

Acute pharyngitis is one of the most common illnesses for which children in the United States visit primary care providers; pediatricians make the diagnosis of acute pharyngitis, acute tonsillitis, or “strep throat” more than 7 million times annually.1
A partial list of the more common microorganisms that can cause acute pharyngitis is presented in Table 27-1 . Most cases in children and adolescents are caused by viruses and are benign and self-limited. Group A β-hemolytic streptococcus (GAS, Streptococcus pyogenes) is the most important bacterial cause. Strategies for the diagnosis and treatment of pharyngitis in children and adolescents are directed at distinguishing the large group of patients with viral pharyngitis that would not benefit from antimicrobial therapy from the significantly smaller group of patients with GAS pharyngitis for whom antimicrobial therapy would be beneficial. Making this distinction is extremely important in attempting to minimize the unnecessary use of antibiotics in children and adolescents.
TABLE 27-1.
Etiology of Acute Pharyngitis
| Etiologic Agent | Associated Disorder(s) or Clinical Findings(s) |
|---|---|
| Bacterial | |
| Streptococci | |
| Group A | Scarlet fever |
| Groups C and G | |
| Mixed anaerobes | Vincent angina |
| Neisseria gonorrhoeae | |
| Corynebacterium diphtheriae | Diphtheria |
| Arcanobacterium haemolyticum | Scarlatiniform rash |
| Yersinia enterocolitica | Enterocolitis |
| Yersinia pestis | Plague |
| Francisella tularensis | Tularemia |
| Fusobacterium necrophorum | Lemierre syndrome (jugular vein septic thrombophlebitis) |
| Viral | |
| Rhinovirus | Common cold |
| Coronavirus | Common cold |
| Adenovirus | Pharyngoconjunctival fever; acute respiratory disease |
| Herpes simplex virus types 1 and 2 | Gingivostomatitis |
| Parainfluenza virus | Common cold; croup |
| Coxsackievirus A | Herpangina; hand, foot, and mouth disease |
| Epstein–Barr virus | Infectious mononucleosis |
| Cytomegalovirus | Cytomegalovirus mononucleosis |
| Human immunodeficiency virus (HIV) | Primary HIV infection |
| Mycoplasmal | |
| Mycoplasma pneumoniae | Acute respiratory disease; pneumonia |
| Chlamydial | |
| Chlamydophila psittaci | Acute respiratory disease; pneumonia |
| Chlamydophila pneumoniae | Pneumonia |
| Non-Infectious Etiologies | |
| Gastroesophogeal reflux disease | Heartburn |
| Laryngopharyngeal reflux | Cough, hoarseness |
| PFAPA syndrome | Periodic fever, aphthous ulcers, adenitis |
| Allergic pharyngitis | Scratchy serration, post-nasal drip, hoarseness |
HIV, human immunodeficiency virus.
Modified from Bisno AL, Gerber MA, Gwaltney JM, et al. Practice guideline for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis 2002;35:113–125, with permission.
Etiology
Viruses are the most common cause of acute pharyngitis in children and adolescents. Respiratory viruses (e.g., influenza virus, parainfluenza virus, rhinovirus, coronavirus, adenovirus, and respiratory syncytial virus), enteroviruses (including coxsackievirus and echovirus), herpes simplex virus (HSV), and Epstein–Barr virus (EBV) are frequent causes of pharyngitis. EBV pharyngitis often is accompanied by other clinical findings of infectious mononucleosis (e.g., generalized lymphadenopathy, splenomegaly), and can be exudative and indistinguishable from GAS pharyngitis. HSV pharyngitis often is associated with stomatitis in children, and tends to affect the entire oral mucosa including the gingival, buccal mucosa, and tongue. Enteroviral pharyngitis can be an isolated finding (herpangina), or part of the spectrum of hand-foot-and-mouth disease, and has a typical appearance. Systemic infections with other viruses (e.g., cytomegalovirus, rubella virus, and measles virus) also can include pharyngitis.
GAS is the most common bacterial cause of acute pharyngitis, accounting for 15% to 30% of the cases in children. Other causative bacteria include groups C and G β-hemolytic streptococci (GCS, GGS). Arcanobacterium haemolyticum is a rare cause in adolescents and Neisseria gonorrhoeae can cause acute pharyngitis in sexually active adolescents. Other bacteria such as Francisella tularensis, Yersinia enterocolitica, and Corynebacterium diphtheriae as well as mixed infections with anaerobic bacteria (e.g., Vincent angina) are rare causes. Chlamydophila pneumoniae and Mycoplasma pneumoniae have been implicated rarely, particularly in adults. Although other bacteria such as Staphylococcus aureus, Haemophilus influenzae, and Streptococcus pneumoniae frequently are isolated from throat cultures of children and adolescents with acute pharyngitis, their etiologic role is not established. Fusobacterium necrophorum, the typical etiologic agent of Lemierre syndrome, also may cause uncomplicated pharyngitis.2 Non-infectious cases of recurrent or prolonged pharyngitis and sore throat include the periodic fever, adenitis, pharyngitis, and aphthous ulcers (PFAPA) syndrome, gastroesophageal reflux and/or laryngopharyngeal reflux, and allergic rhinitis.
Epidemiology
Most cases of acute pharyngitis occur during the colder months of the year when respiratory viruses are prevalent. Spread among family members in the home is a prominent feature of the epidemiology of most of these agents, with children being the major reservoir. GAS pharyngitis is primarily a disease of children 5 to 15 years of age, and, in temperate climates, prevalence is highest in winter and early spring. Enteroviral pharyngitis typically occurs in the summer and early fall.
Gonococcal pharyngitis occurs in sexually active adolescents and young adults. The usual route of infection is through orogenital sexual contact. Sexual abuse must be considered strongly when N. gonorrhoeae is isolated from the pharynx of a prepubertal child. Widespread immunization with diphtheria toxoid has made diphtheria a rare disease in the U.S., with <5 cases reported annually in recent years.
GCS and GGS express many of the same toxins as GAS, including streptolysins S and O, and GCS pharyngitis can have clinical features similar to GAS and can cause elevation of serum antistreptolysin-O (ASO) antibody.3 GCS is a relatively common cause of acute pharyngitis among college students and adults who seek urgent care.4, 5 Outbreaks of GCS pharyngitis related to consumption of contaminated food products (e.g., unpasteurized cow milk) have been reported in families and schools.6 Although there also are several well-documented foodborne outbreaks of GGS pharyngitis, the etiologic role of GGS in acute, endemic pharyngitis remains unclear. A community-wide outbreak of pharyngitis in children was described in which GGS was isolated from 25% of 222 consecutive children with acute pharyngitis seen in a private pediatric office; results of DNA fingerprinting suggested that 75% of isolates belonged to the same GGS clone.7
The role of GCS and GGS in acute pharyngitis may be underestimated. Laboratories may use bacitracin susceptibility to identify GAS; many GCS and GGS are bacitracin-resistant. Additionally, rapid antigen detection tests (RADTs) recognize the GAS cell wall carbohydrate, but are nonreactive with GCS or GGS.8
Clinical Manifestations
Group A Streptococcus
The presence of certain clinical and epidemiologic findings suggests GAS as the cause of an episode of acute pharyngitis (Box 27-1 ). Patients with GAS pharyngitis commonly present with sore throat (usually of sudden onset), severe pain on swallowing, and fever. Headache, nausea, vomiting, and abdominal pain also can be present. Examination typically reveals tonsillopharyngeal erythema with or without exudates, and tender, enlarged anterior cervical lymph nodes. Other findings can include a beefy, red, swollen uvula; petechiae on the palate; and a scarlatiniform rash. No finding is specific for GAS. Many patients with GAS pharyngitis exhibit signs and symptoms that are milder than a “classic” case of this illness. Some of these patients have bona fide GAS infection (i.e., have a rise in ASO antibodies), whereas others are merely colonized and have an intercurrent viral infection. GAS pharyngitis in infants is uncommon, and is difficult to differentiate from viral infections because nasopharyngitis, with purulent nasal discharge, and excoriated nares frequently accompany pharyngitis.
