

Abstract
Background
Non-adherence to oral maintenance therapy in adolescents with inflammatory bowel disease (IBD) is a significant healthcare problem. Knowledge of the prescribed medication can increase medication adherence. We aimed to investigate the relationship between medication adherence and disease-related knowledge of pediatric and adolescent patients with IBD.
Methods
We conducted a “pop quiz” to investigate the disease-related knowledge of pediatric patients with IBD who were followed-up at our institution and reviewed their medical records, including data on sex, diagnosis, age at diagnosis, and disease duration. Medication adherence was evaluated by the doctor in charge, and ≥ 80% of patients constituted the “good adherence group.”
Results
Of 93 patients, 59 (63.4%) were males, and 78 (83.9%) had Crohn's disease. The mean age at diagnosis was 13.8 ± 2.8 years; mean follow-up duration, 4.8 ± 3.4 years; and mean patient age, 18.6 ± 3.7 years. Only 65 patients (69.9%) knew the exact name of the medication they were currently taking, and 34 (36.6%) knew the correct dose. Only 15 patients (16.1%) knew the name of the medications they were previously taking. A total of 64 patients (66.8%) showed an adherence rate of 80% for the weekly prescribed oral medication. The patients in the poor adherence group were significantly older than those in the good adherence group (P = 0.035). The number of hospitalizations per year was statistically higher in the good adherence group (P = 0.024). The proportion of patients who knew the names of the medications they were previously taking and were aware of the side effects of the medications was significantly higher in the good adherence group (P = 0.008 and P = 0.020, respectively).
Conclusion
Adolescent IBD patients have lower oral medication adherence. Knowledge of the prescribed medications taken previously, and the adverse effects of these medications are associated with good adherence. IBD specialists should educate the patients regarding the disease and about their medication.
Keywords: Inflammatory Bowel Disease, Pediatric, Adherence, Knowledge
Graphical Abstract
INTRODUCTION
Inflammatory bowel disease (IBD) is a chronic gastrointestinal inflammation, including Crohn's disease (CD) and ulcerative colitis (UC). It is a life-long idiopathic disorder, and the etiology is unknown.1 The data from the descriptive epidemiology in Japan and Korea show that IBD initially presents during childhood and adolescence in approximately 25% of patients, and the incidence appears to be increasing.2,3 Despite the development of various therapeutic strategies, patients with IBD require lifelong treatment because patients with this disease frequently experience intermittent remissions and unpredictable relapse. Appropriate treatment is critical for intestinal and extraintestinal disease control. After inducing clinical remission of IBD, the emphasis of management shifts is to maintain a symptom-free remission and reduce disease flares through close adherence to one or more maintenance medications typically taken on a daily basis.2,3
In clinical practice, however, a large number of patients are non-adherent to their prescribed medications, and the increasing number of hospital admissions as a result of disease “flare-ups” has a negative impact on the healthcare service utilization, with an overall increase in healthcare costs. A systemic review of previous studies with pediatric and adult IBD participants reported a non-adherence to oral medication rate of 2%–72%.4 Non-adherence to oral maintenance therapy in adolescents with IBD is a significant healthcare problem and can lead to unnecessary escalation of therapy.4 A number of studies indicated that non-adherence to treatment may be associated with a variety of factors, including biological, social, economic, psychological, and emotional factors.5,6 For this reason, various interventions were implemented, such as patient education, to improve adherence, and a number of studies have shown that providing disease-related knowledge to patients effectively increased treatment adherence.7,8 Therefore, it may not be surprising that provision of disease-related education among pediatric patients with chronic diseases such as diabetes, asthma, and IBD is widely accepted. In particular, knowledge on the prescribed medication is an important step in the self-management process; some experts believe that this can occur during childhood or early adolescence, because it is a concrete and tangible accomplishment.9 Nonetheless, the number of current literature reporting the effects of medication-related knowledge and characteristics of pediatric patients with IBD are limited.10
We aimed to investigate the relationship between medication adherence and disease-related knowledge of pediatric patients with IBD from a region in Korea. We aimed to focus on knowledge about the prescribed medications and adverse effects among pediatric populations.
