

Abstract
Buprenorphine is an effective treatment for chronic pain and may reduce opioid-induced hyperalgesia. However, its pharmacological properties make its induction challenging, time-consuming, and can precipitate opioid withdrawal. We present the case of a 66-year-old woman with inadequately controlled postoperative pain despite escalating doses of oxycodone and methadone, who was successfully transitioned to buprenorphine/naloxone using a rapid microinduction technique without precipitating opioid withdrawal. Rapid induction provides an alternative method for transitioning patients from other opioids to buprenorphine/naloxone and facilitates transition of patients with chronic pain to buprenorphine therapy within a shorter window compared to currently existing protocols.
Prevalence of chronic pain ranges from 11% to 39% in adult populations and is ideally managed through multimodal nonpharmacological and pharmacological measures including mindfulness, cognitive behavioral therapy, and nonopioid analgesics.1,2 Opioids are effective for treatment of acute pain through agonism of μ-opioid receptors.3 However, their role in chronic pain is increasingly questioned, given their adverse effects and potential for dependence.3 Furthermore, high-dose opioids can cause opioid-induced hyperalgesia, which may be related to κ-opioid receptor agonism.4
Buprenorphine provides analgesia through μ-opioid receptor agonism.5 In addition, its κ-opioid receptor antagonism property can reduce opioid-induced hyperalgesia caused by other opioids that are κ-opioid receptor agonists.4,5
In contrast to opioids that are full μ-opioid receptor agonists, buprenorphine is a partial agonist.5 Partial agonism results in a ceiling effect on respiratory depression and confers a more favorable safety profile.5 Buprenorphine is commonly combined with naloxone, a competitive opioid receptor antagonist with minimal oral bioavailability, added to discourage illicit parenteral use.6 Buprenorphine has higher binding affinity for the μ-opioid receptor than other opioids, giving it the potential to precipitate opioid withdrawal by displacing other opioids from this receptor.7,8
To avoid precipitated opioid withdrawal, traditional induction of buprenorphine/naloxone requires patients to be in mild-to-moderate withdrawal from other opioids before administration.9,10 The recommended period of abstinence ranges from 12 to 16 hours for short-acting opioids, such as hydromorphone or diacetylmorphine (heroin), and 48–72 hours for longer-acting opioids, such as methadone.11 This period of opioid withdrawal can be poorly tolerated by patients and may discourage induction. The traditional induction method is time-consuming, because it involves administering small doses of buprenorphine/naloxone with an assessment of withdrawal symptoms after each dose.9–12 A microdosing induction regimen for buprenorphine that does not require opioid withdrawal has been described in the literature.13 However, a limitation of this microdosing method is the length of time required to reach a therapeutic dose. We present a case of a successful transition from methadone and oxycodone to buprenorphine/naloxone using a rapid microinduction technique that did not require antecedent opioid withdrawal and did not induce precipitated opioid withdrawal. Written consent was obtained.
CASE DESCRIPTION
A 66-year-old woman was admitted to hospital in October 2018 for elective orthopedic spinal surgery for post-traumatic kyphosis. She injured her back after a fall down a flight of stairs in October 2015, aggravated by a recurrent fall in January 2016. Her falls resulted in an L2 compression fracture progressing to L2 vertebra collapse with kyphosis and spinal stenosis.
The patient reported nociceptive lower back pain with occasional radiation to the right lateral thigh with neuropathic descriptors. Her pain worsened with movement, particularly back extension. Her pain gradually worsened to a standing tolerance of <1 hour, and an inability to ambulate without a cane or walker. Between January 2016 and October 2018, she transitioned from using no opioid medications to a total of 70 mg of oxycodone daily (oxycodone 30 mg controlled release twice daily with additional oxycodone 10 mg as needed).
She experienced constipation secondary to opioids and required regular laxatives. There was a concern of opioid-induced hyperalgesia given the patient’s progressive pain despite increasing oxycodone doses before hospitalization. She had limited benefit from nonopioid analgesic medications including acetaminophen, ibuprofen, and gabapentin.
Medical history included hypertension, non–insulin-dependent diabetes mellitus, and hepatocellular carcinoma in remission. Surgical history included cataract surgery in 2012, rotator cuff repair in 2008, and hysterectomy in 2004. The patient smoked 1 pack of cigarettes daily for the past 30 years. She reported no alcohol or illicit substance use. She used oxycodone as prescribed, with no features of opioid use disorder.
