

Abstract
Various technical tips have been described on the placement of poller screws during intramedullary (IM) nailing; however studies reporting outcomes are limited. Overall there is no consistent conclusion about whether intramedullary nailing alone, or intramedullary nails augmented with poller screws is more advantageous.
We conducted a systematic review of PubMed, EMBASE, and Cochrane databases. Seventy-five records were identified, of which 13 met our inclusion criteria. In a systematic review we asked: (1) What is the proportion of nonunions with poller screw usage? (2) What is the proportion of malalignment, infection and secondary surgical procedures with poller screw usage? The overall outcome proportion across the studies was computed using the inverse variance method for pooling.
Thirteen studies with a total of 371 participants and 376 fractures were included. Mean follow-up time was 21.1 months. Mean age of included patients was 40.0 years. Seven studies had heterogenous populations of nonunions and acute fractures. Four studies included only acute fractures and two studies examined nonunions only.
The results of the present systematic review show a low complication rate of IM nailing augmented with poller screws in terms of nonunion (4%, CI: 0.03–0.07), coronal plane malunion (5%, CI: 0.03–0.08), deep (5%, CI: 0.03–0.11) and superficial (6%, CI: 0.03–0.11) infections, and secondary procedures (8%, CI: 0.04–0.18).
When compared with the existing literature our review suggests intramedullary nailing with poller screws has lower rates of nonunion and coronal malalignment when compared with nailing alone. Prospective randomized control trial is necessary to fully determine outcome benefits.
Cite this article: EFORT Open Rev 2020;5:189-203. DOI: 10.1302/2058-5241.5.190040
Keywords: poller screw, review
Introduction
Tibial and/or fibular shaft fractures accounted for approximately 17% of all lower limb fractures in a population-based study of 32,900 patients in the United Kingdom, with femoral fractures (excluding neck of femur) accounting for 8.7% making these a significant clinical problem.1 In recent years, closed reduction with minimally invasive plating and locked intramedullary nailing have both become widely used treatment modalities for proximal and distal tibial metaphyseal fractures.2–4
Gerhard Küntscher is credited with the invention of intramedullary nail fixation in 1939 for femur fractures. Modny and Bambara introduced locked intramedullary (IM) nails5 which were able to control length and rotation especially in the mid-diaphyseal region. Intra-medullary nailing is the preferred choice of operative management of diaphyseal factures of the lower limb and is also part of the armamentarium for the treatment of metaphyseal fractures. There are limitations with the ‘standard’ practice of IM nailing in the treatment of metaphyseal fractures owing to the long lever arm, metaphyseal enlargement, and epiphyseal–metaphyseal fixation problems, which make reduction and controlling angulation of the shorter bone fragment technically difficult.6,7 This can result in malalignment, malunion, and pain.6–9
The term blocking screw was first introduced by Donald and Seligson in 1983 – as they ‘block’ the nail from malreducing the fracture.10 Krettek et al introduced the term ‘poller screws’. The term ‘poller’ is derived from small metal bollards designed to block or guide traffic. These poller screws functionally decrease the width of the medullary cavity, physically block the nail to assist with reduction, resist displacing muscular forces in the mobile distal fragment, and increase the mechanical stiffness of the bone-implant construct.11 When compared with other techniques described for preventing metaphyseal malalignment during nailing, blocking screws are technically easy and reproducible, they do not require special instrumentation or hardware and there is no need for excessive soft tissue dissection.12 Data on the overall incidence of poller screw utilization are unclear from the literature; however, anecdotally, poller screws are used by experienced surgeons in large trauma centres rather than trainees surgeons. The paucity of articles on poller screws and small patient numbers further supports this. Deciding on the location and the number of blocking screws is often difficult and confusing, with at least four ‘rules’ described in the literature.13–16 Fig. 1 shows fluoroscopic images of the placement of poller screws in a diaphyseal tibial fracture. Fig. 2 details technical tips for the placement of poller screws from experience in our tertiary centre.
Fig. 1.

Fluoroscopic images of the placement of poller screws in a diaphyseal tibial fracture. (A) Displaced comminuted diaphyseal tibial fracture. (B) Intraoperative fluoroscopic (Anterior Posterior) AP image showing placement of two poller screws in the coronal plane (one in the distal and one in the proximal fragment). (C) Distal poller screw placed at the site of comminution very close to fracture line is removed and placed more distally. (D) Guidewire placement: guidewire deflected by poller screws. (E) Lateral image of reamer passing distal poller screw. (F) AP image of reamer passing distal poller screw.
Fig. 2.
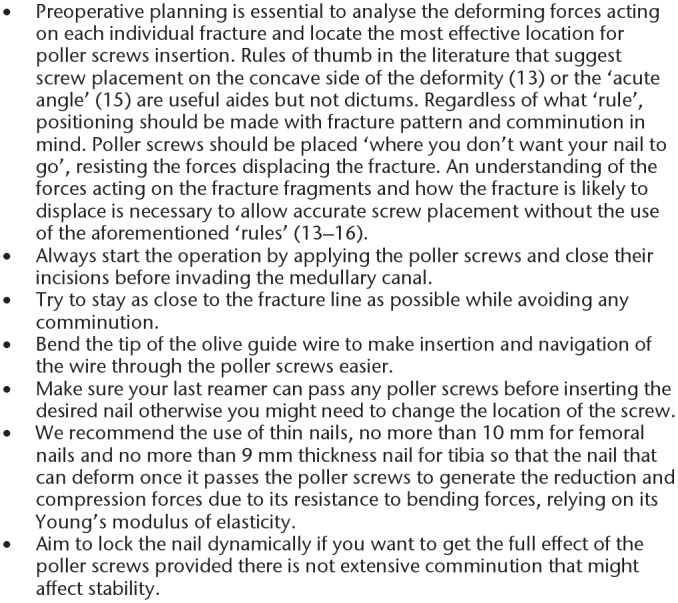
Technical tips for the placement of poller screws.
While technical tips are well described in the literature, outcomes of the treatment of metaphyseal fractures treated with poller screws are limited. Overall, there is no consistent conclusion about whether IM nailing alone, or the method of using IM nails with poller screws is more advantageous as there is a paucity of data comparing the efficacy of the latter treatment. Therefore, we conducted this systematic review to provide more comprehensive and reliable evaluations of the outcomes following poller screw treatments for metaphyseal fractures and nonunions.
Methods
Protocol and registration
This systematic review and metaanalysis was planned, conducted, and reported according to the guidelines of the PRISMA statement. A study protocol was registered with PROSPERO (137490) prior to data abstraction and analysis.