METHODS
Study designs and participants
The IBD Clinic at Pusan National University Children's Hospital conducted a “pop quiz” in the summer of 2018 during their routine treatment to determine the patients' level of knowledge on drugs for IBD. The “pop test” was conducted with the aim of educating patients about their prescribed medications. In the outpatient clinic, patients solved the “pop quiz” before the clinic time. Patients were given 30 minutes or more to take the quiz comfortably. Then, two pediatric gastroenterologists checked the patients' response to the pop quiz during clinic time and educated the patient about their medications according to the score.
We enrolled all patients who answered the “pop quiz.” From the electronic medical records (EMRs), we identified their baseline characteristics including sex, diagnosis, age at diagnosis, and disease duration. Data on the prescribed medications, the number of hospitalizations, endoscopic examinations, and history of surgical treatment were also collected. The information obtained through this “pop quiz” and those obtained from the EMR were retrospectively analyzed.
“Pop quiz” contents
The “pop quiz” consisted of four questions, which assess the patients' knowledge regarding their medications: 1) the name of the medication they are currently taking (and correct dosage), 2) the name of the medication previously taken, 3) the name of the biologic drug (if using a biologic drug), and 4) the adverse effects of the medication taking or previously taken. The responses to questions 1 and 2 of the quiz were rated using a 100-point scale; all patient's responses were compared with the actual prescription in the EMR. For example, if a patient wrote down only azathioprine, and the patient was prescribed azathioprine and steroids, their score was 50. However, the response of question 4 related to the medication' adverse effect was categorized into two groups: if patients remembered two or more correct side effects related to the medication they were taking (or had taken), they were categorized into a good group. For example, if patients who were taking steroids and 5-aminosalicylic acid wrote down “skin rash,” “nausea,” or “anemia,” they were categorized into the good group.
Medication adherence
After the “test”, the doctor in charge met their patient and evaluated the medication adherence of each patient (or parents). All patients were asked to report the amount of medication they took since the last clinic visit, and the doctor in charge validated this during the clinic visit. The amount of medications actually taken were expressed in percentage. Of the total patients, ≥ 80% were classified as “good adherence group.” Since the use of biologic drugs was not considered as a form of self-medication, it was excluded from the analysis of adherence.
Statistics
Descriptive data such as a sex, type of IBD, age at diagnosis, and disease duration were expressed as means, standard deviations, and frequencies. After dividing patients into two groups (good adherence group and poor adherence group), the relationships between group and clinical characteristics were analyzed. The relationships between group and knowledge on prescribed medications obtained from the “pop quiz” were also analyzed.
An independent t-test was used to analyze continuous variables, while χ2 test or Fisher's exact test was used to analyze categorical variables. All statistical analyses were performed using SPSS statistical package version 21.0 for Windows (SPSS Inc., Chicago, IL, USA). A P value of < 0.05 was considered significant.
Ethics statement
This study was conducted after receiving approval from the Institutional Review Board (IRB) of Pusan National University Yangsan Hospital (05-2019-003). This study was a retrospective study of medical records and approved by the IRB for waiver of informed consent.
RESULTS
Study population
A total of 93 patients completed the pop quiz. The baseline characteristics are summarized in Table 1. A total of 59 patients (63.4%) were men, and 78 (83.9%) were diagnosed with CD. The mean age at diagnosis was 13.8 ± 2.8 years, and the mean duration of follow-up was 4.8 ± 3.4 years; the mean age of the patients was 18.6 ± 3.7 years, and 34 patients (36.6%) were aged over 20 years. The mean number of hospitalization was 2.5 ± 1.7 times. For patients who were diagnosed with IBD at the age of 6 months or above, the mean number of hospitalizations per year was 0.8 ± 0.9 times. The mean number of and the total number of endoscopic examinations per year were 4.3 ± 1.5 and 1.3 ± 1.1 times, respectively. Lastly, a total of 36 (38.7%) patients underwent surgery.
