

13.1. Anatomy and physiology of the respiratory system
Rabbits have sensitive nostrils and a good sense of smell. There are 20-25 vibrissae in each upper lip. In healthy rabbits, the nostrils are constantly twitching at a rate of 2-120 times per minute, unless the rabbit is at rest (Brewer and Cruise, 1994) or is unwell. The nasal cavity is lined with a protective layer of mucus that entraps foreign particles and bacteria. The mucus also prevents water loss and enhances the sense of smell. The nasal glands secrete serous fluid into the nasal cavity. In the rabbit, there is glandular tissue along the nasal septum and a cluster of glands, collectively known as the lateral nasal gland, occupy the entire wall between the nasal cavity and maxillary sinus (Bojsen-Moller, 1964). The function of these nasal glands is to moisten inspired air, which has a role in thermoregulation. The position of the conchal and maxillary sinuses and the structures of the nasal cavity are illustrated in Figures 3.9 and Figure 7.1. There is no frontal sinus.
The oropharynx is narrow and the base of the tongue is large in rabbits. The glottis is small. Breathing takes place through the nostrils. Mouth breathing only occurs during severe respiratory distress.
Each lung is divided into cranial, middle and caudal lobes and there is an accessory lobe on the right lung. Respiratory movement in rabbits is mainly diaphragmatic rather than due to the action of the intercostal muscles. The thoracic cavity is small and the thymus, which remains large throughout life, occupies the anterior ventral thoracic cavity (see Figure 13.3 ).
Figure 13.3.
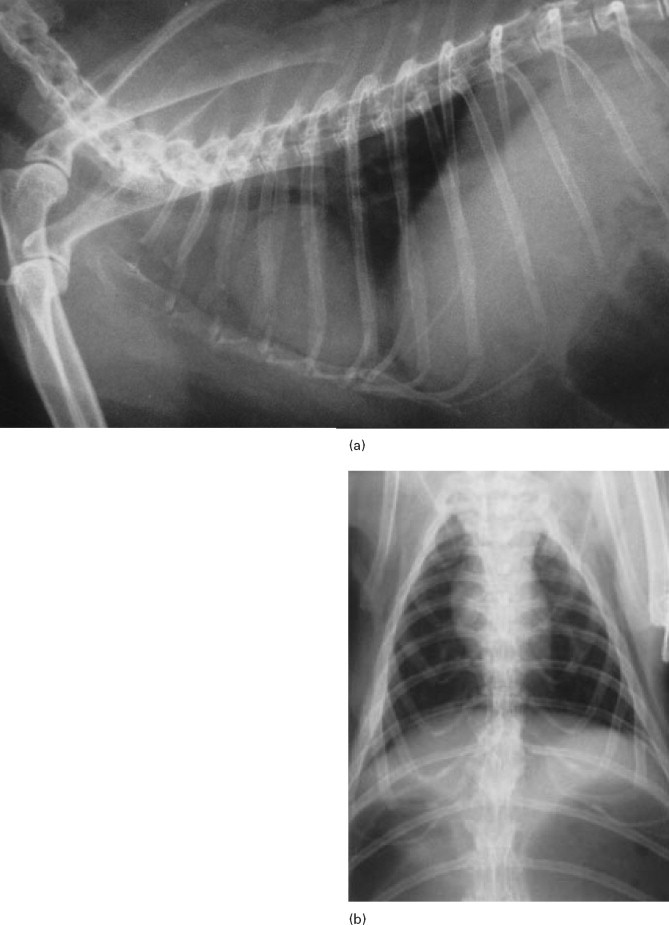
Radiographic anatomy of the thoracic cavity. Sedation or general anaesthesia is required to position a rabbit for thoracic radiography. The forelegs need to be retracted cranially to prevent superimposition of the scapulae on the cranial portion of the thoracic cavity.
-
•The thoracic cavity is small in comparison with the abdominal cavity.
-
•The heart occupies a relatively large volume of the thoracic cavity.
-
•The small cranial lung lobes are not as seen in as much detail as the caudal lobes.
-
•The thymus remains large throughout life.
-
•The aorta and caudal vena cava should be visible.
-
•In obese animals, intrathoracic fat deposits can sometimes be seen (Rübel et al., 1991).
-
•Cartilage rings are often visible within the tracheal wall.
-
•The carina lies at the 4th or 5th intercostal space.
-
•The pulmonary vessels can be seen within the lungs.
- (a) Shows a normal lateral view of the thoracic cavity, and (b) shows the dorsoventral view.