Box 27-1. Clinical and Epidemiologic Characteristics of Group A β-Hemolytic Streptococci (GAS) and Viral Pharyngitis.
Features Suggestive of Gas Etiology
- Sudden onset
- Sore throat
- Fever
- Scarlet fever rash
- Headache
- Nausea, vomiting, and abdominal pain
- Inflammation of pharynx and tonsils
- Patchy discrete exudates
- Tender, enlarged anterior cervical nodes
- Patient aged 5–15 years
- Presentation in winter or early spring
- History of exposure
Features Suggestive of Viral Etiology
- Conjunctivitis
- Coryza
- Cough
- Hoarseness
- Myalgia
- Diarrhea
- Characteristic exanthems
Modified from Bisno AL, Gerber MA, Gwaltney JM, et al. Practice guideline for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis 2002;35:113–125, with permission.
Scarlet fever is associated with a characteristic rash that is caused by a pyrogenic exotoxin (erythrogenic toxin)-producing GAS, and occurs in individuals who lack prior antitoxin antibodies. Although less common and less severe than in the past, the incidence of scarlet fever is cyclical, depending on the prevalence of toxin-producing strains of GAS and the immune status of the population. The modes of transmission, age distribution, and other epidemiologic features are otherwise similar to those of GAS pharyngitis.
The rash of scarlet fever appears within 24 to 48 hours of the onset of signs and symptoms and can be the first sign. The rash often begins around the neck and spreads over the trunk and extremities. It is a diffuse, finely papular (sandpaper-like), erythematous eruption producing bright red discoloration of the skin that blanches with pressure. Involvement often is more intense along the creases in the antecubital area, axillae, and groin, and petechiae along the creases can occur (Pastia lines). The face usually is spared, although the cheeks can be erythematous with pallor around the mouth (Figure 27-1 ). After 3 to 4 days, the rash begins to fade and is followed by fine desquamation, first on the face, progressing downward. Occasionally, sheet-like desquamation occurs around the fingernails periungually, the palms, and the soles. Pharyngeal findings are the same as with GAS pharyngitis. In addition, the tongue usually is coated and the papillae are swollen. With desquamation, the reddened papillae are prominent, giving the tongue a strawberry appearance.
Figure 27-1.

Child has group A streptococcal pharyngitis and scarlatiniform rash, with characteristic circumoral pallor.
(Courtesy of J.H. Brien©.)
Viruses
The presence of certain clinical findings (e.g., conjunctivitis, cough, hoarseness, coryza, anterior stomatitis, discrete ulcerative lesions, viral exanthema, myalgia, and diarrhea) suggests a virus rather than GAS as the cause of an episode of acute pharyngitis (see Box 27-1).
Adenovirus pharyngitis typically is associated with fever, erythema of the pharynx, enlarged tonsils with exudate, and enlarged cervical lymph nodes. Adenoviral pharyngitis can be associated with conjunctivitis, when illness is referred to as pharyngoconjunctival fever; pharyngitis can persist up to 7 days and conjunctivitis up to 14 days, when both resolve spontaneously. Outbreaks of pharyngoconjunctival fever have been associated with transmission in swimming pools; widespread epidemics and sporadic cases also occur.
Enteroviruses (coxsackievirus, echovirus, and enteroviruses) are associated with erythematous pharyngitis but tonsillar exudate and cervical lymphadenopathy are unusual. Fever can be prominent. Resolution usually occurs within a few days. Herpangina is a specific syndrome caused by coxsackieviruses A or B or echoviruses and is characterized by fever and painful, discrete, grey-white papulovesicular/ulcerative lesions on an erythematous base in the posterior oropharynx (Figure 27-2 ). Hand-foot-and-mouth disease is characterized by painful vesicles and ulcers throughout the oropharynx associated with vesicles on the palms, soles, and sometimes on the trunk or extremities. Enteroviral lesions usually resolve within 7 days.
Figure 27-2.

Child with posterior pharyngeal grey-white papulovesicular lesions characteristic of enteroviral herpangina.
(Courtesy of J.H. Brien©.)
Primary oral HSV infections usually occur in young children and typically produce acute gingivostomatitis associated with ulcerating vesicular lesions throughout the anterior mouth including the lips, sparing the posterior pharynx. HSV gingivostomatitis can last up to 2 weeks and often is associated with high fever. Pain can be intense and the poor oral intake can lead to dehydration. In adolescents and adults HSV also can cause mild pharyngitis that may or may not be associated with typical vesicular, ulcerating lesions.
EBV pharyngitis during infectious mononucleosis can be severe, with clinical findings identical to those of GAS pharyngitis (Figure 27-3A ). However, generalized lymphadenopathy and hepatosplenomegaly also can be present. Posterior cervical lymphadenopathy and presternal and periorbital edema are distinctive if present. Fever and pharyngitis typically last 1 to 3 weeks, whereas the lymphadenopathy and hepatosplenomegaly resolve over 3 to 6 weeks. Laboratory findings include the presence of atypical lymphocytosis (Figure 27-3B), heterophile antibodies, viremia (by PCR), and specific antibodies to EBV antigens. If amoxicillin has been given, an intense maculopapular rash is expected (Figure 27-3C).
Figure 27-3.

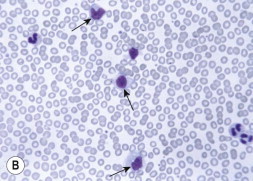

(A) Pharyngeal erythema and exudate of Epstein–Barr virus (EBV). (B) Peripheral blood smear showing atypical lymphocytes (arrows) in a patient with EBV mononucleosis. Note the abundant cytoplasm with vacuoles, and deformation of cell by surrounding cells. (C) Diffuse erythematous raised rash in adolescent with EBV mononucleosis who received amoxicillin; note predominance on trunk and coalescence.
(Courtesy of J.H. Brien©.)
Other Bacteria
A. haemolyticum pharyngitis can resemble GAS pharyngitis, including the presence of a scarlatiniform rash. Rarely, A. haemolyticum can produce a membranous pharyngitis that can be confused with diphtheria.
Pharyngeal diphtheria is characterized by a greyish brown pseudomembrane that can be limited to one or both tonsils or can extend widely to involve the nares, uvula, soft palate, pharynx, larynx, and tracheobronchial tree. Involvement of the tracheobronchial tree can lead to life-threatening respiratory obstruction. Soft-tissue edema and prominent cervical and submental lymphadenopathy can cause a bull-neck appearance.
Fusobacterium necrophorum may be a common cause of non-streptococcal pharyngitis, occurring in as many as 10% of adolescents and young adults with pharyngitis.9 F. necrophorum appears to cause typical signs of bacterial pharyngitis (high fever, odynophagia, lymphadenopathy, and exudative tonsillitis), and can cause concomitant bacteremia.10 The frequency of progression from tonsillitis to Lemierre syndrome is unknown.