Table 1. Baseline characteristics of patients (n = 93).
| Characteristics | Values | |
|---|---|---|
| Male sex | 59 (63.4) | |
| Diagnosis | ||
| CD | 78 (83.9) | |
| UC | 15 (16.1) | |
| Age at diagnosis, yr | 13.8 ± 2.8 | |
| Age at interview, yr | 18.6 ± 3.7 | |
| < 20 | 59 (63.4) | |
| ≥ 20 | 34 (36.6) | |
| Duration of follow-up, yr | 4.81 ± 3.4 | |
| Medical history | ||
| 5-aminosalicylic acid, sulfasalazine or mesalamine | 93 (100) | |
| Steroid | 89 (95.7) | |
| Immunomodulator, azathioprine or methotrexate | 68 (73.1) | |
| Biologic, infliximab or adalimumab | 55 (59.1) | |
| No. of hospitalizations | 2.5 ± 1.7 | |
| No. of hospitalizations/yr (n = 87)a | 0.8 ± 0.9 | |
| No. of endoscopic examinationsb | 4.3 ± 1.5 | |
| No. of endoscopic examinations/yr (n = 87)a | 1.3 ± 1.1 | |
| No. of patients who underwent surgery | 36 (38.7) | |
Values are presented as number (%) or mean ± standard deviation.
CD = Crohn's disease, UC = ulcerative colitis.
aSix patients with a follow-up of less than 6 months were excluded; bEndoscopic examinations include duodenofibroscopy, capsule endoscopy, and colonoscopy.
Level of knowledge on prescribed medications
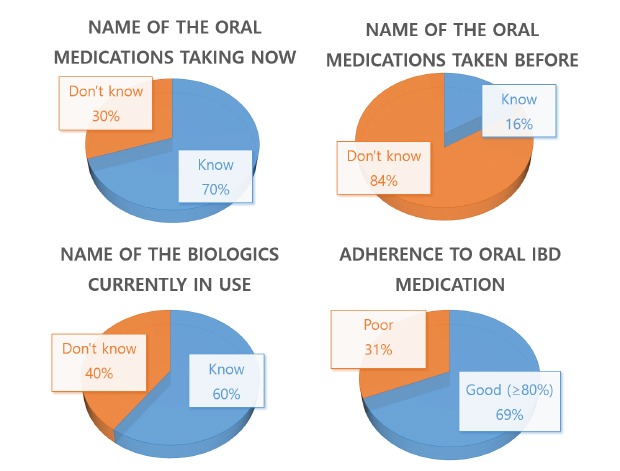
Only 65 patients (69.9%) knew the exact name of the medication they are currently taking, while 34 (36.6%) knew the correct dose. Only 15 patients (16.1%) knew the name of the medications they were previously taking. Among the 55 patients using biologic drugs, 33 (66.0%) knew the correct brand name of the medication. Twenty-one patients (22.6%) answered that they knew one or more adverse effects associated with the medications that they were taking (Table 2).
Table 2. Knowledge on prescribed medication (n = 93).
| Variables | No. of patients with knowledge on the below mentioned variables (%) | |
|---|---|---|
| Name of the medications taking now | 65 (69.9) | |
| Correct dosage of the medication | 34 (36.6) | |
| Name of the medications taken before | 15 (16.1) | |
| Name of biologic drugs (if using a biologic drug) (n = 55)a | 33 (60.0) | |
| Adverse effects of medications previously taken | 21 (22.6) | |
aTotal number of patients who used biologic drugs was 55 (59.1%).
