

ABSTRACT |
Background:
The stressful work environment, long working hours and sedentary activities inherent to jobs in banks reflect on the employees’ lifestyle with consequent effects on their health.
Objective:
To describe the lifestyle and nutritional status of employees of a chain of banks in Pelotas, Brazil.
Method:
Cross-sectional descriptive study conducted with employees aged 18 or older of a chain of banks in Pelotas. We collected information on the demographic, economic, nutritional and lifestyle profile by means of questionnaire Individual Lifestyle Profile (ILP) and anthropometric measurements. Statistical analysis was performed with software STATA® 12.0.
Results:
The sample comprised 82 employees, most of whom were male (67.1%). We detected poor dietary habits (high fat-rich food and sweets and low fruit/vegetable intake) and sedentary behavior. The results for domains preventive behavior, social relationships and stress control pointed to a healthy lifestyle: the participants were usually aware of their blood pressure and cholesterol levels, succeeded in keeping calm and reported to actively seek friendships. Overweight and elevated waist circumference prevailed. Fat-rich food and sweets intake, knowledge and control of blood pressure and cholesterol and waist circumference significantly differed as a function of sex.
Conclusion:
The results evidenced poor dietary habits and physical activity, in addition to overweight, which point to the need for actions to improve the lifestyle and nutritional status of the analyzed population of workers.
Keywords: lifestyle, nutritional status, occupational health
RESUMO |
Introdução:
O ambiente estressante, as longas jornadas de trabalho e a característica sedentária das atividades realizadas no setor bancário refletem no estilo de vida dos trabalhadores, com repercussões importantes na saúde.
Objetivo:
Descrever o estilo de vida e o estado nutricional de funcionários de uma rede bancária de Pelotas.
Método:
Estudo transversal descritivo, com trabalhadores com idade igual ou superior a 18 anos de uma rede bancária de Pelotas. Foram coletadas informações referentes ao perfil demográfico, econômico, nutricional e de estilo de vida por meio do questionário Perfil do Estilo de Vida Individual (PEVI) e medidas antropométricas. As análises estatísticas foram realizadas no programa STATAâ versão 12.0.
Resultados:
A amostra foi composta de 82 trabalhadores, a maioria homens (67,1%). Quanto ao estilo de vida, constataram-se hábitos alimentares inadequados (com alto consumo de alimentos gordurosos/doces e baixo consumo de frutas/verduras) e comportamento sedentário. Por outro lado, notou-se que os componentes comportamento preventivo, relacionamento social e controle do stress apresentaram estilo de vida saudável, demonstrando que os bancários costumam conhecer a pressão arterial e os níveis de colesterol, manter-se calmos e cultivar amizades. Observou-se prevalência de sobrepeso e circunferência da cintura elevada. Entre os sexos, houve diferença significativa em ingestão de alimentos gordurosos e doces, conhecimento e controle da pressão arterial e dos níveis de colesterol e circunferência da cintura.
Conclusão:
Os resultados apresentaram um estilo de vida inadequado nos componentes nutrição e atividade física, além de sobrepeso entre os funcionários, evidenciando a necessidade de ações para melhorar o estilo de vida e o estado nutricional desses indivíduos.
INTRODUCTION
Noncommunicable diseases (NCD) are considered one of the main public health problems and as the leading cause of death according to the World Health Organization (OMS)1. This situation is particularly worrisome in developing countries, such as Brazil, as they have not yet succeeded in eradicating infectious diseases and the rate of NCD is growing quite fast2. The main causes of NCD are physical inactivity, poor diet, smoking and alcohol consumption, in addition to other factors such as obesity, arterial hypertension and high serum cholesterol1.
All the aforementioned conditions might be the result of the fast-pace and stressful lifestyle that became common in the globalized world3. Long working hours and pressure to improve productivity might interfere with the lifestyle of workers as a result of occupational stress, with negative impact on their quality of life4.