Diagnosis
Distinguishing between GAS and viral pharyngitis is key to management in the U.S. Scoring systems that incorporate clinical and epidemiologic features attempt to predict the probability that the illness is caused by GAS.11, 12 Clinical scoring systems are helpful in identifying patients at such low risk of GAS infection that a throat culture or RADT usually is unnecessary. However, in a 2012 systematic review of 34 articles with individual symptoms and signs of pharyngitis assessed and 15 articles with data on prediction rules, no symptoms or signs individually or combined into prediction rules could be used to diagnose GAS pharyngitis with a probability of ≥85%.13 Adding to the complexity of diagnosis is the ability to distinguish between GAS pharyngitis and other bacterial pathogens such as GCS, which have very similar clinical manifestations.3 Therefore, recent guidelines from the Infectious Diseases Society of America (IDSA),14 as well as guidelines from the American Academy of Pediatrics (AAP)15 and the American Heart Association (AHA),16 indicate that microbiologic confirmation (either with a throat culture or RADT) is required for the diagnosis of GAS pharyngitis.
The decision to perform a microbiologic test on a child or adolescent with acute pharyngitis should be based on the clinical and epidemiologic characteristics of the illness (see Box 27-1). A history of close contact with a documented case of GAS pharyngitis or high prevalence of GAS in the community also can be helpful. More selective use of diagnostic studies for GAS will increase not only the proportion of positive test results, but also the percentage of patients with positive tests who are truly infected rather than merely GAS carriers.
Because adults infrequently are infected with GAS, and rarely develop rheumatic fever, 2001 practice guidelines from the Centers for Disease Control and Prevention (CDC), the American Academy of Family Physicians (AAFP), and the American College of Physicians–American Society of Internal Medicine (ACP–ASIM) recommend the use of a clinical algorithm without microbiologic confirmation as an acceptable approach to the diagnosis of GAS pharyngitis in adults only.17 Although the goal of this algorithm-based strategy was to reduce the inappropriate use of antibiotics in adults with pharyngitis, such an approach could result in the administration of antimicrobial treatment to an unacceptably large number of adults with non-GAS pharyngitis.18
According to a study intended to assess the impact of six different guidelines on the identification and treatment of GAS pharyngitis in children and adults,19 guidelines that recommended selective use of RADTs and/or throat culture and treatment based only on positive test results significantly reduced the inappropriate use of antibiotics in adults. In contrast, the empiric strategy proposed in the CDC/AAFP/ACP–ASIM guidelines resulted in the administration of unnecessary antibiotics to an unacceptably large number of adults. Therefore, diagnosis of adults by symptom-complex only has been discouraged by the latest AHA scientific statement.16
Throat Culture
Culture on sheep blood agar of a specimen obtained by throat swab is the standard laboratory procedure for the microbiologic confirmation of GAS pharyngitis.20 If performed correctly, a throat culture has a sensitivity of 90% to 95%.21 A negative result can occur if the patient has received an antibiotic prior to sampling.
Several variables impact on the accuracy of throat culture results. One of the most important is the manner in which the swab is obtained.22, 23 Throat swab specimens should be obtained from the surface of both tonsils (or tonsillar fossae) and the posterior pharyngeal wall. Other areas of the pharynx and mouth are not acceptable sampling sites and should not be touched during the procedure.
Anaerobic incubation and the use of selective culture media have been reported to increase the sensitivity of throat cultures.24, 25 However, data regarding the impact of the atmosphere of incubation and the culture media are conflicting, and, in the absence of definite benefit, the increased cost and effort associated with anaerobic incubation and selective culture media are difficult to justify.25, 26, 27, 28
Duration of incubation can impact the yield of throat cultures. Cultures should be incubated at 35°C to 37°C for at least 18 to 24 hours prior to reading. An additional overnight incubation at room temperature, however, identifies substantially more positive cultures. In a study performed in patients with pharyngitis and negative RADT, 40% of positive GAS cultures were negative after 24 hours of incubation but positive after 48 hours.29 Therefore, although initial therapeutic decisions can be guided by negative result at 24 hours, it is advisable to wait 48 hours for definitive results.
The clinical significance of the number of colonies of GAS present on inoculated agar is controversial. Although density of bacteria is likely to be greater in patients with bona fide acute GAS pharyngitis than in GAS carriers, there is too much overlap in the colony counts to permit differentiation on the basis of degree of positivity alone.26
The bacitracin disk test is the most widely used method in physicians’ offices for the differentiation of GAS from other β-hemolytic streptococci on a sheep blood agar plate. This test provides a presumptive identification based on the observation that >95% of GAS demonstrate a zone of inhibition around a disk containing 0.04 units of bacitracin, whereas 83% to 97% of non-GAS are not inhibited by bacitracin.26 An alternative and highly specific method for the differentiation of β-hemolytic streptococci is the performance of a group-specific cell wall carbohydrate antigen detection test directly on isolated bacterial colonies for which commercial kits are available. Additional expense for the minimal improvement in accuracy may not be justified.26
Rapid Antigen Detection Tests
RADTs developed for the identification of GAS directly from throat swabs are more expensive than blood agar cultures, but offer speed in providing results. Rapid identification and treatment of patients with GAS pharyngitis can reduce the risk of the spread of GAS, allow the patient to return to school or work sooner, and speed clinical improvement.21, 30 In addition, in certain environments (e.g., emergency departments) the use of RADTs compared with throat cultures has significantly increased the number of patients appropriately treated for GAS pharyngitis.31, 32
The majority of currently available RADTs have specificities of ≥95% compared with blood agar cultures.33 Therapeutic decisions, therefore, can be made with confidence on the basis of a positive RADT result. However, the sensitivity of RADTs is between 70% and 90%.33 Although some patients with falsely negative RADT results merely are GAS carriers, a large proportion truly are infected with GAS.34
The first RADTs utilized latex agglutination methodology, were relatively insensitive, and had unclear endpoints.33 Subsequent tests based on enzyme immunoassay techniques had a more sharply defined endpoint and increased sensitivity. RADTs using optical immunoassay (OIA) and chemiluminescent DNA probes may be more sensitive than other RADTs and perhaps even as sensitive as blood agar plate cultures,33 but because of conflicting and limited data about the OIA and other commercially available RADTs, advisory groups still recommend a confirmatory blood agar culture for children and adolescents who are suspected on clinical grounds of having GAS pharyngitis and have a negative RADT result.
The relative sensitivities of different RADTs can only be determined by direct comparisons in the same study. There have been only five reports of direct comparisons of different RADTs.35, 36, 37, 38, 39 Only a handful of studies have investigated the performance of RADTs in actual clinical practice and physician investigators have concluded differently about adequacy of test performance.29, 36, 37, 38, 39, 40, 41 In one study,29 performed over three winter periods and using on-site office testing in a pediatric group practice, RADT had a sensitivity of approximately 85% compared with a single blood agar plate culture. Investigators in a different pediatric group practice reviewed their experience with 11,427 RADTs performed between 1996 and 1999.42 Only 2.4% of specimens negative by RADT were positive by culture.42 A retrospective review of over 19,000 clinical RADTs performed in a heterogeneous inpatient and outpatient group demonstrated a negative predictive value (NPV) ranging from 90% to 96% and a maximum sensitivity of 77% to 86%.39 Physicians electing to use any RADT in children and adolescents without culture backup of negative results should do so only after demonstrating with adequate sample size calculation that the RADT is as sensitive as throat culture in their own practice.14, 15
Neither blood agar culture nor RADT accurately differentiates individuals with GAS pharyngitis from carriers. However, use facilitates withholding antimicrobial therapy in the great majority of patients with GAS sore throat. There are an estimated 6.7 million visits to primary care providers by adults who complain of sore throat each year in the U.S.; antimicrobial therapy historically was prescribed at 73% of these visits.43 With encouragement for judicious use of antibiotics, trends show a modest decline in the use in children and adolescents diagnosed with pharyngitis to 69% in one study in 1999 to 2000,44 and to 54% in another study in 2003.45
Follow-up Testing
The majority of asymptomatic persons who have a positive throat culture or RADT after completing a course of appropriate antimicrobial therapy for GAS pharyngitis are GAS carriers,46 therefore follow-up testing is not indicated routinely. Follow-up throat culture (or RADT) for an asymptomatic individual should be performed only in those with a history of rheumatic fever, and should be considered in patients who develop acute pharyngitis during outbreaks of acute rheumatic fever or poststreptococcal acute glomerulonephritis, and in individuals in closed or semi-closed communities during outbreaks of GAS pharyngitis.46
Other Diagnostic Considerations
Antistreptococcal antibody titers have no value in the diagnosis of acute GAS pharyngitis, but are useful in prospective epidemiologic studies to differentiate true GAS infections from GAS carriage. Antistreptococcal antibodies are valuable for confirmation of prior GAS infections in patients suspected of having acute rheumatic fever or other non-suppurative complications.