Bloodwork indicated normal renal function (creatinine = 36 μmol/L, estimated glomerular filtration rate = 108 mL/min/1.73 m2), liver transaminitis (alanine aminotransferase = 74 units/L, aspartate aminotransferase = 4 units/L, alkaline phosphatase = 125 units/L, γ-glutamyl transferase = 1843 units/L), and unremarkable liver function tests (bilirubin = 8 μmol/L, albumin = 39 g/L, international normalized ratio [INR] = 1.3). Computed tomography (CT) scan of the lumbar spine showed L2 and L3 fractures of marked deformity with severe canal and right foraminal narrowing at L2–L3, and multilevel degenerative changes with moderate canal and bilateral foraminal narrowing at L4–L5.
The patient underwent 11-hour surgery on the day of admission, including a T11–L5 posterolateral fusion, L2 posterolateral vertebral column resection, L3/L4 interbody fusion, and L4/L5 interbody fusion, with no surgical complications. Intraoperatively, she received general anesthesia of sufentanil 0.15 μg/kg/h and dexmedetomidine 0.4 μg/kg/h infusions, and a total of fentanyl 250 μg, hydromorphone 4 mg, ketamine 60 mg, and lidocaine 50 mg intravenously. Postoperatively, she received a hydromorphone infusion of 0.6 mg/h for 24 hours, then 0.2 mg/h for 5 days before discontinuation, and a ketamine infusion of 10 mg/h for 24 hours, 5 mg/h for 24 hours, then 2.5 mg/h for 24 hours before discontinuation. She remained on oral oxycodone throughout the perioperative period.
She continued her home medications of amlodipine, metformin, buspirone, and acetaminophen. Additional medications in hospital included cotrimoxazole, dalteparin, ferrous fumarate, magnesium glucoheptonate, docusate sodium, sennosides, polyethylene glycol, clonidine, pregabalin, and methadone.
The patient’s back pain persisted after surgery, requiring escalating opioid doses. Her pain was functionally debilitating, interfering with ambulation, transfers, and self-care. She used 135–205 mg of oxycodone daily (30 mg extended-release 3 times daily with supplemental immediate-release doses as needed). As increasing doses of oxycodone had only partial effect, methadone was initiated at 5 mg 3 times daily on postoperative day (POD) 9. Regular dosing of extended-release oxycodone was discontinued. Oxycodone 5–10 mg every 3 hours as needed was continued. Methadone was titrated to 8 mg 3 times daily on POD 13. Methadone helped decrease the usage of as-needed oxycodone, though she continued to take 60–80 mg of oxycodone daily in addition to methadone 24 mg daily. The Complex Pain and Addiction Consult Service was consulted in the context of escalating opioid use with poorly controlled postoperative pain.
Given concerns of opioid-induced hyperalgesia and safety risks with full μ-opioid agonism, a decision was made to transition from methadone and oxycodone to buprenorphine. A rapid microdosing induction was considered the ideal option to minimize the time required to reach therapeutic buprenorphine doses. Methadone was decreased to 6 mg 3 times daily on POD 21 to reduce the risk of precipitated opioid withdrawal with buprenorphine/naloxone induction. A urine drug screen before induction was positive for opiates and methadone (as prescribed) and negative for fentanyl, benzodiazepines, cannabinoids, cocaine, and amphetamines.
A 3-day rapid microdosing titration of buprenorphine/naloxone was initiated on POD 22 as indicated in the Table. She was given sublingual buprenorphine/naloxone 0.25 mg/0.0625 mg every 3 hours for 8 doses, then 0.5 mg/0.125 mg every 3 hours for 8 doses, then 1 mg/0.25 mg every 3 hours for 8 doses. During the 3-day induction, she continued methadone 6 mg 3 times daily and oxycodone 5–10 mg every 3 hours as needed. The amount of oxycodone used during the 3-day titration remained consistent between 60 and 80 mg daily. On the fourth day, buprenorphine/naloxone was consolidated to 12 mg/3 mg once daily and methadone was discontinued. On the fifth day, buprenorphine/naloxone was increased to 16 mg/4 mg once daily and oxycodone was discontinued (Figure).
Table.
