

ABSTRACT
Body composition analysis may provide valuable information about the assessment of balance between fluid, fat, and fat-free mass. The present study assessed whether the regular increase in water consumption has any significant effects on measurements of body composition using BIA. A total of 140 subjects participated in this study. Body composition analyses of the subjects were performed for five times using foot to foot BIA; first at baseline and four times, after 15 minutes of each 500 mL water intakes. There was overestimation in body fat mass compared to the baseline and increased significantly after water intakes in males (2.08% in 500 mL, 3.80% in 1000 mL, 5.88% in 1500 mL, and 7.92% in 2000 mL, p < 0.05) and in females (3.4% in 500 mL, 5.7% in 1000 mL, 7.8% in 1500 mL, and 9.4% in 2000 mL, p < 0.05). In contrast, there was markedly underestimation of total body water and fat-free mass in males (35% and 50%) and females (17% and 22%), respectively, at the end of the study. Thus, overestimation of body fat mass and lower estimation of total body water and fat-free mass with closely to the amount of water retention using BIA application should be considered in health-related clinical practice.
KEYWORDS: Bioelectrical impedance analysis, fat mass, fat free mass, total body water, body composition
1. Introduction
Nutrition status that is the sum of balance between intake, absorption and utilization, can be reflect individual’s fitness status and existence risk of cardiovascular and metabolic impairment. Importantly, any impairment of nutritional conditions may have a remarkable effect on the content of body composition and trigger many serious clinical conditions [1,2]. The assessment of body composition has long been used to obtain important information with regard to health status of the individual [3,4]. Thus, the effective measurement of body composition becomes extremely important in clinical medicine.
Measurements of anthropometric parameters including weight, height, or dimensions of the body are mainly used to reflect the amount of body fat and its distribution in population. Body mass index (BMI), which is calculated by dividing body weight (in kilogram) by the height (in meters) squared, has generally been used to identical individual’s body weight status, especially fat content and above 30 kg/m2 has been accepted as risk of obesity. However, BMI does not provide information with regarding relative proportions fat and lean mass of the individual [5]. Measurement of waist and waist to hip ratio also used as a potential indicator of health risk reflecting abdominal obesity which is important for cardiovascular and diabetic patients [6].
Approximately in the last five years, it has been suggested that body composition could be assessed by measuring resistance to electrical activity from different parts of the body [7]. This method has been termed as bioelectrical impedance analysis (BIA) and widely used for evaluation of body compartments in many clinical and non-clinical situations [8–10]. BIA is considered to be easily, noninvasively, quickly applied non-invasive method and provide reliable outcome in research and clinical trials. BIA method could be separately measure total body water (TBW), fat-free mass (FFM), fat mass (FM), percent fat mass (% FM) other body compartments [11]. Validation of BIA on effective measurement of body compositions has been shown in result of some studies [3,12] and questioned in some studies [13,14]. An invalid estimation of body composition as a result of altered hydration status using BIA measurement has been suggested [15]. However, in some clinical studies, water retention by those with eating disorders and variation of hydration status with diseases and environmental conditions may significantly affect body composition measurement using BIA. So far there is no study that evaluated controlled and regular acute water intake and responses of BIA method on measurement of body composition analysis.
The present study aimed to assess the impact of acute water intake on estimates of body composition predicted by a single frequency BIA foot-to-foot appliance in healthy males and females.
2. Materials and methods
In the present study, 80 males (mean±SE age: 21.8 ± 0.1 years; height: 176 ± 0.7 cm, and BMI: 22.37 ± 0.2 kg/m2) and 60 females (mean±SE age: 21.5 ± 0.2 years; height: 165 ± 0.8 cm and BMI: 20.88 ± 0.3 kg/m2) voluntarily participated. The study protocol was approved by the Local Ethics Committee (Registration Number: 2019.01.15 and Decision Number: 2017-KAEK-189_2019.02.28_13). A signed informed writing consent was approved from each subject before participated study. Measurement of height and weight values were performed by an expert scientist subjects had no eat or drink for the preceding 12 hours. BMI was calculated as the weight in kilograms divided by the square of height in meters (kg/m2). Height was measurement to the nearest 0.1 cm without shoes using an audiometer.