13.2. Respiratory diseases
13.2.1. Pasteurellosis
Pasteurella multocida is associated with a number of diseases of rabbits (see Section 16.5.1). Pasteurellosis is not a recognized problem in wild rabbits but is a serious disease in colonies of commercial or laboratory rabbits. In pet rabbits, although P. multocida is found as an opportunist pathogen in many secondary infections, primary pasteurellosis is uncommon. It is usually encountered in the newly acquired rabbit that has recently been bought from a breeder or pet shop. Respiratory disease is the most common manifestation. Acute infections and septicaemia occur, especially in young animals, but chronic, insidious recurrent infections are more common in the adult pet rabbit. Rhinitis, conjunctivitis, nasolacrimal duct infections, otitis media, tracheitis and bronchopneumonia can all be caused by Pasteurella multocida. The organism can spread to other sites from the nasal cavity where it can reside as a commensal organism. Infection often persists despite mucosal and humoral antibody responses in addition to effusive neutrophilic exudation. The deleterious effect of pasteurellosis on laboratory colonies of rabbits and interference with experimental procedures has resulted in the evolution of expensive ‘pasteurella-free’ rabbits for use in research. The epidemiology of pasteurellosis is discussed in Section 16.5.1. Many predisposing factors trigger disease.
13.2.2. Respiratory disease due to pasteurellosis
Pet rabbits are often already infected with P. multocida when they are purchased from a pet shop or breeder. The development of rhinitis and other respiratory tract problems in the newly acquired young rabbit is likely to be due to pasteurellosis. In the older animal, stress or poor husbandry can result in a flare up of a latent infection. Poor air quality, caused by high ammonia levels, or dusty hay irritate the respiratory tract and predisposes secondary infection. Many owners like to protect their rabbits from inclement weather by covering the hutch or placing them in a poorly ventilated damp shed during the winter months. Ventilation and good air quality is important in disease prevention. Pasteurellosis can be spread between animals and the disease is endemic in most breeding establishments. It often causes problems in premises, such as sanctuaries, where several animals are housed in close proximity. A distance of greater than 1.8 m (6 feet) or ‘sneezing distance’ is needed to control the spread of infection between individuals (Whittaker, 1989).
13.2.3. Rhinitis (‘snuffles’)
Repetitive sneezing and upper respiratory tract noise is a feature of rhinitis. Rhinitis and sinusitis can be manifestations of pasteurellosis, although other organisms such as staphylococci or Bordetella can also be involved. The differential diagnosis of upper respiratory tract disease in rabbits includes nasal foreign bodies and periapical abscesses of the maxillary incisors or premolars. Both these conditions are common in the pet rabbit so it cannot be assumed that all rabbits with a purulent nasal discharge are suffering from pasteurellosis or that all cases of ‘snuffles’ are due to infectious agents.
In the initial stages of pasteurellosis, the nasal discharge is serous and the condition is responsive to antibiotic therapy. In advanced cases, the nasal discharge is thick, yellow and viscid. Copious amounts of mucopurulent material can be discharged from the nostrils and form crusts on the surrounding skin. Affected rabbits wipe the purulent discharges from their nose with their forepaws, which become matted and discoloured. Coughing is not as common as sneezing and snortling. Respiratory noises may be audible to the owner who may think their rabbit is ‘wheezing’. Anorexia can occur, perhaps due to a reduced sense of smell or because it is difficult to chew and breathe at the same time. Grooming difficulties occur because the rabbit finds it difficult to breathe and groom simultaneously. Response to antibiotic therapy is poor in advanced cases and relapse is common. Post-mortem examination of the sinuses and nasal passages of rabbits with chronic rhinitis shows why these cases are so difficult to treat. The nasal cavity is filled with pus, which can spread into the paranasal sinuses (see Figure 7.1 and Figure 13.1 ). The pus becomes thick and inspissated. There is ulceration of the mucous membranes and osteomyelitis of the turbinates causing severe atrophy and erosion (Deeb, 1997). The presence of pus in the nasal cavity impedes gas exchange and causes physical discomfort and irritation.
Figure 13.1.