Some jobs involve greater exposure to occupational stress, with consequent loss of productivity and impaired quality of life, as e.g. those of employees of financial institutions4,5. The characteristics inherent to the job lead this population of workers to develop a sedentary behavior. They spend most of the working time sitting and are exposed to a stressful environment as a function of the goals to be met and the responsibility related to handling large amounts of money6,7. The sedentary nature of work at financial institutions is associated with several problems, such work-related musculoskeletal disorders8,9. In a study that investigated the association of quality of life with sociodemographic and occupational factors, lifestyle and musculoskeletal symptoms among bank employees in Jequie, Bahia, Brazil, Nunes and Mascarenhas5 found that many participants often complained of bodily pain during the working hours, eventually requiring sick leave. Then, it is worth noticing that many individuals have trouble to fall into a refreshing sleep, with direct impact on their energy and performance.
Diet is one further aspect that deserves consideration, as the literature shows that bank employees have poor dietary habits characterized by high consumption of refined carbohydrates and fat and low intake of fruit and vegetables10,11 — actually, a profile common to the overall Brazilian population12. As a rule, the daily food intake is distributed between just two meals, lunch and dinner, one of them characterized by poor nutritional quality for mostly consisting of snacks or fast food from cafeterias and/or restaurants11.
The combination of the just mentioned dietary habits and sedentary behavior results in high frequency of overweight/obesity among bank employees, and excess abdominal fat in particular, which is considered a significant risk factor for countless diseases and is significantly associated with higher frequency of cardiovascular events13.
As a function of the aforementioned considerations, the aim of the present study was to describe the lifestyle and nutritional status of employees of a chain of banks in Pelotas, Rio Grande do Sul, Brazil.
METHOD
The present cross-sectional descriptive study was conducted with employees of a chain of banks in Pelotas. The sample comprised employees aged 18 years old or older from both sexes who agreed to participate in the study by signing an informed consent form. There were 98 active employees at the six bank branches on the day of data collection. The participants were recruited by means of convenience sampling: all employees present were invited to participate to a total of 82. The study was performed from September through November 2017.
Pregnant women, employees under 18 years old, those on leave at the time of data collection or with clinical conditions likely to interfere with the measurement of body weight and height — such as swelling, ascites, amputations or orthopedic problems — were excluded.
The participants were interviewed by a duly trained investigator during breaks based on a semi-structured questionnaire with open- and closed-ended questions.
The following variables were selected to characterize the sample demographic profile: age (years), sex (male or female), self-reported ethnicity (categorized as white or non-white), marital status (single, married, divorced, widowed), educational level (complete secondary school, incomplete or complete higher education), working time (hours), length in the job (years) and current position. The socioeconomic profile of the sample was investigated with the questionnaire developed by the Brazilian Market Research Association (Associação Brasileira de Empresas de Pesquisa–ABEP) which defines five purchasing power categories, the highest being A and the lowest E, according to the availability of consumer goods and employees in the household, educational level of the family head and use of public services14.
Lifestyle was investigated by means of the questionnaire Individual Lifestyle Profile (ILP) validated by Nahas et al.15. ILP comprises 15 questions distributed across five domains — diet, physical activity, preventive behavior, social relationships and stress control. Each item is responded on a Likert scale ranging from 0 to 3. Scores 0 (“It is absolutely not a part of your lifestyle”) and 1 (“Sometimes is a part of your lifestyle”) represent a negative lifestyle profile. Scores 2 (“Almost always true relative to your behavior”) and 3 (“Always true relative to your behavior”) represent a positive lifestyle profile.
For investigation of the nutritional status, body weight was measured with the participants barefooted, using a TANITA® Ironman BC558 electronic scale with 150 kg of maximum capacity and 100-gram precision. Height was measured with the participants standing and the head aligned to the Frankfurt plane, using non-extensible CARDIOMED tape measure with 150 cm of length and reverse scale, attached to a wall 50 cm from the ground level, resulting in a maximum height of 200 cm and medium point in 100 cm16. The participants’ nutritional status was categorized based on the body mass index (BMI) defined as the ratio of body weight (kg) to height squared (m2); following WHO17 underweight was considered as BMI <18.5 kg/m2, normal weight BMI 18.5 to 24.5 kg/m2, overweight BMI 25.0 to 29.9 kg/m2 and obesity BMI≥30 kg/m2.
Abdominal fat was assessed based on the waist circumference (WC) measured directly on the skin on the narrowest part of the body between the chest and the hips with non-extensible CARDIOMED tape measure with 150 cm of length. When the smallest circumference could not be visualized, measurements were made on the midpoint between the last rib and the iliac crest16. WC was measured during expiration, without pressing the tape measure against the skin. The results were categorized according to the cutoff points established by WHO to define increased and substantially increased risk of metabolic complications, to wit, 94 cm and 102 cm for men and 80 cm and 88 cm for women, respectively17.