Systematic literature review
A PRIMSA-compliant systematic literature review was conducted. The authors searched the EMBASE, MEDLINE and Cochrane databases for terms “poller screw” OR “blocking screw” in the title and/or abstract published prior to June 2019. In addition, a manual search was also performed for additional literature in print format. Reference lists from published original articles and previous reviews were scanned for additional relevant studies.
Study eligibility
We considered studies in any language featuring a population with fractures or nonunions who had undergone intramedullary nailing with poller screw augmentation and measured radiographic outcomes.
Inclusion criteria:
Studies involving poller screws.
Studies reporting union and complications.
Exclusion criteria:
Case reports, studies detailing technique only, conference abstracts, review articles, letters to the editor.
Studies using IM nailing for limb lengthening or arthrodesis.
Primary outcome: Radiological union.
Secondary outcomes: Complications including nonunion, malalignment, delayed union, pain, infection.
Study selection
Management of the search results was carried out in Covidence Systematic Review Software (www.covidence.org). Two reviewers (MT and AA) worked independently and in duplicate, screened all titles and abstracts to determine inclusion. In the event of disagreement or insufficient information in the abstract, the full text was reviewed, again independently and in duplicate. We resolved conflicts by consensus. The initial search retrieved 75 studies. After automated removal of duplicates by Covidence, 65 titles and abstracts were examined and 27 articles were short-listed. After full text review of the short-listed papers, 13 studies were identified as suitable. The search protocol is summarized in the PRISMA flow diagram (Fig. 3).
Fig. 3.
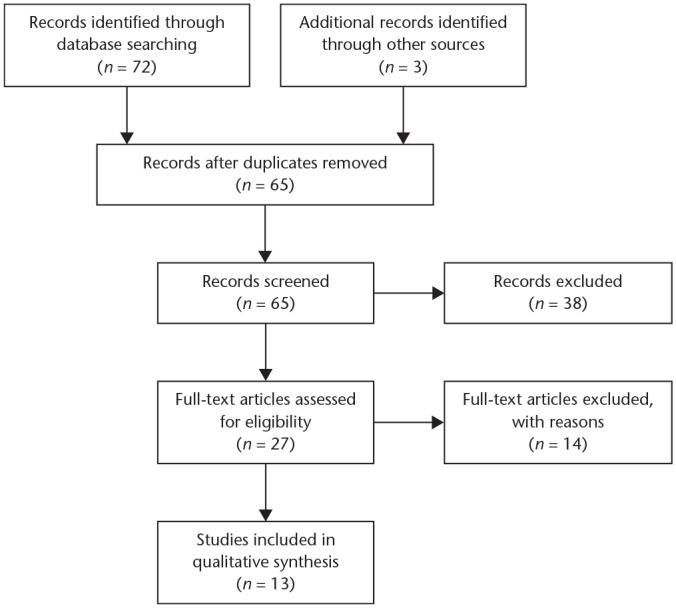
PRISMA flowchart.
Data extraction
Table 1 details the demographic data extracted from the identified articles. Table 2 details the number and position of the poller screws used. The outcome measures reported by each study are detailed in Table 3. The following outcome parameters were extracted and analysed:
Table 1.
Description of studies and demographic characteristics
| Study | Year | Country | Study design | Number of participants | Comparison group | Average age (years) | Inclusion | Exclusion | Fracture classification (type, numbers) |
|---|---|---|---|---|---|---|---|---|---|
| Ricci et al19 | 2001 | USA | Case series (prospective) | 12 (four had been previously treated with IM tibial nailing for proximal tibia fractures and were thought to be unacceptably aligned) | No | 47 | Extraarticular fractures of the proximal third of the tibial shaft. | None | OTA classification (42A, 4; 42B, 7; 42C, 1) |
| Moongilpatti Sengodan et al12 | 2014 | India | Case series (prospective) | 20 | No | 37.75 | Displaced distal tibial metaphyseal fractures (acute fractures and delayed union). Both open and closed fractures were included in the study. | Tibial diaphyseal and proximal tibial metaphyseal fractures. Metaphyseal fractures treated with statically locked intramedullary nails but with additional procedures such as fibular plating. | AO classification (43 A1, 5; 43 A2, 11; 43 A3, 4) |
| Krettek et al11 | 1999 | Germany | Case series (prospective) | 21 fractures in 20 patients | No | 44 | Displaced fractures of the proximal or distal third tibia which were either extraarticular or had a non-displaced intraarticular extension. | None | AO classification (A, 5; B, 9; C, 7) |
| Seyhan et al24 | 2013 | Turkey | Case series (retrospective) | 15 | No | 38.8 | Distal diaphyseal or metaphyseal fracture of femur. Acute fracture only. |
None | AO classification (A, 13; B, 1; C, 1) |
| Seyhan et al20 | 2012 | Turkey | Case series (retrospective) | 21 | No | 41.4 | Distal tibial diaphyseal or metaphyseal extra articular fractures and received blocking screw and intramedullary nail treatment. Acute fracture only. |
None | AO classification (A, 19; B, 2) |
| Kim et al31 | 2018 | Korea | Case series (retrospective) | 10 treated with poller screws* | No | 46.8 | Infraisthmal femoral shaft fracture treated with exchange nailing with a poller screw for nonunion. | None | AO classification (A, 8; B, 2) |
| Kulkarni et al21 | 2012 | India | Case series (retrospective) | 75 fractures 70 patients | No | 33 | IMN supplemented with poller screws for fractures (n = 60) or for delayed union (n = 10) or malalignment (n = 5) of the proximal metadiaphyseal tibia. | Tibial fractures with the proximal fragment < 7 cm, proximal intraarticular tibial fractures, or non-displaced fractures were excluded. | AO classification (A, 50; B, 15; C, 10) |
| Van Dyke et al29 | 2018 | USA | Case series (retrospective) | 46 treated with blocking screws | Yes – RIMN without poller screws | 38.6 | All patients with an infraisthmal femur fracture treated with a RIMN. Acute fracture only. |
Skeletally immature patients, pathologic fractures, and patients without sufficient radiographic follow-up. |
AO classification (31A, 10; 32B, 12; 32C, 16; 33 All; 8) |
| Seyhan et al26 | 2012 | Turkey | Case series (retrospective) | 12 treated with blocking screws | Yes – Comparison of reduction with clamp vs cerclage vs blocking screw | 47.9 | Subtrochanteric femoral fractures treated with IMN. Acute fracture only. |
None | Seinsheimer (2A, 2; 2B, 3; 3B, 7) |
| Shah et al27 | 2015 | Nepal | Case series (retrospective) | 60 | No | 34 | Extraarticular, displaced fractures of the proximal (n = 24) or distal (n = 36) third of tibia. | None | AO classification (A, 15; B, 27; C, 18) |
| Bhangadiya et al22 | 2016 | India | Case series (retrospective) | 50 | No | 35 | Metadiaphyseal tibia fractures. | Intraarticular fractures of proximal and distal tibia, non-displaced and those who were treated conservatively, and who were medically unfit were excluded from the study. | AO classification (A, 38; B, 7; C, 5) |
| Gao et al28 | 2009 | China | Case series (retrospective) | 12 | No | 35.6 | Diaphyseal nonunion in the femur (n = 5) and tibia (n = 7). | None | AO classification (A, 4; B, 7; C, 1) |
| Song23 | 2019 | South Korea | Case series (retrospective) | 23 | Yes – Comparison with 26 patients who underwent IM nailing without poller screws | 39.2 | Infraisthmal acute femur-shaft fractures treated with antegrade nailing with or without poller blocking screws. | Pathologic fractures, bisphosphonate-related atypical fractures, adolescent patients, deep intramedullary infection cases, and patients for whom there were insufficient available radiographs until union. | AO classification (32A, 8; 32B, 10; 32C, 5) |
Note. IM, intramedullary; IMN, intramedullary nail; OTA, Orthopaedic Trauma Association; RIMN, Retrograde Intramedullary Nail.