Before participating in the study, all volunteers completed a health screening questionnaire form and potential participants were excluded if they were alcohol users, smokers, had a history of serious diseases of liver, cardiovascular, gastrointestinal, renal, diabetes, hypertension, or malignance. Volunteers were also excluded if they had been following a weight loss program or had participated in a regular exercise training program (trained subjects with high muscular did not participate). The subjects’ appearance was also controlled for musculoskeletal deformity (e.g., scoliosis or kyphosis). Subjects including criteria; they were free of any chronic or acute disease, e.g., renal, respiratory, metabolic, cardiac, liver disease; they should use no, smoking, alcohols or any drugs that may effects metabolic systems. The young, healthy subjects were included in this study (age between 18 and 25 years). All subjects were free of any musculoskeletal, metabolic, cardiac, respiratory, and renal disease. To avoid edema especially female subjects should not be in the menstrual phase. Body composition was measured in the morning at approximately 08:00–09:00 AM. Foot-to-foot BIA measurements were determined using a Tanita single frequency body fat analyzer (TBF 300A JAPAN). On subjects were advised to adhere to the standards of BIA measurements [16]. To avoid influence of food intake or exercise on BIA measurements, all subjects have no food or liquid intake before at least 12 hours and no diuretic medication last one week with empty gastrointestinal system and bladder. Foot to foot BIA was applied on a pressure contact electrode system. Body mass was measured to the nearest 0.1 kg while the measurement of impedance was performed. The FM, %FM, FFM, and TBW were estimated using manufacturer predictive equations and recorded to the computer for analysis. To avoid any errors may come from alteration in body fluid distribution, subjects waited for at least 10 minutes prior to testing. The subjects were asked to remove all metal and jewelry and wearing light weight clothes. The ‘’sedentary mode’’ was selected for all female and male subjects.
This study conducted of 4 stage following basal measurements of body composition. Stage 1, all subjects had 500 ml water intake and second measurement was performed after 15 minutes and recorded. Then each subjects had second 500 ml water intake (totally 1000 mL) as stage 2. Then, third 500 ml (increased to 1500 mL) as a stage 3 water intake. Lastly, stage 4, with fourth 500 ml water intake and totally increased to 2000 mL and study completed. All measurement was performed after 15 minutes of water intake in each stage.
Analyses were conducted on compare body weight, fat mass, body fat percent, fat-free mass, and total body water from BIA measurement in response to do regular water intakes of 500 mL for four times. A one-way ANOVA test was applied to detect differences between each stages in the same group. Analysis of date obtained from this study was performed separately by male and female gender. Pearson’s correlation coefficients were applied to examine any significant relations between parameters measured using BIA. Moderate correlations were defined as R values of 0.41 to 0.7 and strong correlations were accepted above 0.71 [17]. It was accepted as significant p < 0.05.
3. Results
The mean values (±SEM) of the baseline measurement and the changes of the body composition parameters measured by foot to foot BIA method after an increase in the quantity of water (4 x 500 mL) used for hydration are presented in Table 1. A regular increase of water consumption (500 mL 1000 mL, 1500 mL, and 2000 mL) resulted in an increase of body weight mean values of 471 g, 957 g, 1426 g, and 1894 g in male and 487 g, 978 g, 1443 g, and 1891 g in female subjects, respectively.
Table 1.
The mean (±SEM) values of body weight (BW), fat mass (FM) percent of body fat (%BF), fat-free mass (FFM), and total body water (TBW) in response to the baseline and for each stage of water intake (every 500 mL of water) in male and females
| BM (kg) | FM (kg) | %BF (%) | FFM (kg) | TBW (kg) | ||
|---|---|---|---|---|---|---|
| Male | Baseline | 69.36 ± 0.9 | 9.28 ± 0.4 | 12.97 ± 0.4 | 60.09 ± 0.6 | 43.09 ± 0.4 |
| Stage 1 | 69.83 ± 0.9* | 9.47 ± 0.4* | 13.21 ± 0.4* | 60.36 ± 0.6* | 43.30 ± 0.4* | |
| Stage 2 | 70.32 ± 0.9* | 9.72 ± 0.4* | 13.45 ± 0.4* | 60.57 ± 0.6* | 43.45 ± 0.4* | |
| Stage 3 | 70.79 ± 0.9* | 9.94 ± 0.4* | 13.69 ± 0.4* | 60.85 ± 0.6* | 43.63 ± 0.4* | |
| Stage 4 | 71.26 ± 0.9* | 10.17 ± 0.4* | 13.88 ± 0.4* | 61.09 ± 0.6* | 43.79 ± 04* | |
| Female | Baseline | 57.52 ± 1.0 | 12.98 ± 0.6 | 21.88 ± 0.7 | 44.55 ± 0.5 | 31.94 ± 0.4 |
| Stage 1 | 58.01 ± 1.0* | 13.45 ± 0.6* | 22.52 ± 0.7* | 44.56 ± 0.5NS | 31.95 ± 0.4NS | |
| Stage 2 | 58.50 ± 1.0* | 13.50 ± 0.6* | 22.95 ± 0.7* | 44.71 ± 0.5* | 32.07 ± 0.4* | |
| Stage 3 | 58.97 ± 1.0* | 14.19 ± 0.6* | 23.37 ± 0.7* | 44.85 ± 0.5* | 32.21 ± 0.4* | |
| Stage 4 | 59.41 ± 1.1* | 14.51 ± 0.7* | 23.69 ± 0.7* | 44.99 ± 0.5* | 32.29 ± 0.4* |
*: Significant differences compared to baseline.
