

Abstract
Background
The gamification of digital health provisions for older adults (eg, for rehabilitation) is a growing trend; however, many older adults are not familiar with digital games. This lack of experience could cause stress and thus impede participants’ motivations to adopt these technologies.
Objective
This crossover longitudinal multifactorial study aimed to examine the interactions between game difficulty, appraisal, cognitive ability, and physiological and cognitive responses that indicate game stress using the Affective Game Planning for Health Applications framework.
Methods
A total of 18 volunteers (mean age 71 years, SD 4.5; 12 women) completed a three-session study to evaluate different genres of games in increasing order of difficulty (S1-BrainGame, S2-CarRace, and S3-Exergame). Each session included an identical sequence of activities (t1-Baseline, t2-Picture encode, t3-Play, t4-Stroop test, t5-Play, and t6-Picture recall), a repeated sampling of salivary cortisol, and time-tagged ambulatory data from a wrist-worn device. Generalized estimating equations were used to investigate the effect of session×activity or session×activity×cognitive ability on physiology and cognitive performance. Scores derived from the Montreal Cognitive Assessment (MoCA) test were used to define cognitive ability (MoCA-high: MoCA>27, n=11/18). Kruskal-Wallis tests were used to test session or session×group effects on the scores of the postgame appraisal questionnaire.
Results
Session×activity effects were significant on all ambulatory measures (χ210>20; P<.001) other than cortisol (P=.37). Compared with S1 and S2, S3 was associated with approximately 10 bpm higher heart rate (P<.001) and approximately 5 muS higher electrodermal activity (P<.001), which were both independent of the movement caused by the exergame. Compared with S1, we measured a moderate but statistically significant drop in the rate of hits in immediate recall and rate of delayed recall in S3. The low-MoCA group did not differ from the high-MoCA group in general characteristics (age, general self-efficacy, and perceived stress) but was more likely to agree with statements such as digital games are too hard to learn. In addition, the low-MoCA group was more likely to dislike the gaming experience and find it useless, uninteresting, and visually more intense (χ21>4; P<.04). Group differences in ambulatory signals did not reach statistical significance; however, the rate of cortisol decline with respect to the baseline was significantly larger in the low-MoCA group.
Conclusions
Our results show that the experience of playing digital games was not stressful for our participants. Comparatively, the neurophysiological effects of exergame were more pronounced in the low-MoCA group, suggesting greater potential of this genre of games for cognitive and physical stimulation by gamified interventions; however, the need for enjoyment of this type of challenging game must be addressed.
Keywords: silver gaming, serious games, stress, cognitive training, brain training games, exercise games, ICT
Introduction
Background
Playing digital games is quickly becoming a common pastime for many older adults [1,2]. Games are pleasurable activities when they offer a balanced mixture of challenge, reward, and competition. Playing games together is a social activity that may mitigate feelings of isolation. Playing games alone offers relaxation and distraction. Digital games have several potential advantages: they may offer higher sensory stimulation by their visual and sound effects; they may challenge executive and motor skills, visual attention, and speed of reaction in decision making; and they can also be customized in interface or level of difficulty. Research indicates that many older adults are onboard with serious digital play [3-7]. To develop serious games (ie, games in which the intention is to benefit tangibly from game play and attempt to deliver cognitive, emotional, or rehabilitation training to older adults) is a growing trend [8-15].
Although emerging data suggest that digital playing can improve cognitive, physical, and emotional health in older adults [16-23], the results are not conclusive. Currently, there are two dominant research streams addressing the complexity of developing serious games for seniors: (1) game designers evaluate the effectiveness of a game in terms of accessibility and meaningful and enjoyable play [6,24-32], and (2) health researchers focus mainly on their cognitive [33-36] or specific motor-related effects [19,25,37-49] in controlled trials. An empirical framework to evaluate the efficacy of different game-based health interventions that bridges these two fields is much needed [50,51].
At present, the inadequate design of computer games and low accessibility of game technologies are the major impediments to their adoption by seniors [42,52,53]. Successful games foster time-on-task and promote more effective learning because they raise motivation and arouse players’ interest, for instance, by providing instantaneous and informative feedback, intrinsic rewards, and features that allow players to self-assess and adjust the levels of game difficulty to their skills [54]. These neurological signals may transfer to positive psychological effects such as enjoyment and challenge resulting from gameplaying [55]. Several studies have shown that in general, more seniors prefer the ease and pleasure of casual games (preferably with an intellectual component) over more cognitively demanding action games [3,56,57]. However, interindividual variations in game perception and motivation are important factors that engender the game-playing experience [58,59]. Thus, while digital games are increasingly prevalent among the seniors who are offered access to digital devices, many seniors are not familiar with or accustomed to digital game playing. As such, the mere promise of functional enhancement through such activities may not suffice to motivate them to overcome the barriers of unfamiliarity with the technology, if they have access to that technology. Inserting a for-health computerized intervention, even if ludic, may still introduce stress either because it seems too difficult to master and thus underlines their disabilities, or because it is an unfamiliar and burdensome imposition on their lifestyle. Therefore, it is important to ask whether the adoption of proscribed gamified interventions for older adults may be too stressful.
Objectives
This study aimed to address the question on whether the adoption of proscribed gamified interventions for older adults may be too stressful. To that end, a hybrid data/model-driven mixed methods framework for Affective Game Planning for Health Applications (AGPHA) was proposed [60]. AGPHA builds on the theory of appraisal and coping by Lazarus (summarized in Figure 1) and emphasizes that motivational, relational, and cognitive factors determine individual differences in perception of, and ability to cope with, new challenges (for an ontology by Lazarus, see [61]). These differences may manifest as quantifiable variations in the stress system of the body, including marked changes in cortisol response and autonomic signals such as heart rate (HR), skin conductance, and gut reflexes. These physiological reactions are the body’s nonspecific response to the perception of stress [62], and usually the intensity of these responses depends on an individual’s biological and psychological coping resources [63].
Figure 1.
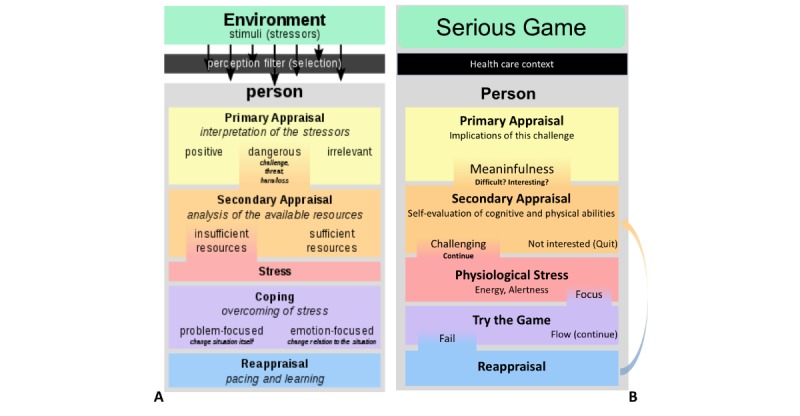
(A) Diagram of Lazarus and Folkman’s Transactional Theory of Stress (Source: Wikipedia, Philipp Guttmann), (B) our adaptation of Lazarus’s model to be tested in the Affective Game Planning for Health Applications framework.
Figure 1 shows our adaptation of the theory by Lazarus [61]. When presented with a challenge, an individual’s primary appraisal determines its relevance, threat, and benefits. If it is irrelevant, the individual can ignore it. If it is threatening, they have to respond to it. If the challenge is beneficial, they may choose to respond to it. In case of games for health, the challenge is not threatening to one’s health, but if the games are introduced in the context of health care or cognitive fitness, they can be challenging to an individual’s self-esteem because the player may feel pressured to learn the game and perform well. How an individual responds to the game challenge will depend on the individual’s coping style and their cognitive, emotional, or physiological reserves. If they have a negative attitude toward the game, they might avoid it, or feel stressed by trying it. However, if they have a positive attitude, or an investment (such as expectation that it will improve cognitive function), then they will try to learn and overcome the challenges of the game. This is when the player enters the secondary stage of appraisal. In the secondary stage of appraisal, if the challenge is feasible, then the player may experience what is termed as flow; otherwise, it becomes stressful. Again, at the secondary appraisal, the personality and cognitive and physical reserves of the individual play a role in moderating the magnitude of the stress response and the behavioral outcome (in this case, playing further or giving up).
In the context of gamified strategies for cognitive training or testing, the complex relationship between stress and cognition deserves attention. It is well established that physiological stress responses modulate the function of central cognitive structures such as the hippocampus and the prefrontal cortex [64,65]. Stress interferes with learning through myriad cognitive processes, especially attention, reward processing, and decision making [66,67], which are important for habitual and complex activities that define an individual’s adaptation strategies in the course of life. Actual or perceived decline in cognitive abilities can influence a senior’s primary and secondary appraisal of the game and discourage them to try. Diminished cognitive abilities can make the game more challenging and thus lead to more pronounced physiological stress responses, which might cause health-related side effects that need to be monitored or avoided. It is also possible that excessive game stress would lead to distraction or memory failure, thereby impeding learning and skill development, which are important for motivation to replay.
Therefore, in evaluating whether games are stressful or not, AGPHA asks three central questions:
What are the characteristics of individuals who choose to play?
Is the playing experience quantifiably stressful?
Which intra- or intersubject factors (eg, appraisal, cognitive abilities, health status) predict variations in game-related stress, game-learning, and retention?
Study Aims and Hypotheses
In this study, we provide an example of deploying the AGPHA framework to investigate the relation between game stress and cognitive abilities of the senior game players, introduced to three unfamiliar gaming experiences. In this study, we have tested the following hypotheses:
Playing unknown digital games will be stressful to older adults.
Game difficulty and general cognitive abilities predict a quantifiable increase in reflexive (ie, variations caused in physiological or neuropsychological function) and reflective (ie, subjective evaluation of the postgame experience) stress responses.
This study includes the following elements: (1) a survey element to allow us to understand the biases related to individual characteristics that attract older adults to the topic of gamified cognitive enhancement, (2) a within-subject factor (three genres of presumably cognitive enhancing games: brain training, car racing, and exercise gaming) that allows us to introduce variations in the phenomenology of gaming experience, (3) a between-subject factor (cognitive ability determined by the Montreal Cognitive Assessment [MoCA]) that allows us to investigate intersubject variations in game experience, and (4) two categories of reflexive (cortisol, ambulatory signals, and neuropsychological tests) and reflective (postgame evaluation of the game-play experience based on intrinsic motivation) outcome measures that would allow us to compare the sensitivity of objective biomarkers against subjective ratings.
Methods
Participant Recruitment
We adopted a snowball survey method to recruit potential participants and assess the characteristics of seniors who showed interest in the topic of gamified approaches to cognitive enhancement. With approval from the institutional review board, we targeted a general mailing list of the PERFORM Centre; this list consisted of individuals interested in volunteering for preventative health studies. We invited individuals older than 65 years to participate in Finding Better Games for Older Adults: An Objective Assessment of Interactions Between Appraisal, Arousal and Cognitive Benefits of Electronic Playing. The recruitment period lasted approximately 2 months. The survey asked questions about how they evaluated game-related activities in relation to a range of other activities (eg, gaming vs exercising, or talking with people rather than playing). The survey also included the General Self-Efficacy Scale (a 10-item scale) [68]; University of California, Los Angeles (UCLA) Loneliness Scale [69]; and Perceived Stress Scale (9-item scale [70]) to control for confounding chronic stress or tendency to become more easily stressed. We also asked participants to self-evaluate their state of mental and physical wellness as good, bad, or could be better.
