

Abstract
Infectious diseases occur based on the interrelationship of the capabilities of the host and the virulence of the microorganism. Each person has a terrain that determines the susceptibility to infection and response to an infection. According to the theory of endobiogeny, the majority of symptoms related to an infectious disease are related to the patient’s response to the infector and not the intrinsic agent itself. This chapter discusses common infectious maladies: rhinopharyngitis, sinusitis, otitis media, tonsillitis, and bronchitis. For each of these disorders, the neuroendocrine and emunctory elements in the precritical and critical terrain are discussed. Treatment options are discussed based on treating the patient rather than the microorganism.
Keywords: Bronchitis; Endobiogeny; History of medicine, 19th century; Infectious disease; Otitis media; Neuroendocrine system; Rhinopharyngitis; Sinusitis; Tonsillitis; Virchow, Pasteur and Koch
Introduction
We define infection as a pathogenic interaction of one living system within the terrain of another living system. The term “infection” is derived from the Latin inficere meaning to taint. What is tainted is the coherence of the metaself (self + symbiotes—cf. Chapter 5) and the metastable functioning of this terrain. From this unitary definition, we derive the actors in the dyad: the nonself organism (the infector) and the terrain of the aggressed organism(s) (the infected). Infections are the dynamic of the virulence of the infector relative to the adaptive capabilities of the infected. The greater the virulence is, and the less competent adaptive capabilities are, the greater the risk of infection. Since the time of Koch and Pasteur, the exclusive line of evaluation and treatment has been the infector, with no consideration for the terrain of the infected. This is like while having a hole in one’s roof and clogged gutters on a rainy day, focusing on dispersing rain clouds rather than fixing the house.
We must make a distinction between infection and infectious disease. Infection is the presence of an organism within another organism(s) due to insufficient defense capabilities. Virchow (d. 1902), physician-pathologist and the founder of cellular pathology, recognized that organisms exist in tissues without causing disease.1 Infectious disease, then, is the syndrome that results from both the specific virulence of the infector and the adaptive and adaptative responses of the infected organism(s).
The endobiogenic approach to infectious disorders is rich, combining teleological, anatomical, and functional considerations of each area of the organism. It involves ascertaining the answer to seven queries: (1) why this structure is infected: teleology of structure and function, (2) why this patient is infected: precritical terrain, (3) why this organism infected: the organism and its virulence—absolute and relative to the competency of host defenses, (4) why these symptoms are manifested: critical terrain during an infection, (5) what is the benefit of the infectious symptoms: its adaptive or adaptative role, (6) what is the current net state of the terrain: mechanisms and consequences of endogenous response of the infected, and response of the infector, and (7) how to manage: personalization of treatment based on the reality of both the infected and the infector.
We discourage a view of seeing potential pathogens as enemies to be eliminated, or the external environment as one needing to become sterile. The world is full of Life. Each living being has its own path of existence and environment for survival. We cannot alter this fact of nature. To make it sterile is to sterilize Life. What can be done is to strengthen the buffering capacity and adaptability of the patient for the fullest expression of their Life and vitality. This allows for the greatest degrees of freedom with respect to where they go, how they live, what they do, and what they eat, without fear of invasion, infection, and disease.
Ear, nose, and sinus disorders
Rhinopharyngitis
Rhinopharyngitis is an infectious disorder of the nasal (rhino-) and pharyngeal (pharynx-) mucosa. A congestive terrain with insufficient peripheral cortico-thyrotropic adaptation of immunity favors infections in this region of the body.
Anatomy review
The nasal cavity consists of folds of mucosal tissue situated inferior to the sinus cavities and superior to the oral cavity (Fig. 9.1 ). It has a contiguous relationship with the pharynx. It is surrounded by cartilage in the most anterior position and bone in the inferior and superior regions. The posterior-inferior portion has a wall of soft tissue.
Fig. 9.1.

The nasopharynx and contiguous structures. See text for details.
(Reproduced from Blausen.com staff (2014). Medical gallery of Blausen Medical 2014. WikiJ Med 2014;1(2). doi:10.15347/wjm/2014.010. [CC BY 3.0] from Wikimedia Commons.)
Functional review
The nasal cavity is the origin of the airways. Respiration is an unceasing and essential function. The integrity, patency, and safety of the nasal cavities are essential to this activity. The nose extends more anterior from the surface of its origin than any other part of the body. It is literally the vanguard of chemical surveillance of the quality of air and risk of exposure to nonself actors with each inhalation: microorganisms, particulate, and gaseous chemical entities. Due to the constant aggression on the nasal airway, it has a high turnover rate and is subjected to permanent, intermittent relative adaptive congestion, one nostril alternating with the other.2
The nasal airway has three primary functions: respiration, defense, and olfaction. Respiration is divided into inspiration and expiration. The functions of the mucosa during inspiration are three: (1) determination of air quality, (2) humidification, and (3) filtration of air. The purposes of exhalation are two: (1) egress of carbon dioxide (acid-base balance) and (2) intonation of speech. The requirements of defense arise from the first function of respiration.3 The purpose of olfaction is to determine information crucial to the survival of the organisms: location and integrity of foods,4 the presence of organism of the same or different species, and reproduction.5, 6
ANS
Parasympathetic activity is implicated in the passive nutritive congestion of the sinuses.7 This allows for this tissue to maintain its high rate of turnover. Because it is inefficient to congest both sinuses at the same time, the organism alternates the relative tonus of para and alpha. For example, the right nostril will be congested (para > alpha) for repair and growth, while the left is open (para = alpha). The alternation of ANS function is crucial to maintain a physiologic congestion.
Cause: Precritical terrain
The induction of rhinopharyngitis occurs when there is a confluence of adaptative congestion and insufficient immunity and the presence of a virulent organism. The pharynx is implicated because of its contiguous anatomical and functional relationships with the nasal airway.
The precritical ANS state is spasmophilia with elevated histamine. The elevated histamine can be local to the mucosa as a defense mechanism, associated with alpha-sympathetic as an autacoid, or both.8 The emunctory terrain is oversolicitation of the exocrine pancreas, and, congestion of the gallbladder and intestines. The primum movens of the precritical terrain is a local spasmophilia with para > alpha and beta that is delayed or insufficiency relative to the alpha tone. Related to the nutritive congestive activity of para (and histamines), one finds a hyperinsulinism, which favors congestion, hyperemia, and infections. The excess presence of glucose favors both the growth of tissue and pathogens. Thus, the endocrine pancreas is implicated in rhinopharyngitis.
Oversolicitation of the exocrine pancreas favors mucous production (cf. The Theory of Endobiogeny, Volume 3, Chapter 2).9 Biliary and intestinal congestion favor autointoxication and diminished extracellular communication networks. In our experience, a diet that strains the gallbladder (high fat, fried foods, etc.) or the pancreas (high fat, high glycemic, hard to digest animal proteins) can contribute to nasal congestion. Table 9.1 summarizes the rhinopharyngitis terrain.