(a) Sagittal section through the head to show the position of the paranasal sinuses. This figure was drawn from a post mortem specimen of a sagittal section through a decalcified head. The nasal conchae have been removed. There are two paranasal sinuses in rabbits: the conchal sinus and the maxillary sinus. There is no frontal sinus. Both the conchal and the maxillary sinus form blind cavities. At the cranial end of each sinus there is a single opening into the nasal passage. The structures of the nasal cavity are illustrated in Figure 3.9. The position of the paranasal sinuses is also illustrated in Figure 7.1. (b) Chronic infection of the conchal sinus. This figure is a lateral view of the nasal cavity of an 18-month-old Dwarf Lop female rabbit with chronic rhinitis. The rabbit had started sneezing and developed a nasal discharge shortly after she was purchased at 10 weeks of age. Antibiotic therapy and mucolytic therapy failed to cure the condition although the symptoms were temporarily alleviated. Radiology shows increased radiopacity of the conchal sinus indicating the presence of infection. There is erosion of the turbinates. The conchae and ethmoturbinates are not visible on the radiograph. Rhinitis was due to infection and not related to dental disease.
13.2.3.1. Differential diagnosis of rhinitis
The clinical history can be very suggestive of pasteurellosis. Young rabbits that have recently been stressed by weaning, change in routine and transport are often exposed to infection at the breeding establishment where they originated. Rabbits housed with several others in sheds and outhouses are susceptible. In older, individual pet rabbits, bacterial infection is less likely to be a cause of rhinitis than dental disease, which is common. Nasal foreign bodies can cause rhinitis (see Section 13.3). Myxomatosis is another possible cause of rhinitis. Myxomatosis in rabbit colonies can present as rhinitis in association with ocular discharge. Aerosol infection is more likely to give respiratory tract signs that insect spread (see Section 16.6.1). Myxomatosis is progressive and almost invariably fatal.
Bacteriology can be used to identify bacteria that are present in the nasal passages of rabbits with rhinitis and to ascertain antibiotic sensitivity. The rabbit's nose is sensitive and it can be difficult to insert the swab deep into the nasal passages in the conscious animal. Sedation or anaesthesia is usually required to take a deep nasal swab for culture.
Underlying dental problems can be diagnosed by visual examination and by radiography (see Section 7.6 and Figure 13.1a). The structures of the nose and teeth can be assessed on skull radiographs. The paranasal sinuses can be identified (see Figure 7.5 and Figure 13.1) and abnormalities may be detected radiologically. Opacity of the conchal sinus indicates the presence of exudate (see Figure 13.1b). Erosion of the ethmoturbinates can be seen on a well-exposed radiograph. However, the presence of P. multocida or other bacterial infection and erosion of the turbinates does not rule out the possibility of an underlying foreign body or perapical abscess. Large abscesses or rhinoliths can form in the nasal passages because of tooth root infection (see Plate 17).
13.2.4. Otitis media
Pasteurella multocida primarily resides in the nasal cavity but can spread via the eustachian tube to the tympanic bulla and affect the middle ear (see Plate 27). Infection can spread further to affect the inner ear and vestibular apparatus or track through the acoustic meatus and along the vestibulocochlear nerve. On post-mortem examination abscesses can be found in the cranial cavity.
It is not easy to diagnose otitis media in the live rabbit. The presence of exudate in the external ear canal does not signify the presence of otitis media. In many pet rabbits, especially lop eared breeds, it is difficult to visualize the tympanic membrane due to the presence of waxy ear secretion. Post-mortem examination of the horizontal ear canal of pet rabbits often reveals the presence of inspissated pus that occludes the horizontal canal. The presence of purulent material in the external ear canal does not necessarily signify the presence of pus in the tympanic bulla. Neither does pus in the tympanic bulla always cause otitis interna and vestibular symptoms (see Section 12.4.3). Radiological changes can often be seen as an incidental finding on skull radiographs (see Figure 13.2 ). It seems likely that rabbits with pus in the external ear canal and/or the tympanic bulla will have impaired hearing although they may appear clinically normal. Some observant owners can detect hearing deficits in their pets and aggression in rabbits has been attributed to deafness when rabbits have been startled by the unheard approach of their owners.
Figure 13.2.