Kim paper data presented here are the averaged raw data for the 10 patients treated with poller screws, not the entire cohort.
Table 2.
Number and position of poller screws
| Study | Number of poller screws | Additional information on placement | ||
|---|---|---|---|---|
| 1 (no. of patients) | 2 (no. of patients) | 3 (no. of patients) | ||
| Ricci et al19 | 9 | 3 | 0 | Of the patients with two poller screws; two patients had posterior and lateral screws and one patient had two medial screws. |
| Moongilpatti Sengodan et al12 | 9 | 11 | In seven cases single blocking screws were used on the concave side of the deformity, close to the fracture site in the short fragment. In two cases single blocking screws were used on the convex side of the deformity, near the end of the nail. In the remaining cases two blocking screws were placed, the first one on the concave side of the deformity close to the fracture site and the second screw on the convex side of deformity near the end of the nail in the distal fragment. | |
| Krettek et al11 | 13 | 6 | 2 | In 13 fractures a single poller screw was used, placed on the concave side of the deformity. |
| Seyhan et al24 | 13 | 2 | 0 | Only two patients had two poller screws used (one in the sagittal and one in the coronal). |
| Seyhan et al20 | 20 | 1 | 0 | 18 medial, two posterior, one medial and anterior (both planes). |
| Kim et al31 | 2 | 6 | 2 | – |
| Kulkarni et al21 | 45 | 27 | 3 | When a single poller screw was used it was placed on the concave side of the deformity. |
| Van Dyke et al29 | 33 | 12 | 0 | All screws were in the coronal plane. |
| Seyhan et al26 | 12 | 0 | 0 | All patients had a single poller screw used to aid reduction in this arm of the study. |
| Shah et al27 | – | – | – | – |
| Bhangadiya et al22 | 38 | 7 | 0 | – |
| Gao et al28 | – | 20 | – | Two blocking screws were placed adjacent to the nail on the coronal plane according to the potential translation direction of the shorter fragment. |
| Song23 | – | 23 | – | Two 5.0 mm cortical screws were used as poller screw anteroposteriorly in the metadiaphyseal flaring area, 2 or 3 cm above the distal interlocking screw holes. |
Note. — indicates not reported by the study.
Table 3.
General outcome information
| Study | Outcomes measures | Time to union mean (range) | Complications | Definition of malunion | Definition of nonunion | Follow-up interval mean (range) | Observations |
|---|---|---|---|---|---|---|---|
| Ricci et al19 | Radiographic union; coronal alignment; sagittal alignment | __ | Nonunion, malunion, osteomyelitis, secondary surgical procedures | More than 5° in the coronal and sagittal planes | Nonunion was defined as absence of progressive fracture healing for three consecutive months | 35 (19–54) weeks One patient lost to follow-up |
No complications directly related to the use of blocking screws. One patient had osteomyelitis and one patient had a persistent nonunion. One additional patient required removal of proximal interlocking screws because of pain. |
| Moongilpatti Sengodan et al12 | Radiographic union; coronal alignment; sagittal alignment; Karlstorm-Olerud score | __ | Delayed union, malunion, deep infection, secondary surgical procedures | Not defined, Trafton’s recommendation referenced in their discussion | Not defined | Inconsistent (abstract states maximum of three years, text states with a minimum follow-up of five years) | Secondary procedure was required in only one case to achieve union (5%). Dynamization was carried out six weeks after interlocking nailing that developed deep infection. Patient was previous treated with an Ex-Fix. In one case a new fracture line appeared while introducing the nail after placement of poller screw but alignment and union were unaffected. |
| Krettek et al11 | Time to union; coronal alignment; sagittal alignment; Karlstorm-Olerud score | __ | Nonunion, malunion, deep infection, secondary surgical procedures Nerve injury (Not related to poller screw) |
Not defined | Not defined | 8.5 months (12 to 29) Two patients lost to follow-up |
The indications for intramedullary nailing included acute fractures (n = 13), delayed unions (n = 3) and misaligned fractures (n = 5) treated previously with external fixation (n = 2) or intramedullary nailing (n = 5). Reoperation One patient had autogenous bone graft for delayed union. Three implants removed after union was achieved; reason not given. |
| Seyhan et al24 | Time to union mean | 12.6 (8–32) weeks | Delayed union, secondary surgical procedures | Not defined | Not defined | 26.6 months | Two implants removed due to implant discomfort after union was achieved. |
| Seyhan et al20 | Radiographic union; coronal alignment; sagittal alignment | __ | Nonunion, malunion, deep infection, secondary surgical procedures | An angle greater than 5° on any plane was considered as misalignment in radiological assessment | Not defined | 21.0 (12–36) months | An angle greater than 5° on any plane was considered as misalignment in radiological assessment. 1/21 had a fissure at blocking screw. 1/ 21 developed 8° of flexion deformity and nonunion. They underwent autografting and subsequently united. |
| Kim et al31 | Radiographic union; range of motion | __ | No complications i.e. infections, implant breakages, rotational deformities > 5°, or shortening of the lower limbs occurred | Rotational deformities > 5° | Not defined | 17.1 (12–42) months | |
| Kulkarni et al21 | Time to union; coronal alignment; sagittal alignment; knee rating scale of the Hospital for Special Surgery | __ | Nonunion, malunion, anterior knee joint pain, superficial infections, secondary surgical procedures | Not defined | Not defined | 30.8 (24–45) months | 47/70 patients underwent removal of the nails and screws. 5/70 cases on nonunion were resolved by bone grafting. |
| Van Dyke et al29 | Radiographic union; coronal alignment; sagittal alignment | 21.6 weeks | Nonunion, malunion, secondary surgical procedures | Not defined | The need for any secondary surgical intervention including nail dynamization, bone grafting, or exchange nailing was considered nonunion in this study | Follow-up to union | |
| Seyhan et al26 | Radiographic union; coronal alignment; sagittal alignment; Harris Hip Score; operation times; fluoroscopy times | 15±6 weeks (SD) | Number but not nature of complications recorded Secondary surgical procedures |
Not defined | Not defined | 21.83 months | 2/12 patients in the blocking screw group had reintervention but the nature of this operation was not listed. 3/12 patients had complications but what the complications were was not listed. |