Table 9.1.
Summary of terrain, BoF indices, treatment goals in rhinopharyngitis
| Physiology | Systems | Subsystem | Activity | BoF index | Value |
|---|---|---|---|---|---|
| Congestion | ANS | Para | ↑ | – | – |
| Alpha | Variable | Leukocyte mobilization | ↑/↓ | ||
| Histamine | ↑ | Evoked histamine | ↑ | ||
| Beta | Nl/↓ | Platelet mobilization | ↓ or < LMI | ||
| Somatotropic | Insulin | ↑ | Insulin | ↑/↓ | |
| Pancreas | Exocrine | Congested | Somatostatin | ↑ | |
| Lymphatics | Lymphatics | Congested | – | – | |
| Immunity | Corticotropic | Adrenal cortex | ↓ | Adrenal cortex | ↓ |
| Thyrotropic | Thyroid | ↓ | Thyroid | ↓ | |
| Thyroid efficiency | ↓ for age | ||||
| Thymus | ↓ | Interleukin-1 | ↓ | ||
| Emunctories | Spleen | Congested | Platelet mobilization | ↓ | |
| Liver | Congested | Leukocyte mobilization | ↑/↓ | ||
| Detoxification | Emunctories | Gallbladder | Congested | – | – |
| Intestines | Congested | – | – |
Agent: Direct inducers of pathology
Given the precritical terrain, the etiology of rhinopharyngitis is in three factors: pathogenic organisms, environmental irritants, and structural factors. These include nasal polyps, deviated septum, and tonsil hypertrophy. The later impairs the flow of nasal secretions through the pharynx.7
Response: Critical terrain
The critical terrain involves adrenal cortex and peripheral thyroid. Thymus and spleen may also be implicated.
Dysregulation of immune activity involves the two catabolic axes. There is peripheral adrenal cortex insufficiency, which exacerbates hyperhistaminemia. Peripheral thyroid activity is insufficient. Because of the importance of thyroid activity in children from 1 to 7 years of age, they are particularly susceptible to ENT disorders, especially when there is a latent hypothyroidism (Chapter 10, Table 10.4). Finally, one may find insufficiency of thymic response to immune development (children) or acute infection (children and adults). Congestion of the spleen can diminish the filtering of pathogenic organisms as well as the development and function of immunity. When alpha activity is quantitatively elevated in the ENT region, it can congest lymphatics and lymph nodes, compromising local immune defense mechanisms.
Treatment guidelines
The majority of pathogenic organisms implicated in rhinopharyngitis are viruses.3 Thus, antibiotics are not applicable unless they are used as a secondary treatment for inflammation,10 which we do not recommend as routine practice. Our preferred approach to treatment is to address the underlying elements of the pre- and critical terrain noted earlier. Because the interior of the nose is directly accessible, essential oils are a particularly efficient treatment.
ANS
Goals:
-
●
Para: reduce hyper-vagal states
-
●
Alpha: block or reduce
-
●
Beta: support
Endocrine
Corticotropic
Thyrotropic
Peripheral: support peripheral thyroid function and reduce central factors as required
-
1.
Avena sativa
Thymus: support function
-
1.
Rhodiola rosea
Somatotropic
Support endocrine pancreatic efficiency
-
1.
Agrimonia eupatora: for complex emunctory implications: hepatobiliary and exocrine/endocrine pancreas involvement
-
2.
Plantago major: histamine and infectious pathologies are implicated in disease
-
3.
Juglans regia: particularly well suited for children as a gemmotherapy for blood sugar regulation
Sample treatment
-
1.
ANS-drainage: Plantago major MT 60 mL, Juglans regia GM 30 mL, Avena sativa MT 30 mL, Thymus vulgaris EO 1.5 mL, Lavandula angustafolia EO 1 mL, 3 mL three times per day × 6–10 days
-
2.
Immuno-endocrine: Rhodiola rosea MT 60 mL, Ribes nigrum GM 60 mL: 3 mL three times per day × 6–10 days
-
3.
Topical treatment, 6 years and older; for children 2–5 years: remove Mentha piperita
-
●
Lavandula angustafolia 4 drops, Eucalyptus smithii 2 drops, Thymus vulgaris, ct. linalool 1 drop, Mentha piperita 1 drop + carrier oil, 14 mL
-
●
Instructions: (1) mix well in a small glass container, (2) saturate a cotton-tipped applicator, (3) apply to lower nostrils 4–6 times per day, and (4) apply topically to nose, avoiding the eyes, 3 times per day
Diet
-
1.
Acute: liquid diet
-
2.
Subacute and chronic: pancreas and gallbladder sparing (gluten and dairy avoidance most important)
Sinusitis
Sinusitis is an infectious disease affecting the sinus cavities. The physiologic factors are similar to rhinopharyngitis but with a more intense active congestion by alpha-sympathetic.
Anatomy review
There are four symmetrical pairs of sinus cavities: frontal, sphenoid, ethmoid, and maxillary. The maxillary sinuses are contiguous with the nasal mucosa via the middle nasal concha (Fig. 9.2 ).
Fig. 9.2.
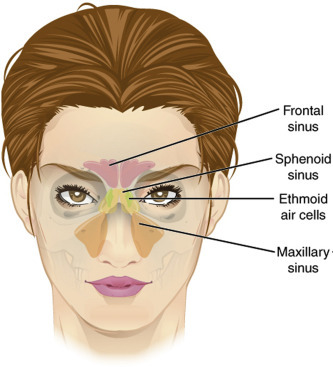
Anatomy of the sinuses. See text for details.
(Reproduced from OpenStax College [CC BY-SA 3.0] via Wikimedia Commons.)
Functional review
The activity of the sinuses is closely aligned with that of the rhinopharynx. Sinusitis is implicated as a source of rhinitis and vice versa. The sinuses serve five primary functions: (1) ventilation, (2) information, (3) humidification, (4) structure, and (5) defense. Ventilation allows for air exchange and equilibrium of pressure between the cranium and the general cephalic unit. Information refers to the provision of chemical information about quality of air. The sinuses serve as a secondary source of humidification, which keeps nasal mucous hydrated. The light-weight cavities of the sinuses form a light-weight structural support for the nose and first cranial nerve. Finally, the sinuses are a source of defense and containment: it contains exogenous aggressors to protect the body through its own defense system, which includes macrophages, immunoglobulins, mucous, antimicrobial secretions, etc.3, 15, 16
Cause: Precritical terrain
The precritical terrain is similar to that of rhinopharyngitis. Patients with chronic type 1 allergies are susceptible to sinus congestion for reasons discussed in prior chapters.
Local and regional agents that exacerbate the precritical terrain
-
1.
The following increase the general risk for sinusitis: (a) cysts, (b) granulomas, and (c) polyps
-
2.
