

Abstract
Systemic sclerosis can affect multiple internal organs, including the liver and lungs. Nintedanib, an antifibrotic approved for treatment of interstitial lung disease associated with systemic sclerosis, may have activity outside of the lungs. This study explored the effect of preventive and therapeutic nintedanib treatment in a 3-week carbon tetrachloride (CCL4)-induced (500 mg/kg/day twice weekly for 3 weeks) model of hepatic inflammation and fibrosis in C57Bl/6 mice (aged 8 weeks, n = 5 per group). Mice also received nintedanib (30 or 60 mg/kg/day) either each day for 21 days (preventive treatment) or from day 7 or day 14 (therapeutic treatment). Preventive nintedanib treatment at both doses significantly reduced CCL4-induced increases in myeloperoxidase (p < 0.01), hepatic collagen (p < 0.001), and interleukin (IL)-6 (p < 0.01) in the liver. Nintedanib also significantly reduced hepatic necrosis (p < 0.01 and p < 0.05), inflammation (p < 0.001 and p < 0.05), fibrosis (p < 0.001 and p < 0.05) and IL-1β (p < 0.05 and p < 0.001) at both 30 and 60 mg/kg/day, respectively. Therapeutic treatment with nintedanib at 30 and 60 mg/kg/day significantly reduced CCL4-induced serum alanine aminotransferase from day 7 (p < 0.05 and p < 0.001) and day 14 (p < 0.01 and p < 0.05), respectively. Increases in tissue inhibitor of metalloproteinase-1 were significantly reduced by nintedanib at 60 mg/kg/day from day 7 only (p < 0.001), and nintedanib completely blocked elevation of IL-6 and IL-1β levels regardless of dose or start of treatment (p < 0.05–p < 0.001). In both the preventive and therapeutic treatment schedules of the study, nintedanib treatment was beneficial in attenuating CCL4-induced pathology and reducing hepatic injury, inflammation, and fibrosis, demonstrating that nintedanib has antifibrotic and anti-inflammatory activity outside of the lungs.
1. Introduction
Nintedanib is a small-molecule tyrosine kinase inhibitor that targets the receptors of certain fibrosis-related kinases, including PDGF, FGF, VEGF, and transforming growth factor-beta (TGFβ) [1, 2]. Nintedanib also inhibits tyrosine kinases of the Src family such as Src, Lck, and Lyn and CSF1R that are involved in inflammation, proliferation, and immunological activation [2].
Systemic sclerosis (SSc) is a chronic disease characterised by endothelial dysfunction, resulting in alterations of the microvasculature, immune dysregulation, fibroblast dysfunction, and subsequent fibrosis [3]. Due to the heterogeneity of the disease, SSc remains a major clinical challenge for both physicians and patients [4]. The clinical course is variable, but SSc can affect multiple internal organs, particularly early in the disease, including the lungs, liver, kidneys, and heart [5, 6].
Nintedanib is an antifibrotic treatment currently approved in the United States, Canada, and Japan to slow the rate of decline in pulmonary function in adults with interstitial lung disease (ILD) associated with SSc (SSc-ILD) and in many countries for idiopathic pulmonary fibrosis (IPF). The INPULSIS [7] and TOMORROW [8] trials demonstrated the beneficial effects of nintedanib in patients with IPF. A pooled analysis of data from both trials showed that nintedanib was associated with a reduction in the annual rate of decline in forced vital capacity (FVC), fewer acute exacerbations, and the preservation of health-related quality of life [9].
Although the clinical course of SSc-ILD can vary, many patients experience disease progression with a decline in FVC associated with death [10, 11]. In the SENSCIS trial, nintedanib reduced the annual rate of decline in FVC compared with placebo [12]. The INBUILD trial evaluated nintedanib in patients with ILDs that have a progressive fibrosing phenotype; a subset of patients in the study have ILD associated with a connective tissue disease (CTD), e.g., rheumatoid arthritis (RA). Nintedanib reduced the annual rate of decline in FVC in the overall population, as well as in subgroups of patients with usual interstitial pneumonia-like or other fibrotic patterns [13]. Nintedanib has been well tolerated, with an acceptable safety profile and with diarrhoea the most common adverse event [7, 8, 12].
In addition to being associated with pulmonary manifestations, CTDs may also have an effect on the liver, typically as biochemical changes with a cholestatic or hepatocellular pattern. In rare cases, patients with CTDs may develop progressive liver disease, including liver fibrosis [14]. Given that multiple organs can be affected in patients with CTD, as well as the known antifibrotic and anti-inflammatory action of nintedanib, we planned to explore what effect nintedanib might have on liver injury.