| Shah et al27 | Radiographic union; coronal alignment; sagittal alignment; knee rating scale of the Hospital for Special Surgery | 5.6 months | Nonunion, malunion, anterior knee joint pain, superficial infections, neurovascular injury, secondary surgical procedures | < 5° valgus or varus deformity, sagittal not defined | Not defined | 12 months | 24/60 patients underwent removal of the nails and screws; reasons not given. |
| Bhangadiya et al22 | Radiographic union; coronal alignment; sagittal alignment; ROM; AOFAS Ankle-Hindfoot Scale; Rasmussen’s Functional Score System | 4.1 (3–9) months | Nonunion, malunion, anterior knee joint pain, superficial infections, neurovascular injury, secondary surgical procedures | Not defined | Not defined | 28.9 (20–33) months | Two cases had nonunion which was treated with bone grafting; the other patient was malunited. |
| Gao et al28 | Time to union; coronal alignment; sagittal alignment; ROM | 7.8 (4.7–13.5) months | No complications i.e. nonunion, malunion, pain, loss of ROM occurred, secondary surgical procedures | Angulation > 5°, rotational deformity > 10°, or shortening > 2 cm | Not defined | 1.5 (1–2) years | All patients achieved union without a secondary procedure. |
| Song23 | Union; coronal alignment; | 19.8 ± 3.2 weeks (SD) | Nonunion, malunion, infection | Angulation > 5°, rotational deformity > 15°, or shortening > 2 cm | Union was defined as the ability to bear full weight without pain, with callus bridging in three of four cortices on radiographs | 18.3 ± 2.0 months | Comparison was made to IM nailing alone. Union rate was significantly higher in poller screw group than IM nail alone. Two poller screws after nailing took a mean of 21 minutes extra operation time. |
Note. — indicates not reported by the study; IM, intramedullary; SD, standard deviation; ROM, range of motion; AOFAS, American Orthopaedic Foot & Ankle Society.
Incidence of nonunion. Nonunion cases included those fractures that developed osseous nonunion at the time of follow-up. Delayed unions were not included in the nonunion rate if the fractures subsequently healed.
Incidence of infection. The infections were divided into superficial and deep infections. Superficial infections were defined as wound infections that resolved with antibiotic treatment without surgical intervention. Deep infections were defined as infections requiring surgical debridement and/or osteomyelitis.
Incidence of malalignment. The definition of malalignment was determined according to the authors’ definition (where provided). Definitions are listed in Table 3.
Incidence of secondary surgical procedures.
Where information was incomplete of lacking, corresponding authors were contacted by email.
Data analysis
Analysis was conducted in R, using the R package meta, to compute the overall outcome proportion across the studies, using the inverse variance method for pooling.17
Risk of bias assessments
The potential risk of bias of the studies was assessed using MINORS, a methodological index for non-randomized studies.18 See Appendix 1 (729.8KB, pdf) .
Results
Thirteen studies with a total of 371 participants and 376 fractures were included in this systematic review. Mean follow-up time was 21.1 months and mean age of included patients was 40.0 years. Description of studies and demographic characteristics of patients analysed are displayed in Table 1. No randomized control trails (RCTs) were identified in our literature search.
Complications
The various complications reported by each study are detailed in Table 2. Where meaningful; the overall outcome proportion across the studies was computed using the inverse variance method for pooling; 95% confidence intervals and weighting given to each study are displayed. All studies reported the absence or presence of nonunion as an outcome measure. Eight studies reported no nonunions in patients treated with poller screws. Five studies19–23 reported nonunions with the proportions of nonunions being 9.1%, 4.8%, 6.7%, 4% and 4.3% respectively. The overall outcome proportion of nonunion was 4% with narrow confidence intervals of 0.03–0.07 (Fig. 4). In Ricci et al, the nonunion patient had postoperative malalignment of 6° valgus as a lateral blocking screw to control valgus malalignment was not used.19 Seyhan et al’s nonunion patient also had malunion with 8° of flexion deformity and nonunion.20 Two articles did not give further details on the nonunion cases.21,22
Fig. 4.

Overall outcome proportion of nonunion.
Eight studies reported time to union.21–28 The combined mean time to union was 17 weeks. Van Dyke et al’s definition of nonunion as per Table 1 made it difficult to determine what the true nonunion rate was, as any secondary procedure would be counted as a nonunion by their definition (39.1%) which is an atypical definition when compared with the rest of the literature.29
All bar two studies,24,26 with a combined total of 349 patients, reported coronal plane alignment at the time of fracture union. Two of the studies, by Seyhan et al,24,26 did not state that coronal alignment (or sagittal alignment) were checked on the postoperative films and these studies were therefore excluded from the malalignment analysis. The overall outcome proportion of malalignment was 5% with confidence intervals 0.05–0.08 (Fig. 5). Seven studies did not provide a definition of malunion (see Table 3).11,12,21,22,24,26,29 Where deformity was described as a continuous variable we defined malunion of tibial fractures as 5° of varus–valgus angulation as per Trafton’s recommendation.30 Malunion owing to deformity in the coronal plane was more clearly reported than malunion due to deformity in the sagittal plane. Seven studies reported coronal malunion12,19–23,27 with incidences of 9.1%, 10.0%, 4.7%, 1.3%, 5.0%, 2.0% and 8.7% respectively. While all bar one study23 listed sagittal alignment as an outcome measure, only seven studies reported sagittal alignment postoperatively.11,12,19–22,31 Of those seven studies only one20 reported sagittal malalignment in one patient with a distal tibial fracture (Table 3).
Fig. 5.

Overall outcome proportion of malalignment.
Ten studies, with a combined total of 303 patients, commented on superficial infection (Fig. 6). Three studies had superficial infection as a reported complication21,22,27 with outcome proportions of 5.3%, 20.0% and 4.0% respectively. The overall outcome proportion of superficial infection was 6% with confidence intervals 0.03–0.11. Where superficial infection was not specifically noted as a recorded complication of interest, these studies were omitted from the pooled calculations so as not to assume non-reporting meant absence of infection.
