

ABSTRACT
Coffee enemas are often used by naturopathic practitioners to treat a number of diseases, including cancer. However, there is no supportive evidence, and its use comes with major risks. We report a case of proctocolitis in a healthy patient after coffee enema treatment. To our knowledge, only 3 other cases of this adverse effect exist in the literature.
INTRODUCTION
Proponents of coffee enemas advocate for its use in treating various medical diseases and believe that it is capable of curing advanced cancer via enzyme activation and toxin excretion.1 However, there has been no science-based evidence to verify these claims, and its use is associated with harmful effects, such as electrolyte imbalance and sepsis.2,3 We report a case of coffee enema-induced proctocolitis.
CASE REPORT
A 40-year-old white woman presented with acute onset of lower abdominal pain, hematochezia, and tenesmus. She denied recent travel history, illnesses, or contact with any sick people. She had a history of mixed-type irritable bowel syndrome and biliary colic but had never experienced rectal bleeding or hematochezia. Although her family's medical history included a brother who has ulcerative colitis and her aunts who suffer from Crohn's disease, the patient denied any previous diagnosis of inflammatory bowel disease (IBD).
On physical examination, the patient was exquisitely tender to palpation in her lower abdomen, particularly in the suprapubic region. Computed tomography scan showed severe proctocolitis from the distal descending colon to the rectum, her white blood cell count was 21.8 × 109 cells/L with a neutrophilic predominance, the C-reactive protein was 23 mg/L, and fecal leukocyte antigen was positive. However, Clostridioides difficile, Shiga toxin, stool culture, lipase, and liver function tests were unremarkable. On day 2, the patient revealed using approximately 500 mL of room temperature coffee enema several hours before the onset of her symptoms. She used 4 feminine douching bottles to squeeze the black coffee, which she purchased at a fast-food establishment, into her rectum. She reported that the coffee “never came back out.” The patient received instructions to do so from her naturopathic doctor to clear her gallstones. She completed a rehabilitation program for narcotic addiction and reported a preference for enema over pharmacologic agents to maintain her health in a natural way.
Flexible sigmoidoscopy performed on day 3 displayed severe inflammation up to 60 cm depth of insertion (Figure 1). A biopsy revealed necrotic mucosa and purulent exudate, but no crypt abscesses (Figure 2). Repeat C. difficile laboratory tests were negative, and she was then started on 60 mg methylprednisolone and 40 mg dicyclomine administered 4 times daily. By day 6, she could tolerate oral intake but complained of continued pain, which was relieved by dicyclomine. Repeat flexible sigmoidoscopy up to 30 cm depth on day 10 demonstrated improved severity of proctocolitis (Figure 3). Exploration farther than 30 cm was not sought because mucosa began to appear normal at that point. Biopsy showed ulceration and granulation tissue of the rectum, but no pathologic changes of the sigmoid colon (Figure 4). She was discharged on day 13 on a prednisone taper after demonstrating improved abdominal pain and resolution of rectal bleeding, the ability to tolerate oral intake, and a decreased white blood cell count of 13.8 × 109 cells/L. The patient was scheduled for a postdischarge colonoscopy but did not arrive for her appointment and could not be reached to arrange for a follow-up.
Figure 1.
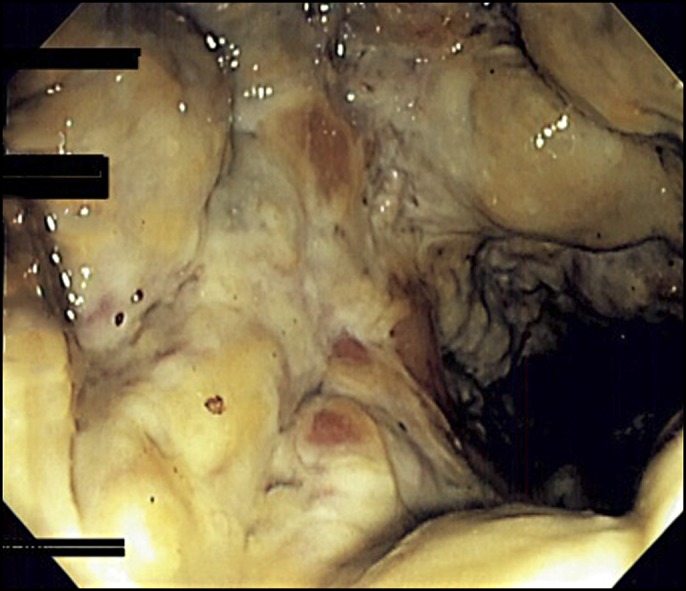
Flexible sigmoidoscopy on day 3 showing severe rectal inflammation.