Study Sample
Those who completed the survey and could commit to three 120-min tests in our research facility were invited to participate in the follow-up experiments. On the basis of previous work [71], we estimated a sample of 20 participants sufficient to provide pilot data with 80% power to detect a difference of 0.17 (log [Cortisol nmol/mL]) in response to a psychological stress challenge between the study arms with an SD of 0.26 and one-tailed paired t test (P=.05, where more difficult games were expected to cause higher stress). We performed medical screening using the Physical Activity Readiness Questionnaire (PAR-Q+) to rule out hazards such as movement disorders that would increase the risk of falling, epileptic seizures, and visual impairments that would prohibit participants from playing digital games safely. Participants were required to be capable of walking continuously for 20 min; literate; and able to watch a television, a computer, and an iPad screen. Before participation, they signed an informed consent approved by the institutional ethics review board. They were free to discontinue the study at any moment. No financial compensation was offered.
Experimental Design
Aim 1 was to determine whether novel gaming experiences induce a psychophysiological stress response, and whether there is a relation between appraisal of the game experience and psychophysiological measures. Aim 2 was to determine whether differences in cognitive abilities predict variations in game-related stress. Cognitive abilities were assessed by MoCA Original 7.0, a 30-point standardized outcome measure that is used clinically to screen for milder forms of cognitive impairment [72].
Following the AGPHA framework, we collected multifactorial data to create a comprehensive profile of the emotional, cognitive, and biological characteristics of the participants. Table 1 summarizes data that we collected in the study. A semistructured interview—to assess the challenge, excitement, enjoyment, goals, and likelihood to play and replay a game—was also performed, but those results are beyond the scope of this paper and will be presented separately.
Table 1.
Study variables.
| Variable category and variable type | Screening | Baseline | Brain training | Car race | Dance | |
| Characteristics | ||||||
|
|
Demographics | ✓ | N/Aa | N/A | N/A | N/A |
|
|
UCLAb Loneliness Index | ✓ | N/A | N/A | N/A | N/A |
|
|
Perceived Stress Scale | ✓ | N/A | N/A | N/A | N/A |
|
|
General Self-Efficacy | ✓ | N/A | N/A | N/A | N/A |
|
|
Self-assessment of mental/physical health | ✓ | N/A | N/A | N/A | N/A |
|
|
Prestudy appraisal of game (IFc) | ✓ | N/A | N/A | N/A | N/A |
| Cognitive | ||||||
|
|
Montreal Cognitive Assessment (IF) | N/A | ✓ | N/A | N/A | N/A |
|
|
Picture Encode/recall (DVd) | N/A | N/A | ✓ | ✓ | ✓ |
|
|
Stroop (DV) | N/A | N/A | ✓ | ✓ | ✓ |
| Biometrics | ||||||
|
|
Heart rate and heart rate variability (DV) | N/A | ✓ | ✓ | ✓ | ✓ |
|
|
Electrodermal activity (DV) | N/A | ✓ | ✓ | ✓ | ✓ |
|
|
Accelerometer (CVe) | N/A | ✓ | ✓ | ✓ | ✓ |
|
|
Saliva cortisol (DV) | N/A | ✓ | ✓ | ✓ | ✓ |
| Subjective | ||||||
|
|
Postgame appraisal survey (DV/IVf) | N/A | N/A | ✓ | ✓ | ✓ |
|
|
STAI-6g (DV) | N/A | N/A | ✓ | ✓ | ✓ |
aN/A: not applicable.
bUCLA: University of California, Los Angeles.
cIF: independent factor.
dDV: dependent variable.
eCV: control variable.
fIV: independent variable.
gSTAI: Spielberger State-Trait Anxiety Inventory.
The experimental design was a repeated measures crossover study (Figure 2). Participants were fully informed about the intention of the study, and no deception was used:
Figure 2.
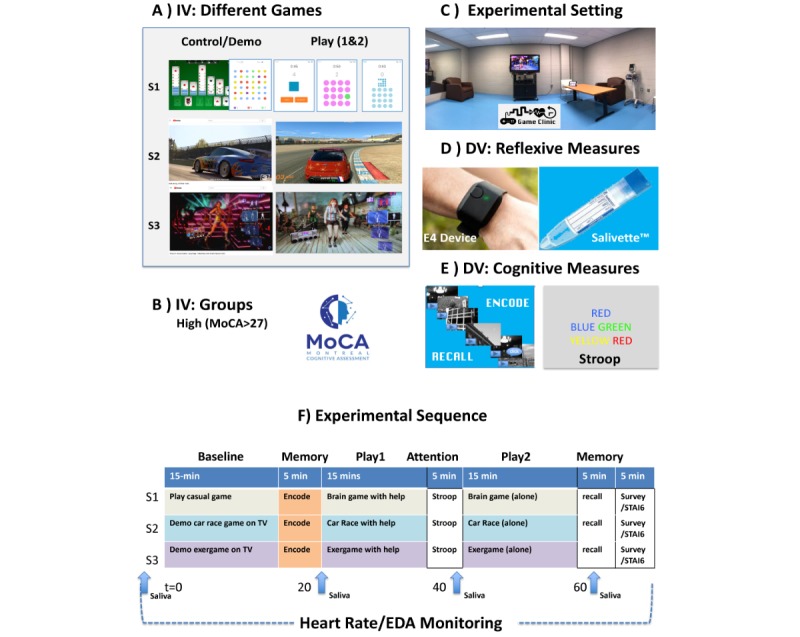
Experimental methods and procedure. (A) Different games that were used; (B) Montreal Cognitive Assessment tool was used as a predicting factor; (C) the experiment room, a small studio located at PERFORM Centre’s Gym; (D) devices used for measurement. DV: dependent variable; EDA: electrodermal activity; IV: independent variable; MoCA: Montreal Cognitive Assessment.
We would like to hear how you evaluate different games which are suggested to enhance cognitive function. We want to know how you appraise them in terms of fun, difficulty, or benefits. We will also collect physiological data using an arousal-sensing device that you will be wearing on your wrist and from saliva samples that let us know if the game stressed your body.
Because this was a repeated measures study, we expected that increased familiarity with our experimental setting would reduce their overall stress. For this reason, we presented the games in increasing degrees of complexity and difficulty. Identical functional assessments (cognitive tests) were incorporated to control for learning effects. This design, accounting for habituation, allowed us to use the first (and presumably the simplest game) as a reference against which to compare gradual changes in game appraisal and familiarity with the game.
Procedures
The study took place between 10 AM and 4 PM. Participants were asked to refrain from eating and drinking sweetened or caffeinated beverages or engaging in strenuous physical activity for at least 2 hours before their appointment at PERFORM. Each session was completed on separate days, with 3 to 7 days between visits. Each visit lasted about 2 hours. The details of the experimental procedure are presented in Multimedia Appendix 1. Briefly, session 1 served as the baseline as we introduced players to cognitive training games played on iPAD (MindGame, by Tom Lake). In session 2, we introduced a visually and cognitively more complex game, using an iPad (Real Racing 3, v 5.4.0, Electronic Arts Inc), which allowed players to steer the car using the gyroscopic features of the iPad and thus required minimal efforts in learning the control buttons. In session 3, we introduced an exergame (Dance Central by Harmonix, MS Studios). In this game, players copy the moves of a virtual choreographer while the motion tracking Kinect evaluates them against the queued movement.
Outcome Measures
Postgame Appraisal
To study the relation between the participant’s subjective appraisal of the gaming experience, we administered an exit survey at the end of each session, which was loosely based on the intrinsic motivation inventory and tapped into the question of enjoyment (The experience was enjoyable, The experience was interesting), competence (The game was difficult), tension (The experience was stressful; I found this to be a frustrating experience. These games are visually intense), choice (I liked to play this game again; I will play this game again. I did not like this experiment), and value (This game help improve my mental wellness, I think this game is useless; These games are cognitively stimulating). Instead of a 7-choice scale to measure degrees of satisfaction, we decided to implement a 4-choice response (definitely disagree, somewhat disagree, somewhat agree, and definitely agree), ranging from –2 to 2, but we allowed participants to add comments if they did not know the answer. We coded these responses to 0 or I don't know.
Saliva Cortisol
Saliva cortisol is often measured as a biomarker of a latent psychological modulation to the stress system [73]. Cortisol production displays a typical diurnal rhythm with a peak in the morning hours (8-10 AM), followed by a periodic pattern consisting of ultradian oscillations (20-120 min periods) [74,75]. We therefore ensured to schedule the visits at the same time for each individual, and we timed the experiment to avoid measuring the sharp rise in the awakening cortisol. Free circulating cortisol was assessed from saliva, collected using the Salivette device (Figure 2). The samples were frozen at −80°C, centrifuged at 4°C for 10 min, and analyzed using luminescence-immunoassay (IBL International) using enzyme-linked immunosorbent assay (at PERFORM Centre). The intra- and interassay coefficient variability was less than 12% and 5%, respectively.
Electrodermal Activity and Heart Rate Variability
Since 1970s, the electrodermal activity (EDA) and the heart rate variability (HRV) have been used as proxy markers of sympathetic autonomic response to arousing or stressful stimuli, finding successful application in laboratory experiments involving human-computer interface and games [76-82]. We used the E4 device (Empatica, Inc), a light wrist-wearable device for continuous monitoring of the physiological signals. The E4 band (Figure 2) was properly fit on the wrist of the nondominant arm. This device is equipped with 4 sensors: (1) photoplethysmography sensor to measure cardiac activity, (2) EDA sensor to measure skin conductance as a marker of arousal and stress, (3) 3-axis accelerometer (ACC) to measure the amount of movement along the x-, y-, and z-axes, and (4) optical thermometer to measure skin temperature.
To facilitate the replicability of our study, we downloaded preprocessed data from the Empatica data portal. We used our in-house MATLAB software on these data to extract data for each activity (by averaging signals’ amplitudes normalized to the duration of different activities). An activity denotes a specific interval measured from the onset of each experimental step. Activities were delimited using a tag button on the E4, which was pressed every time we administered a new task. A research assistant also kept track of detailed timing of the experiment. Because EDA is sensitive to the activity of sweat glands, the room temperature was maintained at 23°C. However, we also collected data from the temperature sensor and ACC on the E4 device to rule out confounding effects related to thermal or movement noise.
Stress-Sensitive Cognitive Tests
The triggering of physiological signals to stress serves the metabolic modulation of reward processing [83] and attention [84] systems that help individuals initiate an appropriate adaptive response to stress; thus, it can interfere with cognitive functions performed during or immediately after stress. We included a set of simple cognitive tasks to assess whether, despite the potential learning effect due to repeated nature of the design, increasing game difficulty would affect performance in cognitive tasks. The first set of cognitive tests used a picture encode/delayed recall memory test, which we have previously shown to be sensitive to stress modulations of the hippocampal function both under tasks [71] and under stress-inducing drug conditions [85]. In addition, we administered a simple Stroop word color test to assess an individual’s cognitive processing speed and their selective attention accuracy. The Stroop test has been shown to be sensitive to physical exertion and cognitive challenge [86,87]. All cognitive tests were presented at a minimal level of difficulty (with 3-second delay between stimuli) to ensure these tasks did not introduce added stress.
