in patients with complex partial seizures. Epilepsy Research 1994;18(2):149‐54. [DOI] [PubMed] [Google Scholar]
- Ramsay RE, Uthman BM, Augustinsson LE, Upton ARM, Naritoku D, Willis J, Treig T, Barolat G, Wernicke JF, First international Vagus Nerve Stimulation Study Group. Vagus nerve stimulation for treatment of partial seizures: 2. Safety, side effects, and tolerability. Epilepsia 1994;35(3):627‐36. [DOI] [PubMed] [Google Scholar]
- The Vagus Nerve Stimulation Study Group. A randomized controlled trial of chronic vagus nerve stimulation for treatment of medically intractable seizures. Neurology 1995;45(2):224‐30. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Clarke 1997 {published data only}
- Clarke BM, Upton ARM, Griffin H, Fitzpatrick D, DeNardis M. Seizure control after stimulation of the vagus nerve: clinical outcome measures. Canadian Journal of Neurological Sciences 1997;24(3):222‐5. [DOI] [PubMed] [Google Scholar]
Cukiert 2013 {published data only}
- Cukiert A, Cukiert CM, Burattini JA, LIma AM, Forster CR, Baise C, et al. A prospective long‐term study on the outcome after vagus nerve stimulation at maximally tolerated current intensity in a cohort of children with refractory secondary generalized epilepsy. Neuromodulation 2013;16(6):551‐6. [DOI: 10.1111/j.1525-1403.2012.00522.x; PUBMED: 23738578 ] [DOI] [PubMed] [Google Scholar]
DeGiorgio 2000 {published data only}
- DeGiorgio CM, Schachter SC, Handforth A, Salinsky M, Thompson J, Uthman B, et al. Prospective long term study of vagus nerve stimulation for the treatment of refractory seizures. Epilepsia 2000;41(9):1195‐2000. [DOI] [PubMed] [Google Scholar]
Garcia‐Navarrete 2013 {published data only}
- Garcia‐Navarrete E, Torres CV, Gallego I, Navas M, Pastor J, Sola RG. Long‐term results of vagal nerve stimulation for adults with medication‐resistant epilepsy who have been on unchanged antiepileptic medication. Seizure 2013;22(1):9‐13. [DOI] [PubMed] [Google Scholar]
George 1994 {published data only}
- George R, Salinsky M, Kuzniecky R, Rosenfeld W, Bergen D, Tarver WB, et al. Vagus nerve stimulation for treatment of partial seizures: 3. Long‐term follow‐up on first 67 patients exiting a controlled study. Epilepsia 1994;35(3):637‐43. [DOI] [PubMed] [Google Scholar]
Hornig 1997 {published data only}
- Hornig GW, Murphy JV, Schallert G, Tilton C. Left vagus nerve stimulation in children with refractory epilepsy: an update. Southern Medical Journal 1997;90(5):484‐8. [DOI] [PubMed] [Google Scholar]
Marras 2013 {published data only}
- Marras CE, Chiesa V, Benedictis A, Franzini A, Rizzi M, Villani F, et al. Vagus nerve stimulation in refractory epilepsy: new indications and outcome assessment. Epilepsy and Behavior 2013;28(3):374‐8. [DOI] [PubMed] [Google Scholar]
Marrosu 2003 {published data only}
- Marrosu F, Serra A, Maleci A, Puligheddu M, Biggio G, Piga M. Correlation between GABA‐A receptor density and vagus nerve stimulation in individuals with drug‐resistant partial epilepsy. Epilepsy Research 2003;55(1‐2):59‐70. [DOI] [PubMed] [Google Scholar]
Marrosu 2005 {published data only}
- Marrosu F, Santoni F, Puligheddu M, Barberini L, Maleci A, Ennas F, et al. Increase in 20‐50 Hz (gamma frequencies) power spectrum and synchronization after chronic vagal nerve stimulation. Clinical Neurophysiology 2005;116(9):2026‐36. [DOI] [PubMed] [Google Scholar]
Morris 1999 {published data only}
- Morris GL 3rd, Mueller WM, The Vagus Nerve Stimulation Group. Long‐term treatment with vagus nerve stimulation in patients with refractory epilepsy. Neurology 1999;53(8):1731‐5. [DOI] [PubMed] [Google Scholar]
Muller 2010 {published data only}
- Muller K, Fabo D, Entz L, Kelemen A, Halasz P, Rasonyi G, et al. Outcome of vagus nerve stimulation for epilepsy in Budapest. Epilepsia 2010;51(Suppl.3):98‐101. [DOI] [PubMed] [Google Scholar]
NCT00215215 2005 {published data only}
- NCT00215215. Effectiveness study comparing treatment with drug(s) or adjunctive VNS therapy for pharmacoresistant partial seizures. http://ClinicalTrials.gov/show/NCT00215215 2005.
NCT01118455 2004 {published data only}
- NCT01118455. Trial to assess vagus nerve stimulation therapy vs. anti‐epileptic drug treatment in children with refractory seizures. http://ClinicalTrials.gov/show/NCT01118455 2004.