Figure 2.
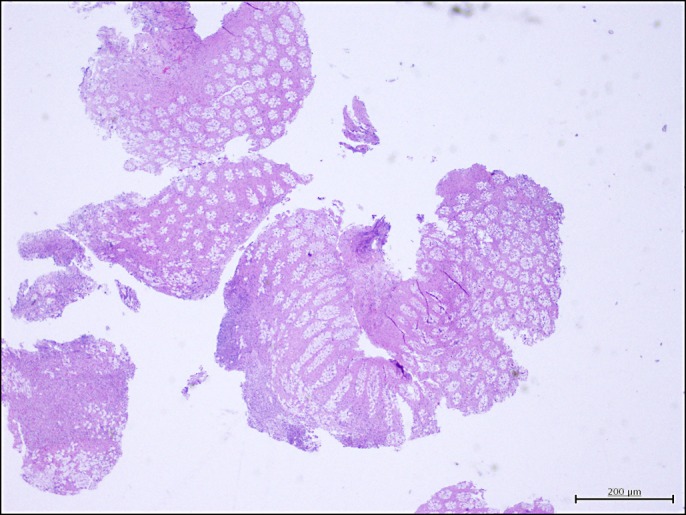
Hematoxylin & eosin stain on day 3 showing necrotic mucosa with acute inflammation and purulent exudate.
Figure 3.
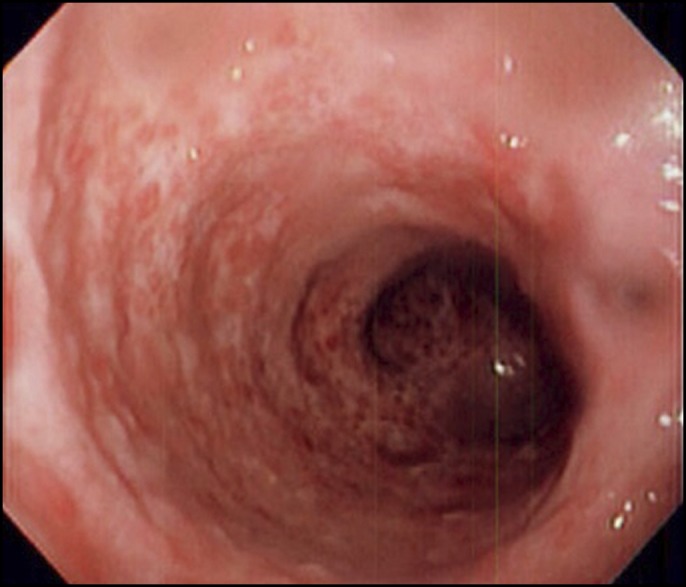
Flexible sigmoidoscopy on day 10 showing inflamed rectal mucosa improved from previous examination.
Figure 4.