Polymerase chain reaction (PCR) testing for GAS from tonsillar tissue has been shown to be highly sensitive,47 but is not currently available clinically, and expense likely will restrict its use in clinical practice.
The need to definitively diagnose non-GAS causes of pharyngitis occurs rarely and generally only in those who are very ill or have prolonged symptoms. A. haemolyticum will not be identified using standard throat culture methods (intended to identify only GAS), and requires use of standard respiratory culture methods. N. gonorrhoeae can be identified either by selective growth media or by using nucleic acid amplification tests. EBV is routinely diagnosed using the heterophile antibody (monospot), but low sensitivity in younger children necessitates the use of specific antibody testing or serum PCR. Other common viruses such as HSV, adenoviruses, and enteroviruses could be identified in general viral cultures and/or by PCR.
Treatment
Antimicrobial therapy is indicated for individuals with symptomatic pharyngitis after the presence of GAS has been confirmed by throat culture or RADT. In situations in which the clinical and epidemiologic findings are highly suggestive of GAS, antimicrobial therapy can be initiated while awaiting microbiologic confirmation, provided that such therapy is discontinued if culture or RADT is negative. Antimicrobial therapy for GAS pharyngitis shortens the clinical course of the illness.30 However, GAS pharyngitis usually is self limited, and most signs and symptoms resolve spontaneously within 3 or 4 days of onset.48 In addition, initiation of antimicrobial therapy can be delayed for up to 9 days after the onset of GAS pharyngitis and still prevent the occurrence of acute rheumatic fever.49
Antimicrobial Agents
Penicillin and its congeners (such as ampicillin and amoxicillin), as well as numerous cephalosporins, macrolides, and clindamycin, are effective treatment for GAS pharyngitis. Several advisory groups have recommended penicillin as the treatment of choice for this infection.14, 15, 50 GAS has remained exquisitely susceptible to β-lactam agents over five decades.51 Amoxicillin often is used because of acceptable taste of suspension; efficacy appears to equal penicillin. Orally administered macrolides (clarithromycin and erythromycin) or azalides (azithromycin) also are effective (see below). Sulfa drugs, including trimethoprim/sulfamethoxazole, and tetracyclines are not effective and should not be used for GAS pharyngitis.
Following a meta-analysis of 35 clinical trials completed between 1970 and 1999 in which a cephalosporin was compared with penicillin for the treatment of GAS tonsillopharyngitis, it was first suggested that cephalosporins should be the treatment of choice for GAS tonsillopharyngitis.52 However, several methodologic flaws (most notably, the inclusion of GAS carriers) have led to controversy regarding this conclusion.53 Indirect evidence of the superiority of cephalosporins over penicillins to prevent treatment failures and relapses continues to appear;54, 55 however, there has not been a prospective study to clarify the issue beyond doubt. Although the use of cephalosporins for GAS pharyngitis could reduce the number of persons (especially chronic carriers) who harbor GAS after completing therapy, empiric first-line use would be associated with substantial economic and possibly ecologic cost. There are compelling reasons (e.g., its narrow antimicrobial spectrum, low cost, and impressive safety profile) to continue to use penicillin as the drug of choice for uncomplicated GAS pharyngitis. Selected use of a first-generation cephalosporin as the drug of choice may be appropriate for patients at high risk of complications (such as a history of rheumatic fever), with severe symptoms, or with a suspected treatment failure or relapse.
Dosing Intervals and Duration of Therapy
Oral penicillin must be administered multiple times a day for 10 days in order to achieve maximal rates of GAS eradication. Attempts to treat GAS pharyngitis with a single daily dose of penicillin have been unsuccessful.56 Reduced frequency of dosing and shorter treatment courses (<10 days) may result in better patient adherence to therapy. Several antimicrobial agents, including clarithromycin, cefuroxime, cefixime, ceftibuten, cefdinir, and cefpodoxime, are effective in GAS eradication when administered for ≤5 days57, 58, 59, 60, 61, 62 and effective eradication with once-daily dosing has been described for amoxicillin, azithromycin, cefadroxil, cefixime, ceftibuten, cefpodoxime, cefprozil, and cefdinir.14, 58, 61, 63, 64, 65, 66 However, the endpoints of these studies generally are eradication of GAS, not symptomatic improvement or prevention of rheumatic fever (the two main clinical reasons for treatment). In addition, many agents have a broader spectrum of activity and, even if administered for short courses, can be more expensive than standard therapy.58 Therefore, additional studies are needed before these short-course or once daily-dose regimens can be recommended routinely.14
Table 27-2 gives recommendations for several regimens with proven efficacy for GAS pharyngitis.14 Intramuscular benzathine penicillin G is preferred in patients unlikely to complete a full 10-day course of therapy orally.
TABLE 27-2.
Antimicrobial Therapy for Group A β-Hemolytic Streptococci (GAS) Pharyngitis
| Route of Administration, Antimicrobial Agent | Dosage | Duration |
|---|---|---|
| Oral | ||
| Penicillin | Children: 250 mg bid or tid | 10 days |
| Adolescents and adults: 250 mg tid or qid | 10 days | |
| Adolescents and adults: 500 mg bid | 10 days | |
| Intramuscular | ||
| Benzathine penicillin G | 6.0 × 105 U (for patients ≤27 kg) | 1 dose |
| 1.2 × 106 U (for patients >27 kg) | 1 dose | |
| Mixtures of benzathine and procaine penicillin G | Varies with formulationa | |
| Oral, for patients allergic to penicillin | ||
| Erythromycin | Varies with formulation | 10 days |
| First-generation cephalosporinsb | Varies with agent | 10 days |
bid, twice daily; tid, three times daily; qid, four times daily.
Dose should be determined on basis of benzathine component.
These agents should not be used to treat patients with immediate-type hypersensitivity to β-lactam antibiotics.
Modified from Bisno AL, Gerber MA, Gwaltney JM, et al. Practice guideline for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis 2002;35:113–125, with permission.
Macrolide and Lincosamide Resistance
Although GAS resistance to penicillin has not occurred anywhere in the world,67 there are geographic areas with relatively high levels of resistance to macrolide antibiotics.68, 69 The rate of GAS resistance to macrolides in the U.S. generally has remained <5%. In an investigation of 245 pharyngeal isolates and 56 invasive isolates of GAS obtained between 1994 and 1997 from 24 states and the District of Columbia, only 8 (2.6%) isolates were macrolide-resistant.51 A prospective, multicenter, U.S. community-based surveillance study of pharyngeal GAS isolates recovered from children 3 to 18 years of age during three successive respiratory seasons between 2000 and 2003 found macrolide resistance of <5% and clindamycin resistance of 1%,70 and no evidence of increasing erythromycin minimum inhibitory concentrations over the 3-year study period. There was, however, considerable geographic variability in macrolide resistance rates in each study year, as well as year-to-year variability at individual study sites.70
Higher resistance rates have been reported occasionally. For example, 9% of pharyngeal and 32% of invasive GAS strains collected in a San Francisco study during 1994 to 1995 were macrolide-resistant.71 During a longitudinal investigation of GAS disease in a single elementary school in Pittsburgh, investigators found that 48% of isolates of GAS collected between 2000 and 2001 were resistant to erythromycin; none was resistant to clindamycin.72 Molecular typing indicated that this outbreak was due to a single strain of GAS. Clinicians should be aware of local resistance rates.