The encode/recall test consisted of two parts. In the first part (the encode condition), the participant was presented with 50 black and white images of random scenes, places, people, and objects. Each image stayed on screen for 3 seconds; thus, the participant had time to commit it to memory. This set of 50 pictures included 14 unique pictures and 36 nonunique pictures that were shown more than once. The participant was asked to press m as soon as they saw a familiar picture. They were told to remember these pictures for a recall test at the end of the session. In the second part (delayed recall), 45 black and white images were shown. This set included 15 pictures from the encode session and 30 new pictures. Participants were asked to press m as soon as they detected a previously seen picture. In both sessions, each picture remained on the screen for 3 seconds. If no answer was provided, the screen would proceed to the next picture. This test was implemented in E-Prime, and we recorded the number of hits, misses, and false alarms, both for the encode and the recall conditions. We had designed 3 sets of unique encode/recall pairs. In other words, none of the pictures seen in session 1 were repeated in the pictures presented in sessions 2 or 3.
We also wanted to measure the reaction time (RT) to the Stroop effect, that is the time it takes a player to process the incongruency between the color of a word read, and the color represented by the word. At each trial of this test, a brief training session was held to ensure the players understood the test objectives. Following the training session (1 min), a randomly selected color word (red, yellow, blue, or green) was presented to the participants. The color of the word on the screen may or may not have been congruent with the word itself. The stimuli (50) were randomly selected from a stack of 320 cards (80 of which were incongruent). The participants were asked to press a colored key on the keyboard, which was associated with the color of letters of the word, as fast as they could. In our implementation, we provided immediate feedback on whether the participants provided the correct answer or not. The participants were told that their scores would depend on how fast they responded to each card, but the time interval between cards was set to 5 seconds. The test was implemented in E-Prime, and we recorded the number of correct responses and the RT to correct response.
Statistical Analysis
Our research questions were as follows:
Can we detect within-subject game-related (ie, Session) differences in appraisal, physiological patterns over time (ie, ti: Activityi), and cognitive measures (immediate and delayed recall, and Stroop RT to correct)?
Do differences related to cognitive abilities (measured by MoCA) predict differences in outcome measures for different sessions (S1: Brain training; S2: CarRace; and S3: Exergame) and activities (t1: Baseline; t2: Encode; t3: Play1; t4: Stroop; t5: Play2; t6: Recall)?
To examine the effect of session×activity in each outcome measure, we used generalized estimating equations (GEEs) with a robust estimator and an autoregression working correlations matrix. GEE is a special form of the general linear model that is recommended for longitudinal repeated measurements of within-subject data over time [88]. In all GEE models, S1 and t1 were used as within-subject references. For the group comparisons, all physiological factors were normalized to the within-subject, within-session baseline measures. For tests that included ambulatory measures as a dependent variable (EDA, HR, and HRV), we controlled for movement (measured from ACC) and duration of each activity. All results were plotted (mean and SEM), and post hoc comparisons were reported with least significant difference correction.
To explore differences in game appraisal between sessions, or between groups, we performed nonparametric tests (Spearman correlation and Kruskal-Wallis) on Likert scales. Results were plotted in terms of response frequency to each appraisal question to visually illustrate game- or group-related differences in the patterns of attitude toward games.
All statistical analyses were performed with SPSS (version 24 for Mac; IBM Corp). MoCAGroup×Session×Activity plots (mean, SEM) were generated with Prism (version 8 for Mac; GraphPad Inc).
Results
Who Wants to Play?
In total, 42 adults meeting the age criteria (>65 years) completed the survey, 19 of whom volunteered to enroll in the experimental study. Only 1 participant dropped out of the experimental phase after the first visit because of extreme physical discomfort that forced her to eat and drink (thus invalidating the cortisol sampling). Differences in participant characteristics are presented in Table 2. No significant group differences were observed (all P>.5).
Table 2.
Participant characteristics.
| Characteristics | Participated in experiment | Did not participate further | |
| Gender, n | |||
|
|
Male | 6 | 10 |
|
|
Female | 13 | 13 |
|
|
Other | 0 | 0 |
| Mental health, n | |||
|
|
Good | 17 | 13 |
|
|
Could be better | 2 | 2 |
| Physical health, n | |||
|
|
Good | 14 | 10 |
|
|
Could be better | 5 | 5 |
| Age (years), mean (SD) | 70.47 (4.49) | 69.70 (4.20) | |
| Education (years), mean (SD) | 16.26 (3.68) | 16.22 (2.58) | |
| Generalized Self-Efficacy, mean (SD), maximum n=40 | 33.79 (2.80) | 32.42 (4.77) | |
| Perceived Stress Scale, mean (SD), maximum n=40 | 17.78 (3.83) | 18.46 (3.83) | |
| Loneliness Index, mean (SD), maximum n=80 | 11.21 (11.36) | 18.8 (15.54) | |
Figure 3 summarizes the game attitude distribution in our sample. The response frequencies are ranked based on the largest number of favorable (I agree) responses to a given question in the sample who completed the study. Overall, those who completed the study and those who did not join the experiment after the screening had a positive attitude toward games; however, those who did not participate were not in disagreement but more frequently gave I don’t know responses to various game-related questions. Kruskal-Wallis tests showed that those who participated in the experimental phase gave more positive responses to the following items: In general, I prefer face-to-face conversations to an online conversation (χ21=6.7; P=.01); I prefer solo digital games (χ21=4.1; P=.04); I wish there were games for my age or interest (χ21=4.2; P=.04). The participants more frequently disagreed with the following items: Digital Games are too hard to learn (χ21=5.3; P=.02) and Digital games are disruptive to my real life (χ21=2.8; P=.09).
Figure 3.
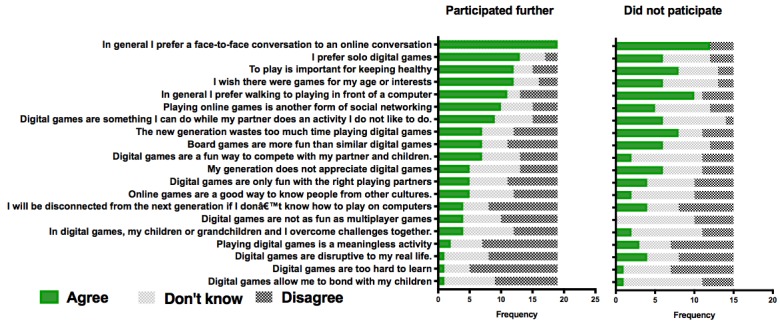
Participants’ appraisal of gaming before enrollment in the study.
Effects of Game Type on Reflexive Outcomes
Physiological Response
Figure 4 illustrates the effects of games and activities on different signals measured during the experiment (mean, SEM). Session by activity interactions had a significant effect on EDA (χ210=26; P=.004), HR (χ210=24.5; P=.006), HRV (χ210=96; P<.001) but not on Cortisol (χ26=6.5; P=.37). In all sessions, we observed the highest levels of cortisol at the baseline, followed by an exponential decline in cortisol levels. Detrending the cortisol levels to remove this decline did not change the outcome of the statistical inference.
Figure 4.
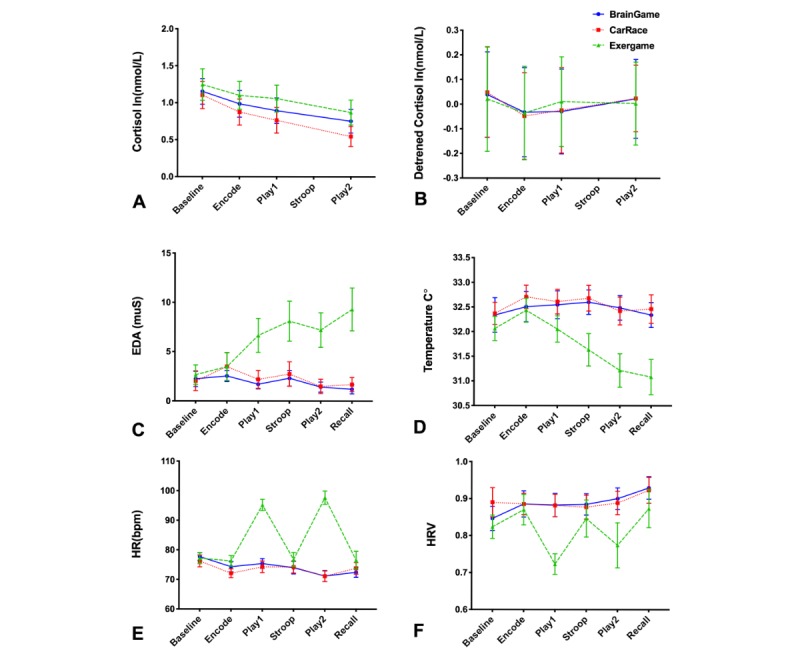
The profile of physiological signals changes over time. The only immediate significant game-related change was observed in heart rate and heart rate variability variables. HR: heart rate; HRV: heart rate variability.
The main effect of Session was significant for EDA (χ22=20.6; P<.001), HR (χ22=23.4; P<.001), and HRV (χ22=33.3; P<.001). The effects of control variables (acceleration and duration) were not significant on any of the outcome measures (albeit a trend was observed for a positive association between acceleration and HR (P=.08). There were no significant differences between S1 and S2, but EDA in S3 was significantly higher than that in S1 (mean difference 4.3 muS; P<.001; 95% CI 2.77 to 5.9) and S2 (mean difference 3.97 muS; P<.001; 95% CI 2.4 to 5.5), expectedly as a result of physical activity. The HR in S3 was higher than that in S1 (mean difference 10.02 bpm; P<.001; 95% CI 7.5 to 12.2) and S2 (mean difference 9.6 bpm; P<.001; 95% CI 7.2 to 12 bpm) and the previous two sessions, but the difference between S1 and S2 was not significant. The main effect of Activity was significant only for HR (χ25=28.8; P<.001) and HRV (χ25=79.3; P<.001).
Cognitive Performance
We had hypothesized that if a game was stressful, then it would interfere with cognitive processing. Indeed, we found that different game sessions affected the rate of correct immediate recall in the encode (χ22=10.2; P=.006) and delayed recall (χ22=24.6; P<.001), as well as on Stroop’s RT to correct (χ22=6.5; P<.05) but not on Stroop rate of correct response (χ22=2.5; P=.29). Post hoc tests showed significant reduction of performance in the exergame session (S3) compared with baseline (brain training, S1) during encode (mean difference −12.6%; P=.02; 95% CI −23.5 to −1.68) and recall (mean difference −22.96; P<.001; 95% CI −35.6 to −10.2). A similar trend was observed in comparison of Car Race (S2) vs S1 (for encode, mean difference −10.9; P=.09; 95% CI −23.3 to 1.45; and for recall, mean difference −11.48; P=.06; 95% CI −23.4 to 0.47). No difference in encode rates was observed between S3 and S2, but there was a trend of reduced correct recalls (mean difference −11.48%; P=.08; 95% CI −24.0 to 1.06). Stroop RT was also slower in S3 vs S1 (mean difference 440 ms; P=.006; 95% CI 130 to 759) and S2 vs S1 (mean difference 269 ms; P=.03; 95% CI 20 to 510). Because encode and recall rates were correlated (r=.631; P<.001), we controlled for the effect of encode hit rates in the GEE model that estimated the effect of the session on recall hits. Regardless, the effects of Session on recall performance remained significant (χ22=16.1; P<.001). These results suggest that even though the participants had become familiar with the tasks, their performance did not improve by the third session; it declined instead, suggesting that the exergame was the most challenging and potentially the most stressful game of the three. Figure 5 illustrates how this stress effect on performance was exacerbated in the group with lower MoCA scores.
