

Abstract
The study examined factors that influenced Americans' avoidance of domestic travel due to confirmed cases of Ebola in the United States in late 2014. The Health Belief Model served as a theoretical framework for the study. Data were generated from 1613 Americans from an online survey. Perceived susceptibility and self-efficacy were found to significantly influence domestic travel avoidance. The findings also supported the significant role of perceived risk, subjective knowledge, age, and gender. Given the possibility that an Ebola outbreak may reemerge in the future and the emergence of additional health-related crises (e.g., Zika virus), the findings may also aid the tourism industry in planning for and responding to other health pandemics.
Keywords: Ebola, Health Belief Model, Travel avoidance, United States
Highlights
-
•
Participants show low perception risk of contracting Ebola.
-
•
Several variables were positively associated with travel avoidance.
-
•
Participants were aware the contagious nature of Ebola.
-
•
Respondents had high self-efficacy.
1. Introduction
One of most visible media stories in 2014 was the Ebola outbreak. Prior to the 2014 West Africa outbreak, the world had experienced a series of global disease outbreaks such as Severe Acute Respiratory Syndrome (SARS) in 2002–2004 and H1N1 influenza virus in 2009. In 2009, both the global financial crisis and the H1N1 pandemic impacted global travel, with a 4% decrease to 880 million international arrivals (Leggat, Brown, Aitken, & Speare, 2010). Several studies have consistently found that pandemics contribute to heightened concerns about international travel (Lee et al., 2012, Kuo et al., 2008).
Responses to an outbreak have often affected levels of concern and travel intentions. For instance, during the rising prevalence of H1N1 in 2009, the Australian Government introduced a series of procedures that were geared toward incoming and outgoing travelers (Leggat et al., 2010). In addition, Leggat, Brown, and Speare (Leggat et al., 2010) found that while more than half of Queensland travelers showed some concern over the pandemic, a majority would not postpone travel even if they demonstrated H1N1-like symptoms. Another study by Lee et al. (2012) found that perceptions associated with H1N1 were not significant predictors of travel intentions. However, Reisinger and Mavondo (2005) found that perceptions of a disease are important indicators of altered travel patterns. One possible explanation is that travelers might develop adaptive behaviors (personal health interventions) which may prevent them from contracting the disease.
Public perceptions associated with the Ebola outbreak were mostly negative in the U.S. A Washington Post-ABC News survey found that almost two-thirds of Americans were concerned about a widespread Ebola epidemic in the U.S. (Dennis & Craighill, 2014). However, the same survey also found that more than half of the sample was very confident in the federal government's ability to effectively respond to the outbreak in the U.S. Similarly, another survey conducted by Global Business Travel Association found that most respondents surveyed believed that the outbreak had a marginal effect on business travel (Martin, 2014). Nonetheless, the aforementioned surveys did not explain underlying determinants of such behaviors, nor did they explain whether or not domestic travelers were concerned with the disease outbreak, both of which are critical for travel awareness campaigns.
While much has been written on the relationship between pandemic disease and international travel, little is known about potential travelers' behaviors regarding domestic travel during a pandemic outbreak. Understanding travelers' behaviors warrants further exploration because of the unique nature of the Ebola outbreak in the U.S and several confirmed Ebola cases within the U.S. In addition, constant media coverage of Ebola cases in the U.S. might lead to travel avoidance even for travel within the U.S. Likewise, there is a paucity of literature which examines perceptions, beliefs, and attitudes that travelers have pertaining to the transmission and prevention of Ebola. While health experts argued that the possibility of contracting Ebola in the U.S is marginal, public opinion might be altered due to constant media coverage. Coupled with the fact that this was the first time that Ebola cases were confirmed in the U.S., the authors were interested to know to what extent such perceptions might influence travel intentions. Additionally, minimal attention has been given to the relationship between a pandemic and domestic travel.
Because the dynamic nature of a pandemic means that behaviors can have a substantial impact on the course of an outbreak (Halloran et al., 2008), understanding individuals' behavior and its relation to their perceptions of risk is therefore imperative in terms of effective control of an infectious disease outbreak (Ibuka, Chapman, Meyers, Li, & Galvani, 2010). The Health Belief Model (HBM) is often considered an alternative because it considers risk perceptions to be one of the key drivers of behaviors (Brewer & Hallman, 2006). The model suggests that engagement in a protective behavior may be influenced by perceived costs and benefits of such a behavior (Chapman & Coups, 1999).
This study employed the Health Belief Model (HBM) as the theoretical framework to examine how cognitive factors might have influenced behavioral responses in the event of an Ebola outbreak. In this study, we explored determinants of travel avoidance during an Ebola outbreak. Specifically, the research questions for this study were:
-
1)
What is the relationship between perceived travel risk and the likelihood of travel avoidance in the U.S. due to Ebola?
-
2)
What is the relationship between perceived susceptibility and the likelihood of travel avoidance in the U.S. due to Ebola?
-
3)
What is the relationship between perceived severity and the likelihood of travel avoidance in the U.S. due to Ebola?
-
4)
What is the relationship between self-efficacy and the likelihood of travel avoidance in the U.S. due to Ebola?
-
5)
What is the relationship between subjective knowledge and the likelihood of travel avoidance in the U.S. due to Ebola?
-
6)
What is the relationship between select sociodemographic factors and the likelihood of travel avoidance in the U.S. due to Ebola?
Fig. 1 outlines our guiding framework.
Fig. 1.
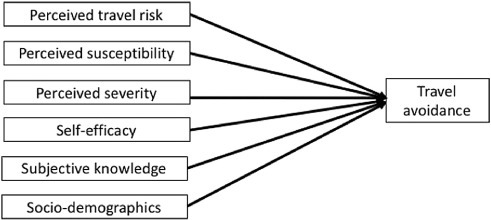
Guiding framework.
2. Context of the study
The Ebola outbreak in 2014 resulted in collaboration between nations in order to contain the epidemic. The disease is derived from one or more strains of the Ebola virus that may be transmitted either from person to person or from animal to human (World Health Organization, 2014). Some of the symptoms associated with the virus are: fever, fatigue, vomiting, muscle pain, and severe headache (Mayo Clinic, 2014). On average, an infected individual has an approximate 30% chance of surviving the disease and more than 1000 individuals had succumbed to the virus by the end of 2014 (Frieden, Damon, Bell, Kenyon, & Nicol, 2014).
The Centers for Disease Control and Prevention (CDC) (2015a) recommends that individuals practice basic sanitation (use soapy water when washing hands or alcohol-based sanitizer), avoid funeral or burial rituals for Ebola victims, avoid an infected individual's blood or bodily fluids, and refrain from contact with non-human primates and bats. The 2014 outbreak of the Ebola virus occurred primarily on the African continent. Due to fear of the Ebola virus, there were warnings against travel to affected nations. Countries which suffered Ebola outbreaks included Uganda, Congo, and West Africa (i.e. Guinea, Liberia, Sierra Leone) (Centers for Disease Control and Prevention, 2015b). The Centers for Disease Control and Prevention (2015b) issued a Level 3 Travel Advisory (Avoid Non-Essential Travel) for the nations of Liberia, Sierra Leone, and Guinea.
The belief at that time was that there was little risk of Ebola spreading from the infected African regions and becoming a massive pandemic affecting other geographic regions throughout the world (Gomes et al., 2014). Though air travel is a popular means of travel, there was little risk of contraction Ebola on commercial flights, a fact not well known to the vast majority of travelers. Thus, it was necessary to educate the general public about the minimal dangers associated with international flights.
Screenings at major airports that dealt with flights from Ebola-affected African nations was one method that the World Health Organization used in an attempt to contain the virus. Bogoch et al. (2015) estimated that 2–8 travelers with the Ebola virus departed monthly on a commercial flight from Liberia, Sierra Leone, and Guinea. Both entry and exit screenings of passengers coming from Africa into Europe or other Western nations helped to detect at least 50% of infected individuals (Read, Diggle, Chirombo, Solomon, & Baylsis, 2015).