NS: not significant.
In males, percent of body FM varied among the subjects, but in total, it increased significantly to 2.08% (from −5.8% to 10.7%) in stage 1, 3.80% (from −3.9% to 13.6%) in stage 2, 5.88% (from −0.7% to 15.3%) in stage 3, and 7.92% (from-1.9% to 21.4%) in stage 4 (p < 0.05). Similarly, the percentage of body fat mass also varied, but in total, it increased in females compared baseline: 3.4% (from −0.9% to 17.3%) in stage 1, 5.7% (from 0.02% to 19.7%) in stage 2, 7.8% (from 1.1% to 34.6%) in stage 3, and 9.4% (from 0.03% to 29.7%) in stage 4 (p < 0.05).
Importantly, measurements of body FM using BIA were significantly increased after each stage of water intakes in male and female subjects (Figure 1). The change of FM obtained from male and female subjects was 190 g and 460 g for 500 mL water intake; 445 g and 805 g for 1000 mL water intake; 660 g and 1141 g for 1500 mL water intake; and 891 g and 1453 g for 2000 mL water intake, respectively.
Figure 1.
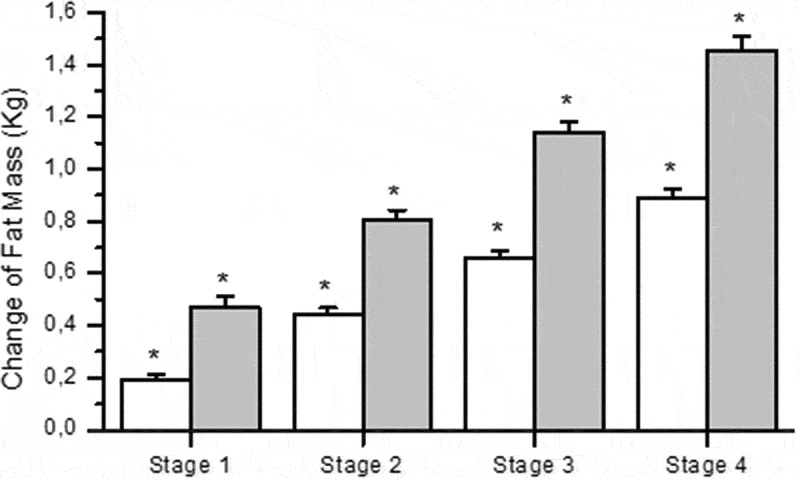
Measurements of change in body fat mass using bioelectrical impedance analysis in response to each 500 mL of water intake in male (n = 80, white column) and female (n = 60 gray column) subjects. * represent the significance compared to baseline values
Following water intake, significant differences between changes of TBW and amount of consumption in all stage in both males and females were observed (Figure 2). There was markedly lower estimation change of TBW in stage 1: 42% (212 g), stage 2: 37% (368 g), stage 3: 37% (548 g), and stage 4: 35% (700 g) in males. There was also markedly lower estimation of TBW in female subjects in stage 1: 0.6% (3 g), stage 2: 13% (130 g), stage 3: 18% (265 g), and stage 4: 17% (348 g).
Figure 2.
