

Abstract
Community-acquired pneumonia (CAP) is defined as an acute infection of the pulmonary parenchyma in a patient who has acquired the infection in the community and has not had recent hospitalization or association with other healthcare facilities such as nursing homes, dialysis centers, and outpatient clinics. CAP is a common and potentially serious illness, particularly in elderly patients and those with significant comorbidities. CAP may be caused by myriad pathogens, but bacteria are the most common causes. Bacteria have traditionally been divided into two groups: typical and atypical agents. Typical organisms include Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, group A streptococci, Moraxella catarrhalis, anaerobes, and aerobic gram-negative bacteria. Atypical organisms include Legionella species, Mycoplasma pneumoniae, Chlamydophila (also known as Chlamydia) pneumoniae, and Chlamydophila psittaci. This chapter will focus on the general approach to CAP in adults, with a concentration primarily on typical bacterial causes. Other chapters focus specifically on pneumonia caused by aspiration, viruses, or atypical organisms.
Disease Burden
CAP is associated with significant morbidity and mortality and considerable costs of care. In the United States, CAP is the most frequent cause of death resulting from infectious diseases and is the eighth leading cause of death overall. The mortality rate of patients treated on an outpatient basis is <1%; for those who require admission to the hospital, it averages 12% but increases to 30% to 40% for those with severe CAP who require admission to the intensive care unit (ICU). The overall rate of CAP ranges from 8 to 15 per 1000 persons per year; the highest rates are at the extremes of age. More cases occur during the winter months. The economic cost exceeds $17 billion a year.
Pathogenesis and Risk Factors
The primary route of pathogens into the lungs is by microaspiration of upper airway contents. Although the respiratory tract is constantly exposed to particulate material, the lower airways are usually sterile because of the pulmonary defense mechanisms, which include the anatomy of the nasal passages, the cough reflex, the ciliary respiratory epithelium, and humeral and cellular factors (e.g., immunoglobulins, complement, macrophages, and neutrophils). CAP occurs when there is a defect in host defenses, exposure to a particularly virulent microorganism, or an overwhelming inoculum. Other routes for pathogens to the lung are hematogenous spread, direct spread from a contiguous focus, and macroaspiration. There are several predisposing conditions (Box 26-1 ).
Box 26-1. Predisposing Conditions of Community-Acquired Pneumonia.
-
•
Alterations in the level of consciousness, which predispose to both macroaspiration of stomach contents (because of stroke, seizures, drug intoxication, anesthesia, and alcohol abuse) and microaspiration of upper airway secretions during sleep
-
•
Smoking
-
•
Alcohol consumption
-
•
Toxic inhalations
-
•
Pulmonary edema
-
•
Uremia
-
•
Malnutrition
-
•
Administration of immunosuppressive agents (solid organ or stem cell transplant recipients or patients receiving chemotherapy)
-
•
Mechanical obstruction of a bronchus
-
•
Being elderly (there is a marked increase in the rate of pneumonia in persons ≥65 years)
-
•
Cystic fibrosis
-
•
Bronchiectasis
-
•
Chronic obstructive pulmonary disease (COPD)
-
•
Previous episode of pneumonia or chronic bronchitis
-
•
Uncontrolled comorbidities (e.g., congestive heart failure, diabetes)
Once bacteria reach the lungs, they can cause an inflammatory response that results in disease. This is best studied with S. pneumoniae, which in the absence of opsonizing antibodies, rapidly multiplies in the alveolar spaces, leading to local hyperemia, edema, and mobilization of neutrophils. The filling of alveoli with bacteria, red cells, and fluid leads to significant increase in weight of the lung in this early phase of consolidation (Figure 26-1 ). Subsequently this leads to advanced consolidation with increased neutrophils, pulmonary cells, and fibrin.
Figure 26-1.

Pneumococcal pneumonia.
Microbiology
Although numerous pathogens have been associated as a cause of CAP, a limited range of key pathogens cause the majority of cases (Table 26-1 ). The predominant pathogen continues to be S. pneumoniae (pneumococcus), which accounts for approximately two thirds of all cases of bacteremic pneumonia. Other causative agents include (but are not limited to) H. influenzae, M. pneumoniae, C. pneumoniae, Legionella species, enteric gram-negative bacteria (Enterobacteriaceae), Pseudomonas aeruginosa, S. aureus, anaerobes (aspiration pneumonia), and respiratory viruses (influenza, adenovirus, respiratory syncytial virus, parainfluenza, coronavirus). S. aureus (Figure 26-2 ) and gram-negative bacilli (such as Klebsiella species; Figure 26-3 ) are less frequently isolated and are the cause in selected patients (e.g., patients with severe CAP requiring intensive care admission or those who have recently received antimicrobial therapy or have pulmonary comorbidities). The frequency of other causes—for example, Mycobacterium tuberculosis, C. psittaci (psittacosis), Coxiella burnettii (Q fever), Francisella tularensis (tularemia), and endemic fungi (histoplasmosis, coccidioidomycosis, blastomycosis)—varies with epidemiologic setting.