Relationships between clinical characteristics, knowledge, and medication adherence
Sixty-four patients (66.8%) had taken more than 80% of prescribed oral medications every week (Table 3). The average age of the poor adherence group was significantly higher than the good adherence group (P = 0.035). The number of hospitalizations per year was statistically higher in the good adherence group (P = 0.024) (Table 4). In addition, although we analyzed the correlation between the number of surgeries and the location and behavior of the disease to estimate disease activity, statistically significant results of adherence were not observed. The proportion of patients who knew the names of the drugs they were previously taking and that of patients who knew the side effects of the drugs were significantly higher in the good adherence group (P = 0.008 and P = 0.020, respectively) (Table 5). The number of patients with UC (40%) who had poor adherence to medications was higher than that of patients with CD (29.5%), but not statistically significant (Table 6).
Table 3. Adherence to medicationsa (n = 93).
| Adherences | Values |
|---|---|
| Good, ≥ 80% | 64 (68.8) |
| Poor, < 80% | 29 (31.2) |
Values are presented as number (%).
aBiologic drugs were excluded from the analysis of adherence.
Table 4. Characteristics associated with medication adherence.
| Variables | Good adherence (n = 64) | Poor adherence (n = 29) | P value | |
|---|---|---|---|---|
| Male sex | 40 (63.5) | 19 (65.5) | 0.782 | |
| CD | 55 (87.3) | 23 (79.3) | 0.426 | |
| Age at diagnosis, yr | 13.2 ± 2.7 | 13.7 ± 3.1 | 0.343 | |
| Age at interview, yr | 17.6 ± 4.0 | 19.4 ± 3.1 | 0.035 | |
| Duration of follow-up, yr | 4.7 ± 3.3 | 5.7 ± 3.4 | 0.215 | |
| No. of hospitalizations | 2.5 ± 1.9 | 2.4 ± 1.2 | 0.693 | |
| No. of hospitalizations/yr (n = 87)a | 0.8 ± 1.0 | 0.6 ± 0.4 | 0.024 | |
| No. of endoscopic examinations | 4.3 ± 1.5 | 4.5 ± 1.4 | 0.484 | |
| No. of endoscopic examinations/yr (n = 87)a | 1.4 ± 1.2 | 1.1 ± 0.9 | 0.322 | |
| No. of patients who underwent surgery | 0.6 ± 0.8 | 0.7 ± 1.1 | 0.536 | |
Values are presented as number (%), mean ± standard deviation.
CD = Crohn's disease
aSix patients with a follow-up of less than 6 months were excluded.
Table 5. Knowledge of medication associated with adherence.
| Variables | Good adherence (n = 64) | Poor adherence (n = 29) | P value | |
|---|---|---|---|---|
| Name of the medications currently taken | 73.44 ± 42.7a | 68.97 ± 47.1a | 0.652 | |
| Correct dosage of the medication | 27 (42.9) | 7 (24.1) | 0.082 | |
| Name of the medications previously taken | 42.39 ± 36.9a | 20.62 ± 33.1a | 0.008 | |
| Name of biologics (if using biologic drugs) (n = 55)b | 25 (39.7) | 8 (27.6) | 0.260 | |
| Adverse effects of medications | 18 (28.6) | 3 (10.3) | 0.020 | |
Values are presented as number (%), mean ± standard deviation.
aValues are presented using a 100-point scale; bTotal number of patients who used biologic drugs was 55 (59.1%).
Table 6. Diagnosis and medication adherence (n = 93).
| Variables | Adherence of medications | Total | χ2 | ||
|---|---|---|---|---|---|
| Good | Poor | ||||
| Diagnosis | 0.648 | ||||
| CD | 55 (70.5) | 23 (29.5) | 78 (100.0) | ||
| UC | 9 (60.0) | 6 (40.0) | 15 (100.0) | ||
| Total | 64 | 29 | 93 | ||
Values are presented as number (%).
CD = Crohn's disease, UC = ulcerative colitis.