Hepatic injury by carbon tetrachloride (CCL4) or ethanol causes inflammation, steatosis, and fibrosis that is toll-like receptor (TLR)4 and TGFβ-signalling dependent [1] and models human liver cirrhosis. Nintedanib, which reduces TGFβ and inflammatory mediators, may therefore have antifibrotic efficacy outside its known activity in the lungs. A previous preclinical acute study has shown antifibrotic effects of nintedanib in a 4-day CCL4 model of liver injury and fibrosis [15].
This study aimed to investigate whether nintedanib has antifibrotic activity outside of the lungs. The current study was undertaken to explore the effect of preventive and therapeutic nintedanib treatment in a 3-week CCL4-induced animal model of liver inflammation and fibrosis.
2. Materials and Methods
2.1. CCL4-Induced Model of Liver Fibrosis
We used a CCL4-induced model of hepatic inflammation and fibrosis in C57Bl/6 mice (Janvier, Le Genest-Saint-Isle, France). Mice were aged 8 weeks and caged in groups of five with ad libitum access to food and water. Animals received intraperitoneal CCL4 (Sigma-Aldrich, St. Louis, Missouri, United States) at 500 mg/kg/day twice weekly for 3 weeks to induce hepatic injury, inflammation, and fibrosis. Hepatic fibrosis was analysed at day 21. This study was approved by the regional ethics committee (CL2007-021).
2.2. Study Design
The study included two parts: a preventive and a therapeutic protocol. In the preventive phase, nintedanib treatment started simultaneously with CCL4 injections from day 0 to evaluate the effect of nintedanib in preventing hepatic injury. In the therapeutic phase, drug treatment was started on day 7 or day 14 of CCL4 injections to evaluate the effect of nintedanib in treating already established hepatic injury and fibrosis.
2.3. Treatment Protocols
Nintedanib 30 and 60 mg/kg/day (provided by Boehringer Ingelheim Pharma GmbH & Co. KG) was administered once daily by oral gavage. Administration volume was 10 mL/kg body weight. In the preventive protocol (Figure 1), there were four treatment groups (n = 10 per group): control (corn oil); CCL4 and oral vehicle; CCL4 and nintedanib 30 mg/kg/day; and CCL4 and nintedanib 60 mg/kg/day. In the therapeutic protocol, there were six treatment groups (n = 10 per group): control (corn oil); CCL4 and oral vehicle; CCL4 and nintedanib at 30 mg/kg/day starting at day 7; CCL4 and nintedanib 60 mg/kg/day starting at day 7; CCL4 and nintedanib at 30 mg/kg/day starting at day 14; and CCL4 and nintedanib 60 mg/kg/day starting at day 14.
Figure 1.
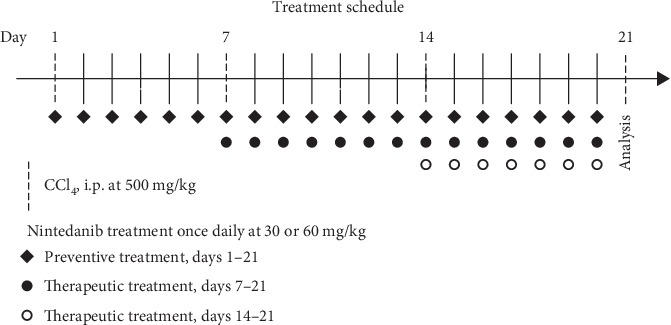
Treatment schedule in a mouse model of liver fibrosis. During the preventive phase, drug treatment started simultaneously with CCL4 injections from day 0. In the therapeutic phase, drug treatment was administered on day 7 or day 14 of CCL4 injections. Mice received nintedanib 30 or 60 mg/kg/day once daily. CCL4: carbon tetrachloride; i.p.: intraperitoneal.
2.4. Analyses
Body weight and clinical signs were recorded daily. All other analyses were conducted on day 21. Mice were euthanised at day 21 of the study, and the macroscopic analysis of the liver and liver weight changes was recorded postmortem. Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were determined in serum. Left liver lobes were homogenised to determine myeloperoxidase (MPO) activity, total liver collagen concentration by Sircol™ assay, interleukin (IL)-1β, IL-6, tumour necrosis factor-alpha (TNFα), and TGFβ by enzyme-linked immunosorbent assay. Right liver lobes were fixed for histology (haematoxylin and eosin and Sirius Red F 3B staining) for semiquantitative assessment of liver necrosis, inflammatory cell infiltration, and fibrosis on a scale of 0–5 (0 = least severe and 5 = most severe). Details of the methods can be found in Seki et al. [1] and Lisbonne et al. [16].