Table 26-1.
Most Common Causes of Community-Acquired Pneumonia
| AMBULATORY PATIENTS | HOSPITALIZED (NON-ICU) | SEVERE (ICU) |
|---|---|---|
|
|
|
ICU, Intensive care unit.
Influenza A and B, adenovirus, respiratory syncytial virus, parainfluenza.
Adapted from Mandell LA, Wunderink RG, Anzueto A, et al: Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults, Clin Infect Dis 44(suppl 2):S27-S72, 2007; based on collective data from recent studies.
Figure 26-2.
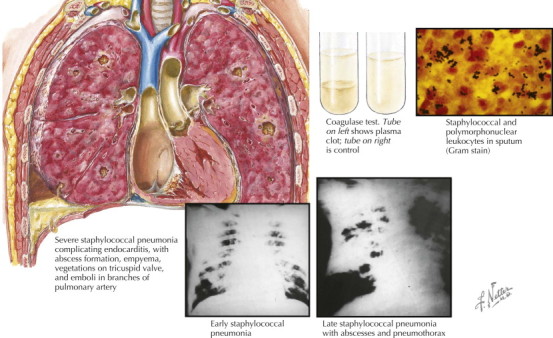
Staphylococcal pneumonia.
Figure 26-3.

Klebsiella (Friedländer's) pneumonia.
Recently, a community-associated methicillin-resistant S. aureus (CA-MRSA) strain has emerged as a cause of severe CAP associated with hemorrhagic and necrotizing complications and usually following influenza infection. CA-MRSA is more virulent than the traditional nosocomial MRSA strains, and strains of CA-MRSA tend to be more susceptible to antimicrobial agents than hospital-acquired MRSA strains. The majority of CA-MRSA strains contain a novel type IV staphylococcal cassette chromosome (SCCmec) gene and also carry the Panton-Valentine leukocidin (PVL) genes, which produce toxins that create lytic pores in cell membranes of neutrophils, inducing release of chemotactic factors that promote inflammation and tissue destruction. Such patients often have necrotizing pneumonia and abscesses (see Figure 26-2). Although PVL toxins may be a highly linked epidemiologic marker for CA-MRSA strains, it remains unclear whether PVL is the major virulence determinant of CA-MRSA.
Antimicrobial resistance, especially the emergence of multidrug-resistant S. pneumoniae, has escalated worldwide over the last two decades. Risk factors for drug-resistant S. pneumoniae include very young age (<2 years) and old age (>65 years); β-lactam, macrolide, or fluoroquinolone therapy within the previous 3 months; alcoholism; medical comorbidities; immunosuppressive illness or therapy; and exposure to a child in a daycare center. Available data suggest that a clinically relevant level of penicillin resistance is a minimum inhibitory concentration (MIC) of ≥4 mcg/mL. At this breakpoint the rate of penicillin resistance for pneumonia for most locations in North America is ≤10%
Clinical Features
Symptoms and signs of CAP include cough (either productive or nonproductive), pleuritic chest pain, shortness of breath, temperature higher than 38° C, and crackles on auscultation. Mucopurulent sputum production is more frequently found in association with bacterial pneumonia, whereas scant or watery sputum production is more suggestive of an atypical pathogen. Although there are classic descriptions of certain types of sputum production and particular pathogens (e.g., pneumococcal pneumonia and rust-colored sputum), these clinical descriptions usually do not help with initial clinical decision making regarding treatment because the clinical presentations of the specific pathogens are variable. Gastrointestinal symptoms (nausea, vomiting, diarrhea) and mental status changes may accompany respiratory manifestations.
On physical examination the majority of patients are febrile, although this finding is frequently absent in older patients. Increased respiratory rate is frequently noted, and this may be the most sensitive sign in elderly patients; tachycardia is also common. Chest examination reveals audible rales in most patients, and approximately one third have evidence of consolidation. However, no clear constellation of symptoms and signs has been found to accurately predict whether or not the patient has pneumonia.