NCT01178437 2009 {published data only}
- NCT01178437. Transcutaneous non‐invasive stimulation of the vagus nerve for the treatment of difficult‐to‐treat epilepsy. http://ClinicalTrials.gov/show/NCT01178437 2009.
Ronkainem 2006 {published data only}
- Ronkainen E, Korpelainen JT, Heikkinen E, Myllyla VV, Huikuri HV, Isojarvi JIT. Cardiac autonomic control in patients with refractory epilepsy before and during vagus nerve stimulation treatment: a one‐year follow‐up study. Epilepsia 2006;47(3):556‐562. [DOI] [PubMed] [Google Scholar]
Rossignol 2009 {published data only}
- Rossignol E, Lortie A, Thomas T, Bouthiller A, Scavarda D, Mercier C, et al. Vagus nerve stimulation in pediatric epileptic syndromes. Seizure 2009;18(1):34‐7. [DOI] [PubMed] [Google Scholar]
Salinsky 1996 {published data only}
- Salinsky MC, Uthman BM, Ristanovic RK, Wernicke JF, Tarver WB, The Vagus Nerve Stimulation Study Group. Vagus nerve stimulation for the treatment of medically intractable seizures: results of a 1‐year open‐extension trial. Archives of Neurology 1996;53(11):1176‐80. [DOI] [PubMed] [Google Scholar]
Scherrrmann 2001 {published data only}
- Scherrmann J, Hoppe C, Kral T, Schramm J, Elger CE. Vagus nerve stimulation: clinical experience in a large patient series. Journal of Clinical Neurophysiology 2001;18(5):408‐14. [DOI] [PubMed] [Google Scholar]
Shimizu 1995 {published data only}
- Shimizu H, Ishijima B, Nakamura K, Asakura T, Ohtsuki T, Yoshimoto T, et al. Effect of vagal stimulation on intractable epilepsy. Psychiatry and Clinical Neurosciences 1995;49(3):S254‐5. [DOI] [PubMed] [Google Scholar]
Sirven 2000 {published data only}
- Sirven JI, Sperling M, Naritoku D, Schachter S, Labar D, Holmes M, et al. Vagus nerve stimulation therapy for epilepsy in older adults. Neurology 2000;54(3):1179‐1182. [DOI] [PubMed] [Google Scholar]
Uthman 1993 {published data only}
- Uthman BM, Wilder BJ, Penry JK, Dean C, Ramsay RE, Reid SA, et al. Treatment of epilepsy by stimulation of the vagus nerve. Neurology 1993;43(7):1338‐45. [DOI] [PubMed] [Google Scholar]
Wang 2004 {published data only}
- Wang LN, Zhao LF, Wang YZ. Basic and clinical study of vagus nerve stimulation in the treatment of epilepsy. Chinese Journal of Clinical Rehabilitation 2004;8(13):2516‐7. [Google Scholar]
Wang 2009 {published data only}
- Wang H, Chen X, Lin Z, Shao Z, Sun B, Shen H, et al. Long‐term effect of vagus nerve stimulation on interictal epileptiform discharges in refractory epilepsy. Journal of the Neurological Sciences 2009;284(1‐2):96‐102. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Boon 2001 {published data only}
- Boon P, Vonck K, D'Havé M, Laere K, Michielsen G, Thiery E, et al. Results of vagus nerve stimulation for refractory epilepsy in Ghent, Belgium. Abstracts of the XVII World Congress of Neurology. 2001.
Gates 2005 {published data only}
- Gates JR, Liow K, Granner M, Louis E, Leroy R, Albers L, et al. Vagus nerve stimulator (VNS) parameter settings: high stimulation vs low stimulation [abstract]. Epilepsia 2005;46(Suppl 8):223, Abstract no: 2.390. [Google Scholar]
Klinkenberg 2014 {published data only}
- Klinkenberg S, Borne CJH, Aalbers MW, Verschuure P, Kessels AG, et al. The effects of vagus nerve stimulation on tryptophan metabolites in children with intractable epilepsy. Epilepsy & behavior 2014;37:133‐8. [DOI] [PubMed] [Google Scholar]
Landy 1993 {published data only}
- Landy HJ, Ramsay RE, Slater J, Casiano RR, Morgan R. Vagus nerve stimulation for complex partial seizures: surgical technique, safety, and efficacy. Journal of Neurosurgery 1993;78(1):26‐31. [DOI] [PubMed] [Google Scholar]
Leach 2001 {published data only}
- Leach JP, Leach VM, Harrison E, Chadwick DW, Eldridge P. Vagal nerve stimulation: a blinded controlled trial of efficacy [abstract]. Epilepsia 2001;42(Suppl 7):206, Abstract no: 2.334. [Google Scholar]
Ney 1998 {published data only}
- Ney G. Vagus nerve stimulation. American Journal of Managed Care 1998;4(9):S495‐500. [Google Scholar]
Scherrmann 2001 {published data only}
- Scherrmann JM, Hoppe C, Kuczaty S, Sassen R, Elger CE. Vagus nerve stimulation (VNS): efficacy of standard stimulation versus rapid cycle: a randomized controlled trial [abstract]. Epilepsia 2001;42(Suppl 7):282, Abstract no: 3.205. [Google Scholar]
References to ongoing studies
DRKS00003689 2012 {published data only}
- DRKS00003689. A randomized, controlled, double‐blind, two‐arm clinical trial to assess safety and efficacy of transcutaneous vagus nerve stimulation (t‐VNS®) in patients with drug‐resistant epilepsy. http://www.drks.de/DRKS00003689 2012.