DISCUSSION
Non-adherence to prescribed medications of patients is among the challenges in the treatment of IBD. In this retrospective analysis, a relatively large number of pediatric and adolescent patients with IBD had a low adherence to prescribed medications. Similar to the results of previous studies,4,11,12 only 66.8% of patients took more than 80% of the medications. Moreover, the older age group had lower adherence to prescribed medications than the pediatric group. A study conducted in adults with IBD showed that non-adherence was significantly associated with age below 30 years.10 In another pilot study, the non-adherence rates of young adults (age, 18–25 years) and pediatric patients (age, 12–18 years) were 17% and 5%, respectively.13 Patients aged below 12 years had better medication adherence than teens, which may be due to the greater reliance on parents to administer the medications.14 This finding suggests that the parent's role is important in pediatric patients, and special care should be taken to increase the medication adherence among adolescent IBD patients.
In this study, we only targeted outpatients during the same period, so the results showed a relatively high proportion of patients who used biologics because patients who took biologics were required to visit the hospital regularly. An adult study from Italy showed that adults being treated with biologics had an adherence of 94.9%, which is better than those who were treated with oral treatment.15 On the other hand, in a systematic review of adult IBDs, even patients receiving anti-tumor necrosis factor (TNF) therapy showed an adherence of only 82.6%.16 In our study, whether patients used biologics (anti-TNFs) or not did not influence oral medication adherence (67.3% vs. 71.1%). A previous adult study from Portugal also showed a similar result.17
In this study, the high average number of hospitalizations per year was associated with good medication adherence. The frequency of admission may be an indicator of disease exacerbation. Disease aggravation is known to have an effect on medication adherence.5,6 Inpatients receive sufficient care from doctors and nurses, and have more time to be educated about the disease itself and their medications. This may increase the medication adherence among patients who are frequently hospitalized. Meanwhile, one study conducted in an outpatient setting reported no association between frequency of clinic visits and medication adherence or outcome in children with IBD.18 Moreover, in chronic disorders, fixed outpatient clinic appointments result in inefficiencies in healthcare services and inconvenience for patients, as well as high rates of noncompliance.19 Patients with IBD, like other chronic diseases, are managed by a specialist during regular clinic follow-up visits. This suggests that more efficient programs to promote increasing medication adherence should be developed in the outpatient setting.
We found out that the knowledge about prescribed medications previously taken and the adverse effects of medications was associated with good adherence among pediatric patients with IBD. The majority of those who knew the names of the medications that they were prescribed in the past also knew the names of the medications they were currently taking. We estimate this difference in knowledge as a degree of concern or interest for the disease or medication rather than the intellectual ability of the patient. Several previous studies reported a number of factors that affect medication adherence in patients with chronic illness, such as age, culture, education and socioeconomic status, family structure, and even taste; however, previous studies show that the contents are somewhat contradictory.10,19,20 Among these many factors, patients' knowledge about their prescribed medications is the very important factor that can improve treatment adherence among IBD patients.10 Not only knowledge related to medication, many other studies reported that providing patients with disease-related knowledge had a good impact on improving treatment compliance.7,12,21 Furthermore, knowledge on prescribed medication can be part of the early stage of self-management among adolescent patients with IBD.22 However, like our study, many adolescents were not aware of the dosage of IBD drugs and were not aware of the adverse effects of the drugs.22 To promote medication adherence and improve patient progress, patients should be educated about the medication prescribed to them. In patients who were non-adherent to treatment, a single personalized counseling session with an IBD pharmacist has been shown to effectively increase medication adherence by the second year.23 Due to the limited hospital resources, especially the number of physicians, it is necessary to determine other methods of improving the quality of treatment of patients using a multidisciplinary approach.
The present study does have some limitations. This study analyzed the patients' responses to the “pop quiz” performed during the course of care in a care setting where only two gastroenterologists were assigned to treat a large number of pediatric IBD patients. We focused only on the patients' level of knowledge on the prescribed medication, among the many factors known to affect medication adherence. Additionally, all patients except four were taking two or more drugs, though we did not quantify for adherence and knowledge to individual drugs. The “pop quiz” was conducted using a not well-quantitatively designed questionnaire, which may have influenced the results. Moreover, prejudice may also exist as the patients relied solely on their memory to answer all questions in the pop quiz. However, in our study, all answers were checked directly by the individual attending gastroenterologist, assuming that the information obtained during the clinic time would be relatively more accurate than those obtained from a simple “pop quiz.” Finally, the patients were not analyzed according to the disease itself or the severity of the disease, since most of them were in remission at the time of investigation. Beginning with this study, we hope this is the basis for a large-scale study that investigates the effects of other or multiple factors on adherence.