Statistical analysis was performed with software STATA® version 12.0. Descriptive analysis is presented as means and standard deviation. Means were compared with the Student’s t-test for paired samples and associations were investigated with the χ2 or Fisher’s exact test. The significance level was set to 5% in all the analyses.
The present study was approved by the research ethics committee of School of Medicine, Universidade Federal de Pelotas (CEP/FAMED/UFPEL) ruling no. 2,258,928. The participants were delivered an informed consent form at the onset of the study.
RESULTS
We analyzed 82 employees allocated to the bank six branches in Pelotas. The average age of the sample was 44.0±9.0 years old. As Table 1 shows, 67.1% of the participants were male, 91.5% white, 59.8% married, 86.6% had completed higher education and 60.9% corresponded to social class B.
Table 1. Sample description according to sociodemographic and occupational aspects. Pelotas (RS), 2017 (n=82).
| Variables | n | % |
|---|---|---|
| Sex | ||
| Female | 27 | 32.9 |
| Male | 55 | 67.1 |
| Ethnicity | ||
| White | 75 | 91.5 |
| Non-white | 7 | 8.5 |
| Marital status | ||
| Single | 19 | 23.2 |
| Married | 49 | 59.8 |
| Divorced | 12 | 14.6 |
| Widowed | 2 | 2.4 |
| Educational level | ||
| Complete secondary school | 2 | 2.5 |
| Incomplete higher education | 9 | 10.9 |
| Complete higher education | 71 | 86.6 |
| Working hours | ||
| 6 | 38 | 46.3 |
| 8 | 44 | 53.7 |
| Length in the job (years) | ||
| Up to 5 | 7 | 8.6 |
| 5–10 | 12 | 14.6 |
| >10 | 63 | 76.8 |
| Current position | ||
| Clerk | 18 | 21.9 |
| Business assistant | 12 | 14.7 |
| Teller | 14 | 17.1 |
| Module manager | 3 | 3.7 |
| Customer relationship manager | 27 | 32.9 |
| Account manager | 2 | 2.4 |
| General manager | 6 | 7.3 |
| Socioeconomic level | ||
| A | 27 | 32.9 |
| B | 50 | 60.9 |
| C | 5 | 6.2 |
In regard to their occupational profile (Table 1) a little more than half of the participants (53.7%) worked 8 hours/day and the largest proportion as customer relationship managers (32.9%). About 76.8% of the employees had worked more than 10 years at the institution.
Table 2 describes the results relative to the participants’ lifestyle. We found a high prevalence of negative dietary habits, especially regarding the daily intake of fruit and vegetables, which were seldom or never consumed by 70% of the sample, while only eight participants (9.8%) reported to avoid fat-rich food and sweets. About 52.5% of the participants scored low on the item relative to the number of daily meals (four or five), i.e. eating several meals a day was not a part of the participants’ lifestyle.
Table 2. Participants’ lifestyle profile. Pelotas (RS), 2017 (n=82).