Other Treatment Considerations
There is currently no evidence from controlled studies to guide therapy of acute pharyngitis when either β-hemolytic group C or group G streptococcus is isolated. If one elects to treat, the regimen should be similar to that for GAS pharyngitis, with penicillin as the antimicrobial agent of choice.8
Acyclovir treatment of HSV gingivostomatitis initiated within 72 hours of the onset of symptoms shortens the duration of illness and decreases the number of lesions.73 Use of antiviral medications for primary EBV pharyngitis has been shown to interrupt viral replication temporarily, but symptomatic relief is negligible and does not justify the use of acyclovir. Corticosteroids are recommended for EBV pharyngitis only when tonsillar enlargement threatens airway patency.15 Several reviews of the large group of heterogeneous studies of use of corticosteroids for GAS and non-GAS pharyngitis conclude a small but measurable benefit in pain reduction, especially when initiated early in the course of severe illness.74, 75, 76, 77 While no adverse outcomes related to corticosteroids were reported, the modest and short-lived benefit of treatment versus potential for harm weigh against their use.
Treatment Failures, Chronic Carriage, and Recurrences
Antimicrobial treatment failure for GAS pharyngitis can be classified as either clinical or bacteriologic failure. The significance of clinical treatment failure (usually defined as persistent or recurrent signs or symptoms suggestive of GAS pharyngitis) is difficult to determine without repeated isolation of the infecting strain of GAS (i.e., true bacteriologic treatment failure).
Bacteriologic treatment failures can be classified as either true or apparent. True bacteriologic failure refers to the inability to eradicate the specific strain of GAS causing an acute episode of pharyngitis with a complete course of appropriate antimicrobial therapy. No penicillin-resistant strains of GAS have ever been identified. The following factors have been suggested but not established definitively: (1) penicillin tolerance (i.e., a discordance between the concentration of penicillin required to inhibit and to kill the organisms);78, 79 (2) enhancement of colonization and growth of GAS by pharyngeal flora or inactivation of penicillin by production of β-lactamases;67 (3) resistance of intracellular organisms to antimicrobial killing.80
Apparent bacteriologic failure can occur when newly acquired GAS isolates are mistaken for the original infecting strain, when the infecting strain of GAS is eradicated but then rapidly reacquired, or when adherence to antimicrobial therapy is poor. However, most bacteriologic treatment failures are manifestations of the GAS carrier state. Chronic carriers have GAS in their pharynx but no clinical illness or immunologic response to the organism, can be colonized for 6 to ≥12 months, are unlikely to spread GAS to close contacts, and are at very low (if any) risk for developing suppurative or nonsuppurative complications.81, 82 During the winter and spring in temperate climates, as many as 20% of asymptomatic school-aged children carry GAS.81 GAS carriers should not be given antimicrobial therapy; the primary approach to the suspected or confirmed carrier is reassurance. A throat culture or RADT should be performed whenever the patient has symptoms and signs suggestive of GAS pharyngitis, but should be avoided when symptoms are more typical of viral illnesses (see Box 29-1). Each clinical episode confirmed with a positive throat culture or RADT should be treated. Identification and eradication of the streptococcal carrier state are desirable in certain specific situations. When antimicrobial therapy is employed, oral clindamycin (20 mg/kg per day up to 450 mg, divided into 3 doses) for 10 days is preferred,51 but intramuscular benzathine penicillin (alone or in combination with procaine penicillin) plus oral rifampin (20 mg/kg per day divided into 2 doses; maximum dose, 300 mg for 4 days beginning on the day of the penicillin injection)37 also is effective. Chronic carriage can recur upon re-exposure to GAS.
In a patient with symptoms suggesting GAS following treatment, a throat culture (or RADT) usually is performed and, if positive, many clinicians would elect to administer a second course of penicillin therapy.
The patient with repeated episodes of acute pharyngitis associated with a positive throat culture (or RADT) is a common and difficult problem for the practicing physician. The fundamental question is whether this patient is experiencing repeated episodes of GAS pharyngitis or is a GAS carrier experiencing repeated episodes of viral pharyngitis. The latter situation is by far the more common. Such a patient is likely to be a GAS carrier if: (1) clinical and epidemiologic findings suggest a viral etiology; (2) there is little clinical response to appropriate antimicrobial therapy; (3) throat culture (or RADT) is positive between episodes of pharyngitis; and (4) there is no serologic response to GAS extracellular antigen (e.g., ASO, anti-deoxyribonucleases B). In contrast, the patient with repeated episodes of acute pharyngitis associated with positive throat cultures (or RADTs) for GAS is likely to be experiencing repeated episodes of bona fide GAS pharyngitis if: (1) clinical and epidemiologic findings suggest GAS pharyngitis; (2) there is a demonstrable clinical response to appropriate antimicrobial therapy; (3) throat culture (or RADT) is negative between episodes of pharyngitis; and (4) there is a serologic response to GAS extracellular antigens. If determined that the patient is experiencing repeated episodes of true GAS pharyngitis, some physicians have suggested use of prophylactic oral penicillin V. However, the efficacy of this regimen has not been proven, and antimicrobial prophylaxis is not recommended except to prevent recurrences of rheumatic fever in patients who have experienced a previous episode of rheumatic fever. Tonsillectomy may be considered in the rare patient whose symptomatic episodes do not diminish in frequency over time and in whom no alternative explanation for the recurrent GAS pharyngitis is evident. However, tonsillectomy has been demonstrated to be beneficial for a relatively small group of these patients, and any benefit is relatively short-lived.83, 84
Complications
GAS pharyngitis can be associated with suppurative and nonsuppurative complications (See Chapter 118, Streptococcus pyogenes Group A Streptococcus). Suppurative complications result from the spread of GAS to adjacent structures and include peritonsillar abscess, para- and retropharyngeal abscess, cervical lymphadenitis, sinusitis, otitis media, and mastoiditis. Before antimicrobial agents were available, suppurative complications of GAS pharyngitis were common; however, antimicrobial therapy has greatly reduced the frequency of such complications.
Acknowledgments
The authors are indebted to the scholarship of Michael Gerber who wrote this chapter in prior editions that have served as a comprehensive template upon which we have provided updated information.