Rapid Microinduction Titration Schedule for Buprenorphine/Naloxone From Methadone Plus Oxycodone
| Buprenorphine/Naloxonea | Oxycodone | Methadone | |||||
|---|---|---|---|---|---|---|---|
| Dosing | Total Daily Dose (mg) | Dosing | Total Daily Dose (mg) | Dosing | Total Daily Dose (mg) | COWS | |
| Day 0 | N/A | … | 5–10 mg PO q3h PRN | 70 | 6 mg PO q8h | 18 | N/A |
| Day 1 | 0.25 mg SL q3h | 2 | 5–10 mg PO q3h PRN | 60 | 6 mg PO q8h | 18 | 0–4 |
| Day 2 | 0.5 mg SL q3h | 4 | 5–10 mg PO q3h PRN | 80 | 6 mg PO q8h | 18 | 1–2 |
| Day 3 | 1 mg SL q3h | 8 | 5–10 mg PO q3h PRN | 70 | 6 mg PO q8h | 18 | 1–2 |
| Day 4 | 12 mg SL daily | 12 | 5–10 mg PO q3h PRN | 60 | Discontinued | 1–5 | |
| Day 5 | 16 mg SL daily | 16 | Discontinued | … | N/A | ||
Abbreviations: COWS, clinical opiate withdrawal scale; N/A, not applicable; PO, orally; PRN, as needed; q3h, every 3 h; q8h, every 8 h; SL, sublingual.
Expressed as milligrams of buprenorphine in buprenorphine/naloxone sublingual tablet.
Figure.
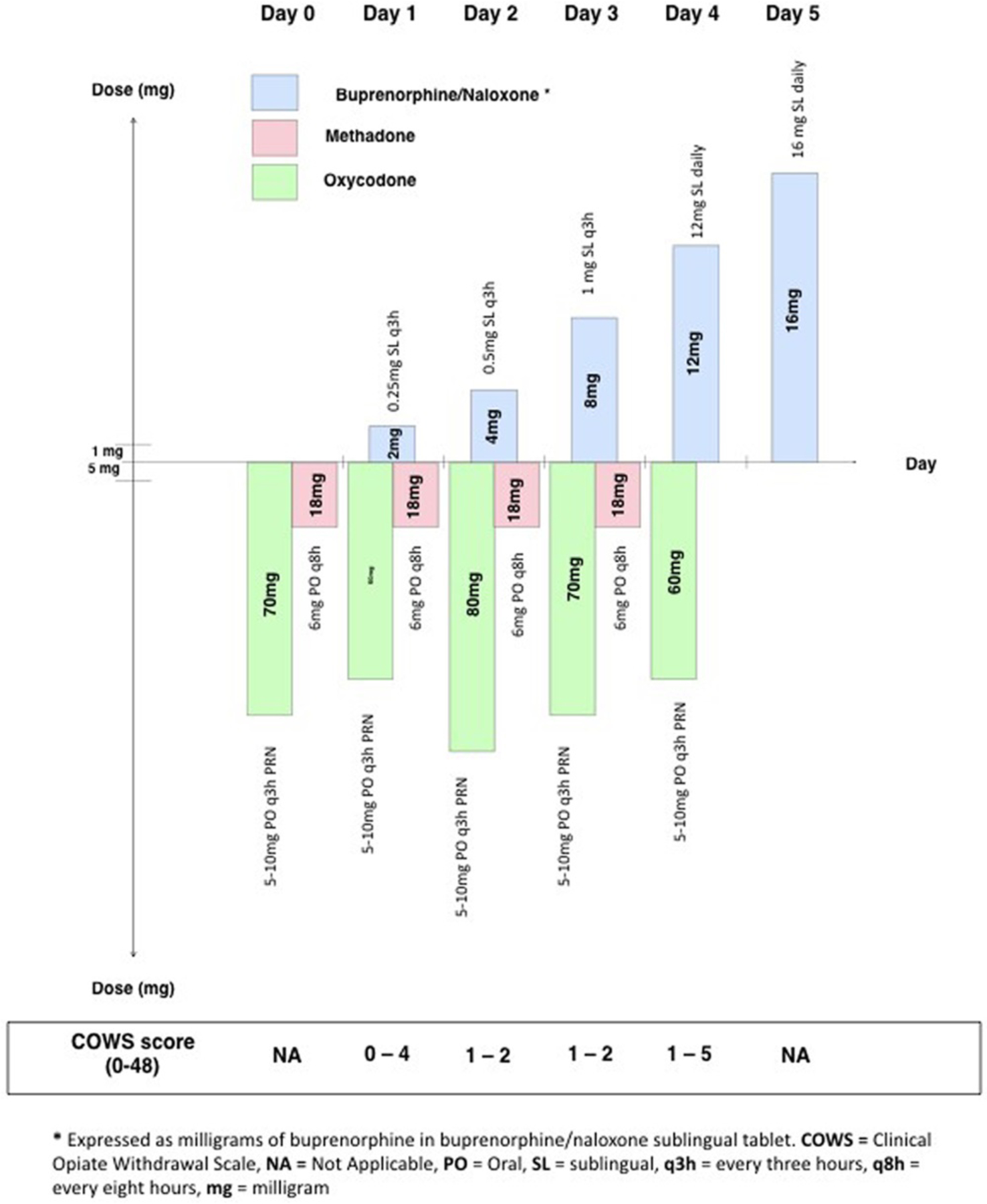
Rapid microinduction titration schedule for buprenorphine/naloxone from methadone plus oxycodone.
