

ABSTRACT
Education intervention effectiveness to improve bed net care and repair knowledge or practices is unclear. To assess intervention effectiveness, we systematically reviewed eight peer-reviewed literature databases and 16 malaria organizations (PROSPERO protocol CRD42019123932) using pre-specified combinations of ‘education intervention’, ‘mosquito net’, and ‘malaria’ search terms. Data were abstracted for 29 of 43 studies meeting inclusion criteria, of which 16 studies included education as amain focus. Of these 16, there was evidence of intervention effectiveness among half of the studies, which reported improvements in knowledge or practices, while four had mixed results, and four had unclear results. Overall there is no clear conclusion regarding the effectiveness of education interventions to improve net care and repair, though some instructional methods suggest more success than others. Interventions used combinations of instructional methods; passive mass education (6), active mass education (12), and interpersonal methods (8). Interventions combining mass and interpersonal methods resulted in positive improvements (four positive, one mixed). We found no evidence that interventions grounded in health behavior theory achieved more positive results than those not grounded in theory, potentially because net care education was typically asecondary objective. Of 289 gray literature results, 286 (99%) were net distribution reports from Against Malaria Foundation describing 136 distributions; eighty of which (58.8%) mentioned no education related to net care and repair. We found lack of involvement of experts in education among included interventions. Involving trained instructors with expertise in education theory and instructional strategies may improve instruction quality to yield more effective interventions.
KEYWORDS: Malaria, education interventions, care and repair, LLIN, bed nets
Introduction
The distribution of long lasting insecticide treated nets (LLINs) is a key strategy for malaria prevention. In recent decades, bed net technology has evolved along with the recommendations for maintaining them. The first generation of untreated nets offered physical protection from mosquito bites and showed the ability to reduce parasitemia [1] but required careful handling to avoid rips and tears. The introduction of insecticide treated bed nets (ITNs) led to greater reductions in malaria morbidity and mortality [2,3] as a reduction in vector populations was coupled with physical protection, particularly when deployed at high levels within communities [4–6]. Introducing ITNs required campaigns to treat existing nets and distribute new nets that were already impregnated with insecticide, which met challenges in reaching high levels of net treatment and retreatment [7]. Care recommendations for older ITN models care included (1) washing the net the day prior to treatment/retreatment, (2) soaking the net in the insecticide mixture, (3) gently wringing out the net, (4) drying flat in the shade (5) washing gently, as seldom as possible, (6) and regular retreatment [8].
The newest models of bed nets are LLINs, which do not require retreatment with insecticide. LLINs have an intended effective life of 3–5 years. LLIN care recommendations include (1) never to seldom washing, at most once every 3 months (2) washing gently with mild soap, (3) drying in the shade and avoiding exposure to direct sunlight (4), tying or hanging the net up during the day and (5) quickly repairing all holes [9]. Recommendations for some OlysetTM brand nets include a regeneration process by exposing washed nets to sunlight for 5–6 h in the original transparent vinyl packaging [10].
Bed net care and repair refers to the actions taken to adhere to maintenance instructions, prevent damage, and repair damage to nets [11]. Many studies describing net care and repair behaviors conclude that education interventions or behavior change communication (BCC) strategies should be implemented to improve care and repair adherence [12–19]. Education interventions are activities that include a form of messaging aimed at changing or improving knowledge and/or behaviors. These include interventions such as BCC, Information, Education, and Communication (IEC) campaigns, and social marketing campaigns.
Changing health behaviors are a goal of many public health initiatives, and malaria education interventions are no different. Health behavior theories guide understandings of health behaviors. Previous studies have shown that grounding behavior change interventions within appropriate theory is essential for comprehensive and effective campaigns [20,21]. A systematic review of health behavior articles from 2000 to 2005 revealed that 35.7% of the included studies mentioned theory [22]. For interventions to translate into evidence-based public health practice, they must be described in appropriate detail for comparability and replication [23]. Furthermore, education interventions involve instruction as their core – methods to convey content to the target audience. Beyond sound health behavior theory, interventions should describe the specific instructional strategies employed [24], as delivery of the educational events is highly important to the intervention’s success.
While multiple studies suggest education interventions should be used to improve adherence to bed net care and repair recommendations, the evidence of intervention effectiveness across differing contexts remains unclear. Identifying the types of approaches that lead to better adherence to net care and repair recommendations will allow for more comprehensive and effective education interventions.
Methods
We conducted a systematic literature review to evaluate whether education interventions increase knowledge of or adherence to recommended bed net care and repair practices. Net durability or longevity was evaluated as a potential secondary outcome. We searched for interventions targeting either ITNs or LLINs. Though ITNs are no longer distributed, interventions focusing on ITNs were included because many of the recommendations for care of ITNs and LLINs overlap, and we were interested in change in knowledge or practices. Information abstracted included the specific care and repair practices targeted and the degree to which interventions applied educational and health behavior theories.
Search strategy
The protocol was registered through PROSPERO International Prospective Register of Systematic Reviews on 30 April 2019 (registration number CRD42019123932). We worked with a medical librarian (DM) to identify studies through a literature search using controlled vocabulary terms and key word combinations for ‘education intervention’ terms, ‘mosquito net’ terms and malaria (Table 1, Appendix 1) with no language restrictions. Specific LLIN brands (Table 1) were included in the ‘mosquito net’ terms to capture titles that may only include a brand name rather than a more general term. The search was conducted on 13 February 2019 in MEDLINE PubMed (1946–2019, 13 February), Embase (1947–2019, 13 February), Cochrane Controlled Register of Trials CENTRAL (1966–2019, 13 February), Bibliomap (indexing date not reported – 13 February 2019), ProQuest Dissertations & Theses (1982–2019, 13 February), Trials Register of Promoting Health Interventions TRoPHI (2004–2019, 13 February) and Clarivate Web of Science Core Collection (1900–2019, 13 February) databases (Table 2). Citations were imported into EndNote X8 (Thomas Reuters) for deduplication and management.
Table 1.
Search terms adapted for use in database searches for peer-reviewed studies.
| Category | Search Terms |
|---|---|
| Bed nets | ‘mosquito nets’ [Mesh] ‘LLIN’ ‘LLINs’ ‘long lasting insecticide treated nets’ ‘long lasting insecticide treated bednets’ ‘long lasting insecticide treated bed nets’ ‘long lasting insecticidal nets’ ‘long-lasting insecticide-treated nets’ ‘ITN’ ‘ITNs’ ‘Insecticide treated nets’ ‘insecticide treated bednets’ ‘insecticide treated bed nets’ ‘Icon Life’ Yorkool Olyset Netprotect Permanet |
| Malaria | ‘Malaria’ [Mesh] Malaria |
| Education interventions | ‘health education’ [Mesh] ‘health behavior’ [Mesh] ‘intervention’ ‘education intervention’ ‘malaria education’ ‘education campaign’ ‘behavior change’ ‘behaviour change’ |
Table 2.