References
- 1.Woodwell D. Office visits to pediatric specialists, 1989. Adv Data. 1992:1–9. [PubMed] [Google Scholar]
- 2.Jensen A, Hagelskjaer Kristensen L, Prag J. Detection of Fusobacterium necrophorum subsp. Funduliforme in tonsillitis in young adults by real-time PCR. Clin Microbiol Infect. 2007;13:695–701. doi: 10.1111/j.1469-0691.2007.01719.x. [DOI] [PubMed] [Google Scholar]
- 3.Fretzayas A, Moustaki M, Kitsiou S. The clinical pattern of group C streptococcal pharyngitis in children. J Infect Chemother. 2009;15:228–232. doi: 10.1007/s10156-009-0694-8. [DOI] [PubMed] [Google Scholar]
- 4.Meier FA, Centor RM, Graham L, Jr, Dalton HP. Clinical and microbiological evidence for endemic pharyngitis among adults due to group C streptococci. Arch Intern Med. 1990;150:825–829. [PubMed] [Google Scholar]
- 5.Turner JC, Hayden FG, Lobo MC. Epidemiologic evidence for Lancefield group C beta-hemolytic streptococci as a cause of exudative pharyngitis in college students. J Clin Microbiol. 1997;35:1–4. doi: 10.1128/jcm.35.1.1-4.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Arditi M, Shulman ST, Davis AT, Yogev R. Group C beta-hemolytic streptococcal infections in children: nine pediatric cases and review. Rev Infect Dis. 1989;11:34–45. doi: 10.1093/clinids/11.1.34. [DOI] [PubMed] [Google Scholar]
- 7.Gerber MA, Randolph MF, Martin NJ. Community-wide outbreak of group G streptococcal pharyngitis. Pediatrics. 1991;87:598–603. [PubMed] [Google Scholar]
- 8.Gerber MA. Non-group A or B streptococci. In: Behrman RE, Kliegman RM, Jenson HB, editors. Nelson Textbook of Pediatrics. Saunders; Philadelphia: 2004. pp. 883–884. [Google Scholar]
- 9.Centor RM. Expand the pharyngitis paradigm for adolescents and young adults. Ann Intern Med. 2009;151:812–815. doi: 10.7326/0003-4819-151-11-200912010-00011. [DOI] [PubMed] [Google Scholar]
- 10.Centor RM, Geiger P, Waites KB. Fusobacterium necrophorum bacteremic tonsillitis: 2 cases and a review of the literature. Anaerobe. 2010;16:626–628. doi: 10.1016/j.anaerobe.2010.08.005. [DOI] [PubMed] [Google Scholar]
- 11.Attia MW, Zaoutis T, Klein JD, Meier FA. Performance of a predictive model for streptococcal pharyngitis in children. Arch Pediatr Adolesc Med. 2001;155:687–691. doi: 10.1001/archpedi.155.6.687. [DOI] [PubMed] [Google Scholar]
- 12.Wald ER, Green MD, Schwartz B, Barbadora K. A streptococcal score card revisited. Pediatr Emerg Care. 1998;14:109–111. doi: 10.1097/00006565-199804000-00005. [DOI] [PubMed] [Google Scholar]
- 13.Shaikh N, Swaminathan N, Hooper EG. Accuracy and precision of the signs and symptoms of streptococcal pharyngitis in children: a systematic review. J Pediatr. 2012;160:487–493. doi: 10.1016/j.jpeds.2011.09.011. [DOI] [PubMed] [Google Scholar]
- 14.Bisno AL, Gerber MA, Gwaltney JM., Jr Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Infectious Diseases Society of America. Clin Infect Dis. 2002;35:113–125. doi: 10.1086/340949. [DOI] [PubMed] [Google Scholar]
- 15.American Academy of Pediatrics . Group A streptococcal infections. In: Pickering L, editor. Red Book: Report of the Committee on Infectious Diseases. American Academy of Pediatrics; Elk Grove Villiage, IL: 2009. pp. 616–628. [Google Scholar]
- 16.Gerber MA, Baltimore RS, Eaton CB. Prevention of rheumatic fever and diagnosis and treatment of acute streptococcal pharyngitis: a scientific statement from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young, the Interdisciplinary Council on Functional Genomics and Translational Biology, and the Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Academy of Pediatrics. Circulation. 2009;119:1541–1551. doi: 10.1161/CIRCULATIONAHA.109.191959. [DOI] [PubMed] [Google Scholar]
- 17.Cooper RJ, Hoffman JR, Bartlett JG. Principles of appropriate antibiotic use for acute pharyngitis in adults: background. Ann Intern Med. 2001;134:509–517. doi: 10.7326/0003-4819-134-6-200103200-00019. [DOI] [PubMed] [Google Scholar]
- 18.Bisno AL, Peter GS, Kaplan EL. Diagnosis of strep throat in adults: are clinical criteria really good enough? Clin Infect Dis. 2002;35:126–129. doi: 10.1086/342056. [DOI] [PubMed] [Google Scholar]
- 19.McIsaac WJ, Kellner JD, Aufricht P. Empirical validation of guidelines for the management of pharyngitis in children and adults. JAMA. 2004;291:1587–1595. doi: 10.1001/jama.291.13.1587. [DOI] [PubMed] [Google Scholar]
- 20.Breese BB, Disney FA. The accuracy of diagnosis of beta streptococcal infections on clinical grounds. J Pediatr. 1954;44:670–673. doi: 10.1016/s0022-3476(54)80008-4. [DOI] [PubMed] [Google Scholar]
- 21.Gerber MA. Comparison of throat cultures and rapid strep tests for diagnosis of streptococcal pharyngitis. Pediatr Infect Dis J. 1989;8:820–824. doi: 10.1097/00006454-198911000-00032. [DOI] [PubMed] [Google Scholar]
- 22.Brien JH, Bass JW. Streptococcal pharyngitis: optimal site for throat culture. J Pediatr. 1985;106:781–783. doi: 10.1016/s0022-3476(85)80354-1. [DOI] [PubMed] [Google Scholar]
- 23.Gunn B, Mesrobian R, Keiser J. Cultures of Streptococcus pyogenes from the oropharynx. Lab Med. 1985;16:369–371. [Google Scholar]
- 24.Lauer BA, Reller LB, Mirrett S. Effect of atmosphere and duration of incubation on primary isolation of group A streptococci from throat cultures. J Clin Microbiol. 1983;17:338–340. doi: 10.1128/jcm.17.2.338-340.1983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Schwartz RH, Gerber MA, McCoy P. Effect of atmosphere of incubation on the isolation of group A streptococci from throat cultures. J Lab Clin Med. 1985;106:88–92. [PubMed] [Google Scholar]
- 26.Gerber MA. Diagnosis of pharyngitis: methodology of throat cultures. In: Shulman S, editor. Pharyngitis: Management in an Era of Declining Rheumatic Fever. Praeger; New York: 1984. pp. 61–72. [Google Scholar]
- 27.Kellogg JA, Manzella JP. Detection of group A streptococci in the laboratory or physician's office: culture vs. antibody methods. JAMA. 1986;255:2638–2642. [PubMed] [Google Scholar]
- 28.Roddey OF, Jr, Clegg HW, Martin ES. Comparison of throat culture methods for the recovery of group A streptococci in a pediatric office setting. JAMA. 1995;274:1863–1865. [PubMed] [Google Scholar]
- 29.Armengol CE, Schlager TA, Hendley JO. Sensitivity of a rapid antigen detection test for group A streptococci in a private pediatric office setting: answering the Red Book's request for validation. Pediatrics. 2004;113:924–926. doi: 10.1542/peds.113.4.924. [DOI] [PubMed] [Google Scholar]
- 30.Randolph MF, Gerber MA, DeMeo KK, Wright L. Effect of antibiotic therapy on the clinical course of streptococcal pharyngitis. J Pediatr. 1985;106:870–875. doi: 10.1016/s0022-3476(85)80228-6. [DOI] [PubMed] [Google Scholar]