Maxillary affectations: dental infections
-
3.
Maxillary and frontal sinus: chronic rhinopharyngitis
Agent: Induction of disease
In sinusitis, the nature of aggression can either be a single substantial aggression, or prolonged and repetitive aggressions that fragilize the terrain3:
-
1.
Allergy flare-up
-
2.
Rhinopharyngitis
-
3.
Adaptive demands that increase alpha
-
4.
Metabolic demands that increase para with a reactive alpha
-
5.
Weather and geographic changes with a sudden increase in hydrostatic pressure
-
6.
Altered ventilation
-
7.
Blocked drainage: that is, nasal endothelial edema and inflammation (Fig. 9.3 ), adenoid hypertrophy (Fig. 9.4).
Fig. 9.3.
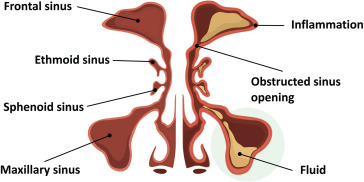
Obstructed maxillary sinus. An obstructed sinus does not allow for the functions of the sinuses to occur efficiently. The stagnation of fluid makes it susceptible to infections, shown here affected the patient’s left frontal and maxillary sinuses.
(Reproduced from logika600/Shutterstock.com.)
Fig. 9.4.

The oronasal tonsils. The oronasal tonsils (adenoids, palatine tonsils, lingual tonsils) when enlarged may obstruct the drainage of fluids from the nose, sinuses, and eustachian tubes.
(Reproduced from Blausen.com staff (2014). Medical gallery of Blausen Medical 2014. WikiJ Med 2014;1(2). doi:10.15347/wjm/2014.010. [CC BY 3.0] from Wikimedia Commons.)
Response: Critical terrain
Due to the partially or fully enclosed nature of the sinus cavities, those susceptible to sinusitis are those in whom the alpha-sympathetic activity is quantitatively more elevated than parasympathetic and as compared to those who only experience rhinopharyngitis with the same terrain. Recall that in rhinopharyngitis, para is greater than alpha.
-
1.ANS
-
a.Para: hyperfunctioning with congestion and hypersecretions
-
b.Alpha: hyperfunctioning to isolate the sinuses and protect the regional tissues
-
c.Beta: hypofunctioning, prolongs:
-
i.Congestion
-
ii.Obstruction
-
iii.Stagnation of secretions
-
i.
-
a.
-
2.
Endocrine: cf. rhinopharyngitis
-
3.
Emunctory: cf. rhinopharyngitis
General treatment guidelines
There is a potential role for the use of antibiotics in acute sinusitis, though even this is questionable, both in adults and children. A majority of cases resolve without treatment.17 In chronic sinusitis, or, chronic recurrent sinusitis, antibiotics are not effective in resolving the recidivistic nature of the infection.18 Considering the long-term risk of cancer in patients correlating with total life-time utilization of antibiotics,19, 20, 21 we don’t recommend antibiotics as an exclusive method of treating chronic recurrent sinusitis. Given the risk of evolution of chronic sinusitis to allergic (extrinsic) asthma (cf. The Theory of Endobiogeny, Volume 3, Chapter 2), it become all the more capital to treat the underlying precritical terrain.22 According to the theory of endobiogeny, the order of priority and intensity of therapy in sinusitis is at variance with that of rhinopharyngitis due to the location and function and accessibility of the sinuses. The top areas of focus are the sinuses and gallbladder.
Drainage
-
1.Local:
-
a.Sinus rinses: saline ± bicarbonate ± hydrolats (peppermint, chicory, pine, balsam fir, etc.) or dilute tisanes (thyme, chamomile, lavender, and peppermint)
-
b.Essential oils: dilute and apply topically over sinuses (cf. below)
-
a.
-
2.Gallbladder11, 12
-
a.Acute sinusitis: intense drainage, that is, 1–2 mL per dose, 3–4 times a day with complete avoidance of fried foods, cooked animal fats, and creamy foods
-
i.Carduus marianus
-
ii.Raphanus niger
-
iii.Agrimonia eupatora
-
i.
-
b.Subacute: less intense drainage, that is, 0.5–1.5 mL per dose, 2–3 times per day with restricted consumptions of foods noted above
-
a.
-
3.
Pancreas, exocrine, and endocrine: moderate and permanent support, even after infection has resolved: cf. Rhinopharyngitis
-
4.
Spleen: in cases linked to allergies or chronic inflammation
-
5.
Liver: as needed: cf. Rhinopharyngitis
This recipe addresses ANS imbalances, drainage, is mucolytic, strongly antiinfectious and antiinflammatory.
ANS, general
-
1.Alpha: support during acute sinusitis to relaunch beta and open up sinus passages11, 12
-
a.Citrus limon (lemon) EO
-
b.Cupressus sempervirens (cypress) see materia medica for fuller discussion of actions
-
i.Galenic: essential oil
-
ii.Summary: optimal for ear, nose, and throat maladies; treats and drains the terrain, broad-acting antimicrobial
-
iii.Lymph: lymphatic decongestant; Immune: antioxidant, antiinflammatory (vascular), stimulates immune system; ENT: drains tonsils; ID: (EO only) antiviral (influenza, HSV, coronavirus, varicella, hepatitis A): prophylactic (inhibits virus entry into host cells), lytic mechanism; ENT: drainer, mucolytic, antitussive, ANS: parasympatholytic, mild alpha-sympathomimetic (vasoconstrictor) by inhibiting COMT enzyme; Neuro: antalgic, antineuralgic
-
iv.Use: viral infections of ENT (esp. with spring and autumn flare-ups in chronic infections), upper and lower respiratory tracts, the elderly and children, hypervagal responses to infection with anergy, viral hepatitis; viral-induced asthma
-
v.Method: EO: topical; nebulized: 1–2 drops in 3 mL 0.9% saline
-
i.
-
a.
-
2.Parasympatholytics: reduce at all times, more intensely in the postacute phase
-
a.Thymus vulgaris EO, tisane
-
b.Cupressus sempervirens EO
-
a.
Endocrine
-
1.
Corticotropic: cf. Rhinopharyngitis
-
2.
Thyrotropic: cf. Rhinopharyngitis
-
3.
Somatotropic: cf. Rhinopharyngitis
Sample treatment
-
1.
ANS-drainage: Plantago major MT 60 mL, Carduus marianus MT 30 mL, Cynara scolymus MT 30 mL, Thymus vulgaris EO 1.5 mL, Lavandula angustafolia EO 1 mL, 4 mL three times per day × 6–10 days, then 2.5–3 mL twice per day for an additional 6–10 days if season of recurrent sinusitis
-
2.