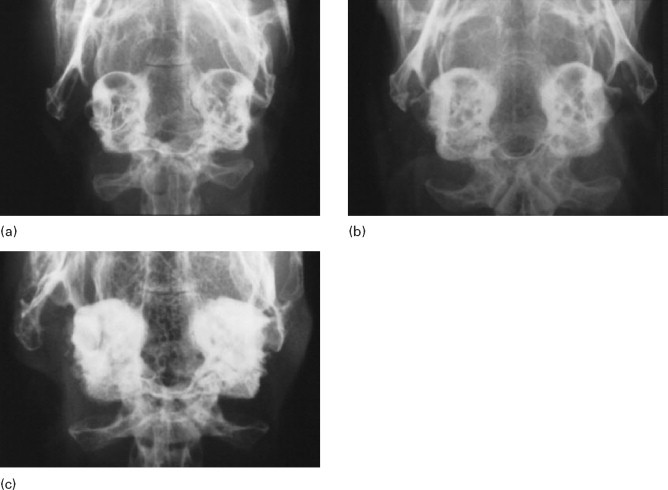
Radiographic changes of the tympanic bulla. (a)–(c) are dorso ventral views of the caudal area of the skull to show progressive changes of the tympanic bullae from normal (a) to severe (c); (b) was an incidental finding on a rabbit that was radiographed to investigate his dental disease.; and (c) was of a 3-year-old French Lop male that was rescued by the RSPCA from a small shed containing between 20-30 rabbits. Upper respiratory problems were endemic. The rabbit appeared totally deaf and was ataxic. He was quiet and subdued. He was euthanased due to dental problems. Post-mortem examination showed pus in both tympanic bullae.
In a study by Flatt et al. (1977), otitis media was found in 4% of 2001 young rabbits and 32% of adults slaughtered for human consumption. The animals were clinically healthy on ante-mortem inspection. Gross lesions included the presence of white tenacious exudate filling the tympanic bulla. The mucous membrane lining the bulla was thickened, translucent and discoloured. The eustachian tube was dilated and filled with pus. Microscopic lesions consisted of an accumulation of heterophils in the lumen of the tympanic bulla and in the mucosa and underlying periosteum. In some of the affected ears, the simple squamous epithelium over the tympanic membrane and auditory ossicles had undergone squamous metaplasia with necrosis of the mucosa in severe cases. In the rabbits with periosteal changes, the thickened periosteum was infiltrated by a variable number of heterophils, plasma cells and lymphocytes. Occasionally granulation tissue was present. In some cases, the tympanic membrane was ruptured and a suppurative exudate was present in the tympanic cavity and the external auditory canal.
13.2.5. Pneumonia
Septicaemia and acute suppurative pneumonia can be caused by Pasteurella multocida. Infection can be peracute and cause rapid death (see Plate 28). Chronic pneumonia and abscesses in the thoracic cavity also occur. Poor exercise tolerance and increased respiratory rate may not be obvious to owners of pet rabbits that are confined to hutches or small runs with no opportunity to exercise. These individuals pose a poor anaesthetic risk due to poor gas exchange in consolidated lungs.
13.2.6. Treatment of pasteurellosis
Pasteurellosis is a difficult condition to cure. Acute upper or lower respiratory infections can be responsive to prompt antibiotic and non-steroidal anti-inflammatory medication. An antibiotic that is unlikely to cause diarrhoea but is effective against Pasteurella multocida should be selected. Examples include enrofloxacin, trimethoprim sulpha combinations, tetracyclines, parenteral cephalexin or penicillin. In vitro, most rabbit isolates of P. multocida are susceptible to penicillin, chloramphenicol, tetracycline, erythromycin, novobiocin and nitrofurans with a variable susceptibility to streptomycin, kanamycin, neomycin and sulphonamides. P. multocida is usually resistant to clindamycin and lincomycin (Manning et al., 1989). Penicillin has been used widely to treat rhinitis in laboratory rabbits (Gaertner, 1991). Concurrent infection with other pathogens such as Bordetella bronchiseptica can affect the response to therapy. Tilmicosin is an effective antibiotic in the treatment of acute pasteurellosis in sheep and has been used to treat rabbits despite the possibility of a fatal adverse reaction to the drug (see Section 4.2.1.11).
Long-term or periodic courses of antibiotic can be given to control long-standing infections although they are unlikely to be curative. Antibiotics can also be introduced directly into the nose. Some rabbits will tolerate this procedure. Gentamicin is available as an ophthalmic preparation (Tiacil, Virbac) that can be used as nose drops. Purulent exudate needs to be removed before the drops are instlled.