- 31.Lieu TA, Fleisher GR, Schwartz JS. Clinical evaluation of a latex agglutination test for streptococcal pharyngitis: performance and impact on treatment rates. Pediatr Infect Dis J. 1988;7:847–854. [PubMed] [Google Scholar]
- 32.Ayanruoh S, Waseem M, Quee F. Impact of rapid streptococcal test on antibiotic use in a pediatric emergency department. Pediatr Emerg Care. 2009;25:748–750. doi: 10.1097/PEC.0b013e3181bec88c. [DOI] [PubMed] [Google Scholar]
- 33.Gerber MA, Shulman ST. Rapid diagnosis of pharyngitis caused by group A streptococci. Clin Microbiol Rev. 2004;17:571–580. doi: 10.1128/CMR.17.3.571-580.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gerber MA, Randolph MF, Chanatry J. Antigen detection test for streptococcal pharyngitis: evaluation of sensitivity with respect to true infections. J Pediatr. 1986;108:654–658. doi: 10.1016/s0022-3476(86)81036-8. [DOI] [PubMed] [Google Scholar]
- 35.Roe M, Kishiyama C, Davidson K. Comparison of Biostar Strep A OIA optical immune assay, Abbott Testpack Plus Strep A, and culture with selective media for diagnosis of group A streptococcal pharyngitis. J Clin Microbiol. 1995;33:1551–1553. doi: 10.1128/jcm.33.6.1551-1553.1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Roosevelt GE, Kulkarni MS, Shulman ST. Critical evaluation of a CLIA-waived streptococcal antigen detection test in the emergency department. Ann Emerg Med. 2001;37:377–381. doi: 10.1067/mem.2001.114090. [DOI] [PubMed] [Google Scholar]
- 37.Gieseker KE, Mackenzie T, Roe MH, Todd JK. Comparison of two rapid Streptococcus pyogenes diagnostic tests with a rigorous culture standard. Pediatr Infect Dis J. 2002;21:922–927. doi: 10.1097/00006454-200210000-00007. [DOI] [PubMed] [Google Scholar]
- 38.Schwartz RH. Evaluation of rapid streptococcal detection tests. Pediatr Infect Dis J. 1997;16:1099–1100. doi: 10.1097/00006454-199711000-00028. [DOI] [PubMed] [Google Scholar]
- 39.Mirza A, Wludyka P, Chiu TT, Rathore MH. Throat culture is necessary after negative rapid antigen detection tests. Clin Pediatr (Phila) 2007;46:241–246. doi: 10.1177/0009922806290219. [DOI] [PubMed] [Google Scholar]
- 40.Nerbrand C, Jasir A, Schalen C. Are current rapid detection tests for group A streptococci sensitive enough? Evaluation of 2 commercial kits. Scand J Infect Dis. 2002;34:797–799. doi: 10.1080/0036554021000026953. [DOI] [PubMed] [Google Scholar]
- 41.Gieseker KE, Roe MH, MacKenzie T, Todd JK. Evaluating the American Academy of Pediatrics diagnostic standard for Streptococcus pyogenes pharyngitis: backup culture versus repeat rapid antigen testing. Pediatrics. 2003;111:e666–e670. doi: 10.1542/peds.111.6.e666. [DOI] [PubMed] [Google Scholar]
- 42.Mayes T, Pichichero ME. Are follow-up throat cultures necessary when rapid antigen detection tests are negative for group A streptococci? Clin Pediatr (Phila) 2001;40:191–195. doi: 10.1177/000992280104000402. [DOI] [PubMed] [Google Scholar]
- 43.Linder JA, Stafford RS. Antibiotic treatment of adults with sore throat by community primary care physicians: a national survey, 1989–1999. JAMA. 2001;286:1181–1186. doi: 10.1001/jama.286.10.1181. [DOI] [PubMed] [Google Scholar]
- 44.McCaig LF, Besser RE, Hughes JM. Trends in antimicrobial prescribing rates for children and adolescents. JAMA. 2002;287:3096–3102. doi: 10.1001/jama.287.23.3096. [DOI] [PubMed] [Google Scholar]
- 45.Linder JA, Bates DW, Lee GM, Finkelstein JA. Antibiotic treatment of children with sore throat. JAMA. 2005;294:2315–2322. doi: 10.1001/jama.294.18.2315. [DOI] [PubMed] [Google Scholar]
- 46.Gerber MA. Treatment failures and carriers: perception or problems? Pediatr Infect Dis J. 1994;13:576–579. doi: 10.1097/00006454-199406000-00036. [DOI] [PubMed] [Google Scholar]
- 47.Lee JH, Uhl JR, Cockerill FR., 3rd Real-time PCR vs. standard culture detection of group A beta-hemolytic streptococci at various anatomic sites in tonsillectomy patients. Arch Otolaryngol Head Neck Surg. 2008;134:1177–1181. doi: 10.1001/archotol.134.11.1177. [DOI] [PubMed] [Google Scholar]
- 48.Brink WR, Rammelkamp CH, Jr, Denny FW, Wannamaker LW. Effect in penicillin and aureomycin on the natural course of streptococcal tonsillitis and pharyngitis. Am J Med. 1951;10:300–308. doi: 10.1016/0002-9343(51)90274-4. [DOI] [PubMed] [Google Scholar]
- 49.Catanzaro FJ, Stetson CA, Morris AJ. The role of the streptococcus in the pathogenesis of rheumatic fever. Am J Med. 1954;17:749–756. doi: 10.1016/0002-9343(54)90219-3. [DOI] [PubMed] [Google Scholar]
- 50.Dajani A, Taubert K, Ferrieri P. Treatment of acute streptococcal pharyngitis and prevention of rheumatic fever: a statement for health professionals. Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young, the American Heart Association. Pediatrics. 1995;96:758–764. [PubMed] [Google Scholar]
- 51.Kaplan EL, Johnson DR, Del Rosario MC, Horn DL. Susceptibility of group A beta-hemolytic streptococci to thirteen antibiotics: examination of 301 strains isolated in the United States between 1994 and 1997. Pediatr Infect Dis J. 1999;18:1069–1072. doi: 10.1097/00006454-199912000-00008. [DOI] [PubMed] [Google Scholar]
- 52.Casey JR, Pichichero ME. Meta-analysis of cephalosporin versus penicillin treatment of group A streptococcal tonsillopharyngitis in children. Pediatrics. 2004;113:866–882. doi: 10.1542/peds.113.4.866. [DOI] [PubMed] [Google Scholar]
- 53.Shulman ST, Gerber MA. So what's wrong with penicillin for strep throat? Pediatrics. 2004;113:1816–1819. doi: 10.1542/peds.113.6.1816. [DOI] [PubMed] [Google Scholar]
- 54.Casey JR, Kahn R, Gmoser D. Frequency of symptomatic relapses of group A beta-hemolytic streptococcal tonsillopharyngitis in children from 4 pediatric practices following penicillin, amoxicillin, and cephalosporin antibiotic treatment. Clin Pediatr (Phila) 2008;47:549–554. doi: 10.1177/0009922808315212. [DOI] [PubMed] [Google Scholar]
- 55.Casey JR, Pichichero ME. Symptomatic relapse of group A beta-hemolytic streptococcal tonsillopharyngitis in children. Clin Pediatr (Phila) 2007;46:307–310. doi: 10.1177/0009922806293919. [DOI] [PubMed] [Google Scholar]
- 56.Gerber MA, Randolph MF, DeMeo K. Failure of once-daily penicillin V therapy for streptococcal pharyngitis. Am J Dis Child. 1989;143:153–155. doi: 10.1001/archpedi.1989.02150140039016. [DOI] [PubMed] [Google Scholar]
- 57.Pichichero ME, Casey JR. Bacterial eradication rates with shortened courses of 2nd- and 3rd-generation cephalosporins versus 10 days of penicillin for treatment of group A streptococcal tonsillopharyngitis in adults. Diagn Microbiol Infect Dis. 2007;59:127–130. doi: 10.1016/j.diagmicrobio.2007.04.010. [DOI] [PubMed] [Google Scholar]