Figure 5.

Differences in cognitive performance between sessions and Montreal Cognitive Assessment groups (*P<.05; **P<.005; ***P<.001). MoCA: Montreal Cognitive Assessment.
Effects of Game Type on Reflective Outcomes
The experimental sessions did not cause changes in anxiety states as measured by the 6-item Spielberger State-Trait Anxiety Inventory Scale (χ22=2.0; P=.36). However, participants did express an emotional response to the playing experience, as shown in Figure 6. Because our sample was small, we did not perform any factor analysis. Instead, we chose to illustrate the frequency of affirmative responses to each of the game appraisal questions at the end of the session. Most participants found all three games to be enjoyable, interesting, stimulating to cognition, and beneficial to mental wellness.
Figure 6.
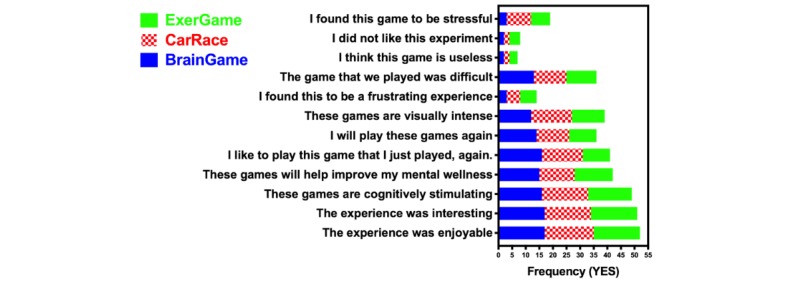
Frequency of responding positively to the postgame appraisal questionnaire at the end of each session.
We evaluated game-related differences in appraisal of the session using a Kruskal-Wallis comparison of Likert-scale responses to each item. We did not find significant differences related to the experimental session in scoring items. The test statistics are presented in Multimedia Appendix 1. Although we did not perform any factor analysis, we explored the correlation among the variables. It is worth reporting that there was a significant positive correlation between expressing a will to play the game again (I will play this game again) and finding the game Good for Mental Wellness (Spearman =0.826, n=54; P<.001), Cognitively Stimulating (Spearman (N=54)=0.545; P<.001), and Enjoyable (Spearman =0.639, n=54; P<.001), confirming the link between meaningfulness and enjoyment. There was also a negative correlation between expressing a Will to Play the Game again, and finding it Frustrating (Spearman =−0.438, n=54; P<.001) and Useless (Spearman =−0.617, n=54; P<.001). A more detailed analysis of these results is beyond the scope of this report and will be presented separately, together with the qualitative data [89].
Effects of Cognitive Ability on Outcome Measures
Characteristics of the Sample in Montreal Cognitive Assessment Groups
To examine whether cognitive reserve would predict the stressfulness of the gaming experience, the sample was split based on MoCA scores to low-MoCA (MoCA<27; n=8; mean 24.62, SD 1.41) and high-MoCA (MoCA ≥27; n=11; mean 28.27, SD 1.19) groups.
Independent t tests did not show significant differences in age (95% CI −3.8 to 2.3; P=.53), Perceived Stress Scale (95% CI −3.36 to 4.36; P=.73), General Self-Efficacy (95% CI −3.6 to 2; P=.53) or Loneliness scale (95% CI −19 to 2; P=.13)
Montreal Cognitive Assessment Group Differences in Game Appraisal
Figure 7 illustrates the patterns of game appraisal in the MoCA groups. In the screening questionnaires, the high-MoCA groups had a generally more positive attitude toward playful experience. The Kruskal-Wallis test demonstrated that in the pre-enrollment appraisal questionnaire, the low-MoCA group considered digital games too hard to learn (χ21=4.05; P<.05), but other scores were not significantly different. In the postgame appraisal questionnaires, the low-MoCA group disliked the experience more (χ21=5.1; P<.03) and found the game more useless (χ21=4.92; P<.03), less interesting (χ21=4.90; P<.03), and visually more intense (χ21=5.6; P<.02); no other differences were statistically significant.
Figure 7.
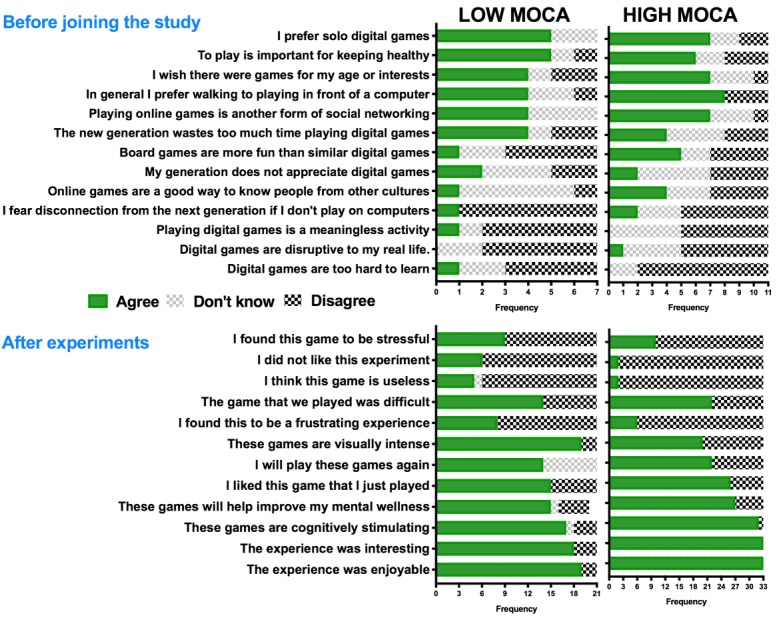
Response frequencies to the pre-enrollment and the postgame appraisal questionnaires.
Montreal Cognitive Assessment Group Differences in Physiological Response
We expected individuals with lower MoCA scores to find the games more challenging and therefore be more stressed by it. To compare the groups, we first normalized all the physiological variables to the within-session and within-subject baseline. Figure 8 illustrates group differences in the pattern of physiological signals over time. Because the physiological profile was significantly different between sessions, we compared group differences separately for each session. A GEE model with independent variable MoCA was then tested for each physiological dependent variable. The results are summarized in Multimedia Appendix 1. The only significant differences in reflexive responses to the experiment were observed in the cortisol levels in the first session (S1) and in the HR during the CareRace (S2).
Figure 8.
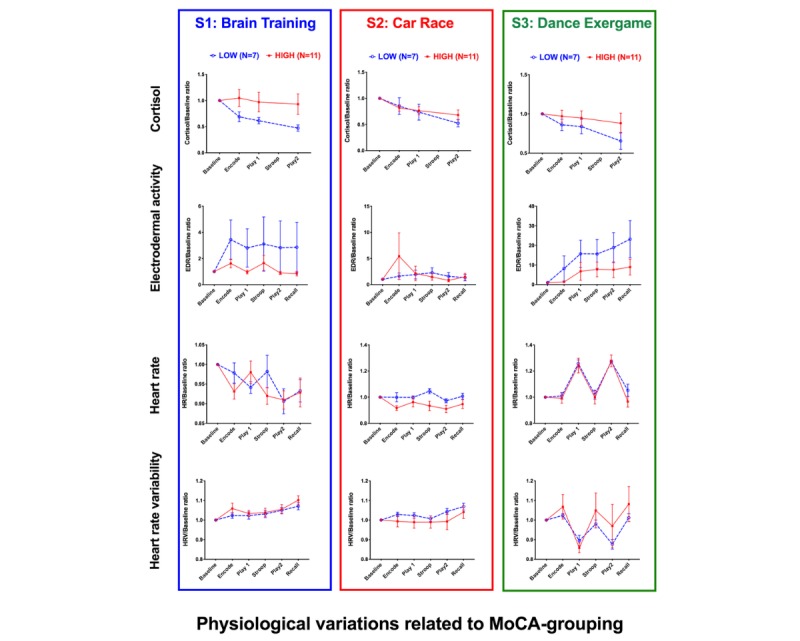
Group×activity interaction effects. All results shown are normalized to the baseline (within-subject, and within-session) and plotted as mean+standard error of the mean. MoCA: Montreal Cognitive Assessment.
In S1, cortisol in the low-MoCA group had a significantly larger drop from the baseline (mean difference −0.218; P=.046; 95% CI 0.004 to 0.432). This effect can reflect the fact that the low-MoCA group was more stressed about taking part in the study from the onset. Although not statistically significant, this group showed a steeper decline in cortisol level in the exergame session as well.
In S2, the low-MoCA group increased their HR with respect to baseline and compared with the high-MoCA group. A trend for increased HR during cognitive tests during S1 (Encode and Stroop) was also observed in the first session. These effects might suggest that irrespective of games, the low-MoCA group found the cognitive challenges in the experiment difficult and stressful.
Montreal Cognitive Assessment Group Differences in Cognitive Tests
We expected that the performance of the low-MoCA group in cognitive tasks would be significantly reduced compared with that of the high-MoCA group. As Figure 5 illustrates, the interactions between MoCA Group and Session were mainly driven by session effects, which affected both groups similarly. The GEE test (Sessioni×MoCA) revealed significant interaction effects on all cognitive variables (all P<.005), except Stroop Correct (χ25=7.4; P=.19). Post hoc analyses show that for both groups, performance in memory tasks was significantly lowered in S3 vs S1 (12% less hits in immediate recall, P<.001; and 22% less hits in delayed recall, P<.001). The Stroop RT was significantly increased in S3 vs S1 (mean difference 461 ms; P=.001). In the low-MoCA group, a small reduction in Stroop accuracy was observed between S3 and S1 (mean difference −2.1%; P<.03) and between S3 and S2 (mean difference −2.33%; P=.008). The Stroop RT to correct in S3 was also the highest and significantly different from that of S1 (mean difference 535 ms; P<.001). The only significant difference between the two groups was in percentage of correct Stroop in S3 (mean difference 2.03%; P<.03). Although the game difficulty affected the Stroop performance in the low-MoCA group, it did not have any impact on the performance of the high-MoCA group.
Discussion
Summary
This study presents a prototype for AGPHA, which incorporates quantitative methods from stress research, to design serious games for use by older adults. The theoretical basis of AGPHA considers appraisal as the first criterion for the evaluation of gamified strategies for seniors’ health care. We performed a mixed methods study to investigate whether playing unfamiliar digital games in the context of their cognitive benefits would be stressful for older adults. We measured stress both reflectively (using appraisal questionnaires before enrollment and after each game-play session), and reflexively (using a wearable device to measure electrodermal response, HR, and HRV; as well as from saliva cortisol). We found an overall positive attitude toward games and a significant link between general cognitive abilities (measured using MoCA, a clinical instrument that measures short-term memory, orientation, visuospatial and executive functions, language abilities, abstraction, and attention) and the degree to which different games (especially the more difficult one, exergame) affect the game-related physiological and cognitive responses. In the following sections, we discuss the main findings, the questions that arise from this research, and the limitations to overcome in future work.