Chronic pasteurellosis is manifested by the presence of copious quantities of thick, viscid, mucopurulent material that presents a physical barrier to medication. The pus is often in inaccessible sites such as the nasal passages, paranasal sinuses, tympanic bullae or even the brain. Surgery, such as trephination, to remove the pus, provide drainage and create a route for local medication, is theoretically possible. Bulla osteotomy has been suggested as a treatment for rabbits with severe, refractory, chronic otitis media in association with vestibular signs such as head tilt and anorexia (Redrobe, 2000). The surgical technique has been described (Swindle and Shealy, 1996; Redrobe, 2000), but there are no follow-up reports of the success of the procedure. Anecdotally, the results of bulla osteotomy are disappointing. Anorexic rabbits are not good surgical subjects. Trephination of sinuses has not been described in rabbits but rarely provides freedom from clinical signs of chronic sinusitis in cats.
The chances of successful treatment of pasteurellosis are greater in sites where the pus can be removed, e.g. by flushing an infected nasolacrimal duct or removing an abscess or infected organ such as a uterus or testicle. Dacryocystitis, facial abscesses or purulent nasal discharges are often associated with underlying dental disease that needs to be addressed if there is to be any hope of success in treating the secondary pasteurella infection (see Section 7.5.5 and 8.1).
In cases of rhinitis, it is important to establish adequate systemic hydration by ensuring adequate fluid intake. Dry airways result in increased viscosity of secretions, decreased ciliary function, inflammation, and degeneration of the mucosa. The inclusion of fresh leafy vegetables in the diet can increase a rabbit's fluid intake. Water can be added to inspired gases by the use of humidifiers or placing the rabbit in a steamed-up room such as a bathroom. Nebulization is sometimes used as a method of introducing antibiotic, decongestants and other agents directly into the respiratory tract and to loosen secretions and bring relief. Nebulization introduces charged particles into the respiratory tract as an aerosol. In other species, nebulization is used to treat lower respiratory tract disease. Medication introduced by nebulization is unlikely to reach the tympanic bullae or paranasal sinuses or to penetrate thick mucopurulent exudate in rabbits. Mucolytic agents such as bromexine or N-acetyl-cysteine have been recommended for nebulization in rabbits with rhinitis (Meredith, 2000). In other species, N-acetyl-cysteine is irritating to mucosal surfaces and can inactivate certain antibiotics when it is mixed with them (McKiernan, 1983). Systemic bromhexine (Bisolvon, Boehringer Ingelheim) can be used as a mucolytic in rabbits. In cattle and pigs, when bromhexine is administered simultaneously with oxytetracycline, the antibiotic in the bronchial mucus is considerably increased (product datasheet).
Occasionally, zealous owners administer human decongestants to their rabbits. There is no proven efficacy in the use of such products in the treatment of ‘snuffles’.Oxymetazoline is a common topical nasal decongestant that has been investigated in experimentally induced infections of the maxillary sinus in rabbits (Bende et al., 1996). Paradoxically, a higher degree of inflammation was found in the oxymetazoline treated sinuses. The authors concluded that oxymetazoline nose drops interfere with the normal defence mechanisms possibly by a decrease in mucosal blood flow.
Key points 13.1.
-
•
Healthy rabbits can twitch their nose at a rate of 2-120 times per minute
-
•
The nasal gland of the rabbit is well developed and humidifies inspired air, which is part of temperature regulation
-
•
Mouth breathing only occurs during severe respiratory distress
-
•
P. multocida is a significant cause of acute and chronic respiratory disease in rabbits
-
•
Rhinitis (‘snuffles’) can be caused by dental disease or nasal foreign bodies as well as pasteurellosis. Other bacterial and fungal agents can also be involved
-
•
In the initial stages, when the nasal discharge is serous, antibiotics can be effective in the treatment of pasteurellosis. As the disease progresses, the discharge becomes a thick, viscid, mucopurulent exudate that is refractory to treatment
-
•
Osteomyelitis and erosion of the nasal turbinates occurs in long-standing infections. Pus can be present in the sinuses or tympanic bullae. Abscesses may develop in the brain
-
•
Treatment of advanced cases of rhinitis is unlikely to be successful. Antibiotics may be effective in controlling the disease. Long-term or intermittent periodic antibiotic therapy may be indicated
-
•
Antibiotics can be introduced into the nose using nose drops
-
•
Hydration of the nasal mucosa is important. The inclusion of fresh vegetables in the diet will increase water intake. Steam therapy by placing the rabbit in a steam filled room may be helpful
-
•
Nebulization can be used to introduce antibiotics and/or mucolytics into the respiratory tract and to loosen secretions. Nebulization is more likely to be effective in the treatment of lower respiratory tract disease than in cases of rhinitis, sinusitis or otitis media where mucopurulent exudates form an effective barrier
-
•
The mucolytic agent, bromhexine (Bisolvon, Boehringer Ingelheim) can be given orally or by nebulization
-
•
Human decongestants are unlikely to be effective.