All data are presented as mean ± standard error of the mean. Statistical differences between groups were analysed by one-way analysis of variance with subsequent Dunnett's multiple comparison test for all parametric data and Kruskal–Wallis test for nonparametric data (GraphPad Prism 5.04). Statistical significance was accepted at p < 0.05. All groups were tested against CCL4-treated positive control animals.
3. Results
3.1. Preventive Treatment
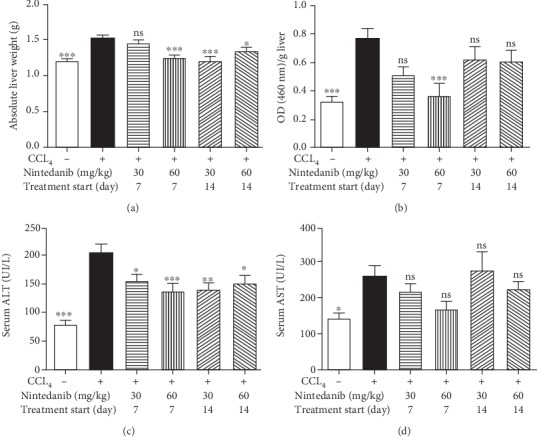
Nintedanib treatment resulted in a dose-dependent weak trend towards reduced body weight (< 5% at 60 mg/kg/day) compared with control or CCL4-only treated animals, with no statistical difference at day 21 (data not shown). Nintedanib had no effect on CCL4-induced liver weight gain (Figure 2(a)), and no other alterations of major organs were observed. Neutrophil recruitment into the liver was assessed by MPO activity determined in liver homogenate (Figure 2(b)). Nintedanib treatment with either 30 or 60 mg/kg/day significantly reduced MPO activity (p < 0.01). In mice treated with nintedanib, there was a significant reduction of CCL4-induced increase in ALT at 30 and 60 mg/kg/day (p < 0.0001) and AST serum levels at 60 mg/kg/day (p < 0.05) (Figures 2(c) and 2(d)).
Figure 2.
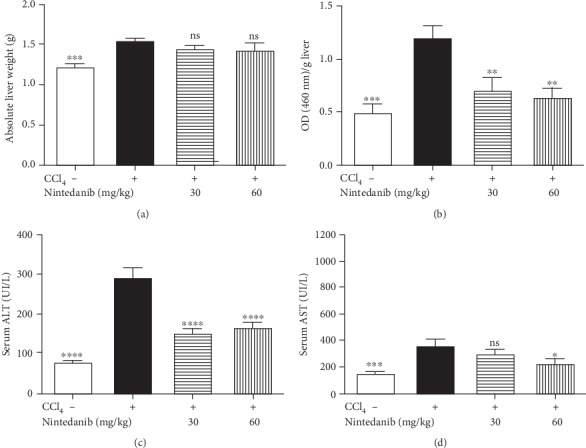
Effect of nintedanib on (a) liver weight and concentration in liver tissue of (b) myeloperoxidase (optical density), (c) serum alanine aminotransferase, and (d) serum aspartate aminotransferase during the preventive phase. Data are presented as mean ± standard error of the mean; n = 5 per group. Statistical significance is shown as: ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001, ∗∗∗∗p < 0.0001. ALT: alanine aminotransferase; ASP: aspartate aminotransferase; CCL4: carbon tetrachloride; ns: not significant.