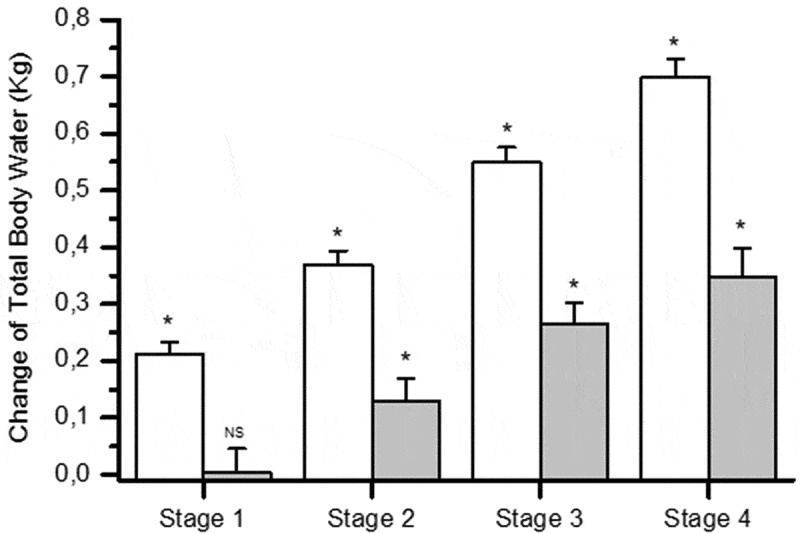
Measurements of change in total body water using bioelectrical impedance analysis in response to each 500 mL of water intake in male (n = 80, white column) and female (n = 60 gray column) subjects. * represent the significance compared to baseline values
In males, change of FFM varied among the subjects, but in total, it increased significantly to 275 g (−200 g and 900 g) in stage 1, 486 g (−1800 g and 1100 g) in stage 2, 763 g (200 g and 1200 g) in stage 3, and 1000 g (300 g and 1700 g) in stage 4 (p < 0.05). However, FFM did not change significantly in females compared baseline in stage 1 (varied between −1600 g and 600 g). The increase in FFM was observed 158 g (varied between −1000 g and 800 g) in stage 2, 293 g (varied between −900 g and 1100 g) in stage 3 and 431 g (varied between −900 g and 1500 g) (p < 0.05). There was a strong negative correlation between change of FM and TBW in female subjects (R = −0.73558, p < 0.0001) and male subjects (R = −0.78546 p < 0.0001) after stage 4.
4. Discussion
It has been revealed that BIA is a useful, easily applicable, and inexpensive tool for the evaluation of body composition of obese [10], cardiometabolic disorders [1–4], cancer [8], and hemodialysis patients [18]. Obtaining confidential information with regarding specific proportion of each section of body composition (TBW, FFM, %FM and FM) in health and also some disorder is a continue interest of clinical and scientist.
Despite the effectiveness of BIA in body composition obtained from many studies, the accuracy of this method has been questioned under the condition of fluid and electrolyte imbalance such as edema, ascites, or water loss [13]. There is currently no satisfactory information regarding the effects of regularly increasing small amount of water intake on body composition analyses using BIA method. Importantly, the results of the present study clearly show that the performance of BIA measurements in healthy populations might be influenced by the amount of acute water consumption.
In literature, changes in body composition using BIA methods after fluids intake in the range of 350 to 1000 mL have been studied. The reports revealed no significant differences in body composition analysis after 350 mL and [19] or 500 mL water intake [20]. It has been reported that acute food and water intake may have minor impact on body composition measurement using BIA method [21].
The increase of %FM in response to the one-time water intake has been reported [22]. A small increase of %FM after 591 mL of fluid which has been shown and suggested, has not any significant effects on clinical practice [23]. Effects of different hydration status (hypo-hydration or super-hydration states) on body composition analysis showed significant differences in body composition analysis in trained athletes [24] but no significant difference in wrestler [25].
Underlying assumption of valid BIA measurements may be decreased owing to the water retention caused by diseases. In literature, effects of water intake on measurement of body composition using BIA method has been studied with different amount and content of liquid application. Following regularly increasing water intake, the change in body weight and also change in impedance may have significant effects on body composition [23]. During the study, 2 L volume of water intake may have been responsible for the changes in impedance and TBW [26].
In this study, a 500 mL of water was applied for four times in every 15 minutes period to subjects (male and female) and variation of body composition (FFM, TBW, %FM, and FM) were evaluated using BIA. There was overestimation in %FM and FM values but underestimation in TBW and FFM values in both subject groups (Figure 1 and Table 1). Therefore, acute alterations in hydration do indeed lead to changes in body mass resulting in changes in BIA-derived body fat percentage [22,24,27].