Principal Findings
What Are the Characteristics of Those Who Participated
Our snowball sampling survey was important in informing the results about the characteristics of those who found the topic of serious games interesting. Interindividual variations in game perception and motivation are important factors that engender the gameplaying experience [58,59]. The AGPHA framework [60] builds on the appraisal theory of stress and coping [90]. When confronted with a new challenging encounter, the primary appraisal process is to categorize it as irrelevant, benign-positive, or stressful, depending on what implications it would have for the individual’s well-being. If the person has no investment in the outcome of the challenge, then they will have no need for it and will not commit to engaging with it. On the contrary, if they perceive immediate or potential benefits, they are willing to try it and enter the secondary appraisal stage. It is in the second stage that the individual focuses on evaluating the challenge: Is it feasible and within my physical cognitive abilities?
Our recruitment advertisement targeted a large mailing list of people interested in preventive health care and attracted 42 responses to the survey. Therefore, the number of individuals who entered the primary appraisal stage was not large. Of those, only 19 agreed to enter the secondary appraisal process. Those who did not participate were more likely to agree with the statement Digital games are too hard to learn, suggesting that from the onset, those with less confidence about their cognitive abilities excluded themselves from the experimental phase. Overall, the patterns of response (Figure 3) illustrated that the participating group had a generally more positive attitude toward gaming activities. The participating and nonparticipating groups did not differ in any other characteristics (eg, age, education, self-efficacy)
It must be emphasized that the participating sample had high self-efficacy and was well educated and socially and cognitively active. Thus, the following discussion hinges on the fact that the participants in the study were not representative of the aging population who are in need of cognitive or physical assistance. To address their needs by gamified digital interventions, we must repeat this experiment in a group with pronounced cognitive or physical disabilities (eg, in a nursing home or a rehabilitation center). Theoretically, any factors (such as accessibility or executive difficulty) that influence game appraisal will theoretically change the subsequent reflective and reflexive outcomes as well.
Are New Gaming Experiences Stressful for Seniors?
The second question we asked was whether playing a new digital game would cause stress. If this were the case, then we would expect to observe a significant increase in cortisol and ambulatory signals after the introduction of each game. As the patterns of signal in Figure 4 illustrate, this was not the case.
Cortisol is the hallmark of a latent psychosocial response to stress, but we did not see any significant cortisol effect after any of the gaming activities in the experiment. One explanation is that the highest levels of cortisol were measured at arrival time. This could have resulted from the participant’s anticipation of the session, or from exertion of walking to our center. Because the hypothalamic pituitary adrenal stress system is regulated through a negative feedback mechanism, it is plausible that while the body was downregulating the high levels of basal cortisol, the system was not as responsive to the stress that may have been introduced during game play [91]. Detrending the cortisol signal to remove the sharp decay showed only a mild (and statistically insignificant) increase in cortisol post exergame.
While the cortisol response results from complex and relatively slow neuroendocrine processes, the EDA and HRV mark sympathetic autonomic response and have widely been used in human-computer interface studies [76-82]. The exergame was physiologically more demanding and higher physiological response was expected. Indeed, we observed significant differences in EDA, HR, and HRV, which significantly changed during the exergame (Figure 4) independent of the effect of movement and body temperature (measured on E4).
Interestingly, reflexive and reflective responses were not corresponding. Despite being more difficult, the exergame was not subjectively rated as more stressful (Figure 6). Nevertheless, the lowering of performance in cognitive tasks, which became statistically significant in the stress-sensitive recall task [71], indicates that it had a more pronounced interference with cognitive processing. This interpretation is consistent with previous reports that have shown a link between cognition and training with exergames [92-95]. In other words, the fact that exergame affects the cognitive performance immediately proves that it exercises the brain. Given that effects of stress on cognition are mediated through reward processing [83] and attention [84] systems, the challenge for game designers as well as gerontologists is to evaluate to what extent, for whom, and which exercises can become beneficial to the neurological health of aging individuals.
Effect of Cognitive Abilities on Stress Response to Games
Our third question was whether differences in cognitive ability (based on MoCA) predicted differences in reflective (Figure 7) and reflexive (Figure 8) response to games.
In terms of primary appraisal, the low-MoCA group found digital games too hard to learn. In the secondary appraisal (ie, after playing), the low-MoCA group was less likely to enjoy the game or find it interesting, less likely to find it useful, and more likely to find the game visually more intense. However, the groups did not differ in finding the games difficult or stressful. According to the appraisal theory, these anticipatory and perceptual differences should predict an increased stress response.
Indeed, physiological reactions to the games were stronger in the low-MoCA groups, although they were not statistically significant. The exception was in cortisol levels. The low-MoCA group had 21% more decrease in cortisol levels with respect to baseline during the first session (brain training). This effect may have resulted from the anticipatory stress of the first session, or from the MoCA test itself, which was administered before the experiment began, and possibly caused a social evaluative stress.
Despite differences in perception and cortisol dynamics, cognitive performance in the first session was not significantly different between the two groups, and they both had high rates of correct responses to cognitive tests (>80%). However, in both groups, the performance in those tasks was lowered by increasing game difficulty and more pronounced in the low-MoCA group (Figure 5).
Van Reekum et al [80] have demonstrated the correlation between autonomic responses (cardiac and electrodermal signals) and performance in an action video game. It is plausible that the low-MoCA group experienced higher states of arousal as a result of adaptive coping to compensate for their initial discomfort with the game. This interpretation is consistent with the observation of Birks et al [58], who have argued that adding extrinsic motivation increases the efforts of those who do not have high levels of affinity with their game avatar. Thus, an increased stress response in the low-MoCA group could indicate the player’s increased engagement with the game. Whether this engagement will lead to a desire to repeat play needs to be tested.
Comparison With Previous Studies
Intergenerational Considerations
To the best of our knowledge, this is the first quantitative crossover study to have compared the psychophysiological responses of older adults to different genres of marketplace games, with different levels of complexity in aesthetics, dynamics, and mechanics of games. Intergenerational differences in such studies must address differences in needs and values, as well as differences in physiology.
Poels et al [79] used a similar study design, but their participants were 19 young players. In the study by Poels et al, participants were monitored for hedonic and physiological reactions to four action games with different aesthetic features (two first-person shooters and two race games, with varying degrees of visual complexity). Their study indicated that initial physiological reactions predicted the likelihood of repeat playing in the long term.
Mandryk and Atkins [81] found that galvanic skin response, facial electromyograms, and cardiovascular responses can be used in machine learning algorithms to dynamically compute the degrees of valence and arousal during a gameplay session in 24 young gamers. Their study showed a high convergence between the subjective ratings of games and the machine-predicted levels of emotion and arousal.
In our study, postgame appraisal suggests that the desire to play the game again was highest in the brain training game (14 of 18 players indicated that they will play those games again), which was associated with lower levels of physiological response. In other words, it appears that younger players in the study by Poels et al [79] played games to induce a physiological response, whereas older players in our study preferred a game that did not induce strong reflexive responses.
Our findings are consistent with previous reports that in general, more seniors prefer the ease and pleasure of casual games (preferably with an intellectual component) over more cognitively demanding action games [3,56,57]. Our observations raise the following important questions that cannot be addressed in this study. What are the intergenerational differences in game appraisal? How are these differences in game appraisal correlated to age-related differences in physiological and cognitive reserves? Are physiological measures appropriate for evaluation of seniors desire to engage in the game challenge?
The Importance of Context
In a meta-analysis of 48 studies, involving uniplayer games (excluding exergames), Van der Vijgh et al [96] demonstrated and argued that although games can explain up to 57% of stress-related physiological variations (HR and blood pressure), it is not the game alone but the context of the experimental design and the study characteristics that moderate the stressful response to games.
In this study, we wanted to make the participants comfortable with games (eg, by sequencing the games from simple in the first session to hard in the last session). However, these games were presented in a serious context by the title of the study An Objective Assessment of Interactions Between Appraisal, Arousal and Cognitive Benefits of Electronic Playing. If the study characteristics (which we modified by altering the games in the different sessions) are important, then arguably, our complex experimental setting, and the inclusion of the memory and Stroop tests (even though simplified) could have altered the phenomenology of the experience and thus have hindered the physiological responses to the gameplay alone. Nevertheless, our complex experimental setup allows to illustrate the complexity arising from contextual factors that interact with psychophysiological adaptation. In real life, games are not experienced as isolated laboratory events, but in relation to other activities. The complexity of Group×Session×Activity interactions with physiological signals (Figure 8) provides evidence to concur with Van der Vijgh et al [96] that it is the context in which games are experienced that counts.
Stress and Performance
Acute stress is not necessarily a maladaptive response. Stress interacts with learning and cognitive function through myriad physiological and behavioral cascades [64,84]. The evolutionary function of an acute physiological stress response is to focus and consolidate the lessons to be learned from surviving new challenges [65,84,97,98].
Van Reekum et al [80] have demonstrated a correlation between autonomic responses (cardiac and electrodermal signals) and performance in an action video game. In our design, neither could we reliably record nor did we want to measure the player’s performance in the commercial games that we presented. Instead, we used the simple version of a Stroop test in which RT is expected to be affected by acute stress [71,86], and which seems to acutely improve after casual exergaming in a younger sample [87]. We also used an encoding/recall task, which we have previously shown to be sensitive to acute stress [71,85]. Although these measures were not chosen to be difficult (eg, the number of Stroop trials was very small) or to measure specific cognitive domains, they served as control variables to help us assess whether game difficulty could have an impact that exceeded the learning effect.
We found that the RT to a very simple Stroop (4 color, 75% incongruent stimuli) increased with game difficulty and that delayed recall accuracy decreased with game difficulty, especially in those with lower MoCA scores. Although we cannot infer about how games interacted with cognition, we demonstrate that such cognitive tests may offer a lower cost measure to trace effects of repeated play on neuropsychological factors that underlie cognition. As we have argued in introduction of the AGPHA framework [60], to document such data can potentially guide the decisions made in the design cycle, in terms of how to activate specific cognitive targets by modifying game aesthetics and dynamics.
Limitations
Sample Size
This study is limited primarily by the sample size, which was estimated with the expectation of 80% of power to detect a cortisol response to an explicit stress challenge [71]. In older adults, stress responses to the same task may be blunter than those in a younger sample [99]. Age-related variations in stress sensitivity may be connected to a myriad of endocrinological or psychological factors, all of which need to be carefully modeled using larger samples [100]. Adding multifactorial quantitative measurements (growing in availability and reducing in cost) to larger crowdsourced experiments such as the one conducted by Birks et al [101] could provide a finer grained picture of the physiological embodied qualities of a game experience. This would be of considerable importance for the clinical industries that are emerging around the utilization of game-based interventions in mental health care [32].
In addition, the complexity of our setup makes our ambulatory measurements more susceptible to instrumentation noise. Despite setting up the procedure to be identical and obtaining repeated measures of cortisol and ambulatory signals at baseline, we did not achieve interclass correlations above 70%. Endocrine measurements (eg, cortisol) are sensitive to factors such as time of the day (circadian rhythms), activity before sampling, and states of health and medications. Although we controlled and measured all of these factors, our small sample size does not allow including all of them in our statistical models. These factors must be controlled for in larger studies.
Experimental Complexity and Analytical Limits
The second limitation of this study is inherent to its experimental design. We wanted these experiments to be participatory and gave primacy to the participant’s appraisal of games in relation to their cognitive benefits. We therefore avoided stressful elements such as keeping scores or time pressure. The main experimental variants were gradual increase in game complexity and MoCA categorization. Our repeated measures experimental design is advantageous in terms of statistical power but is not immune to habituation effects, which is a very important and confounding factor in stress studies.