Databases and malaria organizations searched for malaria education intervention records.
| Peer-Reviewed Literature Databases | Gray Literature: Malaria Organizations |
|---|---|
| BiblioMap | African Leaders Malaria Alliance |
| Cochrane Central Register of Controlled Trials (CENTRAL) | Against Malaria Foundation |
| Embase | Bill & Melinda Gates Foundation |
| ProQuest Dissertations and Theses Global | The Global Fund |
| PubMed | Imagine No Malaria |
| Trials Register of Promoting Health Interventions (TRoPHI) | Kenya NGOs Alliance Against Malaria |
| Web of Science | Malaria Atlas Project |
| JSTOR | Malaria Consortium |
| Malaria No More | |
| Medicines for Malaria Venture | |
| National Institute of Malaria Research | |
| Nothing But Nets | |
| Roll Back Malaria | |
| South African Malaria Initiative | |
| United States Agency for International Development | |
| World Health Organization |
The searches identified 6,507 studies prior to removing duplicates. Deduplication in EndNote X8 (Thomas Reuters) resulted in 5,927 studies. Studies were reviewed following the protocol set forth by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Initial screening of titles and abstracts was completed by two reviewers (ES, CS) with a third reviewer (KE) assessing discrepancies, according to the following study inclusion criteria: malaria education intervention, communication campaign, or behavior change campaign pertaining to bed net care and repair practices for ITNs or LLINs. Studies published in English, Spanish, and French were reviewed due to the language abilities of the three reviewers. We managed data in Google Sheets (Google, Mountain View, CA) with individual reviewer columns hidden to other reviewers to maintain a blinded screening process.
After initial screening, full-text articles for 446 studies were retrieved and screened by two reviewers (ES, CS) with a third reviewer (KE) assessing discrepancies through the same blinded process as initial screening. Studies were assessed according to the same inclusion criteria as in the initial screening process with the application of the following exclusion criteria (Figure 1): malaria intervention that does not pertain to bed net care and repair, education intervention not relevant to malaria, review papers, conference abstracts, and commentary/opinion pieces.
Figure 1.
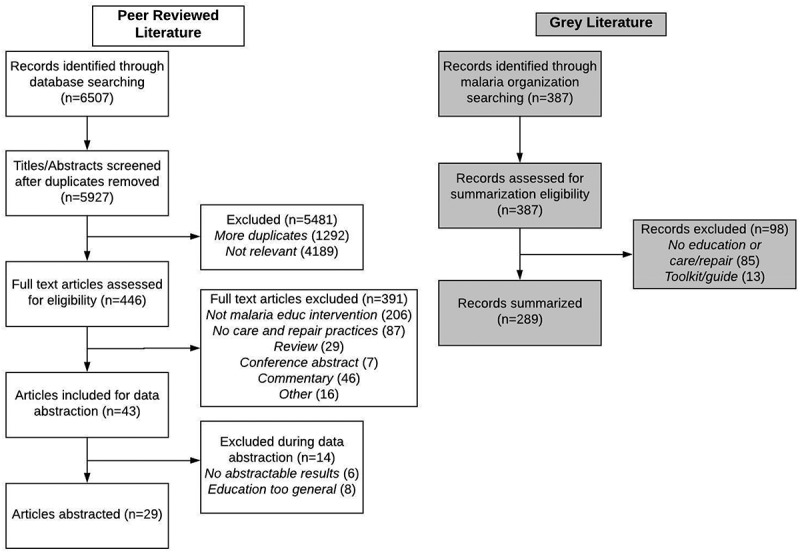
PRISMA scheme of record selection and exclusion criteria.
Gray literature was identified through relevant organizations that support bed nets for malaria prevention (Table 2). We developed the list of organizations to be searched through Google searches including ‘malaria organizations’, ‘malaria non-governmental organizations’, and variations of ‘mosquito net distributions’ and ‘mosquito net donations’. Organizations were searched from 12 to 20 March 2019. We navigated all headings and links within organizational websites to identify all records related to malaria education and/or bed net care and repair practices were retrieved and reviewed to be summarized.
Data abstraction
The resulting 43 peer-reviewed studies were included for data abstraction. We collected details of the study location, population, years of intervention, and category of malaria endemicity (endemic vs. epidemic areas). Additionally, we abstracted data on the intervention purpose and description, the care and repair practices targeted, the results from intervention and comparison groups, the types and descriptions of education activities, and the details of any health behavior theories, education theories, and/or instructional strategies described within the methods.
Quality assessment
Due to the variety of study designs including quantitative and qualitative designs, a single existing quality screening tool was not appropriate to assess the quality of the included studies in relation to the study question. Therefore, we developed a 6-item quality criteria tool (Table 3) and scored the studies that had education interventions as a main component. Studies received either 1 (contains the criteria item) or 0 (does not contain the criteria item) points for each quality criteria, resulting in a potential score range between 0 and 6. Articles containing 1–2 criteria received 1 star, those containing 3–4 received 2 stars, and those containing 5–6 received 3 stars.
Table 3.
Education intervention quality criteria tool in relation to the study question.
| Quality Criteria | 1 point | 0 points | |
|---|---|---|---|
| 1 | Was there a well-defined comparison group? | Yes (1) | No (0) |
| 2 | Was the comparison group selected appropriately? | Yes (1) | No or answer to question 1 = 0 (0) |
| 3 | Was there an explicit link to appropriate health behavior theory? (An appropriate theory is one that targets the appropriate level of audience of individual, community, children, or adults) | Yes (1) | No (0) |
| 4 | Was there an adequate description of educational activities? | Yes (1) | No (0) |
| 5 | Were the educational activities equitable for diverse learners? (Equitable activities include the implementation of multiple types of activities such as audio, visual, interpersonal, etc) | Yes (1) | No (0) |
| 6 | Was there hypothesis testing of the differences between groups pertaining to net care knowledge and/or practices? | Yes (1) | No (0) |
Results
Records were excluded through the screening process because they were not malaria education interventions (n = 206) or because they were education interventions, but were not related to bed net care and repair practices in any way (n = 87) (Figure 1). Others were found to be conference abstracts (n = 7), commentary pieces (n = 46), reviews (n = 29), or were excluded for other reasons (n = 16). Of the 43 remaining articles, we abstracted data from 29, excluding 14 in the process because they lacked care or repair results (n = 6) or because the education was too general, meaning we found no evidence that education on net care and repair practices was provided (n = 8).
After searching multiple malaria organizations (Table 2) we identified 387 records pertaining to malaria education (Figure 1) in the gray literature search. We screened all of these records for eligibility to be summarized, excluding 98 in the process. We excluded records if they did not mention anything about malaria health education or bed net care and repair (n = 85) or if they were toolkits or guides, hence not an activity that included education on care and repair (n = 13). This resulted in 289 gray literature records to be summarized (Figure 1).
Peer reviewed literature
Malaria education as a main focus
Key findings of education on net care and repair knowledge and/or practices are described for each article in Table 4. An education intervention was the main activity of 16 (55.2%) of the 29 included peer-reviewed articles (Table), and a relatively minor activity of the remaining 13 articles (44.8%). Of the 16 articles with education intervention as a main activity, 12 were studies conducted in sub-Saharan Africa, and the remaining four conducted in Latin America, the Middle East, and Southeast Asia (Table). Regarding the main outcomes measured in Table 3, six studies focused on increasing ITN or LLIN use [25–30], six focused on generally improving malaria knowledge, attitudes, and/or practices [27,29–33], and five focused more specifically on outcomes related to net durability or care and repair [34–38]. Among the care and repair practices addressed in the articles, nine provided education of ITN treatment or retreatment with insecticide [26,27,30–34,39,40], four educated about net storage during the day [25,36–38], two about appropriate soap types to use in washing nets [37,38], one about recommended drying practices [37], and one about the manner of washing nets gently [38] (Table 4).