A study performed in morbidly obese patients also revealed overestimation of body fat using BIA method due to increased extracellular water [13]. It is logical to expect change in plasma sodium concentrations after water intakes which may quite possible to effect BIA measurements [28]. Hyperhydration condition may cause underestimation of TBW using foot-to foot BIA measurements [29].
The change of TBW measured using BIA in response to do water intake has been shown in Figure 2. There was markedly underestimation in TBW in female subjects compared to males. Interestingly in stage 1, there was no significant change in TBW despite 500 mL of water intake (Figure 1). The increase in BW after water intake showed small differences which could be result of error in the measurement of BIA device [20].
In stage 1 (500 mL of water intake), we have found significant variations in %BF values among male subjects in individually (from −5.8% to 10.7%), but mean values of %BF within 2% which is considered as optimal size of error [20]. However, with increasing water intake, overestimation of %BF increased regularly to 3.8% in stage 2, 5.8% in stage 3, and 7.9% in stage 4. Interestingly, every 500 mL of water intake causes an additional 2% of increase in %BF measured by BIA method. Effects of water intake have markedly higher effects on %FM estimation in females compared to males in BIA measurements. Measurement of %FM was 3.4% in stage 1 which is higher than accepted normal range of 2%. Increased water intake caused overestimation of %FM in stage 2 (5.7%), in stage 3 (7.8%), and in stage 4 (9.4%). Interestingly there was no negative %FM measurement in females (except stage 1) during the study. Acute water application caused significantly alteration in body composition analyses using BIA method. These variations in body composition compartment also varied between male and female subjects, and increased water intake causes more increase in %FM and FM in females than those of male subjects. Consequently, the large variability and weak validity of BIA measurements under condition of water retention raise question whether it makes sense to continue BIA application.
Funding Statement
This study is supported by Yozgat Bozok University ‘Scientific Research Project’ (BAP) unit.
References
- [1].Bosy-Westphal A, Braun W, Geisler C, et al. Body composition and cardiometabolic health: the need for novel concepts. Eur J Clin Nutr. 2018;72(2):638–5. [DOI] [PubMed] [Google Scholar]
- [2].Maffeis C, Morandi A.. Body composition and insulin resistance in children. Eur J Clin Nutr. 2018;72(9):1239–1245. [DOI] [PubMed] [Google Scholar]
- [3].Andreoli A, Garaci F, Cafarelli FP, et al. Body composition in clinical practice. Eur J Radiol. 2016;85(8):1461–1468. [DOI] [PubMed] [Google Scholar]
- [4].Yang EM, Park E, Ahn YH, et al. Measurement of fluid status using bioimpedance methods in korean pediatric patients on hemodialysis. J Korean Med Sci. 2017;32(11):1828–1834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Lavie CJ, Milani RV, Ventura HO, et al. Body composition and heart failure prevalence and prognosis: getting to the fat of the matter in the ‘obesity paradox. Mayo Clin. 2010;85(7):605–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Mousavi SV, Mohebi R, Mozaffary A, et al. Changes in body mass index, waist and hip circumferences, waist to hip ratio and risk of all-cause mortality in men. Eur J Clin Nutr. 2015;69(8):927–932. [DOI] [PubMed] [Google Scholar]
- [7].Nyboer J. Electrorheometric properties of tissues and Øuids. Ann NY Acad Sci. 1970;170:410–420. [Google Scholar]
- [8].Haverkort EB, Reijven PL, Binnekade JM, et al. Bioelectrical impedance analysis to estimate body composition in surgical and oncological patients: a systematic review. Eur J Clin Nutr. 2015;69(1):3–13. [DOI] [PubMed] [Google Scholar]
- [9].Nagano M, Suita S, Yamanouchi T. The validity of bioelectrical impedance phase angle for nutritional assessment in children. J Pediatr Surg. 2000;35(7):1035–1039. [DOI] [PubMed] [Google Scholar]