| Domain — n (%) | Never (negative) | Seldom (negative) | Almost always (positive) | Always (positive) |
|---|---|---|---|---|
| Nutrition | ||||
| Fruit and vegetables | 24 (29.3) | 35 (42.7) | 14 (17.1) | 9 (10.9) |
| Avoids fat-rich food and sweets | 10 (12.2) | 42 (51.2) | 22 (26.8) | 8 (9.8) |
| 4 to 5 full meals | 21 (25.7) | 22 (26.8) | 22 (26.8) | 17 (20.7) |
| Physical activity | ||||
| 30 minutes of moderate-to-intense activity | 43 (52.4) | 21 (25.6) | 12 (14.6) | 6 (7.4) |
| Stretching and strength training twice per week | 29 (35.4) | 19 (23.2) | 13 (15.8) | 21 (25.6) |
| Walking or cycling as mode of transport | 31 (37.8) | 18 (21.9) | 14 (17.1) | 19 (23.2) |
| Preventive behavior | ||||
| Blood pressure and cholesterol | 3 (3.7) | 22 (26.8) | 17 (20.7) | 40 (48.8) |
| Non-smoking and moderate alcohol consumption | 18 (21.9) | - | 7 (8.6) | 57 (69.5) |
| Complies with traffic rules | 2 (2.5) | 1 (1.2) | 11 (13.4) | 68 (82.9) |
| Social relationships | ||||
| Seeks friendships | - | 5 (6.1) | 21 (25.6) | 56 (68.3) |
| Group activities, with friends | 4 (4.9) | 24 (29.3) | 27 (32.9) | 27 (32.9) |
| Active in the community | 12 (14.6) | 31 (37.8) | 23 (28.1) | 16 (19.5) |
| Stress control | ||||
| Spares time to relax | 10 (12.2) | 18 (21.9) | 20 (24.4) | 34 (41.5) |
| Keeps calm during discussions | 3 (3.7) | 18 (21.9) | 38 (46.3) | 23 (28.1) |
| Work and leisure time | 3 (3.7) | 24 (29.2) | 32 (39.0) | 23 (28.1) |
Forty-three participants (52.4%) reported to never perform at least 30 minutes of moderate-to-vigorous intensity physical activity either continuous or accumulated five or more days per week. About 58.6% of the sample reported not to perform stretching or strength training at least twice per week. Thirty-three participants (40.3%) reported to walk or cycle as mode of transport and to prefer stairs to elevators as routine.
The results relative to domain preventive behavior were overall favorable. A large part of the participants (69.5%) reported to always or almost always be aware of and control their serum cholesterol and blood pressure. The prevalence of favorable answers for avoidance of smoking and moderate alcohol consumption and compliance with traffic rules was 78.1% and 96.3%, respectively.
All the responses corresponding to domain social relationship were favorable. About 96.3% of the participants reported to always or almost always seek to make friends, 65.8% to participate in group activities and 47.6% to be active in the community.
Finally, also the results for domain stress control were favorable. Almost 75% of the participants reported to succeed in keeping themselves calm during discussions. However, only 12.2% of the sample reported to spare at least 5 minutes to relax every day. About 32.9% of the participants seldom or never succeed in keeping balance between work and leisure time.
On comparison per sex (Table 3) significant difference was found for intake of fat-rich food and sweets, which prevalence was significantly higher for the men (p=0.016). Within domain preventive behavior, 32 men and 25 women gave favorable responses to the item on awareness and control of blood pressure and cholesterol; this difference was significant (p=0.002).
Table 3. Lifestyle profile according to sex. Pelotas (RS), 2017 (n=82).
| Domain n (%) | Sex | p | |||
|---|---|---|---|---|---|
| Male | Female | ||||
| Negative | Positive | Negative | Positive | ||
| Nutrition | |||||
| Fruit and vegetables | 41 (69.5) | 14 (60.9) | 18 (30.5) | 9 (39.1) | 0.602 |
| Avoids fat-rich food and sweets | 40 (76.9) | 15 (50.0) | 12 (23.1) | 15 (50.0) | 0.016 |
| 4 to 5 full meals | 29 (67.4) | 26 (66.7) | 14 (32.6) | 13 (33.3) | 1.00 |
| Physical activity | |||||
| 30 minutes of moderate-to-intense activity | 41 (64.1) | 14 (77.8) | 23 (35.9) | 4 (22.2) | 0.396 |
| Stretching and strength training twice per week | 36 (75.0) | 19 (55.9) | 12 (25.0) | 15 44.1) | 0.095 |
| Walking or cycling as mode of transport | 31 (63.3) | 24 (72.7) | 18 (36.7) | 9 (27.3) | 0.474 |
| Preventive behavior | |||||
| Blood pressure and cholesterol | 23 (92.0) | 32 (56.1) | 2 (8.0) | 25 (43.9) | 0.002 |
| Non-smoking and moderate alcohol consumption | 15 (83.3) | 40 (62.5) | 3 (16.7) | 24 (37.5) | 0.155 |
| Complies with traffic rules | 2 (66.7) | 53 (67.1) | 1 (33.3) | 26 (32.9) | 1.000 |
| Social relationships | |||||
| Seeks friendships | 5 (100) | 50 (64.9) | 0 (0.0) | 27 (35.1) | 0.166 |
| Group activities, with friends | 18 (64.3) | 37 (68.5) | 10 (35.7) | 17 (31.5) | 0.805 |
| Active in the community | 27 (62.6) | 28 (71.8) | 16 (37.2) | 11 (28.2) | 0.482 |
| Stress control | |||||
| Spares time to relax | 17 (60.7) | 38 (70.4) | 11 (39.3) | 16 (29.6) | 0.459 |
| Keeps calm during discussions | 12 (57.1) | 43 (70.5) | 9 (42.9) | 18 (29.5) | 0.290 |
| Work and leisure time | 18 (66.7) | 37 (67.3) | 9 (33.3) | 18 (32.7) | 1.00 |
The results of the assessment of nutritional status based on BMI (Figure 1) showed that 78.8% of the men and 21.2% of the women fell within the range for overweight (p=0.96), 27.4±5.4 kg/m2 on average. Risk of metabolic complications based on WC was increased, 95.9±12.5 cm for the men and 87.5±14.9 cm for the women, p=0.01. The column on the left on Figure 1 corresponds to the men and the column on the right to the women (p=0.177).