Table 4.
Characteristics, key findings, and quality scores of peer-reviewed articles with a malaria education main focus.
| Author, Year ★ [citation] | Country, Intervention years, Sample size | Main outcomes | Care and repair practices addressed | Key care and repair findings | Theoretical framework, level of use | Care and repair conclusions |
|---|---|---|---|---|---|---|
| Marsh, 1996 [25] ★★★ | Kenya, 1993–1994, 200 mothers & 50 household heads | ITN use | Storage, washing frequency, repair | Knowledge of bed net messages among children increased from 58.2% pre-education to 80.5% 3 months post-education. Post-intervention, between 33-50% of parents reported hearing messages from children, and specific bed net messages could be recalled by 30% of mothers. | Community Research & Health Education Framework, Built upon | Improved knowledge |
| Mfaume, 1997 [34] ★ | Tanzania, 1993, 44 mosque attendees | ITN retreatment | Retreatment | Post intervention 52-98% of households regularly retreated their nets | None | Unclear |
| Minja, 2001 [26] ★★ | Tanzania, 1996–1997, 26 focus groups, 39 in-depth interviews, 204 survey respondents | ITN ownership and use | Treatment/retreatment | Pre-IEC campaign 3% of survey respondents had treated nets and 34% had knowledge of retreatment. Post-IEC campaign, ITN ownership and use increased to >50% | Social Marketing, Informed by | Unclear |
| Rhee, 2005 [27] ★ | Mali, 2003, 133 households | ITN use, malaria knowledge | Treatment/retreatment | Education intervention had no effect on household net treatment/retreatment (OR 1.6, 95% CI 0.8,3.3) | None | Mixed. Improved practices at individual, but not household level |
| Alvarado, 2006 [31] ★★★ | Colombia, 1995–1997, 450 respondents from 20 villages | Malaria knowledge, attitudes, and practices, malaria incidence | Treatment/retreatment | Intervention led to no change in net retreatment (OR 0.88, 96% CI 0.57,1.86). | Precede-Proceed Model, Applied | Did not improve practices |
| Panter-Brick, 2006 [35] ★★★ | The Gambia, 2003, 92 households | Bed net repair | Repair | Mean % holes repaired increased from 27-41% (p < 0.001) No improvement in net quality |
Social Ecology Model, Informed by | Mixed. Improved practices, did not improve net quality |
| Nonaka, 2008 [32] ★★★ | Laos, 2004–2005, 130 schoolchildren, 103 guardians of schoolchildren, & 130 married women without children | Malaria knowledge, attitudes, practices | Treatment/retreatment was 1 of 7 points in the Malaria Attitudes score | Difference in mean Malaria Attitudes score of 1.6 points (p < 0.001) between intervention and control groups | None | Improved attitudes |
| Widmar, 2009 & Ho, 2012 [39,40] ★★ | Tanzania, 2007–2008, 344 households | LLIN coverage | Retreatment, repair | Knowledge that LLINs do not require retreatment increased from 23.5–39.4% (p < 0.001) and knowledge to repair nets increased from 37.1–90.4% from pre-intervention to 15 month follow up | Theory of Planned Behavior, Informed by | Improved knowledge |
| Ayi, 2010 [33] ★★★ | Ghana, 2007–2008, 186 schoolchildren & 383 adults | Malaria knowledge, parasite prevalence | Retreatment | Net retreatment increased from 21.5–50.0% (p < 0.001) in the intervention group and from 25.3–30.5 (p > 0.05) in the control group from pre-education to follow up |
Health Promoting School Concept, Participitory Learning and Action Instructional Model, Informed by | Improved practices |
| Rickard, 2011 [28] ★★★ | Ghana, 2008–2009, 61 households | ITN use | Washing, repair, general maintenance | Knowledge of net repair increased from 54.7–81.3% (p < 0.001) from baseline to 1 year post intervention | None | Improved knowledge |
| Ahmadi, 2012 [29] ★ | Iran, 2009, 2563 households | LLIN use, malaria perceptions and practices | Washing frequency | 76.3% of untreated net households washed every 6 months compared to 68.9% of LLIN households. 23.7% of untreated net households washed every year compared to 31.1% of LLIN households | None | Unclear |
| Amoran, 2012 [30] ★★★ | Nigeria, ~2010, 400 nursing mothers | ITN knowledge and use | Retreatment | From pre-intervention to follow up, increase in knowledge of when to retreat ITNs from 39-76% (p < 0.001) among intervention group compared to 17.0–17.8% (p > 0.05) among the control group | None | Improved knowledge |
| Harvey, 2013 [36] ★★ | Peru, 2000–2001, 15 households | Treatment, net care | Storage during day | In phase 1, 33% of households stored their nets properly during the day at least 80% of the time compared to 47% of households in phase 2 | Trials of Improved Practices, Applied | Unclear |
| Helinski, 2015 [37] ★★★ | Uganda, 2013–2014, 870 households | LLIN durability | Storage during day, washing frequency, soap type, drying, repair | No difference between intervention and comparison group in the increase in net repairs from baseline to follow up (5.6–56.4% intervention group, 3.4-48% comparison group) Knowledge at follow up: Handle nets with care 39.9% int, 28.3% comp (p = 0.059) Keep away from fire 16.6% int, 17.6% comp (p = 0.800) Keep away from rats 21.3% int, 11.4% comp (p = 0.007) Keep away from children 29.3% int, 15.5% comp (p = 0.003) Roll/tie up when not in use 57.0% int, 51.1% comp (p = 0.215) Wash less often 16.7% int, 31.9% comp (p = 0.001) Wash with ordinary soap 62.0% int, 73.9% comp (p = 0.014) Dry in shade 61.2% int, 52.7% comp (p = 0.080) Repair holes 58.5% int, 10.3% comp (p < 0.001) |
Net Care and Repair Conceptual Framework, Informed by | Mixed. Improved knowledge, did not improve net durability |
| Koenker, 2015 [38] ★★★ | Nigeria, 2012–2014, 2170 households | LLIN care and repair behaviors, net condition | Storage during day, washing frequency, soap type, washing manner | No difference between intervention and control group in the increase of observed repairs at follow up (10.5–26.5% intervention, 10.3–17.8% controls p > 0.05) Nets tied up during the day were more likely to be in serviceable condition at follow up (OR 2.70 95% CI 1.50,4.86) 50.1% of nets survived to follow up among households that recalled care and repair messages compared to 30.9% of nets among households that could not recall messages Recall of messages at follow up Handle carefully 61% int, 35% cont (p < 0.05) Avoid fire 22% int, 12% cont (p < 0.05) Repair early 26% int, 12% cont (p < 0.05) Tie/fold up when not in use 36% int, 30% cont (p > 0.05) Don’t soil with food 22% int, 11% cont (p < 0.05) Wash only when dirty 21% int, 11% cont (p < 0.05) Use mild soap 46% int, 27% cont (p < 0.05) Wash gently 41% int, 29% cont (p > 0.05) Reported practices at follow up Keep away from children 49% int, 31% cont (p < 0.05) Keep away from pests 23% int, 12% cont (p < 0.05) Roll/tie up when not in use 43% int, 30% cont (p > 0.05) Handle with care 38% int, 25% cont (p < 0.05) Don’t soil with food 27% int, 13% cont (p < 0.05) Keep away from fire 15% int, 10% cont (p > 0.05) Wash gently 46% int, 30% cont (p < 0.05) Wash only when dirty 42% int, 36% cont (p < 0.05) Inspect regularly for holes 11% int, 5% cont (p > 0.05) Repair quickly 12% int, 4% cont (p < 0.05) |
P-Process, Built | Improved knowledge, improved practices |
★Quality rating: ★ = meets 1–2 quality criteria, ★★ = meets 3–4 quality criteria, ★★★ = meets 5–6 quality criteria. ITN – Insecticide treated net, LLIN – Long lasting insecticide treated net, Treated/retreatment refers to treating or retreating a bed net with insecticide, OR- Odds ratio, CI – Confidence interval, Int – Intervention group, Cont – Control group, Comp – Comparison group A Data are estimates abstracted from a figure.
