

Abstract
Objectives:
The aim of this study is to compare the depth of cure of two composite materials (SDR and Filtek bulk-fill) cured at variable increment depths (2, 4, and 6 mm) and voltages (180 and 220 volts).
Materials and Methods:
Each sample of the composite material was packed in a mold of 2 mm, 4 mm, and 6 mm and curing light (quartz tungsten halogen) of optimal intensity was exposed for 20 s at 2 different voltages on each specimen. After curing, the specimens were removed and the composite on the nonexposed end was scraped with a plastic instrument. The remaining composite thickness was measured using a digital Vernier caliper. The reading was divided by half to follow the ISO 4049 method. Independent sample t-test, one-way ANOVA, and linear regression analysis were applied. Level of significance was kept at 0.01.
Results:
The mean DOC of SDR and Filtek were 1.93 ± 0.82 and 1.77 ± 0.65 mm. Lowering the voltage from 220 to 180 volts reduced the depth of Filtek from 1.87 ± 0.74 to 1.67 ± 0.54 mm, whereas the DOC of SDR remained unchanged at 1.93 mm at the two voltages. The adjusted R2 for the depth of cure was 0.93 when the increment thickness, voltage, and restorative material were taken together in the regression model.
Conclusions:
There was no statistically significant difference between SDR and Filtek for the depth of cure at 2 and 4 mm increments. However, at 6 mm increment, the SDR cured significantly deeper than the Filtek. Around 91% variation in the depth of cure of these composites materials is explained by increment thickness alone.
Keywords: Dental composite restoratives, depth of cure, polymerization
Introduction
Depth of cure of resin composites is essential for the clinical success of these materials. It has been observed that if the composite is inadequately polymerized, it results in poor development of its physical properties.[1] During polymerization of a composite restoration, shrinkage of the restorative material can occur as freely moving monomers get converted to highly cross-linked polymers. This polymerization shrinkage creates contraction stresses at tooth-restoration interface. The resultant volumetric contraction gives rise to unrelieved stresses and can eventually lead to sensitivity, marginal staining, and secondary caries.[2,3] All these can have catastrophic results on the longevity of the restoration. Factors such as matrix phase of the composite material,[4] amount of fillers loaded,[5] polymerization rate,[6] and the C factor of the cavity influence the magnitude of the polymerization contraction.
Light curing the posterior composite resin restorations is associated with the decrease in curing-light intensity with the depth of the material. It has been proven that the intensity of light at a given depth and for a given irradiance period is critical in monomer conversion, and is significantly associated with mechanical properties, biocompatibility, color stability of the material and thus, the longevity of the restoration.[7]
Many options have been proposed to overcome or minimize the shrinkage stresses that develop during polymerization. It has been recommended that composite resins should be placed in increments of 2-mm thickness and should be in contact with no more than two walls of the cavity preparation, to reduce the C-factor. However, it has been observed that polymerization shrinkage stresses still develop regardless of the technique employed and remains a significant factor in the failure of these types of restorations.[8] Applying a low-elastic modulus liner as the first increment between the tooth structure and the resin composite has also shown to minimize the internal stresses which develop while curing.[9] Other methods include selecting a particular type of curing light to decrease the shrinkage. Quartz tungsten halogen (QTH) light units have been widely used in dental offices, although newer LED type curing units are now more commonly available. To adequately cure a 2 mm increment of resin composite, a QTH light unit must deliver a minimum power intensity of 300–400 mW/cm2 in a 40 s cure.[10] However, if the restoration does not receive sufficient energy at the correct wavelength, the degree of conversion will remain inadequate; resulting in a weak restoration with poor mechanical properties.[11]
In the last few years, there has been a trend toward developing resin restorations which can save time during the placement step. The composition of these new materials has been altered in different ways to allow for the increased depth of curing while retaining the low shrinkage values.[12] Bulk-fill composites are one of the examples of these types of restorations. These have been developed with a promise of greater depth of cure because their clinical recommendations suggest that they can be placed in a 4-mm bulk increment.[13] An important limitation with conventional resin-based restorations was an increased treatment time due to the placement of restorative in increments and chances of incorporation of air or moisture contamination between increments. Bulk-fill flowable composites are supposed to save time and reduce the chances of air entrapment by allowing bulk cure. However, the flowable composite needs to be subsequently covered by a conventional composite on the occlusal aspect. Nevertheless, an ideal bulk-fill material would be one that could be placed into a cavity preparation with a high C-factor but would still exhibit very little polymerization shrinkage stress while maintaining a high degree of cure throughout the bulk of the restoration.