Immuno-endocrine: Rhodiola rosea MT 60 mL, Ribes nigrum GM 60 mL: 3 mL three times per day × 6–10 days
-
3.Topical application, Use: 2 years and older:
-
a.Eucalyptus ssp. 5 drops, Cupressus sempervirens 3 drops, Thymus vulgaris, ct. linalool 2 drops, Citrus limon 1 drop + carrier oil, 14 mL
-
b.Instructions: (1) mix well in a small glass container, (2) apply topically to sinus cavities, avoiding the eyes, 3–4 times per day during acute sinusitis and 2–3 times per day for chronic sinusitis, (3) saturate a cotton-tipped applicator, and (4) apply to lower nostrils 2–4 times per day when signs of rhinopharyngitis are also present
-
a.
Diet
-
1.
Pancreas- and gallbladder-sparing
Tonsillitis
Tonsillitis is an infectious disorder involving the lymphoid tissue of the naso-oral region—the very tissue designed to protect the ear nose and throat from infections.
Anatomy review
There refers to three sets of lymphoid tissues which are commonly referred to as “tonsils”: adenoids, palatine, and lingual.23 As becomes readily apparent (Fig. 9.4 ): tonsil enlargement, even when noninfected, creates a terrain that favors rhinopharyngitis, sinusitis, otitis media (OM), and airway obstruction with all that that implies.
Functional review
The tonsils sit at the cross roads of digestion, respiration, and immunity. They serve as the primary immune-protection against respiratory and digestive pathogens. They are a lymphoid tissue containing B and T lymphocytes, and macrophages.
Cause: Precritical terrain
The precritical terrain develops from adaptative neuroendocrine-emunctory imbalances meant to regulate the structure and function of lymphoid tissue.
ANS
-
1.
Para: hyperfunctioning
Endocrine
The endocrine imbalances are different from the upper airway conditions. The follicular nature of lymphoid tissue and implication of thyroid-stimulating hormone (TSH) in lymphoid activity implicates gonado-thyrotropic coupling that plays an important role in the growth of lymphoid tissue. The exocrine pancreas and endocrine pancreas are implicated because of their role in the adenoidal tissue growth.
-
1.Gonadotropic
-
a.Hyper-follicle-stimulating hormone (FSH)
-
i.Congests mucosal tissue
-
ii.Stimulates estrogens
-
i.
-
b.Hyperestrogenism
-
i.Makes an appeal to TSH (cf. below)
-
ii.Favors overproliferation of immune cells and hence the lymphoid tissues in which they are housed
-
i.
-
c.TSH
-
i.Horizontal stimulation by FSH: increased release of lymphocytes from the thymus which overpopulate the tonsils
-
ii.Radial stimulation by estrogens:
-
1.T-cell proliferation
-
2.Adenoid histological growth
-
1.
-
iii.Implicated: insufficient peripheral thyroid response relative to the level of TSH demand
-
i.
-
a.
-
2.Somatotropic
-
a.Pancreas, endocrine: hyperinsulinism with elevated insulin resistance: increased nutrition for growth of cells
-
a.
Emunctory
-
1.
Pancreas, exocrine: oversolicitation participates in adenoidal growth
-
2.
Congestion of other lymphoid tissue favors a greater reliance on tonsils for immune defense
-
3.
Gallbladder: insufficient toxin elimination
Agents of aggression
-
1.
Rhinopharyngitis
-
2.
Sinusitis
-
3.
Infection
Response: Critical terrain
ANS
Sympathetic hyperfunctioning with active congestion of lymphoid tissue favoring stasis and infections
-
1.Para: hyperfunctioning
-
a.Exudative pharyngitis (with puss): nonstreptococcal antibiotic use not as strongly indicated in immunocompetent patients
-
a.
-
2.Alpha: Hyperfunctioning (congestion of lymphoid tissue)
-
a.Nonexudative pharyngitis: Streptococcus use antibiotics to avoid rheumatic cardiac and renal complications
-
a.
-
3.
Beta: normal, insufficient, or delayed
Endocrine
-
1.
Corticotropic, peripheral: insufficient response to infection
-
2.
Thyrotropic, peripheral: insufficient response to infection
Emunctory
-
1.
Exocrine pancreas oversolicited, participates in immune cell production along with estrogens and TSH
Treatment guidelines: General
-
1.Pancreas11, 12
-
a.Drain: Rubus fructicosa leaf or bud (GM)
-
b.Reduce oversolicitation (with ENT benefit)
-
i.Avena sativa MT, BH
-
ii.Agrimonia eupatora MT, BH
-
iii.Plantago major MT, BH
-
iv.Juglans regia MT, GM, BH
-
v.Eucalyptus ssp. EO, BH
-
vi.Pancreas sparing diet
-
i.
-
c.During active infection
-
i.Vitis vinifera (grape bud) GM: antistreptococcal
-
ii.Eucalyptus ssp. EO exudative tonsillitis, especially in vagotonics
-
iii.Zingiber officinale when thyroid insufficiency implicated
-
iv.Cinnamoma zeylanicum EO in cold, asthenic patients with active infection
-
i.
-
a.
-
2.Thyrotropic
-
a.Reduce thryotropin-releasing hormone (TRH) if playing a role in FSH relaunching
-
i.Viburnum lantanum GM
-
ii.Leonurus cardiaca MT, BH
-
i.
-
b.Support peripheral thyroid to reduce TSH
-
i.Avena sativa (all ages): polyvalent in tonsillitis
-
ii.Zingiber officinale (8 years and older): if adrenal cortex and/or androgen insufficiency also present
-
iii.L-tyrosine + iodine: general support for thyroid production of hormones
-
i.
-
a.
-
3.Corticotropic: support adrenal cortex as needed
-
a.Reduce adrenocorticotropic hormone (ACTH) horizontal relaunching of FSH
-
i.Ribes nigrum GM
-
ii.Quercus pedunculata GM
-
i.
-
a.
-
4.Pituitary: support general relaunching if recurrent infections
-
a.Rhodiola rosea
-
b.Inula helenium
-
a.
General approach to treatment
Because tonsillitis most commonly affects young children, a sample tincture is presented that is palatable. The use of medicinal plants for treatment of tonsillitis does not obviate the need to consider standard of care therapies.
Infection-endocrine: Olea europaea GM 30 mL Vitis viniferis GM 30 mL, dose: 1.5 mL QID for 6–10 days
Drainage: Plantago major MT 30 mL, Avena sativa MT 30 mL, Eucalyptus spp. EO 12 drops, Cinnamoma zeylanicum 3 drops, dose: 1.5 mL QID for 6–10 days
Specific treatment guidelines: Exudative pharyngitis (white)
ANS
- 1.
Drainage
- 1.
-
2.Liver and gallbladder
-
a.Carduus marianus MT, BH
-
b.Agrimonia eupatora MT, BH
-
c.Plantago major MT, BH
-
a.
Specific treatment guidelines: Nonpurulent pharyngitis (red)
Drainage
- 1.
- 2.