In conclusion, pediatric IBD specialists should educate patients not only about the disease itself but also the importance of adherence to medications, which may increase adherence to medications and control their diseases. We are confident that this study will be an important resource for the development of future educational programs. As the results of similar studies accumulate, it is necessary to develop a special education program for pediatric patients with IBD to improve medication adherence, especially in the outpatient setting.
Footnotes
Disclosure: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Lee YJ.
- Data curation: Lee YJ, Lim JK.
- Formal analysis: Lee YJ, Lim JK.
- Methodology: Lee YJ, Lim JK.
- Writing - original draft: Lim JK.
- Writing - review & editing: Lee YJ, Park JH.
References
- 1.Podolsky DK. Inflammatory bowel disease. N Engl J Med. 2002;347(6):417–429. doi: 10.1056/NEJMra020831. [DOI] [PubMed] [Google Scholar]
- 2.Lee HA, Suk JY, Choi SY, Kim ER, Kim YH, Lee CK, et al. Characteristics of pediatric inflammatory bowel disease in Korea: comparison with EUROKIDS data. Gut Liver. 2015;9(6):756–760. doi: 10.5009/gnl14338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yang SK, Yun S, Kim JH, Park JY, Kim HY, Kim YH, et al. Epidemiology of inflammatory bowel disease in the Songpa-Kangdong district, Seoul, Korea, 1986–2005: a KASID study. Inflamm Bowel Dis. 2008;14(4):542–549. doi: 10.1002/ibd.20310. [DOI] [PubMed] [Google Scholar]
- 4.Spekhorst LM, Hummel TZ, Benninga MA, van Rheenen PF, Kindermann A. Adherence to oral maintenance treatment in adolescents with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2016;62(2):264–270. doi: 10.1097/MPG.0000000000000924. [DOI] [PubMed] [Google Scholar]
- 5.Moradkhani A, Kerwin L, Dudley-Brown S, Tabibian JH. Disease-specific knowledge, coping, and adherence in patients with inflammatory bowel disease. Dig Dis Sci. 2011;56(10):2972–2977. doi: 10.1007/s10620-011-1714-y. [DOI] [PubMed] [Google Scholar]
- 6.Kane SV. Systematic review: adherence issues in the treatment of ulcerative colitis. Aliment Pharmacol Ther. 2006;23(5):577–585. doi: 10.1111/j.1365-2036.2006.02809.x. [DOI] [PubMed] [Google Scholar]
- 7.Hawthorne AB, Rubin G, Ghosh S. Review article: medication non-adherence in ulcerative colitis--strategies to improve adherence with mesalazine and other maintenance therapies. Aliment Pharmacol Ther. 2008;27(12):1157–1166. doi: 10.1111/j.1365-2036.2008.03698.x. [DOI] [PubMed] [Google Scholar]
- 8.Sood A, Midha V, Sood N, Kaushal V. Self-reported disease awareness--a questionnaire survey of ulcerative colitis patients. Indian J Gastroenterol. 2001;20(1):6–8. [PubMed] [Google Scholar]
- 9.Baldassano R, Ferry G, Griffiths A, Mack D, Markowitz J, Winter H. Transition of the patient with inflammatory bowel disease from pediatric to adult care: recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2002;34(3):245–248. doi: 10.1097/00005176-200203000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Tae CH, Jung SA, Moon HS, Seo JA, Song HK, Moon CM, et al. Importance of patients' knowledge of their prescribed medication in improving treatment adherence in inflammatory bowel disease. J Clin Gastroenterol. 2016;50(2):157–162. doi: 10.1097/MCG.0000000000000431. [DOI] [PubMed] [Google Scholar]