Figure 1.
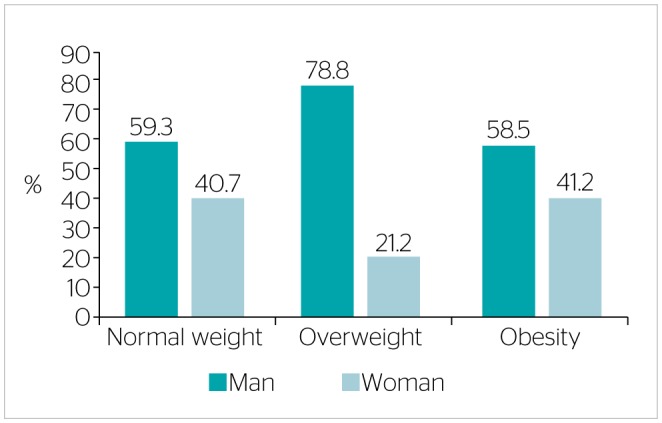
Percent distribution of the analyzed bank employees per nutritional status category and sex. Pelotas (RS), 2017 (n=82).
DISCUSSION
A good state of health demands an adequate lifestyle. Poor habits are associated with high probability of risk for some NCD18. Bank employees represent one of the categories of workers with poor lifestyles as a function of the stressful nature of their work routine, which results in considerable physical exhaustion and leads them to avoid physical activity and adopt a high-calorie diet as compensation. All these aspects contribute to make them gain weight, with consequent impairment of their quality of life13.
The sociodemographic and occupational characteristics of the analyzed sample are similar to those described in the study by Hirani et al.13 with bank employees in India; most were male and white and their average age was 40 years old. Most participants had completed graduate education, worked 8 hours/day and had worked more than 10 years for the current employer. Also Nunes and Mascarenhas5 found a similar profile, however, the average age of the sample was 38 years old and most participants were brown skinned. Most of the participants in the present study were male, had completed higher education, a stable partner and worked 8 hours/day.
As concerns lifestyle, the results of the present study evidence a high prevalence of poor dietary habits, mainly in regard to the daily fruit and vegetable and fat-rich food intake. Our findings are similar to those reported by Skapino and Alvarez Vaz11, which showed that the number of fruit and vegetable servings were below the recommended ones, i.e. less than three per day. In turn, the prevalence of trans-fat–rich processed food and sugar-sweetened beverages intake was 37.5 and 27.9%, respectively. Although this is an unhealthy dietary pattern, it is the one common to the overall Brazilian population12. As is known, the dietary habits might influence the development of NCD1, however, more studies with bank employees on this subject are necessary.
In their study, Eze et al.10 found that bank employees do not engage in healthy dietary habits for prioritizing practical solutions. These workers usually do not eat breakfast or lunch at home, do not bring food to work and above all do not tend to eat three full daily meals. Most of them often eat at restaurants, fast food or food bought from street vendors, probably as a function of the short lunch breaks, of only 15 minutes for employees who work 6 hours/day and one hour for those who work 8 hours/day. Their diet mainly comprises high-calorie, sodium-, fat- and sugar-rich food with poor nutritional value. We obtained similar results in the present study: 52.5% of the participants reported a poor feeding schedule, with less than four meals a day, and only 36.6% of the participants avoided fat-rich food and sweets.