The first of these kind of composites introduced was SDR (Dentsply, USA), a posterior bulk-fill flowable base material which can be cured up to a depth of 4 mm. It has a photoactive group in a modified urethane dimethacrylate resin having 60%–70% less shrinkage when compared to other conventional methacrylate-based resins.[14] SDR is available in one universal shade, and it has to be overlaid with a posterior composite for replacing missing occlusal/facial enamel after the initial increment. SDR is also said to have a self-leveling feature that allows it to intimately adapt to the prepared cavity walls, whereas Filtek bulk-fill (3M-ESPE, USA) lacks this feature.[15] Literature suggests that polymerization stresses for SDR composites are considerably lower than that of other flowable materials.[16] Filtek bulk-fill is available in four different shades, i.e., A1, A2, A3, and universal with filler loading of 42% by volume.[17]
Bulk-fill flowable composites are generally recommended for use as base/liner underclass I and II restorations. They can also be used exclusively for Class III and V restorations. Mostly, they are used as core build-up materials when at least half of the coronal tooth structure is remaining to provide structural support to the tooth for the crown preparation. At present, there is a growing trend toward the use of bulk-fill materials among clinicians due to simplified protocol. However, because of the lower mechanical properties of most bulk-fill composites, their use as primary restorations under high occlusal load is controversial.[18]
In addition to the intensity and voltage of the curing units,[19] the exposure time and wavelength of the light determine the depth of cure. The type of photoinitiator incorporated in the composite material,[20] the shade of the resin,[21] the size of filler particles as well as the amount of filler present, the thickness of the restorative increment, the viscosity of the composite[22] are also important.
The objective of this study was to compare the mean depth of cure of two composite materials (SDR and Filtek bulk-fill) cured at incremental depth of 2, 4, and 6 mm as determined by the ISO 4049 method at 2 different voltages, i.e., 180 and 220 volts.
The null hypothesis was that there would be no significant difference in the mean depth of cure of the two materials, i.e., SDR and Filtek bulk-fill.
Materials and Methods
Since it was an in vitro study done on composites, Ethics Review Committee exemption was sought. No ethical considerations were present in this in vitro study. The study was conducted in Dec 2016 at the dental clinics in Aga Khan Hospital, Karachi, Pakistan.
The sampling technique was simple random. Inclusion criteria were SDR (Dentsply, USA) and Filtek bulk-fill (3M, ESPE, USA) flowable composite materials. Whereas any damaged, improperly cured or expired material was excluded from the study. The sample size was calculated using a statistical calculator “Sample Size Determination in Health Studies, WHO.” Reference for sample size calculation was taken from the study of Garoushi et al.[17] who reported that the mean depth of cure of cure of SDR to be 4.30 mm (±0.30) and for Filtek bulk-fill to be 4.7 mm (±0.15). Keeping this difference at the level of significance of 0.01 and power of study at 0.99, our sample size per group turned out to be 28, which was inflated to 42 composites per group.
Each sample of the composite material (SDR and bulk-fill) was packed in a mold of 2, 4, and 6 mm. The curing light (QTH) of optimal intensity was exposed for 20 s at 220 volts over each sample, after which the specimen was taken out of the mold. The composite on the nonexposed end was scraped with a flat plastic instrument using gentle force. This remaining material was measured using a digital Vernier caliper. The reading was divided by half to follow the ISO 4049 method of measuring the depth of cure. Three readings per sample were generated and their mean was taken. The same procedure was repeated with 180 volts. A voltage converter was used to step-down the voltage. The study flow diagram is depicted in Figure 1 and armamentarium is shown in Figures 2 and 3.