Fig. 6.

Overall outcome proportion of superficial infection.
Eight studies, with a combined total of 216 patients, commented on deep infection (Fig. 7). Four studies had deep infection as a reported complication11,12,19,23 with proportions of 9.1% (1 patient), 10.0% (2 patients), 5.0% (1 patient) and 8.7% (2 patients) respectively. The overall outcome proportion of deep infection was 5% with confidence intervals 0.03–0.11. These studies had insufficient information to correlate incidence of infection with open fractures.
Fig. 7.

Overall outcome proportion of deep infection.
Data on secondary surgical procedure rates were highly variable and breakdown of the secondary surgical procedures was not reported by Van Dyke et al29 or Seyhan et al.26 The secondary surgical procedure rate included grafting, revisions and any reported cases of removal of metal work (see Table 2). Data on secondary surgical procedure rates from 11 studies with a combined total of 291 patients were analysed. The overall outcome proportion of secondary surgical procedures was 8% with confidence intervals 0.04–0.18 (Fig. 8). Reoperation rate ranged from 2%22 to 40% by Shah et al for removal of metal work.27 No reasons for removal of metal work were given and this study was therefore excluded from the analysis. Song did not formally collect information on reoperation and therefore have been excluded.23
Fig. 8.

Overall outcome proportion of secondary procedures.
Seven studies had heterogenous population of nonunions and/ =or malunions in addition to acute fractures.11,12,19,21,22,27,29 Four studies included only acute fractures20,23,24,26 and two studies examined nonunions only.28,31 Two studies mixed results for both distal and proximal tibial fractures.11,27 Gao et al reports outcomes from a mixed population of femoral and tibial nonunions.28
A subgroup analysis of femoral versus tibial only studies shows the rates of malunion are lower in femoral fractures. Two studies29,31 looking exclusively at femoral fractures, with a combined total of 56 patients, and nine studies of exclusively tibial lesions, with a combined total of 293, were analysed.11,12,19–23,27,28 The overall outcome proportion of malalignment was 2% (CI: 0.0–0.14) for femoral fractures (Fig. S1) compared with 5% in tibial fractures (CI: 0.03–0.09) (Fig. S2).
Four studies24,26,29,31 with a combined total of 83 patients found that the overall outcome proportion of nonunion in femoral fractures treated with poller screws was 3% (CI: 0.01–0.10) (Fig. S3). Nine studies11,12,19–23,27,28 with a combined total of 293 patients found that the overall outcome proportion of nonunion in tibial fractures treated with poller screws was 5% (CI: 0.03–0.08) (Fig. S4).
Only one femoral study commented on deep and/or superficial infection rates making subgroup analysis meaningless.
Femoral fractures had an increased risk of reoperation compared with tibial fractures. Four studies24,26,29,31 with a combined total of 83 patients found an overall outcome proportion of 21% (CI: 0.08–0.43) (Fig. S5) versus just 5% (CI: 0.03–0.09) across six studies with 210 patients with tibial lesions (Fig. S6).12,19–22,28
A subgroup analysis of nonunion versus acute fractures demonstrates no appreciable difference in the rate of malunion. Neither nonunion study28,31 reported coronal malalignment post exchange nailing and poller screw insertion. The overall outcome proportion of malunion using the inverse variance method for pooling was 4% (CI: 0.01–0.24) with a combined total of 22 patients (Fig. S7) compared with 5% in acute fractures (Fig. S8). The overall outcome proportion of reoperation using the inverse variance method for pooling was 4% (CI: 0.01–0.24) with a combined total of 22 patients (Fig. S9). This is much lower than the rate of reoperation in acute fracture only studies20,24,26,29 of 18% (CI: 0.07–0.41) with a combined total of 94 patients (Fig. S10).
Discussion
Poller screws have been purported to expand the indication for intramedullary nailing and reduce rates of nonunion and malunion seen with IM nailing of metaphyseal fractures. Poller screws are placed before nail insertion and often before reaming to control alignment in both the sagittal and coronal planes, depending on the position and direction of the screws.32 While poller screw biomechanics has been described, the outcomes of poller screw augmentation of IM nailing has not. Our results show a low complication rate of IM nailing augmented with poller screws in terms of nonunion (4%), coronal plane malunion (6%), deep (5%) and superficial (6%) infections, and secondary procedures (8%). Our pooled analysis compares favourably to the complication rates reported in the treatment of metaphyseal fractures with IM nailing alone. In a systematic review incorporating 489 distal tibial fractures treated with intramedullary nailing, Zelle et al showed a nonunion rate of 5.5%, an infection rate of 4.3%, and a malunion rate of 16.2%, and 16.4% of the patients required secondary surgical procedures.33 The nonunion rates are favourable when compared with the nonunion rate of 12% in a review of 1003 patients treated with reamed intramedullary nailing of tibial fractures.34 Combined small retrospective studies with a total of 183 patients treated with intramedullary nailing of extraarticular proximal tibia fractures reported an average malreduction rate of 8.2%.3
Our review suggests that poller screw augmentation of IM nailing reduces the incidence of both nonunion and malalignment. It is interesting to note that half the studies reporting nonunion were nonunions associated with malalignment. In Ricci et al, the nonunion patient had postoperative malalignment of 6° valgus, as a lateral blocking screw to control valgus malalignment was not used.19 Seyhan et al’s nonunion patient also had malunion with 8° of flexion deformity and nonunion.20 This reinforces the importance of a stable mechanical environment for healing and highlights that poller screws are not a panacea for nonunion. Radiological studies by our group suggest that increase in fracture stability associated with poller screw use is most pronounced at the site contralateral to the poller screw, as evidenced by the significantly smaller size of contralateral versus ipsilateral callus. With simple spiral fractures of the distal tibia, a single poller screw may be sufficient to provide an increase in stability in all planes.35 Depending on fracture pattern, at least one poller screw in the sagittal and one in the coronal plane may be needed to fully control alignment to avoid the failure seen in one patient in Ricci et al’s cohort.19 Table 2 shows that the majority of studies used just one poller screw despite treating complex fracture patterns. Our group have evolved the way we use poller screws from the use of a single screw to create a corridor inside the bone, ‘first-generation’ of poller screw, through to the ‘third-generation’ of poller screw with poller screw placement on both sides of the fracture line to create long-term compression and reduce the working length of the nail.36
The principle of poller screw use is the same with both femoral and tibial fractures; however, different anatomical considerations and different deforming forces affect position of screw placement. The subcutaneous nature of the tibia compared with the femur makes placement of poller screws in the tibia easier. The strong muscular coverage of the femur makes drilling and screw insertion more difficult and increases the possibility of losing the screws in the soft tissue. We recommend either using a screwdriver that locks into the screw head if available or tying a strong surgical thread to the screw before inserting to aid screw retrieval should a problem be encountered. In our subgroup analysis, femoral fractures did not demonstrate an increased risk of malunion compared with tibial fractures, despite the above challenges to poller screw placement. Femoral fractures, however, did have an increased rate of reoperation when compared with tibial fractures (21% vs. 5%); however, this may be attributed to the difference in sample size of 83 and 210 respectively.