- 11.Hommel KA, Davis CM, Baldassano RN. Objective versus subjective assessment of oral medication adherence in pediatric inflammatory bowel disease. Inflamm Bowel Dis. 2009;15(4):589–593. doi: 10.1002/ibd.20798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cervený P, Bortlík M, Kubena A, Vlcek J, Lakatos PL, Lukás M. Nonadherence in inflammatory bowel disease: results of factor analysis. Inflamm Bowel Dis. 2007;13(10):1244–1249. doi: 10.1002/ibd.20189. [DOI] [PubMed] [Google Scholar]
- 13.Jeganathan J, Lee CH, Rahme A, Tiao DK, Weston C, Dutt S, et al. IBD clinical. Medication adherence in transitional inflammatory bowel disease patients: a multi-center pilot study. J Gastroenterol Hepatol. 2014;29(S2):111. [Google Scholar]
- 14.LeLeiko NS, Lobato D, Hagin S, McQuaid E, Seifer R, Kopel SJ, et al. Rates and predictors of oral medication adherence in pediatric patients with IBD. Inflamm Bowel Dis. 2013;19(4):832–839. doi: 10.1097/MIB.0b013e3182802b57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bucci C, Zingone F, Tammaro S, Iovino P, Santonicola A, Ciacci C. Factors predicting the adherence to the therapy of Italian IBD patients. Gastroenterol Res Pract. 2017;2017:6719345. doi: 10.1155/2017/6719345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lopez A, Billioud V, Peyrin-Biroulet C, Peyrin-Biroulet L. Adherence to anti-TNF therapy in inflammatory bowel diseases: a systematic review. Inflamm Bowel Dis. 2013;19(7):1528–1533. doi: 10.1097/MIB.0b013e31828132cb. [DOI] [PubMed] [Google Scholar]
- 17.Campos S, Portela F, Sousa P, Sofia C. Inflammatory bowel disease: adherence to immunomodulators in a biological therapy era. Eur J Gastroenterol Hepatol. 2016;28(11):1313–1319. doi: 10.1097/MEG.0000000000000704. [DOI] [PubMed] [Google Scholar]
- 18.Kluthe C, Tsui J, Spady D, Carroll M, Wine E, Huynh HQ. The frequency of clinic visits was not associated with medication adherence or outcome in children with inflammatory bowel diseases. Can J Gastroenterol Hepatol. 2018;2018:4687041. doi: 10.1155/2018/4687041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Franks TJ, Burton DL, Simpson MD. Patient medication knowledge and adherence to asthma pharmacotherapy: a pilot study in rural Australia. Ther Clin Risk Manag. 2005;1(1):33–38. doi: 10.2147/tcrm.1.1.33.53598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tomar SK, Kedia S, Singh N, Upadhyay AD, Kamat N, Bopanna S, et al. Higher education, professional occupation, and upper socioeconomic status are associated with lower adherence to medications in patients with inflammatory bowel disease. JGH Open. 2019;3(4):302–309. doi: 10.1002/jgh3.12160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Haaland D, Day AS, Otley A. Development and validation of a pediatric IBD knowledge inventory device: the IBD-KID. J Pediatr Gastroenterol Nutr. 2014;58(3):313–319. doi: 10.1097/MPG.0000000000000210. [DOI] [PubMed] [Google Scholar]
- 22.Fishman LN, Houtman D, van Groningen J, Arnold J, Ziniel S. Medication knowledge: an initial step in self-management for youth with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2011;53(6):641–645. doi: 10.1097/MPG.0b013e3182285316. [DOI] [PubMed] [Google Scholar]
- 23.Tiao DK, Chan W, Jeganathan J, Chan JT, Perry J, Selinger CP, et al. Inflammatory bowel disease pharmacist adherence counseling improves medication adherence in Crohn's disease and ulcerative colitis. Inflamm Bowel Dis. 2017;23(8):1257–1261. doi: 10.1097/MIB.0000000000001194. [DOI] [PubMed] [Google Scholar]