We assessed whether studies were informed by or utilized health behavior and/or instructional theories or models (Table 5). Of the 16 articles that had health education as a main activity, 10 were informed by, applied, or built health behavior theories [25,26,31,33,35–40] while six mentioned no grounding in theory (Table 4) [27–30,32,34]. Of those mentioning theory, six were informed by theory, two applied theory, and two built novel theory. Based on the key bed net care and repair findings, we determined whether there was evidence that the education interventions led to improvements in care and repair knowledge, practices, and/or net durability. There were eight studies that reported overall improvements [25,28,30,32,33,38–40], though it is important to note that two articles reported on the same study [39,40]. There were four studies with mixed results [27,31,35,37], and four in which it was unclear whether improvements occurred [26,29,34,36]. There was no apparent pattern in care and repair conclusions in regard to whether theory was mentioned or how theory was used (Table 5). Of those articles not grounded in theory (n = 6), 50% reported positive care and repair outcomes, while five (50%) of the articles grounded in theory (n = 10) reported positive care and repair outcomes.
Table 5.
Care and repair conclusions in relation to theory use of education interventions.
Table 6 describes the care and repair conclusions in relation to the types of education strategies implemented. Mass education includes passive interventions where no personal contact is made between those implementing and the recipients of the education or active interventions where there is personal contact between education implementers and recipients. There were six interventions that used passive mass education, which included activities such as posters, slogans, print and audiovisual media, pamphlets, t-shirts, radio programs, newspapers, maintenance labels, and social marketing [26,30,33,35,37,38]. Active mass education activities were conducted within 12 interventions and included dramas, music, poetry, art, demonstrations, community events and workshops, lectures, small group flip-chart presentations, and advocacy by community health workers [25,26,30–35,37-40]. Interpersonal education involves activities such as education through house-to-house visits, establishing village bed net committees that talk with community members, dialogs and conversations, debates, training local health leaders, and individual flip-chart education. Eight interventions used interpersonal methods [25,27,28,32,33,36–38]. Discerning between mass and interpersonal education methods, there were six interventions that used mass strategies only, and three interventions that used interpersonal strategies only (Table 6). Care and repair conclusions of those six that used only mass education were two positive, one negative, two unclear, and two mixed results (Table 6). There was a positive, unclear, and mixed result each from those three articles using only interpersonal strategies. Stronger results were observed from interventions that combined at least one mass education strategy with interpersonal methods, where four interventions had positive care and repair results and one had mixed results (Table 6).
Table 6.
Care and repair conclusions in relation to education methods ★ indicates quality score.
| Mass education |
||||
|---|---|---|---|---|
| [citation] ★ | Care and repair conclusions | Passive mass education | Active mass education | Interpersonal education |
| [25] ★★★ | Positive | X | X | |
| [34] ★ | Unclear | X | ||
| [26] ★★ | Unclear | X | X | |
| [27] ★ | Mixed | X | ||
| [31] ★★★ | Negative | X | ||
| [35] ★★★ | Mixed | X | X | |
| [32] ★★★ | Positive | X | X | |
| [39,40] ★★ | Positive | X | ||
| [33] ★★★ | Positive | X | X | X |
| [28] ★★★ | Positive | X | ||
| [29] ★ | Unclear | |||
| [30] ★★★ | Positive | X | X | |
| [36] ★★ | Unclear | X | ||
| [37] ★★★ | Mixed | X | X | X |
| [38] ★★★ | Positive | X | X | X |
Figure 2 depicts the care and repair outcomes through the interaction between education type (mass vs. interpersonal vs. both) and theory use. The only clear pattern in outcomes exists among interventions that used both mass and interpersonal education methods, regardless of theory use. Of these interventions, four reported positive results and one reported mixed results. The intervention [32] that used both education methods, but did not use theory, reported positive net care and repair results. A variety of results were found among articles that used a single method of education and did or did not use theory (Figure 2).
Figure 2.
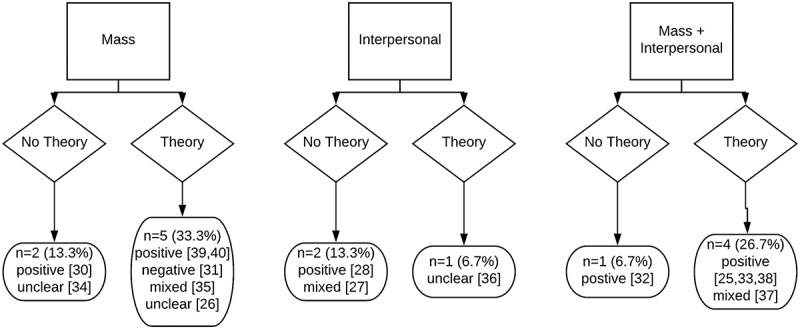
Care and repair conclusions in relation to education methods and theory use.
Quality assessment
Education intervention quality was assessed for the 16 articles that had health education as a main activity (Table 4) using the rubric detailed above (Table 3, Appendix F). We classified the education intervention component of three articles as single star [27,29,34], of which two had unclear results and one had mixed results of bed net care and repair measurements. Four articles had two stars for their education intervention components [26,36,39,40]. Two of these articles had unclear care and repair conclusions, while improved knowledge was measured in the other two. However, the two articles reporting improved knowledge were describing the same study [39,40]. There were nine articles that received three stars, six of which reported improvements in care and repair knowledge and/or practices [25,28,30,32,33,38], and three of which reported mixed results of care and repair knowledge or practices [31,35,37]. None of the one-star quality-rated education interventions, all of the two-star interventions, and six of the three-star interventions mentioned a theoretical framework.
Malaria education as a minor element
Of the 13 articles that contained an element of malaria education, but for which education was not a main focus, nine were studies conducted in sub-Saharan Africa, and the remaining four in South and Southeast Asia and South America (Table 5). The main outcomes studied ranged from malaria indices [41–43], aspects of bed net care and repair [10,44–47], program evaluation [43,48,49], and bed net coverage and/or use [44,46,47,50,51]. The bed net care and repair practices addressed by the articles in Table 4 include washing frequency [10,41,42,46,47,50–52], ITN treatment and/or retreatment with insecticide [42,44–46,48,49,52], net storage during the day [42], bed net repair [10,42,44,52], appropriate soap type [47], proper drying practices [47,51], and general care messages [43,45]. Only one of the 13 articles in Table 4 mentioned theoretical framework. Snow et al. (1999) used social marketing strategies to increase net ITN retreatment and found that house-to-house retreatment schemes can be highly effective in increasing retreatment, but that the delivery mechanism is more important than social marketing [45]. Overall, five articles reported improvements in bed net care and repair knowledge and/or practices [42,47–49,52], three articles had mixed results [44,45,51], four had unclear results [41,43,46,50], and one reported negative results following education efforts [10] (Table 5).