Otitis media
OM is an infectious disorder involving the serosal tissue of the eustachian tube resulting in tympanic pressure, pain, inflammation, and fever.
Anatomical and functional review
The tympanum and inner ear cavity are serosal structures of mesodermal origin, which implicates the gonadotropic axis. The serosal structures produces secretions that act as a defense against infections from the nasopharynx.24 Ciliary activity moves the fluid and anything trapped within it. It also equalizes ear pressure and allows for appropriate tympanic response to sound. The eustachian tube also allows for passive drainage of serosal fluid and participates in equalization of pressure.24 It is supported by muscles that can become dysfunctional in spasmophilic states, favoring OM due to stasis of fluid. While there are numerous contributing factors, the diminished angle of drainage in infants and toddlers compared to older children and adults makes them particularly susceptible (Fig. 9.5 ).25
Fig. 9.5.
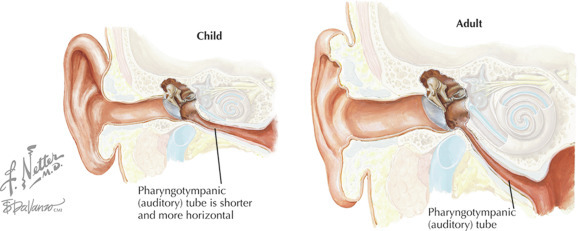
Eustachian tube anatomy in infants vs adults. Infants have a narrower angle to the eustachian tube that is more susceptible to stasis and stagnation, allowing microorganisms to grow in its protein-rich environment.
(Courtesy of Netter medical illustration used with permission of Elsevier. All rights reserved.)
Cause: Precritical terrain
ANS
The ANS dysfunction is spasmophilic, as with the other ENT disorders discussed. However, the role of the ANS is not only in congestion of the serosa, but stasis of serosal fluid.
-
1.
Para: hyperfunctioning
-
2.
Alpha: often hyperfunctioning due to solicitation of lymphatics
Endocrine
Cf. Rhinopharyngitis
-
1.
Corticotropic, peripheral: insufficient response to an infectious aggression
-
2.
Thyrotropic, peripheral: insufficient response to an infectious aggression
Emunctory
Listed in order of implication in disease and importance of treatment for prevention of recurrent OM:
-
1.
Pancreas, exocrine (overgrowth of tissue)
-
2.
Liver (autointoxication)
-
3.
Gallbladder (autointoxication)
-
4.
Intestine (autointoxication)
Immunity
Compromised immunity from lack of, or, insufficient duration of breast feeding, and maternal postnatal diet are correlated with increased risk of OM in infancy and early childhood.26
Agents of aggression:
There are two general categories: impaired drainage and increased exposure to potential pathogens:
-
1.Impaired drainage
-
a.Generalized and regional spasmophilia (effects on eustachian tube)
-
i.Change of seasons
-
ii.Sudden changes in weather
-
iii.Psychic aggressions
-
iv.Cosmobiologic events
-
i.
-
b.Sudden changes in altitude
-
c.Blowing nose forcefully
-
d.Enlarged adenoidal tonsils27
-
a.
- 2.
Response: Critical terrain
Serosal fluid is rich in protein. In a precritical terrain, when there is simultaneously substantially diminished or blocked drainage of serosal fluid and establishment of virulent organisms a patient is susceptible to otitis media with effusion (OME).
ANS
-
●
Hyper-para further elevated
-
●
Hyper-alpha further elevated
-
●
Beta: often delayed, sometimes insufficient, worsening congestion
Beta-surge results in risk of tympanic membrane perforation and external drainage.
Endocrine
Cf. Rhinopharyngitis
Emunctories
Adaptative response exacerbates the precritical emunctory imbalances
Drainage of the liver is more imperative in OM than in other ENT disorders
Treatment Guidelines
Symptomatic
Local treatments
Distention of the tympanic membrane can cause significant discomfort for children. As with treatment of the nasal cavity, ready access to the tympanum from the ear canal allows for direct application of therapeutics with rapid onset of action for relief. Local application of symptomatic therapies is preferred because it allows for the regional and systemic response to infections to continue and reach its natural conclusion.
-
1.Antiinfectious and antiinflammatory:
-
a.Dexamethasone 0.1%/ciprofloxacin 0.3%
-
a.
-
2.Analgesic/antipyretic/decongestant
-
a.Antipyrine 5%/benzocaine 5%/phenylephrine 5%
-
a.
Recipe for nonpharmaceutical analgesic/antipyretic/decongestant/antiinfectious/antiinflammatory topical remedy
-
1.
Slice 1 clove raw garlic in 3–4 pieces32
-
2.
Simmer at low heat in 30 mL olive oil for 10 min
-
3.
Remove from heat and cool until comfortable when dropped on back of hand
-
4.
Place in a 1 oz glass jar
- 5.
Instruction
-
a.
Have child lay on their side, head parallel to the ground
-
b.
Life the affected ear up and out
-
c.
Add 3–4 drops of the oil
-
d.
Take a cotton ball and twist a portion and insert fine tip into ear canal to prevent leakage of admixture
-
e.
Repeat every 2–3 h while the child is awake until relief is achieved
Emunctory drainage
-
1.
Hepatobiliary, cf. above
-
2.
Pancreas, cf. above
-
3.
Intestinal regulation, cf. above
ANS
-
1.
Para: block, cf. above
-
2.
Alpha: block, cf. above
-
3.Beta: block with spasms only
-
a.Crataegus oxycantha
-
a.
Endocrine
-
1.
Corticotropic, cf. above
-
2.
Thyrotropic, cf. above
-
3.
Somatotropic, cf. above
Diet
-
1.
Pancreas sparing diet
-
2.
Liquids: soups, fruit juices rich in vitamin C
Lifestyle
-
1.
Avoid rapid changes in altitude
-
2.
Avoid blowing nose aggressively
Mechanical
-
1.
Cranial work
-
2.
Evaluate for short frenulum and oral-motor competency
Sample treatment
Dosed for children 2–4 years of age
-
1.
Drainage: Ulmus campestre (hedge maple) GM 10 mL, Vitis vinifera GM 30 mL, Olea europaea GM 20 mL, Dose: 1–2 mL four times per day × 4 days, then 1–2 mL three times per day for 6 days
-
2.
Immuno-endocrine: Quercus pedunculata GM 15 mL, Ribes nigrum GM 45 mL: 2 mL four times per day × 4 days, then 2 mL three times per day for 6 days
-
3.
Garlic/EO blend: insert in affected during time of administration of tinctures; also, use needed up to every 2 h for pain to affected ear canal
Acute bronchitis
Bronchitis is an infection of the upper airways of the lungs that occurs due to local inflammation and congestion.