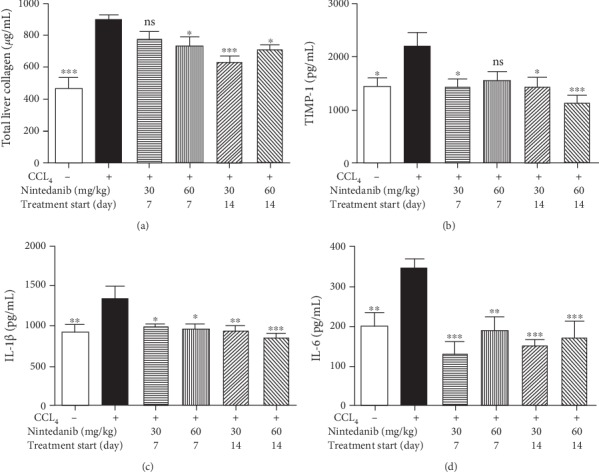
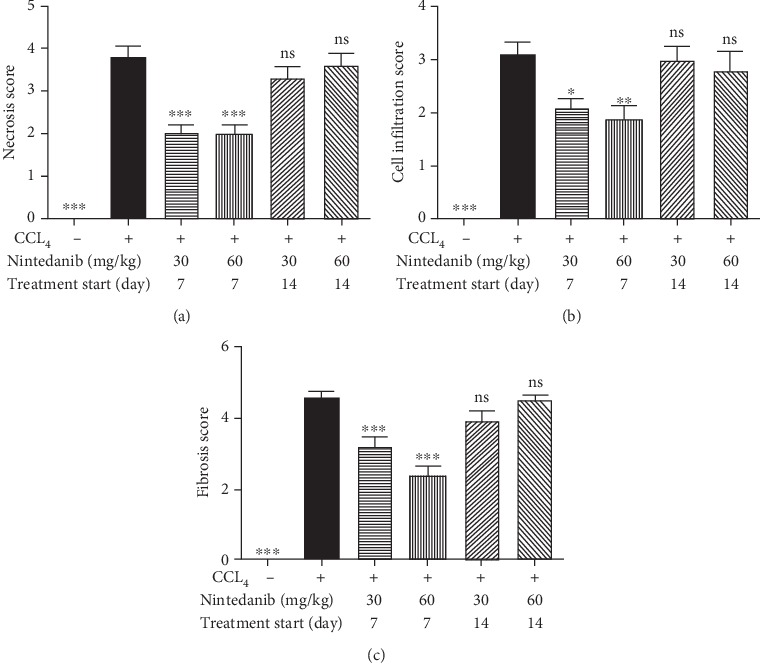
Nintedanib at both doses blocked CCL4-induced increase in hepatic collagen (p < 0.001) (Figure 3(a)). Nintedanib reduced tissue inhibitor of metalloproteinase (TIMP)-1, IL-1β, and IL-6 in the liver (Figures 3(b)–3(d)). This reduction was significant at both doses for IL-6 (p < 0.01) and for IL-1β (30 mg/kg/day; p < 0.05 and 60 mg/kg/day; p < 0.001). TNFα, TGFβ, and C-X-C motive ligand-1 (KC) levels were not affected by nintedanib administration (data not shown). Nintedanib significantly reduced liver necrosis (p < 0.01 and p < 0.05), infiltration of inflammatory cells (p < 0.001 and p < 0.01), and fibrosis (p < 0.001 and p < 0.05) at both 30 and 60 mg/kg/day, respectively, as assessed by semiquantitative scoring of histology samples (Figures 4 and 5).
Figure 3.
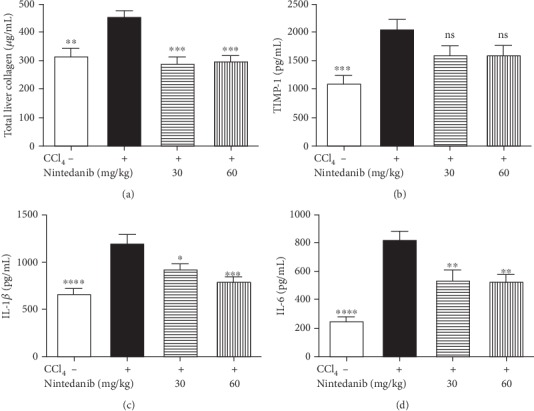
Effect of nintedanib on (a) total liver collagen and concentration in liver tissue of (b) TIMP-1, (c) IL-1β, and (d) IL-6 during the preventive phase. Data are presented as mean ± standard error of the mean; n = 5 per group. Statistical significance is shown as ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001, ∗∗∗∗p < 0.0001. CCL4: carbon tetrachloride; IL-1β: interleukin-1β; IL-6: interleukin-6; ns: not significant; TIMP-1: tissue inhibitor of metalloproteinase.
Figure 4.
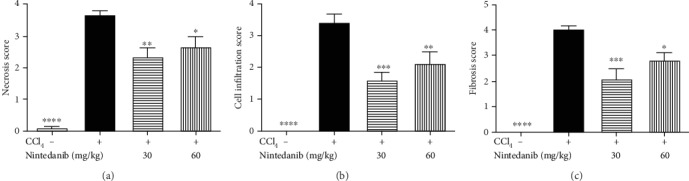
Effect of nintedanib on (a) liver necrosis, (b) liver inflammatory cell infiltration, and (c) liver fibrosis score during the preventive phase. Data are presented as mean ± standard error of the mean; n = 5 per group. Statistical significance is shown as ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001, ∗∗∗∗p < 0.0001. CCL4: carbon tetrachloride; ns: not significant.