The Centers for Disease Control and Prevention in the U.S. issued guidelines pertaining to travelers coming to the U.S. from Ebola-affected nations. The Centers for Disease Control and Prevention recommended that asymptomatic travelers be monitored; however, they were not required to be placed in quarantine (McCarthy, 2014). Some countries issued their own precautions regarding Ebola screenings. Nigeria screened all incoming flight passengers for the disease (Gostin, Lucey, & Phelan, 2014). Among other nations, Gambia and Kenya issued travel bans on passengers arriving from Guinea, Liberia, and Sierra Leone (Poletto et al., 2014).
Some scientists and healthcare professionals contended that the travel ban or quarantine could translate into the misuse of needed medical supplies (Folayan & Brown, 2015). They also cited past failures of quarantines associated with the SARS illness (Barbisch, Koenig, & Shih, 2015) and the possible negative repercussions that travel bans may have had on the economies of struggling nations (Mackenzie, 2014).
3. Literature review
3.1. Health Belief Model
In order to gauge respondents' opinions and perceptions pertaining to the Ebola virus, we utilized constructs derived from the Health Belief Model (HBM). The HBM is a theoretical model which examines variables which predict, influence, and explain why individuals engage in certain risk-related behaviors (Rosenstock et al., 1988, Ayele et al., 2012, Nicholls, 2006, Chen et al., 2011, Setbon and Raude, 2010). Individuals are more likely to engage in risk reduction behaviors if they feel susceptible to a specific illness/condition, perceive the illness/condition to be severe, and/or believe that preventive behaviors outweigh the costs of engagement (Chapman & Skinner, 2008). The model contains six major key constructs: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy.
The HBM is an effective tool in creating and implementing health interventions to change individuals' maladaptive behavioral patterns. The model has been successful in promoting health education (Sharifirad et al., 2009, Cross et al., 2006) or compliance of healthy dietary regimens (Deshpande, Basil, & Basil, 2009). When assessing the model's constructs, perceived barriers and perceived benefits have been found to have the strongest predictive powers (Janz and Becker, 1984, Carpenter, 2010). Perceived severity has been found to exhibit the weakest predictive power for behavior choices (Janz & Becker, 1984). Several factors that may have moderating influences on the predictive power of the HBM are: length of time when measuring beliefs and behavior; treatment vs. prevention actions; and regimens pertaining to certain behaviors (Carpenter, 2010). One study discovered that individuals are more accepting of preventive measures when they believe that there are benefits to adopting the behavior and if they perceive that they are susceptible to a particular disease (Brewer & Fazekas, 2007).
Perceived susceptibility explains individual belief(s) about the risk of contracting an illness (Brewer & Fazekas, 2007). In many circumstances, individuals who perceive that they are at high risk of contracting a disease or condition are more likely to take preventive measures (Brewer et al., 2007). Those who suffer from the symptoms of a disease are likely to believe that preventive and avoidant actions will help decrease the risk of developing a disease (Gao, Nau, Rosenbluth, Scott, & Woodward, 2000).
Perceived severity relates to individual concern with the seriousness of a condition (Brewer & Fazekas, 2007). Individuals that perceive a disease to be severe are more likely to engage in preventive measures (Hanson & Benedict, 2002). This is consistent with theories which suggest that, in general, people avoid unpleasant stimuli in most instances. Not all studies yielded a positive relationship between high perceptions of severity and engagement in preventive measures. For example, a study looking at condom usage in Africa found that subjects' perceptions of the severity of AIDS/HIV did not increase their usage of condoms during sexual intercourse (Hounton, Carabin, & Henderson, 2005).
Perceived benefits are associated with the outcomes of a certain behavior to minimize susceptibility to a disease or illness (Hanson & Benedict, 2002). Individuals who perceive that there are benefits to adopting certain behaviors are more likely to perform those behaviors. This can translate into adherence to treatment or preventive measures (Adams & Scott, 2000). In order to have members from a target population get vaccines, it would be paramount to promote the benefits derived from getting the vaccines. Those who perceive few or no benefits associated with vaccines are less likely to engage in this behavior (Smith et al., 2011). Many successful prevention programs, which seek to change human behavior, take the importance of perceived benefits into account (Epstein, Griffin, & Botvin, 2000).
In some instances, perceived benefits may not be sufficient enticement for individuals to engage in certain behaviors. Stroud, Minahan, and Sabapathy (2009) found perceived benefits associated with exercising were not sufficient in promoting physical activity in sufferers of multiple sclerosis. The researchers found that self-efficacy was more effective as a positive predictor of exercise in individuals diagnosed with multiple sclerosis than perceived benefits. Therefore, while perceived benefits may predict acquisition of behaviors, this is not conclusive.
Perceived barriers identify concerns about performing health promotion behaviors (Hanson & Benedict, 2002). Individuals may utilize a cost-benefit analysis in weighing the perceived barriers against the perceived benefits. Individuals who perceive more barriers than benefits to performing a behavior are less likely to perform the said behavior (Janz & Becker, 1984). An effective strategy in employing individuals to adopt a targeted behavior is to minimize their perceived barriers (Buglar, White, & Robinson, 2010). In the present study, the probable perceived barriers (e.g., contraction of the Ebola virus) may hinder respondents' desires to perform the advocated risk reduction behavior.
Cues to action are strategies or sources of information that promote adoption of a behavior (Cerkoney & Hart, 1980), such as information about Ebola at the airport. Many individuals may weigh the perceived benefits against the perceived barriers to a particular behavior before taking action. Sometimes this may not be sufficient and, as such, individuals need to feel motivated to perform the targeted behavior. Successful strategies for adoption of behaviors utilize specific cues which are associated with conducting the target behaviors (Cerkoney & Hart, 1980).
Self-efficacy measures one's level of confidence to adopt a behavior. High levels of self-efficacy may lead to the likelihood that behavior is initiated and sustained throughout aversive situations (Bandura, 1977). Interventions which aim to increase the use of healthy preventive methods will need to take into account the impact of an individual's perceptions of their self-efficacy. This can be crucial in helping individuals adopt important preventive health behaviors that may lead to averting fatalistic outcomes (Tavafian et al., 2009, Iskender and Akin, 2010).
The HBM has been employed to predict risk perceptions associated with the transmission of pandemic influenza A/H1N1 (Setbon & Raude, 2010), acceptability of A/H1N1 vaccines (Lau et al., 2010), and acceptability of childhood influenza vaccinations (Chen et al., 2011). The usage of the HBM constructs of perceived susceptibility and perceived severity are associated with individuals engaging in recommended protective behaviors (Bish & Michie, 2010). The constructs of perceived barriers and perceived benefits have been successfully utilized to predict the utilization of influenza vaccines (Chen, Fox, Cantrell, Stockdale, & Kagawa-Singer, 2007). In addition, perceived travel risk, subjective knowledge, and socio-demographic factors were added to the model to explore the roles of the aforementioned determinants of travel avoidance based on previous studies (Floyd, Gibson, Pennington-Gray, & Thapa, 2003).
3.2. Perceived travel risk
Risk perceptions have long been scrutinized within the tourism literature (Hales and Shams, 1991, Roehl and Fesenmaier, 1992). Risk is typically denoted as the shock, threat, and crises that can negatively impact the tourism industry (Law, 2006). Additionally, risk is often defined as what is perceived and experienced by visitors during the process of purchasing and consuming services in the destination (Tsaur et al., 1997, Reisinger and Mavondo, 2005). To date, risk has been consistently found to be a major concern for international visitors (Yavas, 1990, Pine and McKercher, 2004, Schroeder et al., 2013).
Prior studies revealed that tourists' risk perceptions are multifaceted and depend on visitors' characteristics. Roehl and Fesenmaier (1992) classified tourists into three risk perception groups: risk neutral, functional risk, and place risk. The risk neutral visitors refer to those who do not perceive travel as risky. The functional risk visitors consider the possibility of mechanical, equipment, and organizational risk. The place risk group, on the other hand, perceived travel as being risky. Furthermore, perceptions of risk might also be affected by individual personality (Carr, 2001) and nationality (Seddighi & Theochaous, 2001).