The clinical opiate withdrawal scale (COWS) is an 11-item scale used to rate signs and symptoms of opiate withdrawal, with scores ranging from 0 to 48.14 Before induction of buprenorphine/naloxone, the COWS score was 1. On day 1 of the induction, the COWS score ranged from 0 to 4. On days 2 and 3, the COWS score ranged from 1 to 2. On day 4, the COWS score ranged from 1 to 5. Scoring on the COWS was generated primarily by generalized aches and anxiety. The patient received interdisciplinary monitoring on a neuro-ortho spine inpatient unit, including nursing, physiotherapy, and occupational therapy. She received routine neuro-vital sign monitoring throughout the day.
The patient reported no significant withdrawal symptoms with transition from methadone and oxycodone to buprenorphine/naloxone. She reported improved pain and function, with an ability to transfer and ambulate independently with a walker. She had improved mood and was motivated for hospital discharge.
DISCUSSION
We presented a case where an inpatient with poorly controlled postoperative pain despite escalating opioid doses was transitioned to buprenorphine/naloxone from methadone and oxycodone using a rapid microdosing induction. Given the patient’s chronic opioid use, a standard induction of buprenorphine/naloxone may have resulted in precipitated opioid withdrawal or uncontrolled pain during the transition. In addition, a therapeutic dose of buprenorphine/naloxone was reached without the requirement of preceding opioid withdrawal. Superior analgesia was achieved with buprenorphine/naloxone as the sole opioid.
The strength of this case is the demonstration of a novel technique to transition patients from methadone and oxycodone to buprenorphine/naloxone in a monitored setting. One limitation was the low dosage of methadone (6 mg 3 times daily) before buprenorphine/naloxone induction. This technique warrants repetition with higher methadone doses, because withdrawal symptoms may be more pronounced in such cases.
To our knowledge, the only microdosing protocol for buprenorphine in literature is the “Bernese method” described in a case series of 2 patients with opioid use disorder. The “Bernese method” utilized buprenorphine at low doses daily or twice daily to avoid precipitated opioid withdrawal.13 The hypothesis was that successive, small doses of buprenorphine would slowly accumulate at μ-opioid receptors displacing the full agonist opioids.13 Our study postulates that doses can be administered more rapidly given buprenorphine’s time to peak plasma concentration of approximately 1 hour.6 The risk of more severe opioid withdrawal symptoms with a rapid induction technique can be mitigated by frequent patient monitoring. Rapid induction confers patient benefits and may have financial benefits by shortening the duration of subtherapeutic doses and suboptimally controlled pain. The “Bernese method” patients required 10 or more days to achieve therapeutic doses of buprenorphine, whereas our patient reached therapeutic dose within 5 days.13 A recent case series has demonstrated the feasibility of a similar rapid microdosing technique for transition to buprenorphine/naloxone from hydromorphone.15
Full μ-opioid agonists may provide better control of acute pain than partial μ-agonists in the early postoperative period. For this reason, premature introduction of buprenorphine may lead to suboptimal pain management in the immediate postoperative setting. Buprenorphine’s partial μ-opioid agonism may also lead to less effective analgesia in chronic pain management. However, when initiated at the appropriate time, the limitation of partial μ-opioid agonism is balanced by the potential reduction of opioid-induced hyperalgesia through buprenorphine’s κ-opioid antagonism.4,5 The risk of precipitated withdrawal should be considered, though has not been studied with our rapid induction method. Patients and practitioners may hesitate to use buprenorphine/naloxone due to the required period of opioid withdrawal before induction and the risk of precipitated opioid withdrawal with traditional induction.11 A rapid microdosing induction method can avoid these barriers, and increases the availability of buprenorphine/naloxone as an analgesic option.15 Buprenorphine/naloxone also carries a superior safety profile compared to other opioids, and can decrease the risk of overdose.8–11