The number of bed net care and repair messages varied between the 29 peer-reviewed studies. More than half of interventions provided education on only one care and repair recommendation (15 studies), four articles educated on two recommendations, six articles on three recommendations, and only three studies educated on four or more recommendations (Tables 4 and 5).
Gray literature
Of the 289 gray literature records included for summarization (Figure 1), 286 (99%) were from the Against Malaria Foundation [53]. These records encompass 136 net distributions completed by various organizations between 2006 and 2017 across 26 countries in sub-Saharan Africa, five countries in South and Southeast Asia, and three countries in Latin America. Each distribution included a pre-distribution report and at least one distribution report detailing the plans and completed actions of the distributions including education components. We summarized the specific bed net care and repair education messages reported through these distribution reports (Figure 3). More than half (80, 58.8%) of the distributions did not mention any aspects of bed net care and repair, while 38 (27.9%) of the distributions included messaging around general net care defined as stating only ‘maintenance’ or ‘general care instructions’. There were 26 (19.1%) of distributions addressing specific care and repair practices including washing (15.4%), drying (6.6%), avoiding damage (2.2%), appropriate storage during the day (2.2%), repair (1.5%), and appropriate soap types (0.7%) (Figure 3). These do not add to 100% because some reports included both general care and at least one specific care practice.
Figure 3.
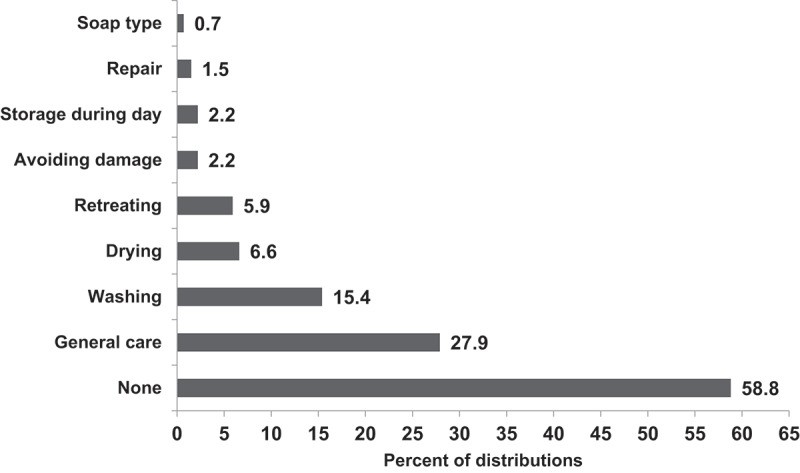
Bed net care and repair messages reported among 136 against malaria foundation-funded bed net distributions.
The remaining three gray literature records included were from Imagine No Malaria (one record) and Malaria Consortium (two records). Imagine No Malaria did not detail a particular education intervention, but rather reported that the organization supports bed net distributions by training community health workers to educate households on proper net use and care of nets during bed net delivery and installation activities [54].
Malaria Consortium included two particular projects that contained components of bed net care and repair education. The Pioneer Project conducted from 2009 to 2014 in Uganda promoted the message to ‘Dry your net under the shade after washing it’ though net care was not a main focus of BCC activities [55]. Interviews and focus groups discussions from The Malaria Prevention and Control Project in Mozambique from 2011 to 2017 discussed exposure to net care and repair messaging during a LLIN distribution 6 months prior [56]. Participants had high awareness that net care and repair is important and good recall of messages to repair torn or damaged nets, but the accurate recall of other care recommendations was inconsistent [56]. Specifically, respondents did not know appropriate net washing locations (in the river vs. a washtub or bucket) or whether nets should be dried in the shade or sun [56].
Discussion
Education interventions resulted in improvements in bed net care and repair knowledge and/or practices in less than half of all included peer-reviewed articles (n = 13, 44.8%) and in eight (50%) of the articles with an education intervention as a main study component. Interventions that received three stars in the quality assessment included an appropriately selected comparison group, be grounded in theory, and use equitable instructional activities (Appendix 2). Evaluation of education intervention effectiveness is discussed¸ including assessment of theoretical grounding, education strategies and methods, and the implications on net durability and longevity.
Theoretical grounding
Theory based health education interventions are considered more effective than non-theory based interventions [21] because they outline the rationale and process for how the intervention will result in change [57]. However, we found no differences in success between interventions grounded in theory and those that did not mention theory.
Interventions that were informed by or applied theory achieved varied net care and repair results. Though there were only two interventions that built or built upon theory, both resulted in positive care and repair outcomes. Building or building upon theory may be the most successful way to implement education interventions because it requires detailed context-specific knowledge of the target populations, as care and repair practices are known to vary by community [12]. However, a larger evidence base is needed to determine how utilizing health behavior theory influences the success of education interventions aimed at improving bed net care and repair practices. The wide variety of theories utilized potentially obfuscates the relationship between theory and intervention effectiveness. No two articles used the same theory, which is not surprising, given the large number of health behavior theories available. As of the 1990s, 66 health behavior theories and models were found among 536 articles to inform education intervention designs [58], and more theories and models are continually developed for differing health contexts such as the net care and repair conceptual framework [38] utilized by Helinski et al [37].
Education
Comparison groups
It is difficult to synthesize the effectiveness of education interventions on changing knowledge or behaviors among studies that do not adequately describe the selection of appropriate comparison groups. In particular, exposure misclassification may impact observed intervention outcomes if comparison groups are contaminated with intervention messaging. Without clear descriptions of comparison groups, it becomes difficult to judge if message contamination influenced outcomes. Some studies attempt to measure contamination. Interventions that used passive mass education methods surveyed respondents on exposure to specific intervention slogans [37,38]. Additionally, some studies purposefully select control or comparison groups to limit the possibility of contamination. Amoran et al. randomly selected intervention and control sites in geographically separated areas [30]. Helinksi et al. chose culturally similar, but geographically separated sites where the populations spoke different languages [37], and Koenker et al. chose a control site that was culturally similar to the intervention site, but that was outside of the range of broadcasting services [38]. Further evidence of intervention effectiveness could be obtained through demonstrating temporality, dose-response relationships between behavior change and exposure to education activities, and methods to minimize effects of non-randomization [59].
Descriptions of instructional strategies
Interventions receiving three stars in the quality assessment detailed replicable descriptions of the instructional strategies that were implemented; however, they still lacked a framework for the actual provision of the instructional events. Health education interventions are inherently multidisciplinary, often requiring expertise in public and global health, health promotion, and anthropology, yet they appear to lack involvement of experts in education – those that understand and apply learning theories and instructional frameworks. Of the articles with malaria education as a main focus (Table 4), only three indicate author affiliations with individuals outside of public health, medical, and anthropology realms including one author from a humanities department [31] and authors from a center for communication programs [37,38]. In 2005, Kinzie linked health behavior theories and instructional frameworks specifically to provide instructional design strategies for health educators [24], but this resource was not referenced by any of the articles in Table 3. Though not related to net care and repair, one intervention that aimed to improve malaria knowledge among travelers explicitly utilized learning theory to develop an educational game that resulted in significant knowledge improvements [60]. More emphasis should be placed on the learning process for differing audiences (whether across varied geographical areas, different levels of learners, or differing cultural contexts) in designing and implementing malaria education interventions, particularly interventions that educate through interpersonal communication.