Anatomy
The bronchi are the main airways leading to the lobes of the lungs (Fig. 9.6 ). They have a series of cartilaginous rings that provide structural support during the negative pressure of inspiration. The main bronchus is contiguous with the trachea, which is superior to it. The main bronchus splits into two branches: left and right. The left bronchus further splits into left superior and left inferior branches. Further divisions of the airway are referred to as bronchioles. They have a considerably smaller diameter and lack the cartilaginous rings.
Fig. 9.6.

Anatomy of the upper and lower airways. See text for details.
(Reproduced from CFCF [CC BY-SA 3.0] from Wikimedia Commons.)
Review of general function
With respect to gas exchange, the bronchi are “dead space.” Its roles are centered around qualifying the air and protecting the lungs and the body. It conducts oxygen into the lungs during inspiration and carbon dioxide out during expiration. It provides additional conditioning of air (after the nasal airway) by further humidifying it. It provides immunologic and environmental defense in three ways: bronchial-associated lymphoid tissue (BALT), mucous, and cilia. Mucous traps particulate matter and the cilia move it cephalad allowing for it to be expectorated.
Cause: Precritical terrain
The precritical terrain is a global neuroendocrine hyperfunctioning with fragilization of the bronchi. This may occur via numerous factors, discussed below in the order of importance in the general rate of anabolic functioning. All factors listed are overfunctioning
-
1.Endocrine
-
a.Pituitary
-
b.Thyroid: TSH, T4
-
c.Pancreas, endocrine
-
d.Adrenal cortex (lesser role)
-
a.
-
2.
ANS: para
-
3.Emunctory
-
a.Defense
-
i.Exocrine pancreas: mucous production
-
ii.Spleen: immunity
-
i.
-
b.Congestion
-
i.Colon
-
ii.Liver
-
iii.Skin
-
i.
-
a.
The net effect is a local congestion and fragilization of the bronchi.
Agent: Induction of bronchitis
In the face of the fragilization and congestion of the bronchopulmonary unit, exposure to aggressors further degrades the bronchi and solicits a local and global neuroendocrine- emunctory response. This response will determine the type of bronchitis. Viruses are the most common cause of acute bronchitis. Noninfectious agents can trigger an acute-on-chronic bronchitis. The four key factors to consider are: (1) pathogens, (2) particulate matter and gasses (allergens, tobacco smoke, etc.), (3) gastric secretions with micro-aspiration, and (4) cold.33
Response: Induction of acute bronchitis
Acute bronchitis develops as a maladapted response to the local aggression on the airways. It can be divided into two categories: wet or dry (Fig. 9.7 ) based on the ANS response during illness. Dry, inspiratory coughing is related to hyper-alpha predominance. Wet, expiratory coughing is related to a hyper-para predominance. The quality and quantity of mucous is further determined by the endocrine and exocrine pancreatic response that predominates in the adaptation response. The treatment must be tailored to the type of bronchitis.
Fig. 9.7.

Bronchitis terrain. The precritical terrain (yellow) of bronchitis is shown in the upper 1/4th of the image, where the factors related to global disequilibrium of anabolism are presented. In the second section, around oxygen demand are the fragilizers that allow for the aggressor to lead to the critical terrain. The lower half of the image shows the critical terrain specific to acute vs chronic bronchitis and acute wet vs acute dry bronchitis. Acute dry bronchitis (purple) has an inspiratory cough and a predominance of alpha > para. Acute wet bronchitis is an expiratory cough with a predominance of para > alpha that occurs in vagotonic individuals. The quality of mucous then further differentiates the particularities of the critical terrain in the individual and allows for a personalized approach to treatment.
(© 2015 Systems Biology Research Group.)
Symptomatic treatment of acute bronchitis
Pharmacologic treatment with antibiotics is only modestly effective, and carries the typical short- and long-term risks associated with antibiotics already discussed.34, 35 Given the self-limited nature of most cases of acute bronchitis,36 then, a nonpharmacological approach is worth considering. Both symptomatic treatment as well as that of the terrain has been quite effective.11, 37
Inflammation is the common local histopathology. All forms of acute bronchitis should be treated with antiinflammatory and antiinfectious agents when implicated. Key symptomatic treatments are listed in Table 9.2 with indication of symptom(s) treated.11, 12 For more severe symptoms, essential oils can be nebulized in a 5% concentration (3 drops per 3 mL of solution). In our experience, two highly efficient essential oils are Cupressus sempervirens and Lavandula angustafolia. For wet bronchitis, use 3% normal saline, as it helps dissolve inspissated mucous.38 For dry bronchitis, 0.9% normal saline suffices. Also see The Theory of Endobiogeny, Volume 3, Chapter 2 for additional approaches to nebulization of essential oils.
Table 9.2.
Summary of polyvalent plants for acute wet and dry bronchitis
| Plant | Antispasm | Decongestant/pulm. drainer | Antiinflam. | Antiallergic | Antiinfect. | Mucolytic/expectorant | Emollients |
|---|---|---|---|---|---|---|---|
| Agrimonia eupatora | • | • | • | • | |||
| Arctium lappa | •a | • | • | ||||
| Cupressus sempervirensb | • | • | • | • | • | ||
| Eucalyptus sspb | • | • | • | • | • | ||
| Glycyrrhiza glabra | • | • | • | • | |||
| Inula helenium | • | • | • | • | |||
| Lavandula angustafoliab | • | • | • | • | |||
| Plantago major | • | •a | • | • | • | ||
| Malva sylvestrisc | • | • | • | ||||
| Viola tricolor | •a | • | • | • |
Indirect decongestant.
Can be diffused or nebulized as an essential oil.
Parasympathomimetic: use at regulating doses in wet, hyper-para bronchitis.
Drainage
Drainage is listed in order of importance (Table 9.3 ). One will note that many of the medicinal plants listed are the same as those used for symptomatic treatment of the critical terrain.11, 12
Table 9.3.
Drainage of organs implicated in acute bronchitis that also have pulmonary tropism
| Organ | Plantago major | Viola tricolor | Agrimonia eupatora | Ceanothus americanus |
|---|---|---|---|---|
| Exocrine pancreas | • | • | ||
| Spleen | • | |||
| Intestines | • | • | • | |
| Liver | • | • | • | |
| Skin | • |
Endocrine
- 1.
-
2.Thyrotropic: reduce global hyperfunctioning of the axis11, 12
-
a.Leonorus cardiaca MT, BH especially with tachycardia or nervous asthenia
-
b.Vibernum lantanum GM for inflammation implicating TRH, allergic-asthmatic bronchitis and for pulmonary drainage
-
c.Zea mais GM especially with inflammation and intense fatigue
-
d.Cornus sanguinea GM especially for inflammation and blood-tinged expectorations
-
a.
- 3.
Summary of approach to wet bronchitis
-
1.
Reduce para > alpha
-
2.
Bronchospasm
-
3.
Reduce excess production of secretions: exocrine pancreas
-
4.
Break up mucous: mucolytics
-
5.