We suggest using this rapid microdose induction method in inpatients with suspected opioid-induced hyperalgesia who may benefit from transition to buprenorphine/naloxone. The target dose is driven primarily by patients’ subjective pain and opioid withdrawal symptoms. We aim for conversion to a total dose of buprenorphine 12 mg on the third day of induction, though this dose can be increased to manage pain or opioid withdrawal, or decreased to mitigate adverse effects such as sedation. The dosing frequency may depend on the nature of the patient care setting. Microdosing induction is possible in the outpatient setting with regular assessment of COWS scores by a trained clinician. A less frequent dosing regimen may be more practical for outpatients, such as the induction used in the Bernese method.13 Future research is needed to examine efficacy and safety of microdosing induction compared to conventional dosing initiation in controlled trials, with larger sample size, and in diverse patient populations.
Funding:
M.N. is supported by Frederick Banting and Charles Best Canada Graduate Scholarships (funding reference number = 157934).
Footnotes
The authors declare no conflicts of interest.
REFERENCES
- 1.Nahin RL. Estimates of pain prevalence and severity in adults: United States, 2012. J Pain. 2015;16:769–780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67:1001–1006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dowell D, Haegerich TM, Chou R. CDC Guideline for prescribing opioids for chronic pain–United States, 2016. JAMA. 2016;315:1624–1645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Velayudhan A, Bellingham G, Morley-Forster P. Opioid-induced hyperalgesia. Contin Educ Anesth Crit Care Pain. 2014;14:125–129. [Google Scholar]
- 5.Chen KY, Chen L, Mao J. Buprenorphine-naloxone therapy in pain management. Anesthesiology. 2014;120:1262–1274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chiang CN, Hawks RL. Pharmacokinetics of the combination tablet of buprenorphine and naloxone. Drug Alcohol Depend. 2003;70:S39–S47. [DOI] [PubMed] [Google Scholar]
- 7.Volpe DA, McMahon Tobin GA, Mellon RD, et al. Uniform assessment and ranking of opioid μ receptor binding constants for selected opioid drugs. Regul Toxicol Pharmacol. 2011;59:385–390. [DOI] [PubMed] [Google Scholar]
- 8.Orman JS, Keating GM. Spotlight on buprenorphine/naloxone in the treatment of opioid dependence. CNS Drugs. 2009;23:899–902. [DOI] [PubMed] [Google Scholar]
- 9.Bruneau J, Ahamad K, Goyer MÈ, et al. ; CIHR Canadian Research Initiative in Substance Misuse. Management of opioid use disorders: a national clinical practice guideline. CMAJ. 2018;190:E247–E257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kampman K, Jarvis M. American Society of Addiction Medicine (ASAM) national practice guideline for the use of medications in the treatment of addiction involving opioid use. J Addict Med. 2015;9:358–367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.A Guideline for the Clinical Management of Opioid Use Disorder. British Columbia Centre on Substance Use. Available at: http://www.bccsu.ca/wp-content/uploads/2017/06/BC-OUD-Guidelines_June2017.pdf. Accessed November 27, 2018.
- 12.Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014. CD002207. [DOI] [PubMed] [Google Scholar]
- 13.Hämmig R, Kemter A, Strasser J, et al. Use of microdoses for induction of buprenorphine treatment with overlapping full opioid agonist use: the Bernese method. Subst Abuse Rehabil. 2016;7:99–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wesson DR, Ling W. The Clinical Opiate Withdrawal Scale (COWS). J Psychoactive Drugs. 2003;35:253–259. [DOI] [PubMed] [Google Scholar]
- 15.Klaire S, Zivanovic R, Barbic SP, et al. Rapid micro-induction of buprenorphine/naloxone for opioid use disorder in an inpatient setting: a case series [published online ahead of print March 22, 2019]. Am J Addiction. 2019;28:262–265. [DOI] [PubMed] [Google Scholar]