Types of instructional strategies
Though not explicitly defined as such, the interventions receiving three stars employed equitable educational activities, meaning activities accessible to diverse learners. This follows a principle of universal design for instruction which is often discussed among post-secondary educators [61], but is applicable to all instructional settings. Offering various ways of delivering educational content allows information to be accessible to multiple types of learners [61]. In the context of BCC campaigns, this means using various messaging tactics including visual, auditory, and interpersonal communication strategies to send a unified message. For example, one intervention employed only one mode of education (auditory messages during sermons) [34] while other interventions combined multiple instructional activities such as flipbooks, radio messaging, posters, and drama performances [25,26,28,30–33,35-38]. A review of malaria social and behavior change communication campaigns concluded that interventions using multiple activities, increased the likelihood of resulting behavior change [62]. Providing multiple types of educational activities is particularly important in areas with disparities in literacy rates. Written materials along with other visual and auditory methods can ensure that populations with varying literacy levels are exposed to the same messaging in a way they can best learn.
Overall educational methods
Interventions reached target populations using mass education, interpersonal education, or a combination of the two. It is likely using a combination of mass and interpersonal strategies is most effective, as all five interventions using a combination reported positive (four studies) or mixed (one study) care and repair results [25,32,33,37,38]. There was no discernable pattern of care and repair conclusions among interventions that used only mass or interpersonal education methods, however, these conclusions are tenuous due to the small sample size of interventions.
Comparing care and repair results across interventions is further complicated because implementation of education exposure differs between passive mass, active mass, and interpersonal education methods. Passive mass education is the easiest to implement consistently, while more variation dependent on the individuals providing instruction is expected with active mass and interpersonal education. Rhee et al. implemented interpersonal education to increase the proportion of retreated ITNs, but obtained mixed results where more individuals who received education retreated ITNs, but there was no difference between intervention and control households in the number that retreated nets [27]. A potential explanation for weak results was found due to interaction in retreatment outcomes depending on the field guide who implemented the education even though all guides received the same training [27]. Interventions using individuals to provide instruction should have ensure training in education theory and instructional strategies to obtain the greatest possible effectiveness and highest possible degree of consistency between educators. For example, a school based education intervention that improved ITN retreatment practices in Ghana [33] specifically trained instructors in Participatory Learning and Action (PLA), an evidence-based facilitated approach that actively engages participants in the targeted interventions [63].
Comprehensive versus single message education
There is a lack of comprehensive care and repair messaging among both education interventions and bed net distributions. Ten (63%) of the articles with malaria education as a main component addressed only a single care and repair practice, 3 (18.8%) educated on 2–3 practices, and only three (18.8%) interventions educated on four or more practices. Though four interventions focused on net storage during the day (important for preventing holes and maintaining net integrity), very few interventions provided education on LLIN care behaviors most influential for maintaining insecticide effectiveness (soap type and drying location). Nine of the interventions in Table 4 focused on ITN treatment or retreatment, which are practices no longer relevant for LLINs. This lack of comprehensive care messaging and lack of LLIN-specific interventions make it very difficult to conclude that education interventions are effective in improving net care knowledge and practices.
Additionally, very few of the included interventions were solely focused on improving care and repair knowledge and/or practices. Most interventions were concerned with other outcomes such as improving net use, thus care and repair education was a relatively minor priority. There was also a serious lack of specificity in net care education of distributions funded by the Against Malaria Foundation. In fact, 86.7% of distribution reports described no care and repair messaging or very general messaging described on as ‘net care’ or ‘net maintenance’ (Figure 3). To achieve maximal improvements in net longevity and durability, comprehensive education interventions dedicated to improving care and repair practices are needed, and net distribution campaigns should ensure that care and repair messaging is consistent and comprehensive. One such intervention that focused on net care and repair knowledge and practices incorporated comprehensive messaging and resulted in improved care and repair knowledge, practices, and net longevity [38], suggesting that education interventions can lead to promising results, though more evidence is needed.
Impacts on bed net durability and longevity
While education interventions led to marginal improvements in knowledge and practices, there is little evidence that these improvements improved net durability and longevity, largely because only three studies measured bed net durability as an outcome. One found that education increased care and repair knowledge and attitudes, but did not improve net durability [37] and one found that repair practices significantly increased, but did not improve net condition [35]. The other found that nets tied up while not in use were more likely to be in serviceable condition at follow up [38]. More education interventions of bed net care and repair that measure net durability as an outcome are needed. Future interventions should be conducted through LLIN distributions before nets are used to demonstrate an effect between bed net care and repair education and improved net durability and longevity. Furthermore, more emphasis on net care education should be placed on net distributions funded by non-governmental organizations (NGOs) such as the Against Malaria Foundation (AMF) to ensure all net recipients are receiving complete and accurate net care recommendations. When an organization wishes to implement a net distribution funded by AMF, they are required to provide plans for educational components of the distribution [53]. However, this requirement is vague and does not specify particular content that should be conveyed. This lack of specificity resulted in no mention of any education plans or education conducted regarding net care or repair in more than half of the 136 completed distributions (Figure 3).
Limitations
The search terms ‘Plasmodium’ and ‘Anopheles’ were not included in the search strategies, and thus could have resulted in missed records. However, this is likely a minor issue considering the volume of records assessed from a wide variety of databases. Due to the variety of study designs of the included interventions, the quality assessment used was not a standardized or validated assessment tool. Rather, it is a way to highlight important elements of education interventions and should be evaluated as a description rather than a judgment. We transparently reported the scoring of each included study so that readers can evaluate our decision and make their own judgments (Supplemental Table 1).
Conclusions and recommendations
It is difficult to make strong conclusions regarding the efficacy of education interventions on improving net care and repair knowledge, practices, or durability as most of the included interventions educated on care and repair as a secondary or minor objective. We did not find evidence that interventions grounded in health behavior theory achieved more positive results than those not grounded in theory. Interventions that employed both mass and interpersonal education showed promising results that warrant further investigation.
For increased rigor and comparability of future education interventions, we recommend the following:
Because education interventions on care and repair practices must be highly context-specific, a focus on training instructors in pertinent education theory and appropriate instructional strategies may help improve education quality and consistency to yield stronger results.
Interventions should be planned, monitored, evaluated, and reported using guidance put forth by the RBM working group. There is a wealth of material freely available including standardized indicators, survey development guidance, and checklists to ensure complete reporting [57,64–65].