Perceptions of risk depend on the type of risk perceived (Reisinger and Mavondo, 2005, Yuksel and Yuksel, 2007). There are seven risks frequently discussed in the consumer behavior literature: financial, functional, physical, social, psychological, satisfaction, and time (Schiffman & Kanuk, 1991). Roehl and Fesenmaier (1992) later identified three dimensions of perceived risk: physical/equipment risk, vacation risk, and destination risk. Sonmez and Graefe (1998) identified four types of risks as most often associated with tourism: financial, psychological, satisfaction, and time. Similarly, Maser and Weiermair (1998) classified travel-related risks into several categories including, but not limited to: natural disasters, hygiene and diseases, crime, and accidents. Richter (2003) added health concerns as another category. These risk factors have been widely examined and consistently found to increase visitors' level of perceived destination risk (Larsen et al., 2009, Pizam and Mansfeld, 1996). Moreover, Barton (1994) classified 12 possible types of disasters that could affect visitors; three of them were related to natural environments, bacterial infection, and terrorist or war-related activities.
As indicated, notwithstanding some exceptional situations, visitors typically mitigate their risks when traveling (Law, 2006). Past studies have frequently shown that the tourism industry is often vulnerable because of direct or indirect incidents that might impede the safety of visitors (Maser and Weiermair, 1998, Seddighi and Theochaous, 2001, Elsrud, 2001). In their study, Leggat and Klein (2001) found that visitors often become anxious and largely depend on the destinations and the host communities for support when something goes awry. To date, there are several studies that have been conducted in the area of risk and travel decision making that demonstrate declines in tourism demand. For instance, the Bali bombings (Wilks & Moore, 2003), SARS and bird flu in Asia (Pine & McKercher, 2004), tsunami in Southeast Asia (Morison, 2005), and the Olympic Games in London (Schroeder et al., 2013) all have been studied in reference to travel and destination risk.
Sonmez and Graefe (1998), for instance, found that perceived risk is a significant predictor of avoiding certain destinations. Likewise, Buttle and Bok (1996) found that environmental influences could affect consumer behavior. Other studies have confirmed that risk perceptions are pivotal factors that influence visitors' travel decisions. When individuals perceive that potential risks outweigh benefits, they are more likely to modify their travel to the destination. In turn, this negatively affects tourism-related businesses and images associated with destinations. Implications of SARS show how a region's economy can be impacted as a consequence of fear of contracting a disease (Yanni, Marano, & Han, 2010).
Leggat et al. (2010) found that while the outbreak of H1N1 in 2009 was of some concern to more than half of the residents of Queensland, Australia, a majority of respondents would not have postponed travel even if they exhibited symptoms consistent with the pandemic. Although a majority of this research is case-based, continuous research in the area of pandemics, risk, and travel is critical to providing information for the tourism industry to better respond in times of health-related crises.
4. Methods
An online survey was administered to over 2000 random adults in the U.S. in October 2014. Respondents spent an average of 13 min to complete the survey. A Dillman online survey procedure was used to increase participation (Dillman, Smyth, & Christian, 2009). This included two reminder emails. In the end, a total of 1613 completed surveys were available for this study.
4.1. Construct operationalization
There were six independent variables in this study. First, perceived travel risk associated with Ebola was measured using 11 statements on a 5 point Likert scale with 1 = strongly disagree and 5 = strongly agree, which were adapted from Lee et al. (2012). Second, perceived susceptibility was measured using five statements measuring the level of the perceived susceptibility associated with Ebola using a 5 point Likert scale with 1 = strongly disagree and 5 = strongly agree, that were adopted from Buglar et al. (2010). Third, perceived severity was measured with four statements measuring the level of the perceived severity associated with Ebola with 1 = strongly disagree and 5 = strongly agree, that were adopted from Akompab et al. (2013). Fourth, self-efficacy was measured using five statements regarding an individual's self-efficacy associated with Ebola with 1 = strongly disagree and 5 = strongly agree, that were adopted from Lee et al. (2012) and Anagnostopoulous, Dimitrakaki, Niakas, and Tountas (2013). These items were adapted to measure the associated construct due to relevancy and robustness. Fifth, subjective knowledge was measured by asking respondents to rate their knowledge associated with Ebola on a 5 point Likert scale where 1 = not at all knowledgeable to 5 = very knowledgeable. Sixth, sociodemographic factors were measured by asking respondents their age, gender, education, household income, and frequency of past international travel. The dependent variable was measured by one question on the likelihood of avoiding travel within the U.S. due to the recent Ebola cases on a 5 point Likert scale of 1 = extremely unlikely to 5 = extremely likely.
4.2. Data analysis
Multi stage data analysis was used to answer the research questions in this study. First, descriptive analysis was used to examine the spread and normality of the data. Second, reliability tests were conducted to ensure the consistency of the items. Finally, an ordered response model (McKelvey & Zavoina, 1975) was employed to relate the likelihood of travel avoidance within the U.S. to the aforementioned independent variables. The model recognized the inherent ordering in the outcome variables of interest and allows for calculation of the probability of each level of outcome as a function of explanatory factors. A statistical analysis was performed using the SPSS 22 package.
5. Results
5.1. Profiles of respondents
Of the 1613 completed surveys, males represented 47.3% of the sample and females represented 52.7%. The average age was 47 years old with the youngest age of 19 and the oldest age of 87. Approximately 36% had college degrees and 21.3% had some college credit. Those with advanced degrees represented 18% of the sample. The sample was skewed toward Caucasians, who represented over 87% of the sample, which calls for caution in interpreting the data. Those with a 2013 annual household income of between $50,001 and $75,000 represented 21% of the sample, while 18% of the sample earned $75,001 to $100,000 in 2013. A majority of the sample (73%) had not traveled internationally within the past 12 months. Over 75% of respondents indicated that they were somewhat knowledgeable about Ebola (M = 3.31, SD = 0.95) and that they were slightly comfortable flying domestically (M = 3.50, SD = 1.35). Table 1 outlines the key sociodemographic factors of our sample.
Table 1.
Sociodemographic factors.
| Variable | Number | Percent |
|---|---|---|
| Age Mean = 47 | 1613 | |
| Youngest = 19 | ||
| Oldest = 87 | ||
| Gender | ||
| Male | 763 | 47.3 |
| Female | 850 | 52.7 |
| Education | ||
| Less than high school | 23 | 1.4 |
| High school | 237 | 14.7 |
| Some college | 344 | 21.3 |
| College degree | 585 | 36.3 |
| Advanced degree | 291 | 18.0 |
| Some graduate school | 82 | 5.1 |
| Technical school | 51 | 3.2 |
| Race and ethnicity | ||
| Caucasian/white | 1418 | 87.9 |
| Black/African American | 45 | 2.8 |
| Asian | 60 | 3.7 |
| Native Hawaii/Pacific Islander | 3 | 0.2 |
| Hispanic/Latino | 45 | 2.8 |
| American Indian/Alaskan Natives | 9 | 0.6 |
| Multi ethnic/mixed race | 15 | 0.9 |
| Other | 18 | 1.1 |
| 2013 household income | ||
| Under $24,000 | 171 | 10.6 |
| $24,001–$35,000 | 174 | 10.8 |
| $35,001–$50,000 | 247 | 15.3 |
| $50,001–$75,000 | 339 | 21.0 |
| $75,001–$100,000 | 290 | 18.0 |
| $100,001–$125,000 | 178 | 11.0 |
| $125,001–$150,000 | 95 | 5.9 |
| Above $150,000 | 119 | 7.4 |
| International travel | ||
| None | 1185 | 73.5 |
| More than 1 | 428 | 26.5 |
Subjective Ebola knowledge on a 1–5 scale (Not at all knowledgeable –very knowledgeable) M = 3.31 (SD = 0.95).
Comfort of flying domestically on a 1–5 scale (very uncomfortable – very comfortable) M = 3.50 (SD = 1.45).