Two studies, both studying the use of poller screws in the treatment of nonunion, reported no complications.28,31 Krettek et al reported no complications related to poller screws, one patient developed a rotational malalignment greater than 15°.11 Despite this both papers state that there were no complications related to the poller screws.11,19,22 It could be argued that the improper positioning of poller screws contributed to nonunion and/or malunion, and therefore should be considered a complication of ‘improper’ poller screw placement rather than a complication due to the poller screws themselves. Moreover, comparing the outcomes of different studies has been complicated by different definitions of outcome measures. This was a particular challenge for secondary procedure data where information on the definition and nature of reoperation was not detailed, and attempts to contact corresponding authors were unsuccessful.21,26,27 Our review showed large variation in rates of secondary procedures ranging from 2.0% to 39.1% for Van Dyke et al.29 Email communication with the Van Dyke group revealed that the majority of secondary procedures were distal interlocking screw removal for dynamization purposes. Next most frequent was distal screw removal for broken screws or painful hardware. Lastly, there were a variety of secondary procedures including bone grafting, irrigation and debridement of infection, exchange nailing, and knee arthroscopy for persistent knee complaints.
Several limitations exist and should be discussed. Firstly, the available literature includes no prospective, randomized, clinical trials. Three of the included studies were prospective case series11,12,19 and ten were retrospective case series.20–24,26–29,31 The conclusions that can be drawn from these studies are limited by the lack of adequate control groups in all bar two studies.23,29 This is reflected in the low mean MINORS score of the included studies of 10.1 out of 16. Secondly, many studies included heterogenous populations, mixing results for distal and proximal tibial fractures,11,27 acute fractures and nonunion11,12,19,21,22,27,29 and femoral and tibial nonunions.28 We decided to include both nonunion and acute fractures for two reasons. Firstly, poller screws behave the same at the fracture site, biomechanically neutralizing shear forces and increase the amount of compression through the fracture line be that the fracture line of an acute fracture or nonunion. Secondly, there were limited published articles and inclusion of nonunions increased sample size and facilitated subgroup analysis in our attempt to elucidate whether the outcomes differed depending on age of fracture.
Our limited subgroup analysis comparing populations with only femoral fracturs with only tibial fractures data demonstrates that femoral fractures treated with poller screws have lower rates of malunion than their tibial counterparts; however, femoral fractures have an increased rate of reoperation. Comparison of reoperation rate in a population of nonunion versus acute fractures only showed a lower rate of reoperation than in the nonunion population (4%) compared with 18% amongst acute fractures. This, however, could be due to selection bias where, in the case series published by Gao et al and Kim et al focus was given to nonunion ‘success stories’ and there is no correction made for the number of operations the participants of these studies had prior to poller screw insertion.28,31 Furthermore, insufficient detail on which fracture types required reoperation and the number and positioning of poller screws in the acute fracture studies does not permit an accurate assessment of whether or not the poller screw placement was correct and provided accurate reduction. We stress that it is the positioning of poller screws to neutralize shear forces and convert these forces to compressive forces at the fracture site and not merely the presence of poller screws which facilitates union.
Given non-randomization, there is a high risk of selection bias. Poller screws may have been the treatment of choice for the most challenging fractures when other types of reduction had failed. Seyhan et al’s study comparing reduction techniques for subtrochanteric femoral fractures stated that blocking screws were only used when clamp reduction failed.26 Seyhan et al’s 2013 study states ‘patients with blocking screws most commonly sustained high-energy traumas, and many patients had polytrauma and open fractures’. This may under-estimate the benefit of blocking screws because the groups do not have similar baseline characteristics.24
As an alternative to poller screws, K wires have been described as reduction aids and used in a similar fashion to poller screws to aid centralization of IM nails, which are removed post locking screw insertion. Poyanlı et al place K wires before the guidewire, as we do with poller screws.37 Poyanlı et al conclude that by locking the nail in different directions, appropriate reduction can be maintained until the bone in their series of 13 patients. Biewener et al described the ‘palisade method’ for treatment of distal tibial diametaphyseal fractures.38 They placed K wires sequentially to guide an intramedullary nail with a good central position into a distal short fragment. After proximal and distal fixation of the nail, the K wires were removed to prevent loss of reduction. No data were offered on the impact the ‘palisade method’ had on operative time or damage to soft tissues or infection rates. While K wire constructs may aid reduction in theatre, neither study measured the difference in radiographic reduction immediately postoperatively and at union, therefore it is not possible to quantitively assess maintenance of reduction.37,38 Without studies comparing the outcomes of removable K wires etc. with permanent poller screws, it is not possible to draw conclusions on the efficacy of one techniques over the other; however, the poller screws will continue to maintain reduction and resist the deforming muscular forces that will be at play when the patient mobilizes postoperatively.
This systematic review demonstrates challenges in summarizing therapeutic evidence for rare and heterogeneous conditions. Outcomes following the use of poller screws have been examined only in case reports and case series, and while these study designs are near the bottom of the hierarchy of evidence, a new paradigm suggests that systematic reviews are a lens that can be helpful for appraising and synthesizing available data of all types, providing recognition of the inherent limitations of the data.39
Perceived disadvantages of poller screws were referenced in two studies; one stated that both fluoroscopy and operative times were significantly longer than fracture reduction by clamp or cerclage, the other that the addition of poller screws increased operative time by a mean of 21 minutes when compared with IM nailing alone.23,26 The need for fluoroscopy throughout the procedure, extending operative time and causing extra exposure to radiation, was beyond the scope of this systematic review but should be studied in greater detail. Propagation or creation of a fracture line while introducing the nail after placement of a poller screw is, anecdotally, a perceived complication of poller screw use. However, this complication was only noted by one author in a single case where alignment and union were unaffected.12
The results of the present systematic review show low complication rates for IM nailing augmented with poller screws in terms of nonunion (4%), coronal plane malunion (5%), deep (5%) and superficial (6%) infections, and secondary procedures (8%) at a mean follow-up of 21.1 months. Based on the current available evidence, we report the following: that poller screw augmentation of intramedullary nailing in the treatment of metaphyseal tibial fractures, infraisthmal femoral fractures and nonunions have lower or comparable complication rates with those reported in the literature for IM nailing alone. Prospective, randomized, clinical trials comparing poller screw augmentation versus IM nailing alone will be necessary to fully determine outcome benefits.