Funding Statement
This work was not supported by any funding mechanisms.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- [1].Burkot TR, Garner P, Paru R, et al. Effects of untreated bed nets on the transmission of Plasmodium falciparum, P. vivax and Wuchereria bancrofti in Papua New Guinea. Trans R Soc Trop Med Hyg. 1990;84:773–779. [DOI] [PubMed] [Google Scholar]
- [2].Alonso PL, Lindsay SW, Armstrong JRM, et al. The effect of insecticide-treated nets on mortality of Gambian children. Lancet. 1991;337:1499–1502. [DOI] [PubMed] [Google Scholar]
- [3].Lengeler C. Insecticide-treated nets for malaria control: real gains. Bull WHO. 2004;82(2):84. [PMC free article] [PubMed] [Google Scholar]
- [4].Binka FN, Indome F, Smith T.. Impact of spatial distribution of permethrin-impregnated bed nets on child mortality in rural northern Ghana. Am J Trop Med Hyg. 1998;59:80–85. [DOI] [PubMed] [Google Scholar]
- [5].Howard SC, Omumbo J, Nevill C, et al. Evidence for a mass community effect of insecticide-treated bednets on the incidence of malaria on the Kenyan coast. Trans R Soc Trop Med Hyg. 2000;94:357–360. [DOI] [PubMed] [Google Scholar]
- [6].Gosoniu L, Vounatsou P, Tami A, et al. Spatial effects of mosquito bednets on child mortality. BMC Public Health. 2008;8:356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Fraser-Hurt N, Lyimo EO. Insecticide-treated nets and treatment service: a trial using public and private sector channels in rural United Republic of Tanzania. Bull World Health Organ. 1998;76(6):607–615. [PMC free article] [PubMed] [Google Scholar]
- [8].World Health Organization . 2002. Instructions for treatment and use of insecticide-treated mosquito nets. WHO/CDS/RBM/2002.41.
- [9].Vestergaard . 2014. PermaNet 2.0. [cited 2019 May11]. Available from: <https://www.vestergaard.com/permanet-2-0>
- [10].Shirayama Y, Phompida S, Kuroiwa C, et al. Maintenance behaviour and long-lasting insecticide-treated nets (LLITNs) previously introduced into Bourapar district, Khammouane province, Lao PDR. J Public Health. 2007;121:122–129. [DOI] [PubMed] [Google Scholar]
- [11].NetWorks Summary Series . ITN care & repair: improving net lifespan through behavior change communication. United States Agency for International Development. Baltimore, MD: Johns Hopkins University; 2015. [Google Scholar]
- [12].Gnanguenon V, Azondekon R, Oke-Agbo F, et al. Durability assessment results suggest a serviceable life of two, rather than three, years for the current long-lasting insecticidal (mosquito) net (LLIN) intervention in Benin. BMC Infect Dis. 2014;14. DOI: 10.1186/1471-2334-14-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Azondekon R, Gnanguenon V, Oke-Agbo F, et al. A tracking tool for long-lasting insecticidal (mosquito) net intervention following a 2011 national distribution in Benin. Parasit Vector. 2014;7:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Loll DK, Berthe S, Faye SL, et al. “You need to take care of it like you take care of your soul”: perceptions and behaviors related to mosquito net damage, care, and repair in Senegal. Malar J. 2014;13:322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Hunter GC, Scandurra L, Acosta A, et al. We are supposed to take care of it: A qualitative examination of care and repair behaviour of long-lasting, insecticide-treated nets in Nasarawa State, Nigeria. Mal J. 2014;13. DOI: 10.1186/1475-2875-13-320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Mutuku FM, Khambira M, Bisanzio D, et al. Physical condition and maintenance of mosquito bed nets in Kwale County, coastal Kenya. Malar J. 2013;12:46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Leonard L, Diop S, Doumbia S, et al. Net use, care and repair practices following a universal distribution campaign in Mali. Mal J. 2014;13. DOI: 10.1186/1475-2875-13-435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Scandurra L, Acosta A, Koenker H, et al. “It is about how the net looks”: a qualitative study of perceptions and practices related to mosquito net care and repair in two districts of eastern Uganda. Mal J. 2014;13:504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Wills AB, Smith SC, Anshebo GY, et al. Physical durability of PermaNet 2.0 long lasting insecticidal nets over three to 32 months of use in Ethiopia. Mal J. 2013;12:242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Michie S, Abraham C, Eccles MP, et al. Strengthening evaluation and implementation by specifying components of behaviour change interventions: a study protocol. Implement Sci. 2011;6:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Ann Rev Public Health. 2010;31:399–418. [DOI] [PubMed] [Google Scholar]
- [22].Painter JE, Borba CP, Hynes M, et al. The use of theory in health behavior research from 2000-2005: a systematic review. Ann Behav Med. 2008;35:358–362. [DOI] [PubMed] [Google Scholar]
- [23].Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Kinzie MB. Instructional design strategies for health behaviour change. Patient Ed Couns. 2005;56:3–15. [DOI] [PubMed] [Google Scholar]
- [25].Marsh VM, Mutemi W, Some ES, et al. Evaluating the community education programme of an insecticide-treated bed net trial on the Kenyan coast. Health Policy Plan. 1996;11(3):280–291. [DOI] [PubMed] [Google Scholar]
- [26].Minja H, Schellenberg JA, Mukasa O, et al. Introducing insecticide-treated nets in the kilombero Valley, Tanzania: the relevance of local knowledge and practice for an information, education and communication (IEC) campaign. Trop Med Int Health. 2001;6(8):614–623. [DOI] [PubMed] [Google Scholar]
- [27].Rhee M, Sissoko M, Perry S, et al. Use of insecticide-treated nets (ITNs) following a malaria education intervention in Piron, Mali: a control trial with systematic allocation of households. Malar J. 2005;4:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Rickard DG, Dudovitz RN, Wong MD, et al. Closing the gap between insecticide treated net ownership and use for the prevention of malaria. Prog Community Health Partnersh. 2011;5(2):123–131. [DOI] [PubMed] [Google Scholar]
- [29].Ahmadi M, Vatandoost H, Shaeghi M, et al. Effects of educational intervention on long-lasting insecticidal nets use in a malarious area, southeast Iran. Acta Med Iran. 2012;50(4):279‐287. [PubMed] [Google Scholar]
- [30].Amoran OE, Fatugase KO, Fatugase OM, et al. Impact of health education intervention on insecticide treated nets uptake among nursing mothers in rural communities in Nigeria. BMC Res Notes. 2012;5:444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Alvarado BE, Gomez E, Serra M, et al. Evaluación de una estrategia educativa en malaria aplicada en localidades rurales del Pacífico colombiano. Biomedica. 2006;26(3):342–352. [PubMed] [Google Scholar]
- [32].Nonaka D, Kobayashi J, Jimba M, et al. Malaria education from school to community in Oudomxay province, Lao PDR. Parasitol Int. 2008;57:76–82. [DOI] [PubMed] [Google Scholar]
- [33].Ayi I, Nonaka D, Adjovu JK, et al. School-based participatory health education for malaria control in Ghana: engaging children as health messengers. Malar J. 2010;9:98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Mfaume MS, Winch PJ, Makemba AM, et al. Mosques against malaria. World Health Forum. 1997;18(1):35–38. [PubMed] [Google Scholar]