The third limitation of our study is to have split the sample by MoCA scores. MoCA includes 30 questions, and a score of 1/0 per each question, to account for differences in short-term memory, orientation, visuospatial and executive functions, language abilities, abstraction, and attention. This categorization, especially in the context of evaluating a complex and interactive medium such as a game, is too reductionist. To use MoCA as a discriminating factor provided methodological simplicity to offer a proof-of-concept example of the application of AGPHA framework, but it did not account for the variations in behavioral strategies that compensate for decline in those specific cognitive domains. These issues must be further investigated.
Finally, our test studio (blue-floored and mirrored-walls) and the various assessment tools we used were quite burdensome and far from ecological. To repeat this experiment in a familiar setting and with a simpler design, such as in a living laboratory, a nursing home, or a senior’s community center, will likely produce different results.
Conclusion and Future Work
The field of serious games needs methodological standards to evaluate the efficacy of games that are designed to benefit seniors [50]. Despite its limitations, this pilot study illustrates that the quantitative framework proposed in AGPHA is sensitive to uncovering the within-subject and between-group differences in reflexive and reflective reaction to games. We have used various instruments: surveys and appraisal inventories (which are available free of cost), multiple data from wearable physiological monitors (the device costs ~Can $2500 [~US $1871]), multiple saliva samples (~Can $15 [~US $11.22813] per each sample), and computerized neurocognitive tests (almost free). We found a complex pattern of associations between physiological factors and activities in each session, which suggests that variables such as cortisol and slow EDA signal changes are sensitive for detecting gross effects of experimental procedures. More simple measures—a delayed picture recall test and the RT to a correct response in a nonchallenging version of the Stroop test—were also sensitive enough to detect between-group and between-session variations in response to different games. Better defined cognitive tests can reveal more precise interactions between specific games and specific cognitive domains. The MoCA categorization in this study serves as a proof of concept for the AGPHA framework, but it does not represent the full scope of interindividual variations (eg, in sex, gender, personality, and health state). In larger and more heterogeneous samples, this multivariate approach can be explored from multiple facets to help us develop predictable models of health outcomes benefiting from different serious games.
Acknowledgments
This paper is part of an empirical investigation of Finding Better Games for Older Adults supported by the seed funding from Concordia University’s Office of Research and PERFORM Centre. The authors acknowledge logistic support from McGill Centre for Integrative Neuroscience; the Ageing+Communication+Technologies network; and Technoculture, Arts and Games Centre. The authors would also like to thank Luciano Frizzera and Anna Smyrnova for support with Communications and Gina Haraszti, Christina Weiss, and Sriram Naryanan for technical support through initiation and execution of this project.
Abbreviations
- ACC
accelerometer
- AGPHA
Affective Game Planning for Health Applications
- EDA
electrodermal activity
- GEE
generalized estimating equation
- HR
heart rate
- HRV
heart rate variability
- MoCA
Montreal Cognitive Assessment
- RT
reaction time
Appendix
Supplemental materials.
Footnotes
Conflicts of Interest: None declared.
References
- 1.de Schutter B, Brown JA. Digital games as a source of enjoyment in later life. Games Cult. 2016;11(1-2):28–52. doi: 10.1177/1555412015594273. [DOI] [Google Scholar]
- 2.Marston HR, Freeman S, Bishop KA, Beech CL. A scoping review of digital gaming research involving older adults aged 85 and older. Games Health J. 2016 Jun;5(3):157–74. doi: 10.1089/g4h.2015.0087. [DOI] [PubMed] [Google Scholar]
- 3.de Schutter B. Never too old to play: the appeal of digital games to an older audience. Games Cult. 2011;6(2):155–70. doi: 10.1177/1555412010364978. [DOI] [Google Scholar]
- 4.Kaufman D, Sauvé L, Renaud L, Sixsmith A, Mortenson B. Older adults’ digital gameplay. Simul Gaming. 2016;47(4):465–89. doi: 10.1177/1046878116645736. [DOI] [Google Scholar]
- 5.Loos E, Zonnenveld A. Silver Gaming: Serious Fun for Seniors?. Proceedings of the International Conference on Human Aspects of IT for the Aged Population; ITAP'16; July 17 - 22, 2016; Toronto, Canada. 2016. pp. 330–41. [DOI] [Google Scholar]
- 6.Nap HH, de Kort YA, Ijsselsteijn WA. Senior gamers: preferences, motivations and needs. Gerontechnology. 2009;8(4):247–62. doi: 10.4017/gt.2009.08.04.003.00. https://www.researchgate.net/publication/211726554_Senior_gamers_Preferences_motivations_needs. [DOI] [Google Scholar]
- 7.Loos E. Exergaming: meaningful play for older adults? In: Zhou J, Salvendy G, editors. Human Aspects of IT for the Aged Population. Applications, Services and Contexts. Cham: Springer; 2017. pp. 254–65. [Google Scholar]
- 8.Loerzel V, Clochesy J, Geddie P. Using a community advisory board to develop a serious game for older adults undergoing treatment for cancer. Appl Nurs Res. 2018 Feb;39:207–10. doi: 10.1016/j.apnr.2017.11.030. http://europepmc.org/abstract/MED/29422160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ingadottir B, Blondal K, Thue D, Zoega S, Thylen I, Jaarsma T. Development, usability, and efficacy of a serious game to help patients learn about pain management after surgery: an evaluation study. JMIR Serious Games. 2017 May 10;5(2):e10. doi: 10.2196/games.6894. https://games.jmir.org/2017/2/e10/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tong T, Chignell M, Tierney MC, Lee JS. Test-retest reliability of a serious game for delirium screening in the emergency department. Front Aging Neurosci. 2016;8:258. doi: 10.3389/fnagi.2016.00258. doi: 10.3389/fnagi.2016.00258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Boletsis C, McCallum S. Smartkuber: a serious game for cognitive health screening of elderly players. Games Health J. 2016 Aug;5(4):241–51. doi: 10.1089/g4h.2015.0107. [DOI] [PubMed] [Google Scholar]
- 12.Binder JC, Zöllig J, Eschen A, Mérillat S, Röcke C, Schoch S, Jäncke L, Martin M. Multi-domain training in healthy old age: Hotel Plastisse as an iPad-based serious game to systematically compare multi-domain and single-domain training. Front Aging Neurosci. 2015;7:137. doi: 10.3389/fnagi.2015.00137. doi: 10.3389/fnagi.2015.00137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tarnanas I, Papagiannopoulos S, Kazis D, Wiederhold M, Widerhold B, Tsolaki M. Reliability of a novel serious game using dual-task gait profiles to early characterize aMCI. Front Aging Neurosci. 2015;7:50. doi: 10.3389/fnagi.2015.00050. doi: 10.3389/fnagi.2015.00050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kim K, Choi Y, You H, Na DL, Yoh M, Park J, Seo J, Ko M. Effects of a serious game training on cognitive functions in older adults. J Am Geriatr Soc. 2015 Mar;63(3):603–5. doi: 10.1111/jgs.13304. [DOI] [PubMed] [Google Scholar]
- 15.Reichlin L, Mani N, McArthur K, Harris AM, Rajan N, Dacso CC. Assessing the acceptability and usability of an interactive serious game in aiding treatment decisions for patients with localized prostate cancer. J Med Internet Res. 2011 Jan 12;13(1):e4. doi: 10.2196/jmir.1519. https://www.jmir.org/2011/1/e4/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rose NS, Rendell PG, Hering A, Kliegel M, Bidelman GM, Craik FI. Cognitive and neural plasticity in older adults' prospective memory following training with the Virtual Week computer game. Front Hum Neurosci. 2015;9:592. doi: 10.3389/fnhum.2015.00592. doi: 10.3389/fnhum.2015.00592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Anguera JA, Boccanfuso J, Rintoul JL, Al-Hashimi O, Faraji F, Janowich J, Kong E, Larraburo Y, Rolle C, Johnston E, Gazzaley A. Video game training enhances cognitive control in older adults. Nature. 2013 Sep 5;501(7465):97–101. doi: 10.1038/nature12486. http://europepmc.org/abstract/MED/24005416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhang F, Kaufman D. Physical and cognitive impacts of digital games on older adults: a meta-analytic review. J Appl Gerontol. 2016 Nov;35(11):1189–210. doi: 10.1177/0733464814566678. [DOI] [PubMed] [Google Scholar]
- 19.Chao YY, Scherer YK, Montgomery CA. Effects of using Nintendo Wii exergames in older adults: a review of the literature. J Aging Health. 2015 Apr;27(3):379–402. doi: 10.1177/0898264314551171. [DOI] [PubMed] [Google Scholar]
- 20.Toril P, Reales J, Ballesteros S. Video game training enhances cognition of older adults: a meta-analytic study. Psychol Aging. 2014 Sep;29(3):706–16. doi: 10.1037/a0037507. [DOI] [PubMed] [Google Scholar]
- 21.Basak C, Boot WR, Voss MW, Kramer AF. Can training in a real-time strategy video game attenuate cognitive decline in older adults? Psychol Aging. 2008 Dec;23(4):765–77. doi: 10.1037/a0013494. http://europepmc.org/abstract/MED/19140648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li J, Erdt M, Chen L, Cao Y, Lee S, Theng Y. The social effects of Exergames on older adults: systematic review and metric analysis. J Med Internet Res. 2018 Jun 28;20(6):e10486. doi: 10.2196/10486. https://www.jmir.org/2018/6/e10486/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Peretz C, Korczyn A, Shatil E, Aharonson V, Birnboim S, Giladi Nir. Computer-based, personalized cognitive training versus classical computer games: a randomized double-blind prospective trial of cognitive stimulation. Neuroepidemiology. 2011;36(2):91–9. doi: 10.1159/000323950. [DOI] [PubMed] [Google Scholar]
- 24.de Schutter B, Malliet S. The older player of digital games: a classification based on perceived need satisfaction. Communications. 2014;39(1):67–87. doi: 10.1515/commun-2014-0005. https://www.researchgate.net/publication/261027741_The_Older_Player_of_Digital_Games_A_Classification_Based_on_Perceived_Need_Satisfaction. [DOI] [Google Scholar]