Figure 1.
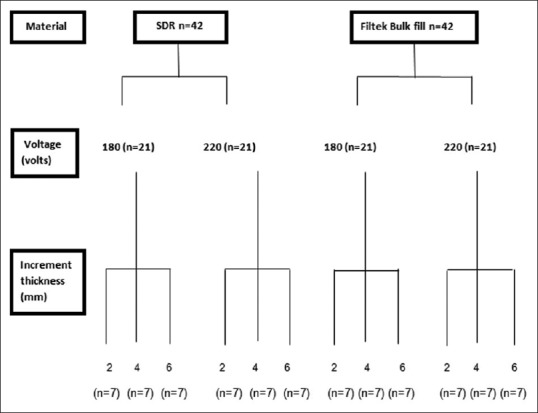
Study flow diagram
Figure 2.
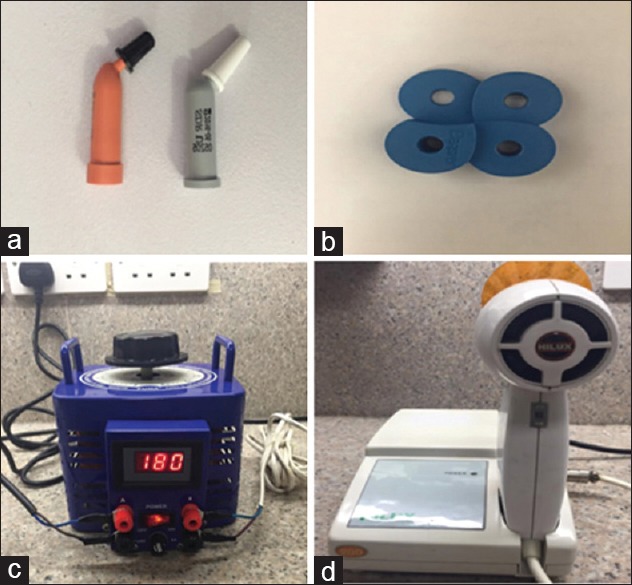
Armamentarium of the experiment. (a) Capsules of the Filtek bulk-fill and SDR restorative material. (b) Plastic molds for packing composites (2, 4, 6, 8 mm depth). (c) Voltage converter. (d) Quartz-Tungten– Halogen curing light
Figure 3.
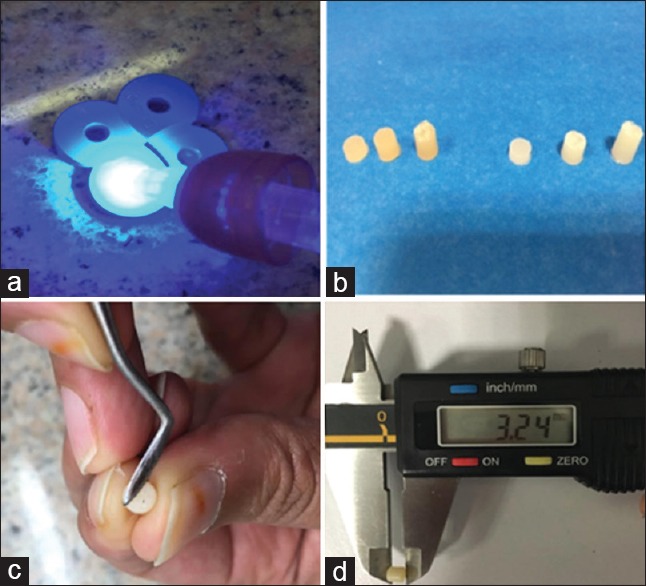
Data collection steps. (a) Curing the composite increment. (b) Cured samples of SDR and Filtek bulk-fill 2, 4 and 6 mm. (c) Scraping the composite according to the ISO 4049 method. (d) Measuring the depth of cure with a digital vernier caliper
Data analysis
SPSS version 20.0 (IBM SPSS Statistics software, New York, USA) was used for data analysis. Mean and standard deviation of continuous variable, i.e., the depth of cure (in mms) were computed. Independent sample t-test and factorial design ANOVA were applied to compare the depth of cure of the two composites at different voltages and increment thickness, respectively. Linear regression analysis was applied treating the depth of cure as an outcome variable. The level of significance was kept at 0.01.