Expectoration: expectorants
Sample treatment of wet bronchitis
Neuroendocrine-infectious: Inula helenium MT 30 mL, Fabiana imbricata MT 30 mL, Ribes nigrum GM 60 mL, Lavandula angustafolia EO 1.5 mL, Satureja montana EO 1 mL: 3 mL three times per day for 10–14 days
Drainage: Agrimonia eupatora MT 60 mL, Plantago major MT 30 mL, Arctium lappa MT 30 mL, Eucalyptus smithii EO 2 mL: 3 mL three times per day for 10 days
Summary of approach to dry bronchitis
-
1.
Reduce alpha
-
2.
Bronchospasm
-
3.
Emollients
-
4.
Support global adrenal function
-
5.
Reduce cortisol
-
6.
Reduce global thyrotropic activity
Sample treatment of dry bronchitis
Neuroendocrine-infectious: Passiflora incarnata MT 40 mL, Vibernum lantanum GM 40 mL, Cornus sanguinea GM 40 mL, Lavandula angustafolia EO 1.5 mL, Cinnamomum zeylanicum EO 1 mL, Dose: 3 mL three times per day for 10–14 days.
Emollient-drainage-infectious: Agrimonia eupatora MT 60 mL, Malva sylvestris MT 60 mL, Eucalyptus smithii or globulus EO 1 mL, Cupressus sempervirans EO 1 mL, Dose: 3 mL three times per day for 10–14 days.
A recipe for spasmodic cough in adults
Regardless of the wet or dry nature, when the cough is spasmodic, the endocrine-infectious treatment can be modified to address the spasm:
Neuroendocrine-infectious: Ribes nigrum GM 60 mL, Populus niger GM 60 mL, Satureja montana EO 0.5 mL, Cinnamomum zeylanicum EO 0.5 mL, dose: 2 mL three times per day.
A recipe for spasmodic cough in children
Children are more taste sensitive. Remove the essential oils from the tincture and utilize a topical blend of antispasmodic essential oils.
Antispasmodic topical essential oil blend
Eucalyptus ssp. EO 8 drops, Lavandula angustafolia EO 4 drops, Cupressus sempervirans EO 3 drops in 1 tbsp (15 mL) carrier oil: mix in a glass bowl, apply with friction rub in circular and cephalad/caudal motions for 3–4 min, then cover chest with a shirt or blanket, then a heated pad or towel. Repeat up to every hour as needed. May also diffuse in an aromatherapy diffuser placed within 0.6 m from the child.
Diet
-
1.
Free of sugars, cooked animal fats
-
2.
Liquid diet during acute phase with root vegetables: turnip, black radish, and juices of carrot, quince, chervil, cabbage, lettuce, mulberry, apple, and turnip
Conclusions
From the perspective of the theory of Endobiogeny, infectious diseases are best viewed as arising from a triadic interaction between the infector, the terrain of the infected, and the environmental factors that favor the former and adversely effect the latter. Among the infectious diseases presented here, few have been shown to be effectively managed with antibiotics as first-line treatment in uncomplicated cases. There is, then a quandary which the physician faces. To use antibiotics may induce harm and is likely not effective. To not treat leaves the patient suffering and is a burden on the family, work and thus on society as a whole. If not this, then what to use? We have found in our nearly five decades of clinical practice the rational clinical usage of medicinal plants quite effective. They can be applied symptomatically, to the critical terrain, or pre-critical terrain to prevent recurrent infections. The approach laid out involves both anti-infectious treatments and drainage, but also regulation of the neuroendocrine determinants of the infectious terrain. In the out-patient population, this approach proves efficient and compassionate to alleviate the burden faced by the patient.
References
- 1.Lyons A.S., Petrucelli R.J. Abradale Press/H.N. Abrams; New York: 1987. Medicine: An Illustrated History. [Google Scholar]
- 2.Heetderks D.L. Observations on the reaction of normal nasal mucous membranes. Am J Med Sci. 1927;174:231–244. [Google Scholar]
- 3.Bachert C., Krysko O., Gevaert P., Berings M., Perez-Novo C., van Crombruggen K. Nasal immunity, rhinitis, and rhinosinusitis. In: Mestecky J., Russel M.W., Cheroute H., Strober W., Kelsall B.L., Lambrecht B.N., editors. Mucosal Immunology. 4th ed. Academic Press; 2015. pp. 1899–1921. Vol. 2 [chapter 100] [Google Scholar]
- 4.Santos D.V., Reiter E.R., DiNardo L.J., Costanzo R.M. Hazardous events associated with impaired olfactory function. Arch Otolaryngol Head Neck Surg. 2004;130(3):317–319. doi: 10.1001/archotol.130.3.317. [DOI] [PubMed] [Google Scholar]
- 5.Kuukasjarvi S., Eriksson C.J.P., Koskela E., Mappes T., Nissinen K., Rantala M.J. Attractiveness of women’s body odors over the menstrual cycle: the role of oral contraceptives and receiver sex. Behav Ecol. 2004;15(4):579–584. [Google Scholar]
- 6.Stern K., McClintock M.K. Regulation of ovulation by human pheromones. Nature. 1998;392(6672):177–179. doi: 10.1038/32408. [DOI] [PubMed] [Google Scholar]
- 7.Naclerio R.M., Bachert C., Baraniuk J.N. Pathophysiology of nasal congestion. Int J Gen Med. 2010;3:47–57. doi: 10.2147/ijgm.s8088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pearlman D.S. Pathophysiology of the inflammatory response. J Allergy Clin Immunol. 1999;104(4 Pt 1):S132–S137. doi: 10.1016/s0091-6749(99)70308-8. [DOI] [PubMed] [Google Scholar]
- 9.Erle D.J., Sheppard D. The cell biology of asthma. J Cell Biol. 2014;205(5):621–631. doi: 10.1083/jcb.201401050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Scaglione F., Rossoni G. Comparative anti-inflammatory effects of roxithromycin, azithromycin and clarithromycin. J Antimicrob Chemother. 1998;41(suppl B):47–50. doi: 10.1093/jac/41.suppl_2.47. [DOI] [PubMed] [Google Scholar]
- 11.Duraffourd C., Lapraz J.C. Masson; Paris: 2002. Traité de Phytothérapie Clinique: Médecine et Endobiogénie. [Google Scholar]