The major blood test abnormality is leukocytosis (typically 15,000 to 30,000 per mm3) with a leftward shift. Leukopenia can occur and generally is associated with a poor prognosis.
Diagnostic Approach
Adult patients who are immunocompetent should be evaluated for pneumonia if they demonstrate signs including cough, sputum production, labored breathing (including altered breath sounds and rales), and/or fever. These symptoms (especially cough) are nonspecific and may also be present in patients with other diseases that should be considered in the differential diagnosis (Box 26-2 , Figure 26-4 ).
Box 26-2. Differential Diagnosis of Cough and Fever.
Infectious
Upper Respiratory Tract
Acute or chronic sinusitis
Lower Respiratory Tract
Acute or chronic bronchitis
Acute exacerbation of chronic obstructive pulmonary disease
Bronchiectasis
Tuberculosis
Noninfectious
Pulmonary embolism or infarction
Pulmonary neoplasm
Radiation pneumonitis
Interstitial lung disease
Sarcoidosis
Collagen vascular disease
Drug-induced pulmonary disease
Hypersensitivity pneumonitis
Granulomatous vasculitis
Eosinophilic pneumonitis
Figure 26-4.
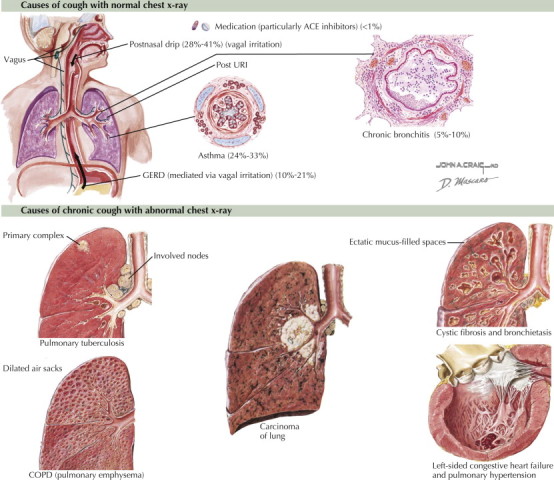
Causes of chronic cough.
The presence of an infiltrate on plain chest radiograph is considered the gold standard for diagnosing pneumonia when clinical features are supportive. Radiologists cannot reliably differentiate bacterial from nonbacterial pneumonia on the basis of the radiographic appearance. Computed tomography (CT) scans are significantly more sensitive in detecting pulmonary infiltrates in patients hospitalized with CAP, but the clinical significance of this finding is unclear.
Determining Severity of Illness and Site of Care
Site of care in patients with CAP affects the overall cost of treatment, the intensity of diagnostic testing, and the empirical antimicrobial(s). A general consensus is that the majority of patients can be safely treated as outpatients. However, selected patients should be hospitalized based on the requirements of care (e.g., need for close observation, respiratory support, intravenous antibiotics, or other concerns). The advantages of not admitting patients for treatment of CAP include decreased cost, patient preference, and avoidance of iatrogenic complications in the hospital. For elderly patients, particularly, a reduction in time in a hospital bed can facilitate better convalescence. Hospitalization should be considered when (1) patients have preexisting conditions that may compromise the safety of home care, (2) patients have hypoxemia, (3) patients are unable to take oral medications, or (4) psychosocial factors can potentially influence effective treatment (such as an unstable home environment or psychiatric disorders that may hinder adherence to therapy). Mortality prediction tools can also help guide clinicians in determining the requirement of hospitalization.
The pneumonia prediction rule, developed over 10 years ago, offers important insights into the risk of mortality. This technique uses a combination of demographic variables, comorbidities, physical observations, and laboratory and radiographic variables to assign patients to one of five classes. Those belonging to pneumonia severity index (PSI) class 1 or 2 have a low risk of mortality (<1%) and can be treated as outpatients. Those in PSI class 3 have a slightly higher risk of mortality (<5%) and may require a brief observational stay in a hospital. Those in PSI class 4 or 5 have the highest mortality risk (8% to 40%) and will require hospitalization; those in PSI class 5 should be admitted to an ICU. Though the PORT prediction rule is effective in determining mortality risk, it is not the most practical approach in the clinical setting as it is partly based on laboratory evaluations that can be time-consuming.