Results
Table 1 describes the depth of cure of the two materials at increment thicknesses of 2, 4, and 6 mm. At 2 mm, both SDR and Filtek cured to a mean depth of cure of 0.95 ± 0.03 mm. At 4 mm, SDR cured to a mean depth of 1.93 ± 0.04, whereas Filtek cured till 1.86 ± 0.26 mm. At 6 mm increment thickness, SDR cured to 2.92 ± 0.05 mm, whereas Filtek bulk-fill cured to a mean depth of 2.43 ± 0.29 mm. At 6-mm depth, the difference between the mean curing depths of the two restoratives came out to be statistically significant [Figure 4].
Table 1.
Depth of cure of the two materials at variable increment thickness
| Increment thickness | Composite | n | Mean DOC (mm) | SD | P |
|---|---|---|---|---|---|
| 2 mm | SDR | 14 | 0.95 | 0.03 | 0.95 |
| Filtek | 14 | 0.95 | 0.03 | ||
| 4 mm | SDR | 14 | 1.93 | 0.04 | 0.62 |
| Filtek | 14 | 1.86 | 0.26 | ||
| 6 mm | SDR | 14 | 2.92 | 0.05 | <0.01 |
| Filtek | 14 | 2.43 | 0.29 |
ANOVA was applied, DOC: Depth of cure assessed with ISO 4049 method and digital vernier caliper; SDR: Smart dentine replacement; SD: Standard deviation
Figure 4.
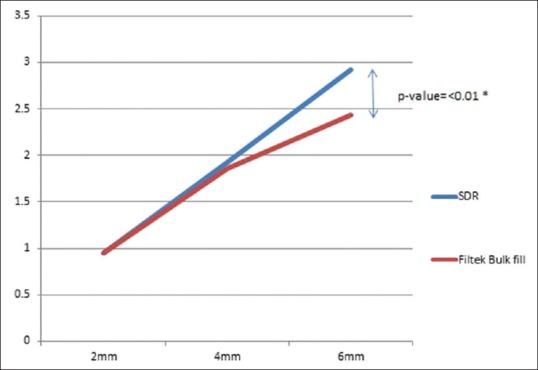
Depth of cure of the two materials at variable increment thickness. *Independent sample t-test reveals a statistically significant difference at 6 mm increment
Table 2 shows the depth of cure of the two composites at 180 and 220 volts at different increment thicknesses. Table 3 shows the linear regression analysis. Increment thickness, voltage, and composite type accounted for 93% variation in the depth of cure, whereas increment thickness and voltage accounted for 92% variation in the depth of cure. Increment thickness alone accounted for 91% variation in depth of cure of the composites.
Table 2.
Depth of cure at variable voltage and increment thickness
| Voltage (volts) | Composite | Increment thickness | n | Mean DOC (mm) | SD | P |
|---|---|---|---|---|---|---|
| 180 | SDR | 2 | 7 | 0.95 | 0.02 | 0.51 |
| 4 | 7 | 1.95 | 0.41 | |||
| 6 | 7 | 2.89 | 0.04 | |||
| Filtek | 2 | 7 | 0.95 | 0.04 | ||
| 4 | 7 | 1.88 | 0.08 | |||
| 6 | 7 | 2.17 | 0.05 | |||
| 220 | SDR | 2 | 7 | 0.94 | 0.04 | |
| 4 | 7 | 1.92 | 0.04 | |||
| 6 | 7 | 2.96 | 0.03 | |||
| Filtek | 2 | 7 | 0.94 | 0.04 | ||
| 4 | 7 | 1.84 | 0.36 | |||
| 6 | 7 | 2.70 | 0.12 |
Factorial design ANOVA was applied; DOC: Depth of cure (mm); SD: Standard deviation; SDR: Smart dentine replacement
Table 3.