- 58.Gerber MA, Tanz RR. New approaches to the treatment of group A streptococcal pharyngitis. Curr Opin Pediatr. 2001;13:51–55. doi: 10.1097/00008480-200102000-00009. [DOI] [PubMed] [Google Scholar]
- 59.Scholz H. Streptococcal-a tonsillopharyngitis: a 5-day course of cefuroxime axetil versus a 10-day course of penicillin V. Results depending on the children's age. Chemotherapy. 2004;50:51–54. doi: 10.1159/000077286. [DOI] [PubMed] [Google Scholar]
- 60.Syrogiannopoulos GA, Bozdogan B, Grivea IN. Two dosages of clarithromycin for five days, amoxicillin/clavulanate for five days or penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatr Infect Dis J. 2004;23:857–865. doi: 10.1097/01.inf.0000138080.74674.a2. [DOI] [PubMed] [Google Scholar]
- 61.Cohen R. Defining the optimum treatment regimen for azithromycin in acute tonsillopharyngitis. Pediatr Infect Dis J. 2004;23:S129–S134. doi: 10.1097/01.inf.0000112527.33870.0d. [DOI] [PubMed] [Google Scholar]
- 62.Brook I, Gober AE. Rate of eradication of group A beta-hemolytic streptococci in children with pharyngo-tonsillitis by amoxicillin and cefdinir. Int J Pediatr Otorhinolaryngol. 2009;73:757–759. doi: 10.1016/j.ijporl.2009.02.004. [DOI] [PubMed] [Google Scholar]
- 63.Shvartzman P, Tabenkin H, Rosentzwaig A, Dolginov F. Treatment of streptococcal pharyngitis with amoxicillin once a day. BMJ. 1993;306:1170–1172. doi: 10.1136/bmj.306.6886.1170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Feder HM, Jr, Gerber MA, Randolph MF. Once-daily therapy for streptococcal pharyngitis with amoxicillin. Pediatrics. 1999;103:47–51. doi: 10.1542/peds.103.1.47. [DOI] [PubMed] [Google Scholar]
- 65.Curtin CD, Casey JR, Murray PC. Efficacy of cephalexin two vs. three times daily vs. cefadroxil once daily for streptococcal tonsillopharyngitis. Clin Pediatr (Phila) 2003;42:519–526. doi: 10.1177/000992280304200606. [DOI] [PubMed] [Google Scholar]
- 66.Lennon DR, Farrell E, Martin DR, Stewart JM. Once-daily amoxicillin versus twice-daily penicillin V in group A beta-haemolytic streptococcal pharyngitis. Arch Dis Child. 2008;93:474–478. doi: 10.1136/adc.2006.113506. [DOI] [PubMed] [Google Scholar]
- 67.Gerber MA. Antibiotic resistance: relationship to persistence of group A streptococci in the upper respiratory tract. Pediatrics. 1996;97:971–975. [PubMed] [Google Scholar]
- 68.Cornaglia G, Ligozzi M, Mazzariol A. Resistance of Streptococcus pyogenes to erythromycin and related antibiotics in Italy. The Italian Surveillance Group for Antimicrobial Resistance. Clin Infect Dis. 1998;27(Suppl 1):S87–S92. doi: 10.1086/514908. [DOI] [PubMed] [Google Scholar]
- 69.Seppala H, Klaukka T, Vuopio-Varkila J. The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. Finnish study group for antimicrobial resistance. N Engl J Med. 1997;337:441–446. doi: 10.1056/NEJM199708143370701. [DOI] [PubMed] [Google Scholar]
- 70.Tanz RR, Shulman ST, Shortridge VD. Community-based surveillance in the United States of macrolide-resistant pediatric pharyngeal group A streptococci during 3 respiratory disease seasons. Clin Infect Dis. 2004;39:1794–1801. doi: 10.1086/426025. [DOI] [PubMed] [Google Scholar]
- 71.York MK, Gibbs L, Perdreau-Remington F, Brooks GF. Characterization of antimicrobial resistance in Streptococcus pyogenes isolates from the San Francisco bay area of Northern California. J Clin Microbiol. 1999;37:1727–1731. doi: 10.1128/jcm.37.6.1727-1731.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Martin JM, Green M, Barbadora KA, Wald ER. Erythromycin-resistant group A streptococci in schoolchildren in Pittsburgh. N Engl J Med. 2002;346:1200–1206. doi: 10.1056/NEJMoa013169. [DOI] [PubMed] [Google Scholar]
- 73.Amir J, Harel L, Smetana Z, Varsano I. Treatment of herpes simplex gingivostomatitis with aciclovir in children: a randomised double blind placebo controlled study. BMJ. 1997;314:1800–1803. doi: 10.1136/bmj.314.7097.1800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Hayward G, Thompson M, Heneghan C. Corticosteroids for pain relief in sore throat: systematic review and meta-analysis. BMJ. 2009;339:b2976. doi: 10.1136/bmj.b2976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Korb K, Scherer M, Chenot JF. Steroids as adjuvant therapy for acute pharyngitis in ambulatory patients: a systematic review. Ann Fam Med. 2010;8:58–63. doi: 10.1370/afm.1038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.O’Brien JF, Meade JL, Falk JL. Dexamethasone as adjuvant therapy for severe acute pharyngitis. Ann Emerg Med. 1993;22:212–215. doi: 10.1016/s0196-0644(05)80205-7. [DOI] [PubMed] [Google Scholar]
- 77.Wing A, Villa-Roel C, Yeh B. Effectiveness of corticosteroid treatment in acute pharyngitis: a systematic review of the literature. Acad Emerg Med. 2010;17:476–483. doi: 10.1111/j.1553-2712.2010.00723.x. [DOI] [PubMed] [Google Scholar]
- 78.Smith TD, Huskins WC, Kim KS, Kaplan EL. Efficacy of beta-lactamase-resistant penicillin and influence of penicillin tolerance in eradicating streptococci from the pharynx after failure of penicillin therapy for group A streptococcal pharyngitis. J Pediatr. 1987;110:777–782. doi: 10.1016/s0022-3476(87)80023-9. [DOI] [PubMed] [Google Scholar]
- 79.Kim KS, Kaplan EL. Association of penicillin tolerance with failure to eradicate group A streptococci from patients with pharyngitis. J Pediatr. 1985;107:681–684. doi: 10.1016/s0022-3476(85)80392-9. [DOI] [PubMed] [Google Scholar]
- 80.Kaplan EL, Chhatwal GS, Rohde M. Reduced ability of penicillin to eradicate ingested group A streptococci from epithelial cells: clinical and pathogenetic implications. Clin Infect Dis. 2006;43:1398–1406. doi: 10.1086/508773. [DOI] [PubMed] [Google Scholar]
- 81.Kaplan EL. The group A streptococcal upper respiratory tract carrier state: an enigma. J Pediatr. 1980;97:337–345. doi: 10.1016/s0022-3476(80)80178-8. [DOI] [PubMed] [Google Scholar]
- 82.Martin JM, Green M, Barbadora KA, Wald ER. Group A streptococci among school-aged children: clinical characteristics and the carrier state. Pediatrics. 2004;114:1212–1219. doi: 10.1542/peds.2004-0133. [DOI] [PubMed] [Google Scholar]
- 83.Paradise JL, Bluestone CD, Colborn DK. Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children. Pediatrics. 2002;110:7–15. doi: 10.1542/peds.110.1.7. [DOI] [PubMed] [Google Scholar]
- 84.Discolo CM, Darrow DH, Koltai PJ. Infectious indications for tonsillectomy. Pediatr Clin North Am. 2003;50:445–458. doi: 10.1016/s0031-3955(03)00030-0. [DOI] [PubMed] [Google Scholar]