The CURB-65 rule uses only five aspects in making a clinical determination—confusion, urea concentration, respiratory rate, blood pressure, and age. Those meeting two or more of these criteria should be considered for hospitalization. However, this method requires a blood sample and laboratory analysis for urea concentration. In response to this, the CRB-65 was designed. It omitted the blood urea measurement and was practical for office-based settings. In CRB-65, a score of 0 equates to home treatment, a score of 1 to hospital-supervised treatment, and a score of 2 or more to hospitalization.
Recommendations regarding admission to the ICU are provided by the Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS) guidelines for management of CAP. According to the IDSA/ATS guidelines, direct admission to the ICU is essential for patients with septic shock requiring vasopressor or for patients with acute respiratory failure requiring intubation and mechanical ventilation. ICU admission should also be considered for patients who have three or more of the following: confusion or disorientation, uremia (blood urea nitrogen ≥20 mg/dL), respiratory rate ≥30 breaths/min, hypotension requiring aggressive fluid resuscitation, Pao 2/Fio 2 ratio ≤250, multilobar infiltrates, leukopenia (white blood count <4000 cells/mm3), thrombocytopenia (platelet count <100,000 cells/mm3), or hypothermia (core temperature <36° C).
Determining Causative Diagnosis
The utility of diagnostic studies to determine the causative agents of CAP is controversial because of the lack of rapid, easily performed, accurate, cost-effective methods that allow immediate results for the majority of patients at the point of service (i.e., the initial evaluation by a clinician in an office or acute care setting). Nevertheless, there is good rationale for establishing a causative diagnosis (i.e., to permit antibiotic selection that permits optimal selection of agents against a specific pathogen, to limit the consequences of antibiotic misuse, and to identify pathogens of potential epidemiologic significance such as Legionella or tuberculosis [TB]).
Routine microbiologic tests are not recommended by most of the recent guidelines for patients managed in the community. However, if a patient has purulent sputum, it is reasonable to send a sample to the laboratory for Gram stain and culture on the basis that the information may be of value for directing specific therapy if the patient's condition is failing to respond to initial empirical therapy.
Investigations that are variably recommended for patients requiring admission include blood cultures, Gram stain and culture, and thoracentesis if there is significant pleural fluid present. Approximately 11% of patients with CAP will have positive blood cultures, more commonly associated with severe illness. Because false-positive blood cultures may be more common than pathogen-positive blood cultures from patients admitted to a general ward, they may have limited benefit for such patients and are considered “optional” in recent guidelines. In more severely ill patients requiring ICU admission, blood cultures may increase the likelihood of finding a pathogen not covered by customary antimicrobial therapy and are recommended for all such patients. The value of performing a sputum Gram stain and culture is limited by the facts that many patients cannot produce a good specimen and the validity of the Gram stain is related directly to the experience of the interpreter; however, when stringent criteria are applied, the specificity for pneumococcal pneumonia can approach 90%. Sputum culture for other pathogens (e.g., Legionella species, fungus, virus, Mycobacterium species) should be obtained based on epidemiologic considerations. M. tuberculosis should be considered when patients are from endemic areas, when the chest radiograph shows an upper lobe cavitary infiltrate, when patients have had prolonged symptoms of cough (often with weight loss and night sweats), when patients are homeless, or when they have a history of exposure to TB.
Because the early administration of therapy is important for the outcome of CAP, an attempt to obtain expectorated sputum should never delay prompt initiation of antimicrobial therapy.
Other tests considered helpful for patients admitted to the hospital include the urinary antigen assays for Legionella and S. pneumoniae and a direct stain (i.e., acid-fast) for detection of mycobacterial infections in patients with epidemiologic risks for TB. Many rapid diagnostic tests such as nucleic acid amplification tests (i.e., polymerase chain reaction [PCR]) assays are early in development and not commonly available, but offer promise for rapid diagnosis and will likely become increasingly utilized in the future. Serologic tests are generally not helpful in the early management of CAP because the determination of acute and convalescent titers is required before the cause can be ascribed to a specific pathogen. Percutaneous transthoracic needle aspiration (PTNA) or other invasive testing (including bronchoscopy and biopsy) is not routinely recommended for the evaluation of patients but may be valuable in immunocompromised hosts, suspected TB in the absence of productive cough, selected cases of chronic pneumonia, pneumonia associated with suspected neoplasm or foreign body, suspected Pneumocystis carinii pneumonia, some cases in which intubation is required, and suspected conditions that require lung biopsy.