Footnotes
ICMJE Conflict of interest statement: The authors declare no conflict of interest relevant to this work.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Supplementary Material
Supplementary material is available online.
References
- 1. Kaye JA, Jick H. Epidemiology of lower limb fractures in general practice in the United Kingdom. Inj Prev 2004;10:368–374. http://www.ncbi.nlm.nih.gov/pubmed/15583259 (date last accessed 14 May 2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Lindvall E, Sanders R, Dipasquale T, Herscovici D, Haidukewych G, Sagi C. Intramedullary nailing versus percutaneous locked plating of extra-articular proximal tibial fractures: comparison of 56 cases. J Orthop Trauma 2009;23:485–492. http://www.ncbi.nlm.nih.gov/pubmed/19633457 (date last accessed 14 May 2019). [DOI] [PubMed] [Google Scholar]
- 3. Hiesterman TG, Shafiq BX, Cole PA. Intramedullary nailing of extra-articular proximal tibia fractures. J Am Acad Orthop Surg 2011;19:690–700. http://www.ncbi.nlm.nih.gov/pubmed/22052645 (date last accessed 14 May 2019). [DOI] [PubMed] [Google Scholar]
- 4. Naik MA, Arora G, Tripathy SK, Sujir P, Rao SK. Clinical and radiological outcome of percutaneous plating in extra-articular proximal tibia fractures: a prospective study. Injury 2013;44:1081–1086. http://www.ncbi.nlm.nih.gov/pubmed/23561582 (date last accessed 14 May 2019). [DOI] [PubMed] [Google Scholar]
- 5. Modny MT, Bambara J. The perforated cruciate intramedullary nail: preliminary report of its use in geriatric patients. J Am Geriatr Soc 1953;1:579–588. http://www.ncbi.nlm.nih.gov/pubmed/13084379 (date last accessed 12 May 2019). [DOI] [PubMed] [Google Scholar]
- 6. Hahn D, Bradbury N, Hartley R, Radford PJ. Intramedullary nail breakage in distal fractures of the tibia. Injury 1996;27:323–327. https://www.sciencedirect.com/science/article/pii/0020138395002286 (date last accessed 14 April 2019). [DOI] [PubMed] [Google Scholar]
- 7. Nork SE, Schwartz AK, Agel J, Holt SK, Schrick JL, Winquist RA. Intramedullary nailing of distal metaphyseal tibial fractures. J Bone Joint Surg Am 2005;87:1213–1221. http://jbjs.org/cgi/doi/10.2106/JBJS.C.01135 (date last accessed 14 April 2019). [DOI] [PubMed] [Google Scholar]
- 8. Newman SDS, Mauffrey CPC, Krikler S. Distal metadiaphyseal tibial fractures. Injury 2011;42:975–984. http://www.ncbi.nlm.nih.gov/pubmed/22073415 (date last accessed 14 April 2019). [DOI] [PubMed] [Google Scholar]
- 9. Robinson CM, McLauchlan GJ, McLean IP, Court-Brown CM. Distal metaphyseal fractures of the tibia with minimal involvement of the ankle: classification and treatment by locked intramedullary nailing. J Bone Joint Surg Br 1995;77:781–787. http://www.ncbi.nlm.nih.gov/pubmed/7559711 (accessed 14 April 2019). [PubMed] [Google Scholar]
- 10. Donald G, Seligson D. Treatment of tibial shaft fractures by percutaneous Küntscher nailing: technical difficulties and a review of 50 consecutive cases. Clin Orthop Relat Res 1983;178:64–73. http://www.ncbi.nlm.nih.gov/pubmed/6883869 (accessed 14 April 2019). [PubMed] [Google Scholar]
- 11. Krettek C, Stephan C, Schandelmaier P, Richter M, Pape HC, Miclau T. The use of poller screws as blocking screws in stabilising tibial fractures treated with small diameter intramedullary nails. J Bone Joint Surg Br 1999;81:963–968. [DOI] [PubMed] [Google Scholar]
- 12. Moongilpatti Sengodan M, Vaidyanathan S, Karunanandaganapathy S, Subbiah Subramanian S, Rajamani SG. Distal tibial metaphyseal fractures: does blocking screw extend the indication of intramedullary nailing? ISRN Orthop 2014;17:542623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Stedtfeld H-W, Mittlmeier T, Landgraf P, Ewert A. The logic and clinical applications of blocking screws. J Bone Joint Surg Am 2004;86-A:17–25. http://www.ncbi.nlm.nih.gov/pubmed/15691104 (date last accessed 12 May 2019). [DOI] [PubMed] [Google Scholar]
- 14. Shahulhameed A, Roberts CS, Ojike NI. Technique for precise placement of poller screws with intramedullary nailing of metaphyseal fractures of the femur and the tibia. Injury 2011;42:136–139. https://linkinghub.elsevier.com/retrieve/pii/S0020138310002652 (date last accessed 12 May 2019). [DOI] [PubMed] [Google Scholar]
- 15. Hannah A, Aboelmagd T, Yip G, Hull P. A novel technique for accurate poller (blocking) screw placement. Injury 2014;45:1011–1014. https://linkinghub.elsevier.com/retrieve/pii/S0020138314000990 (date last accessed 12 May 2019). [DOI] [PubMed] [Google Scholar]
- 16. Muthusamy S, Rozbruch SR, Fragomen AT. The use of blocking screws with internal lengthening nail and reverse rule of thumb for blocking screws in limb lengthening and deformity correction surgery. Strategies Trauma Limb Reconstr 2016;11:199–205. http://www.ncbi.nlm.nih.gov/pubmed/27665618 (date last accessed 12 May 2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Schwarzer G. meta: an R package for meta-analysis. R News 2007;7 https://cran.r-project.org/doc/Rnews/Rnews_2007-3.pdf (date last accessed 13 May 2019). [Google Scholar]
- 18. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 2003;73:712–716. http://www.ncbi.nlm.nih.gov/pubmed/12956787 (date last accessed 9 May 2019). [DOI] [PubMed] [Google Scholar]
- 19. Ricci WM, O’Boyle M, Borrelli J, Bellabarba C, Sanders R. Fractures of the proximal third of the tibial shaft treated with intramedullary nails and blocking screws. J Orthop Trauma 2001;15:264–270. http://www.ncbi.nlm.nih.gov/pubmed/11371791 (date last accessed 9 May 2019). [DOI] [PubMed] [Google Scholar]