Most participants reported not to exercise and to seldom walk, cycle or climb stairs, but prefer the conveniences afforded by urban life. These findings agree with reports in the literature8,13,19 which associate them with risk for comorbidities such as hypertension, obesity and diabetes, in addition to musculoskeletal symptoms7,19,20.
In regard to domains preventive behavior (which comprises attention to and control of the blood pressure and serum cholesterol, smoking and drinking and compliance with traffic rules), social relationships (friendships, group activities and participation in the community) and stress control (sparing time to relax, ability to balance work and leisure and being able to keep calm during discussions) the prevalence of favorable behaviors was high. According to VIGITEL12 (Chronic Disease Telephone-based Surveillance) the overall Brazilian population considerable changed their preventive behavior: a large part of adults usually undergoes some periodic examination, the rate of smokers is considerable decreasing, alcohol abuse (four or more units of alcohol at one time) occurs only among 19% and only 7.3% drive after drinking.
In their study, Coelho et al.20 concluded that the stronger the social support, the lower the susceptibility to emotional exhaustion and depersonalization, factors which are associated with higher stress. In turn, social support seems to have relationship with professional accomplishment.
In the study by Nunes and Mascarenhas5, the highest prevalence corresponded to category very good lifestyle. These authors also found favorable results for the social relationships and psychological quality of life domains. Salaudeen et al.21 found that almost half of the bank employees analyzed in their study were smokers and consumed alcohol daily, which findings disagree from ours.
Several authors observed that stress is a common occurrence among bank employees6,18,20,22. In Nascimento et al.’s study22 more than half of the participants exhibited high levels of stress. After analyzing semi-structured interviews conducted with bank employees in Espirito Santo, Brazil, Da Silva6 identified some factors which contributed to occupational stress, including shortage of personnel to serve customers, unmotivated coworkers, excessively high goals, pressures and high customer turnover.
This situation might give rise to moral conflict and emotional imbalance and eventually also interfere with life outside work. Emotional exhaustion and stress might make workers lose their interest in previously pleasurable activities and motivation, lead to sick leaves and cause depression, anxiety and eventually also suicide23.
For this reason, adequate stress control has paramount importance in regard to the workers’ performance. In their study, Da Silva et al.6 found that managers sought to control trigger situations by holding meetings intended to reduce possible complications and thus succeeded to attenuate the discomfort caused by stress. The participants in the present study reported to try and keep calm, spare time to relax and balance work and leisure.
Most participants were categorized as with overweight/obesity and with WC above the desired levels, which corresponds to the current profile of the Brazilian population18. Similar findings were reported by Addo et al.7 in their study to investigate factors associated with overweight and obesity among employees of a financial institution in Ghana, West Africa, in which the prevalence of excess weight was over 50%. Upon analyzing the prevalence of behavioral and risk factors among employees of a financial institution in Uruguay, also Skapino and Alvarez Vaz11 found high prevalence of overweight and obesity.
Excess abdominal fat is associated with major metabolic changes, which make it a risk factor for cardiovascular diseases, diabetes mellitus and hypertension24. Excess abdominal fat is also associated with poorer quality of life and self-esteem which favor the occurrence of psychopathological problems, such as compulsive overeating and bulimia25.
The aim of the study conducted by Aravindalochanan et al.19 was to establish whether sitting over a long period of time at work and family history of diabetes predispose workers with sedentary jobs to develop this disease. The BMI and WC values they found are similar to ours. The authors concluded that sedentary work and family history of diabetes were a risk factor for disease, and that among males also elevated WC was associated with diabetes. Hirani et al.13 found that most of the participants in their study exhibited excess weight and elevated WC, as in our study. Upon investigating the association of these parameters with sociodemographic variables, they found that the prevalence of abdominal obesity was higher among managers and employees corresponding to the upper socioeconomic class, which variable is further correlated with older age.
As a rule, the literature indicates that while bank employees have satisfactory knowledge about healthy eating and possible risk factors for obesity, diabetes mellitus and arterial hypertension, they do not seek to change their lifestyle to improve and preserve their health10,21. Since having knowledge about healthy eating alone does not suffice to improve their behavior, means should be afforded to this population of workers to put their knowledge into practice. For this purpose, employers could ensure longer meal breaks and provide nutritionally adequate meals.