5.2. Reliability test results
We were interested in the possibility of creating a composite score from the items. Thus, we tested the unidimensionality with reliability tests. Principal component analyses were also conducted and yielded similar results. Reliability tests indicated that all scales had high Cronbach alphas with 0.91, 0.93, 0.80, and 0.87 for perceived travel risk, perceived susceptibility, perceived severity, and self-efficacy scales respectively, which indicated the unidimensionality of the scales. Therefore, a composite score for each scale was created. Table 2 outlines the results of the reliability test for perceived travel risk. Table 3 presents the results of the reliability test for perceived susceptibility. Table 4 presents the results of the reliability test for perceived severity. Table 5 presents the results of the reliability test for self-efficacy.
Table 2.
Perceived travel risk.a
| Item | Mean | SD | Cronbach's Alpha |
|---|---|---|---|
| Perceived travel risk | 0.91 | ||
|
2.53 | 1.19 | |
|
2.34 | 1.14 | |
|
2.70 | 1.16 | |
|
2.40 | 1.17 | |
|
3.17 | 1.27 | |
|
2.78 | 1.25 | |
|
2.80 | 1.27 | |
|
3.14 | 1.23 | |
|
2.63 | 1.09 | |
|
2.92 | 1.13 | |
|
4.24 | 0.91 |
1 = strongly disagree to 5 = strongly agree.
All 1613 responded to the above survey items.
Table 3.
Perceived susceptibility.a
| Item | Mean | SD | Cronbach's Alpha |
|---|---|---|---|
| Perceived susceptibility | 0.93 | ||
|
1.88 | 1.01 | |
|
1.86 | 0.98 | |
|
1.99 | 1.00 | |
|
1.96 | 1.05 | |
|
2.32 | 1.17 |
1 = strongly disagree to 5 = strongly agree.
All 1613 responded to the above survey items.
Table 4.
Perceived severity.a
| Item | Mean | SD | Cronbach's Alpha |
|---|---|---|---|
| Perceived Severity | 0.80 | ||
|
2.87 | 1.00 | |
|
3.34 | 1.10 | |
|
3.64 | 1.01 | |
|
2.63 | 1.15 |
1 = strongly disagree to 5 = strongly agree.
All 1613 responded to the above survey items.
Table 5.
Self-efficacy.a
| Item | Mean | SD | Cronbach's Alpha |
|---|---|---|---|
| Self-Efficacy | 0.87 | ||
|
3.94 | 0.882 | |
|
3.63 | 0.94 | |
|
3.70 | 0.90 | |
|
3.26 | 1.04 | |
|
3.57 | 1.02 |
1 = strongly disagree to 5 = strongly agree.
All 1613 responded to the above survey items.
On average, respondents demonstrated low perceptions of risk on all items. Although the sample indicated that international travel seemed riskier than domestic travel, most respondents agreed that Ebola is a very frightening disease. This is partly explained by the fact that more than half of our sample have never traveled internationally before. The overall mean score for perceived risk was 2.88, indicating an overall low perception of risk associated with Ebola. The overall mean score of the perceived susceptibility scale was 2.00, indicating low perceived susceptibility related to Ebola in general.
The overall mean score for the perceived severity construct was 3.12, which indicated the relative neutrality of the respondents. Nonetheless, it is also important to note that, on average, the respondent also agreed that if they test positive for Ebola, they could pass it to their family and friends who may die because of it.
The overall mean score for self-efficacy was 3.62, indicating a relatively high self-efficacy among our respondents. Likewise, the mean score for subjective knowledge was 3.31(SD: 0.95), indicating relatively neutral subjective knowledge related to Ebola.
5.3. Ordered Response Model results
In the Ordered Response Model, a positive parameter indicated that the corresponding variable was associated with a higher likelihood of avoiding travel in the U.S. due to the recent Ebola cases and a negative parameter indicated the opposite effect. The parameters of the model were estimated using the maximum likelihood estimator. The − 2 Log likelihood at convergence was 3515.222 (χ2 = 1152.526, df = 9, sig. = 0.001), indicating a significant improvement from the baseline model. The model with all independent variables accounted for 55% of the variance in the likelihood of travel avoidance. Table 6 outlines the results of the ordered response model.
Table 6.
Summary of Ordered Response Model.
| Variable | Parameter estimate | Significance |
|---|---|---|
| Perceived travel risk | 1.450 | 0.001⁎ |
| Perceived susceptibility | 0.584 | 0.001⁎ |
| Perceived severity | − 0.041 | 0.58 |
| Self-efficacy | − 0.311 | 0.001⁎ |
| Subjective knowledge | 0.228 | 0.001⁎ |
| Age | − 0.014 | 0.001⁎ |
| Female [ref: male] | 0.324 | 0.002⁎ |
| Frequency of international travel | 0.008 | 0.387 |
| Thresholds | ||
| Avoid travel = 1 | 4.062 | 0.001 |
| Avoid travel = 2 | 5.530 | 0.001 |
| Avoid travel = 3 | 7.449 | 0.001 |
| Avoid travel = 4 | 8.635 | 0.001 |
− 2 Log likelihood at convergence (n = 1613) 3515.222 (χ2 = 1188.493, df = 9, sig. 0.001) Pseudo R2Negelkerke = 0.551.
Sig < 0.05
Related to Research Question 1, the model indicated that there was a positive relationship between perceived travel risk and travel avoidance (β = 1.450, p = 0.001), with those who held higher risk perceptions related to travel showing a higher propensity to avoid travel due to Ebola cases. For Research Question 2, the model indicated that there was a positive relationship between perceived susceptibility and avoiding travel due to Ebola cases (β = 0.584, p = 0.001). As such, those who indicated a higher susceptibility to Ebola also demonstrated a higher propensity to avoid travel.
For Research Question 3, the model revealed no significant relationship between perceived severity and the likelihood of travel avoidance (β = − 0.041, p = 0.58). For Research Question 4, the model revealed a negative relationship between self-efficacy and the likelihood of travel avoidance (β = − 0.311, p = 0.001). That means those with lower self-efficacy were more likely to avoid travel due to Ebola. Regarding Research Question 5, the model found a positive relationship between subjective knowledge and the likelihood of travel avoidance (β = 0.228, p = 0.001), with those exhibiting higher levels of subjective knowledge being more likely to avoid travel due to Ebola.
Research Question 6, which focused on sociodemographic factors, yielded interesting findings. The model found a negative relationship between age and the likelihood to avoid travel (β = − 0.014, p = 0.001), with younger age groups showing a greater propensity of travel avoidance due to Ebola. The model also indicated a positive relationship between gender and travel avoidance (β = 0.324, p = 0.002), with females being more likely to avoid travel due to Ebola. No significant relationship was found between frequency of international travel and the propensity to avoid domestic travel (β = 0.008, p = 0.387). This is probably due to the fact that a majority of the respondents had not previously traveled internationally.
6. Discussion
Previous emerging infectious disease outbreaks such as severe acute respiratory syndrome (SARS) or H1N1 influenza pandemic have had far reaching impacts on travel and tourism, specifically with enhanced health screenings and increased travel delays due to the shutdown of airline travel. While the Ebola outbreak has arguably not had the same impacts, concerns have been raised by travelers and government travel advisories. In this study, more than half of our sample indicated that they had concerns regarding Ebola during travel by air and more than half also indicated that they would not avoid traveling in light of recent Ebola cases in the U.S. This is consistent with the fact that airlines in the U.S. remained operational during the outbreak and that while the U.S. government did designate several airports for passenger screening, especially those traveling back from African countries which includes New York's John F. Kennedy, Chicago's O′Hare, Atlanta's Hartfield-Jackson, Newark's Liberty, and Washington's Dulles Airport, the U.S. government travel advisories did not affect both international and domestic air travel. These findings are also consistent with a survey conducted by the Global Business Travel Association, which indicated that most respondents said the outbreak has had a minimal effect on business travel (Martin, 2014). As such, the quick reactions by the U.S. government to respond to the potential outbreak in the U.S. may have influenced travelers' decisions related to travel and curtailing their travel. Another possible reason is that we only asked respondents about their travel avoidance related to domestic travel (within the U.S.). As such, using international travel as a dependent variable may have yielded different results.