Figure 5.
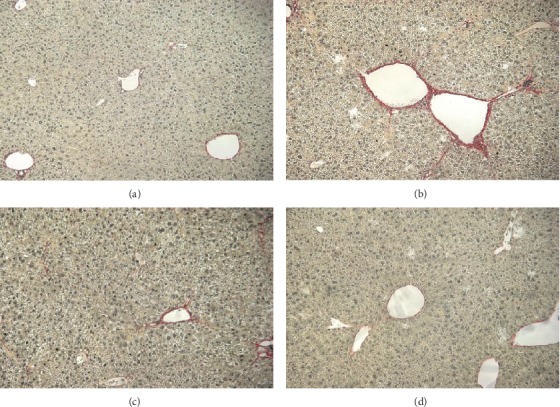
Representative histology slides stained with Sirius Red at 10-fold magnification during the preventive phase of (a) control without CCL4 stimulation, (b) control with CCL4 stimulation, (c) CCL4 and nintedanib at 30 mg/kg/day, (d) CCL4 and nintedanib 60 mg/kg/day. CCL4: carbon tetrachloride.
3.2. Therapeutic Treatment
Nintedanib treatment resulted in a weak trend towards reduced body weight (< 5% at 60 mg/kg/day) compared with control or CCL4-only treated animals from both days 7 and 14 (data not shown). Macroscopic examination of the major organs at necropsy on day 21 did not reveal any major organ alterations. Nintedanib significantly reduced CCL4-induced liver weight gain at both 30 mg/kg/day (from day 14; p < 0.001) and 60 mg/kg/day (from day 7 or 14; p < 0.001 and p < 0.05, respectively) (Figure 6(a)). There was a dose-dependent decrease in MPO if treatment started on day 7 only, reaching significance with 60 mg/kg/day (p < 0.001) (Figure 6(b)). ALT was significantly reduced following treatment with both doses of nintedanib, with treatment starting on either day 7 (p < 0.05 and p < 0.001) or 14 (p < 0.01 and p < 0.05) (Figure 6(c)). There was a nonsignificant trend towards dose-dependent reduction in AST (Figure 6(d)).
Figure 6.
Effect of nintedanib on (a) liver weight and concentration in liver tissue of (b) myeloperoxidase, (c) alanine aminotransferase, and (d) aspartate aminotransferase during the preventive phase. Data are presented as mean ± standard error of the mean; n = 5 per group. Statistical significance is shown as ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001. ALT: alanine aminotransferase; ASP: aspartate aminotransferase; CCL4: carbon tetrachloride; ns: not significant.
Nintedanib significantly reduced the total liver collagen concentration at 30 mg/kg/day (p < 0.001, from day 14) and at 60 mg/kg/day (from day 7 or 14, p < 0.05) (Figure 7(a)). Increases in TIMP-1 were significantly reduced by nintedanib 30 mg/kg/day from days 7 and 14 (p < 0.05), and at 60 mg/kg/day from day 14 only (p < 0.001) (Figure 7(b)). Nintedanib completely blocked elevation of IL-6 and IL-1β levels regardless of dose or start of treatment (p < 0.05–p < 0.001) (Figures 7(c) and 7(d)). TNFα, TGFβ, and KC levels were not affected by nintedanib administration (data not shown). Nintedanib treatment at both doses significantly reduced liver necrosis, inflammation, and fibrosis, as assessed by semiquantitative histology, from day 7 only (Figures 8(a)–8(c)). The reduction in liver fibrosis appeared to be greater at 60 mg/kg/day than at 30 mg/kg/day (Figure 8(c)).
Figure 7.
Effect of nintedanib on (a) total liver collagen and concentration in liver tissue of (b) TIMP-1, (c) IL-1β, and (d) IL-6 during the therapeutic phase. Data are presented as mean ± standard error of the mean; n = 5 per group. Statistical significance is shown as ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001. CCL4: carbon tetrachloride; IL-1β: interleukin-1β; IL-6: interleukin-6; ns: not significant; TIMP-1: tissue inhibitor of metalloproteinase.
Figure 8.
Effect of nintedanib on (a) liver necrosis, (b) liver inflammatory cell infiltration, and (c) liver fibrosis score during the therapeutic phase. Data are presented as mean ± standard error of the mean; n = 5 per group. Statistical significance is shown as ∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001. CCL4: carbon tetrachloride; ns: not significant.