In the present study we did not seek to assess the participants’ level of knowledge nor to establish correlations or causal relationships. Being a cross-sectional descriptive study, we merely described the selected characteristics. Our results corroborate those of other studies and allow us conclude that some aspects of the lifestyle of the analyzed population of bank employees were inadequate and should be changed.
CONCLUSION
The results of the present study point to inadequacies in the lifestyle of the analyzed population, particularly as concerns diet and physical activity, as the participants reported poor dietary habits and sedentary behavior.
The prevalence of excess weight and elevated WC was high, with consequent higher risk of metabolic complications for both the male and female participants. These results indicate that this population should make immediate changes in their behavior.
Actions to raise the awareness on healthy eating and lifestyles, together with strategies to apply knowledge into practice and provision of adequate food in the workplace are likely to improve the nutritional status, and consequently also the quality of life and performance of this population of workers.
Finally, we believe that future studies are necessary, mainly focusing on interventions, to establish which methods are more efficacious to improve the lifestyle, and consequently also the nutritional status of bank employees.
Footnotes
Funding: none
REFERENCES
- 1.Mendis S, World Health Organization Global status report on noncommunicable diseases 2014. Geneva: World Health Organization; 2014. [DOI] [PubMed] [Google Scholar]
- 2.Malta DC, Moura LD, Prado RRD, Escalante JC, Schmidt MI, Duncan BB. Mortalidade por doenças crônicas não transmissíveis no Brasil e suas regiões, 2000 a 2011. Epidemiol Serv Saúde. 2014;23(4):599-608. 10.5123/S1679-49742014000400002 [DOI] [Google Scholar]
- 3.McMichael AJ. Globalization, climate change, and human health. N Engl J Med. 2013;368(14):1335-43. 10.1056/NEJMra1109341 [DOI] [PubMed] [Google Scholar]
- 4.Ziemska B, Klimberg A, Marcinkowski JT. Psychosocial factors and health status of employees at the Poznan University of Medical Sciences. Ann Agric Environ Med. 2013;20(3):539-43. [PubMed] [Google Scholar]
- 5.Nunes EA, Mascarenhas CHM. Qualidade de vida e fatores associados em trabalhadores do setor bancário. Rev Bras Med Trab. 2016;14(3):227-36. 10.5327/Z1679-443520162216 [DOI] [Google Scholar]
- 6.Da Silva FC, Braga PS, Alves LO. A Síndrome de Burnout e a qualidade de vida no setor bancário. : Proceedings of the 9. Simpósio de Excelência em Gestão e Tecnologia; 2012. [Google Scholar]
- 7.Addo PN, Nyarko KM, Sackey SO, Akweongo P, Sarfo B. Prevalence of obesity and overweight and associated factors among financial institution workers in Accra Metropolis, Ghana: a cross sectional study. BMC Res Notes. 2015;8:599 10.1186/s13104-015-1590-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sulaiman SK, Kamalanathan P, Ibrahim AA, Nuhu JM. Musculoskeletal disorders and associated disabilities among bank workers. Int J Res Med Sci. 2015;3(5):1153-8. 10.5455/2320-6012.ijrms20150523 [DOI] [Google Scholar]
- 9.Maier RC, Santos Jr. G. Análise da qualidade de vida: um estudo com colaboradores bancários da cidade de Ponta Grossa-PR. : Proceedings of the 7. Congresso Internacional de Administração; 2010. [Google Scholar]
- 10.Eze NM, Maduabum FO, Onyeke NG, Anyaegunam NJ, Ayogu CA, Ezeanwu BA, et al. Awareness of food nutritive value and eating practices among Nigerian bank workers: Implications for nutritional counseling and education. Medicine. 2017;96(10):e6283 10.1097/MD.0000000000006283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Skapino E, Alvarez Vaz R. Prevalencia de factores de riesgo de enfermedades crónicas no transmisibles en funcionarios de una institución bancaria del Uruguay. Rev Urug Cardiol. 2016;31(2):246-55. [Google Scholar]