NCT00782249 2005 {published data only}
- NCT00782249. Trial comparing different stimulation paradigms in patients treated with vagus nerve stimulation for refractory epilepsy. http://ClinicalTrials.gov/show/NCT00782249 2005.
NCT01281293 2011 {published data only}
- NCT01281293. Vagus nerve stimulation clinical outcomes measured prospectively in patients stimulated. http://clinicaltrials.gov/show/NCT01281293 2011.
NCT01378611 2006 {published data only}
- NCT01378611. Does VNS interact with the serotonergic and immune system in children with intractable epilepsy?. http://ClinicalTrials.gov/show/NCT01378611 2006.
NCT01910129 2013 {published data only}
- NCT01910129. Neurostimulation to the vagus nerve for the reduction in frequency of seizures associated with epilepsy. http://ClinicalTrials.gov/show/NCT01910129 2013.
NCT02089243 2014 {published data only}
- NCT02089243. Controlled Randomized Vagus Nerve Stimulation (VNS) Therapy Versus Resection (CoRaVNStiR). http://ClinicalTrials.gov/show/NCT02089243 2014.
Additional references
Cockerell 1995
- Cockerell OC, Johnson AL, Sander JW, Hart YM, Shorvon SD. Remission of epilepsy: results from the National General Practice Study of Epilepsy. Lancet 1995;346(8979):140‐4. [DOI] [PubMed] [Google Scholar]
Forsgren 2005
- Forsgren L, Beghi E, Oun A, Sillanpaa M. The epidemiology of epilepsy in Europe ‐ a systematic review. European Journal of Neurology 2005;12(4):245‐53. [DOI] [PubMed] [Google Scholar]
Hallbook 2005
- Hallbook T, Lundgren J, Stjernqvist K, Blennow G, Strömblad L‐G, Rosén I. Vagus nerve stimulation in 15 children with therapy resistant epilepsy; its impact on cognition, quality of life, behaviour and mood. Seizure 2005;14(7):504‐513. [DOI] [PubMed] [Google Scholar]
Hauser 1975
- Hauser WA, Kurland LT. The epidemiology of epilepsy in Rochester, Minnesota, 1935 through 1967. Epilepsia 1975;16(1):1‐66. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org. [Google Scholar]
Kirkham 2010
- Kirkham JJ, Dwan KM, Altman DG, Gamble C, Dodd S, Smyth R, et al. The impact of outcome reporting bias in randomised controlled trials on a cohort of systematic reviews. BMJ 2010;340:c365. [DOI: ] [DOI] [PubMed] [Google Scholar]
Krahl 2012
- Krahl SE, Clark KB. Vagus Nerve Stimulation for epilepsy: a review of central mechanisms. Surgical neurology international 2012;3(Suppl 4):S255‐S259. [DOI: 10.4103/2152-7806.103015; PUBMED: 23230530] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kwan 2000
- Kwan P, Brodie MJ. Early identification of refractory epilepsy. New England Journal of Medicine 2000;342(5):314‐9. [DOI] [PubMed] [Google Scholar]
Morris 2013
- Morris GL 3rd, Gloss D, Buchhalter J, Mack KJ, Nickels K, Harden C. Evidence‐based guideline update: vagus nerve stimulation for the treatment of epilepsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2013;81(16):1453‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sackeim 2001
- Sackeim HA, Rush AJ, George MS, Marangell LB, Husain MM, Nahas Z, et al. Vagus Nerve Stimulation (VNS) for treatment‐resistant depression: efficacy, side effects and predictors of outcome. Neuropsychopharmacology 2001;25(5):713–28. [DOI] [PubMed] [Google Scholar]
Schachter 1998
- Schachter SC, Saper CB. Vagus nerve stimulation. Epilepsia 1998;39(7):677‐86. [DOI] [PubMed] [Google Scholar]
Selway 1987
- Selway R, Nashef L. Vagus Nerve Stimulation. From Membranes to Mankind‐ A Practical Guide to Epilepsy. Vol. 48, Epilepsy Society, 1987. [Google Scholar]
Vonck 2014
- Vonck K, Raedt R, Naulaerts J, Vogelaere F, Thiery E, Roost D, et al. Vagus nerve stimulation… 25 years later! What do we know about the effects on cognition?. Neuroscience & Biobehavioural Reviews 2014;45:63‐71. [DOI: 10.1016/j.neubiorev.2014.05.005; PUBMED: 24858008 ] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Privitera 2010
- Privitera MD, Welty TTE, Ficker DDM, Welge J. Vagus nerve stimulation for partial seizures. Cochrane Database of Systematic Reviews 2010, Issue 7. [DOI: 10.1002/14651858.CD002896] [DOI] [PubMed] [Google Scholar]