4. Discussion
In both the preventive and therapeutic treatment schedules of the study, nintedanib treatment attenuated CCL4-induced pathology and reduced hepatic injury, inflammation, and fibrosis.
In the preventive setting, there was a trend towards reduced ALT and AST in serum. Nintedanib treatment diminished neutrophil recruitment and reduced biochemical and inflammatory parameters suggestive of a beneficial effect on liver fibrosis. Both doses of nintedanib had similar preventive activities on most parameters explored but with no dose dependency.
Nintedanib treatment starting at day 7 was, in general, more effective than treatment starting at day 14; liver necrosis, inflammatory cell infiltration, and liver fibrosis, when assessed histologically, were only significantly reduced if treatment was started on day 7. This may have been because the pathology had already progressed too far or because treatment duration was too short to be effective when starting at day 14 (only 7 days of treatment). However, this study was not designed to describe statistically significant differences between treatments started at different time points.
ALT/AST results were different from those seen in clinical trials, where elevated ALT/AST levels at least three times the upper limit of the normal range were observed in 4.9–13.0% of patients with lung fibrosis treated with nintedanib compared with placebo (up to 3.6%), depending on the study [7, 8, 12, 13]. In our mouse model, nintedanib did not increase ALT or AST serum levels. It may be that only patients with already impaired liver function before the start of clinical trials are prone to the increases in ALT and AST following nintedanib treatment.
Similar to our findings, another preclinical model of CCL4-induced liver fibrosis found that nintedanib significantly attenuated collagen accumulation and hepatic stellate cell activation, inhibiting intrahepatic inflammation and angiogenesis [15]. In a choline-deficient, L-amino acid-defined, high-fat diet-fed mouse model of nonalcoholic steatohepatitis, nintedanib also showed anti-inflammatory and antifibrotic effects [17].
Biochemical changes in the liver are common in patients with CTD. In rare cases, patients with CTDs may develop progressive liver disease, including liver fibrosis [14]. Liver involvement of this type is typically attributed to (coexisting) primary liver diseases (e.g., fatty liver disease, viral hepatitis, primary biliary cirrhosis, autoimmune hepatitis, and drug-related liver toxicity), rather than the CTD itself. Drug-induced liver injury is frequent with certain CTDs, particularly with the use of methotrexate in patients with RA, and may lead to progressive fibrosis and cirrhosis [18]. The results of the current study highlight the potential of nintedanib to reduce liver necrosis, inflammation, and fibrosis. As such, using nintedanib for the treatment of ILD in patients with CTDs, including SSc-ILD, may have antifibrotic effects in organs other than the lungs.
Nintedanib reduced and blocked CCL4-induced elevated hepatic IL-6 in both the preventive and therapeutic phases of the study. Similar results were obtained in a mouse model of silica-induced lung fibrosis, where nintedanib reduced the IL-6 concentration in lung tissue [19]. Anti-IL-6 antibody therapy is used to treat RA-ILD, although evidence is controversial, with some studies showing beneficial effects and others finding ILD occurrence or exacerbation following tocilizumab treatment [20, 21]. Interestingly, imatinib mesylate, another kinase inhibitor that has shown antifibrotic effects in the liver in preclinical studies, has been shown to increase serum IL-6 levels in conjunction with liver regeneration [22]. The current study shows a potential systemic effect of nintedanib on IL-6, indicating that further investigation of nintedanib in RA-ILD may be warranted.
However, there are limitations with this study, including those normally associated with animal models of disease. The CCL4 model is also more a model of acute liver injury leading to fibrosis and does not directly correspond to the clinical situation where patients normally present with chronic fibrosis [15]. However, it provides a good indication (along with other animal models of fibrosis discussed above) that nintedanib has antifibrotic activity outside of the lungs.
5. Conclusions
In conclusion, nintedanib demonstrated antifibrotic and anti-inflammatory activity, showing therapeutic potential in this experimental mouse model of CCL4-induced hepatic fibrosis.