13.3. Nasal foreign bodies
Pieces of hay, grass seeds or shafts of hair can enter and become lodged in the nasal cavity. Repetitive sneezing, nose rubbing and a unilateral discharge are indicative of a nasal foreign body. If the foreign material has penetrated deep into the nasopharynx, snortling and dyspnoea can occur which can be mistaken for pneumonia. The patency of the nasal passages can be assessed by occluding each nostril in turn and listening to the respiratory noises. Sometimes the end of a blade of hay or hair shaft can be seen protruding from the nostril (see Plate 29). The foreign body can be gently pulled out. In other cases, endoscopy is required. Dislodging or removing a nasal foreign body often results in a complete recovery.
13.3.1. Endoscopic examination of the nasal passages
The nasal passages can be examined endoscopically. They require flushing to clear away discharges and exudate prior to endoscopic examination. Foreign material can also be flushed out during the procedure. Nasal flushing in rabbits poses problems due to the small nasopharynx and inaccessible larynx. Great care is required to prevent purulent material entering the larynx and trachea. Endotracheal intubation is mandatory and the rabbit should be positioned so fluid drains out of the mouth. The nasal passages are examined using a rigid endoscope such as a 1.9 mm needlescope (Stortz) and irrigation sheath. The endoscope can go from the nostril to the nasopharynx via the ventral meatus and can also be used to explore the turbinate area.
13.4. Dyspnoea
The differential diagnoses for dyspnoea is given in Table 3.2 and includes acute pasteurellosis, viral haemorrhagic disease, heat stroke, cardiac disease and pleural effusions due to cardiac disease. Metastatic tumours can also cause dyspnoea. Uterine adenocarcinomas can metastasize to the lungs where they are seen as multiple spherical opacities (Rübel et al., 1991). Some rabbits with upper respiratory tract disease are dyspnoeic because they cannot breathe through their nose. As in other species, external trauma can cause chest injuries and respiratory problems. Bite wounds from predators can penetrate the chest wall causing serious internal injury and introducing infection. A small external wound can easily be overlooked. Abscesses can develop within the thoracic cavity as result of haematogenous spread from other sites. Auscultation and radiology are useful adjuncts to clinical examination. Radiographic features of the normal chest are illustrated in Figure 13.3. Chronic pneumonia is illustrated in Figure 13.4 .
Figure 13.4.

Pneumonia Figures 13.4a and 13.4b show a lateral and dorsoventral view of a four-year-old Himalayan neutered male rabbit that was thin, anorexic and dyspnoeic. An alveolar pattern can be seen on both views. At post mortem examination, pneumonic changes were found throughout the lung tissue.
13.5. Heat stroke
Rabbits are tolerant of low temperatures and can withstand sub-zero environmental temperatures without discomfort providing they are acclimatized and healthy, and have shelter with plenty of bedding. Their dense fur insulates them from the effects of cold weather but can be a liability in hot weather.
Rabbits do not sweat and cannot pant effectively. The ears play an important part in thermoregulation. Signs of heat stroke are similar to other species: anorexia, increased respiratory rate, prostration, pulmonary oedema, cyanosis and death. Some cases can have blood-tinged fluid from the nose and mouth. A high rectal temperature (in excess of 40°C) is suggestive of heat stroke. Treatment is aimed at reducing body temperature, e.g. bathing in cold water, wetting the ears and blowing them with a cold hair drier. The administration of a vasodilator such as acetylpromazine may be helpful.
13.6. Cardiovascular disease
Most recorded information about cardiac diseases relates to infectious, toxin-induced or diet-related diseases of laboratory rabbits. Heart disease also occurs in pet rabbits and hopefully, more information will become available as rabbits live longer and more diagnostic and therapeutic procedures are adopted for the individual animal. Congenital abnormalities such as ventricular septal defects do occur. Diagnosis and treatment follow the same lines as for dogs and cats with most cases being positively diagnosed by echocardiography. Electrocardiography is also feasible in rabbits. Some reference values for normal parameters determined in laboratory rabbits are give in Box 13.1
Box 13.1. Circulatory data.
| Electrocardiography (from Kozma et al., 1974) | |
| P wave: | 0.1–0.15mv and 0.03–0.04s |
| Low or negative in lead I | |
| Always positive in leads II–III | |
| P–R: | 0.05–0.1s |
| QRS: | 0.015–0.04s |
| Arterial blood pressure | |
| Systolic: | 90–130mmHg |
| Diastolic: | 80–90mmHg |
| Arterial blood pH | |
| 7.2–7.5 | |
13.6.1. Cardiomyopathy
Cardiomyopathy occurs in pet rabbits. Giant breeds appear most susceptible (see Plate 30) but the aetiology is unknown at the present time. Histopathological findings indicate the presence of myocardial fibrosis.