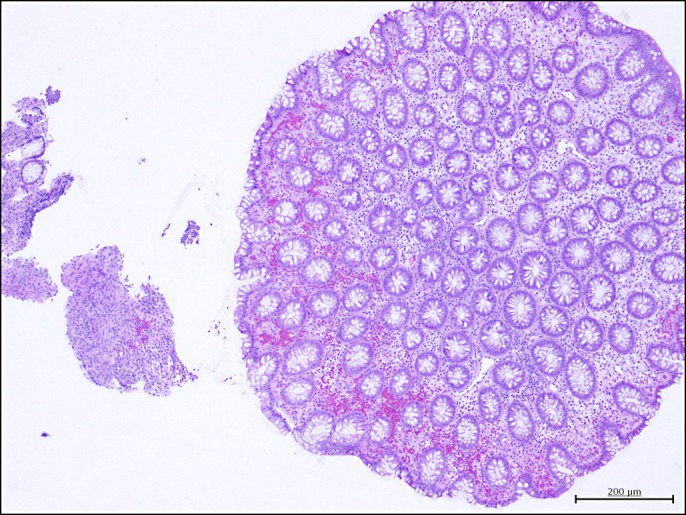
Hematoxylin & eosin stain on day 10 showing healed mucosa with granulation tissue.
DISCUSSION
Although scarce, references to coffee enemas in the literature provide evidence contradicting proponents' claims of its benefit. Supporters propose that the coffee activates antioxidant-like properties via glutathione S-transferase, and rectal administration of it is claimed to dilate bile ducts and excrete toxin-laden bile.4 However, coffee enemas are not correlated with changes in serum levels of glutathione.5 In addition, coffee administered through enema leads to lower serum concentrations when compared with its oral counterpart.6 In a clinical trial that used coffee enemas and other alternative therapies for pancreatic cancer, patients who received chemotherapy survived 3 times longer than those on the more natural regimen.7 Nonetheless, it continues to be promoted to patients by a variety of naturopathic practitioners and websites.8
Adverse effects have been reported with coffee enema use. One patient with a history of advanced breast cancer developed sepsis; 2 other patients acquired severe electrolyte abnormalities.2,3 All 3 cases resulted in death.2,3 Thermal burns from heated coffee enemas have also been reported, resulting in strictures and a subsequent bowel perforation.9,10,11 Three cases of coffee enema-induced proctocolitis exist in the literature.12–14 Our patient presented similarly to these 3 patients; however, our patient's imaging displayed more extensive damage from the anus up to the descending colon. We believe this finding may be from her use of feminine douching bottles providing additional pressure to reach the colon and from her report of coffee retention.
We propose that the mechanisms by which the coffee enema may have induced mucosal damage include ischemia and inflammation. The first biopsy suggested ischemic colitis. Given the distribution of the injury, we believe that damage occurred through local rather than systemic mechanisms. Recent studies of consumed caffeine demonstrated the impaired endothelial function of capillaries and arterioles via endothelium-derived hyperpolarizing factor-mediated vasoactive pathways.15 We hypothesize that additional vasoconstriction through caffeine's antagonism of adenosine receptors, inhibition of phosphodiesterase enzymes, and other molecular effects on endothelial and vascular smooth muscle cells may have contributed to a local ischemic event.16 We wondered whether the patient's strong family history of IBD predisposed her to inflammatory damage via caffeine's antagonism of adenosine receptor A2A, a receptor shown to prevent mucosal inflammation in an animal model of IBD.17 To our knowledge, there are no studies that assess the direct effect of caffeine absorption through colonic mucosa. Our patient denied using heated coffee that would have caused thermal damage.
The patient reported significant relief with dicyclomine, which may be a feasible option for pain control in future similar cases. It is unclear at this time whether recovery is a self-limited process or whether treatment with medication, such as steroids, is required. During recovery, our patient expressed plans to follow up with the same naturopathic physician and blamed herself for using too much coffee. She could not be persuaded that the enemas posed more risk than benefit. A 2015 survey in the United States revealed declining confidence in the medical system.18 It is imperative we work to develop trusting relationships with patients so that they accept our evidence-based practice.19
DISCLOSURES
Author contributions: A. Lee, S. Kabashneh and CP Tsouvalas wrote and edited the manuscript. U. Rahim and MY Khan provided images and edited the manuscript. M. Anees reviewed the manuscript. D. Levine edited the manuscript and is the article guarantor.
Financial disclosure: None to report.
Previous presentation: This case was presented at the American College of Gastroenterology Annual Scientific Meeting; October 25–30, 2019; San Antonio, Texas.
Informed consent was obtained for this case report.