Regression analysis
| Model | R | R2 | Adjusted R2 | SE |
|---|---|---|---|---|
| Increment thickness | 0.95 | 0.91 | 0.91 | 0.22 |
| Increment thickness + voltage | 0.95 | 0.92 | 0.92 | 0.22 |
| Increment thickness + voltage + composite type | 0.96 | 0.93 | 0.93 | 0.22 |
Linear regression analysis was applied, DOC was taken as outcome variable. SE: Standard error; DOC: Depth of cure (mm)
Discussion
ISO 4049 method was used to assess the depth of cure in this study. Several other methods are also available for testing the depth of cure. These include employing with microhardness tests, scraping, and visual inspection. Infrared spectroscopy and laser are considered as direct methods.[23] ISO 4049 is a scraping test and is of qualitative nature where to be tested resin composite is first filled in a mold and then light cured. After curing, it is pushed out of the mold, and the uncured resin composite material on the bottom is then scraped with some instrument leaving a hard specimen. After scraping, the final measurements are taken and divided by 2. The resulting value is recorded as the depth of cure and represents the maximum set material. The rationale for dividing by two is that not all the hardened specimen is actually optimally cured. However, overestimation of the depth of cure is likely to occur with this method compared to the other methods.
Flury et al. studied four flowable composites and concluded that for bulk-fill materials the ISO 4049 method overestimated the depth of cure compared to Vickers hardness profiles.[24] Moore et al. performed a study on flowable, hybrid and packable composites of different shades and also concluded that the ISO 4049 method overestimates the depth of cure.[25] Nevertheless, this test is fairly simple to perform as no special equipment is needed and it's inexpensive; that is why it is commonly used in the assessment of the depth of cure.[26]
The study showed no significant differences of depth of cure among the two composites, i.e., SDR and Filtek bulk-fill flowable at 2 and 4 mm. However, at 6-mm bulk SDR cured significantly better than Filtek bulk-fill. Possible explanation for this observation could be the lighter shade of SDR compared to Filtek bulk-fill. The translucency of dental materials is affected by the difference in the refractive indices between the filler particles and the resin matrix which determines how light is scattered within the material.[27,28] Garoushi et al. employed ISO 4049 method to measure depth of cure composite in 10-mm cylinders. They observed for SDR, it was 4.3 ± 0.30 mm and for Filtek bulk-fill, it was 4.7 ± 0.15 mm.[17]
The greater depth of cure of the bulk-fill composites might be attributed to more efficient initiator systems and higher translucency of these composites.[24] Depth of cure of bulk-fill materials vary with translucency and viscosity, both of which depend on the filler content.[29] Finan et al. assessed the depth of cure of bulk-fill composites using three different techniques, i.e., Vickers hardness number, Fourier transform infrared spectroscopy, biaxial flexure strength, and concluded that bulk-fill flowable composite bases have a depth of cure over 4 mm.[30] Goracci et al.[31] and Campos et al.[32] also revealed that bulk-fill variety of flowable composite can predictably be cured beyond 4 mm. Jang et al.[33] showed that although SDR cured adequately at 4 mm but underwent considerable shrinkage compared to control material.
Garcia et al.[34] reported the mean depth of cure of SDR composites was 5.01 ± 0.03 mm using the ISO scraping method. They used 10 composite samples of 10 mm molds and cured for 20s. Alrahlah et al.[35] studied the depth of cure of bulk-fill composites and found out that Filtek bulk-fill cured to a depth of 4.14 ± 0.28 mm as determined by Vickers hardness profiles. Alshali[36] showed that the degree of conversion SDR was better than the Filtek bulk-fill at 24 h postcure period.