The rabbit myocardium can be affected by several diseases. Vitamin E deficiency, coronavirus infection and some bacterial infections such as salmonellosis and pasteurellosis have been recorded as causes of cardiomyopathy in laboratory rabbits (Marini et al., 1999). Tyzzer's disease not only causes intestinal and hepatic lesions but can also cause a myocarditis resulting in myocardial fibrosis in those animals that survive (Percy and Barthold, 1993). Encephalitozoon cuniculi has been reported as a cause of myocarditis in rabbits (Pakes and Gerrity, 1994). Stress and catecholamines are proven causes of cardiomyopathy and experimental models of the human disease can be provided by keeping rabbits in overcrowded conditions (Weber and Van der Walt, 1975). Myocardial necrosis and fibrosis have been recorded in rabbits anaesthetized with ketamine/xylazine combinations by continuous infusion. Marini et al. (1999) postulate that hypoxaemia and coronary vasoconstriction result in cell death and necrosis. The rabbit has limited collateral coronary circulation and is therefore predisposed to ischaemia induced by coronary vasoconstriction. The authors draw an analogy with rabbits used as models of catecholamine-induced cardiomyopathy in which alpha-adrenergic mediated coronary vasoconstriction occurs. Hypotension and hypoxaemia are further contributory factors.
Key points 13.2.
-
•
Dyspnoea can be caused by upper respiratory disease, pasteurellosis, viral haemorrhagic disease, heat stroke, cardiac disease, trauma or pleural effusion. Pleural effusion can be secondary to primary or secondary neoplasia
-
•
Heat stroke occurs readily in rabbits as they do not sweat or pant effectively. A rectal temperature in excess of 40°C is indicative of heat stroke
-
•
Cardiac disease occurs in pet rabbits.
-
•
Cardiomyopathy of unknown aetiology is associated with giant breeds
-
•
Congenital abnormalities such as septal defects occur
-
•
In laboratory rabbits, vitamin E deficiency, coronavirus, E. cuniculi and bacterial infections such as Tyzzer's disease have been shown to cause myocardial changes.
13.6.2. Arteriosclerosis
Arteriosclerosis is a thickening and hardening of the arteriolar walls resulting from proliferative or degenerative changes. Aortic arteriosclerosis occurs in rabbits and can cause seizures or vague symptoms such as inactivity and weight loss. Mineralization of the aorta occurs in hypercalcaemic rabbits, usually in association with renal disease that impairs calcium excretion. Mineralization of the aorta is seen radiologically (Shell and Saunders, 1989) and on post-mortem examination. Calcification of the aorta is often associated with calcification of the kidney (see Section 14.4.2). Calcification of soft tissues can be caused by excessive intestinal absorption of calcium, such as in cases of vitamin D toxicity.
13.6.3. Coronavirus
Coronaviris infection in rabbits can result in cardiomyopathy and pleural effusion. Experimentally, coronavirus infected rabbits are used as laboratory models to study virus-induced cardiomyopathy. The disease was first discovered in Sweden in the 1960s in rabbits inoculated with emulsified testicular tissue containing Treponema pallidum (human syphilis). Coronavirus was found in the testicular tissue. An analogy has been made between rabbit coronavirus and feline infectious peritonitis. Clinical signs vary, but infected rabbits are generally pyrexic and many die within 5 days of infection. Pulmonary oedema, pleural effusion and dilation of the right ventricle are found at post-mortem. As in feline infectious peritonitis, hypergammaglobulinaemia is a feature of chronic infection that can be manifested by myocardial degeneration, ascites and uveitis. An enteric form has also been described. At the present time, coronavirus induced pleural effusion and cardiomyopathy have only been reported in experimentally inoculated rabbits (DiGiacomo and Mare, 1994). It has not been described in pet rabbits.