- 12.Lapraz J.C., Carillon A., Charrié J.-C. Lavoisier; Paris: 2017. Plantes Médicinales: Phytothérapie Clinique Intégrative et Médecine Endobiogénique. [Google Scholar]
- 13.Kelly G.S. Rhodiola rosea: a possible plant adaptogen. Altern Med Rev. 2001;6(3):293–302. [PubMed] [Google Scholar]
- 14.Pooja B.A.S., Khanum F. Anti-inflammatory activity of Rhodiola rosea—a second-generation adaptogen. Phytother Res. 2009;23(8):1099–1102. doi: 10.1002/ptr.2749. [DOI] [PubMed] [Google Scholar]
- 15.Lundberg J.O. Nitric oxide and the paranasal sinuses. Anat Rec (Hoboken) 2008;291(11):1479–1484. doi: 10.1002/ar.20782. [DOI] [PubMed] [Google Scholar]
- 16.Lundberg J.O., Farkas-Szallasi T., Weitzberg E. High nitric oxide production in human paranasal sinuses. Nat Med. 1995;1(4):370–373. doi: 10.1038/nm0495-370. [DOI] [PubMed] [Google Scholar]
- 17.Abzug M.J. Acute sinusitis in children: do antibiotics have any role? J Infect. 2014;68(suppl 1):S33–S37. doi: 10.1016/j.jinf.2013.09.012. [DOI] [PubMed] [Google Scholar]
- 18.Henderson B., Nair S., Pallas J., Williams M.A. Fibronectin: a multidomain host adhesin targeted by bacterial fibronectin-binding proteins. FEMS Microbiol Rev. 2011;35(1):147–200. doi: 10.1111/j.1574-6976.2010.00243.x. [DOI] [PubMed] [Google Scholar]
- 19.Velicer C.M., Heckbert S.R., Rutter C., Lampe J.W., Malone K. Association between antibiotic use prior to breast cancer diagnosis and breast tumour characteristics (United States) Cancer Causes Control. 2006;17(3):307–313. doi: 10.1007/s10552-005-0445-9. [DOI] [PubMed] [Google Scholar]
- 20.Velicer C.M., Lampe J.W., Heckbert S.R., Potter J.D., Taplin S.H. Hypothesis: is antibiotic use associated with breast cancer? Cancer Causes Control. 2003;14(8):739–747. doi: 10.1023/a:1026323424792. [DOI] [PubMed] [Google Scholar]
- 21.Velicer C.M., Taplin S. Genetic testing for breast cancer: where are health care providers in the decision process? Genet Med. 2001;3(2):112–119. doi: 10.1097/00125817-200103000-00005. [DOI] [PubMed] [Google Scholar]
- 22.Slavin R.G., Spector S.L., Bernstein I.L. The diagnosis and management of sinusitis: a practice parameter update. J Allergy Clin Immunol. 2005;116(6 suppl):S13–S47. doi: 10.1016/j.jaci.2005.09.048. [DOI] [PubMed] [Google Scholar]
- 23.Brodsky L. Modern assessment of tonsils and adenoids. Pediatr Clin N Am. 1989;36(6):1551–1569. doi: 10.1016/s0031-3955(16)36806-7. [DOI] [PubMed] [Google Scholar]
- 24.Mazer B.D. Otitis media. In: DYM L., Bonilla F.A., Sampson H.A., Szefler S.J., Akdis C.A., editors. Pediatric Allergy: Principles and Practice. 3rd ed. Elsevier; 2016. pp. 219–227.e213. [chapter 25] [Google Scholar]
- 25.Sadler-Kimes D., Siegel M.I., Todhunter J.S. Age-related morphologic differences in the components of the eustachian tube/middle ear system. Ann Otol Rhinol Laryngol. 1989;98(11):854–858. doi: 10.1177/000348948909801104. [DOI] [PubMed] [Google Scholar]
- 26.Levi J.R., O'Reilly R. Complementary and integrative treatments: otitis media. Otolaryngol Clin N Am. 2013;46(3):309–327. doi: 10.1016/j.otc.2013.01.001. [DOI] [PubMed] [Google Scholar]
- 27.Deutsch E.S. Tonsillectomy and adenoidectomy. Changing indications. Pediatr Clin N Am. 1996;43(6):1319–1338. doi: 10.1016/s0031-3955(05)70521-6. [DOI] [PubMed] [Google Scholar]
- 28.Revai K., Dobbs L.A., Nair S., Patel J.A., Grady J.J., Chonmaitree T. Incidence of acute otitis media and sinusitis complicating upper respiratory tract infection: the effect of age. Pediatrics. 2007;119(6):e1408–e1412. doi: 10.1542/peds.2006-2881. [DOI] [PubMed] [Google Scholar]
- 29.Wald E.R., Guerra N., Byers C. Upper respiratory tract infections in young children: duration of and frequency of complications. Pediatrics. 1991;87(2):129–133. [PubMed] [Google Scholar]
- 30.Hammaren-Malmi S., Saxen H., Tarkkanen J., Mattila P.S. Passive smoking after tympanostomy and risk of recurrent acute otitis media. Int J Pediatr Otorhinolaryngol. 2007;71(8):1305–1310. doi: 10.1016/j.ijporl.2007.05.010. [DOI] [PubMed] [Google Scholar]
- 31.Ilicali O.C., Keles N., Deger K., Savas I. Relationship of passive cigarette smoking to otitis media. Arch Otolaryngol Head Neck Surg. 1999;125(7):758–762. doi: 10.1001/archotol.125.7.758. [DOI] [PubMed] [Google Scholar]
- 32.Sarrell E.M., Mandelberg A., Cohen H.A. Efficacy of naturopathic extracts in the management of ear pain associated with acute otitis media. Arch Pediatr Adolesc Med. 2001;155(7):796–799. doi: 10.1001/archpedi.155.7.796. [DOI] [PubMed] [Google Scholar]
- 33.Fayyaz J. Bronchitis. Medscape. Pulmonology Web site. https://emedicine.medscape.com/article/297108-overview - a4. Published March 19, 2018. Accessed 17 March 2019.
- 34.Bent S., Saint S., Vittinghoff E., Grady D. Antibiotics in acute bronchitis: a meta-analysis. Am J Med. 1999;107(1):62–67. doi: 10.1016/S0002-9343(99)00167-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Smucny J.J., Becker L.A., Glazier R.H., McIsaac W. Are antibiotics effective treatment for acute bronchitis? A meta-analysis. J Fam Pract. 1998;47(6):453–460. [PubMed] [Google Scholar]
- 36.Singh M., Koyfman A. Are antibiotics effective in the treatment of acute bronchitis? Ann Emerg Med. 2015;65(5):566–567. doi: 10.1016/j.annemergmed.2014.11.018. [DOI] [PubMed] [Google Scholar]
- 37.Lapraz J.-C., de Clermont Tonnerre M.-L. Odile Jacob; Paris: 2012. La Médecine Personnalisée: Retrouver et Garder la Santé. [Google Scholar]
- 38.Baraniuk J.N., Ali M., Yuta A., Fang S.Y., Naranch K. Hypertonic saline nasal provocation stimulates nociceptive nerves, substance P release, and glandular mucous exocytosis in normal humans. Am J Respir Crit Care Med. 1999;160(2):655–662. doi: 10.1164/ajrccm.160.2.9805081. [DOI] [PubMed] [Google Scholar]