In the present study, both composites cured less deep at 180 volts than at an optimal voltage of 220 volts. However, the difference was not statistically significant. At both voltages, SDR performed better than Filtek bulk-fill. Appropriate curing light intensity and voltage are known as critical factors in the degree of conversion of the composite resins. The distance between the curing light tip and the composite material is also crucial.[37] In a study done on microhybrid composites, the influence of voltage and thickness was nearly 62% on the depth of cure.[26] However, in the present study where bulk-fill flowable composites are used, these two variables had 93% impact on the depth of cure. This reveals that voltage fluctuation has no significant bearing on the depth of cure in bulk-fill materials. As electrical voltage fluctuation is a frequent observation in developing countries such as Pakistan, this has an important implication on the performance and longevity of bulk-fill composites.
QTH light was used in this study as it is more commonly available, and the investigators wanted to see the relationship of voltage drop which cannot be assessed by LED types of lights. Dunn and Bush[38] demonstrated that QTH type curing units resulted in significantly harder top and bottom surfaces of the resin-based composite than did the LED units. Jandt et al.[39] confirmed that the mean depth of cure is 20% deeper among composite exposed with QTH light than achieved with LED unit.
The limitations of the present study are that only two varieties of bulk-fill restorative materials were compared. Only QTH light was used. No thermo-cycling was done; lack of which removes the effects of mechanical and thermal stresses that are otherwise inevitable in the oral environment and finally, only ISO 4049 method was employed to assess the depth of cure.
Conclusions
No statistically significant difference was seen between SDR and Filtek bulk-fill for the depth of cure at 2 and 4 mm increments. At 6 mm increment, however, SDR cured significantly deeper than the Filtek bulk-fill
SDR showed the consistently better depth of cure at lowered voltage compared to Filtek bulk-fill
Of all variables, increment thickness has the greatest effect on depth of cure while changes in voltage have a minimal bearing on the depth of cure.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Ferracane JL, Mitchem JC, Condon JR, Todd R. Wear and marginal breakdown of composites with various degrees of cure. J Dent Res. 1997;76:1508–16. doi: 10.1177/00220345970760081401. [DOI] [PubMed] [Google Scholar]
- 2.Anusavice KJ, Shen C, Rawls HR. Phillips' Science of Dental Materials. Toronto: Elsevier Health Sciences; 2013. [Google Scholar]
- 3.Peutzfeldt A. Resin composites in dentistry: The monomer systems. Eur J Oral Sci. 1997;105:97–116. doi: 10.1111/j.1600-0722.1997.tb00188.x. [DOI] [PubMed] [Google Scholar]
- 4.Guggenberger R, Weinmann W. Exploring beyond methacrylates. Am J Dent. 2000;13:82D–4D. [PubMed] [Google Scholar]
- 5.Labella R, Lambrechts P, Van Meerbeek B, Vanherle G. Polymerization shrinkage and elasticity of flowable composites and filled adhesives. Dent Mater. 1999;15:128–37. doi: 10.1016/s0109-5641(99)00022-6. [DOI] [PubMed] [Google Scholar]
- 6.Feilzer AJ, Dooren LH, de Gee AJ, Davidson CL. Influence of light intensity on polymerization shrinkage and integrity of restoration-cavity interface. Eur J Oral Sci. 1995;103:322–6. doi: 10.1111/j.1600-0722.1995.tb00033.x. [DOI] [PubMed] [Google Scholar]