The findings revealed several predictors that may affect domestic travel avoidance in light of Ebola cases, many of which were conflicting in nature and undocumented in the literature on travel risk and contagious diseases. The strongest predictor was perceived travel risk associated with Ebola, with those with higher perceived levels of risk having shown a greater propensity to avoid travel within the U.S. In one study, respondents who viewed themselves at increased risk for SARS were more likely to take precautionary actions to avoid contracting the disease (Brug et al., 2004). In another study, respondents with feelings of high perceived susceptibility were more likely to take preventive measures against the human avian influenza (de Zwart, Veldhuijzen, Richardus, & Brug, 2010).
The findings were largely parallel with previous studies using HBM. For instance, those with higher self-efficacy related to adhering to preventive measures were less likely to avoid travel to locations that are being impacted by infectious diseases. Individuals who reported higher feelings of self-efficacy reported lower levels of susceptibility in acquiring transmissible diseases (Liao, Cowling, Lam, Ng, & Fielding, 2010). This could be explained by the fact that these individuals may strongly believe that since they have control over behavior choices associated with an ailment, they are at a lower risk for transmission.
Interestingly, the study found no significant relationship between perceived severity and travel avoidance. Chen et al. (2011) found that perceived severity was not associated with caregivers seeking influenza vaccinations for their children. A previous study reported that participants' perceived severity of H1N1 did not predict their acceptability of a vaccine for the malady (Coe, Gatewood, Moczygemba, Goode, & Beckner, 2012). Contrary to our findings, several previous studies have confirmed opposite findings. Individuals believing that avoiding travel, especially to places experiencing an epidemic, will help prevent their risk of acquiring the disease (Lau, Griffiths, Choi, & Tsui, 2009). A possible explanation is that while perceived susceptibility of being exposed to Ebola might be steady over time, perceived severity might decrease with increases in knowledge of the disease.
Some studies have found that anxiety associated with a disease may lead some individuals to report lower use of preventive measures (Cowling et al., 2010). Healthcare workers who believed that a vaccine for influenza A (H1N1) was effective were more likely to take it (Seale et al., 2011). Knowledge or previous experiences with vaccines may also lead to the use of vaccines or other preventive measures (Arda et al., 2011).
The current study yielded an interesting finding between the positive relationship between travel avoidance and being female. Perhaps women who perceived more risk from infectious diseases (Brug et al., 2004) may be more likely to act upon those preventive measures adding to increased feelings of self-efficacy. Another possibility is that women, due to their “ethic of care” might be more concerned with becoming sick or having their loved ones become sick. This is an interesting finding which might yield unique results due to the context of a health risk. In contrast to our findings, one study found that women reported lower levels of self-efficacy to engage in protective methods against influenza when compared to men (de Zwart et al., 2007). Understanding differences among men and women in a travel health risk context might provide valuable messaging and targeting information for Destination Management Organizations and members of the travel industry.
Is the risk of contracting a disease a major concern for travelers? According to a study looking at Americans' fears and worries about living outside of the country, this may not be true. American students traveling abroad cited fears associated with contaminated food and water, psychological distress, excessive sun exposure, and physical/sexual assault over fears of contracting certain infectious diseases (e.g. Ebola, the plague) (Hartjes, Baumann, & Henriques, 2009). The avoidance of public transportation is cited as one of the most utilized preventive measures to avoid contracting an infectious disease (Sadique et al., 2007). Thus, understanding differences in residence and travel history and frequency might provide revealing information that may help the travel industry better manage messages targeted toward tourists.
The current study yielded results which indicated that individuals who reported having low levels of self-efficacy were more likely to avoid travel. Self-efficacy plays an important role in whether one chooses to adopt a behavior, specifically a health behavior. Perceived positive outcomes of a behavior were associated with greater confidence in performing the behavior (Maddux, Sherer, & Rogers, 1982). High levels of perceived self-efficacy correlated with an increased willingness for individuals to adopt healthy preventive behaviors (e.g. exercise habits) (Kelly, Zyzanski, & Alemagno, 1991).
These findings have important consequences for public health and travelers. Although this study did not look at specific travel-related preventive measures against Ebola, public education in the U.S. has focused on simple measures, such as hand washing, which travelers could utilize as a preventive measure for Ebola. These findings can also help public health officials to focus education efforts for both international and domestic travelers, especially those who showed higher concern over the outbreak, and might be appropriate audiences for targeted information. Examples of this include providing information in airports, in airport bathrooms, on online tickets, in hotel rooms, and so forth.
Subjective knowledge was found to be positively associated with travel avoidance. This may be partly explained by the relationship between knowledge and the likelihood of anticipated complacence with public health recommendations. As such, greater understanding of Ebola may result in a better command of public health recommendations. Perhaps more imperative, older participants appeared less likely to cancel their travel. Several other studies have noted greater perceived severity of health diseases (Barr, Raphael, & Taylor, 2008), which may in part explain the greater acceptance of public health measures among our sample. As such, they may be proper targets for both public health education and in-coming traveler screening.
There are critical implications from this research. The findings can help policymakers identify issues of high concern among travelers that require management actions, as well as to recognize potentially contentious issues that will require special effort. For example, the role of travel insurance and pre-travel expenses (e.g., nonrefundable hotel booking fee) in influencing travel avoidance. Public perceptions of Ebola have changed during the events surrounding the 2014 outbreak. Our results may support future efforts to evaluate changes in attitudes and perceptions toward the outbreak among travelers due to awareness of 2014 Ebola screening measures at several U.S. ports of entry and Ebola more generally.
The study was limited in that it relied on an online survey to collect data at a time when the outbreak was salient. The survey was conducted in October of 2014 during the height of the Ebola outbreak, during which time the U.S. public was bombarded with media coverage of the outbreak that might have shaped their perceptions. Thus, it may be challenging to generalize the results of the study beyond the time due to the prevalence of information in the media regarding this crisis. Ibuka et al. (2010) also noted that perceptions of disease changed over time along with the media coverage. Specifically, the decline in the engagement in the preventive health strategies (in this case travel avoidance) may also mirror the decline in media attention regarding Ebola in the United States. As such, further study should explore how perceptions of Ebola and other pandemics changed over time and how it relates to media attention, as well as engagement in the recommended health preventive strategies. The survey also relied on self-reported data with its inherent bias, as what respondents report may differ from what they actually do.
7. Conclusion
We believe that the variables identified by respondents regarding travel avoidance due to the Ebola outbreak were relevant. Our results indicated that most respondents considered Ebola to be serious and would take protective measures in response to the outbreak. However, most of them also demonstrated a minimal plan to avoid travel which is parallel with other studies on contagious pandemics. The adapted Health Belief Model helps us to understand this phenomenon. As predicted by the model, those with higher perceptions of risk, perceived susceptibility, and subjective knowledge were found to be more likely to avoid domestic travel, while those with higher levels of self–efficacy demonstrated a lower propensity to avoid travel due to Ebola. It is important to note that the study did not specifically examine the role of “cues to action.” This is not to say that the construct is not important. Rather, we were interested in examining the roles of other constructs in the Health Belief Model. Therefore, it is recommended that future research includes “cues to action” in the model to determine the role of the construct.
Finally, due to the multifaceted nature of the issues, further study needs to be conducted to fully understand the complexity of attitudes toward contagious diseases. Additionally, further research could also explore the relationship between the attitudes and perceptions of travelers and travel destinations. Given the improbability surrounding how the 2014 Ebola outbreak may (re)emerge in the future, our results may contribute in planning for and responding to crises in the context of air travel. For instance, travelers may have also considered other logistic costs, such as fees for changing a travel itinerary or extending planned accommodations, as part of decision making in travel avoidance. Although not directly measured in our study, such factors might influence their attitude toward travel avoidance in the wake of Ebola or other pandemics, which warrant further exploration.
Biographies

Dr. Ignatius Cahyanto is an Assistant Professor at Black Hills State University in South Dakota. His research interest is centered around crisis management for the tourism industry. He is particularly interested in understanding tourists' behavior in the event of crises.