- 20. Seyhan M, Kocaoglu B, Gereli A, Nalbantoglu U, Turkmen M. Treatment for distal tibial fractures with intramedullary nails and blocking screws. Eur J Orthop Surg Traumatol 2012;22:395–401. http://link.springer.com/10.1007/s00590-011-0853-3 (date last accessed 12 May 2019). [Google Scholar]
- 21. Kulkarni SG, Varshneya A, Kulkarni S, et al. Intramedullary nailing supplemented with poller screws for proximal tibial fractures. J Orthop Surg (Hong Kong) 2012;20:307–311. [DOI] [PubMed] [Google Scholar]
- 22. Bhangadiya R. An outcome analysis to determine the uses of poller screw in treatment of displaced proximal and distal shaft metadiaphyseal fractures of tibia treated with intramedullary nailing. Orthop Rheumatol Open Access J 2016;2 http://juniperpublishers.com/oroaj/OROAJ.MS.ID.555585.php (date last accessed 12 May 2019). [Google Scholar]
- 23. Song S-H. Radiologic outcomes of intramedullary nailing in infraisthmal femur-shaft fracture with or without poller screws. Biomed Res Int 2019;2019:9412379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Seyhan M, Cakmak S, Donmez F, Gereli A. Blocking screws for the treatment of distal femur fractures. Orthopedics 2013;36:e936–e941. http://www.ncbi.nlm.nih.gov/pubmed/23823053 (date last accessed 14 April 2019). [DOI] [PubMed] [Google Scholar]
- 25. Gomez MT, Carlson GM, Van Dooren K. Practical approaches to supporting young women with intellectual disabilities and high support needs with their menstruation. Health Care Women Int 2012;33:678–694. [DOI] [PubMed] [Google Scholar]
- 26. Seyhan M, Unay K, Sener N. Comparison of reduction methods in intramedullary nailing of subtrochanteric femoral fractures. Acta Orthop Traumatol Turc 2012;46:113–119. http://www.ncbi.nlm.nih.gov/pubmed/22491436 (date last accessed 12 May 2019). [DOI] [PubMed] [Google Scholar]
- 27. Shah RK, Shah SB. Treatment of diaphysio-metaphyseal fracture of tibia by intramedullary nail in combination with poller screw. J Bone Res Reports 2015;1 http://bone.imedpub.com/treatment-of-diaphysiometaphyseal-fracture-of-tibia-by-intramedullary-nail-in-combination-with-poller-screw.php?aid=6640 (date last accessed 12 May 2019). [Google Scholar]
- 28. Gao KD, Huang JH, Li F, et al. Treatment of aseptic diaphyseal nonunion of the lower extremities with exchange intramedullary nailing and blocking screws without open bone graft. Orthop Surg 2009;1:264–268. http://doi.wiley.com/10.1111/j.1757-7861.2009.00041.x (date last accessed 12 May 2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Van Dyke B, Colley R, Ottomeyer C, Palmer R, Pugh K. Effect of blocking screws on union of infraisthmal femur fractures stabilized with a retrograde intramedullary nail. J Orthop Trauma 2018;32:251–255. [DOI] [PubMed] [Google Scholar]
- 30. Trafton PG. Closed unstable fractures of the tibia. Clin Orthop Relat Res 1988;230:58–67. http://www.ncbi.nlm.nih.gov/pubmed/3284684 (accessed 14 May 2019). [PubMed] [Google Scholar]
- 31. Kim J-W, Yoon Y-C, Oh C-W, Han S-B, Sim J-A, Oh J-K. Exchange nailing with enhanced distal fixation is effective for the treatment of infraisthmal femoral nonunions. Arch Orthop Trauma Surg 2018;138:27–34. http://link.springer.com/10.1007/s00402-017-2802-z (accessed 9 May 2019). [DOI] [PubMed] [Google Scholar]
- 32. Krettek C, Miclau T, Schandelmaier P, Stephan C, Möhlmann U, Tscherne H. The mechanical effect of blocking screws (‘poller screws’) in stabilizing tibia fractures with short proximal or distal fragments after insertion of small-diameter intramedullary nails. J Orthop Trauma 1999;13:550–553. http://www.ncbi.nlm.nih.gov/pubmed/10714781 (accessed 21 May 2019). [DOI] [PubMed] [Google Scholar]
- 33. Zelle BA, Bhandari M, Espiritu M, Koval KJ, Zlowodzki M; Evidence-Based Orthopaedic Trauma Working Group. Treatment of distal tibia fractures without articular involvement: a systematic review of 1125 fractures. J Orthop Trauma 2006;20:76–79. http://www.ncbi.nlm.nih.gov/pubmed/16424818 (accessed 14 May 2019). [DOI] [PubMed] [Google Scholar]
- 34. Dailey HL, Wu KA, Wu P-S, McQueen MM, Court-Brown CM. Tibial fracture nonunion and time to healing after reamed intramedullary nailing: risk factors based on a single-center review of 1003 patients. J Orthop Trauma 2018;32:e263–e269. http://insights.ovid.com/crossref?an=00005131-201807000-00015 (date last accessed 14 June 2019). [DOI] [PubMed] [Google Scholar]
- 35. Cundall-Curry DJ, Lawrence JE, Fountain DM, Krkovic M. The use of poller screws in intramedullary nailing is associated with decreased callus formation. Clin Cases Miner Bone Metab 2019;15:216–220. [Google Scholar]
- 36. Krkovic M. Third generation poller screws. https://www.limbreconstructions.com/third-generation-poller-screws.html (date last accessed 11 June 2019).
- 37. Poyanlı OS, Soylemez MS, Ozkut AT, Esenkaya I, Unal OK, Kılıncoglu V. Use of provisional K wires instead of poller screws for treatment of diametaphyseal fractures of the distal femur and proximal and distal tibia. Acta Orthop Belg 2016;82:579–585. http://www.ncbi.nlm.nih.gov/pubmed/29119900 (date last accessed 10 September 2019). [PubMed] [Google Scholar]
- 38. Biewener A, Grass R, Holch M, Zwipp H. [Intramedullary nail placement with percutaneous Kirschner wires. Illustration of method and clinical examples]. Unfallchirurg 2002;105:65–70. http://www.ncbi.nlm.nih.gov/pubmed/11968561 (date last accessed 10 September 2019). [DOI] [PubMed] [Google Scholar]
- 39. Murad MH, Asi N, Alsawas M, Alahdab F. New evidence pyramid. Evid Based Med 2016;21:125–127. http://www.ncbi.nlm.nih.gov/pubmed/27339128 (date last accessed 12 May 2019). [DOI] [PMC free article] [PubMed] [Google Scholar]