- 25.Bleakley CM, Charles D, Porter-Armstrong A, McNeill MD, McDonough S, McCormack B. Gaming for health: a systematic review of the physical and cognitive effects of interactive computer games in older adults. J Appl Gerontol. 2015 Apr;34(3):NP166–89. doi: 10.1177/0733464812470747. [DOI] [PubMed] [Google Scholar]
- 26.de Schutter B. Gerontoludic design: extending the MDA framework to facilitate meaningful play for older adults. Int J Gaming Comput Mediat Simul. 2017;9(1):45–60. doi: 10.4018/IJGCMS.2017010103. [DOI] [Google Scholar]
- 27.Brox E, Konstantinidis ST, Evertsen G. User-centered design of serious games for older adults following 3 years of experience with Exergames for seniors: a study design. JMIR Serious Games. 2017 Jan 11;5(1):e2. doi: 10.2196/games.6254. https://games.jmir.org/2017/1/e2/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.de la Hera T, Loos E, Simons M, Blom J. Benefits and Factors Influencing the Design of Intergenerational Digital Games: A Systematic Literature Review. Societies. 2017 Jul 10;7(3):18. doi: 10.3390/soc7030018. [DOI] [Google Scholar]
- 29.Ijsselsteijn W, Nap H, de Kort Y, Poels KH. Digital Game Design for Elderly Users. Proceedings of the 2007 conference on Future Play; Future Play'07; November 14 - 17, 2007; Toronto, Canada. 2007. pp. 17–22. [DOI] [Google Scholar]
- 30.Gerling KM, Schulte FP, Masuch M. Designing and Evaluating Digital Games for Frail Elderly Persons. Proceedings of the 8th International Conference on Advances in Computer Entertainment Technology; ACE'11; November 8 - 11, 2011; Lisbon, Portugal. 2011. pp. 1–8. [DOI] [Google Scholar]
- 31.Gerling KM, Mandryk RL, Linehan C. Long-Term Use of Motion-Based Video Games in Care Home Settings. Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems; CHI'15; April 18 - 23, 2015; Seoul, Korea. 2015. pp. 1573–82. [DOI] [Google Scholar]
- 32.Manera V, Ben-Sadoun G, Aalbers T, Agopyan H, Askenazy F, Benoit M, Bensamoun D, Bourgeois J, Bredin J, Bremond F, Crispim-Junior C, David R, de Schutter B, Ettore E, Fairchild J, Foulon P, Gazzaley A, Gros A, Hun S, Knoefel F, Rikkert MO, Tran MK, Politis A, Rigaud AS, Sacco G, Serret S, Thümmler S, Welter ML, Robert P. Recommendations for the Use of Serious Games in Neurodegenerative Disorders: 2016 Delphi Panel. Front Psychol. 2017;8:1243. doi: 10.3389/fpsyg.2017.01243. doi: 10.3389/fpsyg.2017.01243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Green CS, Strobach T, Schubert T. On methodological standards in training and transfer experiments. Psychol Res. 2014 Nov;78(6):756–72. doi: 10.1007/s00426-013-0535-3. [DOI] [PubMed] [Google Scholar]
- 34.Baniqued PL, Kranz MB, Voss MW, Lee H, Cosman JD, Severson J, Kramer AF. Cognitive training with casual video games: points to consider. Front Psychol. 2014 Jan 7;4:1010. doi: 10.3389/fpsyg.2013.01010. doi: 10.3389/fpsyg.2013.01010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Baniqued PL, Lee H, Voss MW, Basak C, Cosman JD, Desouza S, Severson J, Salthouse TA, Kramer AF. Selling points: what cognitive abilities are tapped by casual video games? Acta Psychol (Amst) 2013 Jan;142(1):74–86. doi: 10.1016/j.actpsy.2012.11.009. http://europepmc.org/abstract/MED/23246789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zelinski EM, Reyes R. Cognitive benefits of computer games for older adults. Gerontechnology. 2009;8(4):220–35. doi: 10.4017/gt.2009.08.04.004.00. http://europepmc.org/abstract/MED/25126043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Szanton SL, Walker RK, Lim JH, Fisher L, Zhan A, Gitlin LN, Thorpe RJ, Terzis A. Development of an Exergame for urban-dwelling older adults with functional limitations: results and lessons learned. Prog Community Health Partnersh. 2016;10(1):73–81. doi: 10.1353/cpr.2016.0005. [DOI] [PubMed] [Google Scholar]
- 38.Agmon M, Perry CK, Phelan E, Demiris G, Nguyen HQ. A pilot study of Wii Fit exergames to improve balance in older adults. J Geriatr Phys Ther. 2011;34(4):161–7. doi: 10.1519/JPT.0b013e3182191d98. [DOI] [PubMed] [Google Scholar]
- 39.Graves LE, Ridgers ND, Williams K, Stratton G, Atkinson G, Cable NT. The physiological cost and enjoyment of Wii Fit in adolescents, young adults, and older adults. J Phys Act Health. 2010 May;7(3):393–401. doi: 10.1123/jpah.7.3.393. [DOI] [PubMed] [Google Scholar]
- 40.Keogh JW, Power N, Wooller L, Lucas P, Whatman C. Physical and psychosocial function in residential aged-care elders: effect of Nintendo Wii Sports games. J Aging Phys Act. 2014 Apr;22(2):235–44. doi: 10.1123/japa.2012-0272. [DOI] [PubMed] [Google Scholar]
- 41.Maillot P, Perrot A, Hartley A. Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol Aging. 2012 Sep;27(3):589–600. doi: 10.1037/a0026268. [DOI] [PubMed] [Google Scholar]
- 42.Li J, Xu X, Pham TP, Theng Y, Katajapuu N, Luimula M. Exergames designed for older adults: a pilot evaluation on psychosocial well-being. Games Health J. 2017 Dec;6(6):371–8. doi: 10.1089/g4h.2017.0072. [DOI] [PubMed] [Google Scholar]
- 43.Manlapaz D, Sole G, Jayakaran P, Chapple CM. A narrative synthesis of Nintendo Wii Fit gaming protocol in addressing balance among healthy older adults: what system works? Games Health J. 2017 Apr;6(2):65–74. doi: 10.1089/g4h.2016.0082. [DOI] [PubMed] [Google Scholar]
- 44.Hwang J, Lu AS. Narrative and active video game in separate and additive effects of physical activity and cognitive function among young adults. Sci Rep. 2018 Jul 20;8(1):11020. doi: 10.1038/s41598-018-29274-0. doi: 10.1038/s41598-018-29274-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lee H, Huang C, Ho S, Sung WH. The effect of a virtual reality game intervention on balance for patients with stroke: a randomized controlled trial. Games Health J. 2017 Oct;6(5):303–11. doi: 10.1089/g4h.2016.0109. [DOI] [PubMed] [Google Scholar]
- 46.Ruivo JM, Karim K, OʼShea R, Oliveira RC, Keary L, OʼBrien C, Gormley JP. In-class active video game supplementation and adherence to cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2017 Jul;37(4):274–8. doi: 10.1097/HCR.0000000000000224. [DOI] [PubMed] [Google Scholar]
- 47.Narme P. Benefits of game-based leisure activities in normal aging and dementia. Geriatr Psychol Neuropsychiatr Vieil. 2016 Dec 1;14(4):420–8. doi: 10.1684/pnv.2016.0632. [DOI] [PubMed] [Google Scholar]
- 48.Su H, Chang YK, Lin YJ, Chu IH. Effects of training using an active video game on agility and balance. J Sports Med Phys Fitness. 2015 Sep;55(9):914–21. [PubMed] [Google Scholar]
- 49.Lohse K, Shirzad N, Verster A, Hodges N, van der Loos HF. Video games and rehabilitation: using design principles to enhance engagement in physical therapy. J Neurol Phys Ther. 2013 Dec;37(4):166–75. doi: 10.1097/NPT.0000000000000017. [DOI] [PubMed] [Google Scholar]
- 50.Loos E, Kaufman D. Positive impact of Exergaming on older adults’ mental and social well-being: in search of evidence. In: Zhou J, Salvendy G, editors. Human Aspects of IT for the Aged Population. Applications in Health, Assistance, and Entertainment. Cham: Springer; 2018. pp. 101–12. [Google Scholar]
- 51.Larsen LH, Schou L, Lund HH, Langberg H. The physical effect of Exergames in healthy elderly-a systematic review. Games Health J. 2013 Aug;2(4):205–12. doi: 10.1089/g4h.2013.0036. [DOI] [PubMed] [Google Scholar]
- 52.Wu Z, Li J, Theng YL. Examining the influencing factors of exercise intention among older adults: a controlled study between Exergame and traditional exercise. Cyberpsychol Behav Soc Netw. 2015 Sep;18(9):521–7. doi: 10.1089/cyber.2015.0065. [DOI] [PubMed] [Google Scholar]
- 53.Boot WR, Champion M, Blakely DP, Wright T, Souders DJ, Charness N. Video games as a means to reduce age-related cognitive decline: attitudes, compliance, and effectiveness. Front Psychol. 2013;4:31. doi: 10.3389/fpsyg.2013.00031. doi: 10.3389/fpsyg.2013.00031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Green CS, Bavelier D. Action video game training for cognitive enhancement. Curr Opin Behav Sci. 2015;4:103–8. doi: 10.1016/j.cobeha.2015.04.012. [DOI] [Google Scholar]
- 55.Lieberoth A. Shallow gamification: testing psychological effects of framing an activity as a game. Games Cult. 2015;10(3):229–48. doi: 10.1177/1555412014559978. [DOI] [Google Scholar]
- 56.Chesham A, Wyss P, Müri RM, Mosimann UP, Nef T. What older people like to play: genre preferences and acceptance of casual games. JMIR Serious Games. 2017 Apr 18;5(2):e8. doi: 10.2196/games.7025. https://games.jmir.org/2017/2/e8/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Blocker K, Wright T, Boot WR. Gaming preferences of aging generations. Gerontechnology. 2014;12(3):174–84. doi: 10.4017/gt.2014.12.3.008.00. http://europepmc.org/abstract/MED/29033699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Birk MV, Mandryk RL, Atkins C. The Motivational Push of Games: The Interplay of Intrinsic Motivation and External Rewards in Games for Training. Proceedings of the 2016 Annual Symposium on Computer-Human Interaction in Play; CHI PLAY'16; October 16 - 19, 2016; Austin, TX, USA. 2016. pp. 291–303. [DOI] [Google Scholar]
- 59.Nacke LE, Nacke A, Lindley CA. Brain training for silver gamers: effects of age and game form on effectiveness, efficiency, self-assessment, and gameplay experience. Cyberpsychol Behav. 2009 Oct;12(5):493–9. doi: 10.1089/cpb.2009.0013. [DOI] [PubMed] [Google Scholar]
- 60.Khalili-Mahani N, de Schutter B. Affective game planning for health applications: quantitative extension of gerontoludic design based on the appraisal theory of stress and coping. JMIR Serious Games. 2019 Jun 6;7(2):e13303. doi: 10.2196/13303. https://games.jmir.org/2019/2/e13303/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Lazarus RS. Emotions and interpersonal relationships: toward a person-centered conceptualization of emotions and coping. J Pers. 2006 Feb;74(1):9–46. doi: 10.1111/j.1467-6494.2005.00368.x. [DOI] [PubMed] [Google Scholar]
- 62.Selye H. Stress of Life. New York: Mcgraw-hill; 1978. [Google Scholar]
- 63.Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York: Springer Publishing Company; 1984. [Google Scholar]