Acknowledgments
The authors would like to thank Isabelle Maillet of Immunologie Moléculaire, CNRS and University Orléans for her technical contribution to the study. The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE). The authors received no direct compensation related to the development of the manuscript. Writing, editorial support, and formatting assistance were provided by Helen Keyworth, PhD, of Nucleus Global, which was contracted and funded by Boehringer Ingelheim International GmbH (BI). BI was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Data Availability
To ensure independent interpretation of clinical study results, Boehringer Ingelheim grants all external authors access to all relevant material, including participant-level clinical study data, and relevant material as needed by them to fulfil their role and obligations as authors under the International Committee of Medical Journal Editors criteria. Furthermore, clinical study documents (e.g. study report, study protocol, statistical analysis plan) and participant clinical study data are available to be shared after publication of the primary manuscript in a peer-reviewed journal, and if regulatory activities are complete and other criteria are met per the BI Policy on Transparency and Publication of Clinical Study Data: https://trials.boehringer-ingelheim.com/transparency_policy.html. Prior to providing access, documents will be examined, and, if necessary, redacted and the data will be de-identified, to protect the personal data of study participants and personnel, and to respect the boundaries of the informed consent of the study participants. Clinical Study Reports and Related Clinical Documents can be requested via this link: https://trials.boehringer-ingelheim.com/trial_results/clinical_submission_documents.html. All such requests will be governed by a Document Sharing Agreement. Bona fide, qualified scientific and medical researchers may request access to de-identified, analysable participant clinical study data with corresponding documentation describing the structure and content of the data sets. Upon approval, and governed by a Data Sharing Agreement, data are shared in a secured data-access system for a limited period of 1 year, which may be extended upon request. Researchers should use https://clinicalstudydatarequest.com to request access to study data.
Conflicts of Interest
Lutz Wollin is an employee of Boehringer Ingelheim Pharma GmbH & Co. KG, who developed and market nintedanib. Dieudonnée Togbe is an employee of ArtImmune.
References
- 1.Seki E., de Minicis S., Österreicher C. H., et al. TLR4 enhances TGF-β signaling and hepatic fibrosis. Nature Medicine. 2007;13(11):1324–1332. doi: 10.1038/nm1663. [DOI] [PubMed] [Google Scholar]
- 2.Hilberg F., Roth G. J., Krssak M., et al. BIBF 1120: triple angiokinase inhibitor with sustained receptor blockade and good antitumor efficacy. Cancer Research. 2008;68(12):4774–4782. doi: 10.1158/0008-5472.CAN-07-6307. [DOI] [PubMed] [Google Scholar]
- 3.Varga J., Trojanowska M., Kuwana M. Pathogenesis of systemic sclerosis: recent insights of molecular and cellular mechanisms and therapeutic opportunities. Journal of Scleroderma and Related Disorders. 2017;2(3):137–152. doi: 10.5301/jsrd.5000249. [DOI] [Google Scholar]
- 4.Denton C. P., Khanna D. Systemic sclerosis. Lancet. 2017;390(10103):1685–1699. doi: 10.1016/S0140-6736(17)30933-9. [DOI] [PubMed] [Google Scholar]
- 5.Jaeger V. K., Wirz E. G., Allanore Y., et al. Incidences and risk factors of organ manifestations in the early course of systemic sclerosis: a longitudinal EUSTAR study. PLoS One. 2016;11(10, article e0163894) doi: 10.1371/journal.pone.0163894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Frech T. M., Mar D. Gastrointestinal and hepatic disease in systemic sclerosis. Rheumatic Diseases Clinics of North America. 2018;44(1):15–28. doi: 10.1016/j.rdc.2017.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Richeldi L., du Bois R. M., Raghu G., et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. The New England Journal of Medicine. 2014;370(22):2071–2082. doi: 10.1056/NEJMoa1402584. [DOI] [PubMed] [Google Scholar]
- 8.Richeldi L., Costabel U., Selman M., et al. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. The New England Journal of Medicine. 2011;365(12):1079–1087. doi: 10.1056/NEJMoa1103690. [DOI] [PubMed] [Google Scholar]
- 9.Richeldi L., Cottin V., du Bois R. M., et al. Nintedanib in patients with idiopathic pulmonary fibrosis: Combined evidence from the TOMORROW and INPULSIS® trials. Respiratory Medicine. 2016;113:74–79. doi: 10.1016/j.rmed.2016.02.001. [DOI] [PubMed] [Google Scholar]
- 10.Goh N. S., Desai S. R., Veeraraghavan S., et al. Interstitial lung disease in systemic sclerosis: a simple staging system. American Journal of Respiratory and Critical Care Medicine. 2008;177(11):1248–1254. doi: 10.1164/rccm.200706-877OC. [DOI] [PubMed] [Google Scholar]