- [35].Panter-Brick C, Clarke SE, Lomas H, et al. Culturally compelling strategies for behaviour change: a social ecology model and case study in malaria prevention. Soc Sci Med. 2006;62(11):2810–2825. [DOI] [PubMed] [Google Scholar]
- [36].Harvey SA, Olórtegui MP, Leontsini E, et al. Trials of improved practices (TIPs): A strategy for making long-lasting nets last longer? Am J Trop Med Hyg. 2013;88:1109–1115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Helinski MH, Namara G, Koenker H, et al. Impact of a behaviour change communication programme on net durability in eastern Uganda. Mal J. 2015;14. DOI: 10.1186/s12936-015-0899-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Koenker H, Kilian A, Hunter G, et al. Impact of a behaviour change intervention on long-lasting insecticidal net care and repair behaviour and net condition in Nasarawa State, Nigeria. Malar J. 2015;14:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Widmar M, Nagel CJ, Ho DY, et al. Determining and addressing obstacles to the effective use of long-lasting insecticide-impregnated nets in rural Tanzania. Malar J. 2009;8:315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Ho D. An approach to achieve sustainable bed-net use in rural Tanzania. (1509713). Ann Arbor: Mount Sinai School of Medicine; 2012. [Google Scholar]
- [41].Alonso PL, Lindsay SW, Armstrong Schellenberg JR, et al. A malaria control trial using insecticide-treated bed nets and targeted chemoprophylaxis in a rural area of The Gambia, west Africa. 2. Mortality and morbidity from malaria in the study area. Trans R Soc Trop Med Hyg. 1993;87(Suppl 2):13–17. [DOI] [PubMed] [Google Scholar]
- [42].Brieger W, Onyido A, Sexton J, et al. Monitoring community response to malaria control using insecticide-impregnated bed nets, curtains and residual spray at Nsukka, Nigeria. Health Educ Res. 1996;11(2):133‐145. Retrieved from: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-00183839/full [DOI] [PubMed] [Google Scholar]
- [43].Khadka A, Perales NA, Wei DJ, et al. Malaria control across borders: quasi-experimental evidence from the trans-kunene malaria initiative (TKMI). Malar J. 2018;17(1):224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Kachur SP, Phillips-Howard PA, Odhacha AM, et al. Maintenance and sustained use of insecticide-treated bednets and curtains three years after a controlled trial in western Kenya. Trop Med Int Health. 1999;4(11):728–735. [DOI] [PubMed] [Google Scholar]
- [45].Snow RW, McCabe E, Mbogo CN, et al. The effect of delivery mechanisms on the uptake of bed net re-impregnation in Kilifi District, Kenya. Health Policy Plan. 1999;14(1):18–25. [DOI] [PubMed] [Google Scholar]
- [46].Wacira DG, Hill J, McCall PJ, et al. Delivery of insecticide-treated net services through employer and community-based approaches in Kenya. Trop Med Int Health. 2007;12(1):140–149. [DOI] [PubMed] [Google Scholar]
- [47].Fernando SD, Abeyasinghe RR, Galappaththy GN, et al. Community factors affecting long-lasting impregnated mosquito net use for malaria control in Sri Lanka. Trans R Soc Trop Med Hyg. 2008;102(11):1081–1088. [DOI] [PubMed] [Google Scholar]
- [48].Cham MK, D’Alessandro U, Todd J, et al. Implementing a nationwide insecticide-impregnated bednet programme in The Gambia. Health Policy Plan. 1996;11(3):292–298. [DOI] [PubMed] [Google Scholar]
- [49].Hiwat H, Hardjopawiro LS, Takken W, et al. Novel strategies lead to pre-elimination of malaria in previously high-risk areas in Suriname, South America. Malar J. 2012;11:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Gerstl S, Dunkley S, Mukhtar A, et al. Long-lasting insecticide-treated net usage in eastern Sierra Leone - the success of free distribution. Trop Med Int Health. 2010;15(4):480–488. [DOI] [PubMed] [Google Scholar]
- [51].Ahmed SM, Hossain S, Kabir MM, et al. Free distribution of insecticidal bed nets improves possession and preferential use by households and is equitable: findings from two cross-sectional surveys in thirteen malaria endemic districts of Bangladesh. Malar J. 2011;10:357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Alaii J, Van DBH, Kachur S, et al. Perceptions of bed nets and malaria prevention before and after a randomized controlled trial of permethrin-treated bed nets in western Kenya. Am J Trop Med Hyg. 2003;68(4 Suppl):142‐148. [PubMed] [Google Scholar]
- [53].Against Malaria Foundation . 2019. Distributions. [cited 2019 May11]. Available from: <https://www.againstmalaria.com/Distributions.aspx?MapID=1&StatusID=7>
- [54].Caviness C, Gish A. Five ways the united methodist church has impacted malaria. Imagine No Malaria.[cited 2019 March14] Available from: http://umc.org/how-we-serve/five-ways-the-united-methodist-church-has-impacted-malaria
- [55].Malaria Consortium . Pioneer project 2009-2014: a holistic systems strengthening approach towards malaria control in mid-western Uganda. Successes and lessons. 2014.
- [56].Malaria Consortium . 2018. Nets bring good health: a qualitative inquiry into mosquito net use and care practices in two northern provinces of mozambique. London, United Kingdom; [cited 2019 March14]. Available from: <www.malariaconsortium.org> [Google Scholar]
- [57].The RBM Partnership to End Malaria . The strategic framework for malaria social and behavior change communication 2018-2030. Venier, Switzerland: RBM; 2018. [Google Scholar]
- [58].Glanz K, Lewis FM, Rimer BK. Linking theory, research, and practices. In: Glanz K, Lewis FM, Rimer BK, editors. Health behavior and health education. 2nd ed. San Francisco: Jossey-Bass; 1997. p. 3–18. [Google Scholar]
- [59].RBM Partnership to End Malaria . The art of asking questions: priority research areas and approaches for malaria social and behavior change programs. Venier, Switzerland: RBM; 2019. [Google Scholar]
- [60].Hartjes LB. The development and evaluation of a malaria risk-reduction game for travelers. (3448913). Ann Arbor: The University of Wisconsin - Madison; 2010. [Google Scholar]
- [61].Burgstahler S. Universal design for instruction (UDI): definition, principles, guidelines, and examples. Seattle, WA: University of Washington; 2009. [Google Scholar]
- [62].The Health Communication Capacity Collaborative (HC3) . Malaria SBCC evidence literature review. Baltimore, Maryland: Johns Hopkins Center for Communication Programs; 2017. [Google Scholar]
- [63].Thomas S. What is participatory learning and action (PLA): an introduction. London: Centre for International Development and Training (CIDT); 2004. [Google Scholar]
- [64].RBM Partnership to End Malaria . Malaria social and behavior change communication indicator reference guide: second edition. Venier, Switzerland: RBM; 2017. [Google Scholar]
- [65].RBM Partnership to End Malaria . Developing M&E plans for malaria social and behavior change programs: a step-by-step guide. Venier, Switzerland: RBM; 2019. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Citations
- Vestergaard . 2014. PermaNet 2.0. [cited 2019 May11]. Available from: <https://www.vestergaard.com/permanet-2-0>
- Against Malaria Foundation . 2019. Distributions. [cited 2019 May11]. Available from: <https://www.againstmalaria.com/Distributions.aspx?MapID=1&StatusID=7>
- Caviness C, Gish A. Five ways the united methodist church has impacted malaria. Imagine No Malaria.[cited 2019 March14] Available from: http://umc.org/how-we-serve/five-ways-the-united-methodist-church-has-impacted-malaria