Clinical Management and Drug Treatment
Empirical Antimicrobial Therapy
Until there are better rapid diagnostic methods, the majority of patients will be treated empirically. Although some authorities propose a syndromic approach to therapy (counting on the predictability of a cause based on the presenting clinical manifestations), most data indicate that the presenting clinical features are not specific enough to reliably predict the cause of CAP. Therefore unless there is a specific epidemiologic factor (e.g., influenza epidemic), the empirical approach to initial therapy is usually based on the likelihood that one of the key pathogens is responsible for disease. Recently published guidelines from North America give specific recommendations for empirical therapy for CAP (Table 26-2 ).
Table 26-2.
Epidemiologic Conditions and/or Risk Factors Related to Specific Pathogens in Community-Acquired Pneumonia
| CONDITION | COMMONLY ENCOUNTERED PATHOGEN(S) |
|---|---|
| Alcoholism | Streptococcus pneumoniae, oral anaerobes, Klebsiella pneumoniae, Acinetobacter species, Mycobacterium tuberculosis |
| COPD and/or smoking | Haemophilus influenzae, Pseudomonas aeruginosa, Legionella species, S. pneumoniae, Moraxella catarrhalis, Chlamydophila pneumoniae |
| Aspiration | Gram-negative enterics, oral anaerobes |
| Lung abscess | CA-MRSA, oral anaerobes, endemic fungal pneumonia, M. tuberculosis, atypical mycobacteria |
| Exposure to bat or bird droppings | Histoplasma capsulatum |
| Exposure to birds | Chlamydia (Chlamydophila) psittaci (if poultry—avian influenza) |
| Exposure to rabbits | Francisella tularensis |
| Exposure to farm animals or parturient cats | Coxiella burnettii (Q fever) |
| HIV (early) | S. pneumoniae, H. influenzae, M. tuberculosis |
| HIV (late) | Above plus Pneumocystis jiroveci, Cryptococcus, Histoplasmosis, Aspergillus, atypical mycobacteria (especially Mycobacterium kansasii), P. aeruginosa, H. influenzae |
| Hotel or cruise ship stay in previous 2 weeks | Legionella |
| Travel to or residence in southwestern United States | Coccidioides species, hantavirus |
| Travel to or residence in Southeast and East Asia | Burkholderia pseudomallei, avian influenza, SARS |
| Influenza active in community | Influenza, S. pneumoniae, Staphylococcus aureus, H. influenzae |
| Cough >2 weeks with whoop or posttussive vomiting | Bordetella pertussis |
| Structural lung disease (e.g., bronchiectasis) | P. aeruginosa, Burkholderia cepacia, S. aureus |
| Injection drug use | S. aureus, anaerobes, M. tuberculosis, S. pneumoniae |
| Endobronchial obstruction | Anaerobes, S. pneumoniae, H. influenzae, S. aureus |
| In context of bioterrorism | Bacillus anthracis (anthrax), Yersinia pestis (plague), F. tularensis (tularemia) |
COPD, Chronic obstructive pulmonary disease; CA-MRSA, community-associated methicillin-resistant Staphylococcus aureus; HIV, human immunodeficiency virus; SARS, severe acute respiratory syndrome.
Adapted from Mandell LA, Wunderink RG, Anzueto A, et al: Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults, Clin Infect Dis 44(suppl 2):S27-S72, 2007.
For outpatients, empirical therapy with a macrolide, doxycycline, antipneumococcal fluoroquinolone (e.g., levofloxacin, gemifloxacin, moxifloxacin), or the combination of a β-lactam plus macrolide are recommended treatment options based on risk factors of recent antimicrobial use and comorbidities. For general inpatient treatment, combination therapy with a β-lactam such as cefotaxime, ceftriaxone, ertapenem, or ampicillin-sulbactam plus azithromycin or monotherapy with a respiratory fluoroquinolone is recommended. For patients with severe CAP requiring ICU admission, recommendations are given based on risks for Pseudomonas and/or CA-MRSA. Pseudomonas is an uncommon cause of CAP but should be considered with the following risk factors: history of bronchiectasis or advanced chronic obstructive pulmonary disease with frequent use of antimicrobials or steroids. If CA-MRSA is a consideration, linezolid or vancomycin should be added to the regimen. Although methicillin-resistant strains of S. aureus are still the minority, the excess mortality of inappropriate antibiotic therapy would suggest that empirical coverage should be considered when CA-MRSA is a concern. The best indicator of S. aureus is the presence of gram-positive cocci in clusters in a tracheal aspirate or adequate sputum sample (see Figure 26-2). Clinical risk factors for S. aureus CAP include end-stage renal disease, intravenous drug abuse, prior influenza, and prior antibiotics (especially fluoroquinolones).