Michael Wiblishauser, Ph.D., CHES is an Assistant Professor of Health Education at Lock Haven University, Lock Haven Pennsylvania. His research interests include substance use prevention & treatment, violence prevention, and health disparities.

Dr. Lori Pennington-Gray is the current Director of the Tourism Crisis Management Institute at the University of Florida. Her research primarily focuses on crisis management strategies for the tourism industry.

Ashley Schroeder, Ph.D. is an Assistant Professor at the University of Hawaii at Manoa's School of Travel Industry Management and Managing Director of the University of Florida's Tourism Crisis Management Initiative. Ashley has expertise in destination management and her primary research interest is tourism crisis management.
Contributor Information
Ignatius Cahyanto, Email: ignatius.cahyanto@bhsu.edu.
Michael Wiblishauser, Email: mjw939@lhup.edu.
Lori Pennington-Gray, Email: pengray@hhp.ufl.edu.
Ashley Schroeder, Email: aschroe@hawaii.edu.
References
- Adams J., Scott J. Predicting medication adherence in severe mental disorders. Acta Psychiatrica Scandinavica. 2000;101:119–124. doi: 10.1034/j.1600-0447.2000.90061.x. [DOI] [PubMed] [Google Scholar]
- Akompab D.A., Bi P., Williams S., Grant J., Walker I.A., Augoustinos M. Heat waves and climate change: Applying the HBM to identify predictors of risk perception and adaptive behaviors in Adelaide, Australia. International Journal of Environmental Research and Public Health. 2013;10:2164–2184. doi: 10.3390/ijerph10062164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anagnostopoulous F., Dimitrakaki C., Niakas D., Tountas Y. Validity and reliability assessment of health belief scales for mammography screening in Greek asymptomatic women. Psycho-Oncology. 2013;22:1912–1917. doi: 10.1002/pon.3212. [DOI] [PubMed] [Google Scholar]
- Arda B., Durusoy R., Yamazhan T., Sipahi O.R., Tasbakan M., Pullukcu H., Ulusoy S. Did the pandemic have an impact on influenza vaccination attitude? A survey among health care workers. BMC Infectious Diseases. 2011;11(1):87. doi: 10.1186/1471-2334-11-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ayele T., Abebe T., Girma Self care behavior among patients with diabetes in Harari, Eastern Ethiopia: The HBM perspective. PloS One. 2012;7(4):35515. doi: 10.1371/journal.pone.0035515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review. 1977;84(2):191–215. doi: 10.1037//0033-295x.84.2.191. [DOI] [PubMed] [Google Scholar]
- Barbisch D., Koenig K.L., Shih F.Y. Is there a case for quarantine? Perspectives from SARS to Ebola. Disaster Medicine and Public Health Preparedness. 2015:1–7. doi: 10.1017/dmp.2015.38. [DOI] [PubMed] [Google Scholar]
- Barr M., Raphael B., Taylor M. Pandemic influenza in Australia: Using telephone surveys to measure perceptions of threat and willingness to comply. BMC Infectious Diseases. 2008;8:117. doi: 10.1186/1471-2334-8-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barton L. Crisis management: preparing and managing disasters. Cornell Hotel and Restaurant Administration Quarterly. 1994;35(2):59–65. April. [Google Scholar]
- Bish A., Michie S. Demographic and attitudinal determinants of protective behaviors during a pandemic: A review. British Journal of Health Psychology. 2010;15:797–824. doi: 10.1348/135910710X485826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bogoch I., Creatore M.I., Cetron M.S., Brownstein J.S., Pesik N., Miniota J., Khan K. Assessment of the potential for international dissemination of Ebola virus via commercial air travel during the 2014 west African outbreak. The Lancet. 2015;385(9962):29–35. doi: 10.1016/S0140-6736(14)61828-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brewer N.T., Fazekas K.I. Predictors of HPV vaccine acceptability: A theory-informed, systematic review. Preventive Medicine. 2007;45(2–3):107–114. doi: 10.1016/j.ypmed.2007.05.013. [DOI] [PubMed] [Google Scholar]
- Brewer N.T., Hallman W.K. Subjective and objective risk as predictors of influenza vaccination during the vaccine shortage of 2004–2005. Clinical Infectious Diseases. 2006;43(11):1379–1386. doi: 10.1086/508466. [DOI] [PubMed] [Google Scholar]
- Brewer N.T., Chapman G.B., Gibbons F.X., Gerrard M., McCaul K.D., Weinstein N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychology. 2007;26(2):136–145. doi: 10.1037/0278-6133.26.2.136. [DOI] [PubMed] [Google Scholar]
- Brug J., Aro A.R., Oenema A., de Zwart O., Richardus J.H., Bishop G.D. SARS risk perception, knowledge, precautions, and information sources, the Netherlands. Emerging Infectious Diseases. 2004 doi: 10.3201/eid1008.040283. http://wwwnc.cdc.gov/eid/article/10/8/04-0283_article Retrieved from. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buglar M., White K., Robinson N. The role of self-efficacy in dental patients' brushing and flushing: Testing an extended HBM. Patient Education and Counseling. 2010;78:269–272. doi: 10.1016/j.pec.2009.06.014. [DOI] [PubMed] [Google Scholar]
- Buttle F., Bok B. Hotel marketing strategy and the theory of reasoned action. International Journal of Contemporary Hospitality Management. 1996;8(3):5–10. [Google Scholar]
- Carpenter C.J. A meta-analysis of the effectiveness of the HBM variables in predicting behavior. Health Communication. 2010;25(8):661–669. doi: 10.1080/10410236.2010.521906. [DOI] [PubMed] [Google Scholar]
- Carr N. An exploratory study of gendered differences in young tourists' perception of danger within London. Tourism Management. 2001;22:565–570. [Google Scholar]
- Centers for Disease Control and Prevention Ebola (Ebola Virus Disease): Prevention. 2015. http://www.cdc.gov/vhf/ebola/prevention/ Retrieved on July 2015 from.
- Centers for Disease Control and Prevention Ebola (Ebola Virus Disease): Ebola Outbreaks 2000–2014. 2015. http://www.cdc.gov/vhf/ebola/outbreaks/history/summaries.html Retrieved on July 2015 from.