- 12.Bernal RTI, Malta DC, Iser BPM, Monteiro RA. Método de projeção de indicadores das metas do Plano de Ações Estratégicas para o Enfrentamento das Doenças Crônicas não Transmissíveis no Brasil segundo capitais dos estados e Distrito Federal. Epidemiol Serv Saúde [Internet]. 2016. [cited on Dec. 13, 2017];25(3):455-66. Available at: 10.5123/s1679-49742016000300002 [DOI] [PubMed] [Google Scholar]
- 13.Hirani S, Kuril BM, Lone DK, Ankushe RT, Doibale MK. Obesity prevalence and its relation with some sociodemographic factors in bank employee of Aurangabad city, Maharashtra, India. Int J Community Med Public Health. 2016;3(6):1628-35. 10.18203/2394-6040.ijcmph20161641 [DOI] [Google Scholar]
- 14.Associação Brasileira de Empresas de Pesquisas Critério de classificação econômica Brasil 2015 e atualização das distribuições de classes para 2016 [Internet]. Brasil: ABEP; 2016. [cited on Jul. 1, 2017]. Available at: www.abep.org [Google Scholar]
- 15.Nahas MV, de Barros MV, Francalacci V. O pentáculo do bem-estar-base conceitual para avaliação do estilo de vida de indivíduos ou grupos. Rev Bras Ativ Fís Saúde. 2000;5(2):48-59. 10.12820/rbafs.v.5n2p48-59 [DOI] [Google Scholar]
- 16.Brasil. Ministério da Saúde. Orientações para coleta e análise de dados antropométricos em serviços de saúde: norma técnica do sistema de Vigilância Alimentar e Nutricional - SISVAN. Brasília: Ministério da Saúde; 2011. [Google Scholar]
- 17.World Health Organization Consultation on Obesity, World Health Organization Division of Noncommunicable Diseases, World Health Organization. Programme of Nutrition, Family and Reproductive Health. Obesity: preventing and managing the global epidemic: report of a WHO Consultation on Obesity, Geneva, 3-5 June 1997 [Internet]. Geneva: World Health Organization; 1998. [cited on Jul. 1, 2017]. p. 9-10. Available at: http://apps.who.int/iris/handle/10665/63854 [PubMed] [Google Scholar]
- 18.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção de Saúde. Vigitel Brasil 2016: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: estimativas sobre frequência e distribuição sociodemográficas de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados brasileiros e no Distrito Federal em 2016. Brasília: Ministério da Saúde; 2017. [Google Scholar]
- 19.Aravindalochanan V, Kumpatla S, Rengarajan M, Rajan R, Viswanathan V. Risk of diabetes in subjects with sedentary profession and the synergistic effect of positive family history of diabetes. Diabetes Technol Ther. 2014;16(1):26-32. 10.1089/dia.2013.0140 [DOI] [PubMed] [Google Scholar]
- 20.Coelho JAPDM, Souza GHSD, Cerqueira CLCD, Esteves GGL, Barros BNR. Estresse como preditor da Síndrome de Burnout em bancários. Rev Psicol Organ Trab. 2018;18(1):306-15. 10.17652/rpot/2018.1.13162 [DOI] [Google Scholar]
- 21.Salaudeen AG, Musa OI, Babatunde OA, Atoyebi OA, Durowade KA, Omokanye LO. Knowledge and prevalence of risk factors for arterial hypertension and blood pressure pattern among bankers and traffic wardens in Ilorin, Nigeria. Afr Health Sci. 2014;14(3):593-9. 10.4314/ahs.v14i3.14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nascimento ISS, da Costa Nascimento LT, Lyra FA. Fatores estressores e qualidade de vida: uma análise sobre o trabalho dos caixas bancários. Rev Formadores. 2017;10(1):6-19. [Google Scholar]
- 23.Bruno WP. Bancários não são máquinas. Saúde dos Bancários. São Paulo: Publisher Brasil; 2011. p. 21-32. [Google Scholar]
- 24.World Health Organization Waist circumference and waist-hip ratio: report of a WHO expert consultation. Geneva: World Health Organization; 2011. p. 12-18. [Google Scholar]
- 25.Djalalinia S, Qorbani M, Peykari N, Kelishadi R. Health impacts of obesity. Pak J Med Sci. 2015;31(1):239-42. 10.12669/pjms.311.7033 [DOI] [PMC free article] [PubMed] [Google Scholar]