Pathogen-Directed Therapy
Treatment options are obviously simplified if the causative agent is established or strongly suspected (Box 26-3 ). Diagnostic procedures that provide identification of a specific cause within 24 to 72 hours can still be useful for guiding continued therapy. If, for example, an appropriate culture reveals the isolation of penicillin-susceptible S. pneumoniae, therapy can be specified by selecting a narrow-spectrum agent (such as penicillin or amoxicillin). This will hopefully reduce the selective pressure for resistance. This information is often available at the time of switch from parenteral to oral therapy and may be used to direct specific antimicrobial choices.
Box 26-3. Recommended Empirical Antibiotics for Community-Acquired Pneumonia.
Outpatient Treatment
-
1Previously healthy and no use of antimicrobials within the previous 3 months:
-
•A macrolide
-
•Doxycycline
-
•
-
2Presence of comorbidities or use of antimicrobials within the previous 3 months (in which case an alternative from a different class should be selected):
-
•Respiratory fluoroquinolone (moxifloxacin, gemifloxacin, levofloxacin [750 mg])
-
•β-Lactam plus a macrolide
-
•
-
3
In regions with a high rate (>25%) of high-level (minimum inhibitory concentration [MIC] ≥16 mcg/mL) macrolide-resistant Streptococcus pneumoniae, consider use of alternative agents listed above in 2 for patients without comorbidities.
Inpatients, Non–Intensive Care Unit Treatment
-
•
Respiratory fluoroquinolone
-
•
β-Lactam plus a macrolide
Inpatients, Intensive Care Unit Treatment
-
•
A β-lactam (cefotaxime, ceftriaxone, ampicillin-sulbactam) plus either azithromycin or a respiratory fluoroquinolone (for patients allergic to penicillin, a respiratory fluoroquinolone and aztreonam are recommended).
Special Concerns
-
1If Pseudomonas is a consideration (risk factors include bronchiectasis and chronic obstructive pulmonary disease with frequent antimicrobial or steroid use):
-
•An antipneumococcal, antipseudomonal β-lactam (piperacillin-tazobactam, cefepime, imipenem, meropenem) plus either ciprofloxacin or levofloxacin (750-mg dose)
-
•The above β-lactam plus an aminoglycoside and azithromycin
-
•The above β-lactam plus an aminoglycoside and an antipneumococcal fluoroquinolone (for patients allergic to penicillin, substitute aztreonam for above β-lactam)
-
•
-
2
If community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) is a consideration, add linezolid or vancomycin.
Adapted from Mandell LA, Wunderink RG, Anzueto A, et al: Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults, Clin Infect Dis 44(suppl 2):S27-S72, 2007.
Duration of Therapy
Patients should be treated for a minimum of 5 days as long as they have been afebrile for 48 to 72 hours and are clinically stable relative to baseline status. A longer duration of therapy is recommended for patients with bacteremic S. aureus pneumonia because of the risks for associated endocarditis and deep-seated infection; patients with extrapulmonary infection (especially meningitis); patients with P. aeruginosa pneumonia; and patients with infection caused by less common pathogens. Potential benefits of therapy shorter than 10 days include improvement of patient compliance and reduction of microbial resistance, cost, and adverse events such as Clostridium difficile infections.
Prognosis
In most patients fever is reduced within 3 to 4 days of therapy; however, cough and fatigue will often persist for several weeks even in patients with mild disease. Symptoms can be expected to last longer in more seriously ill patients. Such information should be imparted to patients for better awareness of their illness and anticipated clinical course.
Up to 15% of patients may not respond appropriately to initial antibiotic therapy. Nonresponse can be defined as absence or delay in achieving clinical stability within several days or actual clinical deterioration. A number of possibilities, both infectious and noninfectious, should be considered (Table 26-3 ). A systematic assessment of patients should take these considerations into account. The most common causes of treatment failure are lack of or delayed response by the host despite appropriate antibiotics and infection with an organism that is not covered by the initial antibiotic regimen. Antibiotic changes in this time period should be considered only for patients with deterioration or in whom new culture data or epidemiologic clues suggest alternative causes.
Table 26-3.