- Cerkoney K.A.B., Hart L.K. The relationship between the HBM and compliance of persons with diabetes mellitus. Diabetes Care. 1980;3(5):594–598. doi: 10.2337/diacare.3.5.594. [DOI] [PubMed] [Google Scholar]
- Chapman G.B., Coups E.J. Predictors of influenza vaccine acceptance among healthy adults. Preventive Medicine. 1999;29(4):249–262. doi: 10.1006/pmed.1999.0535. [DOI] [PubMed] [Google Scholar]
- Chapman V.L., Skinner C.S. The Health Belief Model. In: Glanz K., Rimer B.K., Viswanath K., editors. Health behavior and health education: theory, research, and practice. 4th ed. Jossey-Bass; San Francisco: 2008. pp. 45–65. [Google Scholar]
- Chen J.Y., Fox S.A., Cantrell C., Stockdale S.E., Kagawa-Singer M. Health disparities and prevention: Racial/ethnic barriers to flu vaccinations. Journal of Community Health. 2007;32(1):5–20. doi: 10.1007/s10900-006-9031-7. [DOI] [PubMed] [Google Scholar]
- Chen M.F., Wang R.H., Schneider J.K., Tsai C.T., Jian D.D.S., Hung M.N., Lin L.J. Using the HBM to understand caregiver factors influencing childhood influenza vaccinations. Journal of Community Nursing. 2011;28:29–40. doi: 10.1080/07370016.2011.539087. [DOI] [PubMed] [Google Scholar]
- Clinic M. Diseases and conditions: Ebola virus and Marburg virus. Symptoms. 2014 http://www.mayoclinic.org/diseases-conditions/ebola-virus/basics/symptoms/con-20031241 Retrieved on January 2, 2016 from. [Google Scholar]
- Coe A.B., Gatewood S.B.S., Moczygemba L.R., Goode J.V.K.R., Beckner J.O. The use of the HBM to assess predictors of intent to receive the novel (2009) H1N1 influenza vaccine. Innovations in Pharmacy. 2012;3(2):1–11. doi: 10.24926/iip.v3i2.257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cowling B.J., Ng D.M.W., Ip D.K.M., Liao Q., Lam W.W.T., Wu J.T., Fielding R. Community psychological and behavioral responses through the first wave of the 2009 influenza A(H1N1) pandemic in Hong Kong. The Journal of Infectious Diseases. 2010;202(6):867–876. doi: 10.1086/655811. [DOI] [PubMed] [Google Scholar]
- Cross M.J., March L.M., Lapsley H.M., Byrne E., Brooks P.M. Patient self-efficacy and health locus of control: Relationships with health status and arthritis-related expenditure. Rheumatology (Oxford) 2006;45(1):92–96. doi: 10.1093/rheumatology/kei114. [DOI] [PubMed] [Google Scholar]
- de Zwart O., Veldhuijzen I.K., Elam G., Aro A.R., Abraham T., Bishop G.D., Brug J. Avian influenza risk perception, Europe and Asia. Emerging Infectious Diseases. 2007;13(2):290–293. doi: 10.3201/eid1302.060303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Zwart O., Veldhuijzen I.K., Richardus J.H., Brug J. Monitoring of risk perceptions and correlates of precautionary behavior related to human avian influenza during 2006–2007 in Netherlands: Results of seven consecutive surveys. BMC Infectious Diseases. 2010;10(1):114. doi: 10.1186/1471-2334-10-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dennis B., Craighill P.M. Ebola poll: two-third of Americans worried about possible widespread epidemic in U.S. The Washington Post. 2014;(October 14) https://www.washingtonpost.com/national/health-science/ebola-poll-two-thirds-of-americans-worried-about-possible-widespread-epidemic-in-us/2014/10/13/d0afd0ee-52ff-11e4-809b-8cc0a295c773_story.html Retrieved on June 11, 2015 from. [Google Scholar]
- Deshpande S., Basil M.D., Basil D.Z. Factors influencing healthy eating habits among college students: An application of the Health Belief Model. Health Marketing Quarterly. 2009;26(2):145–164. doi: 10.1080/07359680802619834. [DOI] [PubMed] [Google Scholar]
- Dillman D., Smyth J., Christian L. Wiley; New York: 2009. Internet, mail, and mixed-mode surveys: The Tailored Design Method. [Google Scholar]
- Elsrud T. Risk creation in traveling backpacker adventure narration. Annals of Tourism Research. 2001;28:597–617. [Google Scholar]
- Epstein J.A., Griffin K.W., Botvin G.J. A model of smoking among inner-city adolescents: The role of personal competence and perceived social benefits of smoking. Preventive Medicine. 2000;31:107–114. doi: 10.1006/pmed.2000.0674. [DOI] [PubMed] [Google Scholar]
- Floyd M.F., Gibson H., Pennington-Gray L., Thapa B. The effect of risk perceptions on intentions to travel in the aftermath of September 11, 2001. Journal of Travel & Tourism Marketing. 2003;15(2/3):19–38. [Google Scholar]
- Folayan M., Brown B. Ebola and the limited effectiveness of travel restrictions. Disaster Medicine and Public Health Preparedness. 2015;1-1 doi: 10.1017/dmp.2015.1. [DOI] [PubMed] [Google Scholar]
- Frieden T.R., Damon I., Bell B.P., Kenyon T., Nicol S. Ebola 2014 — New challenges, new global response and responsibility. The New England Journal of Medicine. 2014;371:1177–1180. doi: 10.1056/NEJMp1409903. [DOI] [PubMed] [Google Scholar]
- Gao X., Nau D.P., Rosenbluth S.A., Scott V., Woodward C. The relationship of disease severity, health beliefs and medication adherence among HIV patients. AIDS Care. 2000;12(4):387–398. doi: 10.1080/09540120050123783. [DOI] [PubMed] [Google Scholar]
- Gomes M.F.C., Piontti P.y., Rossi A., Chao L., Longini D., Halloran I.…Vespignani A. Assessing the international spreading risk associated with the 2014 West African Ebola outbreak. PLoS Currents. 2014;6 doi: 10.1371/currents.outbreaks.cd818f63d40e24aef769dda7df9e0da5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gostin L.O., Lucey D., Phelan A. The Ebola epidemic: A global health emergency. Journal of the American Medical Association. 2014;312(11):1095–1096. doi: 10.1001/jama.2014.11176. [DOI] [PubMed] [Google Scholar]
- Hales C., Shams H. Cautious incremental consumption: A neglected consumer risk reduction strategy. European Journal of Marketing. 1991;25(7):7–21. [Google Scholar]
- Halloran M.E., Ferguson N.M., Eubank S., Longini I.M., Cummings D.A.T., Lewis B.…German T.C. Modeling targeted layered containment of an influenza pandemic in the United States. Proceedings of the National Academy of Sciences of the United States of America. 2008;105(12):4639–4644. doi: 10.1073/pnas.0706849105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanson J.A., Benedict J.A. Use of the HBM to examine older adults' food handling behaviors. Journal of Nutrition Education and Behavior. 2002;34(1):S25–S30. doi: 10.1016/s1499-4046(06)60308-4. [DOI] [PubMed] [Google Scholar]
- Hartjes L.B., Baumann L.C., Henriques J.B. Travel abroad risk perceptions and prevention behaviors of US students. Journal of Travel Medicine. 2009;16(5):338–342. doi: 10.1111/j.1708-8305.2009.00322.x. [DOI] [PubMed] [Google Scholar]
- Hounton S.H., Carabin H., Henderson N.J. Towards an understanding of barriers to condom use in rural Benin using the HBM: A cross sectional survey. BMC Public Health. 2005;5(1):8. doi: 10.1186/1471-2458-5-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ibuka Y., Chapman G.B., Meyers L.A., Li M., Galvani A. The dynamics of risk perceptions and precautionary behavior in response to 2009 (H1N1) pandemic influenza. BioMed Central Infectious Diseases. 2010;10:296. doi: 10.1186/1471-2334-10-296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iskender M., Akin A. Social self-efficacy, academic locus of control; and internet addiction. Computers & Education. 2010;54(4):1101–1106. [Google Scholar]
- Janz N.K., Becker M.H. The HBM: A decade later. Health Education Quarterly. 1984;11(1):1–47. doi: 10.1177/109019818401100101. [DOI] [PubMed] [Google Scholar]
- Kelly R.B., Zyzanski S.J., Alemagno S.A. Prediction of motivation and behavior change following health promotion: Role of health beliefs, social support, and self-efficacy. Social Science & Medicine. 1991;32(3):311–320. doi: 10.1016/0277-9536(91)90109-p. [DOI] [PubMed] [Google Scholar]
- Kuo H.I., Chen C.C., Tseng W.C., Ju L.F., Huang B.W. Assessing impacts of SARS and Avian Flu on international tourism demand to Asia. Tourism Management. 2008;29(5):917–928. doi: 10.1016/j.tourman.2007.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larsen S., Brun W., Øgaard T. What tourists worry about – Construction of a scale measuring tourist worries. Tourism Management. 2009;30(2):260–265. [Google Scholar]
- Lau J.T.F., Griffiths S., Choi K.C., Tsui H.Y. Widespread public misconception in the early phase of the H1N1 influenza epidemic. Journal of Infection. 2009;20:1–6. doi: 10.1016/j.jinf.2009.06.004. [DOI] [PubMed] [Google Scholar]
- Lau J.T.F., Yeung N.C.Y., Choi K.C., Cheng M.Y.M., Tsui H.Y., Griffiths S. Factors in association with acceptability of A/H1N1 vaccination during the influenza A/H1N1 pandemic phase in the Hong Kong general population. Vaccine. 2010;28:4632–4637. doi: 10.1016/j.vaccine.2010.04.076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Law R. The perceived impact of risks on travel decisions. International Journal of Tourism Research. 2006;8:289–300. [Google Scholar]
- Lee C., Son H., Bendle L., Kim M., Han H. The impact of non-pharmaceutical interventions for 2009 H1N1 influenza on travel intentions: A model of goal-directed behavior. Tourism Management. 2012;33:89–99. doi: 10.1016/j.tourman.2011.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leggat P.A., Klein M. Personal safety advice for travelers abroad. Journal of Travel Medicine. 2001;8(1):46–51. doi: 10.2310/7060.2001.5170. [DOI] [PubMed] [Google Scholar]
- Leggat P.A., Brown L.H., Aitken P., Speare R. Level of concern and precaution taking among Australians regarding travel during pandemic (H1N1) 2009: Results from the 2009 Queensland social survey. Journal of Travel Medicine. 2010;17(5):291–295. doi: 10.1111/j.1708-8305.2010.00445.x. [DOI] [PubMed] [Google Scholar]
- Liao Q., Cowling B., Lam W.T., Ng M.W., Fielding R. Situational awareness and health protective responses to pandemic influenza A(H1N1) in Hong Kong: A cross sectional study. PloS One. 2010;5(10) doi: 10.1371/journal.pone.0013350. (e13350) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackenzie D. Ebola travel ban will not work. New Scientist. 2014;224(2992):4–5. [Google Scholar]
- Maddux J.E., Sherer M., Rogers R.W. Self-efficacy expectancy and outcome expectancy: Their relationship and their effects on behavioral intentions. Cognitive Therapy and Research. 1982;6(2):207–211. [Google Scholar]
- Martin H. Ebola scare has had minimal effect on business travel, survey finds. 2014, October 19. http://www.latimes.com/business/la-fi-travel-briefcase-20141018-story.html Retrieved on January 2, 2016 from.