- [10].Ozcelik O, Ozkan Y, Algul S, et al. Beneficial effects of training at the anaerobic threshold in addition to pharmacotherapy on weight loss, body composition, and exercise performance in women with obesity. Patient Prefer Adherence. 2015;13(9):999–1004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Khalil SF, Mohktar MS, Ibrahim F. The theory and fundamentals of bioimpedance analysis in clinical status monitoring and diagnosis of diseases. Sensors (Basel). 2014;14(6):10895–10928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Wu CS, Chen YY, Chuang CL, et al. Predicting body composition using foot-to-foot bioelectrical impedance analysis in healthy Asian individuals. Nutr J. 2015;19(14):52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Coppini LZ, Waitzberg DL, Campos AC. Limitations and validation of bioelectrical impedance analysis in morbidly obese patients. Curr Opin Clin Nutr Metab Care. 2005;8(3):329–332. [DOI] [PubMed] [Google Scholar]
- [14].Haroun D, Taylor SJ, Viner RM, et al. Validation of bioelectrical impedance analysis in adolescents across different ethnic groups. Obesity (Silver Spring). 2010;18(6):1252–1259. [DOI] [PubMed] [Google Scholar]
- [15].Brien CO, Zouny AJ, Sawka MN. Bioelectrical impedance to estimate changes in hydration status. Int J Sport Med. 2002;23(5):361–366. [DOI] [PubMed] [Google Scholar]
- [16].Heyward VH, Wagner DR. Applied body composition assessment. Champaign IL: Human Kinetics; 2004. [Google Scholar]
- [17].Cohen J. Statistical power analysis for the behavioural sciences. Vol. 2. Hillsdale NJ: Lawrence Erlbaum Associates; 1998. [Google Scholar]
- [18].Park JH, Jo YI, Lee JH. Clinical usefulness of bioimpedance analysis for assessing volume status in patients receiving maintenance dialysis. Korean J Int Med. 2018;33(4):660–669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Heiss CJ, Naylor J, Bronco KM, et al. A small food or fluid load has no effect on body composition measured by 3 different methods. Top Clin Nutr. 2008;23(3):229–233. [Google Scholar]
- [20].Kutac P. The effect of intake of water on the final values of body composition parameters in active athletes using two different bioimpedance analyzers. Acta Gymnica. 2014;44(2):107–116. [Google Scholar]
- [21].Androutsos O, Gerasimidis K, Karanikolou A, et al. Impact of eating and drinking on body composition measurements by bioelectrical impedance. J Hum Nutr Diet. 2015;28(2):165–171. [DOI] [PubMed] [Google Scholar]
- [22].Demura S, Yamaji S, Goshi F, et al. The influence of transient change of total body water on relative body fats based on three bioelectrical impedance analyses methods comparison between before and after exercise with sweat loss, and after drinking. J Sports Med Phys Fitness. 2002;42(1):38–44. [PubMed] [Google Scholar]
- [23].Dixon CB, Lovallo SJ, Andreacci JL, et al. The effect of acute fluid consumption on measures of impedance and percent body fat using leg-to-leg bioelectrical impedance analysis. Eur J Clin Nutr. 2006;60(1):142–146. [DOI] [PubMed] [Google Scholar]
- [24].Saunders MJ, Blevins JE, Broeder CE. Effects of hydration changes on bioelectrical impedance in endurance trained individuals. Med Sci Sports Exerc. 1998;30(6):885–892. [DOI] [PubMed] [Google Scholar]
- [25].Utter A, McAnulty SR, Riha BF, et al. The validity of multifrequency bioelectrical impedance measures to detect changes in the hydration status of wrestlers during acute dehydration and rehydration. J Strength Condit Res. 2012;26(1):9–15. [DOI] [PubMed] [Google Scholar]
- [26].Gomez T, Mole PA, Collins A. Dilution of body fluid electrolytes affects bioelectrical impedance measurements. Sports Med Training Rehab. 1993;4(4):291–298. [Google Scholar]
- [27].Kushner RF, Gudivaka R, Schoeller DA. Clinical characteristics influencing bioelectrical impedance analysis measurements. Am J Clin Nutr. 1996;64(3 Suppl):423S–427S. [DOI] [PubMed] [Google Scholar]
- [28].Berneis K, Keller U. Bioelectrical impedance analysis during acute changes of extracellular osmolality in man. Clin Nutr. 2000;19(5):361–366. [DOI] [PubMed] [Google Scholar]
- [29].Matthews EL, Hosick PA. Bioelectrical impedance analysis does not detect an increase in total body water following isotonic fluid consumption. Appl Physiol Nutr Metab. 2019;44(10):1116–1120. [DOI] [PubMed] [Google Scholar]