Recommended Antimicrobial Therapy for Specific Pathogensa
| ORGANISM | PREFERRED ANTIMICROBIAL(S) | ALTERNATIVE ANTIMICROBIAL(S) |
|---|---|---|
| Streptococcus pneumoniae, penicillin nonresistant (MIC <2 mcg/mL) | Penicillin G; amoxicillin | Macrolide; cephalosporins (oral—cefpodoxime, cefprozil, cefuroxime, cefdinir, cefditoren; parenteral—cefuroxime, ceftriaxone, cefotaxime); clindamycin; doxycycline; respiratory fluoroquinoloneb |
| S. pneumoniae, penicillin resistant (MIC ≥2 mcg/mL) | Agents based on susceptibility, including cefotaxime, ceftriaxone, fluoroquinolone | Vancomycin, linezolid, high-dose amoxicillin (3 g/day with penicillin MIC ≤4 mcg/mL) |
| Haemophilus influenzae | Non–β-lactamase producing: amoxicillin β-lactamase producing: second- or third-generation cephalosporin; amoxicillin-clavulanate |
Fluoroquinolone; doxycycline; azithromycinc; clarithromycind |
| Mycoplasma pneumoniae or Chlamydophila pneumoniae | Macrolide; a tetracycline | Fluoroquinolone |
| Legionella species | Fluoroquinolone; azithromycin | Doxycycline |
| Chlamydia psittaci | A tetracycline | Macrolide |
| Coxiella burnettii | A tetracycline | Macrolide |
| Francisella tularensis | Doxycycline | Gentamicin, streptomycin |
| Yersinia pestis | Streptomycin, gentamicin | Doxycycline, fluoroquinolone |
| Anthrax (inhalation) | Ciprofloxacin, levofloxacin, doxycycline (usually with second agent) | Other fluoroquinolones; β-lactam, if susceptible; rifampin; clindamycin; chloramphenicol |
| Enterobacteriaceae | Third-generation cephalosporin; carbapenemd (drug of choice if extended-spectrum β-lactamase producer) | β-lactam or β-lactamase inhibitore; fluoroquinolone |
| Pseudomonas aeruginosa | Antipseudomonal β-lactamfplus ciprofloxacin or levofloxacing or aminoglycoside | Aminoglycoside plus (ciprofloxacin or levofloxacing) |
| Burkholderia pseudomallei | Carbapenem, ceftazidime | Fluoroquinolone, TMP-SMX |
| Acinetobacter species | Carbapenem | Cephalosporin-aminoglycoside, ampicillin-sulbactam, colistin |
|
Staphylococcus aureus: Methicillin susceptible Methicillin resistant |
Antistaphylococcal penicillinh Vancomycin or linezolid |
Cefazolin; clindamycin TMP-SMX |
| Bordetella pertussis | Macrolide | TMP-SMX |
| Anaerobe (aspiration) | β-lactam or β-lactamase inhibitore; clindamycin | Carbapenem |
| Influenza | Oseltamivir or zanamivir | |
| Mycobacterium tuberculosis | Isoniazid plus rifampin plus ethambutol plus pyrazinamide | Refer to American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America guidelines for specific recommendations |
| Coccidioides species | Uncomplicated infection in normal host—no therapy generally recommended; For therapy—itraconazole, fluconazole |
Amphotericin B |
| Histoplasmosis | Itraconazole | Amphotericin B |
| Blastomycosis | Itraconazole | Amphotericin B |
MIC, Minimum inhibitory concentration; TMP-SMX, trimethoprim-sulfamethoxazole.
Choices should be modified based on susceptibility test results and advice from local specialists. Refer to local references for appropriate doses.
Levofloxacin, moxifloxacin, gemifloxacin (not a first-line choice for penicillin-susceptible strains); ciprofloxacin is appropriate for Legionella and most gram-negative bacilli (including H. influenzae).
Azithromycin more active in vitro than clarithromycin for H. influenzae.
Imipenem-cilastatin, meropenem, ertapenem.
Piperacillin-tazobactam for gram-negative bacilli; ticarcillin-clavulanate; ampicillin-sulbactam or amoxicillin-clavulanate.
Ticarcillin, piperacillin, ceftazidime; cefepime, aztreonam, imipenem, meropenem.
750 mg qd.
Nafcillin, oxacillin, flucloxacillin.
Adapted from Mandell LA, Wunderink RG, Anzueto A, et al: Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults, Clin Infect Dis 44(suppl 2):S27-S72, 2007.