- Maser B., Weiermair K. Travel decision-making: From the vintage point of perceived risk and information preferences. Journal of Travel & Tourism Marketing. 1998;7(4):107–121. [Google Scholar]
- McCarthy M. CDC rejects mandatory quarantine for travelers arriving from Ebola stricken nations. BMJ. 2014;349:g6499. doi: 10.1136/bmj.g6499. [DOI] [PubMed] [Google Scholar]
- McKelvey R.D., Zavoina W. A statistical model for the analysis of ordinal level dependent variables. Journal of Mathematical Sociology. 1975;4:103–120. [Google Scholar]
- Morison A. National quirks add cues to grim game of chance. South China Morning Post. 2005;3 January(EDT4) [Google Scholar]
- Nicholls H. Pandemic influenza: The inside story. PLoS Biology. 2006;4(2):e50. doi: 10.1371/journal.pbio.0040050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pine R., McKercher B. The impact of SARS on Hong Kong's tourism industry. International Journal of Contemporary Hospitality Management. 2004;16(2):139–143. [Google Scholar]
- Pizam A., Mansfeld Y. Wiley; New York, NY: 1996. Tourism, crimes and international security issues. [Google Scholar]
- Poletto C., Gomes M.F., Pastore Y., Piontti A., Rossi L., Bioglio L.…Vespignani A. Assessing the impact of travel restrictions on international spread of the 2014 West African epidemic. Eurosurveillance. 2014;19(42) doi: 10.2807/1560-7917.es2014.19.42.20936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Read J.M., Diggle P.J., Chirombo J., Solomon T., Baylsis M. Effectiveness of screening for Ebola at airports. The Lancet. 2015;385(9962):23–24. doi: 10.1016/S0140-6736(14)61894-8. [DOI] [PubMed] [Google Scholar]
- Reisinger Y., Mavondo F. Travel anxiety and intentions to travel internationally: Implication of travel risk perception. Journal of Travel Research. 2005;43:212–222. [Google Scholar]
- Richter L. International tourism and its global health consequences. Journal of Travel Research. 2003;41(4):340–347. [Google Scholar]
- Roehl W., Fesenmaier D. Risk perception and pleasure travel: An explanatory analysis. Journal of Travel Research. 1992;30(4):17–26. [Google Scholar]
- Rosenstock I.M., Strecher V.J., Becker M.H. Social learning theory and the HBM. Health Education & Behavior. 1988;15(2):175–183. doi: 10.1177/109019818801500203. [DOI] [PubMed] [Google Scholar]
- Sadique M.Z., Edmunds W.J., Smith R.D., Meerding W.J., DeZwat O., Brug J., Beutels P. Precautionary behavior in response to perceived threat of pandemic influenza. Emerging Infectious Diseases. 2007;13(9):1307–1313. doi: 10.3201/eid1309.070372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schiffman L., Kanuk L. Prentice Hall; Englewood Cliffs, NJ: 1991. Consumer behavior. [Google Scholar]
- Schroeder A., Pennington-Gray L., Kaplanidou K., Zhan F. Destination risk perceptions among U.S. residents for London as the host city of the 2012 Summer Olympic Games. Tourism Management. 2013;38:107–119. [Google Scholar]
- Seale H., Kaur R., Wang Q., Yang P., Zhang Y., Wang X., MacIntrye C.R. Acceptance of a vaccine against pandemic influenza A (H1N1) virus amongst healthcare workers in Beijing, China. Vaccine. 2011;29(8):1605–1610. doi: 10.1016/j.vaccine.2010.12.077. [DOI] [PubMed] [Google Scholar]
- Seddighi H.M., Theochaous A. Does cultural background of tourists influence the destination choice? An empirical study with special references to political instability. Tourism Management. 2001;22:181–191. [Google Scholar]
- Setbon M., Raude J. Factors in vaccination intention against the pandemic influenza A/H1N1. European Journal of Public Health. 2010;20(5):490–494. doi: 10.1093/eurpub/ckq054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharifirad G., Entezari M.H., Kamran A., Azadbakht L. The effectiveness of nutritional education on the knowledge of diabetic patients using the HBM. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences. 2009;14(1):1. [PMC free article] [PubMed] [Google Scholar]
- Smith P.J., Humiston S.G., Marcuse E.K., Zhao Z., Dorell C.G., Howes C., Hibbs B. Parental delay or refusal of vaccine doses, childhood vaccination coverage at 24 months of age, and the Health Belief Model. Public Health Reports. 2011;126(Suppl 2):135–146. doi: 10.1177/00333549111260S215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sonmez S., Graefe A. Influence of terrorism risk on foreign tourism decision. Annals of Tourism Research. 1998;25(1):112–144. [Google Scholar]
- Stroud N., Minahan C., Sabapathy S. The perceived benefits and barriers to exercise participation in persons with multiple sclerosis. Disability and Rehabilitation. 2009;31:2216–2222. doi: 10.3109/09638280902980928. [DOI] [PubMed] [Google Scholar]
- Tavafian S.S., Hasani L., Aghamofaei T., Zare S., Gregory D. Prediction of breast self-examination in a sample of Iranian women: An application of the HBM. BMC Women's Health. 2009;9(1):37. doi: 10.1186/1472-6874-9-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsaur S.H., Tzeng G.H., Wang K.C. Evaluating tourist risks from fuzzy perspectives. Annals of Tourism Research. 1997;24(4):796–812. [Google Scholar]
- Wilks J., Moore S. APEC International Centre for Sustainable Tourism (AICST); Commonwealth of Australia: 2003. Tourism risk management for the Asia Pacific Region: An authoritative guide for managing crises and disasters. [Google Scholar]
- World Health Organization Ebola virus disease: Fact sheet N°103. 2014. http://www.who.int/mediacentre/factsheets/fs103/en/ Retrieved on January 2, 2016 from.
- Yanni E.A., Marano N., Han P. Knowledge, attitudes, and practices of US travelers to Asia regarding seasonal influenza and H5N1 avian influenza prevention measures. Journal of Travel Medicine. 2010;17:374–381. doi: 10.1111/j.1708-8305.2010.00458.x. [DOI] [PubMed] [Google Scholar]
- Yavas U. Correlates of vacation travel: Some empirical evidence. Journal of Professional Services Marketing. 1990;5(2):3–18. [Google Scholar]
- Yuksel A., Yuksel F. Shopping risk perceptions: Effects on tourists' emotion, satisfaction and expressed loyalty intentions. Tourism Management. 2007;28:703–713. [Google Scholar]