References
- Bende M., Fukami M., Arfors K.E. Effect of oxymetazoline nose drops on acute sinusitis in the rabbit (Abstract) Ann Otol Rhinol Laryngol. 1996;105:222–225. doi: 10.1177/000348949610500309. [DOI] [PubMed] [Google Scholar]
- Bojsen-Moller F. Topography of the nasal glands in rats and some other mammals. Anat Rec. 1964;150:11–24. doi: 10.1002/ar.1091500103. [DOI] [PubMed] [Google Scholar]
- Brewer N.R., Cruise L.J. Physiology. In: Manning P.J., Ringler D.H., Newcomer C.E., editors. The Biology of the Laboratory Rabbit. 2nd edn. Academic Press; 1994. pp. 63–70. [Google Scholar]
- Deeb B.J. Respiratory disease and the pasteurella complex. In: Hillyer E.V., Quesenberry K.E., editors. Ferrets, Rabbits and Rodents, Clinical Medicine and Surgery. W.B.Saunders; 1997. pp. 189–201. [Google Scholar]
- DiGiacomo R.F., Mare J. Viral diseases. In: Manning P.J., Ringler D.H., Newcomer C.E., editors. The Biology of the Laboratory Rabbit. 2nd edn. Academic Press; 1994. pp. 171–197. [Google Scholar]
- Flatt R.E., Deyoung D.W., Hogle R.M. Suppurative otitis media in the rabbit: prevalence pathology and microbiology. Lab Anim Sci. 1977;27:343–347. [PubMed] [Google Scholar]
- Gaertner D.J. Comparison of penicillin and gentamycin for treatment of pasteurellosis in rabbits. Lab Anim Sci. 1991;41:78–79. [PubMed] [Google Scholar]
- Kozma C., Macklin W., Cummins L.M., Mauer R. The anatomy physiology and the biochemistry of the rabbit. In: Weisbroth S.H., Flatt R.E., Kraus A.L., editors. The Biology of the Laboratory Rabbit. Academic Press; 1974. pp. 50–69. [Google Scholar]
- Manning P.J., Digiacomo R.F., Delong D. Pasteurellosis in laboratory animals. In: Adlam C., Rutter J.M., editors. Pasteurella and Pasteurellosis. Academic Press; 1989. pp. 264–289. [Google Scholar]
- Marini R.P., Xiantung L., Harpster N.K., Dangler C. Cardiovascular pathology possibly associated with ketamine/xylazine anesthesia in Dutch Belted rabbits. Lab Anim Sci. 1999;49:153–160. [PubMed] [Google Scholar]
- McKiernan B.C. Lower respiratory tract disease. In: Ettinger S.J., editor. Textbook of Veterinary Internal Medicine, Diseases of the Dog and Cat. 2nd edn. W.B.Saunders; 1983. pp. 760–828. [Google Scholar]
- Meredith A. Respiratory system and disorders. In: Flecknell P.A., editor. Manual of Rabbit Medicine and Surgery. British Small Animal Veterinary Association; 2000. pp. 33–38. [Google Scholar]
- Pakes S.P., Gerrity L.W. Protozoal diseases. In: Manning P.J., Ringler D.H., Newcomer C.E., editors. The Biology of the Laboratory Rabbit. 2nd edn. Academic Press; 1994. pp. 205–224. [Google Scholar]
- Percy D.H., Barthold S.W. Pathology of Laboratory Rodents and Rabbits. Iowa State University Press; 1993. Rabbit; pp. 179–223. [Google Scholar]
- Redrobe S. Surgical procedures and dental disorders. In: Flecknell P.A., editor. Manual of Rabbit Medicine and Surgery. British Small Animal Veterinary Association; 2000. pp. 117–134. [Google Scholar]
- Rübel G.A., Isenbügel E., Wolvekamp P. Diagnostic Radiology of Exotic Pets. Wolfe Publishing Ltd.; 1991. Rabbit. [Google Scholar]
- Shell L.G., Saunders G. Arteriosclerosis in a rabbit. J Am Vet Med Assoc. 1989;194:679–680. [PubMed] [Google Scholar]
- Swindle M.M., Shealy P.M. Common surgical procedures in rodents and rabbits. In: Laber-Laird K., Swindle M.M., Flecknell P., editors. Handbook of Rodent and Rabbit Medicine. Pergamon Press; 1996. pp. 239–255. [Google Scholar]
- Weber H.W., Van der Walt J.J. Cardiomyopathy in crowded rabbits (Abstract) Recent Adv Stud Cardiac Struct Metab. 1975;6:471–477. [PubMed] [Google Scholar]
- Whittaker D. Pasteurellosis in the laboratory rabbit: a review. Vet Ann. 1989;29:285–291. [Google Scholar]