REFERENCES
- 1.Gerson M. The cure of advanced cancer by diet therapy: A summary of 30 years of clinical experimentation. Physiol Chem Phys. 1978;10(5):449–64. [PubMed] [Google Scholar]
- 2.Eisele JW, Reay DT. Deaths related to coffee enemas. JAMA. 1980;244(14):1608–9. [PubMed] [Google Scholar]
- 3.Margolin KA, Green MR. Polymicrobial enteric septicemia from coffee enemas. West J Med. 1984;140(3):460. [PMC free article] [PubMed] [Google Scholar]
- 4.Gerson Therapy Handbook. (https://gerson.org/pdfs/GersonTherapyHandbook.pdf). Accessed July 1, 2019. [Google Scholar]
- 5.Teekachunhatean S, Tosri N, Sangdee C, et al. Antioxidant effects after coffee enema or oral coffee consumption in healthy Thai male volunteers. Hum Exp Toxicol. 2012;31(7):643–51. [DOI] [PubMed] [Google Scholar]
- 6.Teekachunhatean S, Tosri N, Rojanasthien N, Srichairatanakool S, Sangdee C. Pharmacokinetics of caffeine following a single administration of coffee enema versus oral coffee consumption in healthy male subjects. ISRN Pharmacol. 2013;2013:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chabot JA, Tsai WY, Fine RL, et al. Pancreatic proteolytic enzyme therapy compared with gemcitabine-based chemotherapy for the treatment of pancreatic cancer. J Clin Oncol. 2010;28(12):2058–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.7 of the Best Coffees for Enemas Reviewed. (https://enemacoffeereview.com) (2018). Accessed September 16, 2019. [Google Scholar]
- 9.Jones LE, Norris WE. Rectal burn induced by hot coffee enema. Endoscopy. 2010;42(Suppl 2):E26. [DOI] [PubMed] [Google Scholar]
- 10.Sashiyama H, Hamahata Y, Matsuo K, et al. Rectal burn caused by hot-water coffee enema. Gastrointest Endosc. 2008;68(5):1008–9. [DOI] [PubMed] [Google Scholar]
- 11.Kim S, Cha J, Lee C, et al. Rectal perforation due to benign stricture caused by rectal burns associated with hot coffee enemas. Endoscopy 2012;44(Suppl 2):E32–3. [DOI] [PubMed] [Google Scholar]
- 12.Keum B, Jeen YT, Park SC, et al. Proctocolitis caused by coffee enemas. Am J Gastroenterol. 2010;105(1):229–30. [DOI] [PubMed] [Google Scholar]
- 13.Lee CJ, Song SK, Jeon JH, et al. Coffee enema induced acute colitis. Korean J Gastroenterol. 2008;52(4):251–4. [PubMed] [Google Scholar]
- 14.Seo CH, Kim YH. A case of coffee enema-induced colitis. J Korean Soc Coloproctocol. 2009;25(3):193. [Google Scholar]
- 15.Noguchi K, Matsuzaki T, Sakanashi M, et al. Effect of caffeine contained in a cup of coffee on microvascular function in healthy subjects. J Pharmacol Sci. 2015;127:217–22. [DOI] [PubMed] [Google Scholar]
- 16.Echeverri D, Montes FR, Cabrera M, Galán A, Prieto A. Caffeine's vascular mechanisms of action. Int J Vasc Med. 2010;2010:834060–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Odashima M, Bamias G, Rivera-Nieves J, et al. Activation of A2A adenosine receptor attenuates intestinal inflammation in animal models of inflammatory bowel disease. Gastroenterology. 2005;129(1):26–33. [DOI] [PubMed] [Google Scholar]
- 18.Knight Commission on Trust, Media and Democracy. Crisis in Democracy: Renewing Trust in America. (https://knightfoundation.org/reports/crisis-in-democracy-renewing-trust-in-america) (2019). Accessed July 16, 2019. [Google Scholar]
- 19.Baron RJ, Berinsky AJ. Mistrust in science—a threat to the patient-physician relationship. N Engl J Med. 2019;381(2):182–5. [DOI] [PubMed] [Google Scholar]