- 64.Lupien SJ, Lepage M. Stress, memory, and the hippocampus: can't live with it, can't live without it. Behav Brain Res. 2001 Dec 14;127(1-2):137–58. doi: 10.1016/s0166-4328(01)00361-8. [DOI] [PubMed] [Google Scholar]
- 65.Wolf O, Atsak P, de Quervain DJ, Roozendaal B, Wingenfeld K. Stress and memory: a selective review on recent developments in the understanding of stress hormone effects on memory and their clinical relevance. J Neuroendocrinol. 2016 Aug;28(8) doi: 10.1111/jne.12353. [DOI] [PubMed] [Google Scholar]
- 66.Schwabe L, Joëls M, Roozendaal B, Wolf O, Oitzl MS. Stress effects on memory: an update and integration. Neurosci Biobehav Rev. 2012 Aug;36(7):1740–9. doi: 10.1016/j.neubiorev.2011.07.002. [DOI] [PubMed] [Google Scholar]
- 67.Schwabe L, Wolf OT. Stress and multiple memory systems: from 'thinking' to 'doing'. Trends Cogn Sci. 2013 Feb;17(2):60–8. doi: 10.1016/j.tics.2012.12.001. [DOI] [PubMed] [Google Scholar]
- 68.Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In: Johnston M, Weinman J, Wright SC, editors. Measures in Health Psychology: A User's Portfolio. Windsor, England: NFER-NELSON; 1995. pp. 35–7. [Google Scholar]
- 69.Russell D, Peplau LA, Ferguson ML. Developing a measure of loneliness. J Pers Assess. 1978 Jun;42(3):290–4. doi: 10.1207/s15327752jpa4203_11. [DOI] [PubMed] [Google Scholar]
- 70.Hong GS, Kang H, Oh E, Park Y, Kim H. Reliability and Validity of the Korean Version of the Perceived Stress Scale-10 (K-PSS-10) in Older Adults. Res Gerontol Nurs. 2016;9(1):45–51. doi: 10.3928/19404921-20150806-72. [DOI] [PubMed] [Google Scholar]
- 71.Khalili-Mahani N, Dedovic K, Engert V, Pruessner M, Pruessner JC. Hippocampal activation during a cognitive task is associated with subsequent neuroendocrine and cognitive responses to psychological stress. Hippocampus. 2010 Feb;20(2):323–34. doi: 10.1002/hipo.20623. [DOI] [PubMed] [Google Scholar]
- 72.Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005 Apr;53(4):695–9. doi: 10.1111/j.1532-5415.2005.53221.x. [DOI] [PubMed] [Google Scholar]
- 73.Hellhammer DH, Wüst S, Kudielka BM. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology. 2009 Feb;34(2):163–71. doi: 10.1016/j.psyneuen.2008.10.026. [DOI] [PubMed] [Google Scholar]
- 74.Hartmann A, Veldhuis J, Deuschle M, Standhardt H, Heuser I. Twenty-four hour cortisol release profiles in patients with Alzheimer's and Parkinson's disease compared to normal controls: ultradian secretory pulsatility and diurnal variation. Neurobiol Aging. 1997;18(3):285–9. doi: 10.1016/s0197-4580(97)80309-0. [DOI] [PubMed] [Google Scholar]
- 75.Bhake RC, Leendertz JA, Linthorst AC, Lightman SL. Automated 24-hours sampling of subcutaneous tissue free cortisol in humans. J Med Eng Technol. 2013 Apr;37(3):180–4. doi: 10.3109/03091902.2013.773096. [DOI] [PubMed] [Google Scholar]
- 76.Larradet F, Barresi G, Mattos LS. Effects of galvanic skin response feedback on user experience in gaze-controlled gaming: a pilot study. Conf Proc IEEE Eng Med Biol Soc. 2017 Jul;2017:2458–61. doi: 10.1109/EMBC.2017.8037354. [DOI] [PubMed] [Google Scholar]
- 77.Uriarte IO, Garcia-Zapirain B, Garcia-Chimeno Y. Game design to measure reflexes and attention based on biofeedback multi-sensor interaction. Sensors (Basel) 2015 Mar 17;15(3):6520–48. doi: 10.3390/s150306520. http://www.mdpi.com/resolver?pii=s150306520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Mandryk RL, Inkpen KM, Calvert TW. Using psychophysiological techniques to measure user experience with entertainment technologies. Behav Inform Technol. 2006;25(2):141–58. doi: 10.1080/01449290500331156. [DOI] [Google Scholar]
- 79.Poels K, van den Hoogen W, Ijsselsteijn W, de Kort Y. Pleasure to play, arousal to stay: the effect of player emotions on digital game preferences and playing time. Cyberpsychol Behav Soc Netw. 2012 Jan;15(1):1–6. doi: 10.1089/cyber.2010.0040. [DOI] [PubMed] [Google Scholar]
- 80.van Reekum C, Johnstone T, Banse R, Etter A, Wehrle T, Scherer K. Psychophysiological responses to appraisal dimensions in a computer game. Cogn Emot. 2004;18(5):663–88. doi: 10.1080/02699930341000167. [DOI] [Google Scholar]
- 81.Mandryk RL, Atkins MS. A fuzzy physiological approach for continuously modeling emotion during interaction with play technologies. Int J Hum-Comput Stud. 2007;65(4):329–47. doi: 10.1016/j.ijhcs.2006.11.011. [DOI] [Google Scholar]
- 82.Hébert S, Béland R, Dionne-Fournelle O, Crête M, Lupien SJ. Physiological stress response to video-game playing: the contribution of built-in music. Life Sci. 2005 Apr 1;76(20):2371–80. doi: 10.1016/j.lfs.2004.11.011. [DOI] [PubMed] [Google Scholar]
- 83.Vogel S, Klumpers F, Schröder TN, Oplaat K, Krugers H, Oitzl M, Joëls M, Doeller C, Fernández G. Stress induces a shift towards striatum-dependent stimulus-response learning via the Mineralocorticoid receptor. Neuropsychopharmacology. 2017 May;42(6):1262–71. doi: 10.1038/npp.2016.262. doi: 10.1038/npp.2016.262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Schwabe L, Wolf OT, Oitzl MS. Memory formation under stress: quantity and quality. Neurosci Biobehav Rev. 2010 Mar;34(4):584–91. doi: 10.1016/j.neubiorev.2009.11.015. [DOI] [PubMed] [Google Scholar]
- 85.Khalili-Mahani N, Niesters M, van Osch MJ, Oitzl M, Veer I, de Rooij M, van Gerven Joop, van Buchem MA, Beckmann C, Rombouts S, Dahan A. Ketamine interactions with biomarkers of stress: a randomized placebo-controlled repeated measures resting-state fMRI and PCASL pilot study in healthy men. Neuroimage. 2015 Mar;108:396–409. doi: 10.1016/j.neuroimage.2014.12.050. [DOI] [PubMed] [Google Scholar]
- 86.Acevedo EO, Webb HE, Weldy ML, Fabianke EC, Orndorff GR, Starks MA. Cardiorespiratory responses of Hi Fit and Low Fit subjects to mental challenge during exercise. Int J Sports Med. 2006 Dec;27(12):1013–22. doi: 10.1055/s-2006-923902. [DOI] [PubMed] [Google Scholar]
- 87.Gao Y, Mandryk RJ. The Acute Cognitive Benefits of Casual Exergame Play. Proceedings of the SIGCHI Conference on Human Factors in Computing Systems; CHI'12; May 5 - 10, 2012; Austin, TX, USA. 2012. pp. 1863–72. [DOI] [Google Scholar]
- 88.Zeger SL, Liang KY, Albert PS. Models for longitudinal data: a generalized estimating equation approach. Biometrics. 1988 Dec;44(4):1049–60. doi: 10.2307/2531734. [DOI] [PubMed] [Google Scholar]
- 89.Khalili-Mahani N, De Schutter B, Mirgholami M, Holowka Em, Goodine R, DeJong S, McGaw R, Meyer S, Sawchuk K. For Whom the Games Toll: A Qualitative and Intergenerational Evaluation of What is Serious in Games for Older Adults. Comput Game J. 2020 Mar 11; doi: 10.1007/s40869-020-00103-7. [DOI] [Google Scholar]
- 90.Folkman S, Lazarus RS. The relationship between coping and emotion: implications for theory and research. Soc Sci Med. 1988;26(3):309–17. doi: 10.1016/0277-9536(88)90395-4. [DOI] [PubMed] [Google Scholar]
- 91.Henckens M, Klumpers F, Everaerd D, Kooijman S, van Wingen GA, Fernández G. Interindividual differences in stress sensitivity: basal and stress-induced cortisol levels differentially predict neural vigilance processing under stress. Soc Cogn Affect Neurosci. 2016 Apr;11(4):663–73. doi: 10.1093/scan/nsv149. http://europepmc.org/abstract/MED/26668010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Eggenberger P, Wolf M, Schumann M, de Bruin ED. Exergame and balance training modulate prefrontal brain activity during walking and enhance executive function in older adults. Front Aging Neurosci. 2016;8:66. doi: 10.3389/fnagi.2016.00066. doi: 10.3389/fnagi.2016.00066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Wall K, Stark J, Schillaci A, Saulnier E, McLaren E, Striegnitz K, Cohen B, Arciero P, Kramer A, Anderson-Hanley C. The Enhanced Interactive Physical and Cognitive Exercise System (iPACES v2.0): Pilot Clinical Trial of an In-Home iPad-Based Neuro-Exergame for Mild Cognitive Impairment (MCI) J Clin Med. 2018 Aug 30;7(9):pii: E249. doi: 10.3390/jcm7090249. http://www.mdpi.com/resolver?pii=jcm7090249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Garcia JA, Schoene D, Lord SR, Delbaere K, Valenzuela T, Navarro KF. A bespoke Kinect stepping Exergame for improving physical and cognitive function in older people: a pilot study. Games Health J. 2016 Dec;5(6):382–8. doi: 10.1089/g4h.2016.0070. [DOI] [PubMed] [Google Scholar]
- 95.Anderson-Hanley C, Arciero P, Westen S, Nimon J, Zimmerman E. Neuropsychological benefits of stationary bike exercise and a cybercycle exergame for older adults with diabetes: an exploratory analysis. J Diabetes Sci Technol. 2012 Jul 1;6(4):849–57. doi: 10.1177/193229681200600416. http://europepmc.org/abstract/MED/22920811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.van der Vijgh B, Beun R, van Rood M, Werkhoven P. Meta-analysis of digital game and study characteristics eliciting physiological stress responses. Psychophysiology. 2015 Aug;52(8):1080–98. doi: 10.1111/psyp.12431. [DOI] [PubMed] [Google Scholar]
- 97.Roozendaal B, McEwen BS, Chattarji S. Stress, memory and the amygdala. Nat Rev Neurosci. 2009 Jun;10(6):423–33. doi: 10.1038/nrn2651. [DOI] [PubMed] [Google Scholar]
- 98.McEwen B. Stress, adaptation, and disease. Allostasis and allostatic load. Ann N Y Acad Sci. 1998 May 1;840:33–44. doi: 10.1111/j.1749-6632.1998.tb09546.x. [DOI] [PubMed] [Google Scholar]
- 99.Kudielka B, Buske-Kirschbaum A, Hellhammer D, Kirschbaum C. Differential heart rate reactivity and recovery after psychosocial stress (TSST) in healthy children, younger adults, and elderly adults: the impact of age and gender. Int J Behav Med. 2004;11(2):116–21. doi: 10.1207/s15327558ijbm1102_8. [DOI] [PubMed] [Google Scholar]
- 100.Kudielka B, Buske-Kirschbaum A, Hellhammer D, Kirschbaum C. HPA axis responses to laboratory psychosocial stress in healthy elderly adults, younger adults, and children: impact of age and gender. Psychoneuroendocrinology. 2004 Jan;29(1):83–98. doi: 10.1016/s0306-4530(02)00146-4. [DOI] [PubMed] [Google Scholar]
- 101.Birk MV, Friehs MA, Mandryk RL. Age-Based Preferences and Player Experience: A Crowdsourced Cross-sectional Study. Proceedings of the Annual Symposium on Computer-Human Interaction in Play; CHI PLAY'17; October 15 - 18, 2017; Amsterdam, The Netherlands. 2017. pp. 157–70. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental materials.