- 7.Fan PL, Schumacher RM, Azzolin K, Geary R, Eichmiller FC. Curing-light intensity and depth of cure of resin-based composites tested according to international standards. J Am Dent Assoc. 2002;133:429–34. doi: 10.14219/jada.archive.2002.0200. [DOI] [PubMed] [Google Scholar]
- 8.Oliveira LC, Duarte S, Jr, Araujo CA, Abrahão A. Effect of low-elastic modulus liner and base as stress-absorbing layer in composite resin restorations. Dent Mater. 2010;26:e159–69. doi: 10.1016/j.dental.2009.11.076. [DOI] [PubMed] [Google Scholar]
- 9.Choi KK, Condon JR, Ferracane JL. The effects of adhesive thickness on polymerization contraction stress of composite. J Dent Res. 2000;79:812–7. doi: 10.1177/00220345000790030501. [DOI] [PubMed] [Google Scholar]
- 10.Shortall AC, Harrington E. Effect of light intensity on polymerisation of three composite resins. Eur J Prosthodont Restor Dent. 1996;4:71–6. [PubMed] [Google Scholar]
- 11.Lee SY, Greener EH. Effect of excitation energy on dentine bond strength and composite properties. J Dent. 1994;22:175–81. doi: 10.1016/0300-5712(94)90202-x. [DOI] [PubMed] [Google Scholar]
- 12.Al-Mansour K, Al-Sada A, Al-Sinan H. Curing depth of bulk-fill composites – An in vitro study. Pak Oral Dent J. 2015;35:270–4. [Google Scholar]
- 13.Van Ende A, De Munck J, Van Landuyt KL, Poitevin A, Peumans M, Van Meerbeek B, et al. Bulk-filling of high C-factor posterior cavities: Effect on adhesion to cavity-bottom dentin. Dent Mater. 2013;29:269–77. doi: 10.1016/j.dental.2012.11.002. [DOI] [PubMed] [Google Scholar]
- 14.Jin X, Bertrand S, Hammesfahr P. New radically polymerizable resins with remarkably low curing stress. J Dent Res. 2009;88:1651. [Google Scholar]
- 15.Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ, et al. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent. 2012;40:500–5. doi: 10.1016/j.jdent.2012.02.015. [DOI] [PubMed] [Google Scholar]
- 16.Ilie N, Hickel R. Investigations on a methacrylate-based flowable composite based on the SDR™ technology. Dent Mater. 2011;27:348–55. doi: 10.1016/j.dental.2010.11.014. [DOI] [PubMed] [Google Scholar]
- 17.Garoushi S, Säilynoja E, Vallittu PK, Lassila L. Physical properties and depth of cure of a new short fiber reinforced composite. Dent Mater. 2013;29:835–41. doi: 10.1016/j.dental.2013.04.016. [DOI] [PubMed] [Google Scholar]
- 18.Leprince JG, Palin WM, Vanacker J, Sabbagh J, Devaux J, Leloup G, et al. Physico-mechanical characteristics of commercially available bulk-fill composites. J Dent. 2014;42:993–1000. doi: 10.1016/j.jdent.2014.05.009. [DOI] [PubMed] [Google Scholar]
- 19.Taira M, Urabe H, Hirose T, Wakasa K, Yamaki M. Analysis of photo-initiators in visible-light-cured dental composite resins. J Dent Res. 1988;67:24–8. doi: 10.1177/00220345880670010401. [DOI] [PubMed] [Google Scholar]
- 20.Ruyter IE, Oysaed H. Conversion in different depths of ultraviolet and visible light activated composite materials. Acta Odontol Scand. 1982;40:179–92. doi: 10.3109/00016358209012726. [DOI] [PubMed] [Google Scholar]
- 21.Ferracane JL, Aday P, Matsumoto H, Marker VA. Relationship between shade and depth of cure for light-activated dental composite resins. Dent Mater. 1986;2:80–4. doi: 10.1016/s0109-5641(86)80057-4. [DOI] [PubMed] [Google Scholar]
- 22.Hadis M, Leprince JG, Shortall AC, Devaux J, Leloup G, Palin WM, et al. High irradiance curing and anomalies of exposure reciprocity law in resin-based materials. J Dent. 2011;39:549–57. doi: 10.1016/j.jdent.2011.05.007. [DOI] [PubMed] [Google Scholar]
- 23.Aguiar FH, Braceiro A, Lima DA, Ambrosano GM, Lovadino JR. Effect of light curing modes and light curing time on the microhardness of a hybrid composite resin. J Contemp Dent Pract. 2007;8:1–8. [PubMed] [Google Scholar]