Prevention
Vaccines targeting pneumococcal disease and influenza are a mainstay for preventing CAP. Pneumococcal polysaccharide vaccine and inactivated or live-attenuated influenza vaccine should be considered for all patients according to recent recommendations from the Centers for Disease Control and Prevention (CDC). Chemoprophylaxis (i.e., oseltamivir or zanamivir), can be used as an adjunct to influenza vaccination. Clinicians should also intervene to modify some of the associated risk factors for pneumonia in adults. Because smoking is a significant risk factor for CAP, smoking cessation should be attempted; this is particularly important and relevant when patients are hospitalized for pneumonia. In addition, stabilization of underlying conditions (e.g., congestive heart failure, diabetes) and promotion of appropriate nutrition may help to reduce the risk of CAP and thereby promote longer and healthier lives.
Additional Resources
- Centers for Disease Control and Prevention (CDC) Recommendedadult immunization schedule—United States, 2009. MMWR QuickGuide. 2008;57:Q-1–Q-4. www.cdc.gov/mmwr/PDF/wk/mm5753-Immunization.pdf Available at. Accessed April 1, 2009. This article contains 2009 recommendations for adult immunization schedule from the CDC. [Google Scholar]
- Infectious Diseases Society of America (IDSA) Position paper: recommended design features of future clinical trials of antibacterial agents for community-acquired pneumonia. Clin Infect Dis. 2008;47(suppl 3):S249. Evidence-based position paper for evaluation of antimicrobial trials for CAP. [PMC free article] [PubMed] [Google Scholar]
- Joint Commission of Accreditation of Healthcare Organizations A comprehensive review of development and testing for national implementation of hospital core measures. 2009. www.jointcommission.org/NR/rdonlyres/48DFC95A-9C05-4A44-AB05-1769D5253014/0/AComprehensiveReviewofDevelopmentforCoreMeasures.pdf Available at Accessed April 1. A comprehensive review of performance measures for patients admitted to the hospital. This includes a review of the specific measures for pneumonia.
- Mandell LA, Wunderink RG, Anzueto A. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S27–S72. doi: 10.1086/511159. A comprehensive, evidence-based set of recommendations regarding the diagnosis and management of adults with CAP. [DOI] [PMC free article] [PubMed] [Google Scholar]
Evidence
- Aujesky D, Fine MJ. The pneumonia severity index: a decade after the initial derivation and validation. Clin Infect Dis. 2008;47(suppl 3):S133. doi: 10.1086/591394. An update of appropriate use of the pneumonia prediction rule. [DOI] [PubMed] [Google Scholar]
- File TM., Jr Clinical implications and treatment of multiresistant Streptococcus pneumoniae pneumonia. Clin Microbiol Infect. 2006;12(suppl 3):31–41. doi: 10.1111/j.1469-0691.2006.01395.x. A useful review and treatment recommendations of the clinical relevance of drug-resistant S. pneumoniae. [DOI] [PubMed] [Google Scholar]
- File TM., Jr Community-acquired pneumonia. Lancet. 2003;362:1991–2001. doi: 10.1016/S0140-6736(03)15021-0. A comprehensive review of the management of CAP. [DOI] [PMC free article] [PubMed] [Google Scholar]
- File TM., Jr Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122:130–141. doi: 10.3810/pgm.2010.03.2130. An update of economic cost associated with community-acquired pneumonia. [DOI] [PubMed] [Google Scholar]
- Fine MJ, Auble TE, Yealy DM. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997;336:243–250. doi: 10.1056/NEJM199701233360402. An overview of the development and use of the prediction rule, based on severity of illness, for mortality. [DOI] [PubMed] [Google Scholar]
- Lim WS, van der Eerden MM, Laing R. Defining community-acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58:377–382. doi: 10.1136/thorax.58.5.377. An overview of the development and use of the CURB-65 severity of illness model. This is based on five factors: confusion, urea nitrogen, respiratory rate, blood pressure, and age >65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menéndez R, Torres A, Rodríguez de Castro F. Reaching stability in community-acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783. doi: 10.1086/426028. A prospective evaluation of the response to therapy based on severity of illness, treatment, and characteristics of patients. Risk factors for treatment failure included the presence of liver disease, severity of illness, and multilobar pneumonia. [DOI] [PubMed] [Google Scholar]
- Niederman MS. Recent advances in community-acquired pneumonia: inpatient and outpatient. Chest. 2007;131:1205. doi: 10.1378/chest.06-1994. A concise review of advances in the management of CAP. [DOI] [PMC free article] [PubMed] [Google Scholar]