- 11.Goh N. S., Hoyles R. K., Denton C. P., et al. Short-term pulmonary function trends are predictive of mortality in interstitial lung disease associated with systemic sclerosis. Arthritis & Rhematology. 2017;69(8):1670–1678. doi: 10.1002/art.40130. [DOI] [PubMed] [Google Scholar]
- 12.Distler O., Highland K. B., Gahlemann M., et al. Nintedanib for systemic sclerosis-associated interstitial lung disease. The New England Journal of Medicine. 2019;380(26):2518–2528. doi: 10.1056/NEJMoa1903076. [DOI] [PubMed] [Google Scholar]
- 13.Flaherty K. R., Wells A. U., Cottin V., et al. Nintedanib in progressive fibrosing interstitial lung diseases. The New England Journal of Medicine. 2019;381(18):1718–1727. doi: 10.1056/NEJMoa1908681. [DOI] [PubMed] [Google Scholar]
- 14.Chentoufi A. A., Serov Y. A., Alazmi M., Baba K. Immune components of liver damage associated with connective tissue diseases. Journal of Clinical and Translational Hepatology. 2014;2(1):37–44. doi: 10.14218/JCTH.2014.00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ozturk Akcora B., Storm G., Prakash J., Bansal R. Tyrosine kinase inhibitor BIBF1120 ameliorates inflammation, angiogenesis and fibrosis in CCl4-induced liver fibrogenesis mouse model. Scientific Reports. 2017;7:p. 44545. doi: 10.1038/srep44545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lisbonne M., L'Helgoualc'h A., Nauwelaers G., et al. Invariant natural killer T-cell-deficient mice display increased CCl4-induced hepatitis associated with CXCL1 over-expression and neutrophil infiltration. European Journal of Immunology. 2011;41(6):1720–1732. doi: 10.1002/eji.201041006. [DOI] [PubMed] [Google Scholar]
- 17.Susutlertpanya W., Wakuda H., Otani N., et al. Histological evaluation of nintedanib in non-alcoholic steatohepatitis mice. Life Sciences. 2019;228:251–257. doi: 10.1016/j.lfs.2019.05.014. [DOI] [PubMed] [Google Scholar]
- 18.Conway R., Carey J. J. Risk of liver disease in methotrexate treated patients. World Journal of Hepatology. 2017;9(26):1092–1100. doi: 10.4254/wjh.v9.i26.1092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wollin L., Maillet I., Quesniaux V., Holweg A., Ryffel B. Antifibrotic and anti-inflammatory activity of the tyrosine kinase inhibitor nintedanib in experimental models of lung fibrosis. The Journal of Pharmacology and Experimental Therapeutics. 2014;349(2):209–220. doi: 10.1124/jpet.113.208223. [DOI] [PubMed] [Google Scholar]
- 20.Shaw M., Collins B. F., Ho L. A., Raghu G. Rheumatoid arthritis-associated lung disease. European Respiratory Review. 2015;24(135):1–16. doi: 10.1183/09059180.00008014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rubbert-Roth A., Furst D. E., Nebesky J. M., Jin A., Berber E. A review of recent advances using tocilizumab in the treatment of rheumatic diseases. Rheumatology and Therapy. 2018;5(1):21–42. doi: 10.1007/s40744-018-0102-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kuo C. S., Young L. R. Interstitial lung disease in children. Current Opinion in Pediatrics. 2014;26(3):320–327. doi: 10.1097/MOP.0000000000000094. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
To ensure independent interpretation of clinical study results, Boehringer Ingelheim grants all external authors access to all relevant material, including participant-level clinical study data, and relevant material as needed by them to fulfil their role and obligations as authors under the International Committee of Medical Journal Editors criteria. Furthermore, clinical study documents (e.g. study report, study protocol, statistical analysis plan) and participant clinical study data are available to be shared after publication of the primary manuscript in a peer-reviewed journal, and if regulatory activities are complete and other criteria are met per the BI Policy on Transparency and Publication of Clinical Study Data: https://trials.boehringer-ingelheim.com/transparency_policy.html. Prior to providing access, documents will be examined, and, if necessary, redacted and the data will be de-identified, to protect the personal data of study participants and personnel, and to respect the boundaries of the informed consent of the study participants. Clinical Study Reports and Related Clinical Documents can be requested via this link: https://trials.boehringer-ingelheim.com/trial_results/clinical_submission_documents.html. All such requests will be governed by a Document Sharing Agreement. Bona fide, qualified scientific and medical researchers may request access to de-identified, analysable participant clinical study data with corresponding documentation describing the structure and content of the data sets. Upon approval, and governed by a Data Sharing Agreement, data are shared in a secured data-access system for a limited period of 1 year, which may be extended upon request. Researchers should use https://clinicalstudydatarequest.com to request access to study data.