- 24.Flury S, Hayoz S, Peutzfeldt A, Hüsler J, Lussi A. Depth of cure of resin composites: Is the ISO 4049 method suitable for bulk fill materials? Dent Mater. 2012;28:521–8. doi: 10.1016/j.dental.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 25.Moore BK, Platt JA, Borges G, Chu TM, Katsilieri I. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Oper Dent. 2008;33:408–12. doi: 10.2341/07-104. [DOI] [PubMed] [Google Scholar]
- 26.Khan FR, Hasan M, Azam SI. The effect of different shades, voltages and increment thickness on the polymerization depth of a microhybrid composite. Int J Prosthodont Restor Dent. 2012;2:52–6. [Google Scholar]
- 27.Shortall AC, Palin WM, Burtscher P. Refractive index mismatch and monomer reactivity influence composite curing depth. J Dent Res. 2008;87:84–8. doi: 10.1177/154405910808700115. [DOI] [PubMed] [Google Scholar]
- 28.Lee YK, Lu H, Powers JM. Measurement of opalescence of resin composites. Dent Mater. 2005;21:1068–74. doi: 10.1016/j.dental.2005.03.015. [DOI] [PubMed] [Google Scholar]
- 29.Yap AU, Pandya M, Toh WS. Depth of cure of contemporary bulk-fill resin-based composites. Dent Mater J. 2016;35:503–10. doi: 10.4012/dmj.2015-402. [DOI] [PubMed] [Google Scholar]
- 30.Finan L, Palin WM, Moskwa N, McGinley EL, Fleming GJ. The influence of irradiation potential on the degree of conversion and mechanical properties of two bulk-fill flowable RBC base materials. Dent Mater. 2013;29:906–12. doi: 10.1016/j.dental.2013.05.008. [DOI] [PubMed] [Google Scholar]
- 31.Goracci C, Cadenaro M, Fontanive L, Giangrosso G, Juloski J, Vichi A, et al. Polymerization efficiency and flexural strength of low-stress restorative composites. Dent Mater. 2014;30:688–94. doi: 10.1016/j.dental.2014.03.006. [DOI] [PubMed] [Google Scholar]
- 32.Campos EA, Ardu S, Lefever D, Jassé FF, Bortolotto T, Krejci I, et al. Marginal adaptation of class II cavities restored with bulk-fill composites. J Dent. 2014;42:575–81. doi: 10.1016/j.jdent.2014.02.007. [DOI] [PubMed] [Google Scholar]
- 33.Jang JH, Park SH, Hwang IN. Polymerization shrinkage and depth of cure of bulk-fill resin composites and highly filled flowable resin. Oper Dent. 2015;40:172–80. doi: 10.2341/13-307-L. [DOI] [PubMed] [Google Scholar]
- 34.Garcia D, Yaman P, Dennison J, Neiva G. Polymerization shrinkage and depth of cure of bulk fill flowable composite resins. Oper Dent. 2014;39:441–8. doi: 10.2341/12-484-L. [DOI] [PubMed] [Google Scholar]
- 35.Alrahlah A, Silikas N, Watts DC. Post-cure depth of cure of bulk fill dental resin-composites. Dent Mater. 2014;30:149–54. doi: 10.1016/j.dental.2013.10.011. [DOI] [PubMed] [Google Scholar]
- 36.Alshali RZ, Silikas N, Satterthwaite JD. Degree of conversion of bulk-fill compared to conventional resin-composites at two time intervals. Dent Mater. 2013;29:e213–7. doi: 10.1016/j.dental.2013.05.011. [DOI] [PubMed] [Google Scholar]
- 37.Rueggeberg FA, Caughman WF, Curtis JW, Jr, Davis HC. Factors affecting cure at depths within light-activated resin composites. Am J Dent. 1993;6:91–5. [PubMed] [Google Scholar]
- 38.Dunn WJ, Bush AC. A comparison of polymerization by light-emitting diode and halogen-based light-curing units. J Am Dent Assoc. 2002;133:335–41. doi: 10.14219/jada.archive.2002.0173. [DOI] [PubMed] [Google Scholar]
- 39.Jandt KD, Mills RW, Blackwell GB, Ashworth SH. Depth of cure and compressive strength of dental composites cured with blue light emitting diodes (LEDs) Dent Mater. 2000;16:41–7. doi: 10.1016/s0109-5641(99)00083-4. [DOI] [PubMed] [Google Scholar]